Submitted:
12 February 2026
Posted:
13 February 2026
You are already at the latest version
Abstract
One of the most important early causes of death among polytraumatized patients is represented by coagulopathy as a result of alteration of the coagulation pathway with a result that varies from harmful haemorrhagic diathesis to thrombosis. The poly-traumatized patient is characterized by acute posttraumatic coagulopathy resulted by the alteration of tissue integrity and hypo perfusion of peripheral tissues. Consumptive thrombocytopenia together with platelet dysfunction, coagulation factor deficiency, and hyperfibrinolysis, with iatrogenic treatment (massive transfusion, hypothermia, and excess volume repletion solutions) are part of the pathogenesis of posttraumatic coagulopathy. Because of the substantial impact of alteration of the fluid-coagulant status on therapeutic management, it is natural that an early diagnosis will help to improve medical care procedures. This is possible with the help of ROTEM (rotational thromboelastometry) which indicates the type of coagulopathy early on. This method provides information about clot formation, formation kinetics, clot firmness, and about the reverse process fibrinolysis through physical analysis methods of its viscoelastic property. It provides in-depth information compared to the "usual" coagulogram, as the ROTEM method targets the coagulation process as an assembly of the blood in its entirety. Following the review of the currently available data on mortality and morbidity of patients whose treatment plan was guided in real time by dynamic methods of assessing the coagulation status, it can be said that individualized therapy, applied based on successive data, had much better results in terms of the quality of health care, costs, and most importantly in the survival of patients with minimal side effects. Therefore, there is a strong recommendation to approach these tests from the emergency room units and as soon as the patient is admitted to intensive care.
Keywords:
coagulation factor XIII
; ROTEM
; trauma
Introduction
The factor XIII (FXIII) plays an important role in haemostasis, tissue repair, thrombus formation, and multiple pro-inflammatory conditions associated with activation of the coagulation system. Moreover, factor XIII, together with the fibrinogen, contributes to the regulation of the quantity of erythrocytes (red blood cells) included in the thrombus mass, thus influencing the size and final stability of the clot.[1] The biochemical properties of FXIII are as interesting as its unusual biology, generating unique, yet poorly defined mechanisms. In addition to its role in the coagulation pathway, FXIII is essential in several vital biological processes, such as angiogenesis, wound healing, pregnancy maintenance, bone metabolism, and cardiovascular protection. Therefore, patients with severe FXIII deficiency (FXIIID) have prolonged wound healing, recurrent spontaneous abortions, umbilical bleeding, and intracranial haemorrhage. All common coagulation tests, such as bleeding time (BT), activated partial thromboplastic time (APTT), pro-thrombin time (PT), thrombin time (TT), and platelet count, are normal in patients with FXIII deficiency (FXIIID). However, this makes it more difficult to establish the correct diagnosis, especially in the context of multiple trauma in which these tests have a decreasing practical value in the management of bleeding. Diagnosis of the deficiency was previously made with the help of the clot solubility test, which is no longer recommended even for FXIIID screening; currently it is recommended the use of a functional FXIII activity test, and for confirmation of the diagnosis, the molecular analysis [2].
Early detection of severe blood loss is essential for the survival of a patient suffering from profuse bleeding. Common assessment methods used in the hospital environment, such as measuring blood pressure and determining haemoglobin values, most of the time can be misleading. Depending entirely on these criteria can often result in delayed diagnosis of haemorrhagic shock, which is associated with increased mortality. The Advanced Trauma Life Support (ATLS) program trains healthcare professionals to use basic clinical techniques, such as: assessment of vital signs, pulse pressure, skin colour, capillary refill time, and mental status, to assess the severity of trauma, identify and treat immediate life-threatening conditions, and estimate blood loss [3]. A rapid and focused assessment is essential for the prompt recognition of patients who are already in haemorrhagic shock or who are at increased risk of developing it.
A study on the epidemiology of deaths among polytrauma patients showcased that death in the first 48 hours after the accident is caused by excessive haemorrhage in 40% of the cases, and in patients requiring emergency surgery 80% of deaths occur due to diffuse bleeding [4].
Despite the fact that the specialized literature is incomplete in regards to the use of ROTEM protocols in emergency situations, in this paper it is aimed to identify and possibly to emphasize the relationship between early diagnosis and monitoring of FXIII deficiency treatment using the ROTEM method, a connection that would influence clinical outcomes in poly-traumatized patients.
The Impact of Trauma On Fluid-Coagulant Balance
In addition to the quantitative deficit of factors involved in coagulation, the haemorrhage also causes a functional restriction of the haemostatic mechanisms. Disorders such as hyperfibrinolysis, progressive decrease in platelet count, acidosis and hypothermia simultaneously contribute to the deterioration of the coagulation equilibrium, requiring early, intensive and targeted intervention. For a long time, the coagulation disorder with dilution effect has been a strong argument against the use of resuscitation with large volumes of crystalloid solutions, both in the pre-hospital and in-hospital phases. As blood loss continues, plasma components essential for the haemostasis process are not properly replaced, but only diluted. The exclusive administration of crystalloids to restore the circulating volume does not contribute to the restoration of these factors, but, contrary to all beliefs, further reduces their concentration, thus worsening bleeding. Moreover, it has been observed that this type of resuscitation is frequently associated with hyperfibrinolysis, a phenomenon that can have fatal consequences. However, recent studies have shown that dilution is only part of the problem, as coagulopathy can also occur independently of crystalloid administration, mainly in the context of major trauma [5]. Consumptive coagulopathy, which was initially considered the main mechanism responsible for the coagulation disorders observed in patients with massive haemorrhage, is based on the idea of local depletion of factors involved in haemostasis, such as: coagulation factors, platelets, thrombin, and other mediators of the coagulation process. In situations of severe and multisystem tissue injury, such as severe crush trauma, this phenomenon seems to play a important role in the development of haemorrhagic coagulation dysfunction.[6]
The appearance of shock is closely correlated with the development of hyperfibrinolysis and a marked deterioration of the clinical course. When the lysis value at 30 minutes (LY30), determined by thromboelastography (TEG), exceeds the limit of 3%, the risk of death increases almost tenfold [7]. Despite the fact that the fibrinolysis is a normal physiological mechanism, hypoperfusion produces an alteration of the regulatory factors, which leads to excessive activation of the fibrinolytic process. In the context of haemorrhagic shock, tissue plasminogen activators (tPA) transform plasminogen into plasmin, causing their expression to increases systemically. At the same time, the activity of the PAI-1 inhibitor decreases as a result of its depletion and these changes determine uncontrolled clot lysis, favour diffuse hemorrhage, and contribute to the installation of a severe coagulopathy, difficult to control therapeutically [8]. Therefore, in the preoperative, intraoperative and postoperative periods, it is essential that resuscitation measures are applied correctly and consistently, in order to prevent complications caused by tissue hypoperfusion. Last but not least, it should be emphasized that the administration of crystalloids can increase metabolic acidosis, contribute to the occurrence of coagulopathy, alter the immune response, and generate adverse effects on the lungs and kidneys, therefore, limiting their usefulness in patients with extensive haemorrhage [9].
Rotational Thrombolastometry and Thromboelastography
Thromboelastography (TEG) was first presented by Harter in 1948 as a method of global coagulation monitoring, using whole blood (not only plasma), which through a graphic display describes the entire process of clot formation, mechanical behaviour, and its dissolution (fibrinolytic phase). Thromboelastography is a graphic representation of the vascoelastic properties of blood (it clots in a reproduced venous blood flow environment), and it gives information on the kinetics of clot formation, its stability, and firmness. The analysis of kinetics provides essential information on platelet function and the activity of coagulation factors, while the strength and stability of the clot reflect the efficiency of the haemostasis process. Because it assesses the firmness and elasticity of the clot, thrombelastography is sensitive to all interactions between plasma and cellular components involved in coagulation and fibrinolysis. TEG therefore allowing the in vitro measurement of the time required for the initiation of clot formation, its evolution, and the degree of stability and retraction. An important advantage is represented by the fact that the laboratory medicine specialist is not required to be present and the tests can be performed directly in the ward or in the surgical room [10].
There are multiple tests that can be performed using ROTEM:
1). Natem:
It provides a classic thromboelastogram of the whole blood, excluding the additives and it allows a graphical analysis of global haemostasis;
2). Extem:
It contains a tissue activator that provides information similar to PT/INR tests and it analyses the coagulation pathway when the tissue factor (TF) binds to factor VII (FVII) and finally activating the “extrinsic pathway” of coagulation;
3). Fibtem:
It uses cytochalasin D which is a platelet inhibitor that blocks their contribution to coagulation, thus allowing the assessment of the role of fibrinogen in the clot formation process;
4). Intem:
It contains phospholipids and elagic acid as coagulation activators and it reflects the activation of coagulation through the “intrinsic pathway”. The results provided by Intem are similar to those of the a-PTT test and represent the sub-analysis closest to Natem;
5). Aptem:
While it is similar to Extem, it allows the identification of an accentuated fibrinolysis by the addition of a fibrinolysis inhibitor, therefore reversing the changes observed in TEG;
6). Heptem:
It is used for heparinase analysis when it is suspected the presence of heparin analogues in the blood (it affects coagulation). These analogues can be introduced exogenously or endogenously. By adding heparinase to the analysis cuvette, these compounds are degraded and coagulation is fully or partially restored. Heptem can be combined with Intem to differentiate between the effect of heparin and a deficiency of coagulation factors[11].
While INTEM and HEPTEM are second-line tests in the trauma patient, EXTEM and FIBTEM are first-line tests [10].
Figure 1.
Normal thromboelastogram (image taken from https://anesthguide.com/topic/rotem-teg-and-multiplate/).
Figure 1.
Normal thromboelastogram (image taken from https://anesthguide.com/topic/rotem-teg-and-multiplate/).
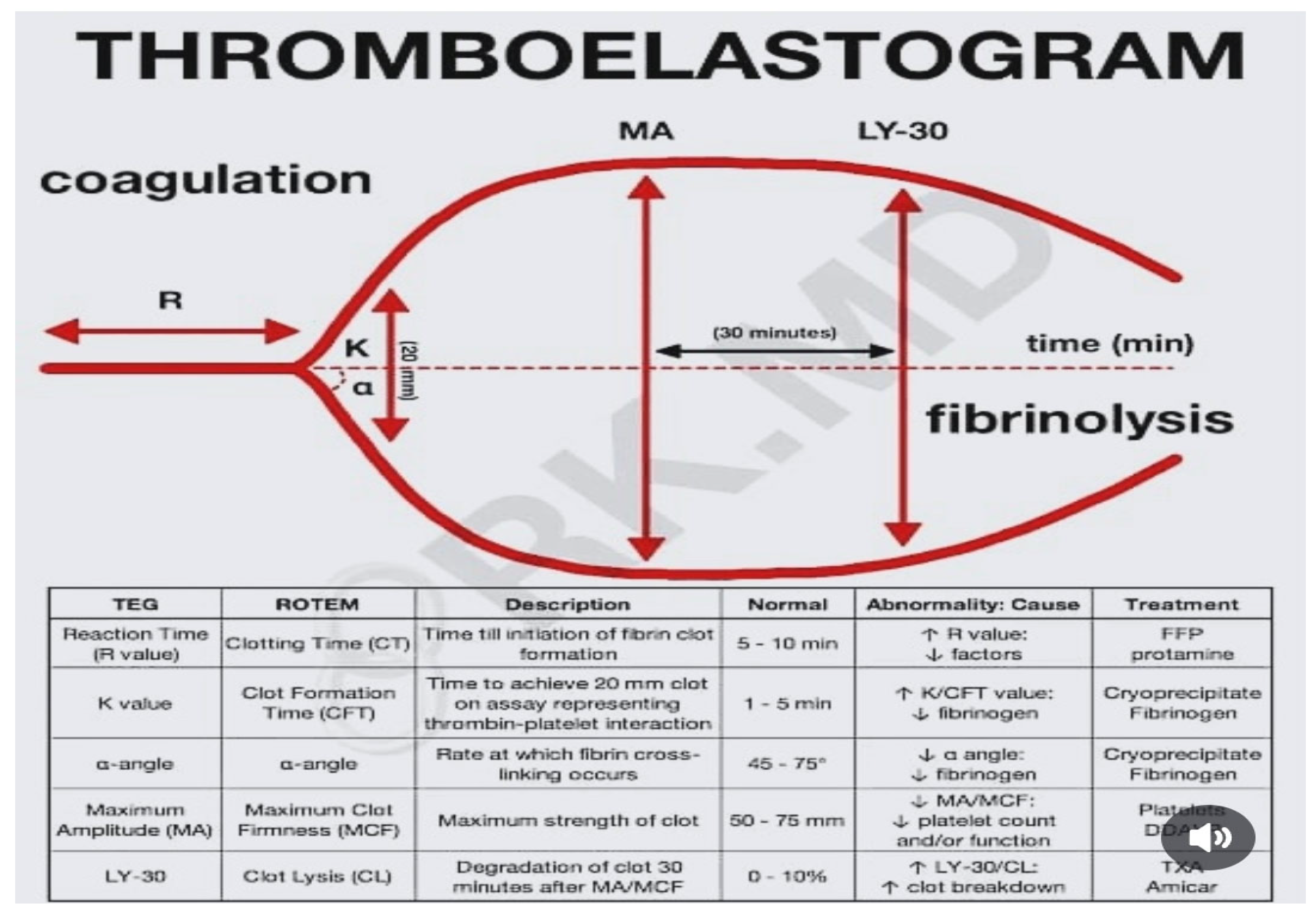
The risk of bleeding because of coagulopathy occurs if the CT or CFT are greater than twice the normal value or if the MCF is less than 45 mm. Haemostasis is good only in the case of a decrease of the coagulation factor reserve if the CFT is between 1.5 and 2 times normal or if the MCF is 45-49 mm, and the hypercoagulable status is defined by a MCF value greater than 72 mm or an alpha angle greater than 83° [10].
Objectives
In this work it is aimed to establish the veracity of the effect of early diagnosis (by ROTEM analysis) and monitoring of treatment of factor XIII deficiency on morbidity and mortality among patients with polytrauma. Secondary, it is aimed to follow the impact of the volume transfused (RBC, PPC, Cryoprecipitate or FXIII conc), haemostasis required time, the possible complications, hospitalization duration and the changes in ROTEM parameters and their correlation with factor XIII activity.
Methods
While building the foundation of this work, it has been established a semantic research in order to highlight a possible relationship between the diagnosis of factor XIII deficiency using the ROTEM method and an earlier and more accurate intervention among polytraumatized patients.
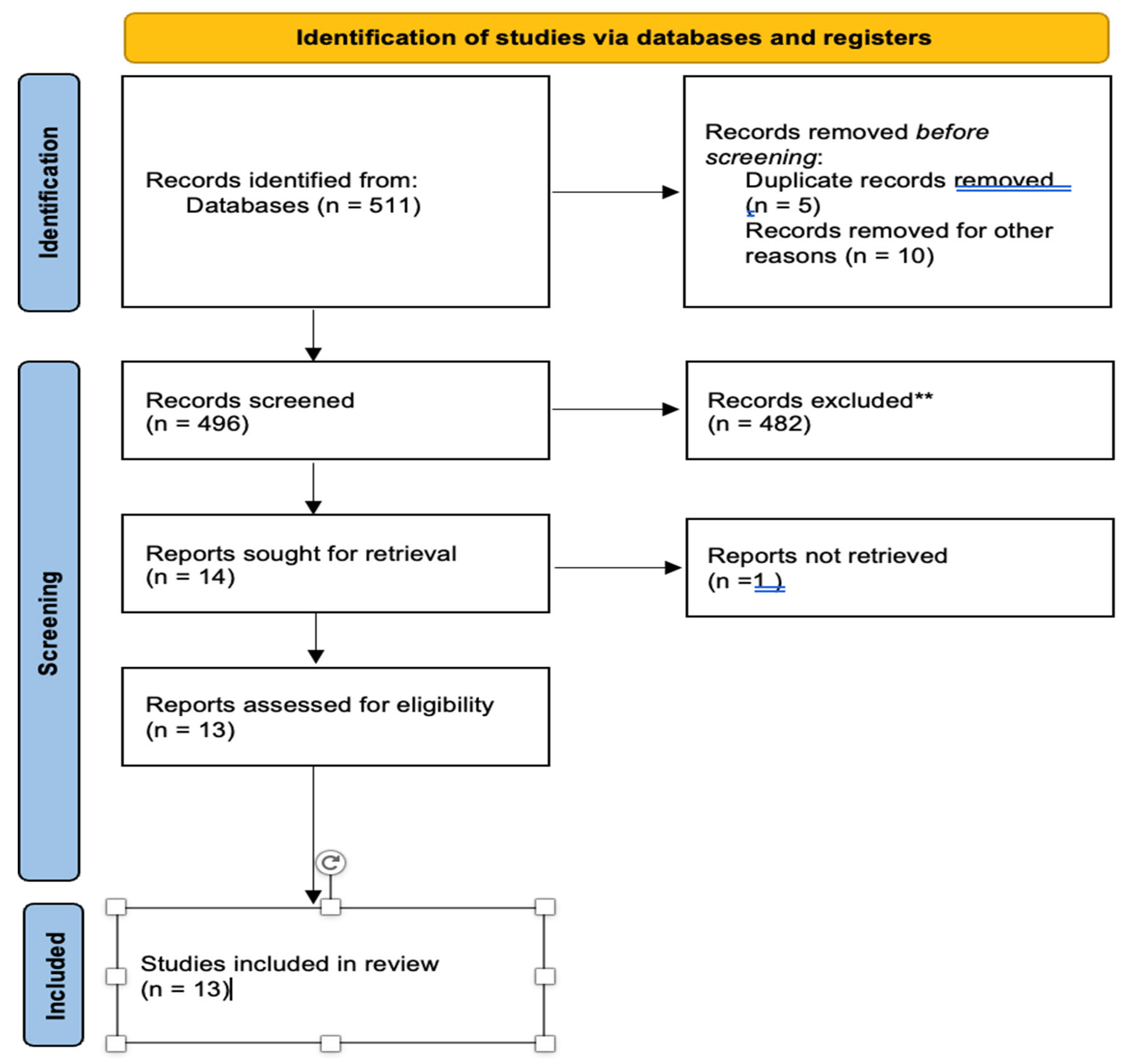
The search for scientific articles was carried out in the PubMed, Scopus and Cochrane Library databases with the indications “ROTEM and factor XIII and trauma” and finally 511 results published over time in different countries were identified. Elicit AI (Ought, 2025) was used as a support tool for identifying and organizing relevant articles. This tool is an assistant based on artificial intelligence that was used to generate an initial list of potentially eligible publications by semantically matching the research question with the content of the abstracts available in the Semantic Scholar database (an algorithm that is not based entirely on the given keywords, but also on understanding the text). Elicit AI Score Threshold function was used alongside manual selection in the process of setting the threshold to 2.7 (out of 5). This value was chosen to achieve a balance between relevance and volume, therefore, reducing the number of articles to 13. With the use of the previous stated tools, the analysis has become more manageable while allowing focused approach on studies significant to the research question. The selected threshold allows the inclusion of articles with moderate to high relevance, therefore, ensuring an efficient review and a detailed critical appraisal while focusing on the important aspects. All articles proposed by Elicit were subsequently manually and independently reviewed in order to confirm their eligibility according to the inclusion and exclusion criteria. In order to increase the timeliness of the results and strengthen the power of recommendation, the preparation of this work was guided by the PRISMA 2020 guideline and is based on the following inclusion criteria:
- Population chosen for the study are polytraumatized adults with suspicion/diagnosis of FXIII deficiency, the type of trauma, and the severity;
- Intervention is mainly targeting measurement of blood coagulation activity and application of targeted treatment adapted to the results of laboratory tests
- Standard: conventional management, i.e. common laboratory analyses or studies without comparator;
- Outcomes and results are focused on mortality, diagnosis time, time until transfusion, blood product type, haemostasis, complications, hospital stay duration, ROTEM parameters and FXIII level;
- The studies targeted were focused on randomized controlled trials (RCT), longitudinal studies, and group studies;
- As an addition, full-text articles in English, published between 2000 and 2025 were selected in order to ensure the relevancy of the study. The search was restricted to studies published since 2000, because from this moment the ROTEM method began to be used on a wider scale considering the administrative circumstances.
This analysis has excluded animal studies and case reports, narrative reviews, letters, and studies which include patients on chronic anticoagulant or antiplatelet therapy.
For each article it has been recorded: author, publication year, sample size, population characteristics, intervention, comparison instruments, main results, and reported statistical indicators. Elicit AI was additionally used to check the consistency of extracted data and to generate preliminary summaries of key variables such as intervention type, primary outcome, study design.
Figure 2.
Study identification from databases and registries.
Results

Table 1.
Included studies presentation.
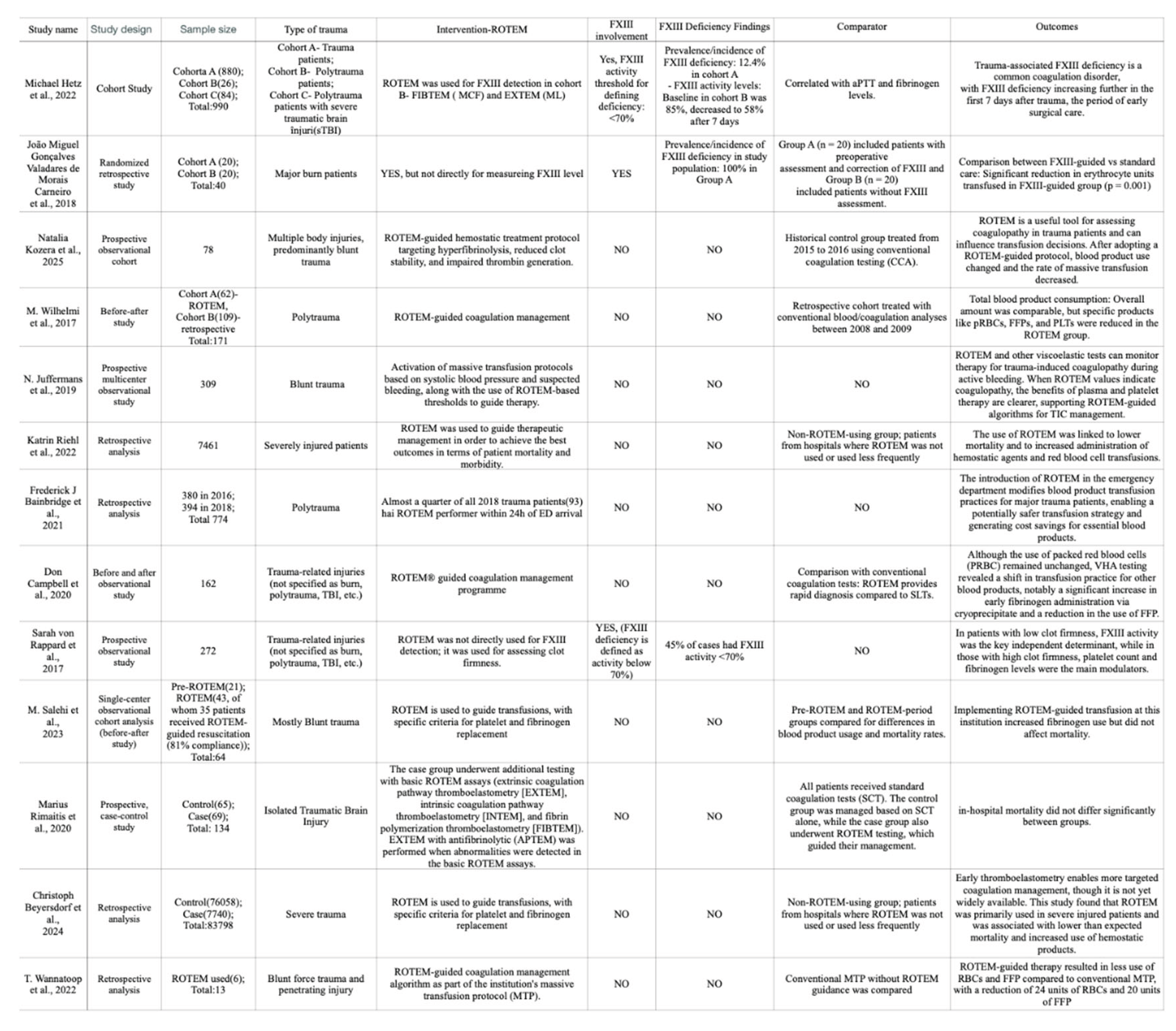
The 13. studies evaluating coagulation management strategies in trauma patients. Between the studies chosen, their importance has varied from studies which targeted factor XIII deficiency and studies which focused more testing ROTEM comprehensive protocols.
The groups analysed were diverse, with sample sizes ranging from 13 to 83,798 patients. Most studies were focused on blunt trauma, and targeted observational or before and after structures, therefore, comparing ROTEM-guided coagulation management with conventional testing. Just two studies were targeted on correcting factor XIII deficiency in the context of burn surgery.
In the burn wounds test population, the factor XIII deficiency was identified using specialized laboratory techniques rather than by ROTEM parameters. The procedure was conducted by collecting blood in citrate tubes, centrifuging, and analysing them by using specific reagents. The deficiency was defined by factor XIII activity smaller than 70%. Standard coagulation tests failed to detect the deficiency, therefore underscoring the need for dedicated assays.
The factor XIII activity was directly measured in the studies conducted by Hetz et al., and ROTEM testing, done by FIBTEM (maximum clot firmness) and EXTEM (maximum lysis) tests, was performed separately. The deficit was defined by factor XIII activity with an upper limit of 70%. ROTEM parameters were used to measure clot stability. The in vitro administration of factor XIII resulted in increased maximum firmness in FIBTEM and reduced maximum lysis in EXTEM.
Most studies using ROTEM were focused on overall optimization of coagulation management, rather than the detection of factor XIII deficiency. ROTEM was commonly performed in the operating room and had a turnaround time of approximately 15 minutes. It was used to guide transfusion decisions according to thresholds established for EXTEM, INTEM, and FIBTEM. The median time to confirmation of haemostasis was 92 minutes with ROTEM compared to 287 minutes when using conventional tests, therefore, demonstrating the superiority in terms of rapidity of results.
Factor XIII deficiency has been shown to be very common in certain trauma subgroups. Evolutionary analysis showed an increase in the deficiency after trauma. In patients with polytrauma, factor XIII activity decreased from 85% at presentation to 58% after seven days, with progressive worsening during the first week, evolution which marked it as a critical stage for early surgical management. Signs of activation and accelerated factor XIII consumption were noted within one hour of trauma.
The deficiency was associated with significant changes in coagulation parameters, with significant differences in age, hemoglobin, fibrinogen, hematocrit, platelet count, aPTT, and INR between patients with factor XIII activity smaller than 70% and those with values bigger than 70%.
In burn surgery, correction of factor XIII deficiency significantly reduced the need for red blood cell mass. Patients evaluated and treated for deficiency required significantly fewer units of red blood cell concentrate (1.95 versus 4.05; p = 0.001). There were no significant differences in the use of fresh frozen plasma, platelets, or fibrinogen concentrates.
The impact of ROTEM use on mortality varied between studies. In the largest retrospective analysis (83,798 patients), the observed mortality in the ROTEM-managed group was 4.1% lower than expected. The analysis suggested that the use of ROTEM could reduce expected mortality by 2.5% (number needed to treat: 40), the difference being statistically significant (p = 0.043). In the case of patients with traumatic brain injury, in-hospital mortality did not differ majorly between groups, but factor XIII activity at six months was significantly different between patients with favourable and unfavourable outcomes, according to the modified Rankin scale.
Changes in ROTEM parameters from the scene of the accident to presentation in the emergency department revealed deterioration in coagulation: both clotting time and clot formation duration increased significantly, while maximum clot firmness decreased for EXTEM, INTEM, and APTEM (p ≤ 0.004). For FIBTEM, the same trends were observed and illustrated an increased clotting time and decreased maximum firmness.
Postoperative, ROTEM parameters improved significantly in patients treated according to the specific protocols, and the number of cases with coagulopathy was reduced. The overall adherence rate to the ROTEM protocols was 85.3%, facilitating coherent coagulation management and superior clot quality. Haemostatic agents were administered considerably more frequently in the subgroup evaluated by ROTEM, with an increased use of products intended to correct coagulopathy. ROTEM allowed the identification of patients with hypofibrinogenemia who required cryoprecipitate exclusively, thus reducing the need for erythrocytes and fresh frozen plasma.
Discussions
Although the benefits of ROTEM protocols are evident in the general management of traumatic coagulopathy, the current literature provides limited evidence regarding the direct impact of rapid detection by ROTEM on the evaluation or treatment of factor XIII deficiency. Currently, the use of specific tests proved its importance for the diagnosis of this deficiency, and the need to integrate factor XIII into trauma patient care algorithms remains a major area of interest for future research. Further studies are needed to clarify the integrated role of factor XIII in guided rapid testing algorithms and to establish standardized intervention protocols in this critical population.
Conclusions
The cumulative analysis of the 13 studies included in this systematic review indicates that factor XIII deficiency is a frequently overlooked condition in the context of major trauma and burn surgery, with relevant clinical consequences on clot stability and transfusion requirements. Although ROTEM has proven to be a powerful tool for the rapid and dynamic assessment of coagulation status, it does not allow the direct diagnosis of factor XIII deficiency, which requires the use of specific laboratory tests. The data analysed show a progressive decrease in factor XIII activity after trauma, reaching critical values in the first days of care; the presence of deficiency correlates with a more severe coagulopathy and with the alteration of global haemostasis parameters.
Targeted correction of factor XIII deficiency, particularly in burn surgery, has been associated with a significant reduction in red blood cell requirements, without a concomitant increase in the risk of thromboembolic complications, suggesting both a transfusion benefit and a potential positive impact on the quality of haemostasis. In parallel, extended protocols guided by ROTEM, and although not aimed at specifically identifying factor XIII deficiency, contribute to optimizing haemostatic management, reduce the use of blood products (red cells and fresh frozen plasma), decrease the frequency of massive transfusion, and facilitate rapid haemostasis compared with conventional methods. In the largest data set evaluated, the use of ROTEM was associated with a significant reduction in mortality, as well as with improvements in major clinical indicators, such as the duration of intensive care unit admission and the incidence of acute respiratory distress syndrome.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lawrence LK Leung: Overview of hemostasis, UpToDate. 2025.
- Dorgalaleh, A.; Rashidpanah, J. Blood coagulation factor XIII and factor XIII deficiency. ScienceDirect. 2016.
- Committee on Trauma: Advanced Trauma Life Support Program; American College of Surgeons: Chicago, 2012.
- Sauaia, A.; Moore, F.A.; Moore, E.E.; Moser, K.S.; Brennan, R.; Read, R.A.; Pons, P.T. Epidemiology of trauma deaths: a reassessment. J Trauma 1995, 38, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Rizoli, S.B.; Scarpelini, S.; Callum, J. Clotting factor deficiency in early trauma-associated coagulopathy. J Trauma 2011, 71, S427–S434. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.R.; Brohi, K.; Dutton, R.P. The coagulopathy of trauma: a review of mechanisms. J Trauma 2008, 65, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Cotton, B.A.; Harvin, J.A.; Kostousouv, V. Hyperfibrinolysis at admission is an uncommon but highly lethal event associated with shock and prehospital fluid administration. J Trauma Acute Care Surg 2012, 73, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Cardenas, J.C.; Matijevic, N.; Baer, L.A. Elevated tissue plasminogen activator and reduced plasminogen activator inhibitor promote hyperfibrinolysis in trauma patients. Shock 2014, 41, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J.B.; Jenkins, D.; Rhee, P. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma 2007, 62, 307–310. [Google Scholar] [CrossRef] [PubMed]
- GRINŢESCU, I.C.; MIREA, L.; BEURAN, M.; GRINŢESCU, I.M. Trombelastometria rotaţională (ROTEM) – o nouă metodă de diagnostic al tulburărilor complexe de hemostază la pacientul politraumatizat. RJMP, 2015. [Google Scholar]
- Knudsen, K. Hemostasis Monitoring and Treatment, ROTEM and TEG in ICU. In The Anesthesia Guide; August 2025. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



