
Submitted:
13 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Research into auxetic foams and their impact on ground reaction forces (GRFs) across diverse neuropathic etiologies is limited. Auxetic foams—closed-cell materials with a negative Poisson’s ratio—conform to irregular foot structures, offering significant rehabilitative potential to mitigate symptoms by optimizing GRF reduction and enhancing gait. Currently, there is a lack of versatile orthoses capable of addressing the heterogeneous subtypes of foot neuropathy. Conducted in collaboration with the National Aeronautics Space Administration/Marshall Space Flight Center (NASA/MSFC), this feasibility study evaluates the efficacy of auxetic foam insoles in reducing vertical GRFs and improving gait across various neuropathic conditions, comparing performance against standard over-the-counter (OTC) insoles. Six participants (five with varying neuropathic etiologies and one healthy control) performed walking trials across force plates (NUL225, NEULOG) under three conditions: barefoot (with socks), OTC insoles, and fabricated auxetic foam insoles. A 3 × 5 Kruskal-Wallis test analyzed the impact of insole type and neuropathic condition on vertical GRFs (?=0.05). Results indicated a significant interaction between insole type and neuropathy. Auxetic foam insoles effectively reduced GRFs in participants with diabetic, neuropathic arthritis, and personal injury-related neuropathy. Qualitative assessments further demonstrated that auxetic foam significantly improved coordination and gait compared to OTC alternatives.
Keywords:
neuropathy
; ground reaction forces
; gait
; auxetic foams
; insoles
; orthotics
; rehabilitation
; health systems engineering
1. Introduction
Peripheral neuropathy encompasses disorders of the nerves outside the brain and spinal cord [1]. Affecting over 20 million people, this condition arises from metabolic, autoimmune, and hereditary factors, as well as trauma, infection, or radiation [1,2,3,4]. Nerve damage often results in impaired balance and coordination, which manifests as increased Ground Reaction Forces (GRFs) during locomotion [1,2,3,4].
GRFs are critical metrics in orthotic design, categorized into vertical, mediolateral, and anterior-posterior components. Vertical GRF is the primary focus for clinicians as it represents the largest force component during gait and is essential for musculoskeletal injury analysis, gait abnormality detection, and the evaluation of prosthetic and orthotic interventions [5,6,7,8,9,10,11,12,13,14,15,16,17,18].
Current orthotic designs primarily target diabetes-related neuropathy, the most prevalent subtype [19,20,21,22,23,24]. Consequently, existing rehabilitative orthoses often overlook other etiologies (e.g., oncology or trauma-related neuropathy) and fail to utilize novel materials that might better mitigate balance and coordination deficits. A comprehensive understanding of specific pathologies and foot types is necessary to inform effective rehabilitative strategies [25,26]. Given the complexity of neuropathy, management must include a detailed evaluation of etiology-specific characteristics, including GRFs [26].
Orthotics alleviate neuropathic pain by providing cushioning and reducing pressure points [27,28,29]. While custom-made orthotics are generally preferred [29,30,31], auxetic foams offer a novel alternative. Characterized by a negative Poisson’s ratio—meaning they expand when stretched and contract when compressed [31] (Figure 1) —these materials provide superior shape conformity, energy absorption, and indentation resistance [32,33,34,35,36,37,38,39]. These unique properties suggest that auxetic foams may be more effective than traditional materials at reducing GRFs across heterogeneous neuropathic subtypes.
2. Materials and Methods
Participants
Six participants were recruited from NASA (Table 1). The cohort included five individuals with neuropathy attributed to diabetes (Subjects A & C), arthritis (Subject B), cancer (Subject D), and personal injury (Subject F), plus one healthy control (Subject E). Subject F utilized leg braces for additional stability. Inclusion criteria mandated a minimum age of 40 years to reflect the higher epidemiological prevalence of peripheral neuropathy in older populations. With the exception of the healthy control, all participants were required to have a confirmed diagnosis of neuropathy. All participants provided informed consent as approved by NASA’s Institutional Review Board.
Auxetic Foam and Insole Fabrication
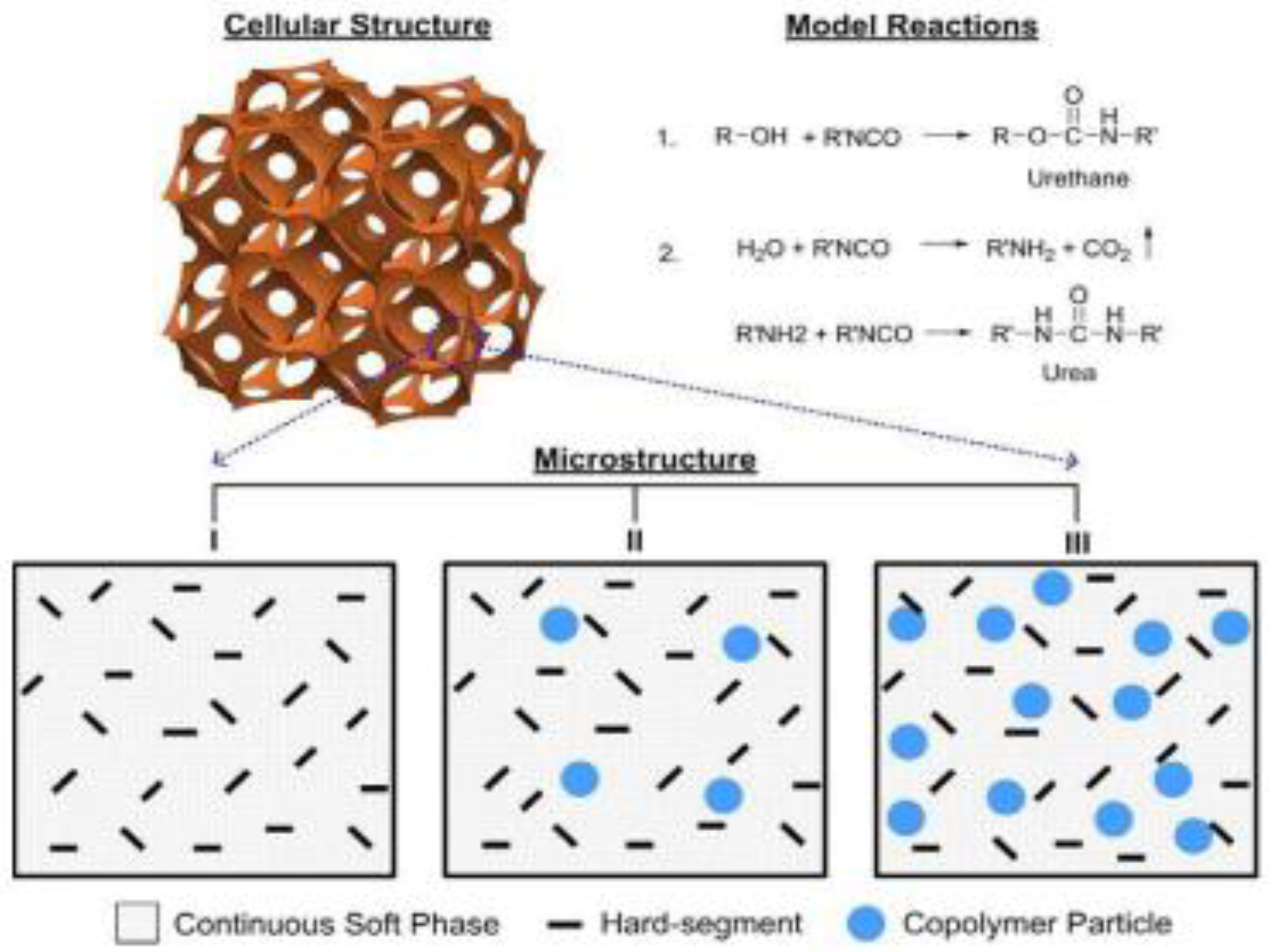
The auxetic material was manufactured at FAMU-FSU via tri-axial compression of conventional polyurethane (PU) foam under elevated temperatures. This process induces buckling of the reticular cell ribs to create a re-entrant structure, which is then fixed into place [38,39]. The material formulation involved reactive foaming and phase separation of urethane, alcohol, and water( Figure 1b).
Figure 1.
b. Illustration of typical polyurethane foaming reaction and phase-separated morphology.
To ensure proper fit, insoles were extracted from standard OTC brands (Eduropro, Comfort Gel, and Athletic Works) to serve as templates. These templates were traced onto the auxetic foam and cut to size, ensuring compatibility with the participants' existing footwear (sizes 6–13) (Figure 2).
Procedures
Baseline data, including age, weight, stride length, and shoe size, were recorded upon arrival(Table 1). Participants performed six walking trials at a self-selected pace across four force plates (Figure 3). Each trial consisted of walking four steps, turning, and returning to the starting position to ensure data collection for both the left and right feet. Testing was conducted under three conditions:
1. Barefoot (with socks).
2. OTC Insoles (non-auxetic).
3. Auxetic Foam Insoles.
Subject F performed additional trials with and without leg braces to isolate the impact of the auxetic material on their specific orthotic requirements. In each cycle, the participants’ peak vertical GRFS were evaluated (Tables A 2–5), and their gait cycles were simultaneously observed using motion capture (MARVUE Video Camera Camcorder 2D device). Figure 3(b) illustrates a participant in the barefoot condition. Data from the fourth force plate were excluded from the final analysis due to inconsistent foot strikes; consequently, peak vertical GRFs from the remaining three plates were utilized.
Figure 3.
b.Subject walking and representative measurement of GRF in the barefoot(with socks) condition.
Figure 3.
b.Subject walking and representative measurement of GRF in the barefoot(with socks) condition.

Measures and Analysis
Peak vertical GRFs and qualitative comfort assessments were compared between auxetic foam and OTC insoles. Due to the small sample size, normality was not assumed; therefore, this feasibility study utilized 3 × 5 (insole × neuropathy subtype) Kruskal-Wallis tests. To account for the two subjects with diabetic neuropathy (A and C) and the use of leg braces by Subject F, four separate statistical iterations were performed(Tables A 6–9). These groupings allowed for a granular analysis of how auxetic material impacts GRFs across specific neuropathic subtypes. The independent variables were insole condition and neuropathic subtype, while peak vertical GRF served as the dependent variable. Data were numerically coded for group identification. The alpha level was set at p<0.05, with a post-hoc Dunn’s test applied to identify specific pairwise differences. Additionally, mean vertical GRFs were calculated per condition to quantify the percentage increase or decrease associated with the auxetic material.
3. Results
Statistically significant differences in vertical GRFs were observed across neuropathic subtypes and insole conditions ( p=0.0001; Tables A 6–9), confirming that both the etiology and the orthotic material significantly influence force distribution. An interaction effect between insole type and neuropathy was also identified. Specifically, auxetic foam reduced vertical GRFs in Subject A (diabetes), Subject D (arthritis), and Subject F (injury, without braces) compared to OTC insoles (Figure 4). Conversely, slight increases in GRFs were noted in Subjects B (cancer), C (diabetes), E (control), and F (injury, with braces) (Figure 5). These increases were attributed to external factors: swift walking cadences in Subjects E and C, the absence of assistive walking sticks for Subject B, and the mechanical influence of leg braces for Subject F. Despite varied GRF data, motion capture confirmed that all participants exhibited improved gait cycles when using the auxetic material.
4. Discussion
This study assessed the efficacy of auxetic foams—multi-phase cellular materials with a negative Poisson’s ratio—in attenuating vertical GRFs compared to standard OTC insoles. This research challenges traditional orthotic design paradigms by applying systems engineering principles to address diverse neuropathic subtypes beyond diabetes. A robust engineering system must account for the synergy between its subsystems; here, the pathological variables of neuropathy and the mechanical properties of rehabilitative orthoses are treated as inseparable components of the patient’s ambulatory system.
The synthesized foam features a re-entrant structure that integrates hard domains for structural integrity with soft domains for elasticity (Figure 1b). Unlike conventional materials, auxetics expand under tension, providing superior shock absorption and pressure relief. The data confirmed that significant performance differences exist across heterogeneous neuropathic conditions. While GRF reductions in Subjects A, D, and F highlight the material's potential for pressure attenuation, instances of increased GRFs in other subjects were likely driven by confounding variables, such as increased gait velocity or the absence of standard mobility aids, rather than material failure. Ultimately, the auxetic foam enhanced gait symmetry for all participants, suggesting benefits beyond simple force reduction that include improved proprioceptive control and overall system stability.
Qualitative Findings
Qualitatively, the auxetic foam insoles significantly enhanced gait by providing superior support and facilitating a more natural heel-to-toe weight transfer.
• Subject A (Diabetic Neuropathy): Transitioned from an antalgic, "twisted" walk with frequent pauses to a fluid, natural gait (Figure 6).
• Subject B (Cancer-related Neuropathy): Showed a reduction in a pre-existing limp, though pauses remained due to the absence of their usual walking sticks.
• Subject C (Diabetic Neuropathy): Exhibited improved weight distribution, though a swifter walking pace resulted in higher recorded forces.
• Subject D (Arthritic Neuropathy): Corrected a steppage gait; instead of landing on the toes, the subject achieved a midfoot-to-heel strike, resulting in a visible improvement in coordination and reduced GRFs (Figure 7).
• Subject E (Control): Displayed greater stability and control despite an increase in force due to a naturally rapid cadence.
• Subject F (Injury-related Neuropathy): Showed a reduction in steppage gait characteristics, gaining more stability from the material's conforming properties.
Limitations and Future Research
This study represents an initial feasibility investigation; thus, the auxetic foam material remains exploratory. In addition to the small sample size, the findings have several limitations. The participant cohort provided only a narrow representation of the broader neuropathic population. Future research should include a larger, more diverse population that varies in age, duration of symptoms, and the specific etiologies of cancer, diabetes, or injury that led to neuropathy. Recruitment challenges due to participants' occupational demands were also noted.
Furthermore, discerning the precise root causes of neuropathy proved challenging when participants presented with potential dual etiologies (e.g., Subject D attributed their condition primarily to arthritis but also had a history of cancer). Such confounding variables complicate the ability to definitively pinpoint the neuropathic cause.
Future iterations of this research should focus on the specificities of these variables (e.g., type 1 vs. type 2 diabetes, type of cancer, nature of injury) during the assessment. Additionally, incorporating more kinematic assessments would allow for an analysis of the auxetic foam’s impact on targeted muscle groups. These steps are necessary to inform the improved design of orthoses for diverse neuropathic conditions.
5. Conclusions
The auxetic foam material proved to be an effective aid in reducing peak vertical GRFs in a subset of neuropathic participants and improving gait cycles across various neuropathic subtypes compared to standard OTC insoles. While the effectiveness varied among subjects, the auxetic foam consistently enhanced comfort and stability for all participants. Overall, the study demonstrated both kinematic and kinetic improvements, warranting further investigation into this promising orthotic material.
Author Contributions:. Conceptualization, L.B..; Methodology, L.B., C.Z., E.J. and S.P.; Software, L.B. and C.Z..; Validation, L.B., C.Z., E.J., and S.P.; Formal Analysis, L.B.; Investigation, L.B, C.Z., E.J., and S.P..; Resources, L.B., C.Z, and E.J..; Data Curation, L.B.; Writing – Original Draft Preparation, L.B. and C.Z. .; Writing – Review & Editing, L.B., C.Z., E.J., and S.P..; Supervision, L.B., C.Z., E.J., and S.P; Project Administration, L.B.
Funding
This research was funded by NASA/MSFC, grant number 80NSSC20M0247 and via in-kind resources by the Department of Industrial and Manufacturing Engineering and High-Performance Materials Institute at Florida Agricultural and Mechanical University under Grant 80NSSC20M0247.
Data Availability Statement
The data related to these studies is available on request from the Corresponding Author.
Acknowledgments
This work was supported by NASA/MSFC, University of Alabama Birmingham(UAB) College of Engineering, and Florida Agricultural and Mechanical University-Florida State University (FAMU-FSU) College of Industrial and Manufacturing Engineering. This work included contributions to the material study design and analysis and CAD analysis from the NASA EM and ES Engineering branches, in which acknowledgement is attributed to Enrique Jackson, Charles D. Wingard, Kevin Young, Leslie Alexander, Barbara Breithaupt, and Eleanor Dickens.
Other acknowledgements are attributed to NASA-MSFC’s former interns and Small Business Technical Coordinator as follows: Danyale Berry (DB), Clarke Miley (CM), Kyra Lee (KL), Chase Robinson, (CR), Ihsaan El-Amin (IE), McKenzie Davis (MD), Laurence Price-Webb (LP, and Angela Lovelady.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| GRF | Ground reaction force |
| NASA | National Aeronautics Space Administration |
| MSFC | Marshall Space Flight Center |
| OTC | Over-the-counter |
Appendix A

Table A2.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects A, B, D, E, and F(with braces).
Table A2.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects A, B, D, E, and F(with braces).
| GRFS data(In Newtons(N)); Subjects A, B, D, E, and F(with braces) | |||||
| Group | Cancer | Diabetes | Disease | Control | Injury |
| Barefoot | 771 | 918 | 817 | 689 | 912 |
| 804 | 938 | 802 | 697 | 864 | |
| 800 | 943 | 466 | 698 | 896 | |
| 793 | 953 | 784 | 690 | 902 | |
| 761 | 923 | 811 | 667 | 892 | |
| 793 | 956 | 779 | 665 | 893 | |
| No auxetic | 764 | 963 | 712 | 709 | 794 |
| 783 | 990 | 798 | 703 | 836 | |
| 798 | 963 | 765 | 432 | 951 | |
| 790 | 969 | 792 | 388 | 953 | |
| 767 | 929 | 787 | 610 | 965 | |
| 797 | 974 | 775 | 730 | 932 | |
| Auxetic | 796 | 957 | 777 | 774 | 944 |
| 826 | 961 | 772 | 674 | 935 | |
| 793 | 939 | 756 | 729 | 981 | |
| 784 | 925 | 757 | 709 | 908 | |
| 790 | 955 | 572 | 738 | 883 | |
| 783 | 958 | 784 | 714 | 932 | |
Table A2 presents the vertical ground reaction forces (GRFs) measured in Newtons (N) for Subjects A, B, D, E, and F (F used braces). Data is grouped into three conditions: barefoot walking, walking with standard insoles ("No auxetic"), and walking with experimental auxetic foam insoles ("Auxetic"). Subject C is excluded from this table to isolate specific neuropathic categories, with Subject A serving as the representative for diabetic neuropathy in this analysis.
Table A3.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects A, B, D, E, and F(without braces).
Table A3.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects A, B, D, E, and F(without braces).
| GRFS data(In Newtons(N)); Subjects A, B, D, E, and F(without braces) | |||||
| Group | Cancer | Diabetes | Disease | Control | Injury |
| Barefoot | 771 | 918 | 817 | 689 | 912 |
| 804 | 938 | 802 | 697 | 864 | |
| 800 | 943 | 466 | 698 | 896 | |
| 793 | 953 | 784 | 690 | 902 | |
| 761 | 923 | 811 | 667 | 892 | |
| 793 | 956 | 779 | 665 | 893 | |
| No auxetic | 764 | 963 | 712 | 709 | 794 |
| 783 | 990 | 798 | 703 | 836 | |
| 798 | 963 | 765 | 432 | 951 | |
| 790 | 969 | 792 | 388 | 953 | |
| 767 | 929 | 787 | 610 | 965 | |
| 797 | 974 | 775 | 730 | 932 | |
| Auxetic | 796 | 957 | 777 | 774 | 807 |
| 826 | 961 | 772 | 674 | 935 | |
| 793 | 939 | 756 | 729 | 631 | |
| 784 | 925 | 757 | 709 | 856 | |
| 790 | 955 | 572 | 738 | 779 | |
| 783 | 958 | 784 | 714 | 832 | |
Table A3 presents the vertical ground reaction forces (GRFs) measured in Newtons (N) for subjects A, B, D, E, and F. This data specifically focuses on conditions where Subject F used no braces. The data is grouped into three conditions: barefoot walking, walking with standard insoles ("No auxetic"), and walking with experimental auxetic foam insoles ("Auxetic"). Subject C is excluded from this table to isolate specific neuropathic categories, with Subject A serving as the representative for diabetic neuropathy in this analysis.
Table A4.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects B, C, D, E, and F(with braces).
Table A4.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects B, C, D, E, and F(with braces).
| GRFS data (In Newtons(N)); Subjects B, C, D, E, and F(with braces) | |||||
| Group | Cancer | Diabetes | Disease | Control | Injury |
| Barefoot | 771 | 1119 | 817 | 689 | 912 |
| 804 | 1095 | 802 | 697 | 864 | |
| 800 | 1165 | 466 | 698 | 896 | |
| 793 | 1148 | 784 | 690 | 902 | |
| 761 | 1102 | 811 | 667 | 892 | |
| 793 | 1078 | 779 | 665 | 893 | |
| No auxetic | 764 | 1130 | 712 | 709 | 794 |
| 783 | 1030 | 798 | 703 | 836 | |
| 798 | 1111 | 765 | 432 | 951 | |
| 790 | 1070 | 792 | 388 | 953 | |
| 767 | 1147 | 787 | 610 | 965 | |
| 797 | 1131 | 775 | 730 | 932 | |
| Auxetic | 796 | 1106 | 777 | 774 | 944 |
| 826 | 1145 | 772 | 674 | 935 | |
| 793 | 1121 | 756 | 729 | 981 | |
| 784 | 1098 | 757 | 709 | 908 | |
| 790 | 1127 | 572 | 738 | 883 | |
| 783 | 1116 | 784 | 714 | 932 | |
Table A4 presents the vertical ground reaction forces (GRFs) measured in Newtons (N) for Subjects B, C, D, E, and F (with braces). Data is grouped into three conditions: barefoot walking, walking with standard insoles ("No auxetic"), and walking with experimental auxetic foam insoles ("Auxetic"). Subject A is excluded from this table to isolate specific neuropathic categories, with Subject C serving as the representative for diabetic neuropathy in this analysis.
Table A5.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects B, C, D, E, and F(without braces).
Table A5.
Vertical Ground Reaction Forces (GRFs) Data in Newtons (N) for Subjects B, C, D, E, and F(without braces).
| GRFS data (In Newtons(N)); Subjects B, C, D, E, and F(without braces) | |||||
| Group | Cancer | Diabetes | Disease | Control | Injury |
| Barefoot | 771 | 1119 | 817 | 689 | 912 |
| 804 | 1095 | 802 | 697 | 864 | |
| 800 | 1165 | 466 | 698 | 896 | |
| 793 | 1148 | 784 | 690 | 902 | |
| 761 | 1102 | 811 | 667 | 892 | |
| 793 | 1078 | 779 | 665 | 893 | |
| No auxetic | 764 | 1130 | 712 | 709 | 794 |
| 783 | 1030 | 798 | 703 | 836 | |
| 798 | 1111 | 765 | 432 | 951 | |
| 790 | 1070 | 792 | 388 | 953 | |
| 767 | 1147 | 787 | 610 | 965 | |
| 797 | 1131 | 775 | 730 | 932 | |
| Auxetic | 796 | 1106 | 777 | 774 | 807 |
| 826 | 1145 | 772 | 674 | 935 | |
| 793 | 1121 | 756 | 729 | 631 | |
| 784 | 1098 | 757 | 709 | 856 | |
| 790 | 1127 | 572 | 738 | 779 | |
| 783 | 1116 | 784 | 714 | 832 | |
Table A5 presents the vertical ground reaction forces (GRFs) measured in Newtons (N) for Subjects B, C, D, E, and F (without braces). Data is grouped into three conditions: barefoot walking, walking with standard insoles ("No auxetic"), and walking with experimental auxetic foam insoles ("Auxetic"). Subject A is excluded from this table to isolate specific neuropathic categories, with Subject C serving as the representative for diabetic neuropathy in this analysis.
Table A6.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects A, B, D, E, and F (braced condition).
Table A6.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects A, B, D, E, and F (braced condition).
| PARAMETER / C OMPARISON | RESULT | |
| KRUSKAL-WALLIS | Observed Value | 192.254 |
| Critical Value | 5.991 | |
| p | <0.0001 | |
| Degrees of Freedom | 2 | |
| alpha | 0.05 | |
| K | ||
| p<0.0001 | ||
| PAIRWISE COMPARISONS | Insole vs. Neuropathy | Significant* |
| p | 0.002 | |
| p=0.002 | ||
| Insole vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 | ||
| Neuropathy vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 |
Table A6 Results were significant (p < .0001) at the α =0.05 level. Data from Subject C (diabetic neuropathy) were excluded to maintain a balanced assessment of various neuropathic etiologies, as diabetic neuropathy was already represented by Subject A.
Table A7.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects A, B, D, E, and F (without braces).
Table A7.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects A, B, D, E, and F (without braces).
| PARAMETER / COMPARISON | RESULT | |
| KRUSKAL-WALLIS | Observed Value | 192.254 |
| Critical Value | 5.991 | |
| p | <0.0001 | |
| Degrees of Freedom | 2 | |
| alpha | 0.05 | |
| K | ||
| p<0.0001 | ||
| PAIRWISE COMPARISONS | Insole vs. Neuropathy | Significant* |
| p | 0.002 | |
| p=0.002 | ||
| Insole vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 | ||
| Neuropathy vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 |
Table A7 Results were significant (p < .0001) at the α = 0.05 level. Data from Subject C (diabetic neuropathy) were excluded to maintain a balanced assessment of various neuropathic etiologies, as diabetic neuropathy was already represented by Subject A.
Table A8.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects B,C, D, E, and F (braced condition).
Table A8.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects B,C, D, E, and F (braced condition).
| PARAMETER / COMPARISON | RESULT | |
| KRUSKAL-WALLIS | Observed Value | 192.254 |
| Critical Value | 5.991 | |
| p | <0.0001 | |
| Degrees of Freedom | 2 | |
| alpha | 0.05 | |
| K | ||
| p<0.0001 | ||
| PAIRWISE COMPARISONS | Insole vs. Neuropathy | Significant* |
| p | 0.002 | |
| p=0.002 | ||
| Insole vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 | ||
| Neuropathy vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 |
Table A8 Results were significant (p < .0001) at the α =0.05 level. Data from Subject A (diabetic neuropathy) were excluded to maintain a balanced assessment of various neuropathic etiologies, as diabetic neuropathy was already represented by Subject C.
Table A9.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects B,C, D, E, and F (without braces).
Table A9.
Kruskal-Wallis and Dunn’s post-hoc test results for Subjects B,C, D, E, and F (without braces).
| PARAMETER / COMPARISON | RESULT | |
| KRUSKAL-WALLIS | Observed Value | 192.254 |
| Critical Value | 5.991 | |
| p | <0.0001 | |
| Degrees of Freedom | 2 | |
| alpha | 0.05 | |
| K | ||
| p<0.0001 | ||
| PAIRWISE COMPARISONS | Insole vs. Neuropathy | Significant* |
| p | 0.002 | |
| p=0.002 | ||
| Insole vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 | ||
| Neuropathy vs. GRFS | Significant* | |
| p | <0.0001 | |
| p<0.0001 |
Table A9 Results were significant (p < .0001) at the α =0.05 level. Data from Subject A (diabetic neuropathy) were ex cluded to maintain a balanced assessment of various neuropathic etiologies, as diabetic neuropathy was already repre sented by Subject C.
References
- Mayo Clinic. Peripheral neuropathy. Mayo Clinic. Published September 2, 2023. updated date not given. Available online: https://www.mayoclinic.org/diseases-conditions/peripheral-neuropathy/symptoms-causes/syc-20352061 (accessed on 7 July 2025).
- Latov, N. Peripheral Neuropathy; Demos Medical Publishing, 2006. [Google Scholar]
- Wiesman, JF. Peripheral Neuropathy: What It Is and What You Can Do to Feel Better; Johns Hopkins University Press, 2016. [Google Scholar]
- McGovern Medical School. Peripheral Neuropathy.UTHealth Neurosciences. Published 2008. updated date not given. Available online: https://med.uth.edu/neurosciences/conditions-and-treatments/nerve-disorders/peripheral-neuropathy/ (accessed on 5 June 2025).
- Martínez-Pascual, D.; Catalán, J.M.; Blanco-Ivorra, A.; Sanchís, M.; Arán-Ais, F.; García-Aracil, N. Estimating vertical ground reaction forces during gait from lower limb kinematics and vertical acceleration using wearable inertial sensors. In Front Bioeng Biotechnol.; Biomechanics, 2023. [Google Scholar] [CrossRef]
- Jiang, X.; Napier, C.; Hannigan, B.; Eng, J.J.; Menon, C. Estimating vertical ground reaction force during walking using a single inertial sensor. Sensors 2020, 20, 4345. [Google Scholar] [CrossRef]
- Daryabor, A.; Saeedi, H.; Ghasemi, M.S.; et al. Influence of heel design in an orthopedic shoe on ground reaction forces during walking. Prosthet Orthot Int. 2016, 40, 598–605. [Google Scholar] [CrossRef]
- Fong, D.T.P.; Chan, Y.Y.; Hong, Y.; Yung, P.S.H.; Fung, K.Y.; Chan, K.M. Estimating the complete ground reaction forces with pressure insoles in walking. J Biomech. 2008, 41, 2597–2601. [Google Scholar] [CrossRef]
- Kharb, A.; Saini, V.; Jain, Y.K.; Dhiman, S. (PDF) A review of gait cycle and its parameters. ResearchGate. January 2011. updated date not given. Available online: https://www.researchgate.net/publication/268423123_A_review_of_gait_cycle_and_its_parameters (accessed on 17 September 2025).
- Derlatka, M.; Parfieniuk, M. Real-world measurements of ground reaction forces of normal gait of young adults wearing various footwear. Sci. Data 2023, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- Hulshof, C.M.; van der Leeden, M.; van Netten, J.J.; et al. The association between peripheral neuropathy and daily-life gait quality characteristics in people with diabetes. Gait Posture 2024, 114, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.; Thorstensson, A. Ground reaction forces at different speeds of human walking and running. Acta Physiol. Scand. 1989, 136, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Ruano, C.; Powell, D.; Chalambaga, E.; Renshaw, D. The effects of tempur insoles on ground reaction forces and loading rates in running. Int. J.Exerc.Sci. 2009, 2, 186–190. [Google Scholar] [CrossRef]
- Medicine, Stanford. Gait Abnormalities. Stanford Medicine 25. Available online: https://stanfordmedicine25.stanford.edu/the25/gait.html (accessed on 17 May 2025).
- Lim, A.; Narale, K. Center of Pressure (COP). Physiopedia. Published 2024.Updated April 29 2024. Available online: https://www.physio-pedia.com/Center_of_Pressure_(COP) (accessed on 29 July 2024).
- Melai, T.; IJzerman, T.H.; Schaper, N.C.; et al. Calculation of plantar pressure time integral, an alternative approach. Gait Posture 2011, 34, 379–383. [Google Scholar] [CrossRef]
- MED-EL Medical Electronics. Muscular imbalance. Available online: https://stiwell.medel.com/orthopaedics/muscular-imbalance (accessed on 24 July 2025).
- Newport Center Family Chiropractic. The Impact of Foot Health on Spinal Alignment. Available online: https://drdigrado.com/the-impact-of-foot-health-on-spinal-alignment-a-chiropractic-perspective/ (accessed on 25 July 2025).
- Bodman, M.A.; Dreyer, M.A.; Varacallo, M.A. Diabetic Peripheral Neuropathy. In StatPearls; StatPearls Publishing, 2024. [Google Scholar]
- Vinik, A.I. Management of neuropathy and foot problems in diabetic patients. Clin.Cornerstone. 2003, 5, 38–55. [Google Scholar] [CrossRef]
- Paton, J.; Bruce, G.; Jones, R.; Stenhouse, E. Effectiveness of insoles used for the prevention of ulceration in the neuropathic diabetic foot: a systematic review. J.Diabetes Complications. 2011, 25, 52–62. [Google Scholar] [CrossRef]
- Kwon, O.Y.; Mueller, M.J. Walking patterns used to reduce forefoot plantar pressures in people with diabetic neuropathies. Phys.Ther. 2001, 81, 828–835. [Google Scholar] [CrossRef]
- Mueller, M.J.; Minor, S.D.; Sahrmann, S.A.; Schaaf, J.A.; Strube, M.J. Differences in the gait characteristics of patients with diabetes and peripheral neuropathy compared with age-matched controls. Phys.Ther 1994, 74, 299–308. [Google Scholar] [CrossRef]
- Mustapa, A.; Justine, M.; Mustafah, N.M.; Manaf, H. The effect of diabetic peripheral neuropathy on ground reaction forces during straight walking in stroke survivors. Rehabil Res and Pract. 2017, 2017, 1–9. [Google Scholar] [CrossRef]
- Kennedy, S. Pathology-Specific Orthotic and Pedorthic Recommendations – Part 1. Hersco Edu Center. 28 May 2022. updated date not given. Available online: https://hersco.com/education-center/pathology-specific-orthotics-1/ (accessed on 12 June 2025).
- Castelli, G.; Desai, K.M.; Cantone, R.E. Peripheral Neuropathy: Evaluation and Differential Diagnosis. Am Fam Physician 2020, 102, 732–739. [Google Scholar]
- Brodsky, J.W.; Pollo, F.E.; Cheleuitte, D.; Baum, B.S. Physical properties, durability, and energy-dissipation function of dual-density orthotic materials used in insoles for diabetic patients. Foot Ankle Int. 2007, 28, 880–889. [Google Scholar] [CrossRef]
- Dynamics, Foot. How Orthotics Help Control Neuropathy. Foot Dynamics. 7 January 2025. updated date not given. Available online: www.footdynamics.com/neuropathy-foot-pain-and-the-role-of-orthotics (accessed on 15 January 2026).
- Robinson, C.; Major, M.J.; Kuffel, C.; Hines, K.; Cole, P. Orthotic management of the neuropathic foot: An interdisciplinary care perspective. Prosthetics and Orthotics International 2015, 39, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Habiba, R.; Amaro, A.; Trindade, D.; et al. Comparative analysis of impact strength among various polymeric materials for orthotic production. Polymers 2024, 16, 1843–1843. [Google Scholar] [CrossRef] [PubMed]
- Kirby, K.A.; Spooner, S.K.; Scherer, P.R.; Schuberth, J.M. Foot orthoses. Foot Ankle Spec. 2012, 5, 334–343. [Google Scholar] [CrossRef]
- Boakye, A.; Chang, Y.; Raji, R.K.; Pibo, M. A review on auxetic textile structures, their mechanism and properties. J Text Sci Fashion Technol. 2019, 2, 1–10. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, S.; Yang, Y.; Liu, Y.; Guo, Y.; Wang, H. Efficacy of auxetic lattice structured shoe sole in advancing footwear comfort—from the perspective of plantar pressure and contact area. Front. Public Health 2024, 12. sect Injury Prevention and Control. [Google Scholar] [CrossRef]
- Liu, Q. (PDF) Literature Review: Materials with Negative Poisson’s Ratios and Potential Applications to Aerospace and Defence. Australian Government Department of Defence: Defence Science and Technology Organisation. August 2006. updated date not given; Available online: https://apps.dtic.mil/sti/tr/pdf/ADA460791.pdf (accessed on 2025).
- Lakes, R. Foam structures with a negative poisson’s ratio. Sci. 1987, 235, 1038–1040. [Google Scholar] [CrossRef] [PubMed]
- Greaves, G.N.; Greer, A.L.; Lakes, R.S.; Rouxel, T. Poisson’s ratio and modern materials. Nat. Mater. 2011, 10, 823–837. [Google Scholar] [CrossRef] [PubMed]
- Waters, T. FSU Scientist invents new foam technology. Tallahassee Democrat. 28 August 2015. Available online: https://www.tallahassee.com/story/news/2015/08/28/fsu-scientist-invents-new-foam-technology/71282888/ (accessed on 25 July 2025).
- Zeng, C.; Li, Y. US10479004B2 - Material systems and methods of manufacture for auxetic foams - Google Patents. Google.com. 19 November 2019. updated date not given. Available online: https://patents.google.com/patent/US10479004B2/en (accessed on 17 June 2025).
- Li, Y.; Zeng, C. On the successful fabrication of auxetic polyurethane foams: materials requirement, processing strategy and conversion mechanism. Polymer 2016, 87, 98–107. [Google Scholar] [CrossRef]
Figure 1.
Auxetic foam expands in the transverse direction when stretched. The top panel shows the material in its original state, while the bottom panel illustrates the lateral expansion (widening) during applied tension, characteristic of a negative Poisson's ratio.
Figure 1.
Auxetic foam expands in the transverse direction when stretched. The top panel shows the material in its original state, while the bottom panel illustrates the lateral expansion (widening) during applied tension, characteristic of a negative Poisson's ratio.
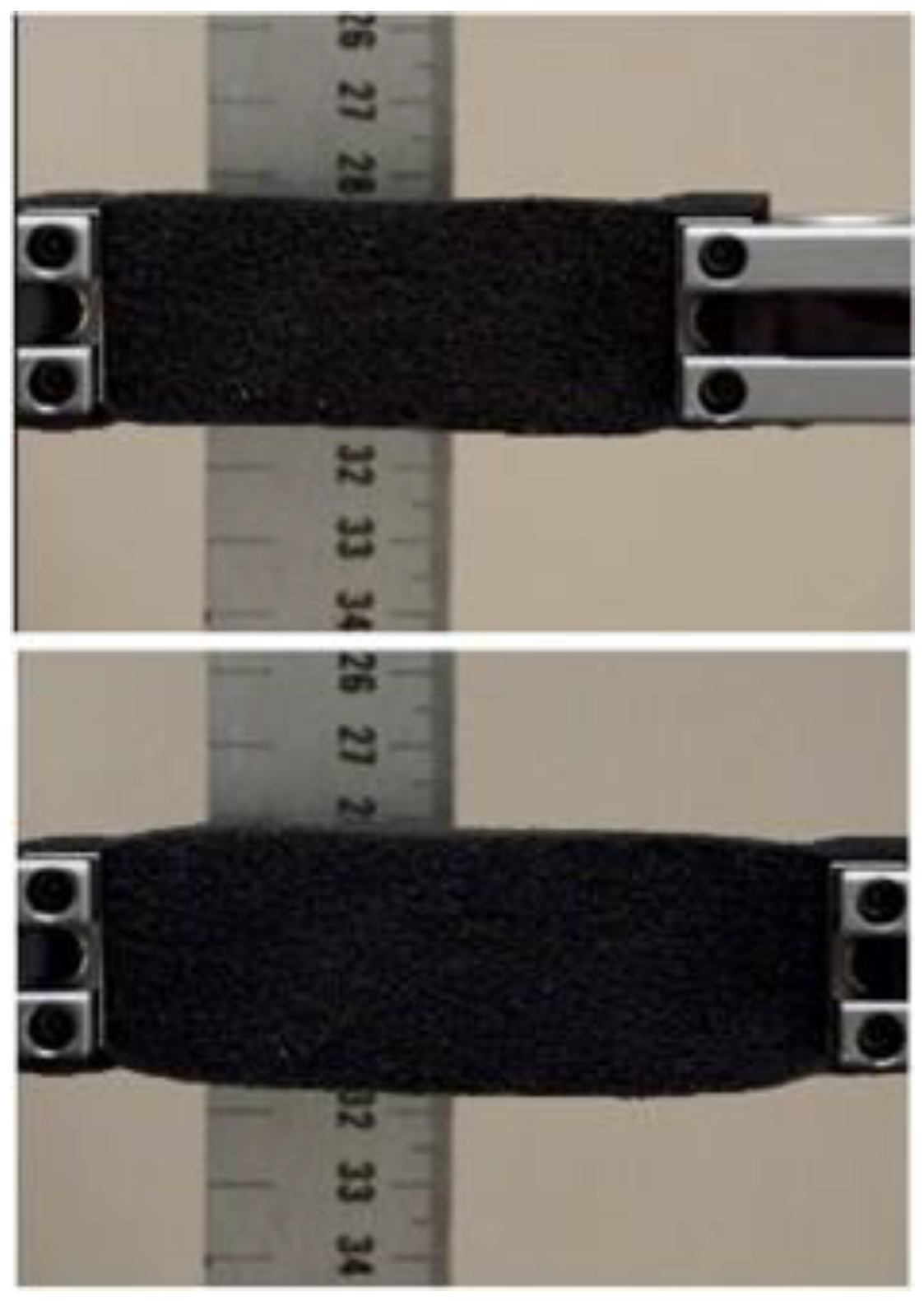
Figure 2.
left: CAD rendering of auxetic foam insole; right: a photograph of the auxetic foam insole.
Figure 2.
left: CAD rendering of auxetic foam insole; right: a photograph of the auxetic foam insole.

Figure 3.
a. Schematic of Neuropathic and Auxetic foam insole test set-up.
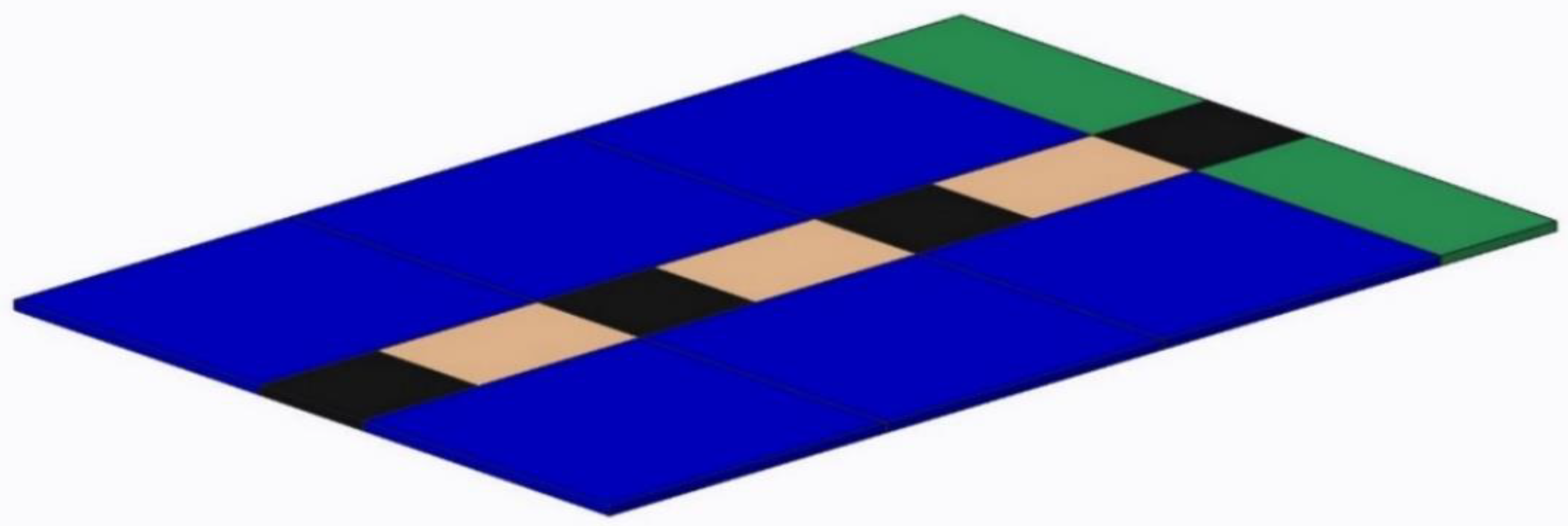
Figure 4.
Subject-specific mean vertical ground reaction forces (N) during ambulation under three insole conditions (Barefoot, OTC, and Auxetic). The data indicate that the use of the Auxetic foam material resulted in lower vertical GRFs across participants with diabetes (A), arthritis (D), and injury-related neuropathy(without braces)(F).
Figure 4.
Subject-specific mean vertical ground reaction forces (N) during ambulation under three insole conditions (Barefoot, OTC, and Auxetic). The data indicate that the use of the Auxetic foam material resulted in lower vertical GRFs across participants with diabetes (A), arthritis (D), and injury-related neuropathy(without braces)(F).
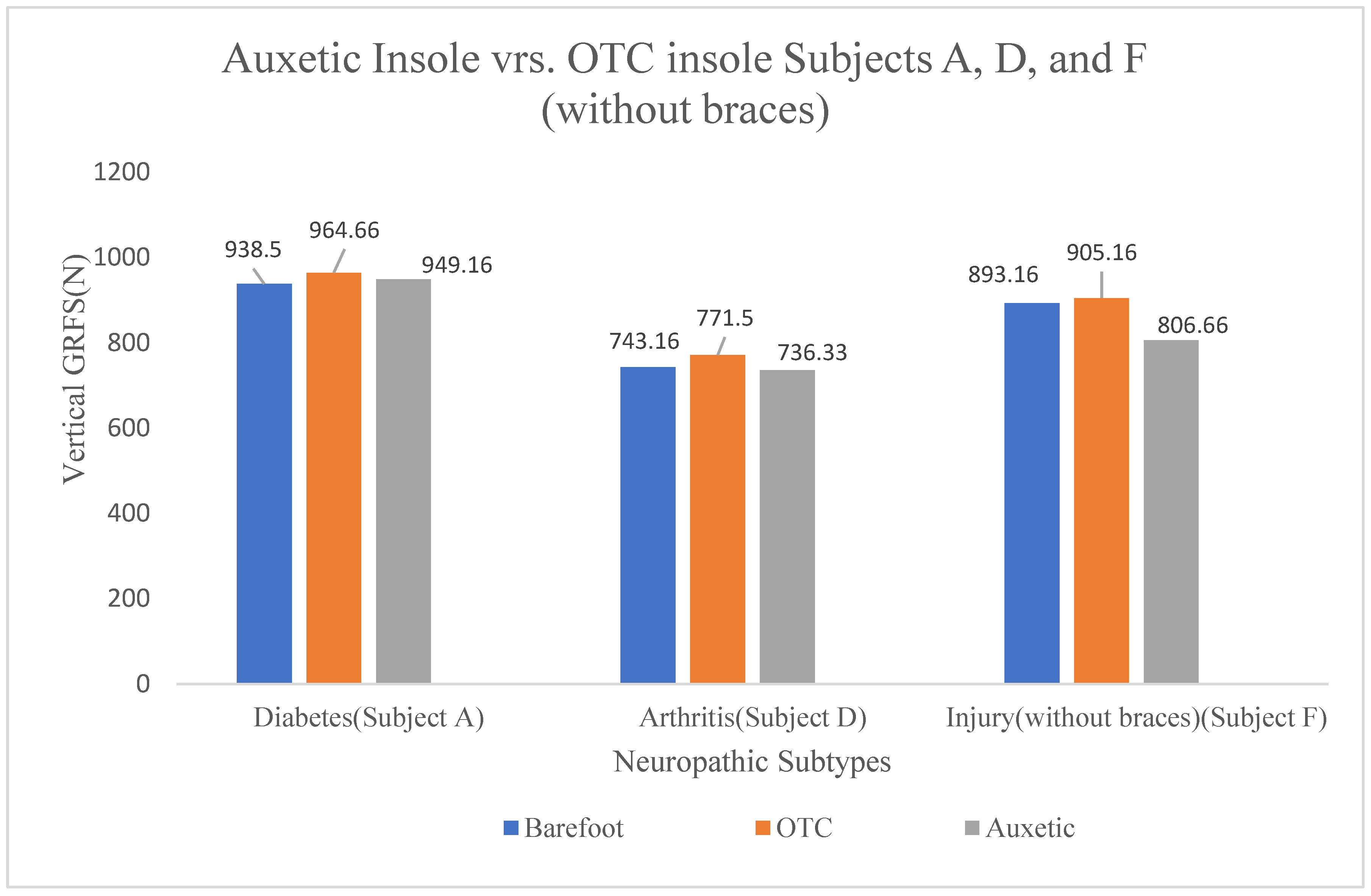
Figure 5.
Subject-specific mean vertical ground reaction forces (N) during ambulation under three insole conditions (Barefoot, OTC, and Auxetic). The data indicate a general increase in vertical GRFs with the use of the Auxetic material across participants with cancer( B), diabetes(C), a healthy control (E), and injury-related neuropathy(brace condition) (F), which may be attributed to external factors.
Figure 5.
Subject-specific mean vertical ground reaction forces (N) during ambulation under three insole conditions (Barefoot, OTC, and Auxetic). The data indicate a general increase in vertical GRFs with the use of the Auxetic material across participants with cancer( B), diabetes(C), a healthy control (E), and injury-related neuropathy(brace condition) (F), which may be attributed to external factors.
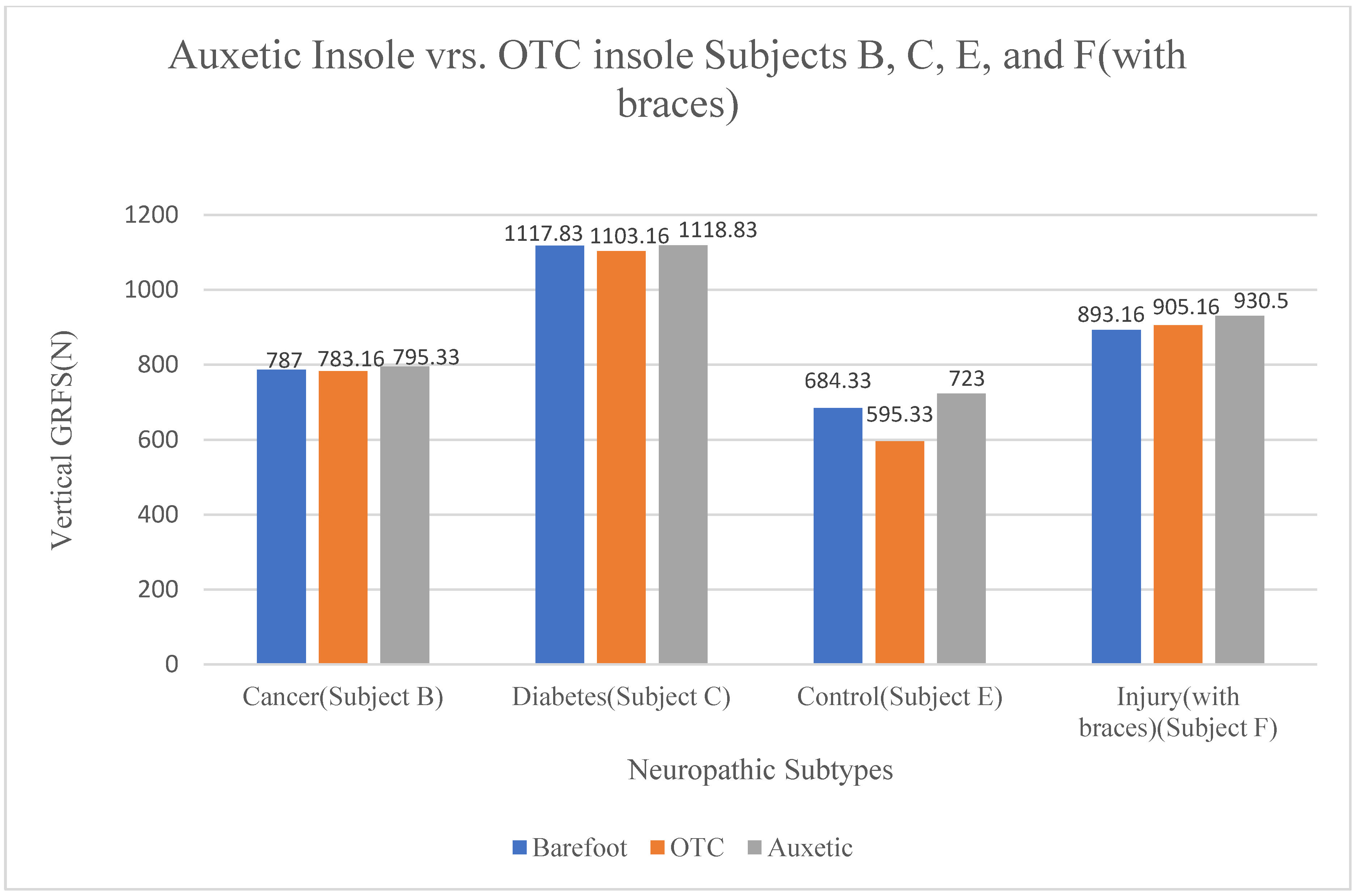
Figure 6.
Auxetic foam material improved gait cycle of Subject A with Diabetic Neuropathy.
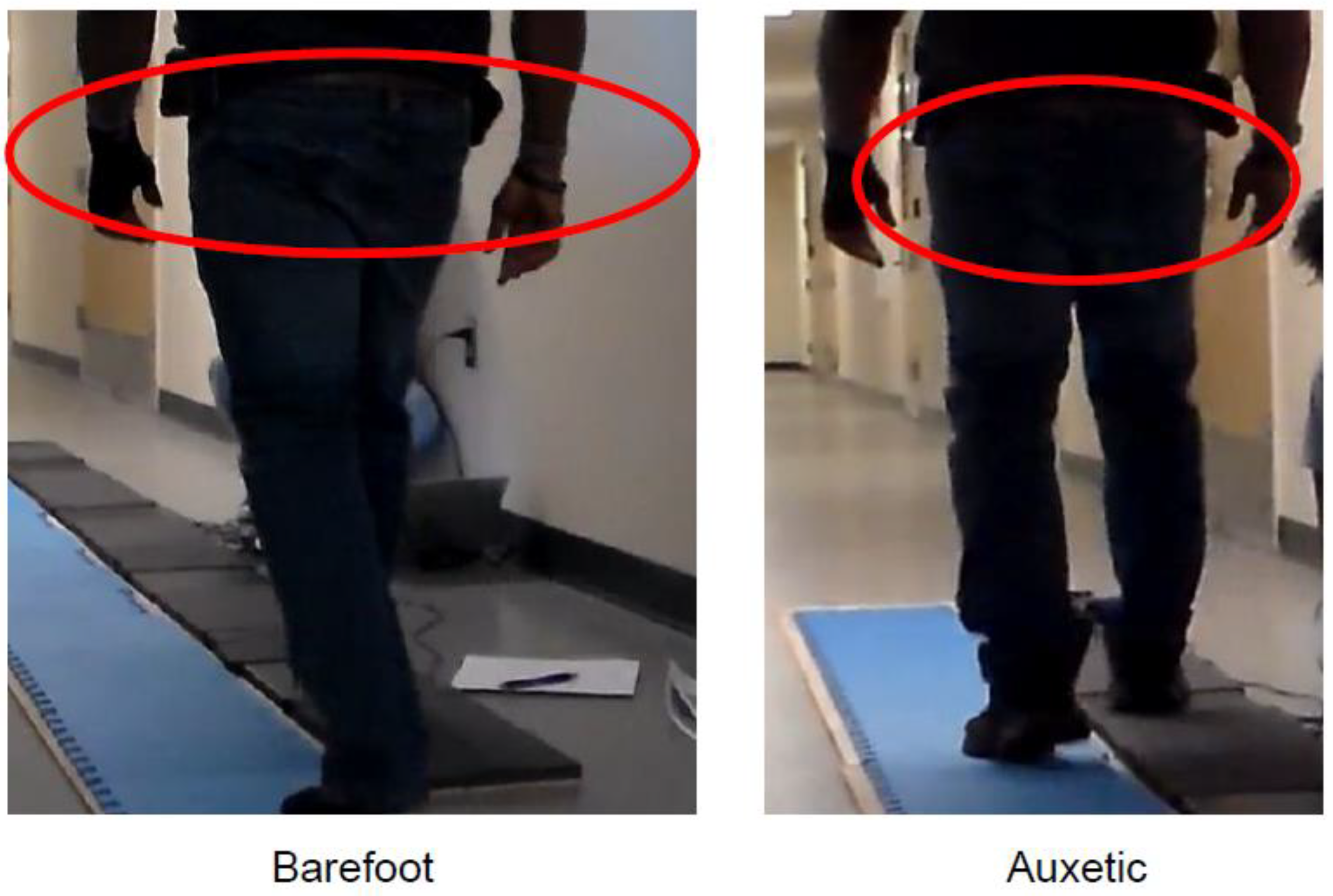
Figure 7.
Auxetic foam material improved gait cycle of Subject D with Neuropathic arthritis.
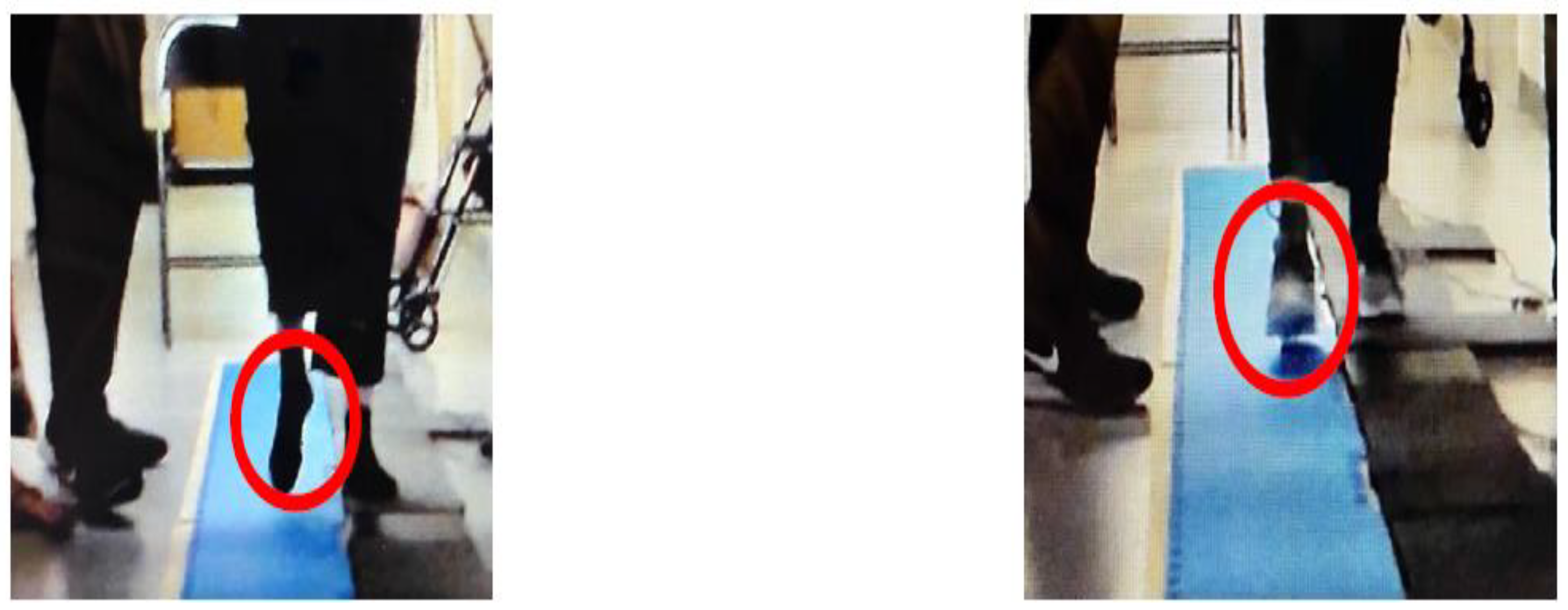
Table 1.
Qualitative Data Analysis of Comfort and Gait Improvement with Auxetic Foam Technology.
| Subject | Gender | Weight | Neuropathy Cause / Attribute | Shoe Size | Shoes & Aids Worn at Site (Current) | Shoe Type for Auxetic Insole | Insole Comfort Level (vs. Current) | Gait Improvement (vs. Current) |
| A | M | 205 lbs | Diabetes | 10W | Timberlands (Dr. Scholl’s) | Eduropro Comfort Gel (Black) | More comfortable | Walking is better |
| B | F | 175 lbs | Cancer | 9.5 | New Balances (Memory Foam) | Athletic Works (White) | More comfortable | Walking is better |
| C | M | 260 lbs | Diabetes | 11 | Slip-on wafers (Foam/Leather) | Athletic Works (Black) | About the same | About the same |
| D | F | 155 lbs | Arthritis / Cancer | 6.5 | Sketchers (No special insole) | Athletic Works (Gray) | About the same | About the same |
| E | F | 158 lbs | Control (No neuropathy) | 6.5W | Sketchers (No special insole) | Athletic Works (Gray) | More comfortable | About the same |
| F | F | 184 lbs | Personal Injury (Car accident) | 10 | Adidas (Dr. Scholl’s) + AFO Braces | Athletic Works (Gray) | More comfortable | Walking is better |
1 This table presents qualitative feedback from subjects using auxetic insoles. Data collected includes subjective comfort levels and perceived gait improvement compared to the subjects' current footwear and aids.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



