Submitted:
12 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Background/Objectives: Inequality in survival across socioeconomic strata has been growing in the US for decades. Traditional measures of this inequality increasingly fail to capture the heterogeneous biological realities of the US population. Using new measures, this study provides a fresh perspective on the dynamics of mortality inequality across ten socioeconomic deciles in the United States from 1982 to 2019. Methods: Data: The data come from annual life tables from US counties, aggregated according to their socioeconomic characteristics. Measures of Inequality: Three measures of inequality are used, capturing survival inequality from different perspectives, inequality in ages of death over the lifecycle, inequality in survival at older ages, and inequality in survival in midlife. For the latter, the equal survivorship age (ESA)—a metric defined as the age at which a specific subgroup’s survival probability from age 20 matches the survival probability from age 20 to 65 of the total population—is used. Results: We find consistently growing inequality, largely unaffected by economic circumstances such as the Great Recession. By 2019, the ESA for the lowest socioeconomic decile was nearly 11 years lower than the ESA of the highest decile. Conclusions: This “survival gap” in the ESA suggests that low-socioeconomic status (SES) populations effectively exhaust their survival “budget” a decade earlier than their high SES counterparts. These findings challenge the equity of the use of universal chronological ages in public policies and underscore the need for “Social-Determinant-Adjusted” geriatric care models. The regularly growing inequality in the ESA suggests the importance of cohort-based influences.
Keywords:
survival inequality
; characteristics approach
; socioeconomic status
; county-based life tables
; deaths of despair
; weathering
; prospective age
; Human Life Indicator
1. Introduction
For nearly a century, the chronological age of 65 has served as the de facto threshold for “old age” in the United States, governing eligibility for Social Security, Medicare, and the focus of geriatric medicine. This uniform boundary assumes a relatively homogeneous aging process across the population. However, recent demographic data indicate that the United States is undergoing a “Great Divergence” in health outcomes, where gains in longevity are disproportionately accrued by the socioeconomically advantaged [1,2,3,4]. This paper applies the Characteristics Approach (CA) framework [5] to U.S. mortality data to challenge the utility of fixed chronological ages in studying heterogeneity in mortality. In a stratified society, a 65-year-old in the bottom strata may be biologically older—in terms of frailty and mortality risk—than a 75-year-old in the top one.
The study of mortality inequality over time in the US at the county level was based on earlier work in the UK [6,7]. Carstairs and Morris [7] studied mortality by geographic units in England, Scotland, and Wales around 1981, using a four-dimensional “deprivation score”. Based on that score, geographic units were divided into seven categories from lowest to highest deprivation score. Earnes et al. [6] built on the work of Carstairs and Morris, using three indices of deprivation and different geographic units. Earnes et al. found that their deprivation indices were closely related to all-source mortality as well as mortality from heart disease and from smoking.
In a series of articles, Singh and Siahpush [8,9] applied the UK methodology to US counties using an 11-factor deprivation index. They divided counties into deciles based on their index. Singh and Siahpush found that, for women in the lowest decile, life expectancy at birth was 1.3 years lower than for those in the highest decile in 1980-82, and fell to 3.3 years lower in 1998-2000. For men, the differences were 3.8 years and 5.4 years, respectively.
Dwyer-Lindgren et al. [10] studied county-level differences in life expectancy at birth from 1980 to 2014. Using principal components methodology, they produced three composite indices, representing socioeconomic race/ethnicity factors, behavioral and metabolic risk factors, and health care factors. The index for socioeconomic race/ethnicity factors included variables for race, ethnicity, education, and income. The index for behavioral and metabolic risk factors included variables for physical activity, obesity, smoking, hypertension, and diabetes prevalence. The index for health care factors included the percentage of the population under 65 insured, a health care quality index, and the number of physicians per 1,000 population. In a model of life expectancy at birth, the index for behavioral and metabolic risks and the index for health care were statistically significant, and the index for socioeconomic race/ethnicity factors was not. Adding both the socioeconomic race/ethnic index and health care index to a model with just an intercept and the behavioral and metabolic risk factors did not raise the adjusted R-squared. The conclusion is that the most important factors influencing life expectancy differences across counties were those associated with behavioral and metabolic risks.
Case and Deaton [3,4,11] studied the increasing inequality in health and survival in the US, focusing on the experiences of white non-Hispanics with only a high school education. In [12], they called the increasing deaths in midlife in that group “deaths of despair.” In [13], they looked at possible causes of the increasing divergence of the mortality rates of white non-Hispanics and other Americans, ranging from increasing income inequality to decreasing access to healthcare. They found that they were not a satisfactory explanation. They produced a tentative possible explanation that they labeled “cumulative disadvantage.” “Cumulative disadvantage” was said to be due to the continuing worsening of the labor market conditions of white non-Hispanics at the time of labor market entry. These worsening conditions had cumulative effects from less investment in human capital to less stable family structures.
Case and Deaton’s view of “cumulative disadvantage” is related to the “weathering” hypothesis [14,15], which posits that the cumulative stress of socioeconomic disadvantage accelerates cellular aging. This results in an earlier onset of chronic disease and frailty for low-SES individuals. Consequently, chronological age becomes a poor proxy for biological age, as the “biological clocks” of the rich and poor run at different speeds [16].
Data on life expectancy at birth reveal one dimension of inequality but hide another one. Life expectancy is the arithmetic average age at death in a life table population. Two arithmetic averages can be the same, but the variability in ages of death over the life cycle could be different. To address differences in the variability of ages of death, Ghislandi, Sanderson, and Scherbov [17] developed the Human Life Indicator (HLI). The HLI is the geometric mean of ages at death in a life table population. It reflects both the arithmetic average age at death and the variation in those ages. The difference between life expectancy at birth and the HLI is a measure of that variation. Larger variations in ages at death result in larger differences between life expectancy at birth and the HLI. An observation with a larger difference would reflect a case where deaths are more concentrated at the earliest and latest portions of the life cycle. An observation of a smaller difference would reflect a case where ages at death were more concentrated.
Van Raalte et al. [18] argues for the importance of studying the variability in ages at death (lifespan inequality) in addition to life expectancy. Sasson [19] showed how life expectancy and lifespan inequality (measured by the standard deviations in ages at death) changed in the US from 1990 to 2010 by educational attainment.
The traditional approach to the study of population aging is increasingly criticized for focusing on chronological age rather than functional ability [20]. Sanderson and Scherbov [5,21,22,23] introduced the concept of Prospective Age, recognizing that, in an environment of differential mortality rates, the definition of “old age” should not be fixed. They defined the Prospective Old-Age Threshold (POAT), a flexible lower bound on the onset of “old age”. It is the age at which the average remaining life expectancy first falls below 15 years. In contrast to a threshold based on a fixed chronological age, such as 65, this threshold of old-age varies across socio-economic conditions and over time. As populations become healthier, the POAT rises, signaling that the onset of “old age” is being delayed. The inequality in POATs expresses the inequality of the onset of “old age”.
2. Materials and Methods
2.1. Data
We utilized a longitudinal dataset of U.S. county life tables from 1982 to 2019, produced for the Society of Actuaries [24,25]. The methodology that was used to produce it was an extension of that in Singh [8,9]. A socioeconomic index score (SIS) is computed for each county in each year. The values of the SIS in 2000 are used to aggregate counties into deciles of equal population size in that year, and the distribution of counties into deciles is then fixed for the entire period (1=lowest, 10=highest, “All”=the total population).
The SIS is based on the normalized values of 11 variables:
1. Percentage of the population aged 25 and over with less than 9 years of education
2. Percentage of the population aged 25 and over with at least 4 years of college education
3. Percentage of the population aged 16 and over employed in a white-collar occupation
4. Unemployment rate for the population 16 years and over
5. Median household income adjusted for local housing costs
6. Ratio of the average household income in the lowest quintile to the average household income in the highest quintile
7. Percentage of the population below the federal poverty threshold
8. Median home value for owner-occupied units
9. Median gross rent for rental units
10. Percentage of housing without a telephone
11. Percentage of housing without complete plumbing
The normalized values are combined based on weights derived from a principal components analysis.
County-level mortality data are derived from the National Center for Health Statistics, and county-level population distributions are derived from the US Decennial Census and the American Community Survey. The methodology of producing life tables using these data is the same as that used to produce the life tables in the Human Mortality Database. This permits the US data to be analyzed in an international perspective. The full description of the methodology used to produce the life tables can be found in [25].
2.2. Key Measures
We employ three measures of population aging that account for heterogeneity: the Human Life Indicator (HLI), the Prospective Old Age Threshold (POAT), and the Equal Survivalship Age (ESA). The HLI measures survival over the lifecycle. The POAT measures survival rates at older ages, and the ESA shows the heterogeneity of survival rates in midlife.
2.2.1. Human Life Indicator (HLI)
Life expectancy at birth is the arithmetic average of ages at death in a life table population. The HLI is the geometric average of ages at death in a life table population. We use it to detect heterogeneity that is manifested as increases in lifespan inequality. When the age pattern of deaths shifts so that the variance in the age at death increases, the HLI falls relative to life expectancy at birth.
2.2.2. Prospective Old-Age Threshold (POAT)
The age x where remaining life expectancy is 15 years:
In standard life table notation:
e(x) = 15 years.
We use the POAT to assess trends in the heterogeneity of aging at older ages.
2.2.3. Equal Survivorship Age (ESA)
We introduce this measure here to assess changes in the pattern of survival rate changes for people in midlife. It is the age in the population under study at which the probability of surviving from age 20 to that age is the same as the probability of surviving from age 20 to age 65 in the aggregate population of the same year (the total population in all the deciles). Because it is benchmarked against a moving national standard, the ESA provides a detrended measure of inequality across the deciles.
In standard life table notation, the ESA for decile d in year t is x where
where is the proportion of the life table population of decile d in year t that survives to age x, and is the proportion of the life table population of the US in year t that survives to age x..
3. Results
3.1. Inequality Over the Lifecycle
The “Great Divergence” is clearly visible in Figure 1 below. For clarity, in all our Figures, we show only the lowest and the highest decile for both sexes combined. In 1982, the gap in life expectancy at birth between Decile 1 (72.9 years) and Decile 10 (75.8 years) was roughly 3 years. By 2019, this gap widened to 6.6 years, with life expectancy in decile 10 reaching 82.4 years while Decile 1 increased more slowly to 75.8 years. Between 2010 and 2019, life expectancy at birth for the entire population stagnated. The stagnation in life expectancy growth observed in the aggregate was a result of life expectancy at birth falling for the least advantaged groups, increasing for the most advantaged, and remaining little changed for the groups in the middle.
Conceptually, the Human Life Indicator (HLI) is life expectancy at birth adjusted for the inequality in the age pattern of deaths. The difference between life expectancy at birth and the HLI provides a measure of that inequality. We show those differences in Figure 2. The difference between life expectancy at birth and the HLI tends to decrease over time for all the deciles, indicating increasing mortality compression. The differences between the first and tenth declines remained roughly constant. There was essentially little change over time in the inequality in lifespan variation across the socioeconomic groups.
3.2. The Divergence in Mortality at Older Ages
We use the POAT to assess inequality in mortality conditions at older ages. In previous work, we have shown that the POAT can be used as a temporally and spatially consistent threshold that distinguishes “older adults” from younger ones [5]. Figure 3 shows the evolution of the POATs. Over time, the POATs show increasing inequality. This divergence is almost completely accounted for by changes from 1982 to 2010. POATs increased from 2010 to 2019, but without any notable further divergence.
3.3. The Divergence in Mortality in Midlife
We present ESAs in Figure 4, and use them to assess the divergence of survival rates in midlife. The ESA is a detrended measure so that stable inequality would appear as parallel lines in that Figure. Instead, the lines diverge relatively consistently, without any clear change in the 2010-2019 period. Figure 4 presents a picture of a persistent growth of inequality that has little year-to-year variation.
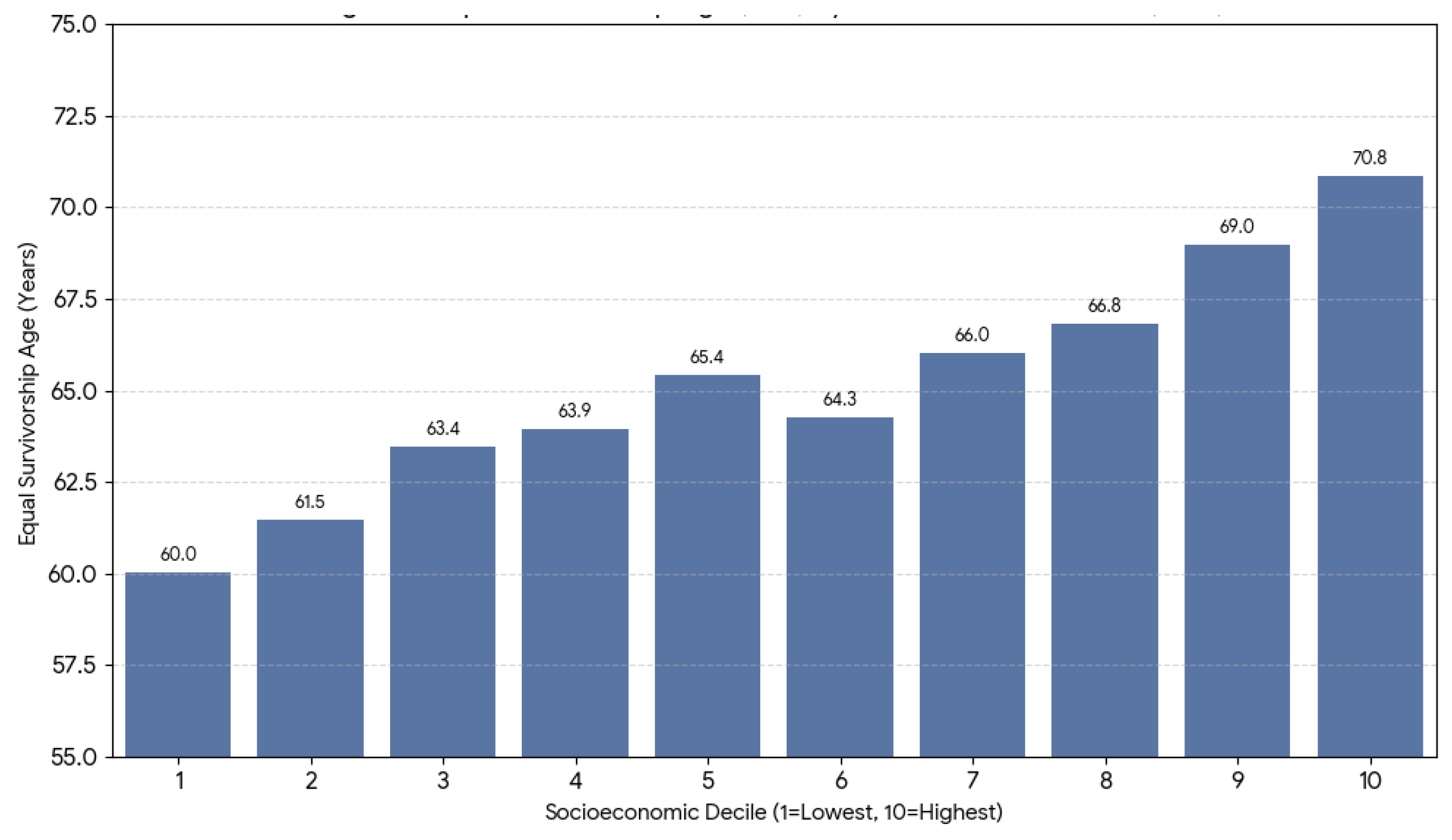
Figure 5 shows the ESA for all ten deciles in 2019. People at all the ages had the same probability of surviving from age 20. For example, people in decile 1 had the same probability of surviving from age 20 to age 60.0 as people in decile 10 had of surviving from age 20 to age 70.8.
4. Discussion
4.1. Policy Implications: The Regressivity of Retirement
The Social Security reform in the US that resulted in the increase in the normal pension age from 65 to 67 occurred in 1983 [26]. The ESA shows much smaller disparities across the socioeconomic deciles in that year. With the records and demographic methods at that time, it would have been difficult to predict what would happen. Now, the almost 11-year gap in the Equal Survivorship Age (ESA) exposes the increasingly regressive nature of raising the federal retirement age. Current proposals to increase the eligibility age are often justified by the “average” increase in life expectancy. However, our data shows that for Decile 1, the “biological” retirement age—adjusted for survival risk—is effectively 60. Raising the chronological threshold disproportionately penalizes low-SES workers who have already exhausted their “survival budget” well before reaching the current cutoff.
4.2. Clinical Implications: Social-Determinant-Adjusted Geriatrics
The POAT data suggest that the onset of “old age” (defined by remaining years of life) occurs nearly 3 years earlier for the poor than the rich (70.3 vs. 73.0 for both sexes combined). However, the ESA suggests the “frailty gap” is much wider. Geriatricians should consider SES as a vital sign. Screening for geriatric syndromes (falls, dementia, sarcopenia) should begin earlier for patients in lower socioeconomic deciles, as their “biological age” significantly outpaces their chronological age.
4.3. Research Implications: Modeling Persistently Growing Inequality in Midlife
The ESA shows persistent increases in survival in the midlife. Explanations of this persistence must include factors where inequality also persistently increases. Education and income are factors commonly associated with longevity. This does not necessarily mean that education and income are factors associated with regularly increasing survival inequality seen in midlife. Income inequality does not change smoothly from year to year. The effects of the dot-com bust in 2000-2002 and the Great Recession in 2008-2009 are barely visible in the ESA figures. It is also unclear what role education plays in the persistent increases in the ESAs.
The persistent and comparatively regular increases in the ESAs favor considering cohort-based explanations such as Case and Deaton’s cumulative disadvantage hypothesis or Geronimus’ weathering hypothesis. Both of these require thinking about the determinants of survival differences in a dynamic context, and this requires new modeling that goes beyond studying the influences on survival rates at a moment in time.
5. Conclusions
The United States is not aging as a single unit. While the wealthy enjoy a “longevity revolution” characterized by delayed aging and high survival certainty, the poor face a “longevity stagnation.” The introduction of the Equal Survivorship Age (ESA) clarifies this disparity: the poorest Americans are effectively running a longer race with a shorter timeline. To achieve health equity, we must move beyond the “myth of the average” and adopt flexible, prospective age thresholds in both clinical practice and social policy.
Author Contributions
Conceptualization, W.S. and S.S.; methodology, W.S. and S.S.; software, W.S. and S.S.; validation, W.S. and S.S.; formal analysis, W.S. and S.S.; data curation, W.S. and S.S.; writing—original draft preparation, W.S. and S.S.; writing—review and editing, W.S. and S.S.; visualization, W.S. and S.S. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data used in this study can be found at https://www.soa.org/resources/research-reports/2020/us-mort-rate-socioeconomic/. Graphs were produced using Microsoft Excel.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HLI | Human Life Indicator |
| POAT | Prospective Old Age Threshold |
| ESA | Equal Survivorship Age |
| CA | Characteristics Approach to the Study of Population Aging |
References
- Chetty, R.; Stepner, M.; Abraham, S.; Lin, S.; Scuderi, B.; Turner, N.; Bergeron, A.; Cutler, D. The Association Between Income and Life Expectancy in the United States, 2001-2014. JAMA 2016, 315, 1750–1766. [CrossRef]
- Dwyer-Lindgren, L.; Baumann, M.M.; Li, Z.; Kelly, Y.O.; Schmidt, C.; Searchinger, C.; Motte-Kerr, W.L.; Bollyky, T.J.; Mokdad, A.H.; Murray, C.J. Ten Americas: A Systematic Analysis of Life Expectancy Disparities in the USA. The Lancet 2024, 404, 2299–2313. [CrossRef]
- Case, A.; Deaton, A. Mortality and Morbidity in the 21st Century. Brookings Pap Econ Act 2017, 2017, 397–476.
- Case, A.; Deaton, A. The Great Divide: Education, Despair, and Death. Annual Review of Economics 2022, 14, 1–21. [CrossRef]
- Sanderson, W.C.; Scherbov, S. Prospective Longevity: A New Vision of Population Aging; Harvard University Press: Cambridge, MA, 2019;
- Eames, M.; Ben-Shlomo, Y.; Marmot, M.G. Social Deprivation and Premature Mortality: Regional Comparison across England. BMJ 1993, 307, 1097–1102. [CrossRef]
- Carstairs, V.; Morris, R. Deprivation: Explaining Differences in Mortality between Scotland and England and Wales. BMJ 1989, 299, 886–889. [CrossRef]
- Singh, G.K.; Siahpush, M. Widening Socioeconomic Inequalities in US Life Expectancy, 1980–2000. Int J Epidemiol 2006, 35, 969–979. [CrossRef]
- Singh, G.K.; Siahpush, M. Widening Rural–Urban Disparities in Life Expectancy, U.S., 1969–2009. American Journal of Preventive Medicine 2014, 46, e19–e29. [CrossRef]
- Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Mackenbach, J.P.; van Lenthe, F.J.; Mokdad, A.H.; Murray, C.J.L. Inequalities in Life Expectancy Among US Counties, 1980 to 2014: Temporal Trends and Key Drivers. JAMA Intern Med 2017, 177, 1003–1011. [CrossRef]
- Case, A.; Deaton, A. Rising Morbidity and Mortality in Midlife among White Non-Hispanic Americans in the 21st Century. Proc Natl Acad Sci USA 2015, 112, 15078–15083. [CrossRef]
- Case, A.; Deaton, A. Rising Morbidity and Mortality in Midlife among White Non-Hispanic Americans in the 21st Century. Proc Natl Acad Sci USA 2015, 112, 15078–15083. [CrossRef]
- Case, A.; Deaton, A. Mortality and Morbidity in the 21st Century. Brookings Pap Econ Act 2017, 2017, 397–476. [CrossRef]
- Geronimus, A.T.; Hicken, M.; Keene, D.; Bound, J. “Weathering” and Age Patterns of Allostatic Load Scores Among Blacks and Whites in the United States. Am J Public Health 2006, 96, 826–833. [CrossRef]
- Geronimus, A.T.; Bound, J.; Waidmann, T.A.; Rodriguez, J.M.; Timpe, B. Weathering, Drugs, and Whack-a-Mole: Fundamental and Proximate Causes of Widening Educational Inequity in U.S. Life Expectancy by Sex and Race, 1990–2015. J Health Soc Behav 2019, 60, 222–239. [CrossRef]
- Crimmins, E.M.; Beltrán-Sánchez, H. Mortality and Morbidity Trends: Is There Compression of Morbidity? J Gerontol B Psychol Sci Soc Sci 2011, 66B, 75–86. [CrossRef]
- Ghislandi, S.; Sanderson, W.C.; Scherbov, S. A Simple Measure of Human Development: The Human Life Indicator. Population and Development Review 2019. [CrossRef]
- Raalte, A.A. van; Sasson, I.; Martikainen, P. The Case for Monitoring Life-Span Inequality. Science 2018, 362, 1002–1004. [CrossRef]
- Sasson, I. Trends in Life Expectancy and Lifespan Variation by Educational Attainment: United States, 1990–2010. Demography 2016, 53, 269–293. [CrossRef]
- WHO World Report on Ageing and Health 2015; World Health Organization: Geneva, Switzerland, 2015;
- Sanderson, W.C.; Scherbov, S. The Characteristics Approach to the Measurement of Population Aging. Popul. Dev. Rev. 2013, 39, 673–685. [CrossRef]
- Sanderson, W.C.; Scherbov, S. Measuring the Speed of Aging across Population Subgroups. PLoS ONE 2014, 9, e96289. [CrossRef]
- Sanderson, W.C.; Scherbov, S. Average Remaining Lifetimes Can Increase as Human Populations Age. Nature 2005, 435, 811–813. [CrossRef]
- Barbieri, M. Socioeconomic Disparities Do Not Explain the U.S. International Disadvantage in Mortality. The Journals of Gerontology: Series B 2022, 77, S158–S166. [CrossRef]
- Barbieri, M. Mortality by Socioeconomic Category in the United States.
- Social Security History Available online: https://www.ssa.gov/history/1983amend.html (accessed on 25 January 2026).
Figure 1.
Trends in Life Expectancy at Birth by Socioeconomic Decile (1982–2019). This figure illustrates the “Great Divergence” in longevity between the highest socioeconomic decile (Decile 10), the lowest decile (Decile 1), and the total U.S. population. While the national average and the top decile show significant gains in life expectancy over nearly four decades, the bottom decile exhibits relative stagnation, resulting in a gap between the deciles that widened from 2.8 years in 1982 to 6.6 years by 2019.
Figure 1.
Trends in Life Expectancy at Birth by Socioeconomic Decile (1982–2019). This figure illustrates the “Great Divergence” in longevity between the highest socioeconomic decile (Decile 10), the lowest decile (Decile 1), and the total U.S. population. While the national average and the top decile show significant gains in life expectancy over nearly four decades, the bottom decile exhibits relative stagnation, resulting in a gap between the deciles that widened from 2.8 years in 1982 to 6.6 years by 2019.
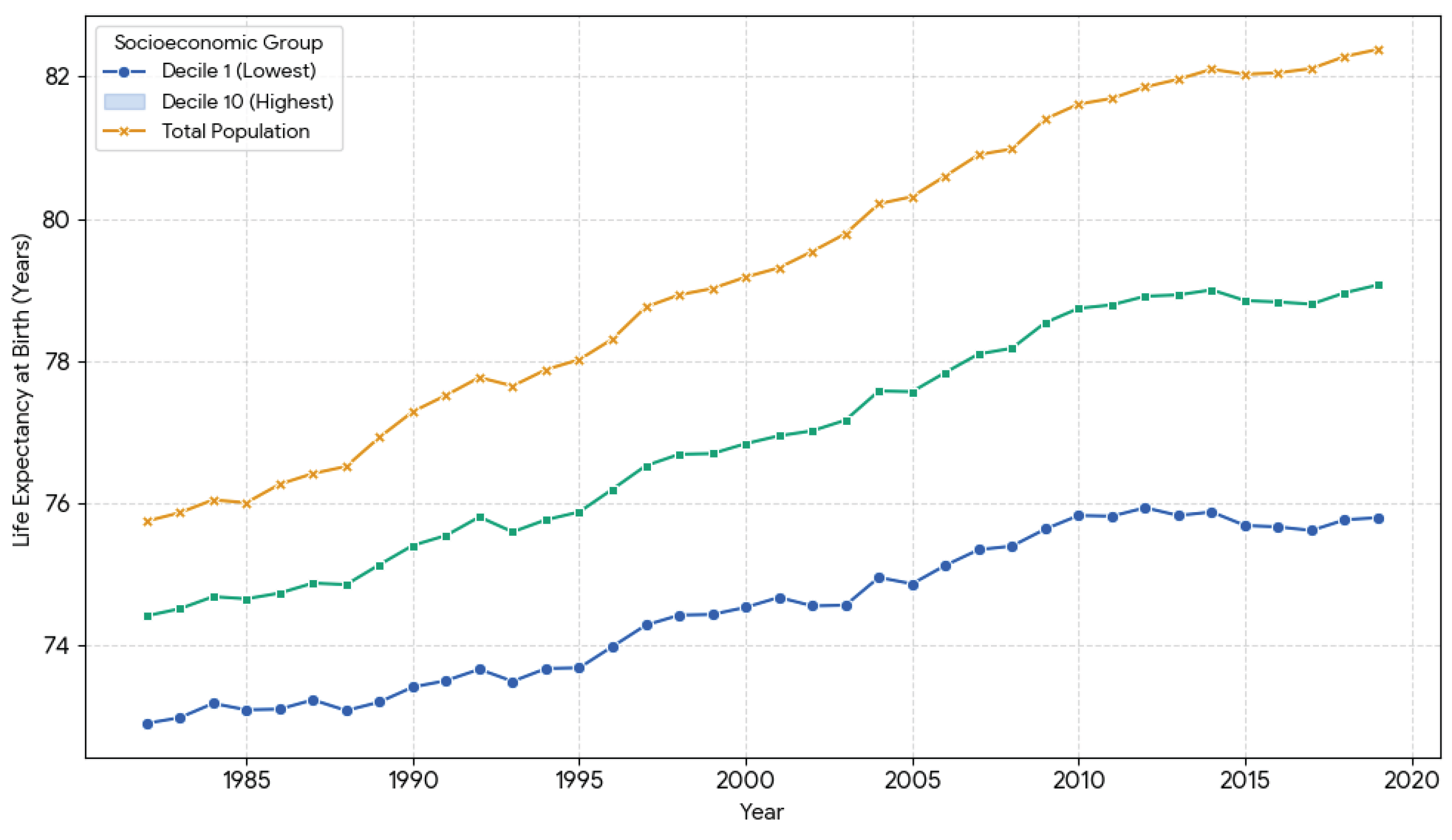
Figure 2.
Temporal Trends in Longevity Inequality (life expectancy at birth minus HLI) (1982–2019). Longevity inequality is measured here as the difference between life expectancy at birth (e0) and the Human Life Indicator (HLI). The Figure shows little change in inequality over time.
Figure 2.
Temporal Trends in Longevity Inequality (life expectancy at birth minus HLI) (1982–2019). Longevity inequality is measured here as the difference between life expectancy at birth (e0) and the Human Life Indicator (HLI). The Figure shows little change in inequality over time.
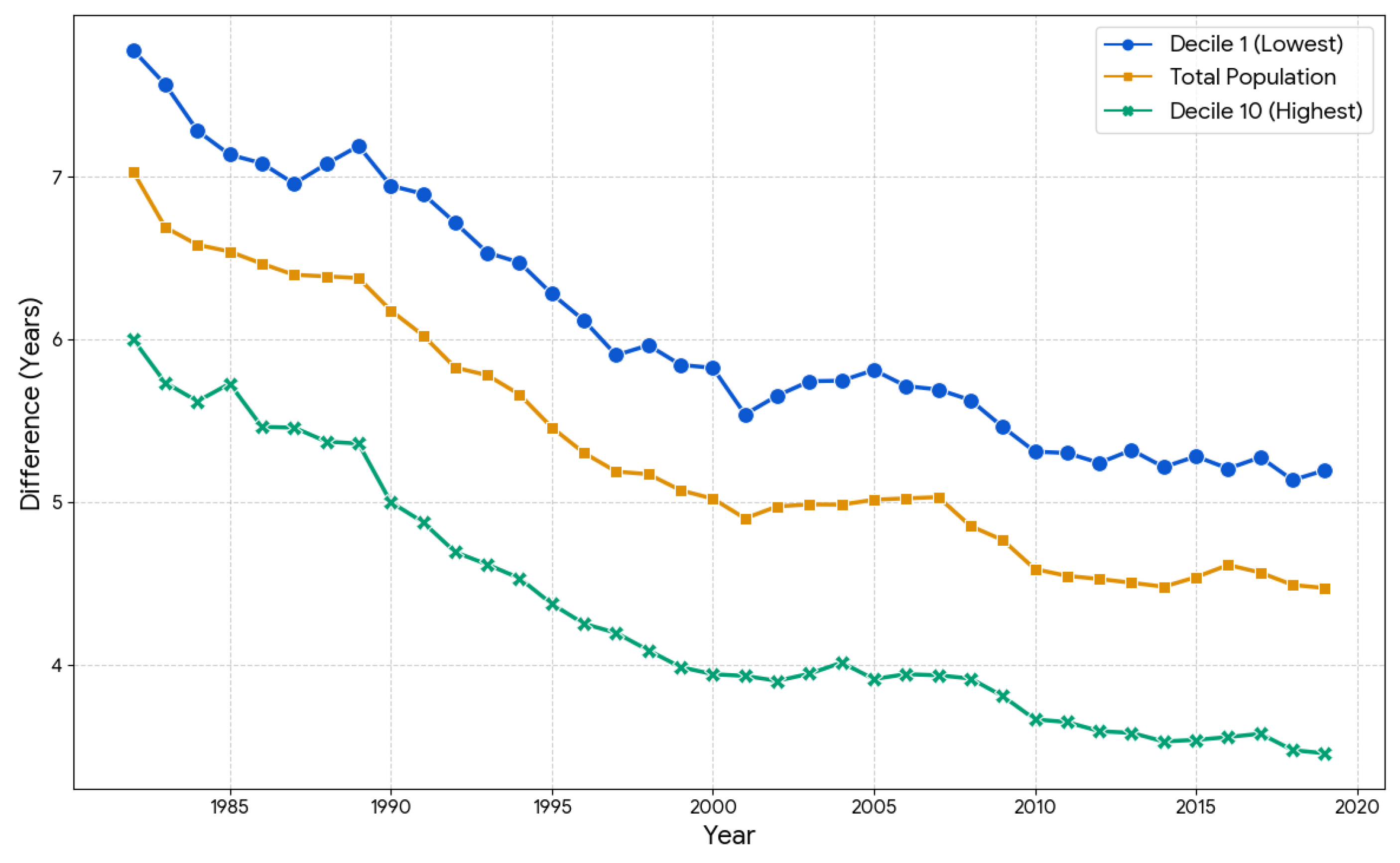
Figure 3.
Evolution of the Prospective Old-Age Threshold (POAT) by Socioeconomic Status (1982–2019). Following the Sanderson-Scherbov framework, the POAT represents the age at which remaining life expectancy is exactly 15 years. This chart shows the “prospective rejuvenation” of the elite, whose old-age threshold has risen toward age 73. In contrast, the threshold for Decile 1 has risen much more slowly, indicating that disadvantaged populations are biologically “older” at younger chronological ages.
Figure 3.
Evolution of the Prospective Old-Age Threshold (POAT) by Socioeconomic Status (1982–2019). Following the Sanderson-Scherbov framework, the POAT represents the age at which remaining life expectancy is exactly 15 years. This chart shows the “prospective rejuvenation” of the elite, whose old-age threshold has risen toward age 73. In contrast, the threshold for Decile 1 has risen much more slowly, indicating that disadvantaged populations are biologically “older” at younger chronological ages.
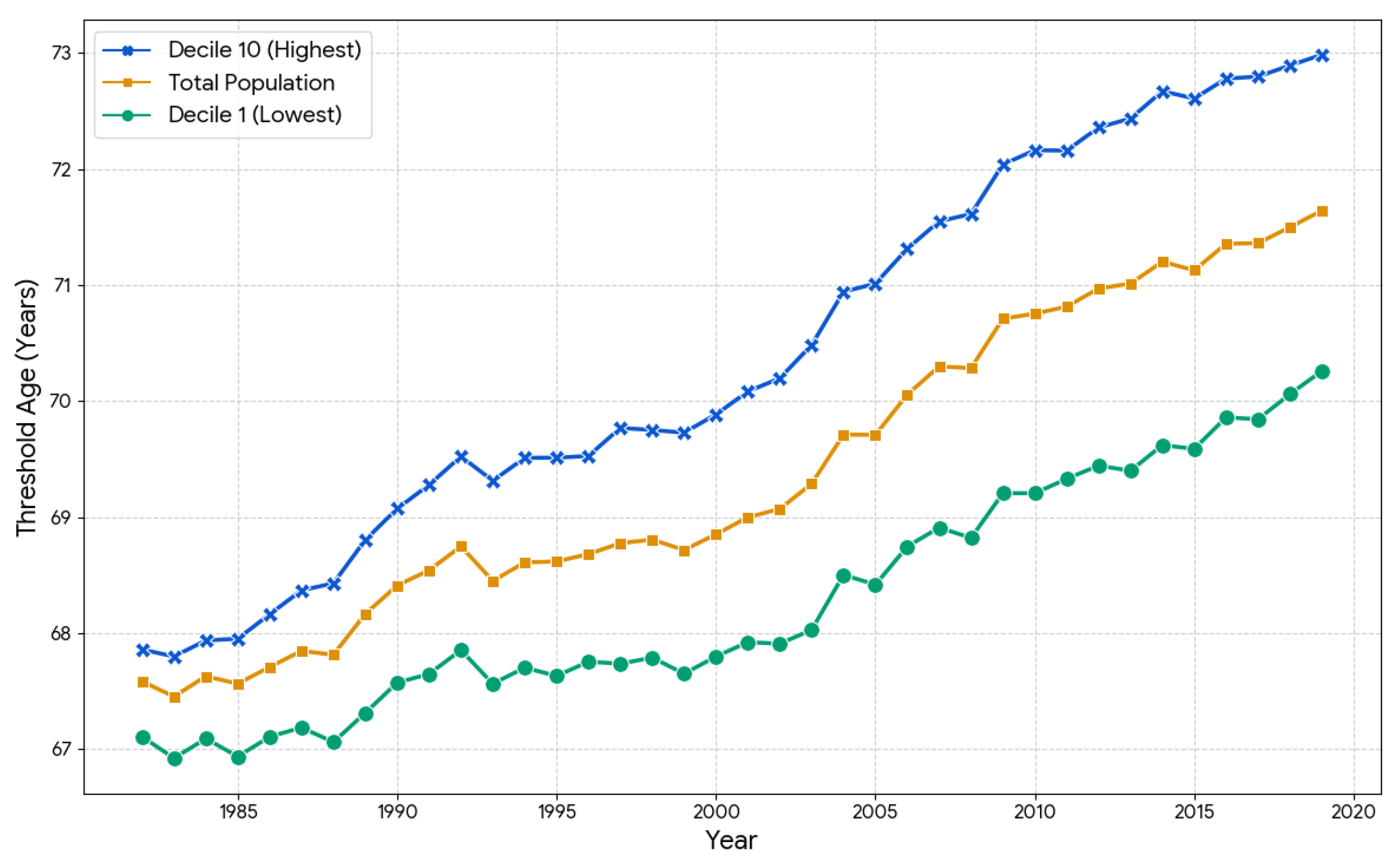
Figure 4.
Divergence of the Equal Survivorship Age (ESA) from the National Benchmark (1982–2019). This figure tracks the ESA over time, using the total population survival probability to age 65 as a fixed benchmark (represented by the horizontal “Total Population” line at 65.0). The chart highlights a critical social divergence: since 1982, the highest decile has gained nearly four years of survival parity, while the lowest decile has seen its survival parity regress from age 63 to age 60, intensifying the socioeconomic “survival tax” during midlife.
Figure 4.
Divergence of the Equal Survivorship Age (ESA) from the National Benchmark (1982–2019). This figure tracks the ESA over time, using the total population survival probability to age 65 as a fixed benchmark (represented by the horizontal “Total Population” line at 65.0). The chart highlights a critical social divergence: since 1982, the highest decile has gained nearly four years of survival parity, while the lowest decile has seen its survival parity regress from age 63 to age 60, intensifying the socioeconomic “survival tax” during midlife.
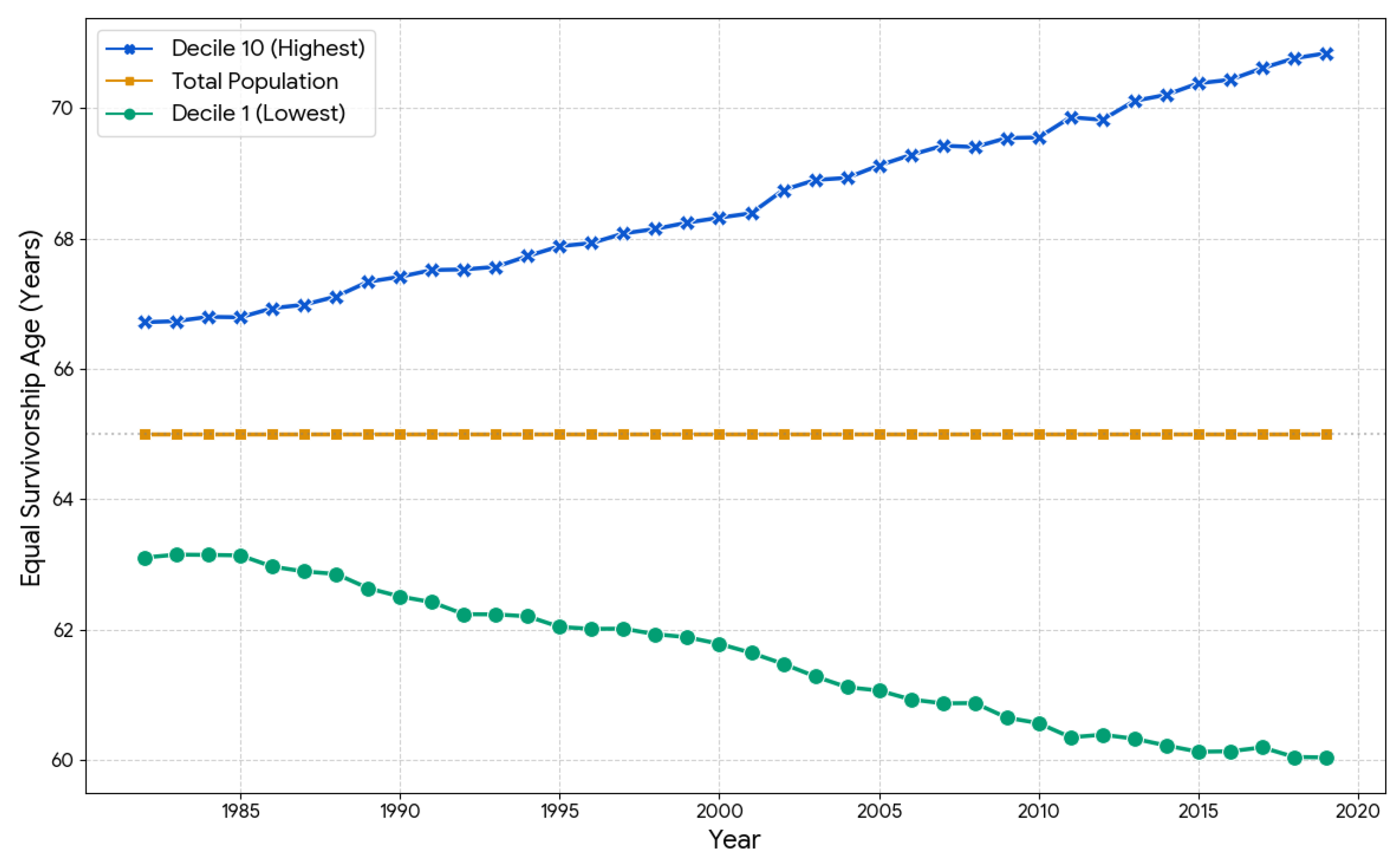
Figure 5.
Gradient of the Equal Survivorship Age (ESA) Across Socioeconomic Deciles (2019). The bar chart displays the ESA for each decile, representing the chronological age at which that group reaches the same survival probability (from age 20) as the national average at age 65. The nearly 11-year gap between Decile 1 (60.0 years) and Decile 10 (70.8 years) demonstrates that individuals in the lowest socioeconomic strata exhaust their “survival budget” more than a decade earlier than those in the highest strata.
Figure 5.
Gradient of the Equal Survivorship Age (ESA) Across Socioeconomic Deciles (2019). The bar chart displays the ESA for each decile, representing the chronological age at which that group reaches the same survival probability (from age 20) as the national average at age 65. The nearly 11-year gap between Decile 1 (60.0 years) and Decile 10 (70.8 years) demonstrates that individuals in the lowest socioeconomic strata exhaust their “survival budget” more than a decade earlier than those in the highest strata.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



