
Submitted:
24 February 2026
Posted:
28 February 2026
You are already at the latest version
Abstract
Overweight and obesity during pregnancy are associated with increased maternal and neonatal risks, yet scalable interventions addressing the psychological processes underlying health behaviours remain limited. This study describes the development and formative evaluation of DEMETRA, a chatbot delivering an Acceptance and Commitment Therapy (ACT)–informed intervention to promote healthier lifestyles in pregnant women. In line with Phase 1 of the Obesity-Related Behavioral Intervention Trials framework, a multidisciplinary team developed a six-session digital program delivered via a rule-based virtual assistant. A mixed-methods design was employed to assess acceptability, usability, and perceived relevance. Sixteen stakeholders (psychologists, communication experts, nutritionists, clinicians, and women) participated in iterative testing; 15 completed quantitative measures (Semantic Differential scales, uMARS, BUS-11) and 16 completed semi-structured interviews. Non-parametric analyses indicated significantly positive evaluations across most communication and content domains, particularly clarity and language appropriateness, whereas session duration and several engagement-related dimensions did not significantly differ from neutrality. Qualitative findings confirmed strengths in clarity, non-stigmatising tone, and multimedia support, while identifying limited personalisation and message pacing as key areas for refinement. Overall, findings support the feasibility and acceptability of translating ACT principles into a chatbot-delivered antenatal intervention and justify progression to subsequent optimisation and early efficacy testing phases.
Keywords:
ACT
; well-being
; pregnancy
; overweight
; eHealth
; mHealth
; development
; usability
; user-centred design
1. Background
Overweight and obesity during pregnancy represent a major public health concern, as they are associated with increased risks of gestational diabetes, hypertensive disorders, cesarean delivery, and adverse neonatal outcomes (Almutairi et al. 2024; Brunner et al. 2025). Moreover, excess weight in pregnancy often persists postpartum and contributes to long-term maternal obesity and metabolic complications (Catalano and Shankar 2017). Interventions targeting nutrition and physical activity have shown some effectiveness in mitigating these risks by preventing excessive gestational weight gain (Shieh et al. 2018; Kurnaz and Karaçam 2025), even when delivered in a mobile health (m-Health) format (Sari et al. 2025).
Yet the implementation of interventions for pregnant women remains challenging due to, among other factors, low adherence, time constraints, and limited access to in-person programs (Bowden et al. 2023; Ernst et al. 2025; Lelorain et al. 2024).
In recent years, digital health technologies, including mobile applications and conversational agents (virtual assistants), have gained increasing attention as scalable tools to deliver psychological interventions (Conrad 2024; Torous et al. 2025). Virtual assistants can provide real-time guidance, foster engagement, and overcome barriers such as stigma, geographic distance, or lack of specialized providers (Conrad 2024; Adler and Van Brunt 2025). Early studies suggest that such technologies may enhance user adherence and satisfaction, particularly in vulnerable populations such as pregnant women.
Acceptance and Commitment Therapy (ACT) has emerged as a transdiagnostic behavioral approach effective in promoting psychological flexibility and sustainable health behavior change (Dindo et al. 2017; Hayes et al. 2013; Yıldız 2020). Promising results regarding ACT-based interventions for supporting weight management, physical activity, and dietary improvements in non-pregnant populations have been found, generating a growing interest in the development of treatment protocols aimed at overweight and obese populations (Iturbe et al. 2022; Chew et al. 2023; Pitil and Ghazali 2024; Schumacher et al. 2025). Preliminary evidence also suggests potential benefits of ACT-based interventions in perinatal health contexts (Waters et al. 2020; Howard et al. 2023), even in digital format (Ashton et al. 2025). However, little is known about the feasibility and acceptability of ACT interventions specifically designed for overweight pregnant women.
1.1. An Acceptance and Commitment Therapy Intervention to Promote Healthier Behaviors and Lifestyles in Overweight Pregnant Women
Interest in the development of ACT-based, digital interventions is growing. ACT-based digital interventions have already been developed for patients suffering from chronic health conditions (Gentili et al. 2021; Levin et al. 2025; Herbert et al. 2022), depression (Lappalainen et al. 2015; Apolinário-Hagen et al. 2024), anxiety (Tobias et al. 2022; Kelson et al. 2019), distressed university students (Levin et al. 2020), as well as for stress management in the general population (Fietta et al. 2024; Klimczak et al. 2023) ACT interventions aimed at either pregnant women (Howard et al. 2023) or overweight and obese populations have also been developed (Schumacher et al. 2025), even in a digitalized format, with promising results (Ashton et al. 2025; Levin et al. 2021). Yet, no attempt has been made in the development of such an intervention for overweight or obese pregnant women, even though they are a growing and at-risk population (Kent et al. 2024).
Different guidelines for the care of pregnant, overweight or obese women have been developed, and while some issues remain debated (e.g., optimal Gestational Weight Gain, National Institute for Health and Care Excellence (NICE), (NICE, 2025) , there is an agreement regarding the importance of physical activity and healthy eating for managing weight related risks for both the mother and the child (Ahmad et al. 2025; Jangra et al. 2025). Therefore, we sought to develop a psychoeducational and motivational intervention rooted in ACT to support pregnant women in their struggle to adopt a healthier lifestyle (Dencker et al. 2016; Jelsma et al. 2016), as well as to provide healthcare workers with a low-cost, scalable intervention to support their efforts.
The content architecture of the digital chatbot intervention was informed by two primary resources: The diet trap (Lillis et al. 2014) and Healthy habits sucks (Lee-Baggley 2019). The former has been successfully employed in interventions for overweight and obese adults, demonstrating benefits in reducing weight-related self-stigma and promoting healthy behaviors (Potts et al. 2022). While we are not aware of empirical evaluations of interventions directly based on Lee-Baggley (2019), the inclusion of content from both sources was guided by the characteristics and needs of our target population. In particular, since intentional weight loss is not recommended during pregnancy (NICE, 2025), the broader behavioral focus of Lee-Baggley (2019) was deemed especially suitable to avoid inadvertently over-emphasizing weight reduction. Lastly, in light of previous results highlighting the potential of using the ACT matrix (Polk and Prevedini 2017) for the development of digitalized ACT interventions (Levin et al. 2017; Krafft et al. 2019), we also employed it. To guide the inclusion of this tool in the intervention, we relied primarily on Polk et al. (2017).
The material obtained through the extraction and reformulation of the content from the aforementioned sources into concise, conversational modules suitable for chatbot delivery covers core ACT concepts - namely acceptance, cognitive defusion, present-moment awareness, values clarification, committed action and more - with a focus on the domains of nutrition and physical activity during pregnancy. The said content was developed not as a substitute for information on the importance of physical activity and healthy nutrition during pregnancy, but as motivational and psychological support for women seeking to adopt healthier habits.
1.2. Present Research
The intervention’s objective is to enhance psychological flexibility in women through ACT-based exercises to promote healthy lifestyles.
The content is delivered through a meticulously designed step-by-step process, in order to promote self-awareness, acceptance, and normalisation of internal states, stress management, and possibly promote overall improvement in psychological well-being. Once perfected based on the results of the current study, this ACT intervention will be fully available to users through digital tools. In particular, it will be delivered by a mobile application and guided by a virtual assistant, DEMETRA. The present research aims to assess the prototype of the DEMETRA chatbot, gathering feedback and needs from key stakeholders to further refine the dialogues from the perspectives of usability, accessibility, and acceptability of the chatbot-delivered intervention.
2. Materials and Methods
The design and development of the chatbot DEMETRA followed the recommendations of the Centre for eHealth Research and Disease Management, which suggests a multidisciplinary approach coupled with continuous and systematic evaluation throughout to improve uptake and impact of eHealth technologies (Van Gemert-Pijnen et al. 2011).
The ACT intervention program is developed iteratively, following the Obesity-Related Behavioral Intervention Trials (ORBIT) model (Czajkowski et al., 2015), which depicts the pathway to translate behavioral science discoveries into behavioral treatments ready for efficacy testing.
The multidisciplinary project team, comprising experts in psychology, eHealth research, and communication, held biweekly meetings during the design and development phase. A user-centred design approach ensured continuous involvement of patients, healthcare providers, and security specialists. Development followed an iterative process through i) intervention content development (identified and adjusted from the reference material) and ii) iterative software development of a prototype and formative evaluation. The development and iterative processes of the ACT-based intervention are shown in Figure 1.
The development of the intervention’s materials was led by one of the authors (AEN), a researcher and psychologist, in collaboration with a multidisciplinary team of psychologists, ACT experts, nutritionists, communication experts, and information technology experts. The team held recurrent meetings to revise the materials as they were developed.
To identify key themes and issues to address in the intervention, both psychologists and non-psychologists team members were required to read Lillis et al. (2014), Lee-Beggley, (2019) and Polk & Schoendorff (2014) to familiarize themselves with ACT’s approach to health and dietary behaviors. Group discussions coordinated by one of the ACT experts were held to make sure that there was a shared understanding of the chosen approach. Lillis et al. (2014) and Lee-Beggley (2019) were chosen for their relevance and being targeted to the general population, so as to inform the team’s communication style choices, as well as helping in identifying key themes within the health behaviors domain.
2.1. Intervention Content Development
Adapting the reference material into a digital format began with a comprehensive review of both the literature and the original manuals. Once the week-by-week thematic structure was defined, a team of psychologists with expertise in communication adapted the material into a chatbot-based, individualised digital format. The process began with the development of the chatbot’s dialogue scripts, followed by the creation of multimedia resources (videos, audio, and images) to convey key information in a more accessible, engaging format for women than text alone.
The initial intervention content was drafted and subsequently refined through iterative cycles, resulting in a six-session program delivered electronically via text, video, and images. Table 1 outlines the six sessions and their respective topics.
The intervention was designed so that DEMETRA—the chatbot—always initiates the interaction. At this stage, users cannot submit specific queries; instead, the chatbot delivers information and prompts self-reflection through targeted questions. User responses are not analysed in the current phase, as this lies outside the scope of the study.
The intervention is scheduled to span six weeks. Each session lasts approximately 10 minutes. On the designated day, DEMETRA provides the participant with psychoeducational material; at the end of each session, participants are given instructions for an exercise to be completed during the subsequent week.
2.2. Iterative Software Development and Formative Evaluation
Adapting ACT interventions through the implementation of the DEMETRA chatbot offers a novel approach to delivering psychological support. Users can participate in comprehensive and effective interventions through personalised sessions. In the initial session, users are prompted to choose one day of the week on which they wish to be contacted by DEMETRA and their preferred time slot (morning, afternoon, or evening). Based on user responses, DEMETRA provides tailored content—for example, DEMETRA asks whether the user would like to review the previous session, whether they prefer to complete a specific exercise immediately or later, and so on, with the dialogue branching accordingly.
In the first iteration, conducted in August 2025, two psychologists and two communication experts tested a preliminary prototype and provided feedback to ensure the intervention program was logically structured. At this co-design stage, the involvement of experienced professionals, alongside end users, was considered crucial. For this reason, in a subsequent study (Test 1), two additional psychologists, three communication experts and three nutritionists were involved to test the low-fidelity prototype. Later, end users were also engaged in the process (Test 2), including four women and four clinicians. Considering the stage of development of the intervention and the aim of the current study, we established the following inclusion criteria to recruit women: being pregnant or having given birth within the last 12 months, pre-pregnancy BMI < 25 and no medical or psychological complications.
Overall, a multistage evaluation of the DEMETRA prototype was conducted between October and December 2025, involving 16 participants.
2.2.1. Study Aims: Quantitative and Qualitative Components
In accordance with the ORBIT model Phase 1 (Design), the primary objective of this formative mixed-methods study was to assess the acceptability, usability, and perceived relevance of the ACT-based digital intervention delivered via the DEMETRA chatbot, prior to efficacy testing. In line with ORBIT’s emphasis on iterative optimization of intervention components, the quantitative component concentrated on early indicators of user experience and perceived value. User evaluations were collected using standardised 5-point Likert-scale instruments, and median scores were compared against a predefined benchmark corresponding to the scale midpoint (3/5). This was operationalised as the minimum threshold of acceptability. This approach enabled the research team to ascertain whether the prototype attained a satisfactory level of usability and perceived quality, sufficient to justify progression to subsequent refinement and testing phases.
The qualitative component provided a deeper, contextualised understanding of how users experienced the intervention and interacted with the chatbot, thereby complementing the quantitative findings. In particular, qualitative data were utilised to investigate the perceived clarity, tone, and appropriateness of the chatbot’s communication style; the structure, pacing, and burden of the sessions; the perceived relevance of the content to the perinatal period; and the extent to which the intervention was experienced as personalised. In accordance with the formative aims of ORBIT Phase 1, qualitative feedback was also used to identify implementation barriers, unmet user needs, and actionable suggestions for improvement. The integration of quantitative and qualitative data was intended to inform iterative refinement of both intervention content and delivery mechanisms, with the objective of optimising the DEMETRA chatbot before advancing to later phases of intervention testing.
2.2.2. Variables Identification
The quantitative evaluation focused on key domains relevant to chatbot-based digital interventions, including communication, session structure, materials, content, engagement, functionality, aesthetics, information quality, subjective quality, and perceived impact. The communication session structure, materials, and content were assessed using an ad hoc Semantic Differential scale (Osgood et al. 1957), developed to capture participants’ perceptions of tone, clarity, and overall communicative effectiveness. The remaining domains were evaluated using validated instruments, namely the User Version of the Mobile Application Rating Scale (uMARS; Stoyanov et al. 2016) and the Italian version of the Chatbot Usability Scale (BUS-11; Borsci et al. 2023).
The uMARS is a tool specifically designed for the evaluation of mobile health applications (mHealth), for which an Italian version has been validated (Morselli et al. 2021). The instrument is composed of 20 items that evaluate engagement, functionality, aesthetics, information quality, subjective quality, and perceived impact. In view of the objectives of the present study and with a view to minimising overlap with chatbot-specific usability measures, the functionality and aesthetics subscales were excluded from the analyses. The BUS-11 is a 11-item scale designed to assess user satisfaction with chatbot interactions. It encompasses accessibility and the quality of functions, the quality of conversation and information, perceived privacy and security, and response time. The scale has been validated in multiple languages, including Italian (Borsci et al., 2023) and thanks to its short length, it enables the rapid evaluation of chatbots at all stages of development.
Subsequent to the completion of the quantitative measures, a semi-structured interview was conducted to explore participants’ experiences in greater depth, with particular attention to perceived strengths, limitations, and suggestions for improvement (see Appendix B for details). The framework method ((Gale et al. 2013)) was employed to analyse the qualitative data, with a view to identifying recurrent patterns and themes that complemented and contextualised the quantitative findings. The employment of a mixed-methods approach resulted in a comprehensive formative evaluation of the DEMETRA prototype, thereby providing direction for subsequent iterations.
2.2.3. Procedure
Convenience sampling was deemed appropriate for the research purpose; therefore, participants were recruited among direct acquaintances via word of mouth, and the aim of the study was clearly stated. Participants were then contacted via email to receive the informed consent form, which included all relevant information. Only once the researchers received the signed consent form were people considered enrolled in the study.
After the enrollment, participants received detailed instructions via email on how to interact with the DEMETRA chatbot, as well as additional information regarding the testing procedure. At the same time, they received the opening session of the intervention on WhatsApp.
For the next two weeks, participants received the intervention every 48 hours, allowing them a reasonable interval to interact with the chatbot at their own pace and on their own schedules. The sessions lasted an average of 15 minutes and provided the user with readable and watchable content. They were required to interact by offering close- and open-ended questions to proceed with the conversation and foster both engagement and self-reflection. The answers provided by participants were neither collected nor analyzed in this prototyping phase, as it wasn’t required by the aim of the study.
Once the testing period ended, participants received the questionnaire via email and were invited to schedule an appointment for the final interview to further report on their expectations, preferences, and concerns regarding the solution tested. The interview questions were designed ad hoc for our study, focusing on topics relevant to the evaluation of the chatbot. The inclusion criteria for participating in the interview were: having completed the prototype test and providing consent to participate in this additional phase. The researcher conducted 16 interviews, which were then analysed and processed using qualitative tools. The conductor initially provided a brief introduction to the interview objectives. Then, participants were asked to answer a series of semi-structured questions regarding their expectations and preferences for using the chatbot. Interviews lasted approximately 15 minutes and were audio-recorded to facilitate later analysis. All data were collected in Italian and pseudonymized, with participants’ informed consent. Confidential audio recordings of semi-structured interviews were used for data analysis, and subjects were identified only by numeric codes. At the study’s conclusion, participants can request the research outcomes from the research manager.
According to Italian Law No. 3/2018, the current study did not require approval by an ethical committee, given i) it was focused on the usability of prototyped digital intervention, ii) no vulnerable group nor patient was involved (participants fell into one of the following categories: psychologists, usability experts, nutrition experts, midwives and women - pregnant or that gave birth in the previous 12 months, pre-pregnancy BMI<25, no medical or psychological complications), and iii) no sensitive health data were collected nor clinical treatment was foreseen. Nonetheless, adherence to ethical principles was ensured.
Participants were not rewarded for their participation.
2.2.4. Data Analysis
The open statistical software Jamovi (jamovi - open statistical software for the desktop and cloud, s.d.) was used to analyze the quantitative data from the Semantic Differential, the BUS-11 and the uMARS. Considering the numerosity of the sample, we used non-parametric tests: the Wilcoxon signed-rank test (W) was used instead of the one-sample t-test (King & Eckersley, 2019; Tomczak & Tomczak-Łukaszewska, 2014). Rank-biserial correlation (r) and corresponding 95% confidence intervals (CI) were reported to indicate effect size (Tomczak & Tomczak-Łukaszewska, 2014). All analysis results were considered significant with a critical P-value set at 0.05.
Qualitative data from the interviews were analyzed using the framework method (Gale et al. 2013), adopting a mainly deductive approach. Prior to analysis, an analytical framework was defined by the research group, identifying thematic categories and codes based on the key variables of the study and the topics guiding the interview questions.
The analysis of each interview began with a familiarization phase, during which audio recordings and transcripts were reviewed to ensure an overall understanding of the content. This was followed by an indexing phase, in which the researcher labeled relevant passages according to the predefined codes. Although a formal open coding phase was not conducted, instances in which the existing coding framework appeared insufficient were noted during analysis.
Following indexing, data were charted into the framework matrix, distinguished according to participant type for interpretation.
3. Results
The pilot evaluation was conducted with 16 participants, including two psychologists, three communication experts, three nutritionists, four mothers, and four clinicians. Of these, 15 responded to the questionnaire (only one mother did not respond), and 16 participated in the semi-structured interview.
The mean age of the subjects who completed the questionnaire was 35.3 years (SD = 7.92, ranging from a minimum of 26 to a maximum of 50 years).
3.1. Quantitative Results
The use of a semantic differential–based questionnaire makes it possible to examine respondents’ average positioning in relation to the four macro-variables under investigation. More specifically, regarding the sub-variables, the Wilcoxon analysis revealed several statistically significant results, as reported in Table 2.
Using a 1–5 scale with a theoretical median of 3 (neutral), participants’ ratings were overall skewed toward the positive pole. Wilcoxon one-sample tests showed statistically significant deviations above the neutral value for 8 out of 9 dimensions (p < 0.05) supporting a systematic shift toward favorable evaluations: empathy and listening (W = 103.5, p = 0.001, r = 0.971), smoothness and fluidity (W = 79.5, p = 0.015, r = 0.747), chatbot interaction (W = 93.5, p = 0.011, r = 0.781), and lexicon (W = 105.0, p < .001, r = 1.000). Similarly, content-related and multimedia dimensions were significantly above neutrality, including videos (W = 105.0, p = 0.001, r = 1.000), infographics (W = 89.0, p = 0.003, r = 0.956), overall content evaluation (W = 115.5, p = 0.002, r = 0.925), and content clarity (W = 91.0, p = 0.001, r = 1.000). The strongest descriptive and inferential signals were observed for content clarity and lexicon (highest means, medians at 4.0, and very large effect sizes), suggesting particularly favourable perceptions of comprehensibility and language appropriateness; however, the concentration of medians at 4.0 and several very large r values (≈ 1.0) may also be consistent with a degree of ceiling tendency in responses. Variability patterns further nuanced these findings: while most items showed moderate dispersion, smoothness and fluidity displayed the highest variability (SD = 0.99), indicating more heterogeneous experiences despite a positive average. In contrast to the generally positive pattern, session duration was the only dimension that did not significantly differ from neutrality (M = 3.23, SD = 0.75; Md = 3.00; W = 31.0, p = 0.328, r = 0.378), aligning with its lower central tendency values and suggesting that perceptions of time allocation remained closer to neutral. Finally, given that multiple one-sample tests were conducted (9 outcomes), the overall pattern remains strongly positive, but the small sample size and the number of comparisons warrant cautious interpretation of the comparatively higher p-values (e.g., for smoothness and chatbot interaction), whereas the lowest p-values (e.g., lexicon, clarity, videos, infographics, content evaluation, empathy) indicate particularly robust departures from neutrality.
BUS-11 results (n = 15) also supported a positive evaluation relative to the neutral benchmark (3) as shown in Table 3.
Wilcoxon signed-rank tests showed significant deviations above neutrality for Accessibility (W = 115.0, p = .002, r = .92), Quality of features (W = 116.5, p = .001, r = .94), Privacy and security (W = 61.5, p = .009, r = .86), and Response time (W = 105.0, p < .001, r = 1.00). Conversation quality was also significantly above neutrality (W = 97.0, p = .037, r = .62), but it showed the lowest central tendency and the smallest effect size among the dimensions, suggesting comparatively greater room for improvement. Across dimensions, effect sizes were predominantly large, indicating that observed differences from the neutral point were not only statistically detectable but also substantively meaningful in this sample.
The uMARS evaluated the respondents’ average positioning in four key dimensions. Detailed results from the Wilcoxon tests are summarised in Table 4.
Information (n = 13; 86.67%) was rated highly and showed a significant positive deviation from neutrality (W = 91.0, p = .002, r = 1.00), suggesting that participants perceived the informational content as particularly strong. By contrast, Engagement (n = 15) did not significantly differ from the neutral benchmark (W = 66.0, p = .160, r = .45), nor did Subjective quality (W = 52.5, p = .089, r = .59) or Perceived impact (W = 90.0, p = .093, r = .50). Although these latter domains showed descriptively above-neutral central tendencies (means and medians > 3), the inferential tests did not provide sufficient evidence to conclude that they differed reliably from neutrality in this sample. Notably, the reduced sample size for the Information domain (n = 13) should be considered when comparing domains, and the relatively larger SDs for Engagement and Perceived impact (≈ 0.8) suggest greater heterogeneity in participants’ experiences.
3.2. Qualitative Results
A psychologist conducted the qualitative interviews to collect additional information. The interviews were carried out and analysed in line with the predefined thematic variables.
3.2.1. Set 1: Communication
Overall, participants appreciated the communication style of DEMETRA, albeit some critiques emerged.
While the majority of participants found the communication style of the chatbot to be fit for the themes and the target audience, some found that the emotional qualities of the communication could be ameliorated. In particular, a couple of participants (1 psychologist and 1 expecting mother) pointed out that the responses the chatbot offers after asking the user about their current well-being seem formulaic and impersonal, albeit correct in content. On a more general level, some testers (among which two usability experts) pointed out that it was evident they were talking with a chatbot due to the cadence with which they were requested to provide feedback in order to proceed in the interactions.
Nonetheless, participants found the chatbot to be supportive and motivating, with psychologists, nutritionists and midwives stating that the chatbot touches on many issues that overweight pregnant women face in their efforts to adopt healthier lifestyles and during gestation.
Interacting with DEMETRA was judged to be both easy and seamless, with many appreciating the close-answer format adopted for the majority of the interactions; many also reported cherishing the possibility of asking the chatbot to repeat or further explain concepts within and between sessions, helping the user follow the dialogue with ease.
An issue that arose repeatedly, though, was the speed at which the chatbot sent the messages, often deemed too fast. While this is something that we could not control on Landbot, we will address the problem moving forward with the development of DEMETRA.
With regards to the adopted language (and as will be further elaborated in the content section) the overwhelming majority of participants found the communication to be easily understandable and accessible.
3.2.2. Set 2: Module Structure
Consistent with the results from the semantic differentials, participants reported conflicting views on session duration, with some participants suggesting lengthening the sessions, some finding them adequate, and others advocating shortening them. Notably, though, expecting mothers expressed favorable evaluations regarding session durations. Interestingly, one expecting mother suggested that the modalities of content delivery and session duration could be more fit for certain users than for others, pointing in particular to the amount of written information provided (versus audio-visual) as a possible risk for younger mothers. Consistent with this comment, many among those who were critical of module structure pointed out that some messages were too verbose, negatively affecting the user experience and possibly leading users to skim through the contents; suggested solutions to target these issues were either splitting said messages into shorter chunks or substituting them with audio-visual content. To quote a nutritionist on the matter: “thinking about my own experience with patients, I noticed that whenever you give lots of written informational material to them, they tend to skip the reading… I’m afraid that once the interaction slows down and the user has to stop and read longer passages, you might lose their attention. I don’t know if it is feasible, but I would consider adopting podcast-like audio messages instead of written texts in those passages”.
Instead, the inclusion of exercises was unanimously deemed a positive aspect of the modules, with two usability experts suggesting to further develop this aspect to ensure higher engagement.
Personalization emerged as a lacking aspect of the intervention: most participants found the pre-structured nature of the dialogue to be evident, with few aspects of the interaction perceived as truly tailored to them. Participants nevertheless reported feeling able to influence the interaction, primarily by determining which conversational branch the chatbot followed.
Lastly, the usage of images and videos was highly appreciated (further developed in the materials section below), with one expecting mother suggesting providing ever more visual content throughout the intervention.
3.2.3. Set 3: Materials
As anticipated in the previous section, the images and videos provided by the chatbot were unanimously appreciated, with many users identifying them as their favorite aspect of the intervention. According to the testers, the visual materials were especially useful in providing an immediate rehearsal or summary of the content, thereby increasing its accessibility and memorability. Notably, psychologists, nutritionists, and midwives alike reported finding the materials highly communicative and clarifying with regard to the concepts being presented, and thus considered them a valuable support for end users.
Nevertheless, two testers reported that the videos’ voice-overs sounded too artificial and robot-like, while a few others provided suggestions for improving specific pieces of content (e.g., particular videos or images).
3.2.4. Set 4: Content
Feedback on the contents of the intervention was unanimously positive, with testers across all categories expressing their appreciation for how the promotion of healthier behaviors was approached. As previously mentioned, participants found the dialogues and sessions to exhaustively cover themes and issues relevant to the needs of the target audience, with midwives, psychologists and nutritionists alike strongly appreciating the lack of emphasis on weight loss or calorie reduction, which would have been potentially detrimental to both the physical and mental health of overweight pregnant women and their unborn children. All the testers found the content to be socially acceptable and sensitive to the target population’s needs.
Content clarity was one of the most appreciated features of the intervention, considered by testers to be resulting from both the adopted language and the ever-present possibility to ask for further clarification. This being said, there were users reporting difficulties with some of the earlier exercises, noting that they struggled to understand whether their instructions and open questions were referring to mental health, physical health or both.
3.2.5. Insights into the Effectiveness of the Intervention
While during the interviews we did not explicitly ask for feedback on the perceived or expected effectiveness of the intervention, participants spontaneously commented on the matter or touched on it when asked about the ideal moment for delivering the intervention.
Generally, testers were optimistic regarding the possible effects of interacting with DEMETRA, highlighting the motivational and supportive features of the chatbot, even though intrinsic motivation was commonly brought up as a perceived requirement for the intervention to be effective. Most interestingly, though, professionals - midwives and nutritionists in particular - expressed highly positive attitudes toward the intervention, welcoming the novel and reportedly needed solution for addressing the psychological and motivational issues users might experience in their effort of adopting healthier lifestyles. Indeed, both categories of professionals reported a general lack of attention to these issues within the healthcare system, despite the increasing relevance and burden associated with weight-related complications during pregnancy. Accordingly, midwives and nutritionists alike considered the intervention potentially effective for users as well as highlighting its value as a supportive tool for their work.
Regarding the optimal timing for delivering the intervention, participants showed a high degree of agreement, generally indicating early pregnancy. Midwives, in particular, consistently identified the beginning of the second trimester (twelfth/thirteenth week) as the most appropriate time. They attributed this to the reduced risk of spontaneous miscarriage, the reduction of first-trimester symptoms, and the perception that patients are more settled and receptive at this point of gestation.
Testers across categories further highlighted the opportunity of capitalizing on the high motivation and interest that expectant mothers can show in early pregnancy.
Lastly, some users suggested continuing the intervention even post-partum.
3.2.6. Overall Assessment
Taken together, the qualitative interviews highlighted a generally positive reception of the intervention across participant categories. Participants consistently appreciated the communication style, clarity of content and use of visual materials, which were widely perceived as supportive, accessible and engaging. Overall, the intervention was judged to be acceptable, understandable and adapt for the target population.
At the same time, though, the analysis revealed several recurring critical points, including limitations in personalization, occasional issues related to message pacing and concerns regarding the length and density of some written messages. While users reported a sense of influence over the interaction, this was primarily associated with navigating predefined conversational paths rather than with content being tailored to individual needs.
Feedback from professionals and potential users alike thus pointed to a combination of strengths and areas for improvement, offering a nuanced picture of the intervention’s current functioning as experienced by different stakeholders.
Table 5 provides quotes from participants reflective of the main positive and negative aspects that emerged from the interviews.
4. Discussion
The present formative study examined the acceptability and usability of a chatbot-delivered, ACT-informed intervention designed to address unhealthy eating behaviours and weight-related challenges during pregnancy. The findings indicate that the intervention was perceived as clear, structured, and relevant. Quantitative evaluations of communication and content quality are supported by qualitative feedback, which highlights the comprehensibility and supportive tone of the chatbot. The findings of this study indicate that the fundamental principles of ACT can be effectively transposed into a digital format that is both palatable and meaningful within the context of antenatal care.
Concurrently, patterns across engagement-related domains exhibited greater heterogeneity. While the user experience was found to be broadly positive, both quantitative and qualitative data indicated variability in perceived interaction depth, pacing, and personalisation. This convergence of findings is consistent with the objectives of ORBIT Phase 1, in which early-stage evaluations are intended to identify strengths and areas for optimisation rather than to establish effectiveness. The results of the study indicate that the intervention’s conceptual and psychoeducational components are well received, while interactive and adaptive features represent key targets for further refinement.
Feedback from healthcare professionals highlighted a structural gap in routine antenatal care, where guidance on nutrition and physical activity is often provided without systematic attention to the psychological and motivational processes that sustain behaviour change. DEMETRA was perceived as addressing this gap by offering structured support focused on acceptance, values, and self-regulation. These components are rarely targeted in standard care pathways.
The findings of this study lend support to the feasibility of chatbot-based delivery of ACT-informed content during pregnancy, and they provide guidance for iterative development that is grounded in empirical evidence. The insights generated through this mixed-methods formative evaluation inform subsequent optimisation efforts and justify progression to later phases of development and testing within the ORBIT framework.
4.1. Strengths, Limitations, and Future Directions
The results of this preliminary study indicate that the utilisation of a chatbot to deliver an ACT-informed intervention, targeting unhealthy eating behaviours and weight-related challenges during pregnancy, is a viable and promising approach. The six-session structure supported fidelity to evidence-based ACT principles while allowing content to be delivered in a concise and accessible format. Digital delivery via chatbot offers clear advantages in terms of scalability, standardisation of content, and potential reach, particularly in contexts where access to specialised psychological or nutritional support may be limited. The intervention was perceived to be clear, well-structured, and relevant to weight-related challenges during pregnancy.
Furthermore, participants indicated that the second trimester of pregnancy was perceived as the most opportune period to engage with the intervention, once both initial, unpleasant symptoms and the risk for spontaneous miscarriage are reduced, and motivation is high- This observation is consistent with prior research emphasising the importance of timing in antenatal behaviour change interventions. In addition, the integration of chatbot-based support with professional guidance, such as nutritional counselling or antenatal care, was proposed by some participants as a particularly effective strategy, as opposed to its provision as a standalone solution.
In accordance with the extant literature on digital health interventions, the present study lends support to the potential of chatbot-delivered programs to promote engagement, provide psychoeducation, and encourage reflection and behaviour change during pregnancy. Participants expressed satisfaction with the systematic and intelligible presentation of content, as well as the intuitive nature of the interaction. Concurrently, the challenges previously identified in the field of chatbot research, including limited flexibility, personalisation, and nuanced responsiveness, were also observed. Reports of repetitive content and constrained interaction pathways reflect ongoing design challenges in balancing automation with individualised support in ACT-based digital interventions.
A significant strength of this study is its participatory and multidisciplinary development process. The involvement of psychologists, ACT experts, nutritionists, communication specialists, and end users throughout the design and formative evaluation phases enhanced the relevance, clarity, and usability of the intervention. Moreover, the integration of quantitative and qualitative methods yielded complementary insights into both measurable aspects of user experience and more nuanced perceptions, consistent with best practices for formative evaluation within the ORBIT framework.
It is imperative to acknowledge the limitations inherent in the interpretation of these findings, which are characteristic of formative evaluations of early-stage digital interventions. Participants identified opportunities for improvement related to personalisation, content variation, and depth of interaction, highlighting the broader challenge of delivering structured, automated interventions while remaining responsive to individual needs and preferences, particularly when addressing sensitive weight-related behaviours during pregnancy. Furthermore, the limited sample size and the high educational level of the participants may restrict the generalisability of the results. The present study concentrated on the evaluation of usability, acceptability, and perceived impact. Behavioral and clinical outcomes, including alterations in eating behaviors and gestational weight gain, were not the focus of the present study. Finally, the relatively limited intervention period and fixed session schedule may have contributed to perceptions of repetitiveness. When considered as a whole, these limitations offer valuable guidance for further refinement and future phases of evaluation.
Future iterations of the DEMETRA intervention should build directly on the formative insights identified in this study. The enhancement of personalisation and flexibility is a key priority, for example through the implementation of more adaptive conversational pathways, increased variability in content delivery, and options for user-driven pacing. Allowing participants to adjust session frequency or revisit selected modules according to their needs may help sustain engagement and reduce perceptions of repetition.
At this developmental stage, DEMETRA relies on structured, rule-based conversational pathways rather than fully adaptive AI-driven dialogue systems. This design choice was intentional and consistent with the formative aims of ORBIT Phase 1, prioritising content fidelity, clarity, and safety over conversational complexity. More adaptive and personalised dialogue features represent a key direction for future iterations
Subsequent research should extend the evaluation beyond usability and acceptability to include preliminary behavioural and clinical outcomes, such as changes in eating behaviours, psychological flexibility, or patterns of gestational weight gain, in line with progression to later ORBIT phases focused on refinement and early efficacy testing. Longer-term studies would also allow examination of sustained engagement across different stages of pregnancy. Ultimately, it is recommended that subsequent research endeavours encompass larger and more heterogeneous samples, incorporating women from diverse socioeconomic, cultural, and educational backgrounds, in addition to those exhibiting a higher propensity for excessive gestational weight gain. The integration of the chatbot within routine antenatal or nutritional care, whether as a low-intensity standalone intervention or as part of a stepped or blended care model, has the potential to further enhance both impact and trust. Furthermore, it may help to clarify the role of chatbot-based ACT interventions in supporting healthy weight-related behaviours during pregnancy.
5. Conclusions
The present study documented the development and formative evaluation of DEMETRA, a chatbot informed by Acceptance and Commitment Therapy (ACT). The purpose of the DEMETRA chatbot is to support overweight and obese women during pregnancy in adopting healthier eating behaviours and lifestyles. In accordance with Phase 1 of the ORBIT framework, the primary objective was not to ascertain efficacy, but rather to evaluate acceptability, usability, perceived relevance, and to identify strengths and areas for refinement prior to subsequent testing.
The findings, when considered as a whole, indicate that the core principles of ACT can be meaningfully and coherently translated into a chatbot-delivered intervention within the antenatal context. DEMETRA was perceived as clear, structured, and appropriate for pregnancy, with particular appreciation for its non-stigmatising, non-weight-loss-centred approach and its focus on values, psychological flexibility, and sustainable health-related behaviours. The utilisation of visual and multimedia materials served to enhance comprehension and accessibility, thereby reinforcing the psychoeducational and motivational objectives of the intervention.
In accordance with the preceding discussion, engagement-related dimensions demonstrated greater variability, and the formative evaluation identified limited personalisation, constrained conversational flexibility, and message pacing as primary targets for optimisation. These findings reflect the known challenges associated with early-stage chatbot-based interventions and underscore the necessity of iterative development to balance standardisation with responsiveness to individual needs, particularly when addressing sensitive weight- and health-related issues during pregnancy.
It is noteworthy that both professionals and potential end users underscored the significance of positioning DEMETRA as a complementary, low-intensity support integrated within routine antenatal or nutritional care, as opposed to a standalone solution. This finding is consistent with the intervention’s designated function as a scalable instrument capable of providing support to healthcare providers while addressing motivational and psychological processes that are frequently inadequately targeted in standard prenatal care.
In conclusion, the present study provides a methodologically rigorous and empirically grounded foundation for the continued development of DEMETRA. The present work supports progression to subsequent ORBIT phases by demonstrating the feasibility and acceptability of a chatbot-delivered ACT intervention tailored to overweight pregnant women, and by clearly delineating priorities for refinement. It is recommended that future research focus on the examination of behavioural and clinical outcomes, the enhancement of adaptive and personalised dialogue systems, and the evaluation of implementation within real-world healthcare settings. Consequently, DEMETRA signifies a potentially valuable application of digitally delivered ACT in promoting healthier lifestyles during pregnancy.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study in line with Italian Law No. 3/2018, art. 2, paragraphs 7 and 10, as i) it focused on the usability of a prototype digital intervention, ii) there is no involvement of patients nor vulnerable groups, iii) no clinical treatment nor sensitive health data collection are foreseen. At the same time, a clear adherence to ethical principles is ensured (voluntary informed consent, privacy protection).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We extend our gratitude to all study participants who dedicated their time, shared their knowledge, and contributed with their invaluable personal and professional experiences to the research.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACT | Acceptance and Commitement Therapy |
| NICE | National Institute for Health and Care Excellence |
| ORBIT | Obesity-Related Behavioral Intervention Trials |
| uMARS | User Version of the Mobile Application Rating Scale |
| BUS-11 | Chatbot Usability Scale |
| SD | Standard Deviation |
Appendix A

Table A1.
List of variables and subvariables investigated and related items used.
| Variable | Subvariables | Items |
| Communication |
empathy and listening skills | judgmental - welcoming, passive listening - active listening, alarming - reassuring, indifferent - sensitive, cold - warm |
| entry 2 | fluency and fluidity | non-sliding - sliding |
| chatbot interaction | boring - engaging, inefficient - efficient, slow - fast, heavy - adequate | |
| vocabulary | abstruse - understandable, technical - common | |
| Module structure | interaction duration | long - short, challenging - easy |
| Material | audios | unpleasant - pleasant, stressful - relaxing, hindering - helpful, useless - functional |
| images | unimaginative - creative, hindering - supportive, unpleasant - pleasant | |
| Content | content evaluation | boring - interesting, soporific - stimulating, of little value - of great value |
| clarity of content | confused - clear, abstruse - understandable |
Appendix B
Table A2.
List of variables and subvariables investigated and related items used.
| Topic investigated | Questions |
| Interaction | 1.1 How did you feel about the interaction with DEMETRA? Were there enough alternatives among the replies to DEMETRA? 1.2 What was the feature of the interaction that you liked the most? And the one you liked the least? 1.3 Have you ever made the mistake of clicking the answer button on a question? Have you wished you could have gone back? |
| Contents | 2.1 If something was not clear to you at first, do you find there is then a way to investigate the topic further? 2.2 Is the mode of communication (length of sentences, terms used, etcetera) appropriate for the content? |
| Engagement | 3.1 Was the communication with the chatbot engaging? Did it entice you to get involved and be consistent in the activities it recommended? |
| General | 4.1 Do you have any concerns? Do you have any criticism? 4.2 When would be the ideal time to take this intervention for a pregnant woman? 4.3 Overall, was the intervention personalized for you? Give a level of personalization from 0 to 10. |
References
- Adler, Jonathan; Van Brunt, Deryk. ‘It Is Time to Realize the Promise of the Digital Mental Health Transformation: Application for Population Mental Health’. Journal of Medical Internet Research 2025, 27 (June), e63791–e63791. [Google Scholar] [CrossRef]
- Ahmad, Md Altamash; Kaur, Rupinder; Singh, Ravinder; Jangra, Sarita; Mehta, Sanjana; Kumari, Pratima. ‘Strategies for Reducing Obesity-Related Complications During Pregnancy’. In Maternal and Child Health, and Nutrition; Sharma, Amit, Singh, Thakur Gurjeet, Eds.; Springer Nature Singapore, 2025. [Google Scholar] [CrossRef]
- Almutairi, Fai S; Alsaykhan, Alaa M; Almatrood, Abrar A. ‘Obesity Prevalence and Its Impact on Maternal and Neonatal Outcomes in Pregnant Women: A Systematic Review’. Cureus 2024, ahead of print. [Google Scholar] [CrossRef]
- Apolinário-Hagen, Jennifer; Drüge, Marie; Guthardt, Lisa; Haller, Elisa. ‘Acceptance and Commitment Therapy for Major Depressive Disorder: Navigating Depression Treatment in Traditional and Digital Settings with Insights from Current Research’. In Recent Advances and Challenges in the Treatment of Major Depressive Disorder;Advances in Experimental Medicine and Biology; Kim, Yong-Ku, Ed.; Springer Nature Singapore, 2024; vol. 1456. [Google Scholar] [CrossRef]
- Ashton, Abbey A.; Wilson, Jane; Slade, Pauline. ‘Feasibility and Acceptability of a Brief Online Acceptance and Commitment Therapy Intervention to Reduce Fear of Childbirth: A Novel Application of a Third-wave Cognitive Behavioral Therapy Focused on Psychological Flexibility and Acceptance’. Acta Obstetricia et Gynecologica Scandinavica 2025, 104(10), 1939–48. [Google Scholar] [CrossRef]
- Borsci, Simone; Prati, Elisa; Malizia, Alessio; Schmettow, Martin; Chamberlain, Alan; Federici, Stefano. ‘Ciao AI: The Italian Adaptation and Validation of the Chatbot Usability Scale’. Personal and Ubiquitous Computing 2023, 27(6), 2161–70. [Google Scholar] [CrossRef]
- Bowden, Emily R; Chang, Anne B; McCallum, Gabrielle B. ‘Interventions to Improve Enablers and/or Overcome Barriers to Seeking Care during Pregnancy, Birthing and Postnatal Period for Women Living with Vulnerabilities in High-Income Countries: A Systematic Review and Meta-Analysis’. Midwifery 2023, 121 (June), 103674. [Google Scholar] [CrossRef]
- Brunner, Kathrin; Linder, Tina; Klaritsch, Philipp; Tura, Andrea; Windsperger, Karin; Göbl, Christian. ‘The Impact of Overweight and Obesity on Pregnancy: A Narrative Review of Physiological Consequences, Risks and Challenges in Prenatal Care, and Early Intervention Strategies’. Current Diabetes Reports 2025, 25(1), 30. [Google Scholar] [CrossRef]
- Catalano, Patrick M; Shankar, Kartik. ‘Obesity and Pregnancy: Mechanisms of Short Term and Long Term Adverse Consequences for Mother and Child’. BMJ 2017, j1. [Google Scholar] [CrossRef] [PubMed]
- Chew, Han Shi Jocelyn; Chng, Samuel; Rajasegaran, Nagadarshini Nicole; Choy, Khun Hean; Chong, Yuen Yu. ‘Effectiveness of Acceptance and Commitment Therapy on Weight, Eating Behaviours and Psychological Outcomes: A Systematic Review and Meta-Analysis’. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 2023, 28(1), 6. [Google Scholar] [CrossRef]
- Conrad, Jordan A. ‘Digitization and Its Discontents: The Promise and Limitations of Digital Mental Health Interventions’. Journal of Contemporary Psychotherapy 2024, 54(3), 209–15. [Google Scholar] [CrossRef]
- Dencker, Anna; Premberg, Åsa; Olander, Ellinor K.; et al. ‘Adopting a Healthy Lifestyle When Pregnant and Obese – an Interview Study Three Years after Childbirth’. BMC Pregnancy and Childbirth 2016, 16(1), 201. [Google Scholar] [CrossRef] [PubMed]
- Dindo, Lilian; Van Liew, Julia R.; Arch, Joanna J. ‘Acceptance and Commitment Therapy: A Transdiagnostic Behavioral Intervention for Mental Health and Medical Conditions’. Neurotherapeutics 2017, 14(3), 546–53. [Google Scholar] [CrossRef] [PubMed]
- Ernst, Kayla; Dasilva, Gabriella; Srivastav, Megha; et al. ‘Challenges in Accessing Mental Health Services in Underserved Pregnant and Postpartum Women: A Scoping Review’. Women 2025, 5(3), 31. [Google Scholar] [CrossRef]
- Fietta, Valentina; Rizzi, Silvia; De Luca, Chiara; et al. ‘A Chatbot-Based Version of the World Health Organization–Validated Self-Help Plus Intervention for Stress Management: Co-Design and Usability Testing’. JMIR Human Factors 2024, 11 (October), e64614. [Google Scholar] [CrossRef]
- Gale, Nicola K.; Heath, Gemma; Cameron, Elaine; Rashid, Sabina; Redwood, Sabi. ‘Using the Framework Method for the Analysis of Qualitative Data in Multi-Disciplinary Health Research’. BMC Medical Research Methodology 2013, 13(1), 117. [Google Scholar] [CrossRef]
- Gentili, Charlotte; Zetterqvist, Vendela; Rickardsson, Jenny; Holmström, Linda; Simons, Laura E; Wicksell, Rikard K. ‘ACTsmart: Guided Smartphone-Delivered Acceptance and Commitment Therapy for Chronic Pain—A Pilot Trial’. Pain Medicine 2021, 22(2), 315–28. [Google Scholar] [CrossRef]
- Hayes, Steven C.; Levin, Michael E.; Plumb-Vilardaga, Jennifer; Villatte, Jennifer L.; Pistorello, Jacqueline. ‘Acceptance and Commitment Therapy and Contextual Behavioral Science: Examining the Progress of a Distinctive Model of Behavioral and Cognitive Therapy’. Behavior Therapy 2013, 44(2), 180–98. [Google Scholar] [CrossRef] [PubMed]
- Herbert, Matthew S.; Dochat, Cara; Wooldridge, Jennalee S.; et al. ‘Technology-Supported Acceptance and Commitment Therapy for Chronic Health Conditions: A Systematic Review and Meta-Analysis’. Behaviour Research and Therapy 2022, 148 (January), 103995. [Google Scholar] [CrossRef]
- Howard, Sarah; Houghton, Consultant Midwife Gillian; White, Ross; Fallon, Vicky; Slade, Pauline. ‘The Feasibility and Acceptability of a Single-Session Acceptance and Commitment Therapy (ACT) Intervention to Support Women Self-Reporting Fear of Childbirth in a First Pregnancy’. Psychology & Health 2023, 38(11), 1460–81. [Google Scholar] [CrossRef]
- Iturbe, Idoia; Echeburúa, Enrique; Maiz, Edurne. ‘The Effectiveness of Acceptance and Commitment Therapy upon Weight Management and Psychological Well-being of Adults with Overweight or Obesity: A Systematic Review’. Clinical Psychology & Psychotherapy 2022, 29(3), 837–56. [Google Scholar] [CrossRef]
- Jangra, Sarita; Vani, Cheppalli; Sharma, Amit; et al. ‘Guidelines for Healthy Weight Management in Expecting Mothers’. In Maternal and Child Health, and Nutrition; Sharma, Amit, Singh, Thakur Gurjeet, Eds.; Springer Nature Singapore, 2025. [Google Scholar] [CrossRef]
- Jelsma, Judith G. M.; Van Leeuwen, Karen M.; Oostdam, Nicolette; et al. ‘Beliefs, Barriers, and Preferences of European Overweight Women to Adopt a Healthier Lifestyle in Pregnancy to Minimize Risk of Developing Gestational Diabetes Mellitus: An Explorative Study’. Journal of Pregnancy 2016, 2016, 1–11. [Google Scholar] [CrossRef]
- Kelson, Joshua; Rollin, Audrey; Ridout, Brad; Campbell, Andrew. ‘Internet-Delivered Acceptance and Commitment Therapy for Anxiety Treatment: Systematic Review’. Journal of Medical Internet Research 2019, 21(1), e12530. [Google Scholar] [CrossRef]
- Kent, Lisa; McGirr, Meabh; Eastwood, Kelly-Ann. ‘Global Trends in Prevalence of Maternal Overweight and Obesity: A Systematic Review and Meta-Analysis of Routinely Collected Data Retrospective Cohorts’. International Journal of Population Data Science 2024, 9(2). [Google Scholar] [CrossRef]
- Klimczak, Korena S.; San Miguel, Guadalupe G.; Mukasa, Miriam N.; Twohig, Michael P.; Levin, Michael E. ‘A Systematic Review and Meta-Analysis of Self-Guided Online Acceptance and Commitment Therapy as a Transdiagnostic Self-Help Intervention’. Cognitive Behaviour Therapy 2023, 52(3), 269–94. [Google Scholar] [CrossRef] [PubMed]
- Krafft, Jennifer; Potts, Sarah; Schoendorff, Benjamin; Levin, Michael E. ‘A Randomized Controlled Trial of Multiple Versions of an Acceptance and Commitment Therapy Matrix App for Well-Being’. Behavior Modification 2019, 43(2), 246–72. [Google Scholar] [CrossRef] [PubMed]
- Kurnaz, Döndü; Karaçam, Zekiye. ‘The Effect of Methods Used in the Management of Maternal Obesity on Pregnancy and Birth Outcomes: A Systematic Review with Meta-Analysis’. International Journal of Obesity 2025, 49(6), 1013–23. [Google Scholar] [CrossRef]
- Lappalainen, Päivi; Langrial, Sitwat; Oinas-Kukkonen, Harri; Tolvanen, Asko; Lappalainen, Raimo. ‘Web-Based Acceptance and Commitment Therapy for Depressive Symptoms With Minimal Support: A Randomized Controlled Trial’. Behavior Modification 2015, 39(6), 805–34. [Google Scholar] [CrossRef]
- Lee-Baggley, Dayna. Healthy Habits Suck: How to Get off the Couch and Live a Healthy Life . In Even If You Don’t Want To; Harris, Russ, Ed.; New Harbinger Publications, 2019. [Google Scholar]
- Lelorain, Sophie; Deruelle, Philippe; Béhal, Hélène; et al. ‘Factors Influencing Participation and Regular Attendance in a Program Combining Physical Activity and Nutritional Advice for Overweight and Obese Pregnant Women’. BMC Pregnancy and Childbirth 2024, 24(1), 449. [Google Scholar] [CrossRef] [PubMed]
- Levin, Michael E.; Aller, Ty B.; Klimczak, Korena S.; Donahue, Marissa L.; Knudsen, Francesca M. ‘Digital Acceptance and Commitment Therapy for Adults with Chronic Health Conditions: Results from a Waitlist-Controlled Trial’. Behaviour Research and Therapy 2025, 188 (May), 104729. [Google Scholar] [CrossRef]
- Levin, Michael E.; Krafft, Jennifer; Hicks, Elizabeth T.; Pierce, Benjamin; Twohig, Michael P. ‘A Randomized Dismantling Trial of the Open and Engaged Components of Acceptance and Commitment Therapy in an Online Intervention for Distressed College Students’. Behaviour Research and Therapy 2020, 126 (March), 103557. [Google Scholar] [CrossRef]
- Levin, Michael E; Petersen, Julie M; Durward, Carrie; et al. ‘A Randomized Controlled Trial of Online Acceptance and Commitment Therapy to Improve Diet and Physical Activity among Adults Who Are Overweight/Obese’. Translational Behavioral Medicine 2021, 11(6), 1216–25. [Google Scholar] [CrossRef]
- Levin, Michael E.; Pierce, Benjamin; Schoendorff, Benjamin. ‘The Acceptance and Commitment Therapy Matrix Mobile App: A Pilot Randomized Trial on Health Behaviors’. Journal of Contextual Behavioral Science 2017, 6(3), 268–75. [Google Scholar] [CrossRef]
- Lillis, Jason; Dahl, JoAnne; Weineland, Sandra M. The Diet Trap: Feed Your Psychological Needs and End the Weight Loss Struggle Using Acceptance and Commitment Therapy; New Harbinger Publications, 2014. [Google Scholar]
- Osgood, Charles Egerton; Suci, George J.; Tannenbaum, Percy H. The Measurement of Meaning; University of Illinois Press, 1957. [Google Scholar]
- Pitil, Patricia Pawa; Ghazali, Siti Raudzah. ‘Acceptance and Commitment Therapy and Weight-Related Difficulties in Overweight and Obese Adults: A Systematic Review’. Psychological Reports 2024, 127(6), 2873–97. [Google Scholar] [CrossRef] [PubMed]
- Polk, Kevin L.; Prevedini, Anna Bianca. La matrice ACT: guida all’utilizzo nella pratica clinica; F. Angeli, 2017. [Google Scholar]
- Potts, Sarah; Krafft, Jennifer; Levin, Michael E. ‘A Pilot Randomized Controlled Trial of Acceptance and Commitment Therapy Guided Self-Help for Overweight and Obese Adults High in Weight Self-Stigma’. Behavior Modification 2022, 46(1), 178–201. [Google Scholar] [CrossRef] [PubMed]
- Sari, Yanti Puspita; Herman, Hermalinda; Fajria, Lili; Herien, Yelly; Susanti, Evi; Lin, Chung-Ying. ‘The Impact of M-Health Interventions on Gestational Weight Gain and Physical Activity among Pregnant Women with Overweight and Obesity: A Meta-Analysis of Randomized Controlled Trials’. Midwifery 2025, 146, 104399. [Google Scholar] [CrossRef]
- Schumacher, Leah M.; Miller, Nicole; Jennings, Emma L.; Chabria, Reena; Butryn, Meghan L. ‘Acceptance and Commitment Therapy for Obesity’. Current Obesity Reports 2025, 14(1), 41. [Google Scholar] [CrossRef] [PubMed]
- Shieh, C.; Cullen, D. L.; Pike, C.; Pressler, S. J. ‘Intervention Strategies for Preventing Excessive Gestational Weight Gain: Systematic Review and Meta-analysis’. Obesity Reviews 2018, 19(8), 1093–109. [Google Scholar] [CrossRef]
- Stoyanov, Stoyan R; Hides, Leanne; Kavanagh, David J; Wilson, Hollie. ‘Development and Validation of the User Version of the Mobile Application Rating Scale (uMARS)’. JMIR mHealth and uHealth 2016, 4(2), e72. [Google Scholar] [CrossRef]
- Tobias, Margaret R.; Landy, Lauren N.; Levin, Michael E.; Arch, Joanna J. ‘A Randomized Trial of Brief Online Interventions to Facilitate Treatment Seeking for Social Anxiety’. Behavior Modification 2022, 46(5), 1137–66. [Google Scholar] [CrossRef]
- Torous, John; Linardon, Jake; Goldberg, Simon B.; et al. ‘The Evolving Field of Digital Mental Health: Current Evidence and Implementation Issues for Smartphone Apps, Generative Artificial Intelligence, and Virtual Reality’. World Psychiatry 2025, 24(2), 156–74. [Google Scholar] [CrossRef]
- Van Gemert-Pijnen; Ewc, Julia; Nijland, Nicol; Van Limburg, Maarten; et al. ‘A Holistic Framework to Improve the Uptake and Impact of eHealth Technologies’. Journal of Medical Internet Research 2011, 13(4), e111. [Google Scholar] [CrossRef]
- Waters, Cerith S.; Annear, Benjamin; Flockhart, Gillean; et al. ‘Acceptance and Commitment Therapy for Perinatal Mood and Anxiety Disorders: A Feasibility and Proof of Concept Study’. British Journal of Clinical Psychology 2020, 59(4), 461–79. [Google Scholar] [CrossRef] [PubMed]
- Yıldız, Erman. ‘The Effects of Acceptance and Commitment Therapy on Lifestyle and Behavioral Changes: A Systematic Review of Randomized Controlled Trials’. Perspectives in Psychiatric Care 2020, 56(3), 657–90. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Development and iterative processes of the ACT-based intervention (Phase 1 of the ORBIT model—Design).
Figure 1.
Development and iterative processes of the ACT-based intervention (Phase 1 of the ORBIT model—Design).
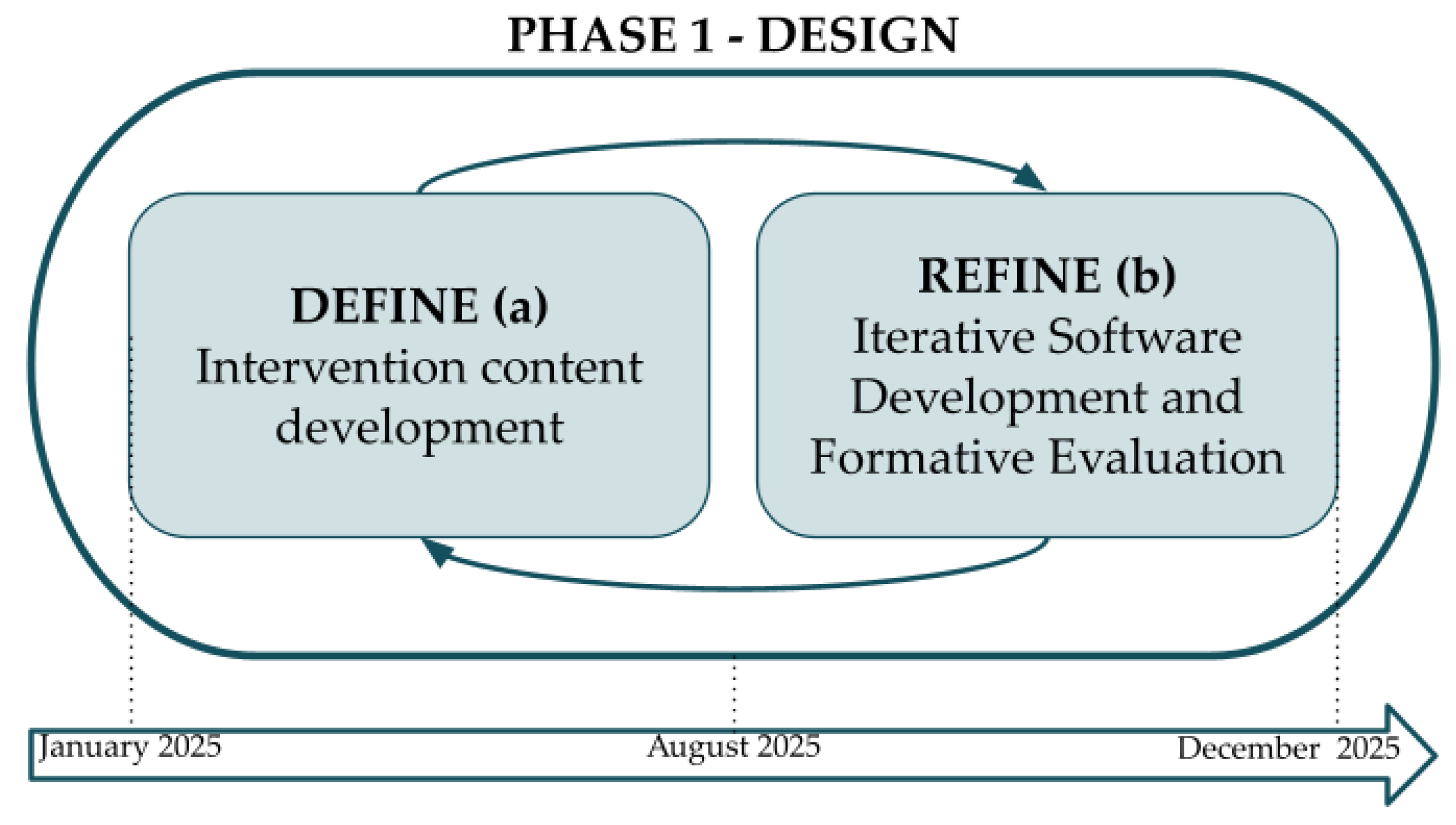
Table 1.
Description of the topics covered week by week.
| Week | Topics |
| Week 0 | Brief introduction to DEMETRA and how the chatbot works |
| Week 1 | Biological drivers of unhealthy behaviors; values; factors influencing body weight. |
| Week 2 | The “Fix me-trap” and controlling thoughts and emotions as sources of suffering. |
| Week 3 | Fusion and obedience to thoughts and feelings, cognitive defusion; introduction to the ACT Matrix for value clarification; internal and external obstacles; behavioral avoidance; thoughts and feelings as unavoidable. |
| Week 4 | Recognizing avoidant behaviors and valued actions using the ACT matrix; the myth of the perfect goal-weight. |
| Week 5 | Emotional eating; mindful eating exercise; |
| Week 6 | Using the matrix in daily life; self-compassion vs self-critique; nine steps to stay on track when pursuing values. |
Table 2.
Results from the Semantic Differential (N=15).
| Participants, n (%) | Values, Mean (SD) | Values, Median (Range) | W | p Value | r | |
|---|---|---|---|---|---|---|
| Empathy and listening | 15 (100) | 3.68 (0.52) | 3.80 (0.14) | 103.5 | 0.001 | 0.971 |
| Smoothness and fluidity | 15 (100) | 3.87 (0.99) | 4.00 (0.26) | 79.5 | 0.015 | 0.747 |
| Chatbot interaction | 15 (100) | 3.72 (0.78) | 3.75 (0.20) | 93.5 | 0.011 | 0.781 |
| Lexicon | 15 (100) | 4.20 (0.59) | 4.00 (0.15) | 105.0 | < .001 | 1.000 |
| Session duration | 15 (100) | 3.23 (0.75) | 3.00 (0.19) | 31.0 | 0.328 | 0.378 |
| Videos | 15 (100) | 4.02 (0.59) | 4.00 (0.15) | 105.0 | 0.001 | 1.000 |
| Infographics | 15 (100) | 3.76 (0.61) | 3.67 (0.16) | 89.0 | 0.003 | 0.956 |
| Content evaluation | 15 (100) | 3.89 (0.64) | 4.00 (0.17) | 115.5 | 0.002 | 0.925 |
| Content clarity | 15 (100) | 4.30 (0.70) | 4.00 (0.18) | 91.0 | 0.001 | 1.000 |
Note. Hₐ μ ≠ 3.
Table 3.
Results from the BUS-11 (N=15).
| Participants, n (%) | Values, Mean (SD) | Values, Median (Range) | W | p Value | r | |
|---|---|---|---|---|---|---|
| Accessibility | 15 (100) | 4.20 (0.78) | 4.00 (0.20) | 115.0 | 0.002 | 0.917 |
| Quality of features | 15 (100) | 4.04 (0.67) | 4.00 (0.17) | 116.5 | 0.001 | 0.942 |
| Conversation quality | 15 (100) | 3.45 (0.66) | 3.50 (0.17) | 97.0 | 0.037 | 0.617 |
| Privacy and security | 15 (100) | 3.80 (0.82) | 4.00 (0.22) | 61.5 | 0.009 | 0.864 |
| Response time | 15 (100) | 4.33 (0.62) | 4.00 (0.16) | 105.0 | < .001 | 1.000 |
Note. Hₐ μ ≠ 3.
Table 4.
Results from the uMARS (N=15).
| Participants, n (%) | Values, Mean (SD) | Values, Median (Range) | W | p Value | r | |
|---|---|---|---|---|---|---|
| Engagement | 15 (100) | 3.35 (0.80) | 3.60 (0.21) | 66.0 | 0.160 | 0.451 |
| Information | 13 (86.67) | 4.23 (0.48) | 4.25 (0.13) | 91.0 | 0.002 | 1.000 |
| Subjective items | 15 (100) | 3.30 (0.61) | 3.50 (0.16) | 52.5 | 0.089 | 0.591 |
| Perceived impact | 15 (100) | 3.47 (0.81) | 3.67 (0.21) | 90.0 | 0.093 | 0.500 |
Note. Hₐ μ ≠ 3.
Table 5.
Main positive and negative aspects emerged from user interviews.
| Communication style and Tone | Module structure | Personalization | Perceived usefulness/effectiveness | |
|---|---|---|---|---|
| Positive | “It gave you time. In several moments it explicitly said things like ‘take all the time you need’ or ‘ I know this takes time’... I really appreciated this, because it didn’t pressure you to respond or rush through the session” -midwife |
“I appreciated when the chatbot included exercises within the session, rather than leaving them to be done independently, because it made it easier to stay engaged throughout the interaction” -usability expert |
“I found it useful to be able to choose whether to repeat or skip certain parts, such as the myths. Having the option to decide based on my needs made the interaction feel more adaptive” -psychologist |
“I really appreciated the aim and overall meaning of the intervention. I think this kind of support can be very useful, especially in helping women see things from a different perspective and find more strength in facing this period.” -expecting mother |
| Negative | “I believe the ‘warmth’ of the intervention could be ameliorated - it really felt like you were talking with a chatbot sometimes… I noticed it repeated some answers - things like ‘Sad moments happen to everyone” - which were fine, even correct you might say, but after reading it once again it felt empty” -psychologist |
“Some sessions felt too long, and at times I interrupted them and continued later, or even forgot to resume them completely” - usability expert |
“Even if you could give different answers, the interaction always brought you back to the same path, so it didn’t really feel personalized” - expecting mother |
“Some of the messages felt quite theoretical and didn’t really push me to put things into practice” - expecting mother |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



