Submitted:
12 February 2026
Posted:
13 February 2026
You are already at the latest version
Abstract
The transition to active rehabilitation in concussion care requires precise tools to identify patients atrisk of persistent post-concussive symptoms (PPCS). While machine learning (ML) offers thepotential to personalize prognosis, current models relying on clinical history and subjective symptomreporting (e.g., SCAT5) have failed to demonstrate significant performance gains over the lastdecade. This perspective article argues that clinical prognostic models have reached a performanceceiling of approximately 0.85 Area Under the Curve (AUC). By reviewing key studies from 2016 to2025, we demonstrate that increasing algorithmic complexity—from logistic regression to deeplearning—yields diminishing returns when applied to subjective inputs. In contrast, modelsincorporating physiological data, such as neuroimaging or fluid biomarkers, consistently break thisceiling, achieving AUCs exceeding 0.95. We conclude that better mathematics cannot correct formissing biological signal, and that the advancement of precision medicine in neurotrauma requires afundamental shift toward multimodal, biological data integration.
Keywords:
concussion
; mTBI
; machine learning
; precision medicine
; traumatic brain injury
1. Introduction
The treatment of concussions has evolved significantly over the last couple of decades. The “rest is the best” approach has shifted towards active rehabilitation. Most patients functionally recover in about four weeks [1]. However, a smaller subset of patients experiences prolonged symptoms, taking months and years to recover [2]. While some risk factors of developing persistent post-concussive symptoms (PPCS) are understood, such as a history of migraines, pre-injury mental health history, and acute symptom severity, there are no widespread tools to prognosticate individual cases [3,4,5]. This limits the application of targeted interventions in the acute phase of injury, such as selective brain cooling or vestibular therapy, which have the potential to lead to quicker symptom resolution [6,7]. In the last ten years, advances in machine learning (ML) and artificial intelligence (AI) have guided attempts to leverage large datasets of concussion patient information to develop predictive models of PPCS. Current prognosis of individual concussion recovery relies on clinical data, including the SCAT5 symptom data, demographic data, and history of migraines [8,9]. However, while ML and AI can optimize these models’ predictive power, there is a performance ceiling when using clinical data. Clinical models hit a performance ceiling at ~0.85 area under the curve (AUC). To break this, we must shift from patient self-reported data to multimodal models that incorporate objective multimodal biomarkers.
2. Discussion
The Clinical Performance Ceiling
Current risk stratification for persistent post-concussion symptoms (PPCS) relies heavily on self-reported symptom checklists and subjective clinical assessments, which have reached a predictive performance ceiling of AUC ~0.85 (Figure 1) [10,11]. Studies using advanced machine learning on clinical variables consistently report area under the curve (AUC) values between 0.65 and 0.81 [11,12]. For instance, even when utilizing specialized tools like the Vestibular Ocular Motor Screening (VOMS) and cognitive performance measures, clinical models for pediatric athletes peak at an AUC of 0.81 [11]. In adolescent female cohorts, clinical-only models using Random Forest and Logistic Regression have achieved modest results with AUCs of 0.73 and 0.70, respectively [13]. Furthermore, large-scale studies on sports-related concussion recovery using psychological and symptomatic factors report an AUC of 0.80, reinforcing a persistent plateau despite the use of sophisticated algorithms like CatBoost [14].
This plateau is further evidenced by the fact that emergency physicians’ diagnostic accuracy for predicting 3-month recovery based on clinical presentation is frequently no better than chance [15]. Traditional clinical prediction tools face logistical difficulties in clinical settings and are less than 70% accurate [16]. A primary driver of this ceiling is the inherent subjectivity of self-report measures, which are prone to the "good-old-days" bias, where patients tend to underestimate their pre-injury problems after a traumatic event [17]. Additionally, common symptoms such as headache, fatigue, and dizziness are not specific to concussion and are frequently reported across healthy and injured populations alike [12,17]. Because subjective symptom reports can be manipulated by individuals seeking to expedite or delay return to activity, relying solely on these metrics creates significant uncertainty in clinical decision-making [16]. Consequently, the diverse behavioral symptomology resulting from unique mechanisms of injury makes it notoriously difficult to predict recovery paths using observation alone [18]. While clinical-only models frequently encounter a performance plateau when forecasting physical return-to-play, they demonstrate a significantly higher predictive ceiling for mental health sequelae [19,20]. This indicates that the subjective data and longitudinal history typically found in Electronic Health Records (EHR) may be inherently better suited. The most effective and accurate non-advanced imaging models utilized either neurocognitive data, longitudinal symptom inventories, psychological inventories, or vestibular/oculomotor screening alongside standard clinical data, strengthening the case for incorporating diverse data types for capturing psychological trajectories rather than for diagnosing acute physiological recovery.[11,20,21,22].for
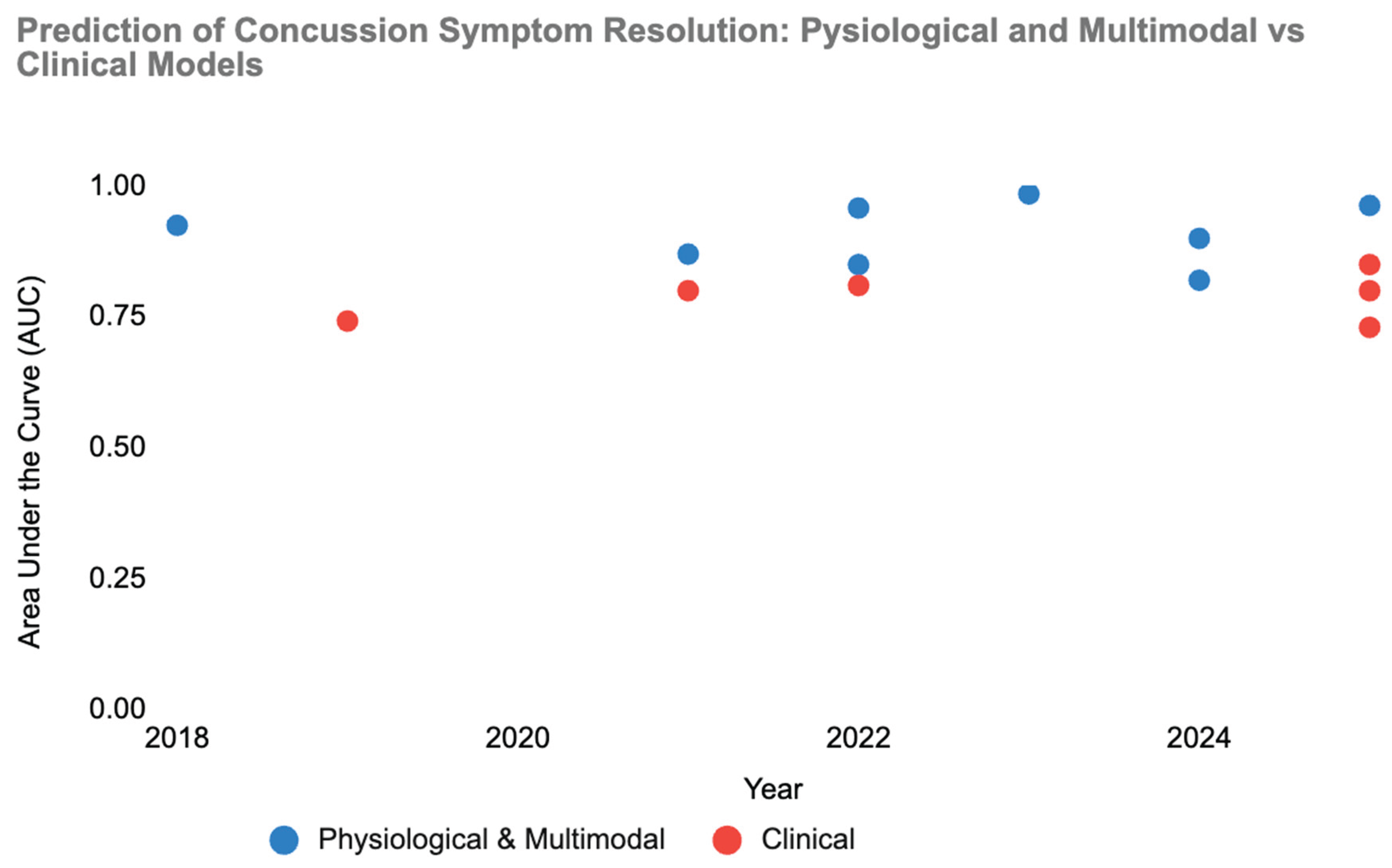
A comparison of prognostic accuracy, as measured by the Area Under the Curve (AUC), for models predicting symptom resolution or functional recovery. Clinical models (Red) utilizing symptoms and demographics have plateaued between 0.74–0.81 AUC over the last six years, despite the application of advanced machine learning. In contrast, Multimodal models (Blue) integrating objective neuroimaging (MEG, MRI) or physiological biomarkers consistently exceed the 0.90 threshold, with recent fusion models achieving near-perfect classification (>0.95). The gap illustrates that predictive precision is currently limited by data source rather than algorithmic complexity.
The Multimodal Breakthrough
While clinical and self-report models appear bound by an upper predictive limit, the integration of objective physiological biomarkers has demonstrated the capacity to shatter this performance ceiling, consistently achieving AUC values exceeding 0.90 (Figure 1) [23,24,25]. By shifting the predictive focus from phenomenological observations to the underlying biological state of the brain, researchers have unlocked a higher tier of diagnostic and prognostic precision that is necessary for individualized care.
The most significant leap in predictive accuracy has been achieved through resting-state magnetoencephalography (rs-MEG). Unlike clinical assessments that rely on a patient’s ability to perceive and report dysfunction, rs-MEG directly measures spontaneous neuronal activity with high spatial and temporal resolution [23]. Huang et al. (2023) developed a machine learning algorithm that integrated rs-MEG source imaging markers across both delta (1–4 Hz) and gamma (30–80 Hz) frequency bands. This combined model predicted pediatric mTBI cases against orthopedic controls with a sensitivity of 95.5% and a specificity of 90.2%, achieving a peak AUC of 0.985 [23]. This represents the highest reported performance in the literature and underscores that regional hyperactivity—particularly in the frontal lobe poles—serves as a definitive neural injury signature that clinical checklists cannot capture [23].
Objective measurements of the brain’s structural framework have also proven superior to clinical data modeling. Utilizing diffusion-weighted MRI (dMRI) and tractography, researchers can identify microstructural disruptions in white matter that correlate with recovery time [10,25]. Bertò et al. (2024) leveraged the mean Fractional Anisotropy (FA) of 16 statistically significant white matter tracts to develop a prognostic model for collegiate athletes. Their Logistic Regression binary classifier achieved an AUC of 0.90 and, notably, a sensitivity of 1.0, meaning the model identified every athlete at risk for persistent symptoms without a single false negative [10]. Similarly, Yates et al. (2025) demonstrated that integrating injury history with automated MRI reports identifying white matter hyperintensities yielded a composite model accuracy of 94.6% and an AUC of 0.963 [25]. These findings suggest that the physical state of white matter tracts, such as the inferior fronto-occipital fasciculus, provides a more reliable prognostic signal than symptom-based resolution [10,25].
The breakthrough into high-precision forecasting also extends to the prediction of specific cognitive sequelae. While traditional neuropsychological evaluations often fail to predict long-term changes, functional MRI (fMRI) biomarkers measured during the acute phase have shown high sensitivity to future working memory (WM) deficits [26]. Chen et al. (2022) utilized machine learning to analyze WM task-induced activation and deactivation maps at baseline. Their model achieved an AUC of 0.958 in identifying patients whose working memory ability at one year post-injury would be worse than their pre-injury baseline [26]. This suggests that early functional connectivity patterns—specifically the imbalance in communication between task-positive and task-negative regions—can forecast a chronic course that clinical inventories might miss during transient periods of symptomatic recovery [26,27].
The breakthrough in performance is best exemplified by models that synthesize multiple physiological modes into a single index. Jacquin et al. (2018) developed an enhanced multimodal Brain Function Index (eBFI) that combined quantitative EEG (QEEG), neurocognitive throughput, and clinical vestibular measures [24]. This integrated approach achieved an AUC of 0.925, successfully separating controls from concussed subjects with prolonged recovery [24]. Even in cases where individual biological markers do not break the 0.90 threshold, such as salivary ncRNA, they still provide significant additive utility. Fedorchak et al. (2021) showed that adding a panel of 16 salivary RNAs to a validated clinical risk score boosted the predictive accuracy from a modest 0.73 to a robust 0.86 AUC [16].
While multimodal machine learning models typically demonstrate superior prognostic performance by integrating objective physiological data, the findings of Hellstrøm et al. (2017) serve as a critical methodological baseline illustrating that the specific type of imaging data used determines whether a model can exceed the established clinical performance ceiling [10,23]. In their study, a clinical-only model (r=0.55) actually outperformed a combined clinical and imaging model (r=0.45) because macrostructural MRI cortical morphometry and subcortical volumes performed at a chance level (r=0.03), offering no added predictive value over demographic and clinical features [28]. This result highlights that traditional structural imaging is often insensitive to the subtle pathophysiological changes of mild traumatic brain injury, which contributes to clinical models plateauing at AUC values between 0.65 and 0.81 [11,12]. To move beyond this plateau, the sources suggest shifting toward microstructural or functional imaging modalities; for instance, models utilizing diffusion-weighted MRI to analyze white matter tracts or resting-state magnetoencephalography (rs-MEG) have consistently surpassed clinical-only metrics, achieving peak AUCs ranging from 0.90 to 0.985 [10,23]. Ultimately, the Hellstrøm results highlight that while multimodal integration is vital for precision medicine, true predictive superiority is only realized when the selected biomarkers move beyond phenomenological observation to capture the specific biological or electrical signatures of the injury [18,23,28].
The Diminishing Returns of Algorithmic Complexity
The evolution of machine learning (ML) architectures in concussion research marks a shift from traditional linear statistics toward non-linear systems capable of managing the inherent complexity and heterogeneity of brain injuries [12]. These diverse architectures—ranging from supervised classifiers to sequential deep learning and unsupervised pattern discovery—have fundamentally changed how researchers identify risk factors and predict recovery trajectories [29,30]. Supervised algorithms, particularly Support Vector Machines (SVM) and Random Forest (RF), have become the primary tools for clinical risk stratification, and are among the first algorithms used for the classification of concussion [31]. SVMs have proven exceptionally powerful when applied to high-dimensional physiological data; for example, an SVM model utilizing Recursive Feature Elimination on rs-MEG source magnitude imaging achieved a near-perfect 0.985 AUC in distinguishing pediatric mTBI from controls [23]. Similarly, SVM architectures have successfully predicted working memory decline at one year with over 83% accuracy by processing task-based fMRI activation maps [26]. Random Forest models provide additional impact through their ability to rank variable importance without overfitting [13]. This architecture allowed researchers to identify that emotional symptom clusters and injury history are most predictive of significant time out of sport, achieving a composite model accuracy of 94.6% [25].
A significant limitation of early models was their "static" nature, providing a single forecast at the time of injury. To address the time-varying nature of recovery, researchers have implemented Sequential Learning architectures like CatBoost and Bidirectional Long Short-Term Memory (BiLSTM) networks. CatBoost has been instrumental in processing multi-dimensional categorical data from vestibular and ocular-motor screenings, producing more parsimonious models that outperform traditional human-driven regression [26]. Furthermore, the application of BiLSTM networks to Electronic Medical Record (EMR) data has enabled real-time, visit-by-visit risk assessments [22]. By embedding temporal information, these models can adjust a patient’s mental health prognosis as new clinical symptoms or subsequent injuries emerge during the 12 months following a concussion [22,32].
While supervised models predict known outcomes, unsupervised learning architectures have been used to discover hidden recovery patterns that clinical definitions may miss. Using Locality-Sensitive Hashing (LSH) and autoencoders, researchers identified 11 distinct blood biomarker trajectories, revealing that specific rising patterns of GFAP and NF-L are associated with higher risks of loss of consciousness [29]. Similarly, tensor decomposition has been used to subgroup patients into four unique headache evolution trajectories, allowing for the early identification of individuals whose symptoms will remain severe without intervention (Mao et al., 2025). The impact of these discovery-based models is a shift toward precision medicine, where treatments are tailored to a patient’s specific biological subtype rather than a broad mTBI diagnosis [29,30].
Novel architectures such as Genetic Fuzzy Trees (GFT) and Genetic Algorithms (GA) offer a unique impact by modeling biological decisions using "if-then" linguistic rules [18]. GFT systems are particularly robust against the uncertainty and small sample sizes common in neuroimaging data, outperforming six other ML methods in predicting symptomatic recovery based on DTI white matter measures [18]. In parallel, Genetic Algorithms have been used to synthesize disparate data types—including QEEG, neurocognitive throughput, and vestibular signs—into a single multimodal Brain Function Index [24]. These specialized systems demonstrate that while architecture is vital for handling data complexity, the most significant performance leaps occur when the algorithm is designed to integrate objective, multimodal physiological inputs [18,24].
Toward Scalable Precision Medicine
The current evidence suggests that concussion management is gradually transitioning from a reliance on subjective clinical assessment toward a precision medicine framework [15,29]. This shift appears to be necessitated by the inherent heterogeneity of mild traumatic brain injury, which varies significantly in its causation and recovery trajectory [29]. While traditional clinical checklists remain the mainstay of practice, they may be reaching a predictive performance plateau that limits the ability of clinicians to accurately identify individuals at high risk for persistent disability [10,11].
The integration of objective, multimodal physiological data provides a potential pathway to exceed this clinical ceiling. Advanced neuroimaging modalities have demonstrated the capacity to identify neural injury signatures that are often invisible to standard clinical screening [10,23]. Furthermore, the identification of biological endophenotypes through unsupervised learning may enable more targeted and individualized interventions, potentially reducing the risk of persistent symptoms [13,29,30]. Ultimately, the shift toward a data-driven precision medicine approach may significantly enhance the accuracy of concussion forecasting compared to unassisted clinical judgment and raise the clinical relevance of advanced imaging techniques following concussive injury [22,32].

Table 1.
Summary of Machine Learning Models for Concussion Prognosis Categorized by Data Modality.
| Author (Year) | Modality Category | Input Data | Algorithm | Outcome | Performance (AUC/Acc) |
| Clinical & Symptom-Based Models | |||||
| Shafiei et al. (2017) | Clinical | 14 variables (Trauma history, substance use) | Neural Network (ANN) | Psychological Symptoms (6 mo) | AUC: 0.87 |
| Nademi et al. (2019) | Clinical | Demographics, History | Nonparametric Models | Psychological Symptoms | AUC: 0.86 |
| Bergeron et al. (2019) | Clinical | SCAT5 Symptom Scores | Machine Learning (Various) | Symptom Resolution | AUC: 0.74 |
| Chu et al. (2022) | Clinical | VOMS, King-Devick, Risk factors | CatBoost | Recovery Time | AUC: 0.78 - 0.84 |
| Dabek et al. (2022) | Clinical | EHR data, Demographics, Military Rank | Neural Networks, SVM | Mental Health Conditions | AUC: 0.82 |
| Mao et al. (2025) | Clinical | Daily Headache Diary (Longitudinal) | Partial Least Squares and Logistic Regression | Headache Trajectories | Accuracy: 0.80- 0.84 |
| Peng et al. (2025) | Clinical | EHR data, SDoH, Pre-existing diagnoses | BiLSTM (Deep Learning) | Mental Health Diagnosis | AUC: 0.89 |
| Bunt et al. (2025) | Clinical | SCAT5, Demographics | Logistic Regression and Random Forest | Persisting symptoms | AUC: 0.70- 0.73 |
| Hellstrøm et al. (2017) | Clinical | MRI Morphometry, Injury Data | Support Vector Regression | 12-Month Outcome (GOSE) | r = 0.55 |
| Thomas and Arnett (2025) | Clinical | Demographics, injury characteristics (LOC/Amnesia), SCAT-3 symptom clusters, BSI-18 psychosocial scores, and ImPACT neurocognitive composites | Random Forest Classification | Prolonged Recovery (>28 days to return-to-play) | AUC: 0.85; Acc: 89.04% |
| Physiological & Multimodal Models | |||||
| Le Sage et al. (2022) | Clinical (with CT) | Age, Sex, History, RPQ Scores | Logistic Regression | PPCS at 90 Days | AUC: 0.85 |
| Hellstrøm et al. (2017) | Multimodal | MRI Morphometry, Injury Data | Support Vector Regression | 12-Month Outcome (GOSE) | r = 0.45 |
| Jacquin et al. (2018) | Multimodal | QEEG, Vestibular, Neurocognitive | Genetic Algorithm (GA) | Prolonged Recovery (>14 days) | AUC: 0.93 |
| Fleck et al. (2021) | Multimodal | DTI measures, Volumetric MRI | Genetic Fuzzy Trees | Symptom Recovery (1 week) | Accuracy: 0.62 |
| Fedorchak et al. (2021) | Biomarker | Salivary RNA, Balance, Cognition | Machine Learning | Symptom Duration (>21 days) | AUC: 0.86 |
| Chen et al. (2022) | Multimodal | fMRI (N-back), Neuropsych evaluation | SVM | Working Memory Decline | AUC: 0.96 |
| Huang et al. (2023) | Imaging | rs-MEG Source Magnitude Imaging | Machine Learning | Symptom Recovery | AUC: 0.99 |
| Bertò et al. (2024) | Imaging | DTI (White Matter Tracts) | Logistic Regression | Persisting Symptoms | AUC: 0.90 |
| Cade & Turnbull (2024) | Physiological | Computerized Eye Tracking | XGBoost (xgbDART) | mTBI Classification | AUC: 0.82 |
| Yates et al. (2025) | Multimodal | MRI Reports, SCAT5, Demographics | Random Forest | Games Missed (>5) | AUC: 0.96 |
Note. AUC = Area Under the Curve; Acc = Accuracy; ANN = Artificial Neural Network; SVM = Support Vector Machine; BiLSTM = Bidirectional Long Short-Term Memory; DTI = Diffusion Tensor Imaging; fMRI = Functional Magnetic Resonance Imaging; MEG = Magnetoencephalography; QEEG = Quantitative Electroencephalography; SDoH = Social Determinants of Health; PPCS = Persistent Post-Concussion Symptoms.
Author Contributions
Zach Napora: Conceptualization, Methodology, Software, Formal Analysis, Investigation, Data Curation, Writing – Original Draft, Visualization, Project Administration. Owen Griffith: Supervision, Conceptualization, Writing – Review & Editing. Semyon Sloubonov: Supervision, Conceptualization, Writing – Review & Editing.
Funding
The authors did not receive any funding for this publication.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Patricios, J.S.; Schneider, K.J.; Dvorak, J.; Ahmed, O.H.; Blauwet, C.; Cantu, R.C.; Davis, G.A.; Echemendia, R.J.; Makdissi, M.; McNamee, M.; et al. Consensus statement on concussion in sport: the 6th international conference on concussion in sport-amsterdam, october 2022. Br J Sports Med 2023, 57, 695–711. [Google Scholar] [CrossRef] [PubMed]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; von Steinbuechel, N. A Multidimensional Approach to Post-concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Register-Mihalik, J.K.; Vander Vegt, C.B.; Cools, M.; Carnerio, K. Factors Associated with Sport-Related Post-concussion Headache and Opportunities for Treatment. Curr Pain Headache Rep 2018, 22, 75. [Google Scholar] [CrossRef] [PubMed]
- Theadom, A.; Parag, V.; Dowell, T.; McPherson, K.; Starkey, N.; Barker-Collo, S.; Jones, K.; Ameratunga, S.; Feigin, V.L. BIONIC Research Group Persistent problems 1 year after mild traumatic brain injury: a longitudinal population study in New Zealand. Br J Gen Pract 2016, 66, e16-23. [Google Scholar] [CrossRef]
- Iverson, G.L.; Gardner, A.J.; Terry, D.P.; Ponsford, J.L.; Sills, A.K.; Broshek, D.K.; Solomon, G.S. Predictors of clinical recovery from concussion: a systematic review. Br J Sports Med 2017, 51, 941–948. [Google Scholar] [CrossRef]
- Anderson, M.; McCorkle, M.; Hammonds, K.; Reynolds, E.; Gilliland, T.; Covert, K.; Driver, S. Early vestibular rehabilitation initiation is associated with faster recovery after sport related concussion. J. Sci. Med. Sport 2025, 28, 222–227. [Google Scholar] [CrossRef]
- Walter, A.E.; Bai, X.; Wilkes, J.; Neuberger, T.; Sebastianelli, W.; Slobounov, S.M. Selective head cooling in the acute phase of concussive injury: a neuroimaging study. Front Neurol 2023, 14, 1272374. [Google Scholar] [CrossRef]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med 2017, 51, 838–847. [Google Scholar] [CrossRef]
- Langer, L.K.; Alavinia, S.M.; Lawrence, D.W.; Munce, S.E.P.; Kam, A.; Tam, A.; Ruttan, L.; Comper, P.; Bayley, M.T. Prediction of risk of prolonged post-concussion symptoms: Derivation and validation of the TRICORDRR (Toronto Rehabilitation Institute Concussion Outcome Determination and Rehab Recommendations) score. PLOS Medicine 2021, 18, e1003652. [Google Scholar] [CrossRef]
- Bertò, G.; Rooks, L.T.; Broglio, S.P.; McAllister, T.A.; McCrea, M.A.; Pasquina, P.F.; Giza, C.; Brooks, A.; Mihalik, J.; Guskiewicz, K.; et al. Diffusion tensor analysis of white matter tracts is prognostic of persisting post-concussion symptoms in collegiate athletes. Neuroimage Clin 2024, 43, 103646. [Google Scholar] [CrossRef]
- Chu; Knell, G; Brayton, RP; Burkhart, SO; Jiang, X; Shams, S. Machine learning to predict sports-related concussion recovery using clinical data. Ann Phys Rehabil Med 2022, 65, 101626. [Google Scholar] [CrossRef]
- Bergeron; Landset, S; Maugans, TA; Williams, VB; Collins, CL; Wasserman, EB; Khoshgoftaar, TM. Machine learning in modeling high school sport concussion symptom resolve. Med Sci Sports Exerc 2019, 51, 1362–1371. [Google Scholar] [CrossRef]
- Bunt; Wilmoth, K; Taylor, E; Bullinger, L; Driskill, T; Shurtz, L; Magill, RT; Hynan, LS; Silver, CH; Didehbani, N; et al. Patterns of concussion recovery and persisting symptoms in adolescent females. J Head Trauma Rehabil 2025. [Google Scholar] [CrossRef]
- Taylor; Shurtz, L; Bunt, SC; Didehbani, N; Cullum, CM; Wilmoth, K. Using machine learning to predict concussion recovery time: the importance of psychological and symptomatic factors. Clin Neuropsychol 2025, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Le Sage, N.; Chauny, J.-M.; Berthelot, S.; Archambault, P.; Neveu, X.; Moore, L.; Boucher, V.; Frenette, J.; De Guise, É.; Ouellet, M.-C.; et al. Post-concussion symptoms rule: derivation and validation of a clinical decision rule for early prediction of persistent symptoms after a mild traumatic brain injury. J Neurotrauma 2022, 39, 1349–1362. [Google Scholar] [CrossRef]
- Fedorchak; Rangnekar, A; Onks, C; Loeffert, AC; Loeffert, J; Olympia, RP; DeVita, S; Leddy, J; Haider, MN; Roberts, A; et al. Saliva RNA biomarkers predict concussion duration and detect symptom recovery: a comparison with balance and cognitive testing. J Neurol 2021, 268, 4349–4361. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, M.; Balart-Sánchez, S.A.; Maurits, N.M.; van der Naalt, J. Self-Reported Complaints as Prognostic Markers for Outcome After Mild Traumatic Brain Injury in Elderly: A Machine Learning Approach. Front Neurol 2021, 12, 751539. [Google Scholar] [CrossRef] [PubMed]
- Fleck; Ernest, N; Asch, R; Adler, CM; Cohen, K; Yuan, W; Kunkel, B; Krikorian, R; Wade, SL; Babcock, L. Predicting post-concussion symptom recovery in adolescents using a novel artificial intelligence. J Neurotrauma 2021, 38, 830–836. [Google Scholar] [CrossRef]
- Nademi, A.; Shafiei, E.; Valizadeh, R. Forecasting psychological symptoms in mild traumatic brain injury: a nonparametric approach . Iranian Journal of Psychiatry and Behavioral Sciences 2018, e82799. [Google Scholar] [CrossRef]
- Shafiei, E.; Fakharian, E.; Omidi, A.; Akbari, H.; Delpisheh, A.; Nademi, A. Comparison of artificial neural network and logistic regression models for prediction of psychological symptom six months after mild traumatic brain injury . Iranian Journal of Psychiatry and Behavioral Sciences 2016, e5849. [Google Scholar] [CrossRef]
- Thomas; Arnett. Get your brain in the game: using machine learning to predict recovery timelines following sports-related concussion. Arch Clin Neuropsychol Off J Natl Acad Neuropsychol 2025, 40, 1533–1545. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Chen, J.; Yin, C.; Zhang, P.; Yang, J. Comparison of machine learning models in predicting mental health sequelae following concussion in youth. AMIA Jt Summits Transl Sci Proc 2025, 2025, 422–431. [Google Scholar] [PubMed]
- Huang; Angeles-Quinto, A; Robb-Swan, A; De-la-Garza, BG; Huang, CW; Cheng, CK; Hesselink, JR; Bigler, ED; Wilde, EA; Vaida, F; et al. Assessing pediatric mild traumatic brain injury and its recovery using resting-state magnetoencephalography source magnitude imaging and machine learning. J Neurotrauma 2023, 40, 1112–1129. [Google Scholar] [CrossRef] [PubMed]
- Jacquin, A.; Kanakia, S.; Oberly, D.; Prichep, L.S. A multimodal biomarker for concussion identification, prognosis and management. Comput. Biol. Med. 2018, 102, 95–103. [Google Scholar] [CrossRef]
- Yates; Yates, E; Li, X; Lu, Y; Yakoub, K; Davies, D; Belli, A; Sawlani, V. Developing a multivariate model for the prediction of concussion recovery in sportspeople: a machine learning approach. BMJ Open Sport Exerc Med 2025, 11, e002090. [Google Scholar] [CrossRef]
- Chen; Chen, YL; Kuo, DP; Li, YT; Chiang, YH; Chang, JJ; Tseng, SH; Chen, CY. Personalized prediction of postconcussive working memory decline: a feasibility study. J Pers Med 2022, 12. [Google Scholar] [CrossRef]
- Griffith, O.; Kelly, J.; Arnett, P.; Downs, D.; Hillary, F.; Slobounov, S.M. Network-Dependent Variability in Functional Connectivity after Mild Traumatic Brain Injury and Repetitive Head Impacts: A Systematic Review. Med. Res. Arch. 2025, 13. [Google Scholar] [CrossRef]
- Hellstrøm; Kaufmann, T; Andelic, N; Soberg, HL; Sigurdardottir, S; Helseth, E; Andreassen, OA; Westlye, LT. Predicting outcome 12 months after mild traumatic brain injury in patients admitted to a neurosurgery service. Front Neurol 2017, 8, 125. [Google Scholar] [CrossRef]
- Bui, L.A.; Yeboah, D.; Steinmeister, L.; Azizi, S.; Hier, D.B.; Wunsch, D.C.; Olbricht, G.R.; Obafemi-Ajayi, T. Heterogeneity in blood biomarker trajectories after mild TBI revealed by unsupervised learning. IEEE/ACM Trans. Comput. Biol. Bioinform. 2022, 19, 1365–1378. [Google Scholar] [CrossRef]
- Mao, L.; Li, J.; Schwedt, T.J.; Wu, T.; Ross, K.; Dumkrieger, G.; Smith, D.C.; Chong, C.D. Identifying and predicting headache trajectories among those with acute post-traumatic headache. Headache 2025, 65, 1124–1133. [Google Scholar] [CrossRef]
- Cao, C.; Tutwiler, R.L.; Slobounov, S. Automatic classification of athletes with residual functional deficits following concussion by means of EEG signal using support vector machine. IEEE Trans Neural Syst Rehabil Eng Publ IEEE Eng Med Biol Soc 2008, 16, 327–335. [Google Scholar] [CrossRef]
- Dabek, F.; Hoover, P.; Jorgensen-Wagers, K.; Wu, T.; Caban, J.J. Evaluation of machine learning techniques to predict the likelihood of mental health conditions following a first mTBI. Front. Neurol. 2022, 12. [Google Scholar] [CrossRef]
Figure 1.
The ‘Performance Ceiling’ in Concussion Prognosis (2018–2025). A comparison of prognostic accuracy, as measured by the Area Under the Curve (AUC), for models predicting symptom resolution or functional recovery. Clinical models (Red) utilizing symptoms and demographics have plateaued between 0.74–0.81 AUC over the last six years, despite the application of advanced machine learning. In contrast, Multimodal models (Blue) integrating objective neuroimaging (MEG, MRI) or physiological biomarkers consistently exceed the 0.90 threshold, with recent fusion models achieving near-perfect classification (>0.95). The gap illustrates that predictive precision is currently limited by data source rather than algorithmic complexity.
Figure 1.
The ‘Performance Ceiling’ in Concussion Prognosis (2018–2025). A comparison of prognostic accuracy, as measured by the Area Under the Curve (AUC), for models predicting symptom resolution or functional recovery. Clinical models (Red) utilizing symptoms and demographics have plateaued between 0.74–0.81 AUC over the last six years, despite the application of advanced machine learning. In contrast, Multimodal models (Blue) integrating objective neuroimaging (MEG, MRI) or physiological biomarkers consistently exceed the 0.90 threshold, with recent fusion models achieving near-perfect classification (>0.95). The gap illustrates that predictive precision is currently limited by data source rather than algorithmic complexity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



