
Submitted:
22 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Background/Objectives: Dental anxiety (DA) is common worldwide and strongly linked to avoidance of dental care, delayed treatment and poorer oral health. Although many studies have examined determinants and management of DA, its broader placement as a potential bottleneck along oral systemic health pathways, from determinants of DA to consequences i.e.oral and systemic outcomes via dental avoidance, has not been clearly mapped across the review literature. This review aimed to conceptually map how existing DA reviews are distributed across this pathway and identify key gaps. Methods: We conducted a conceptual mapping review of DA-focused review articles published between 2005 and 2025. PubMed and Scopus were searched for English-language narrative, systematic, scoping and umbrella reviews and meta-analyses addressing determinants or consequences of DA. One reviewer screened records, extracted review characteristics, and classified each review into predefined domains (determinants, dental avoidance, oral health outcomes, psychosocial impact, and systemic health outcomes) using prespecified coding rules. Classifications were cross-checked using a structured prompt for independent AI-assisted full-text coding. Final codes were adjudicated by the reviewer against the source text. Domains were coded as covered (substantive focus), mentioned (brief mention), or not addressed. or not addressed. No meta-analysis was conducted. The review was not registered and involved no stakeholders. Results: The search identified 851 records; after removing 426 duplicates, 425 unique records were screened, and 40 reviews met inclusion criteria. Narrative reviews were most common (18/40, 45.0%). Determinants dominated the evidence base (psychological 31/40, 77.5%; environmental 27/40, 67.5%). As consequences, avoidance (25/40, 62.5%) and oral health outcomes (21/40, 52.5%) were covered in about half of reviews. Psycho-social impacts were rarely covered (shame/embarrassment 5/40, 12.5%; Oral health-related quality of life 4/40, 10.0%). Systemic health outcomes were least addressed (covered 1/40, 2.5%; mentioned 5/40, 12.5%). Conclusions: Review level evidence supports a pathway from DA to avoidance and poorer oral health, but offers limited synthesis on outcomes beyond the oral domain. Given the oral-systemic link and the role of behavioural barriers to access and delayed treatment, future research should test pathways from DA to quality of life and systemic outcomes using clear mechanisms and appropriate temporal designs.
Keywords:
dental fear
; behavioural bottleneck
; oral–systemic link
; public health
; health equity
1. Introduction
Dental anxiety (DA) is common and is consistently linked to avoidance of dental care, delayed treatment, and poorer oral health [1], which may contribute to oral health inequalities. In parallel, strong evidence links poor oral health to systemic conditions [2,3], and global policy increasingly frames oral health as part of overall health [4]. Yet DA focused reviews and models have rarely connected these two lines of knowledge.
To clarify whether and how DA is positioned within oral systemic health pathways, we conducted a conceptual mapping review of review articles. In this approach, review articles are treated as a record of how the field synthesises and frames evidence. By mapping where DA reviews cluster along a predefined pathway from determinants of DA to avoidance, oral and psychosocial outcomes, and potential systemic outcomes, we assess how far conceptual consensus extends beyond the mouth and identify which parts remain under synthesised at the review level.
To operationalise this mapping, we first clarify how DA related terms are used in review and population based research. We then outline key models of DA determinants and consequences that inform the pathway used in this review. In the clinical dental setting, it may be practical to distinguish dental fear (a normal emotional response to an immediate, genuinely threatening situation) from dental anxiety (anticipatory reactions occurring in the absence of a present trigger) and dental phobia (a clinical disorder defined by DSM/ICD criteria) [5]. However, in population-based research and literature reviews, these terms are frequently used interchangeably, and their boundaries are difficult to operationalise consistently. Accordingly, we use DA as an overarching term in this review, unless a specific diagnostic definition or specific fear is explicitly discussed. In addition, DA has been conceptualised as comprising two closely related components: anticipatory anxiety before the appointment and treatment-related anxiety during dental procedures [6].
Several theoretical models have been proposed to explain how DA develops. Early work drawing on learning theory, such as Rachman’s three-pathway model, described fear acquisition through direct conditioning by painful treatment, vicarious learning from fearful others and negative information from the environment [7]. Weiner and Sheehan later distinguished exogenous pathways (traumatic dental events) from endogenous vulnerability (general anxiety proneness) [8]. Building on this distinction, Locker and colleagues proposed a constitutional vulnerability model in which relatively stable biological and psychological characteristics make some individuals more likely to develop DA when they encounter adverse dental experiences [9]. Such constitutional factors may include stable biological and psychological predispositions (e.g., pain or sensory sensitivity and trait anxiety). Within this broader framework, Armfield’s cognitive vulnerability model focuses specifically on patients’ schemas concerning uncontrollability, unpredictability and dangerousness of dental treatment [10]. McNeil and Randall subsequently integrated these strands in a biopsychosocial framework that brings together constitutional vulnerabilities, learning pathways and situational factors in the dental clinic as interacting determinants of DA [11].
On the consequences side, classical learning theories emphasise negative reinforcement, whereby the immediate relief gained by escaping or avoiding a feared situation strengthens avoidance and maintains fear and anxiety over time [12,13,14]. Applied to dentistry, this logic is captured in the “vicious cycle” model by Berggren and Meynert, in which DA leads to avoidance of dental care, progressive oral deterioration, embarrassment/shame and further increases in anxiety [15]. Later extensions of this model incorporated broader psychosocial consequences, including reduced self-esteem, impaired social functioning and, in severe cases, social withdrawal [16]. Recent work also highlights dental shame as a key psychosocial consequence [17]. Complementing this perspective, the McNeil and Randall framework also specifies a behavioural pathway in which dental fear and anxiety shape appraisals of treatment, perceived costs and benefits of attending, and ultimately patterns of treatment seeking and attendance [11]. Empirical research is largely consistent with these models: higher DA is associated with irregular or symptomatic visiting patterns [18], poorer oral health status and worse oral-health-related quality of life [19].
To date, however, DA-specific conceptual models have focused almost exclusively on dental outcome and psychological determinants; systemic disease has not been explicitly incorporated. This is in contrast to the extensive evidence linking poor oral health – particularly periodontal disease and tooth loss – with a range of systemic conditions such as cardiovascular disease and diabetes [2,3]. From this perspective, DA can be viewed as a behavioural bottleneck in dental attendance that may indirectly influence systemic health through oral infection and low-grade inflammation, and that may contribute to oral health inequalities. Yet it remains unclear how far existing DA-focused reviews have followed this logic and to what extent they have considered outcomes beyond the mouth.
Given this background, the purpose of this review is not to propose a new comprehensive theory, but to clarify how far the existing review literature on DA extends along the hypothesised pathway. We map review articles that address determinants or consequences of DA and identify where synthesis accumulates along the pathway from vulnerability to avoidance, oral health outcomes, and psychosocial impacts such as shame and quality of life, as well as the extent to which systemic health outcomes are discussed. This mapping approach highlights areas that appear well established in the review literature and those that remain under examined. The hypothesised pathways guiding this review are summarised in a working framework (Figure 1), which informed the coding and organisation of the included reviews.
2. Materials and Methods
2.1. Design and Reporting
We conducted a conceptual mapping review of review articles and reported it in accordance with a recently proposed mapping review reporting checklist [20]. To enhance transparency, we provide detailed reporting of the search, screening, and study selection process. This mapping review was not registered, and no a priori protocol was published. No stakeholders (e.g., patients, clinicians, policymakers) were involved in setting the question, conducting the review, or interpreting the findings; the review was initiated and conducted by the authors.
2.2. Eligibility Criteria
Articles were eligible for inclusion if they explicitly addressed DA, dental fear or phobia as a primary focus and discussed either determinants or consequences of DA and were published from 2005 to 2025. Articles were excluded if they did not treat DA as a central topic, focused exclusively on measurement properties or prevalence estimates without reference to determinants or consequences, dealt solely with management that were primarily clinically oriented or intervention approaches, or lacked an accessible abstract in English.
2.3. Search Strategy
To clarify how DA has been positioned within the existing literature, a structured database search of PubMed and Scopus was performed on 14 May 2025. Because our objective was to characterise the scope of DA-focused scholarship, we intentionally anchored the search to “dental anxiety/fear/phobia” and included only reviews that explicitly framed their topic in these terms (in the title/abstract/keywords), rather than broader reviews of dental attendance, avoidance, or access barriers that may not be DA-framed. In PubMed, the search string was: ("dental anxiety"[Title/Abstract] OR "dental fear"[Title/Abstract] OR "dental phobia"[Title/Abstract]) AND (review[Publication Type] OR "systematic review"[Title/Abstract] OR "narrative review"[Title/Abstract] OR "scoping review"[Title/Abstract] OR "meta-analysis"[Title/Abstract]) AND ("2005/01/01"[Date – Publication] : "2025/12/31"[Date – Publication]) AND (english[Language]). Searches were restricted to English-language publications. To widen coverage, Scopus was searched using the following query: TITLE-ABS-KEY("dental anxiety" OR "dental fear" OR "dental phobia") AND TITLE-ABS-KEY("review" OR "systematic review" OR "narrative review" OR "scoping review" OR "meta-analysis") AND PUBYEAR > 2004 AND PUBYEAR < 2026 AND (LIMIT-TO(DOCTYPE, "re")) AND (LIMIT-TO(LANGUAGE, "English")). The search was limited to English-language reviews published between 2005 and 2025. Reference lists of included articles were screened to identify any additional eligible reviews.
2.4. Study Selection and Data Extraction
All screening and data extraction were performed by a single reviewer (M.K.). Titles and abstracts were screened for relevance, with full texts assessed when necessary. Records were imported into Rayyan to support organised screening and reduce clerical error. For each included review, information was extracted on the review type (narrative, systematic, meta-analytic, scoping, or umbrella/overview) and on its substantive focus within the DA pathway. When reviews used mixed approaches, we classified them using a hierarchical rule (meta-analysis > systematic review > scoping > narrative) based on the methods contributing most directly to our mapping question. Each review was classified into one or more of the following domains: determinants (genetic, psychological, physiological, or environmental [experiences, sociodemographic factors and lifestyle factors]), dental avoidance or irregular attendance, oral health outcomes (such as dental caries or periodontal status), psychosocial impacts (shame/embarrassment, oral-health–related quality of life [OHRQoL], general quality of life [QoL]), and systemic health outcomes.
Coding rules. Coding was conducted in two passes by a single reviewer (M.K.). In the first pass, domains were coded using a binary scheme (covered vs not addressed) based primarily on titles/abstracts (and full texts when necessary), focusing on whether each review substantively addressed the domain. In the second pass, the reviewer refined the coding to a 3-level scheme (2=covered, 1=mentioned, 0=not addressed) and applied it consistently across all domains based on full-text assessment; this second-pass coding was performed with AI-assisted verification via independent AI-assisted coding (ChatGPT by OpenAI; GPT-5.2 Thinking, accessed February 2026) to flag potential inconsistencies between the reviewer’s and AI-assisted codes and to help locate supporting passages in the source text. AI outputs were used for verification only; all final codes were determined by the reviewer (M.K.).
For consequence domains (avoidance, oral outcomes, shame, OHRQoL, general QoL, systemic outcomes), we applied a strict consequence-only rule: these were coded only when framed as consequences of dental anxiety/fear (DA/DF; DA/DF→X). If framed as antecedents/correlates (X→DA/DF), the consequence domain was coded 0 and relevant content was captured under determinants (genetic, psychological, physiological, social-environmental) as appropriate. Procedure-related painful dental experiences were coded as social-environmental exposures, whereas stable pain/sensory sensitivity traits were coded as physiological determinants. The full prompt used for AI-assisted cross-checking is provided in Text S1.
We did not conduct a formal quality appraisal (risk-of-bias assessment) of included reviews because our aim was to map what topics were covered and how they were framed in the review literature, rather than to synthesise effect sizes or make judgements about intervention effectiveness.
2.5. Synthesis and Mapping
No meta-analysis was attempted. Instead, a mapping approach was used to situate each review along a proposed pathway from determinants to DA, avoidance, oral health outcomes, and psychosocial impacts. Counts of reviews in each domain and review type were summarised and visualised in two figures: a bar chart showing the distribution of review types across conceptual domains, and a pathway diagram illustrating the number and proportion of reviews occupying each stage of the oral–systemic continuum. This approach enabled the identification of areas where the literature is heavily concentrated as well as domains—such as systemic outcomes—that remain unexplored.
We did not pre-define quantitative thresholds for “adequate evidence.” Instead, we describe clusters as domains that were substantively covered by multiple reviews (coded as “covered”), and gaps as domains that were rarely covered or only briefly mentioned across the included reviews.
3. Results
In this conceptual mapping review of review articles published between 2005 and 2025, searches in PubMed (n=551) and Scopus (n=300) yielded a total of 851 records. After removal of 426 duplicates (50.1%), 425 unique records were screened. We excluded 383 records (reasons not mutually exclusive: administrative/management focus, n=204; not primarily addressing dental fear/anxiety, n=145; diagnosis/prevalence-only, n=33; other, n=5). A total of 40 reviews met the inclusion criteria (screening yield 9.6%). The full list of included reviews (n = 40) is provided in Table S1. The list of all screened records is publicly available in an open repository at https://doi.org/10.5281/zenodo.18523631.
Among the 40 included reviews, the most common format was narrative review (18/40, 45.0%), followed by systematic reviews (12/40, 30.0%) and meta-analyses (8/40, 20.0%). Scoping and umbrella reviews were rare (each 1/40, 2.5%).
Psychological determinants were covered in 31/40 reviews (77.5%), environmental determinants in 27/40 (67.5%), and physiological/biological determinants in 14/40 (35.0%). Genetic factors were rarely covered (3/40, 7.5%). Of the consequences, avoidance was covered in 25/40 reviews (62.5%) and oral health outcomes in 21/40 (52.5%). Psychosocial and quality-of-life outcomes were less often covered: shame/embarrassment in 5/40 (12.5%) and OHRQoL in 4/40 (10.0%). General quality of life was not covered in any review (0/40), but was mentioned in 17/40 (42.5%). Systemic health outcomes were rare, with 1/40 reviews (2.5%) covering them and 5/40 (12.5%) mentioning them.
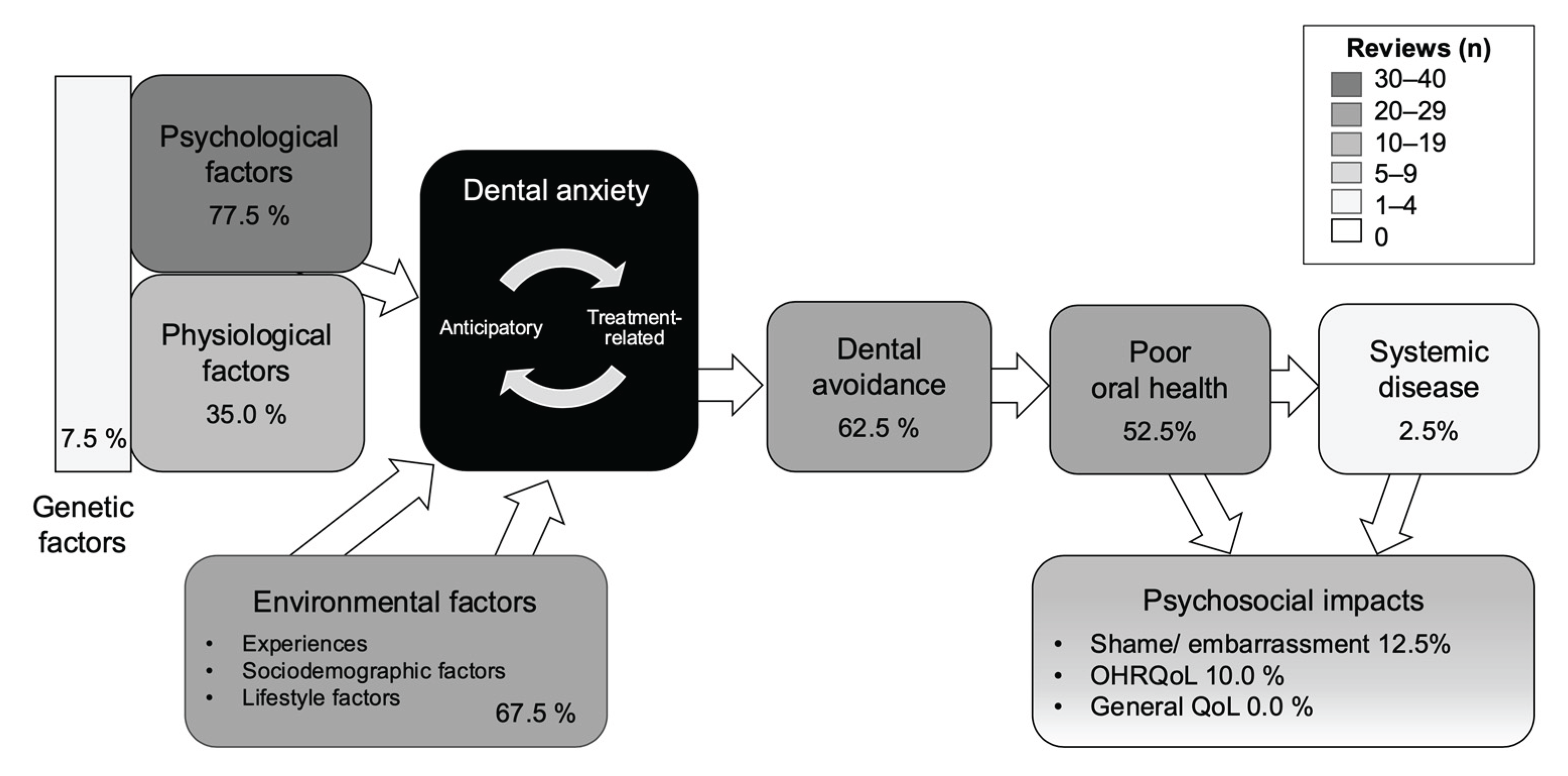
Figure 2 shows the number of reviews that covered and mentioned each domain. Figure 3 maps the coverage proportions onto the conceptual pathway used for classification. Together, the figures show that coverage is concentrated on determinants and on the core consequence from DA to avoidance and poor oral health. In contrast, domains beyond oral outcomes, particularly systemic health and psychosocial impacts, are sparsely covered.
4. Discussion
In this structured mapping of 40 review articles on dental anxiety (DA) published between 2005 and 2025, coverage was concentrated on determinants. Psychological and environmental factors were discussed most often. Consequences were less frequently covered, although around half of the reviews described dental avoidance and oral health outcomes. In contrast, psychosocial impacts, oral health-related quality of life, and systemic health outcomes were rarely covered. Overall, the mapped evidence supports a common pathway from DA to avoidance and poorer oral health, but shows clear gaps for outcomes beyond the oral health.
Reviews that addressed consequences mainly focused on dental avoidance and oral disease. Many papers referred to a cycle in which anxiety leads to avoidance and delayed care, which in turn contributes to worsening oral conditions. This pattern suggests a shared understanding that avoidance is a key behavioural link between DA and poorer oral health. Only a small number of reviews discussed shame or embarrassment as consequences of DA. When present, these terms often appeared within descriptions of a vicious cycle, in which avoidance and oral deterioration contribute to social and emotional burden. The low frequency of coverage suggests that psychosocial consequences remain under-synthesised in the review literature.
A small number of reviews examined oral health-related quality of life as an outcome of DA. A systematic review and meta-analysis in children and adolescents reported a small but consistent association between higher DA and poorer OHRQoL, and an association between poorer OHRQoL and lower self-esteem [21]. A recent systematic review in adults also supported a pathway in which higher DA is linked to reduced attendance and worse OHRQoL [22]. In contrast, general quality of life was mentioned in many reviews but was not treated as a primary outcome or synthesised as a main focus. This suggests that quality of life is increasingly recognised, but remains weakly integrated at the level of review synthesis.
Only one review explicitly modelled systemic health outcomes as consequences of DA, and only five reviews provided brief mentions. Beaudette et al. could extend the pathway to systemic health because they adopted an interdisciplinary framework linking oral health, dietary choices, and chronic disease risk, with DA positioned as an upstream driver [23]. This suggests that approaches that include bridge mechanisms such as diet and nutrition, chronic inflammation, and lifestyle factors may be needed to capture broader consequences beyond oral health. Among the five reviews with brief mention of systemic outcomes, only two named specific diseases, namely Aburas in an umbrella review [24] and Ying in a narrative review [25]. Ying most clearly described the gap, noting that while children’s dental fear is consistently linked to poor oral and mental health, whether DA predicts later systemic complications has not been directly studied [25]. Taken together, clarifying the public health impact of DA will require empirical studies, ideally longitudinal, that treat systemic disease as an outcome and test pathways involving bridge mechanisms.
Links between oral diseases and major systemic conditions such as diabetes, cardiovascular disease, and adverse pregnancy outcomes are now well established. Evidence from prospective cohorts and meta-analyses supports the role of chronic oral infection and inflammation in systemic disease pathways [2,26,27,28]. This scientific consensus has influenced global health policy. The World Health Organization now includes oral health within the framework of Universal Health Coverage and emphasises the importance of removing barriers that limit equitable access to oral health care [4]. Financial and organisational barriers are widely recognised, but DA also acts as major behavioural barrier to dental attendance [29,30,31]. Viewing DA only as an individual psychological concern or a clinical management issue may therefore be too narrow. A public health perspective highlights DA as a potential bottleneck that can widen inequalities in access, prevention, and timely treatment, and may help clarify how avoidance contributes to oral outcomes and quality of life at population level.
The mapping model used in this review was intentionally simplified to summarise areas of consensus across heterogeneous review types. It does not capture all plausible pathways, bidirectional relations, or confounding structures. Much of the underlying primary literature is cross-sectional, and most reviews could not make causal claims. It is also likely that DA sit within a broader network of shared risk factors for oral and systemic disease, including diet [32], tobacco use [33], physical inactivity [34], obesity [35,36], sleep problems [37], alcohol consumption [33], and autonomic nervous function [38], which have been associated with DA, but the evidence is still limited and needs to be confirmed. Integrating DA into common risk factor frameworks is a logical next step, but was beyond the scope of this mapping.
Future work could integrate DA into wider common risk factor frameworks to better understand how it interacts with these broader determinants. In addition, there is a paucity of theoretical development of the mechanisms through which DA might influence oral conditions and systemic disease. This gap is reflected in our mapping. The only review that covered systemic outcomes presented a model linking oral health, dietary choices, and chronic disease risk, with DA positioned as an upstream driver [23]. Future work should move beyond documenting associations and develop testable models with an explicit temporal design [39]. Methodologically, new tools are available to examine the processes by which high DA might influence wider health outcomes. Intensive longitudinal assessment can help test time lagged processes in daily life [40]. These developments may advance the field, especially if regular assessment of DA is introduced in clinical and population studies.
This review has strengths and limitations. Transparent and reproducible screening and classification procedures were applied, and the visual mapping approach allowed us to clearly identify neglected areas in the existing literature, including the near absence of systematic evidence on health outcomes. These features provide a structured overview that clarifies where current knowledge is concentrated and where important gaps remain. At the same time, several limitations should be considered. The search was limited to two major databases and to English-language publications, which may have resulted in omission of relevant grey literature or reviews published in other languages. Screening and categorisation were conducted by a single reviewer, and although predefined criteria and an AI-assisted check were used, the possibility of subjective judgement cannot be excluded. AI was used only to flag potential inconsistencies and did not replace author judgement. The final decisions were made by the reviewer, and the dataset and prompts are publicly available to support transparency and reproducibility. Finally, as a conceptual mapping review, the synthesis does not provide quantitative effect estimates, and heterogeneity across review types limits the extent to which findings can be directly compared.
5. Conclusions
In conclusion, review level evidence strongly supports a pathway from DA to avoidance and poorer oral health, but provides little synthesis on consequences beyond the oral domain. This gap matters because oral health is now recognised as part of overall health, and behavioural barriers to care can contribute to unequal access and delayed treatment. Future research should therefore test pathways from DA to quality of life and systemic outcomes, with clearly defined bridge mechanisms and appropriate temporal designs. This shift from describing associations to testing models is needed to place DA within a public health and equity framework.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Text S1. AI assisted cross check prompt used for domain classification; Table S1. Included review articles and domain coding with rationale (2005–2025): The full screening log is available via Zenodo (https://doi.org/10.5281/zenodo.18523631; files released upon publication).
Author Contributions
Conceptualization, M.K.; methodology, M.K..; software, M.K.; validation, M.K.,V.P., G.H and S.L.; formal analysis, M.K.; investigation, M.K.; resources, M.K.; data curation, M.K.; writing—original draft preparation, M.K.; writing—review and editing, M.K., V.P. G.H and S.L.; visualization, M.K.; supervision, S.L.; project administration, M.K.; funding acquisition, M.K. All authors have read and agreed to the published version of the manuscript.
Funding
Mika Kajita's (MK) contribution to this manuscript was co-funded by the European Union's Horizon Europe Framework Programme for Research and Innovation 2021–2027 under the Marie Skłodowska-Curie grant agreement no. 101126611, as part of the SYS-LIFE postdoctoral programme.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
The list of all screened records is publicly available in an open repository at https://doi.org/10.5281/zenodo.18523631. The full list of included reviews and the rating table, and the AI prompts used in this study are provided in the Supplementary Materials.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (OpenAI) to support drafting evidence notes, consistency checks, and English-language editing, and to flag potential inconsistencies during screening and categorisation based on predefined criteria. The authors reviewed, verified, and edited all content and take full responsibility for the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DA | Dental anxiety |
| DSM | Diagnostic and Statistical Manual of Mental Disorders |
| SANRA | Scale for the Assessment of Narrative Review Articles |
| OHRQoL | Oral Health–Related Quality of Life |
| WHO | World Health Organization |
| UHC | Universal Health Coverage |
References
- Armfield, J.M. What goes around comes around: revisiting the hypothesized vicious cycle of dental fear and avoidance. Community Dent Oral Epidemiol 2013, 41, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Mascarenhas, P.; Viana, J.; Proença, L.; Orlandi, M.; Leira, Y.; Chambrone, L.; Mendes, J.J.; Machado, V. An umbrella review of the evidence linking oral health and systemic noncommunicable diseases. Nat Commun 2022, 13, 7614. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Sanz, M.; Shapira, L.; Brotons, C.; Chapple, I.; Frese, T.; Graziani, F.; Hobbs, F.D.R.; Huck, O.; Hummers, E.; et al. Association between periodontal diseases and cardiovascular diseases, diabetes and respiratory diseases: Consensus report of the Joint Workshop by the European Federation of Periodontology (EFP) and the European arm of the World Organization of Family Doctors (WONCA Europe). J Clin Periodontol 2023, 50, 819–841. [Google Scholar] [CrossRef] [PubMed]
- World Health Assembly. WHA74.5: Oral health; World Health Organization, 31 May 2021. [Google Scholar]
- Ost, L.-G.; Skaret, E. Cognitive behavioral therapy for dental phobia and anxiety; Wiley-Blackwell: Oxford, 2013. [Google Scholar]
- Humphris, G.M.; Newton, J.T. Is the Modified Dental Anxiety Scale (MDAS) a Single or Two Construct Measure? A Theoretical and Pragmatic Perspective. Dent J (Basel) 2025, 13. [Google Scholar] [CrossRef]
- Rachman, S. The conditioning theory of fear-acquisition: a critical examination. Behav Res Ther 1977, 15, 375–387. [Google Scholar] [CrossRef]
- Weiner, A.A.; Sheehan, D.V. Etiology of dental anxiety: psychological trauma or CNS chemical imbalance? Gen Dent 1990, 38, 39–43. [Google Scholar]
- Locker, D.; Poulton, R.; Thomson, W.M. Psychological disorders and dental anxiety in a young adult population. Community Dent Oral Epidemiol 2001, 29, 456–463. [Google Scholar] [CrossRef]
- Armfield, J.M.; Slade, G.D.; Spencer, A.J. Cognitive vulnerability and dental fear. BMC Oral Health 2008, 8, 2. [Google Scholar] [CrossRef]
- McNeil, D.; Randall, C. Dental fear and anxiety associated with oral health care: Conceptual and clinical issues 2014, 165–192.
- Mowrer, O. On the dual nature of learning—a re-interpretation of" conditioning" and" problem-solving. In Harvard educational review; 1947. [Google Scholar]
- Lethem, J.; Slade, P.D.; Troup, J.D.G.; Bentley, G. Outline of a fear-avoidance model of exaggerated pain perception—I. Behaviour Research and Therapy 1983, 21, 401–408. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. PAIN 2000, 85, 317–332. [Google Scholar] [CrossRef]
- Berggren, U.; Meynert, G. Dental fear and avoidance: causes, symptoms, and consequences. J Am Dent Assoc 1984, 109, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Wide, U.; Hakeberg, M. Treatment of Dental Anxiety and Phobia-Diagnostic Criteria and Conceptual Model of Behavioural Treatment. Dent J (Basel) 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Folker, L.; Dolezal, L.; Jespersen, A.P.; Paisi, M.; Withers, L.; Worle, C.; Øzhayat, E.B. Dental Shame: A Call for Understanding and Addressing the Role of Shame in Oral Health. Community Dent Oral Epidemiol 2026, 54, 1–6. [Google Scholar] [CrossRef]
- Liinavuori, A.; Tolvanen, M.; Pohjola, V.; Lahti, S. Longitudinal interrelationships between dental fear and dental attendance among adult Finns in 2000-2011. Community Dent Oral Epidemiol 2019, 47, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Sukumaran, I.; Taylor, S.; Thomson, W.M. The prevalence and impact of dental anxiety among adult New Zealanders. Int Dent J 2020, 71, 122–126. [Google Scholar] [CrossRef]
- Li, Y.; Ghogomu, E.; Hui, X.; Fenfen, E.; Campbell, F.; Khalil, H.; Li, X.; Gaarder, M.; Nduku, P.M.; White, H.; et al. Key concepts and reporting recommendations for mapping reviews: A scoping review of 68 guidance and methodological studies. Research Synthesis Methods 2025, 16, 157–174. [Google Scholar] [CrossRef]
- Alharbi, A.; Freeman, R.; Humphris, G. Dental anxiety, child-oral health related quality of life and self- esteem in children and adolescents: a systematic review and meta-analysis. Community Dent Health 2021, 38, 119–126. [Google Scholar] [CrossRef]
- Mohd Radzi, N.A.; Malek, A.; Firdaus, M.; Che Musa, M.F.; Luai, A. Relationship Between Dental Anxiety, Dental Utilization, and Oral Health-Related Quality of Life: A Systematic Review. Journal of International Oral Health 2024, 16, 335–349. [Google Scholar] [CrossRef]
- Beaudette, J.R.; Fritz, P.C.; Sullivan, P.J.; Ward, W.E. Oral Health, Nutritional Choices, and Dental Fear and Anxiety. Dent J (Basel) 2017, 5. [Google Scholar] [CrossRef]
- Aburas, S.; Pfaffeneder-Mantai, F.; Hofmann, A.; Meller, O.; Schneider, B.; Turhani, D. Dentophobia and dental treatment: An umbrella review of the published literature. Spec Care Dentist 2023, 43, 163–173. [Google Scholar] [CrossRef]
- Ying, J.; Tao, H.; He, Q.; Zhang, Z.; Hu, W.; Chen, S.; Guan, Y. Children's Dental Fear: Occurrence Mechanism and Prevention Guidance. J Multidiscip Healthc 2023, 16, 2013–2021. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D'Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J Clin Periodontol 2020, 47, 268–288. [Google Scholar] [CrossRef] [PubMed]
- Byon, M.-J.; Kim, S.-Y.; Kim, J.-S.; Kim, H.-N.; Kim, J.-B. Association of Periodontitis with Atherosclerotic Cardiovascular Diseases: A Nationwide Population-based Retrospective Matched Cohort Study. International Journal of Environmental Research and Public Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Beukers, N.; Su, N.; Loos, B.G.; van der Heijden, G. Lower Number of Teeth Is Related to Higher Risks for ACVD and Death-Systematic Review and Meta-Analyses of Survival Data. Front Cardiovasc Med 2021, 8, 621626. [Google Scholar] [CrossRef]
- Pohjola, V.; Lahti, S.; Vehkalahti, M.M.; Tolvanen, M.; Hausen, H. Association between dental fear and dental attendance among adults in Finland. Acta Odontol Scand 2007, 65, 224–230. [Google Scholar] [CrossRef]
- Armfield, J.M.; Stewart, J.F.; Spencer, A.J. The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health 2007, 7, 1. [Google Scholar] [CrossRef]
- Milgrom, P.; Newton, J.T.; Boyle, C.; Heaton, L.J.; Donaldson, N. The effects of dental anxiety and irregular attendance on referral for dental treatment under sedation within the National Health Service in London. Community Dent Oral Epidemiol 2010, 38, 453–459. [Google Scholar] [CrossRef]
- Begdache, L.; Ahmed, E.; Malik, S.; Karakaya, M.F. Dental Anxiety and Its Association with Dietary Intake and Food Groups: A Cross-Sectional Study. Dentistry Journal 2023, 11, 240. [Google Scholar] [CrossRef]
- Pohjola, V.; Mattila, A.K.; Joukamaa, M.; Lahti, S. Alcohol use disorder, smoking and dental fear among adults in Finland. Acta Odontol Scand 2013, 71, 300–306. [Google Scholar] [CrossRef]
- Lindenberger, B.L.; Plag, J.; Schumacher, S.; Gaudlitz, K.; Bischoff, S.; Bobbert, T.; Dimeo, F.; Petzold, M.B.; Kirschbaum, C.; Dudás, Z.; et al. Clinical and neurobiological effects of aerobic exercise in dental phobia: A randomized controlled trial. Depress Anxiety 2017, 34, 1040–1048. [Google Scholar] [CrossRef]
- Helal, N.; Faran, L.Y.; Dashash, R.A.; Turkistani, J.; Tallab, H.Y.; Aldosari, F.M.; Alhafi, S.I.; Sabbagh, H.J. The relationship between Body Mass Index and dental anxiety among pediatric patients in Jeddah, Saudi Arabia: a cross-sectional study. BMC Oral Health 2025, 25, 609. [Google Scholar] [CrossRef]
- Sharifian, M.J.; Pohjola, V.; Kunttu, K.; Virtanen, J.I. Association between dental fear and eating disorders and Body Mass Index among Finnish university students: a national survey. BMC Oral Health 2021, 21, 93. [Google Scholar] [CrossRef]
- Almoznino, G.; Zini, A.; Sharav, Y.; Shahar, A.; Zlutzky, H.; Haviv, Y.; Lvovsky, A.; Aframian, D.J. Sleep quality in patients with dental anxiety. J Psychiatr Res 2015, 61, 214–222. [Google Scholar] [CrossRef]
- Somero, A.; Suominen, A.; Pohjola, V.; Ogawa, M.; Sipilä, K.; Kakko, N.; Tulppo, M.; Lahti, S. Autonomic Nervous System Activity and Dental Anxiety in the Northern Finland Birth Cohort (NFBC1966) Population. Dent J (Basel) 2024, 12. [Google Scholar] [CrossRef]
- Collins, L.M. Analysis of longitudinal data: the integration of theoretical model, temporal design, and statistical model. Annu Rev Psychol 2006, 57, 505–528. [Google Scholar] [CrossRef]
- Laurenceau, J.-P.; DiGiovanni, A.M.; Bolger, N. Intensive Longitudinal Methods: Toward a Psychological Science of Daily Life. Annual Review of Psychology 2026, 77, 513–541. [Google Scholar] [CrossRef]
Figure 1.
Conceptual model of dental fear and anxiety from determinants to oral and systemic consequences. Abbreviations: OHRQoL, oral health-related quality of life; QoL, quality of life.
Figure 1.
Conceptual model of dental fear and anxiety from determinants to oral and systemic consequences. Abbreviations: OHRQoL, oral health-related quality of life; QoL, quality of life.
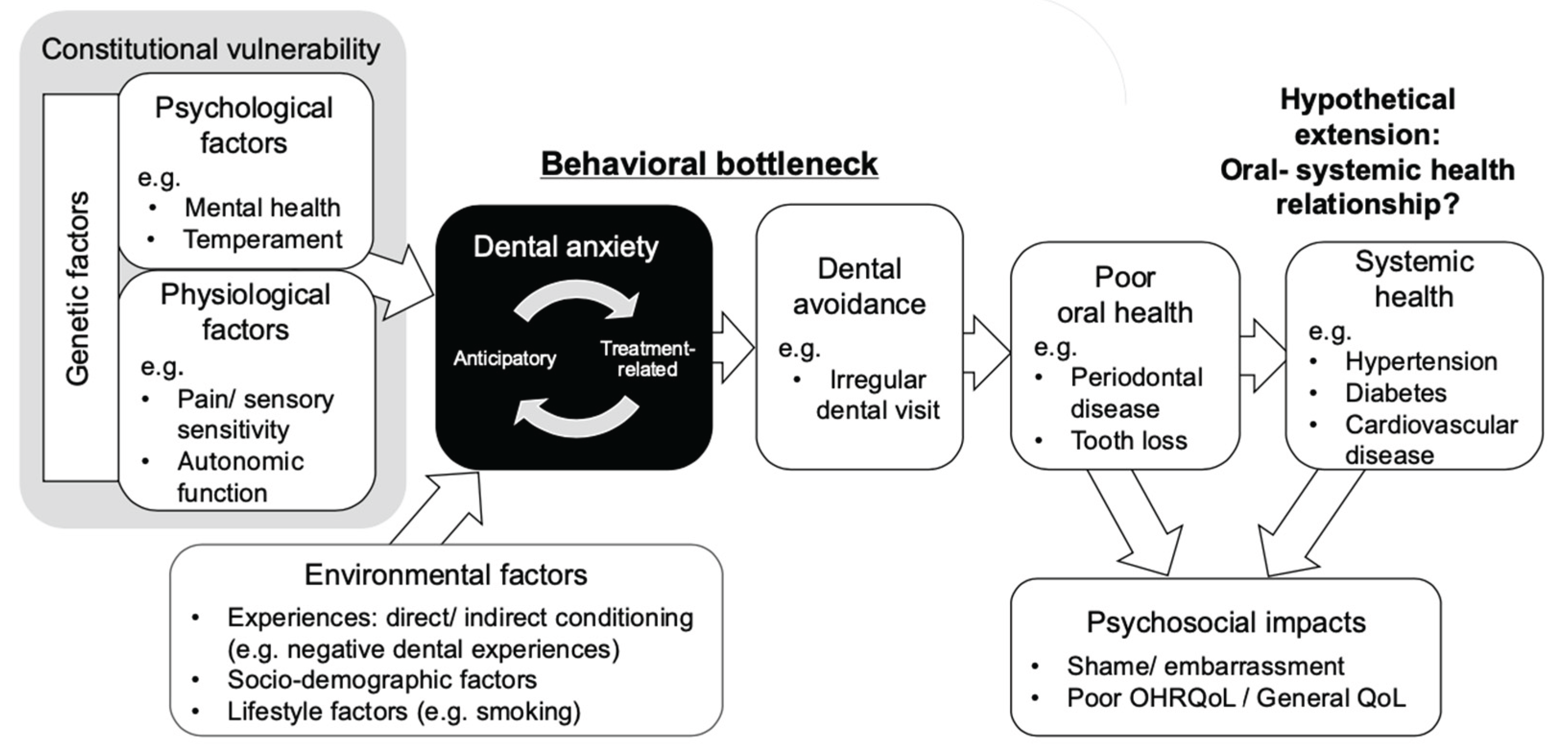
Figure 2.
Domain coverage in dental anxiety reviews (n=40): covered vs mentioned. Abbreviations: Genetics = genetic factors/heritability related to dental anxiety/fear; Psych = psychological factors; Bio/phys = biological/physiological factors; Env = social and contextual factors; Shame/embarrass = shame, embarrassment; OHRQoL = oral health–related quality of life as a consequence; General QoL = overall quality of life/daily functioning as a consequence.
Figure 2.
Domain coverage in dental anxiety reviews (n=40): covered vs mentioned. Abbreviations: Genetics = genetic factors/heritability related to dental anxiety/fear; Psych = psychological factors; Bio/phys = biological/physiological factors; Env = social and contextual factors; Shame/embarrass = shame, embarrassment; OHRQoL = oral health–related quality of life as a consequence; General QoL = overall quality of life/daily functioning as a consequence.
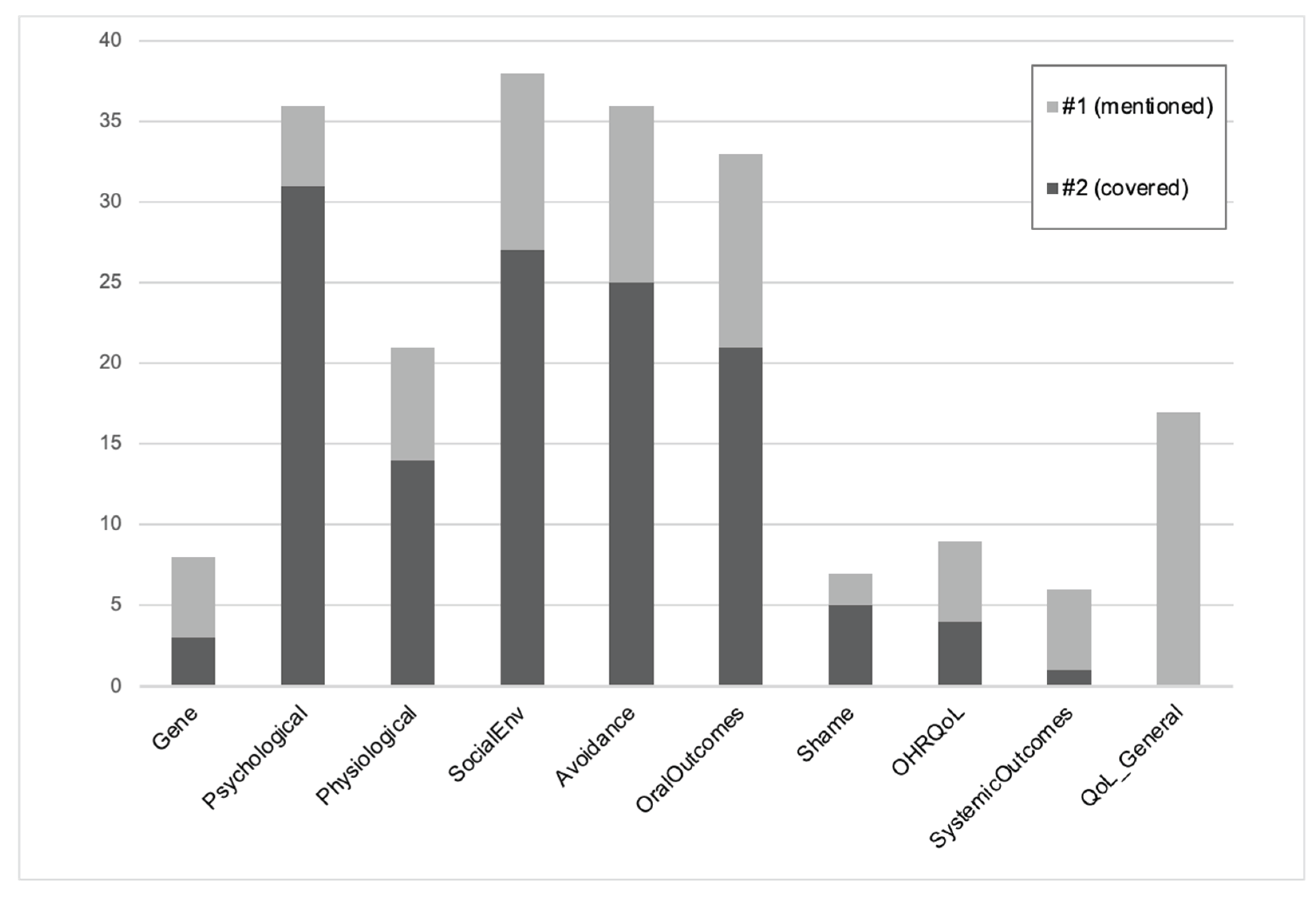
Figure 3.
summarises the distribution of reviews across the putative pathway from determinants to systemic outcomes. Proportions indicate the percentage of included reviews (n=40) that covered each domain. Shading reflects the number of reviews per category. Abbreviations: OHRQoL, oral health-related quality of life; QoL, quality of life.
Figure 3.
summarises the distribution of reviews across the putative pathway from determinants to systemic outcomes. Proportions indicate the percentage of included reviews (n=40) that covered each domain. Shading reflects the number of reviews per category. Abbreviations: OHRQoL, oral health-related quality of life; QoL, quality of life.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



