
Submitted:
22 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Background: Skeletal deep bite malocclusion (Angle Class II division 2) is a prevalent vertical skeletal discrepancy characterized by excessive anterior overbite and a hypodivergent craniofacial growth pattern. Although its clinical features are well documented, the contribution of cranial base morphology to mandibular growth direction during active development remains incompletely understood. Objective: This longitudinal study aimed to evaluate the relationships between cranial base morphology and maxillofacial growth patterns in growing patients with skeletal deep bite malocclusion compared with subjects presenting Angle Class I dentoalveolar anomalies. Materials and Methods: A retrospective longitudinal cohort of 96 pediatric patients aged 7–10 years was analyzed, comprising 54 subjects with skeletal deep bite malocclusion and 42 controls. A total of 298 standardized lateral cephalometric radiographs obtained over an average follow-up period of 24 months were evaluated. Twenty-two cephalometric parameters were measured, including cranial base, linear, and angular maxillofacial variables. Intergroup comparisons were performed using parametric tests, while longitudinal changes were assessed through repeated-measures analysis. Effect sizes and multiple regression modeling were used to determine predictors of skeletal discrepancy severity. Results: The deep bite group demonstrated a characteristic hypodivergent growth pattern, including significantly reduced mandibular plane angle, decreased gonial angle, and diminished lower anterior facial height (p < 0.001). Mandibular body length was slightly increased, indicating predominant horizontal growth rather than mandibular deficiency. Cranial base analysis revealed moderate reductions in posterior cranial base angulation and anterior cranial base length. Regression analysis identified mandibular plane angle, gonial angle, and lower anterior facial height as the strongest predictors of skeletal deep bite severity (R² = 0.58). Longitudinal evaluation confirmed progressive forward mandibular rotation and reduced vertical growth rate. Conclusions: Skeletal deep bite malocclusion is primarily determined by a hypodivergent growth pattern characterized by reduced vertical facial development and forward mandibular rotation. Cranial base morphology plays a secondary modulatory role by influencing mandibular growth direction. Early identification of reduced vertical growth indicators may improve risk assessment and enable timely interceptive orthodontic interventions.
Keywords:
skeletal deep bite
; cranial base morphology
; hypodivergent growth pattern
; mandibular rotation
; cephalometric analysis
; longitudinal craniofacial growth
1. Introduction
Skeletal deep bite malocclusion (Angle Class II division 2) is a complex dento-maxillary anomaly characterized by excessive vertical overlap of the anterior teeth, associated with skeletal, dentoalveolar, and functional disturbances [1,2] (Figure 1). This condition is among the most frequently encountered vertical malocclusions in orthodontic practice and has significant implications for craniofacial growth, functional occlusion, and long-term treatment stability.
Epidemiological studies report a worldwide prevalence of approximately 21%, with considerable variability ranging from 8% to 51% depending on diagnostic criteria, age group, and ethnic background. It affects nearly one-fifth of children and approximately 13% of adults, underscoring its substantial clinical relevance and its potential impact on craniofacial development during active growth phases [1,2,3].
Although skeletal deep bite is highly prevalent, its etiopathogenesis remains complex and multifactorial, involving interactions between cranial base morphology, mandibular growth direction, and vertical facial development. Its etiopathogenesis is multifactorial, involving genetic predisposition, growth disturbances, and environmental influences [1,2,3,4]. Among these, hereditary and genetic factors are widely recognized as primary determinants, particularly through their role in regulating craniofacial growth patterns [5]. Despite its high prevalence, the developmental mechanisms underlying skeletal deep bite remain incompletely understood, particularly regarding the role of cranial base morphology in shaping mandibular growth patterns during active growth stages [1,2,3,4,5].
Embryological studies have demonstrated that genetic influences strongly govern both the rate and direction of development of cranial base structures [2,5,6]. The cranial base serves as a central growth matrix that provides spatial orientation for the maxillofacial complex [6,7]. Consequently, even subtle alterations in its morphology may have significant consequences for sagittal and vertical skeletal relationships [8].
Several researchers emphasized the role of altered ossification rhythms of cranial base synchondroses in the development of dento-maxillary anomalies [8,9]. According to this concept, disturbances in synchondrosis growth may lead to dimensional and positional modifications of the maxilla and mandible through changes in cranial base flexure, thereby influencing the development of occlusal relationships [10,11].
Although numerous investigations have attempted to clarify the involvement of cranial base morphology in the development of skeletal deep bite malocclusion (Angle Class II division 2), the underlying mechanisms remain insufficiently elucidated. Published findings are heterogeneous, reflecting differences in study design, age groups, and cephalometric methodologies [10,11,12].
Most available studies focus primarily on adolescents or adults, while longitudinal analyses conducted during earlier active growth phases are relatively scarce. This limitation is particularly important, as etiopathogenic factors exert their strongest influence during early craniofacial development [2,4,6].
The present study was therefore designed to investigate the correlations between cranial base morphology and maxillofacial development in growing patients with skeletal deep bite malocclusion, compared with individuals presenting dento-maxillary anomalies classified as Angle Class I. The research also aimed to evaluate age- and sex-related variations and to compare the obtained findings with previously published data.
2. Materials and Methods
2.1. Ethical Approval
This retrospective longitudinal cohort study was conducted between January 2021 and December 2025 in the Department of Orthodontics at the University of Medicine, Pharmacy, Science and Technology “George Emil Palade” of Târgu Mureș. Ethical approval was obtained from the institutional Ethics Committee (Approval No. 2709/27.12.2020), and written informed consent was secured from the parents or legal guardians of all participants before inclusion.
2.2. Study Design and Population
A longitudinal observational comparative design was employed to evaluate craniofacial growth patterns in a cohort of pediatric patients undergoing orthodontic assessment. The sample consisted of 96 subjects in active growth stages who were monitored between 2022 and 2024 at the Orthodontics and Dentofacial Orthopedics Clinic.
The longitudinal framework enabled serial evaluation of craniofacial development using standardized lateral cephalometric radiographs obtained at multiple time points during growth. In total, 298 radiographs were analyzed.
Participants were aged between 7 and 10 years at baseline. Based on clinical examination and cephalometric diagnosis, subjects were allocated into two groups:
- Study group: 54 patients presenting skeletal deep bite malocclusion (Angle Class II division 2)
- Control group: 42 patients presenting Angle Class I dentoalveolar malocclusions without skeletal sagittal discrepancies
The unequal group distribution reflected clinical recruitment patterns rather than sampling bias. Age and sex distribution were comparable between groups.
Exclusion criteria included genetic syndromes, metabolic disorders, craniofacial malformations, systemic growth disturbances, and previous orthodontic treatment.
2.3. Cephalometric Analysis
Each participant underwent between two and four lateral cephalometric radiographic examinations during the observation period, with an average follow-up duration of approximately 24 months. Radiographs were obtained at clinically indicated intervals corresponding to active growth phases.
The presence of a defined skeletal deep bite:
- overbite greater than 4 mm,
- decreased mandibular plane angle (FMA < 22°),
- reduced lower anterior facial height relative to age- and sex-matched normative standards.
Cephalometric evaluation included 22 parameters comprising four cranial base measurements and eighteen maxillofacial linear and angular variables. All measurements were performed on digital lateral cephalograms using standardized reference planes and were compared with established normative values for the Caucasian pediatric population.
To assess measurement reliability, 30 randomly selected cephalograms were re-analyzed after a two-week interval. Method error was calculated using Dahlberg’s formula, and intra-class correlation coefficients were computed. All variables demonstrated excellent reproducibility, with ICC values exceeding 0.90.
2.4. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics software.
Normality of variable distribution was evaluated using the Shapiro–Wilk test. Descriptive statistics included means, standard deviations, and 95% confidence intervals.
Intergroup comparisons were conducted using independent-samples t-tests and analysis of variance, as appropriate, while categorical variables were assessed using chi-square tests. Longitudinal changes were evaluated using repeated-measures analysis.
Pearson correlation coefficients were calculated to examine relationships between cranial base parameters and maxillofacial measurements. Effect sizes were quantified using Cohen’s d to assess the magnitude of intergroup differences.
Multiple linear regression analysis was performed to identify predictors of skeletal discrepancy severity. Model assumptions were verified through residual analysis, multicollinearity diagnostics, and variance inflation factor evaluation.
A priori power analysis indicated that a minimum of 34 subjects per group was required to detect moderate effect sizes with 80% statistical power at a significance level of 0.05.
Statistical significance was set at p < 0.05. To mitigate the potential impact of multiple comparisons, statistical findings were interpreted in conjunction with effect sizes and biological plausibility.
3. Results
3.1. Sample Characteristics and Data Distribution
The longitudinal cohort consisted of 96 patients contributing a total of 298 standardized lateral teleradiographs obtained across multiple observation time points. The unequal distribution between the study and control groups reflected the clinical recruitment process rather than sampling bias. The study group included 54 patients presenting the studied skeletal malocclusion features. The control group comprised subjects presenting Angle Class I dento-alveolar malocclusions without skeletal sagittal discrepancies.
Age distribution showed no statistically significant differences between groups (p > 0.05), ensuring comparability in growth stage. Sex distribution was balanced.
Before inferential analysis, data normality was assessed using the Shapiro–Wilk test, which confirmed that the majority of variables followed a normal distribution (p > 0.05). Variables that demonstrated mild deviations from normality were examined through skewness and kurtosis indicators and retained due to the robustness of parametric tests in samples exceeding 30 subjects.
The longitudinal nature of the dataset allowed evaluation of both structural differences and developmental trends, strengthening the interpretive power of the findings.
3.2. Cranial Base Parameters
The cranial base analysis illustrated in Table 1 demonstrated a modest but statistically significant reduction in posterior cranial base angulation in the deep bite group, suggesting a more flexed cranial base configuration. This morphological characteristic may contribute to anterior mandibular positioning and forward rotational growth.
The slightly shorter anterior cranial base length observed in the study group further supports the concept that cranial base morphology may influence mandibular spatial orientation indirectly by modifying skeletal growth vectors. However, effect sizes remained moderate, indicating that cranial base morphology likely acts as a secondary modulating factor rather than a primary etiological determinant.
3.3. Maxillofacial Linear Parameters
Linear measurements (Table 2) demonstrated a consistent pattern of reduced vertical facial dimensions in the deep bite group, particularly in lower anterior facial height (N-Gn and Nsa-Gn), which exhibited large effect sizes. These findings confirm a hypodivergent growth pattern characterized by reduced vertical facial development.
Conversely, mandibular body length (Go-Gn) showed a mild increase, suggesting that deep bite morphology is not associated with mandibular deficiency but rather with horizontal growth predominance and reduced vertical development.
3.4. Angular Maxillofacial Parameters
Angular measurements (Table 3) revealed a characteristic hypodivergent skeletal pattern in the deep bite group. The significantly reduced FMA and gonial angles exhibited the largest effect sizes, confirming a horizontal mandibular growth pattern with forward rotation.
The increased facial axis and mandibular prognathism indicators further support the presence of anterior rotational growth. These findings collectively demonstrate that skeletal deep bite is primarily associated with reduced vertical facial development and forward mandibular rotation rather than sagittal maxillary displacement.
3.5. Regression Analysis
The regression model explained 58% of the variance (R² = 0.58) and identified key predictors:
- FMA (β = −0.47, p < 0.001)
- Gonial angle (β = −0.41, p < 0.001)
- Lower anterior facial height (β = −0.36, p = 0.003)
These results indicate that reduced vertical growth parameters are the primary determinants of skeletal deep bite severity.
3.6. Longitudinal Growth Trends
Repeated-measures analysis confirmed:
- Facial height increased in both groups (p < 0.001)
- Growth increase was significantly smaller in the deep bite group
- Mandibular plane angle showed progressive decrease, consistent with forward rotational growth
4. Discussion
4.1. Study Rationale and Scientific Context
Clarifying the determinants of craniofacial growth remains a central challenge in orthodontics, as skeletal malocclusions rarely originate from isolated anatomical variations [1,2,13]. Instead, they arise from complex interactions among cranial base morphology, mandibular growth direction, vertical facial development, and genetic regulatory mechanisms [5,14]. Among vertical discrepancies, skeletal deep bite is particularly difficult to manage because of its multifactorial origin and its strong association with disturbances in growth pattern [3,5].
A key motivation for this longitudinal investigation was the limited number of studies that simultaneously examine cranial base morphology and maxillofacial growth dynamics during active developmental periods. Classical cephalometric investigations, including those by Björk, Jarabak, and Enlow, have primarily relied on cross-sectional designs, which provide important morphological information but cannot adequately describe growth trajectories [15,16,17,18]. Consequently, the temporal relationship between cranial base development and mandibular growth direction remains incompletely understood [19].
The longitudinal design of the present study allowed assessment of both structural differences and progressive growth changes within a pediatric cohort. The analysis of nearly 300 standardized teleradiographs enabled evaluation of craniofacial growth patterns over time, improving the ability to distinguish true developmental mechanisms from static anatomical associations.
The focus on cranial base morphology is justified by its role as a structural framework guiding maxillofacial development. Variations in its angulation or length may influence spatial positioning of the jaws and contribute to mandibular rotational patterns [19,20]. Although associations between cranial base characteristics and skeletal malocclusions have been reported, their magnitude and clinical significance remain debated [21].
The present findings indicate that cranial base features act primarily as modulatory rather than primary etiological factors in skeletal deep bite development [5,21]. This observation supports contemporary growth models emphasizing mandibular rotational patterns as the dominant determinants of vertical skeletal relationships [15,16,17,18,19].
4.2. Interpretation of Major Findings
One of the most consistent observations in this study was the presence of a hypodivergent skeletal pattern among deep bite patients [3]. Reduced mandibular plane angle, decreased gonial angle, and diminished lower anterior facial height collectively reflect a horizontal growth tendency characterized by forward mandibular rotation [16,17,18].
These results are consistent with classical growth rotation theories proposed by Björk, who described forward mandibular rotation as a defining characteristic of deep bite morphology [15,16]. Similar conclusions were drawn from implant studies conducted by Skieller, which demonstrated a strong association between forward mandibular rotation, reduced vertical development, and increased incisal overlap [22].
The substantial effect sizes observed for lower anterior facial height and mandibular plane angle further highlight the central role of vertical growth deficiency in deep bite development. These findings align with previous reports emphasizing that insufficient vertical facial growth, rather than excessive dentoalveolar eruption alone, is a primary contributor to deep bite malocclusion [23,24].
Mandibular body length was slightly increased in the study group, indicating that deep bite is not typically associated with mandibular deficiency but rather with altered growth direction [1,25]. Regression analysis reinforced this conclusion, identifying mandibular plane angle and gonial angle as the strongest predictors of skeletal deep bite severity, consistent with previous multivariate studies on vertical skeletal relationships [2,3,4,25].
Cranial base parameters demonstrated smaller yet statistically significant differences, particularly in posterior cranial base angulation and anterior cranial base length. This supports Enlow’s concept that cranial base morphology influences mandibular positioning indirectly by modifying spatial growth conditions rather than acting as a primary etiological factor [17]. Such effects likely occur through subtle modulation of mandibular growth vectors [15,22,27].
4.3. Significance of Longitudinal Growth Findings
A major strength of this study lies in demonstrating that skeletal deep bite represents an evolving developmental pattern rather than a static anatomical condition [1,28]. Longitudinal analysis showed that although facial height increased in both groups during growth, vertical development progressed at a significantly slower rate in the deep bite cohort.
These findings indicate that skeletal deep bite results from relative vertical growth deficiency rather than complete growth absence [28,29]. Similar conclusions have been reported in long-term studies showing progressive accentuation of hypodivergent patterns during pubertal development due to continued forward mandibular rotation.
The observed progressive reduction in mandibular plane angle further supports the concept that deep bite severity increases over time [1,2,3,4,15,16,17,18,28,29]. This dynamic process underscores the importance of early monitoring, as opportunities for effective orthopedic intervention diminish with skeletal maturation.
4.4. Clinical Implications
The clinical relevance of these findings is considerable, particularly for early diagnosis and treatment planning. Reduced lower facial height and forward mandibular rotation emerge as key indicators for identifying patients at risk of developing skeletal deep bite.
Early evaluation of mandibular growth direction should therefore be a fundamental component of orthodontic screening. Recognition of hypodivergent growth patterns during mixed dentition enables the timely implementation of interceptive strategies aimed at promoting vertical development [30,31].
The results also emphasize the importance of including cranial base assessment in cephalometric analysis. Although often treated as a stable reference structure, subtle morphological variations may influence mandibular positioning and growth orientation [32,33].
From a therapeutic standpoint, the findings support treatment approaches focused on stimulating vertical development. Orthopedic appliances that encourage posterior dentoalveolar eruption and modify mandibular rotation may be particularly beneficial in hypodivergent patients. Orthodontic mechanics designed to increase lower facial height may also enhance long-term stability [34,35].
4.5. Biological and Scientific Implications
Beyond clinical applications, the present results contribute to understanding craniofacial growth biology. The predominance of forward mandibular rotation supports the concept that skeletal deep bite reflects systemic growth pattern variation rather than isolated dentoalveolar abnormalities [1,2,3,4,28,29].
These findings align with contemporary models emphasizing the interaction between genetic predisposition and functional environmental influences, including muscle activity and occlusal forces [1,2,3,4]. The secondary role of cranial base morphology further highlights the integrated nature of craniofacial development [7,8,9,10,11,12,13,14,19].
Methodologically, the combination of longitudinal cephalometric analysis with advanced statistical modeling strengthens the reliability and clinical relevance of the results. Given the exploratory nature of comparisons, findings were interpreted using effect sizes and biological plausibility rather than strict multiple-testing corrections to reduce Type I error risk.
4.6. Limitations and Future Directions
Several limitations should be acknowledged. The retrospective design may introduce selection bias, although the longitudinal approach partially mitigates this concern. Unequal group sizes may affect statistical precision.
The use of two-dimensional cephalometry represents another limitation, as it cannot fully capture the complexity of craniofacial morphology. Future studies employing three-dimensional imaging techniques could provide more comprehensive insights into spatial growth patterns [36].
5. Conclusions
This longitudinal investigation demonstrates that skeletal deep bite malocclusion is primarily characterized by a hypodivergent growth pattern involving reduced vertical facial development and forward mandibular rotation. Cranial base morphology exerts a secondary modulatory influence on mandibular growth direction.
The progressive nature of these skeletal changes highlights the importance of early diagnosis and timely intervention. Identification of key morphological predictors may improve orthodontic risk assessment, treatment planning, and long-term outcomes.
References
- Watted, N.; Lone, I.M.; Zohud, O.; Midlej, K.; Proff, P.; Iraqi, F.A. Comprehensive Deciphering the Complexity of the Deep Bite: Insight from Animal Model to Human Subjects. J. Pers. Med. 2023, 13, 1472. [CrossRef]
- Pasciuti, E.; Coloccia, G.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Bordea, I.R.; Cardarelli, F.; Di Venere, D.; Inchingolo, F.; Dipalma, G. Deep Bite Treatment with Aligners: A New Protocol. Appl. Sci. 2022, 12, 6709. [CrossRef]
- Piancino, M.G.; Tortarolo, A.; Di Benedetto, L.; Crincoli, V.; Falla, D. Chewing Patterns and Muscular Activation in Deep Bite Malocclusion. J. Clin. Med. 2022, 11, 1702. [CrossRef]
- Bardideh, E.; Tamizi, G.; Shafaee, H.; Rangrazi, A.; Ghorbani, M.; Kerayechian, N. The Effects of Intrusion of Anterior Teeth by Skeletal Anchorage in Deep Bite Patients; A Systematic Review and Meta-Analysis. Biomimetics 2023, 8, 101. [CrossRef]
- Hartsfield, J.K., Jr.; Jacob, G.J.; Morford, L.A. Heredity, genetics and orthodontics—How much has this research really helped? Semin. Orthod. 2017, 23, 336–347. [CrossRef]
- Rasol, O.A.; Hajeer, M.Y.; Sultan, K.; et al. Evaluation of the best method for orthodontic correction of skeletal deep bites in growing patients: A systematic review. Cureus 2024, 16, e62666. [CrossRef]
- Lieberman, D.E.; Hallgrímsson, B.; Liu, W.; Parsons, T.E.; Jamniczky, H.A. Spatial packing, cranial base angulation, and craniofacial shape variation in the mammalian skull: Testing a new model using mice. J. Anat. 2008, 212, 720–735. [CrossRef]
- Polat, O.O.; Kaya, B. Changes in cranial base morphology in different malocclusions. Orthod. Craniofac. Res. 2007, 10, 216–221. [CrossRef]
- Cendekiawan, T.; Wong, R.W.K.; Rabie, A.B.M. Relationships between cranial base synchondroses and craniofacial development: A review. Open Anat. J. 2010, 2, 67–75.
- Almeida, K.C.M.; Raveli, T.B.; Vieira, C.I.V.; Santos-Pinto, A.D.; Raveli, D.B. Influence of the cranial base flexion on Class I, II and III malocclusions: A systematic review. Dent. Press J. Orthod. 2017, 22, 56–66. [CrossRef]
- Al-Gumaei, W.S.; Al-Attab, R.; Al-Tayar, B.; et al. Comparison of spheno-occipital synchondrosis maturation stages with three-dimensional assessment of mandibular growth. BMC Oral Health 2022, 22, 654. [CrossRef]
- Richtsmeier, J.T.; Deleon, V.B. Morphological integration of the skull in craniofacial anomalies. Orthod. Craniofac. Res. 2009, 12, 149–158. [CrossRef]
- Meikle, M.C. Remodeling the dentofacial skeleton: The biological basis of orthodontics and dentofacial orthopedics. J. Dent. Res. 2007, 86, 12–24. [CrossRef]
- Moreno Uribe, L.M.; Miller, S.F. Genetics of the dentofacial variation in human malocclusion. Orthod. Craniofac. Res. 2015, 18 (Suppl. 1), 91–99. [CrossRef]
- Björk, A. Prediction of mandibular growth rotation. Am. J. Orthod. 1969, 55, 585–599. [CrossRef]
- Björk, A.; Skieller, V. Normal and abnormal growth of the mandible: A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur. J. Orthod. 1983, 5, 1–46. [CrossRef]
- Enlow, D.H.; Hans, M.G. Essentials of Facial Growth; WB Saunders: Philadelphia, PA, USA, 1996; pp. 57–156.
- Balderas-González, M.E.; Cruz-Hervert, L.P.; Martínez-Contreras, S.P.; García-Lee, V.; Ortiz-Sánchez, J.D.; Rodríguez-Chávez, J.A.; Jiménez-Corona, M.E.; García-García, G.; Kiseri-Kubati, J.; Sánchez-García, S. Predictability of a mandibular corpus length multivariate model integrating Björk-Jarabak measurements and the cephalometric norm. Cureus 2025, 17, e87864. [CrossRef]
- Myers, M.; Brown, M.D.; Badirli, S.; Eckert, G.J.; Johnson, D.H.; Turkkahraman, H. Long-term predictive modelling of the craniofacial complex using machine learning on 2D cephalometric radiographs. Int. Dent. J. 2025, 75, 236–247. [CrossRef]
- Kasai, K.; Moro, T.; Kanazawa, E.; Iwasawa, T. Relationship between cranial base and maxillofacial morphology. Eur. J. Orthod. 1995, 17, 403–410. [CrossRef]
- Alhazmi, N.; Almihbash, A.; Alrusaini, S.; Bin Jasser, S.; Alghamdi, M.S.; Alotaibi, Z.; Alshamrani, A.M.; Albalawi, M. The association between cranial base and maxillomandibular sagittal and transverse relationship: A CBCT study. Appl. Sci. 2022, 12, 9199. [CrossRef]
- Skieller, V.; Björk, A.; Linde-Hansen, T. Prediction of mandibular growth rotation evaluated from a longitudinal implant sample. Am. J. Orthod. 1984, 86, 359–370. [CrossRef]
- Nanda, S.K. Growth patterns in subjects with long and short faces. Am. J. Orthod. Dentofacial Orthop. 1990, 98, 247–258. [CrossRef]
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. Longitudinal growth changes in subjects with deepbite. Am. J. Orthod. Dentofacial Orthop. 2011, 140, 202–209. [CrossRef]
- Lone, I.M.; Zohud, O.; Midlej, K.; Proff, P.; Watted, N.; Iraqi, F.A. Skeletal class II malocclusion: From clinical treatment strategies to the roadmap in identifying the genetic bases of development in humans with the support of the Collaborative Cross mouse population. J. Clin. Med. 2023, 12, 5148. [CrossRef]
- Jacob, H.B.; Buschang, P.H. Mandibular growth comparisons of Class I and Class II division 1 skeletofacial patterns. Angle Orthod. 2014, 84, 755–761. [CrossRef]
- Agarwal, A.; Pandey, H.; Bajaj, K.; Pandey, L. Changes in cranial base morphology in Class I and Class II division 1 malocclusions. J. Int. Oral Health 2013, 5, 39–42.
- Kim, J.S.; Park, J.H.; Heo, S.; Chae, J.M. Biomechanical and clinical considerations in deep bite treatment using temporary skeletal anchorage devices. J. World Fed. Orthod. 2024, 13, 10–17. [CrossRef]
- Ferrillo, M.; Pandis, N.; Fleming, P.S. The effect of vertical skeletal proportions on overbite changes in untreated adolescents: A longitudinal evaluation. Angle Orthod. 2024, 94, 25–30. [CrossRef]
- Dinu, S.; Igna, A.; Petrescu, E.L.; Braila, E.B.; Dinu, D.C.; Horhat, R.M.; Mihai, C.; Traila, I.A.; Nica, D.F.; Popa, M. Timing of orthodontic intervention for pediatric class II malocclusion: A systematic review on early vs. late treatment outcomes. Children 2025, 12, 1533. [CrossRef]
- Yang, G.; Xiang, X.; Tong, X.; Li, Y.; Liu, Y. Mandibular response after rapid maxillary expansion in mixed dentition children with different vertical growth patterns: A retrospective study. J. Clin. Pediatr. Dent. 2024, 48, 69–78. [CrossRef]
- Anitha, A.M.; Manohar, M.R. Comparative evaluation of cranial base length and flexure on facial parameters in hypodivergent, normodivergent and hyperdivergent patients: A retrospective cephalometric study. J. Contemp. Dent. Pract. 2023, 24, 244–249. [CrossRef]
- Graf, C.C.; Dritsas, K.; Ghamri, M.; Gkantidis, N. Reliability of cephalometric superimposition for the assessment of craniofacial changes: A systematic review. Eur. J. Orthod. 2022, 44, 477–490. [CrossRef]
- Hourfar, J.; Kinzinger, G.S.M.; Frye, L.; Lisson, J.A. Effects of fixed functional orthodontic treatment in hypodivergent and hyperdivergent class II patients—A retrospective cephalometric investigation. Clin. Oral Investig. 2023, 27, 4773–4784. [CrossRef]
- Burashed, H. Changes in the vertical dimension after orthodontic treatment in response to different premolar extraction patterns. Cureus 2023, 15, e38893. [CrossRef]
- Spillers, T., 3rd; Walma, D.A.C.; Spillers, J.D., Jr.; Kau, C.H.; Christou, T. Deep bite correction with the Invisalign system: A case-series study. Eur. J. Dent. 2026, 20, 155–163. [CrossRef]
Figure 1.
Skeletal deep bite maloclussion, exo-endooral aspects, and lateral teleradiography.
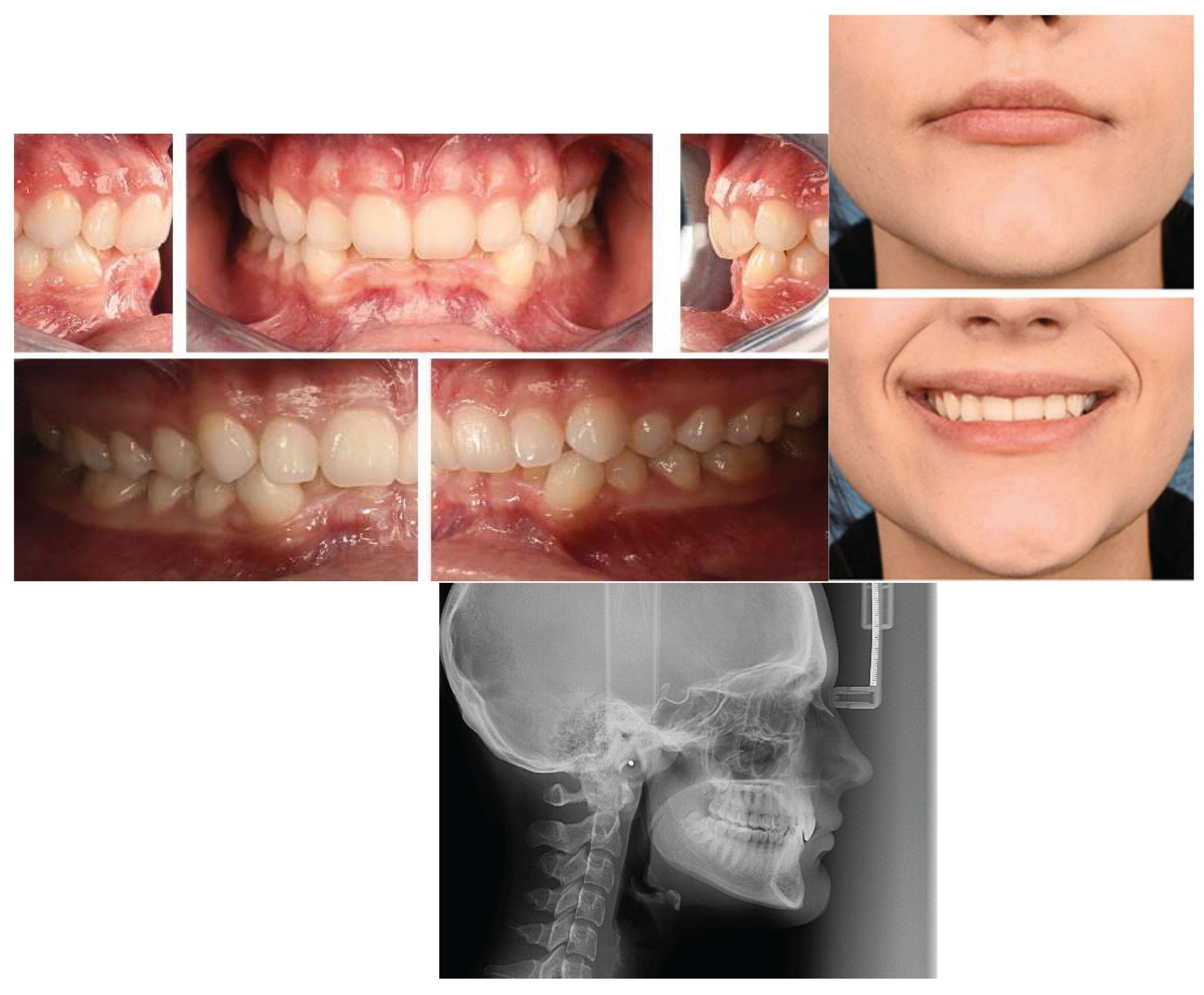

Table 1.
Cranial Base Measurements.
| Parameter | Control Mean | Study Mean | p-value | Cohen’s d |
| ∠N-S-Ba (°) | 127.8 | 126.9 | ns | 0.18 |
| ∠N-Op-Ba (°) | 14.8 | 13.2 | 0.018 | 0.52 |
| S-Ba (mm) | 37.3 | 36.5 | ns | 0.26 |
| S-N (mm) | 60.0 | 58.6 | 0.031 | 0.48 |
Table 2.
Linear Maxillofacial Measurements.
| Parameter | Control | Study | p-value | Effect Size |
| Nsa-Nsp | 42.5 | 39.8 | 0.004 | 0.68 |
| Go-Gn | 57.0 | 59.2 | 0.028 | 0.46 |
| S-Nsp | 39.0 | 35.5 | <0.001 | 0.92 |
| N-Nsa | 40.5 | 38.0 | 0.010 | 0.62 |
| Nsa-Gn | 52.5 | 47.6 | <0.001 | 1.05 |
| N-Gn | 92.0 | 86.3 | <0.001 | 1.12 |
| Nsp-Go | 33.8 | 32.4 | ns | 0.29 |
| Kdl-Go | 40.0 | 41.5 | 0.040 | 0.42 |
Table 3.
Angular Measurements.
| Parameter | Control | Study | p-value | Effect Size |
| ∠N.S.NsaNsp | 6.8 | 5.4 | 0.011 | 0.58 |
| ∠N.S-M | 31.5 | 29.2 | 0.022 | 0.49 |
| ∠N.Nsa-Gn | 159.3 | 165.8 | <0.001 | 1.02 |
| ∠S.Nsp-Go | 104.8 | 98.6 | <0.001 | 1.18 |
| ∠N.Nsa-Pg | 165.0 | 171.2 | <0.001 | 1.10 |
| ∠Go | 111.0 | 104.3 | <0.001 | 1.35 |
| ∠SNA | 81.3 | 80.5 | ns | 0.22 |
| ∠ANB | 3.0 | 5.2 | 0.008 | 0.67 |
| ∠FMA | 24.0 | 18.5 | <0.001 | 1.42 |
| ∠Nsa.Nsp-M | 24.8 | 21.3 | 0.004 | 0.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



