Submitted:
12 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Background: One of the debating issues in trauma care is the effect of “golden hour” when it comes to patient treatment after major injury. Although there is consensus in the medical community that trauma is a time-sensitive issue, empirical analysis on clinical data often ends up with insignificant conclusions on the relationship between time after injury and definitive care. Especially, the literature largely focuses on the association between pre-hospital times and trauma patient mortality. Relationships between pre-hospital times and clinical outcomes such as operative intervention and the length of hospital stay, are relatively understudied.
Method: Based on the records of 488 trauma patients admitted from 2017 to 2021 at an urban Level I trauma center, we investigated the impact of prehospital times on the risk of operative intervention, and the length of hospital stay, using machine learning techniques (decision trees) in conjunction with methods in statistical inference.
Results: Controlling the Revised Trauma Score at 12 or above, the mean length of hospital stay is significantly shorter for patients who had response times (time between dispatch call and EMS arrival) below 32 minutes (p-value 0.05, 3.83 days vs 5.15 days). Patients with on-scene times (time between arrival and departure of EMS vehicle) below 19 minutes had significantly shorter hospital stays (p-value 0.00246, 3.25 days vs 4.47 days). Patients who arrived at the emergency department (total prehospital time) within 61 minutes had significantly shorter hospital stays (p-value 0.041, 3.63 days vs 4.43 days). In terms of operative intervention, patients with total pre-hospital time within 76 minutes had significantly lower risk of operative intervention (p-value 0.0119, 22.6% vs 32.9%).
Conclusion: Although there may exist many confounding factors associated with the length of hospital stays and the risk of operative intervention, this study reveals significant data evidence supporting the existence of an optimal time point, the “golden hour” principle, in trauma care. It suggests the need for rapid responses to reduce the total pre-hospital time, which may significantly minimize the length of hospital stay and reduce the risk of operative interventions.
Keywords:
clinical outcomes
; trauma
; patients
1. Introduction
Traumatic injury is the leading cause of death for individuals forty-five and younger. It is also the fourth leading cause of death for individuals of all ages [1,2,3]. While there is agreement that trauma is a time-sensitive issue, clinical data analyses often end up with insignificant conclusions on the relationship between time after injury and definitive care [4,5,6]. One of the most controversial issues in trauma care is the effect of the “golden hour”, which is related to the time immediately after a patient experiences a severe injury. Published papers indicate rapid medical intervention during pre-hospital time may reduce mortality [6,7,8]. However, few studies consider the impact of pre-hospital times on clinical outcomes such as the length of hospital stay (LOS) and the risk of operative intervention, partially because prehospital time is just one of the complex combination of factors affecting treatment outcomes after trauma injuries [8].
In this paper, we refer to the time between injury and intervention as pre-hospital time. Response time is the amount of time from when the dispatch call is first made to when the EMS vehicle arrives on the scene. On-Scene time is the time from EMS vehicle arrival (on-scene time) to its departure from the first scene. Transport time is the amount of time from the EMS vehicle’s departure from the scene to arrival at the ED. Total pre-hospital time is the amount of time from emergency medical service (EMS) activation (dispatch) to Emergency Department (ED) admission. The total pre-hospital time consists of three components: response time, on-scene time, and transport time. Certainly, the timeframe of intervention and treatment outcome may also depend on other factors such as the nature of the injury and the patient’s underlying health conditions.
Current research [8,9,10] on injury timing and definitive care for trauma patients focuses on the correlation between rapid access to care and the corresponding mortality. In addition to mortality, the overall medical costs also include the length of hospital stay (LOS) and operative intervention. However, the impact between injury timing and LOS has typically been understudied, mainly because of high degrees of data variation [8,9]. For instance, trauma patients who experienced severe injuries and were rushed to the hospital might have shorter hospital stay times if they passed away immediately after arriving at the hospital. In this case, the LOS has nothing to do with prehospital time. Toward this end, the Revised Trauma Score (RTS) is often used to screen out the prognosis of trauma patients before the analysis of clinical outcomes such as mortality, LOS, or operative intervention. In fact, although prehospital times are important, RTS is usually a more significant and determining factor associated with clinical outcomes.
RTS is part of the reason for large data variation. Delays in medical intervention after injury may clinically cause blood clots or related organ damage, which may lead to longer LOS or higher chance of operative intervention. On the other hand, for the dataset under consideration, we have patients who were seriously injured (RTS of 3 or lower) and short prehospital times, however, their values of LOS vary greatly. Clearly, those patients were rushed to the hospital (short pre-hospital time) due to severe injuries. Some of them had short LOS on record because they passed away soon after arriving at the hospital. Some of them had relatively long hospital stay due to severity of the injury. For these patients, the effect of RTS partially confounded and distorted the impact of prehospital time on LOS. Similar confounding impact also appeared to patients with operative intervention. To fairly examine the impact of prehospital times on LOS and operative intervention without interactions on RTS, we confine the dataset to patients who had RTS at 12 or above in the study.
Mechanism of injury, injury patterns, and associated injuries are other critical confounding factors that should be considered. For instance, blunt polytrauma with TBI patients are more likely to stay longer in hospital, while patients with inner city penetrating trauma may require a quick fix and discharge, or could end up with mortality1. Thus, in the dataset, we also excluded patients with penetrating trauma (gunshot wounds and stabbing).
2. Materials and Methods
The database in the study consists of 488 medical records from trauma patients admitted to an urban Level I trauma center during the period from 2017 to 2021. Basic patient characteristics are summarized in Table-1. Because the original dataset contains patients who had low RTS, to avoid confounding effects of RTS, patients with RTS measures below 11 were excluded. With respect to the length of hospital stay, patients with RTS below 11 appear to be characteristically different from patients with RTS above 11 (p-value is 0.00017). The average hospital length for patients with revised trauma scores below 12 (sample mean = 11.8 days, sample standard deviation = 10.9 days, 32 patients) is much longer than the average LOS for patients with RTS values equal to or above 12 (sample mean = 4.04 days, sample standard deviation = 4.53 days, sample size = 427 patients). The small p-value (0.00017< 0.05) indicates that RTS is a strong confounder in the analysis on the relationship between pre-hospital times and LOS. For this reason, we only consider patients with RTS at 12 or higher in the study.
A second confounding factor is the mechanism of injury and method of transportation. This dataset includes patients who were transported to the hospital by air and by ground transportation. Usually, trauma patients with severe injuries or those living in remote locations far from the hospital were transported by air. To avoid possible confounding effect of transport methods, we exclude the small amount (18) patients who were transported by air and only investigated patients who arrived the hospital via ground (n = 409) transportation without penetrating trauma.
In terms of data analytics, conventional methods usually rely on model assumptions, which are debatable for trauma injury data. For example, the principle regarding the “golden hour” is that treatments during a relatively quick time frame post injury have an outsized impact on patient outcomes. However, conventional methods of data analytics rely on the assumption of the underlying parametric relationship between continuous prehospital time and clinical outcome. Model assumptions and inference procedures often hinder valid comparisons and result in insignificant LOS differences for each prehospital time. In this study, we introduce a machine learning method (regression trees and classification trees) to analyze the trauma patient data. For the study on LOS, the method of regression tree is applied to select the best splitting point to form two patient groups with best LOS homogeneity within each group. For operative intervention, the method of classification tree identifies the best partition of different pre-hospital times associated with categorical clinical outcomes (Yes or No) for operative intervention. There is no model assumption hidden behind the decision tree method in the search of optimal time thresholds, the “golden hours”. After identifying the threshold splitting time for prehospital events, statistical methods are used to validate the LOS difference before and after the splitting prehospital time point.
Data description consists of descriptive statistics summarizing trauma patient characteristics in the data. Statistical differences for categorical variables were evaluated using the Pearson’s Chi-square test. As for continuous variables, the LOS comparison is performed using the Student-t or Mann-Whitney Wilcoxon test, when appropriate. Each measure of pre-hospital time (response time, on-scene time, transport to ED time, total pre-hospital time) is fitted with a regression tree to find the threshold (splitting time point) for LOS homogeneity. Correspondingly for operative intervention, classification trees are used to estimate the optimal threshold of splitting time point, which forms homogeneous patient groups on the risk of operative intervention.
The decision tree analyses (and statistical inference) are run in RStudio (2024.12.0 Build 467, 2009-2024 Posit Software, PBC). A p-value of 0.05 is considered statistically significant.

Table 1.
Descriptive Statistics of Prehospital Times of Trauma Patients with RTS ≥ 12.
| Age | Response | On-scene | Transport | Prehospital | RTS | LOS | |
| Mean | 59.79 | 21.50 | 22.07 | 24.10 | 67.66 | 12.07 | 3.97 |
| StD | 22.57 | 22.02 | 10.52 | 16.95 | 39.39 | 0.47 | 4.58 |
| Range | 87 | 180 | 63 | 96 | 233 | 4 | 40 |
| Minimum | 18 | 0 | 0 | 0 | 18 | 12 | 0 |
| Maximum | 105 | 180 | 63 | 96 | 251 | 16 | 40 |
| Sample size | 419 | 417 | 414 | 415 | 415 | 404 | 419 |
| Gender | Frequency | Race | Frequency | Mechanism | Frequency | ||
| Male | 233 (56%) | White | 339 (80.9%) | MVC | 119 (28.4%) | ||
| Female | 186 (44%) | Black | 57 (13.6%) | Assault | 14 (3.3%) | ||
| Hispanic | 15 (3.7%) | OV | 13 (3%) | ||||
| Asian | 2 (0.5%) | Fall | 226 (53.9%) | ||||
| Other | 6 (1.4%) | Other | 47 (11.4%) | ||||
| Unknown | 1 (0.2%) | ||||||
3. Results
We identified 419 trauma patients satisfying the selection criteria for the validation of pre-hospital times related to LOS and operative intervention. Of the patients, 233 (56%) were male and 186 (44%) were female. Most of the patients were White (80.9%). Patient ages in this dataset range from 18 to 105 years. The mean patient age is around 60 years with a standard deviation of 23 years. All patients in the study have a stable revised trauma score (RTS) from 12 to 16 with a standard deviation of 0.47. The length of hospital stays (LOS) range from 0 to 40 days with a mean length of 3.97 days and standard deviation 4.58 days.
LOS. For each of the four pre-hospital times, we fit a regression tree analysis with LOS as the response variable. The regression tree produces an optimal binary splitting time point, where patients are separated into two groups based on LOS homogeneity within each group. We report the analytical results as follows.
Table-2 summarizes the analytical results corresponding to the optimal splitting times of the four pre-hospital events in the dataset.
As shown in Figure 1, the first splitting time point for the total pre-hospital time is 60 minutes (less than 61 minutes). The average LOS of 3.6 days for 232 trauma patients who had total prehospital time less than 61 minutes, and the rest 185 trauma patients had an average LOS of 4.4 days.
Figure-2 indicates a splitting response time of 32 minutes. It separates 323 trauma patients who had response time less than 32 minutes with an average LOS of 3.8 days, versus the rest of 71 patients who had response time more than 32 minutes and less than one hour. The analysis is restricted to 394 patients with response time less than one hour. Patients with response time more than one hour are treated as outliers and excluded from the analysis.
Figure-3 shows the first splitting scene time of 19 minutes. It separates 174 trauma patients who had on-scene time less than 19 minutes (with an average LOS 3.3 days) from the rest of 240 patients who had scene time at least 19 minutes (average LOS 4.5 days).
Operative intervention. Besides the impact of prehospital times on LOS, we also examined the impact of prehospital times on the need of operative intervention using classification trees. This is because the outcome variable is binary (Yes or No on operative intervention), and the regression tree is not applicable to binary response variables [11,12,13]. Table-3 summarizes the analytical outcomes for the risk of operative intervention. Splitting times for response time and on-scene time are not statistically significant for the risk difference on operative intervention. However, the splitting times for the total pre-hospital time (p=0.0119) and transportation time (p=0.0107) are significantly different.
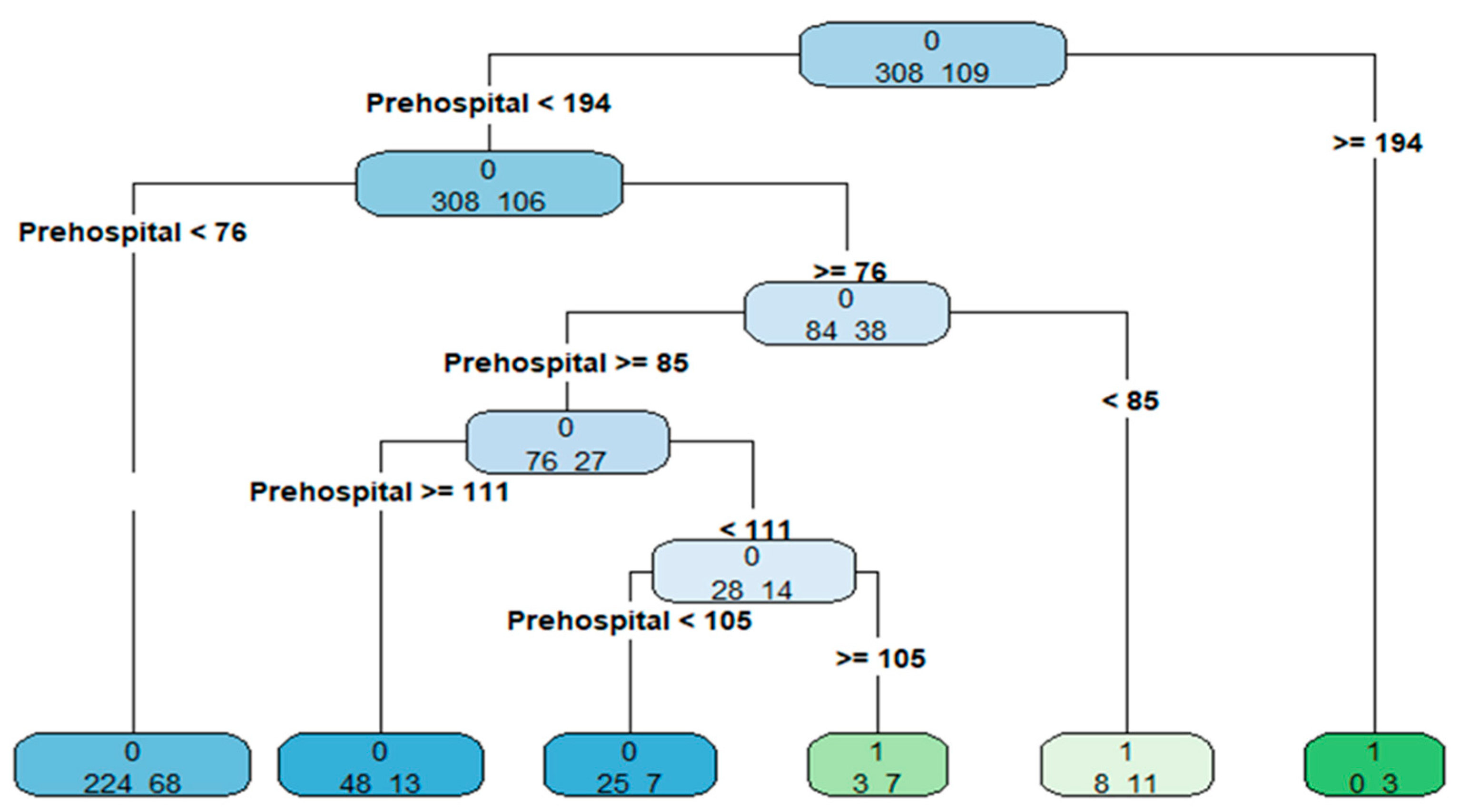
For convenience, the classification tree of operative intervention on total prehospital time is presented in Figure 4.
Figure-4 shows a splitting time of 76 minutes for the total prehospital time on the occurrence of operative intervention.
4. Discussion
Since clinical outcomes of trauma patients highly depend on the severity of injury [8,9,10], we restricted our consideration on trauma patients with revised trauma score (RTS) at 12 or above in this study. In this way, we investigated impacts of prehospital times on clinical outcomes without the major confounding effect of RTS. In terms of the mechanism of injury variable for the type of injury the patient had suffered, trauma patients under consideration in this study were most likely to have either suffered a fall (53.9%, Table 1) or have been involved in a motor vehicle collision (28.4%).
As mentioned above, the total pre-hospital time consists of three components: response time, on-scene time, and transport time to the ED. Table-1 indicates that the variance of the response time (22 minutes) is greater than the mean response time (21.5 minutes). This reflects relatively large response time variation for trauma patients. Compared with the response time, the scene time has relatively smaller standard deviation (relatively more stable), 22.07±10.52. This intuitively makes sense as response time requires dispatch operators to parse why the emergency call is being made and figure out how to get the caller help, while scene time measures the amount of time between EMS arrival and departure for the hospital. In this dataset, the transport time (from departing the first scene to arrival at the ED) is relatively large (ranging from 0 to 96 minutes). However, the mean value of the total pre-hospital time (from EMS activation to the arrival at the ED) is around one hour, 67 minutes.
Transport time on LOS. The LOS regression tree provides a splitting time point of ground transport to the hospital at 6 minutes, which is much shorter than most of the transport time, only 16 patients had transport time less than 7 minutes (Table 2). Although we confined the comparison to patients with ground transportation, the splitting time point is still not statistically significant for the LOS difference between patients with transport time less than 15 minutes versus those with more than 15 minutes transportation time (p-value is 0.2934). This may be partly due to the variation of other factors involved in the data. For instance, traffic conditions, geospatial location of the accident, mechanism of injury, and the impact of Covid-19 restrictions during the timeframe of data collection14-18.
Total prehospital time on LOS. As shown in Figure-1, the splitting time point for the total pre-hospital time to ED arrival is 61 minutes. This is remarkably consistent with the “golden hour” principle for trauma injuries. The corresponding p-value associated with the homogeneous LOS splitting point at 61-minute prehospital time is 0.041, as presented in Table 2. In other words, using this dataset, we are 95% confident that the length of the average hospital stays (LOS) for trauma patients who have pre-hospital times below 61 minutes is shorter than patients who have pre-hospital times above 61 minutes.
Response time on LOS. When we consider the response time (time from EMS activation to arrival at the scene), the difference at the optimal binary splitting point is statistically significant (p=0.05) for LOS. Two patients have missing values for the response time, so we excluded them and were left with 394 patients for the response time analysis. Using the LOS regression tree shown in Figure 2, we identified a splitting time point of 32 minutes for response time on LOS. The mean length of hospital stay is 3.8 days (3.83 ± 4.17 days) for the 323 trauma patients (who had an EMS arrive on the scene less than 32 minutes of the dispatch call being made). For the remaining 71 patients where the EMS arrived on or after 32 minutes but within an hour, the mean length of hospital stay is about 5.2 days (5.15 ± 6.42 days). Patients with response times exceeding an hour were outliers and removed for the purpose of meaningful comparison. As shown in Table 2, the corresponding p-value for the splitting time point is 0.05. This supports the hypothesis that patients with response times below 32 minutes have the mean LOS time shorter than their counterparts.
On-Scene time on LOS. On-Scene time measures the length of time between the arrival of the EMS vehicle on the scene to the departure of the EMS vehicle from the scene [16]. Using the LOS regression tree as shown in Figure 3, the splitting point for on-scene time is 19 minutes. As the analysis in total pre-hospital time and response time, patients with on-scene time below 19 minutes have significantly shorter average hospital stays (LOS) than patients who have scene times more than 19 minutes (p-value = 0.0025).
Risk of operative intervention. Operative intervention is an effective measure in assessing the impact of prehospital times, besides mortality [15,19,20,21]. As shown in Figure 4, for patients with the total prehospital time less than 76 minutes, 62 out of 274 patients needed operative intervention. Compared with the operative intervention rate of 143 patients who got hospital admission longer than 76 minutes, the difference on the rates of operative intervention is statistically significant (p=0.0119). This indicates that patients with shorter prehospital time have lower risk of operative intervention, and the estimated threshold is 76 minutes.
5. Conclusions
There are many factors associated with LOS and operative intervention of trauma patients. The uncertainty behind the data hinders empirical analysis of LOS data using conventional statistical methods due to legitimacy of modelling assumptions. However, as shown in the paper, the machine learning method (decision trees) side-steps traditional model assumptions and identifies significant splitting time points to support the fundamental principle of the “golden hour” in trauma care. The decision tree analysis (using this dataset) suggests that the combination of rapid responses at each step prior to arriving at the point of care may reduce the total pre-hospital time. This may consequently leverage medical burdens for trauma injury patients by optimizing LOS and lowering the risk of operative intervention.
| 1 | We thank the Academic Editor who kindly pointed out this confounding effect in the earlier version of the manuscript. |
References
- Homepage of the American Association for the Surgery of Trauma, https://www.aast.org/trauma-acs-resources/trauma-facts.html.
- Heron M. Deaths: Leading Causes for 2019. Natl Vital Stat Rep. 2021, 70, 1–114. [PubMed]
- Kochanek KD, Xu J, Murphy SL, Miniño AM, Kung H-C. Deaths: final data for 2009. Natl Vital Stat Rep. 2011, 60, 1–116. Available: https://www.ncbi.nlm.nih.gov/pubmed/24974587.
- Beekman, R.; Kim, N.; Nguyen, C.; McGinniss, G.; Deng, Y.; Kitlen, E.; Garcia, G.; Wira, C.; Khosla, A.; Johnson, J.; et al. Temperature Control Parameters Are Important: Earlier Preinduction Is Associated with Improved Outcomes Following Out-of-Hospital Cardiac Arrest. Ann. Emerg. Med. 2024, 84, 549–559. [CrossRef] [PubMed]
- Harmsen AM, Giannakopoulos GF, Moerbeek PR, Jansma EP, Bonjer HJ, Bloemers FW. The influence of prehospital time on trauma patient outcomes: a systematic review. Injury. 2015;46(4):602-609. [CrossRef] [PubMed]
- Brown JB, Rosengart MR, Forsythe RM, Reynolds BR, Gestring ML, Hallinan WM, Peitzman AB, Billiar TR, Sperry JL. Not all prehospital time is equal: Influence of scene time on mortality. J Trauma Acute Care Surg. 2016;81(1):93-100. [CrossRef] [PubMed]
- Chen, C.-H.; Shin, S.D.; Sun, J.-T.; Jamaluddin, S.F.; Tanaka, H.; Song, K.J.; Kajino, K.; Kimura, A.; Huang, E.P.-C.; Hsieh, M.-J.; et al. Association between prehospital time and outcome of trauma patients in 4 Asian countries: A cross-national, multicenter cohort study. PLOS Med. 2020, 17, e1003360. [CrossRef] [PubMed]
- Newgard, C.D.; Meier, E.N.; Bulger, E.M.; Buick, J.; Sheehan, K.; Lin, S.; Minei, J.P.; Barnes-Mackey, R.A.; Brasel, K. Revisiting the “Golden Hour”: An Evaluation of Out-of-Hospital Time in Shock and Traumatic Brain Injury. Ann. Emerg. Med. 2015, 66, 30–41.e3. [CrossRef] [PubMed]
- Berg, G.M.; Wyse, R.J.; Morse, J.L.; Chipko, J.; Garland, J.M.; Slivinski, A.; Lieser, M.; Biswas, S.; Carrick, M.M.; Rhodes, H.; et al. Decreased adult trauma admission volumes and changing injury patterns during the COVID-19 pandemic at 85 trauma centers in a multistate healthcare system. Trauma Surg. Acute Care Open 2021, 6, e000642. [CrossRef] [PubMed]
- Klutts, G.N.; Deloach, J.; McBain, S.A.; Jensen, H.; Sexton, K.W.; Kalkwarf, K.J.; Karim, S.; Bhavaraju, A. Increases in Violence and Changes in Trauma Admissions During the COVID Quarantine. Am. Surg. 2021, 88, 356–359. [CrossRef] [PubMed]
- Chen, J., Chen, L., and Lee C. (2024) Statistical Prediction and Machine Learning, Chapman and Hall, CRC.
- Alhajala H, Hendricks-Jones M, Shawver J, Amllay A, Chen J, et al. (2024) Expansion of Telestroke Coverage in Community Hospitals: Unifying Stroke Care and Reducing Transfer Rate. The Annals of Neurology, 2024 Mar; 95(3):576-582. [CrossRef] [PubMed]
- Chen L. and Chen J. (2023) Refined Machine Learning Approaches for Mask Policy Analysis. Book chapter in the book Healthcare Policy, Innovation and Digitalization edited by E. Cetin and H. Ozen, published by Springer in December 2023, Singapore.
- Chopra, A.; Al Yafi, M.; Luckoski, J.; Das, C.; Sferra, J.; Stanek, S. Management of Massive Upper Gastrointestinal Hemorrhage Secondary to Gastrosplenic Fistula. Am. Surg. 2022, 89, 6224–6226. [CrossRef] [PubMed]
- Al-Embideen S, Tahir J, Stanek S, Al-Jubouri M, Impact of Chronic Obstructive Pulmonary Disease on Patients with Traumatic Rib Fractures, Journal of the American College of Surgeons 236(5):p S126-S127, May 2023. [CrossRef]
- Jarvis, S.; Salottolo, K.; Berg, G.M.; Carrick, M.; Caiafa, R.; Hamilton, D.; Banton, K.; Lieser, M.; Bar-Or, D. Examining emergency medical services' prehospital transport times for trauma patients during COVID-19. Am. J. Emerg. Med. 2021, 44, 33–37. [CrossRef] [PubMed]
- Sabbaghi, M.; Namazinia, M.; Miri, K. Time indices of pre-hospital EMS missions before and during the COVID-19 pandemic: a cross-sectional study in Iran. BMC Emerg. Med. 2023, 23, 1–7. [CrossRef] [PubMed]
- Eskol, J.R.; Zegers, F.D.; Wittrock, D.; Lassen, A.T.; Mikkelsen, S. Increased ambulance on-scene times but unaffected response times during the first wave of the COVID-19 pandemic in Southern Denmark. BMC Emerg. Med. 2022, 22, 1–6. [CrossRef] [PubMed]
- Ritondale, J.B.; Piehl, M.; Caputo, S.B.; Broome, J.; McLafferty, B.B.; Anderson, A.B.; Belding, C.; Tatum, D.; Duchesne, J.; for the Damage Control Resuscitation Study Group; et al. Impact of Prehospital Exsanguinating Airway-Breathing-Circulation Resuscitation Sequence on Patients with Severe Hemorrhage. J. Am. Coll. Surg. 2024, 238, 367–373. [CrossRef] [PubMed]
- Jänig, C.; Schmidbauer, W.; Kollig, E.; Gruebl, T.; Lefering, R.; Hackenberg, L.; Schroeder, D.C.; Bieler, D. Pre-hospital assessment of trauma associated severe hemorrhage (phTASH) – analysis of TraumaRegister DGU® data from 2015-2021. Scand. J. Trauma, Resusc. Emerg. Med. 2025, 33, 1–8. [CrossRef] [PubMed]
- Clements, T.W.M.; Van Gent, J.-M.D.; Kaminski, C.M.; Wandling, M.W.M.; Moore, L.J.M.; Cotton, B.A.M. Are trauma centers penalized for improved prehospital resuscitation? The effect of prehospital transfusion on arrival vitals and predicted mortality. J. Trauma Acute Care Surg. 2024, 97, 799–804. [CrossRef] [PubMed]
Figure 1.
Regression tree of LOS on the total prehospital time.
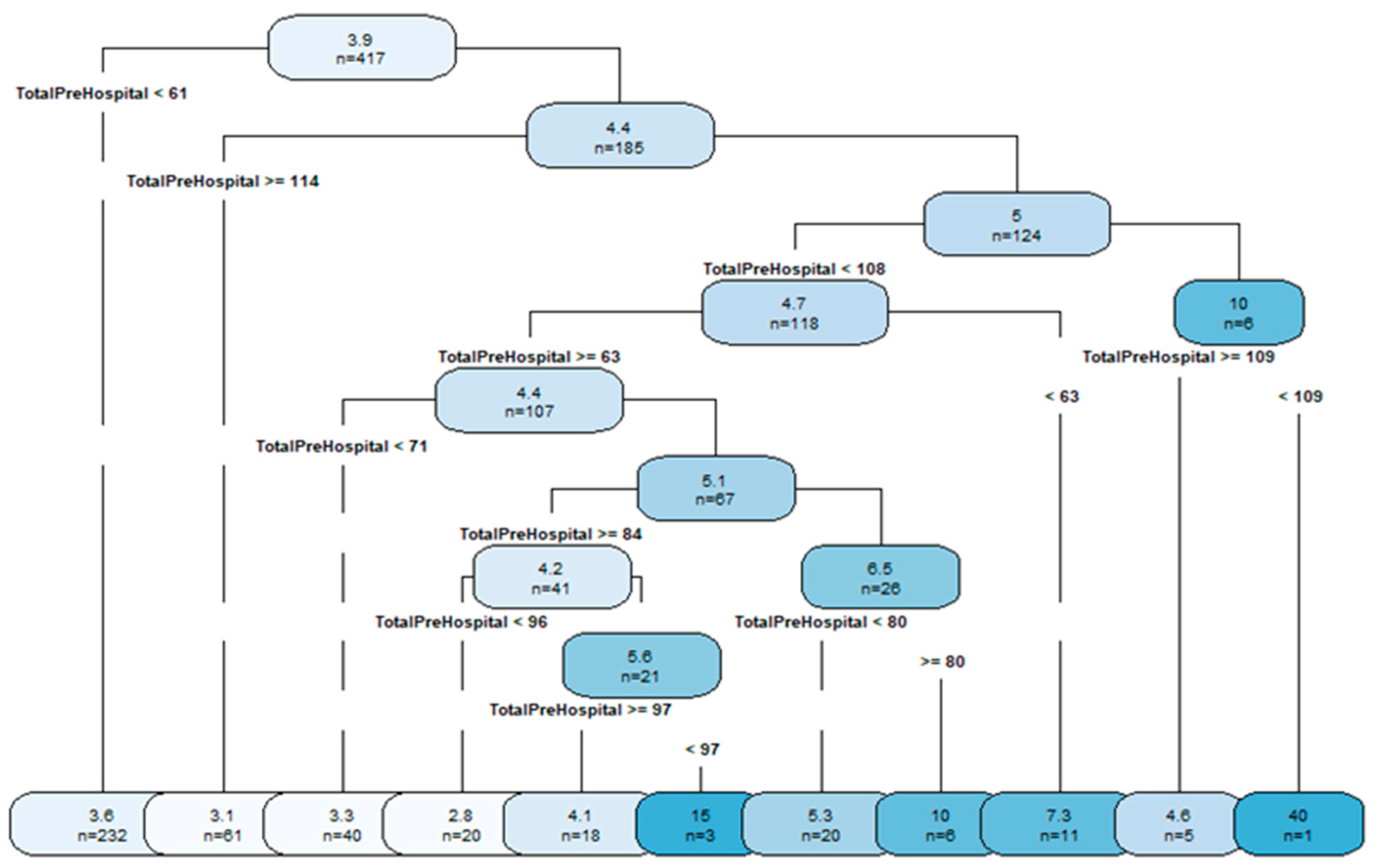
Figure 2.
Regression tree of LOS on response time.
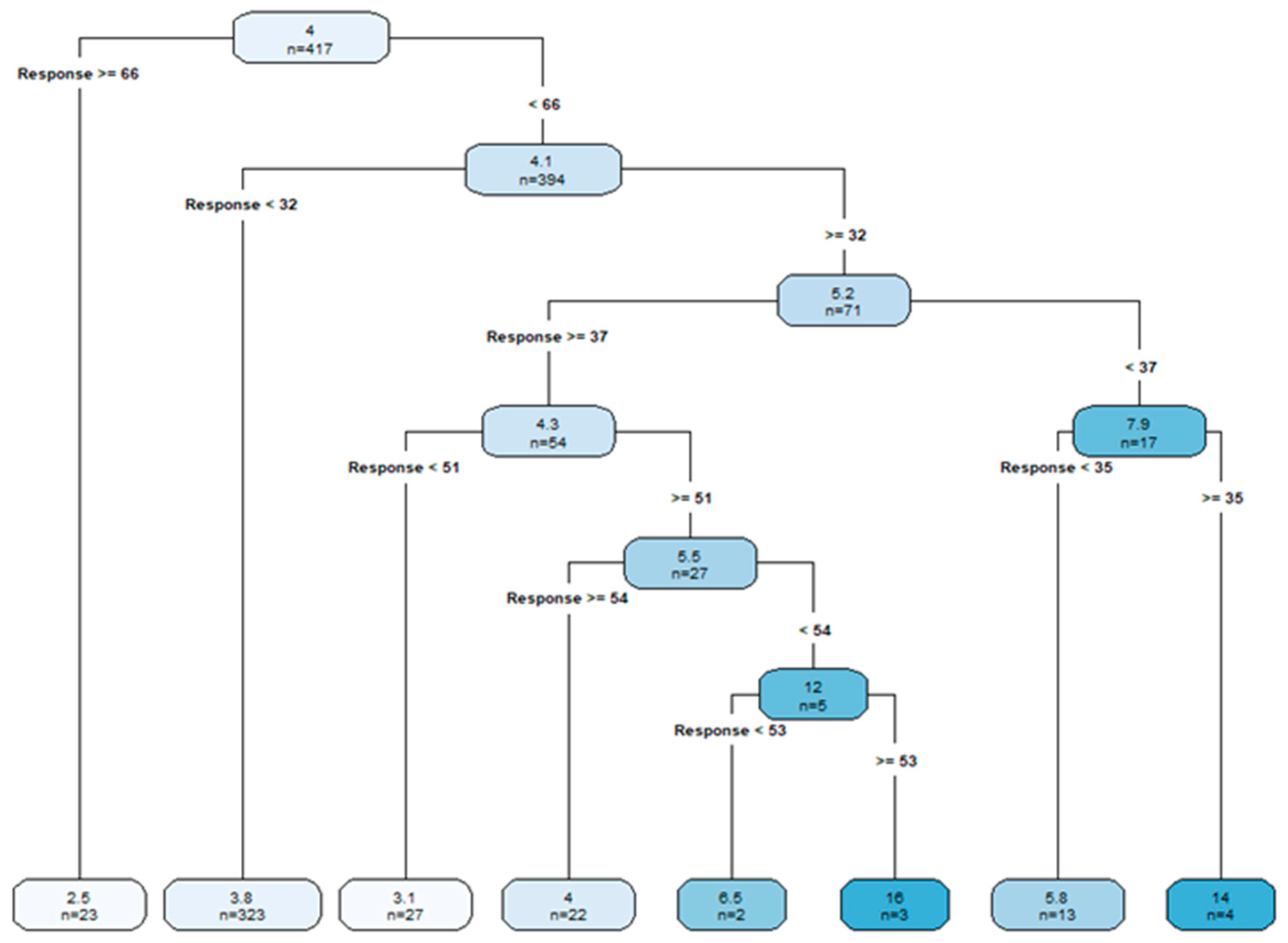
Figure 3.
Regression tree of LOS on the Scene time.
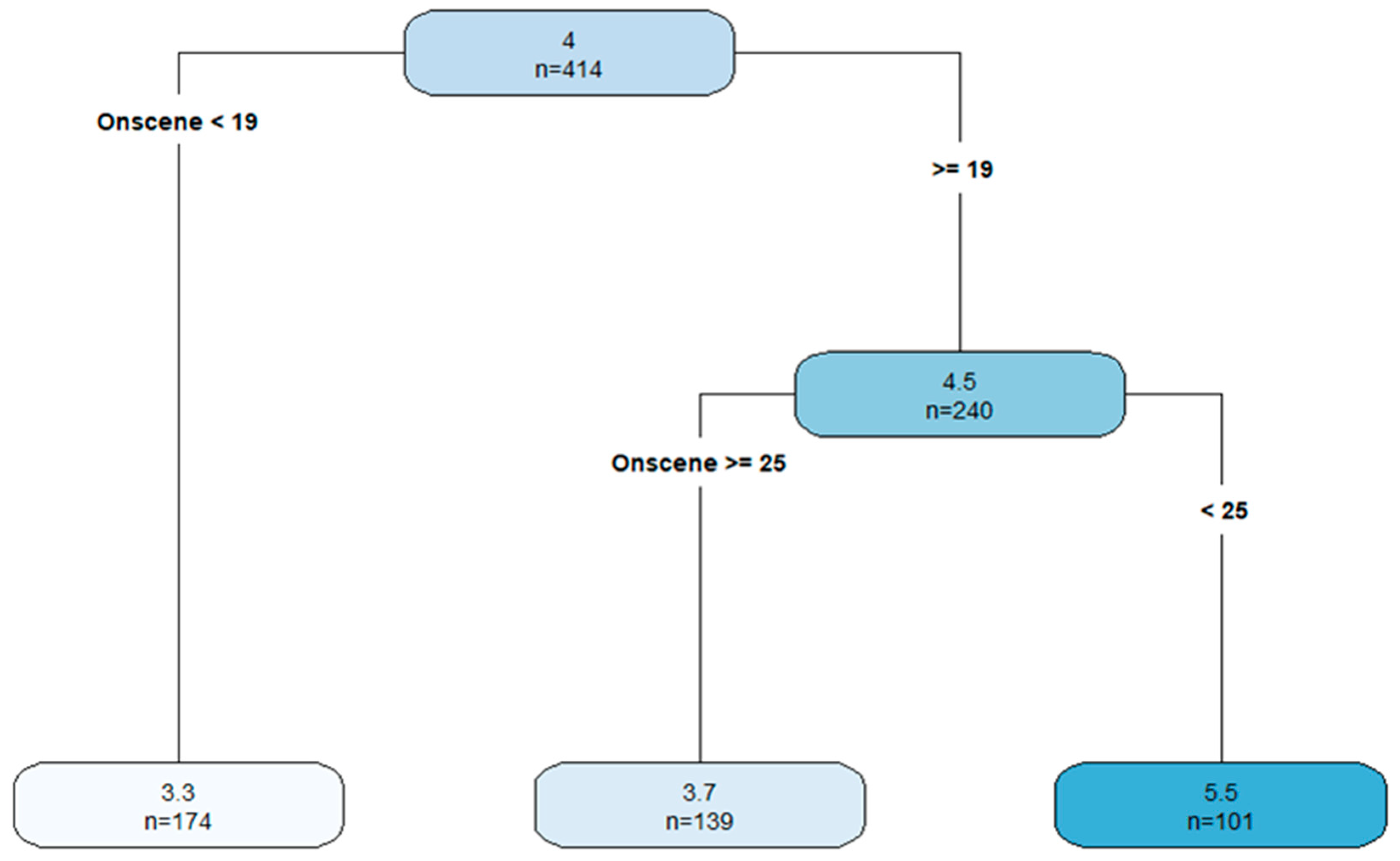
Figure 4.
Classification tree of operative intervention on total prehospital time.
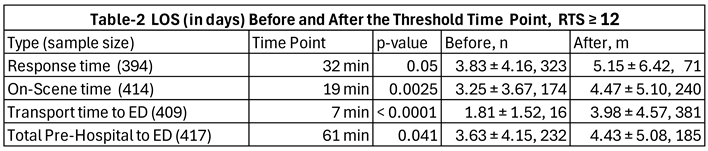 |
Table 3.
Rates of Operative Intervention with Splitting Time Point, RTS ≥ 12.
| Type of Time (N) | Time Point | p-value | Before point, n, x | After point, m, y |
| Response time (401) | 23 min | 0.3746 | 271, 70 | 130, 40 |
| On-Scene time (414) | 30 min | 0.2799 | 334, 90 | 80, 19 |
| Transport time (397) | 7 min | 0.0107 | 27, 2 | 370, 102 |
| Total Pre-Hospital to ED (417) | 76 min | 0.0119 | 274, 62 | 143, 47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



