
Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Organ-on-a-Chip (OOC) technologies, also termed microphysiological systems (MPS), integrate microfluidics, engineered biomaterials, human-derived cells, and on-chip biosensing to model human physiology in microscale devices that deliver quantitative, time-resolved readouts. This review surveys the 2010–2025 literature, emphasizing how sensing, standardized sampling, and analytics enable clinical concordance and fit-for-purpose regulatory use. We synthesize advances in (i) materials, fabrication, and microfluidic design; (ii) organ- and disease-focused case studies; and (iii) translational benchmarks that align chip outputs with clinical pharmacokinetics, toxicology, and biomarker datasets. Across organ systems, platforms increasingly incorporate vascularization, immune components, and organoid hybrids, paired with real-time measurements of barrier integrity, metabolism, electrophysiology, and secreted biomarkers using impedance (TEER), electrochemical, and optical modalities. Representative benchmarking studies report cardiac OOCs achieving AUROC ≥0.85 for torsadogenic risk classification and renal chips improving prediction of transporter-mediated clearance relative to conventional in vitro assays. We summarize validation approaches and regulatory developments relevant to new approach methodologies, including the FDA Modernization Act 2.0, and discuss how AI and multi-omics can automate signal and image analysis, harmonize cross-platform datasets, and support digital-twin workflows that couple OOC measurements to in silico models. Overall, biosensor-enabled OOCs are progressing toward quantitatively benchmarked platforms for safety pharmacology, ADME/PK–PD, and precision medicine.
Keywords:
Organ-on-a-Chip
; microphysiological systems
; microfluidics
; biosensors
; validation
; artificial intelligence
; multi-omics
; precision medicine
1. Introduction
The process of drug discovery and development remains long, costly, and inefficient. The average cost of bringing a new therapeutic to market now exceeds USD 2 billion [1], largely due to the high attrition rate in which more than 90% of candidates entering human clinical trials ultimately fail [2,3]. Despite advances in computational modeling, combinatorial chemistry, and high-throughput screening, translation of preclinical findings into successful clinical outcomes remains limited [3].
A central reason lies in the shortcomings of conventional preclinical models, both in physiological relevance and in the quality and decision-readiness of measurements they produce. Two-dimensional (2D) cell cultures are inexpensive, reproducible, and widely used, yet they lack tissue-level architecture, biochemical gradients, and biomechanical cues [4,5,6]. These oversimplifications yield drug-response data that often fail to predict organ-level toxicities or clinical efficacy, and they typically rely on sparse end-point assays with limited capacity for continuous, non-destructive monitoring. Animal models, while more complex, exhibit significant species differences in pharmacokinetics, immunology, and disease mechanisms [7,8,9,10]. These discrepancies, combined with ethical imperatives to reduce animal use, have accelerated the search for predictive and humane alternatives [11,12]. A concise comparison of conventional 2D cell cultures, animal models, and OOC platforms is summarized in Table 1.
Recent regulatory and computational advances have reinforced this paradigm shift. The U.S. FDA Modernization Act 2.0 has explicitly opened the door for qualified non-animal methods in preclinical safety assessment [16], while emerging technical frameworks for “new approach methodologies” (NAMs) emphasize standardization, quantitative performance metrics, and fitness-for-purpose criteria [17]. In parallel, artificial intelligence (AI) and machine learning (ML) are being embedded into OOC workflows to automate image and signal analysis, fuse multi-omics datasets, and link in vitro readouts to in vivo pharmacokinetics/pharmacodynamics (PK/PD) and clinical endpoints [18]. Together, these developments suggest that OOC platforms can evolve from experimental curiosities into decision-relevant tools in defined contexts of use, particularly when supported by (i) transparent evidence-generation plans, (ii) quantitative benchmarking against clinical references, and (iii) measurement strategies that account for data quality considerations (e.g., calibration, drift, and reproducibility) alongside biological fidelity.
Figure 1 provides an overview of the OOC landscape, illustrating the interplay among core engineering choices (materials, microfluidic architectures, and sensing), biological inputs (primary cells, iPSCs, organoids, and immune components), and analytical and regulatory layers that determine translational impact.
Beyond addressing limitations of traditional models, OOC research has evolved rapidly over the past two decades through advances in materials, fabrication, and biological integration. Early prototypes established feasibility, whereas contemporary platforms are increasingly evaluated for scalability, reproducibility, and regulatory relevance. Table 2 outlines key milestones marking this evolution, from the advent of microfluidics to current efforts in standardization, NAM-aligned performance frameworks, and AI-enabled analytics supporting clinical concordance. Although prior reviews have examined specific aspects of OOC research, such as materials and fabrication [14,15], microfluidics [13,14], or individual organ systems [19,20,21,22,23], fewer have integrated these technological dimensions with translational and regulatory frameworks [16,17] and with AI- and multi-omics–ready measurement outputs that enable quantitative benchmarking and decision readiness [18]. This review addresses that gap by (i) evaluating advances in materials, fabrication, microfluidic control, and sensing-compatible design; (ii) surveying representative organ models across vascular, pulmonary, gastrointestinal, neurological, cardiac, renal, hepatic, cutaneous, and tumor systems, including organoid-on-chip hybrids; and (iii) highlighting how validation frameworks, quantitative benchmarks, AI-enabled analytics, and regulatory pathways are shaping adoption. By linking device-level design choices to data quality, analytically interpretable readouts, and clinical concordance, we position OOCs as potentially decision-impactful tools for safety pharmacology, ADME, and precision medicine.
2. Core Technologies: Engineering a Micro-Physiological World
The ability of Organ-on-a-Chip (OOC) platforms to emulate human physiology depends on four tightly coupled engineering layers: (i) materials, which define biocompatibility, sorption, gas and solute transport, and optical/electrical properties; (ii) fabrication methods, which control feature size, channel geometry, bonding, and scalability; (iii) microfluidic design, which regulates perfusion, shear stress, recirculation, and spatiotemporal gradients; and (iv) integrated biosensing and data acquisition, which convert tissue behavior into time-resolved signals that can be benchmarked, modeled, and ultimately used for decisions [13,14,15,24,25,34,35,36,37]. Iterative advances across these domains have transformed early proof-of-concept devices into increasingly standardized, manufacturable systems that can be integrated with automation, sensing, and data-analytic pipelines [14,15,34,37,38]. In this section, we highlight key material options, fabrication workflows, microfluidic strategies, and measurement considerations that underpin contemporary OOC and microphysiological system (MPS) platforms and influence translational performance.
2.1. Materials: The Foundation of the Chip
Material choice governs biological fidelity, reproducibility, manufacturability, and, critically for translational use, the integrity of measured signals and the stability of test compounds within the device. Key requirements include biocompatibility, suitable mechanical stiffness, controlled gas and solute permeability, optical transparency for imaging, low autofluorescence, limited sorption of hydrophobic molecules, and compatibility with microfabrication, bonding, and sensor integration [13,34,35]. No single material satisfies all constraints; instead, OOC devices increasingly use application-specific combinations of polymers, elastomers, hydrogels, and membranes [34,35,39].
- Polydimethylsiloxane (PDMS). PDMS remains widely used due to its elasticity, transparency, and gas permeability [13,34,36]. Its use enabled landmark devices such as the first lung-on-a-chip, where cyclic strain simulated breathing motions [19]. However, PDMS can absorb hydrophobic drugs and small molecules, introducing variability in pharmacokinetic assays and complicating quantitative interpretation of dose–response behavior [36,39]. Surface modifications (plasma treatment, coatings, copolymers) can reduce absorption but may compromise reproducibility or introduce additional variability over long culture durations [34,35,39].
- Thermoplastics. Polystyrene, polycarbonate, and cyclic olefin copolymer (COC) provide chemically inert, mass-producible alternatives [34,35,40,41]. These materials are compatible with industrial injection molding and hot embossing, allowing reproducible manufacturing at scale [34,40,41]. Their reduced drug absorption can improve PK/PD interpretability, though limited gas permeability necessitates oxygenation strategies for highly metabolic tissues [34,40,41]. Thermoplastics also facilitate standardized interfaces (ports, footprints) that support automation and consistent sensor placement across batches [40,41].
- Hydrogels and ECM mimics. Hydrogels such as collagen, fibrin, gelatin methacrylate (GelMA), and polyethylene glycol (PEG) mimic extracellular matrix (ECM) stiffness and biochemical signaling [35,42,43]. They enable 3D morphogenesis, barrier formation, and immune–epithelial crosstalk. Hybrid ECM–organoid constructs have recently been combined with microfluidics to create organoid-on-chip hybrids with higher physiological fidelity and improved long-term function [42,43]. For measurement-rich workflows, hydrogel composition and remodeling kinetics can also influence diffusion and analyte transport, shaping both biological behavior and sensor readouts.
- Hybrid and smart materials. Multi-material composites and stimuli-responsive polymers enable dynamic tuning of stiffness or porosity [34,35,42,43]. Light- or pH-responsive substrates have been applied to mimic dynamic tissue states and trigger on-demand drug release or matrix remodeling within OOCs [34,42]. These hybrid systems aim to couple mechanical and biochemical fidelity with controlled, quantifiable perturbations that can be tracked using integrated assays.
- Glass. Glass substrates offer exceptional optical clarity, chemical resistance, and low drug absorption, making them attractive for imaging-intensive applications such as blood–brain barrier and neural models [13,34,35]. Limitations include brittleness and challenges for low-cost mass manufacturing, though hybrid polymer–glass devices remain common in academic platforms [13,34]. Glass can also serve as a stable substrate for patterned electrodes and optical windows where signal stability is critical.
- Biodegradable polymers. Polylactic acid (PLA), polycaprolactone (PCL), and related materials are gaining attention for transient devices and remodeling-mimetic systems [34,35]. Their adoption in pharmacology remains limited by variable degradation rates, processing challenges, and the need to control degradation products that could confound biochemical measurements [34,35].
- Paper- and textile-based substrates. Paper-based microfluidics offers ultra-low-cost, disposable platforms with capillary-driven flow, relevant for point-of-care paradigms and low-resource settings [44]. Textile microfluidics has been piloted for wearable biosensing systems enabling conformal contact with skin and continuous sampling of sweat or interstitial fluid [45]. While these approaches trade structural fidelity for accessibility and scalability, they provide design inspiration for disposable or wearable derivatives of OOC and sampling modules [44,45].
- Ceramics and bioinspired composites. Ceramics provide mechanical stability and chemical robustness but integration into microfluidic systems is challenging. Bioinspired elastomers and conductive nanocomposites improve mechanical tunability, drug compatibility, and integration of electrical readouts in cardiac and neural OOCs [34,35,42,43].
- Emerging 2023–2025 advances. New bioinspired elastomers with reduced drug absorption have improved pharmacokinetic fidelity and minimized compound loss to device walls [34,36,39]. Conductive nanocomposite hydrogels enable electrical readouts in neural and cardiac tissues while preserving soft-tissue mechanics [42,43]. Multifunctional hybrid materials with tunable stiffness and sensor-compatible architectures point toward next-generation OOCs that combine mechanical fidelity with real-time quantitative readouts suitable for AI-enabled analytics [34,35,42,43].
In practice, material choices are increasingly evaluated not only for biological performance but also for data quality, including optical clarity and low autofluorescence for imaging, low sorption for PK studies, stable surface chemistry for long-term cultures, and compatibility with electrodes, probes, or imaging windows for sensor-rich experiments [17,34,35,36,42,43]. Material selection thus constrains not only tissue morphology and function but also the reliability of biochemical and omics profiles over time, which in turn influences the interpretability of downstream analytics and clinical-translational modeling [17,34,35,36,42,43].
2.2. Fabrication: Building Complexity at the Micro-Scale
Fabrication governs the resolution, reproducibility, scalability, and sensor-integration readiness of OOC devices. While early platforms prioritized rapid prototyping, translation demands methods that balance architectural fidelity, throughput, and industrial manufacturability, while enabling standardized measurement interfaces. Critical requirements include micrometer-scale dimensional tolerances, robust bonding between layers, compatibility with diverse cell types, and the ability to integrate electrodes, optical access, and fluidic connectors without compromising sterility or assay stability [13,14,15,34,35,37,38,40,41].
- Soft lithography. PDMS-based soft lithography catalyzed the first wave of OOCs by offering rapid prototyping and flexible channel design [13,24,25]. Replica molding against microfabricated masters enabled controlled microchannel geometries and on-chip valves using elastomeric membranes [24,25]. However, variability between batches, limited scalability, and PDMS absorption of small molecules have restricted its translational and regulatory acceptance in some contexts [36].
- 3D printing and bioprinting. Advances in stereolithography, two-photon polymerization, and extrusion-based printing enable fabrication of vascular networks, alveoli, and villus-like structures directly in chip formats [35,42,43]. Multi-material printing (2023–2024) can produce fine features and embed conductive or sensing-compatible elements, allowing co-fabrication of structural, soft, and conductive domains in a single workflow [35,37,42,43]. Bioprinting of cell-laden hydrogels enables spatially controlled deposition, supporting functional cardiac, neural, and vascular tissues with organoid-like architectures [35,42,43].
- Injection molding and hot embossing. Thermoplastic molding supports reproducible, high-throughput production at industrial scale [34,35,40,41]. These approaches reduce inter-laboratory variability and are increasingly adopted for screening platforms [34,40,41]. Molding also enables standardized footprints, alignment guides, ports, and optical windows that improve assay reproducibility and compatibility with automated imaging and plate-based workflows [40,41].
- MEMS and nanofabrication. Microelectromechanical systems (MEMS) introduce valves, pumps, and integrated electrodes that provide automated control of flow and sensing [13,14,34,37,38]. Nanopatterning techniques replicate ECM-like topographies that influence cell alignment, migration, and barrier formation in endothelial, epithelial, and neural models [24,25,35,37]. These methods also support reproducible electrode patterning and stable interfaces for electrical readouts.
- Design-for-manufacturing (2023–2025). Recent work emphasizes aligning fabrication with industrial standards: dimensional repeatability, bonding stability, media compatibility, sterile packaging, and automated handling [34,37,38,40,41]. Hybrid workflows that combine academic prototyping (soft lithography, 3D printing) with industrial molding/embossing provide a practical path to innovation plus reproducibility, and they are increasingly featured in translational OOC roadmaps [34,37,38]. These fabrication requirements are summarized in Figure 2.
Ultimately, fabrication choices must satisfy both biological and operational/data constraints: devices must support long-term culture yet remain robust to automated liquid handling, high-throughput imaging, and standardized sensor readouts that can be aggregated across sites and subjected to AI/ML analysis (Section 4). Minimizing device-to-device variability in channel dimensions, surface roughness, alignment, and bonding quality reduces variability in shear stress, oxygenation, and local microenvironments, thereby stabilizing gene-expression and secretome profiles that underpin omics-based characterization and benchmarking of OOC platforms [34,35,37,38,40,41].
2.3. Microfluidics: Controlling the Microenvironment
Microfluidics distinguishes OOC systems from static cultures by enabling perfusion, mechanical stimulation, and systemic coupling. Proper control of microscale flows governs nutrient delivery, waste removal, biochemical gradients, and the mechanical cues that shape tissue physiology. For translational workflows, flow uniformity, shear-stress calibration, sampling consistency, and long-term stability are critical requirements for reproducibility and quantitative interpretation [13,14,34,37,38].
- Perfusion and gradients. Continuous flow sustains oxygenation and nutrient exchange while removing metabolic waste, supporting long-term tissue viability and barrier integrity. Controlled gradients of cytokines, oxygen, or drugs can replicate physiological or pathological microenvironments and enable mechanistic perturbation studies. Because nutrient and drug distributions shape transcriptional and metabolic states, precise microfluidic control is essential for generating reproducible multi-omics signatures comparable across devices and laboratories [13,14,34,37,38].
- Shear stress and cyclic strain. Physiological mechanical forces regulate endothelial alignment, surfactant secretion in the lung, and peristalsis-like movements in the gut [19,20,37,46]. Microfluidic actuation enables cyclic strain or pulsatile flow, allowing controlled mechanobiological dose–response mapping and improved biomimicry versus static cultures [19,20,37,46].
- Embedded sensors and real-time readouts. Integration of TEER electrodes, oxygen/pH probes, and multi-electrode arrays provides continuous readouts of barrier function, metabolism, and electrophysiology [13,23,35,37,38]. Recent advances integrate miniaturized biosensors and monitoring-compatible formats into thermoplastic devices, supporting high-throughput workflows and generating dense time-series data suitable for AI-based feature extraction and pattern recognition (Section 4.3) [34,37,38,40,41].
- Computational fluid dynamics (CFD). CFD guides design by predicting shear stress, diffusion, and mixing within channels, enabling optimization of geometry and flow regimes prior to fabrication [46]. Hybrid CFD–experimental pipelines have been used to validate vascular and renal chips, reducing design iterations and improving cross-lab reproducibility [46]. These models also bridge to in silico frameworks and digital twins discussed later in multi-organ contexts.
- Closed-loop flow and systemic integration. Multi-organ systems link gut, liver, kidney, and vascular modules to model absorption, distribution, metabolism, and excretion (ADME) [14,15,22,37,38]. Recent work has demonstrated feedback-controlled perfusion regimes with embedded monitoring, supporting long-duration studies and more physiologically relevant systemic coupling [14,15,22,37,38].
Outlook. As OOCs mature, microfluidics is shifting from basic perfusion toward automated, feedback-controlled, multi-organ circuits. Standardization of flow rates, shear forces, media compatibility, and sampling protocols (aligned with emerging NAM guidance) will be essential for reproducibility, industrial uptake, and regulatory validation [13,14,15,16,17,18,34,37,38]. Because microfluidic design shapes the quality and structure of resulting data (imaging, electrophysiology, secretome, and omics), it sets boundary conditions for AI-enabled harmonization, feature extraction, and digital twin development described in Section 4 [16,17,18,37,38].
2.4. Integrated Biosensing and Measurement Validity: From Tissue Function to Decision-Ready Signals
While materials, fabrication, and microfluidics establish the biological microenvironment, integrated biosensing determines whether an OOC produces quantitative signals that are stable, comparable, and suitable for benchmarking against clinical endpoints. In translational contexts, sensor integration is not an add-on; it is a core design axis that influences what can be measured continuously, how perturbations are interpreted, and whether the platform can support standardized evidence-generation and fitness-for-purpose claims [13,16,17,18,23,35,37,38].
2.4.1. What is typically sensed in OOCs
Across organ systems, the most common continuous readouts include:
2.4.2. Integration constraints that affect signal reliability
Sensor performance in-chip is strongly shaped by the same engineering decisions highlighted above:
2.4.3. Calibration, drift, and reproducibility as translational requirements
For OOCs intended for decision support, measurement practices must align with the broader push toward quantitative performance metrics and fit-for-purpose criteria in NAM frameworks [17]. At minimum, OOC studies increasingly need to document:
- How sensors are calibrated (pre-run, in-run checks, or post-run validation using standards where feasible)
- How drift/baseline shifts are handled (e.g., reference channels, internal controls, periodic recalibration, or model-based correction)
2.4.4. Sampling, signal processing, and AI readiness
Continuous sensing produces time-series data streams whose interpretability depends on acquisition choices:
- Sampling strategy (frequency, duration, synchronization across modalities)
- Preprocessing (baseline correction, noise filtering, artifact handling for bubbles/flow disruptions)
- Feature extraction (rates of change, recovery kinetics, oscillatory behavior, event detection) These steps are increasingly linked to AI/ML pipelines that fuse imaging, electrophysiology, and biochemical readouts, enabling outcome prediction, phenotypic clustering, and mapping to PK/PD or clinical endpoints (Section 4.3) [18,37,38]. Notably, the value of AI depends on consistent measurement definitions and stable signal generation; device design choices therefore shape not only biology but also downstream analytic validity.
Outlook. Integrated biosensing is a key bridge between microphysiology and clinical concordance. As regulatory and industrial adoption advances, OOC platforms will be evaluated not only on whether they “look like” tissues, but on whether they produce standardizable quantitative readouts that support benchmarking, evidence generation, and clearly defined contexts of use [16,17,18]. This creates a practical convergence between chip engineering and biosensor discipline: device architectures that reduce sorption and variability, fabrication workflows that support standardized sensor placement, and microfluidics that stabilize sampling conditions collectively enable more reliable and decision-relevant OOC measurements [34,37,38,40,41].
Because the relevance of any biosensor readout is ultimately organ- and context-dependent, sensor performance in organ-on-chip (OOC) platforms should be evaluated with respect to the specific physiological function being modeled rather than in isolation. Barrier organs such as the intestine, lung, kidney, and blood–brain barrier rely primarily on impedance- and permeability-linked measurements to capture dynamic junctional integrity, whereas excitable tissues including the heart and nervous system require high-temporal-resolution electrical and mechanical readouts to resolve functional electrophysiology and contractility. In contrast, metabolically active organs such as the liver and pancreas depend more strongly on chemical and electrochemical sensing of oxygen, nutrients, and secreted biomarkers to quantify functional state and drug response.
Table 3 synthesizes the major biosensing modalities currently integrated into OOC systems, explicitly mapping sensor type to target analytes, dominant performance-limiting factors, and translational readiness within these organ contexts. Rather than ranking technologies by nominal sensitivity, the table emphasizes practical constraints—such as signal drift, biofouling, geometry dependence, and long-term stability—that determine whether sensor outputs can support benchmarking, model validation, and decision-making workflows. This organ-aware framing highlights both the maturity of established sensing approaches (e.g., TEER in barrier models, MEAs in cardiac safety assessment) and the remaining challenges for emerging modalities as OOCs transition from exploratory platforms to translational tools.
3. Applications: Modeling Organ Function and Disease
Organ-on-a-Chip (OOC) systems have been developed for multiple human organ systems. Each model leverages microengineering to reproduce essential features of physiology and pathology, enabling translational applications in drug testing, toxicology, and disease modeling [14,47,48,49,50,51,52,53,54]. For Biosensors-focused translational evaluation, it is helpful to view each OOC as a microphysiological construct plus an embedded measurement stack: the biological architecture establishes the phenotype, while integrated sensing/imaging and standardized sampling convert that phenotype into quantitative, time-resolved signals suitable for benchmarking and decision support (Section 2.4). Below, we review vascular, pulmonary, gastrointestinal, neurological, cardiac, renal, hepatic, cutaneous, tumor, and organoid-on-chip platforms, highlighting mechanistic fidelity, representative case studies, and the dominant readouts used to support contexts of use. These use cases are schematized in Figure 3 (panels A–J) and summarized in Table 4 to emphasize shared design patterns, organ-specific nuances, and typical assay readouts [14,47,48,49,50,51,52,53,54].
3.1. Blood-Vessel-on-a-Chip
Blood-vessel chips are among the most developed OOC platforms because of the central role of the vasculature in human physiology. Endothelialized microchannels under flow reproduce barrier function, shear-stress responses, and inflammatory activation, and are now used to model vascular pathobiology across thrombosis, atherosclerosis, and microvascular disease [47,55,56,57,58].
Dominant quantitative readouts (typical): endothelial barrier integrity (permeability and junctional integrity), thrombus formation kinetics under shear, inflammatory activation signatures, and trans-endothelial transport of therapeutics [47,55,56,57,58].
3.2. Lung-on-a-Chip
The lung was the first OOC successfully demonstrated, capturing the alveolar–capillary interface with epithelial and endothelial layers separated by a porous, flexible PDMS membrane [19]. Cyclic strain simulates breathing motions, while perfusion recreates alveolar blood flow [19,20].
Dominant quantitative readouts (typical): barrier integrity/leakage, cytokine dynamics, aerosol deposition/uptake, and infection kinetics under human-relevant mechanics [14,19,20,45,46].
- Chronic lung disease. Small-airway chips incorporating smooth muscle and immune cells model airway hyperresponsiveness, steroid sensitivity, and chronic inflammation in asthma and COPD, with readouts that correlate to patient phenotypes [20].
3.3. Gut-on-a-Chip
Gut chips are among the most mature and widely adopted OOC systems because they reproduce villus-crypt structures, mucus production, and peristalsis-like cyclic strain under controlled flow [21,61].
Dominant quantitative readouts (typical): barrier integrity (e.g., TEER/permeability surrogates), mucus and epithelial differentiation markers, microbiome-modulated functional responses, and inflammatory mediator dynamics [21,61,62,63,64,65].
- Recent advances (2023–2025). Immune-enhanced gut chips incorporating macrophages, dendritic cells, and lymphocytes enable mucosal immunity modeling, while multi-omics benchmarking aligns chip transcriptomes and epigenetic signatures with patient biopsy datasets; molecular readouts typically include tight-junction proteins (e.g., ZO-1, claudins), mucins, and inflammatory mediators that can be benchmarked against patient biopsies and multi-omics profiles [21,42,61,62,63,64,65,67].
3.4. Brain-on-a-Chip
Brain-on-a-chip platforms predominantly model the blood–brain barrier (BBB) and neurovascular unit, integrating iPSC-derived endothelial cells, astrocytes, pericytes, and neurons for higher physiological fidelity [22,68,69,70,71].
Dominant quantitative readouts (typical): apparent permeability/efflux behavior, tight-junction and transporter markers, and neural activity phenotypes (e.g., calcium imaging or MEA-style readouts) in neurovascular contexts [22,68,69,70,71].
- Neurodegeneration. Microengineered brain disease models combining human neurons and glia with perfused BBB interfaces capture circuit-level dysfunction and disease-relevant phenotypes, including α-synuclein pathology and barrier disruption [22].
- Recent advances (2023–2025). Vascularized brain organoids and tissue-to-tissue BBB chips have improved nutrient delivery, maturation, and assayability, while numerical simulations and other in silico models now help optimize BBB-on-a-chip designs and flow conditions for better reproducibility [42,68,69,70,71,72]. In parallel, AI methods (such as deep learning applied to calcium imaging and multi-electrode recordings) are beginning to detect seizure-like and neuroinflammatory signatures that align with human EEG phenotypes, enabling AI-enhanced endpoint detection for CNS safety and disease modeling [18,73,74].
3.5. Heart-on-a-Chip
Cardiac chips use iPSC-derived cardiomyocytes seeded on patterned, elastomeric substrates, often integrated with microelectrodes to capture contractile function and electrophysiology [23,75].
Dominant quantitative readouts (typical): contractile force proxies, field potential/action-potential waveform features, conduction metrics, and beat-to-beat variability [23,75].
- Drug discovery. Organoid-on-chip and multi-tissue platforms integrating cardiac modules are being used for torsadogenic risk assessment and in vitro human QT prediction, benchmarked against clinical ECG data and regulatory safety pharmacology requirements [23,75]. Deep learning models trained directly on field potential or action-potential waveforms from cardiac MPS have been explored for proarrhythmic risk classification by leveraging waveform morphology and beat-to-beat variability beyond single-channel hERG assays [18,73].
3.6. Kidney-on-a-Chip
Kidney chips reproduce key nephron functions (filtration at the glomerulus and reabsorption/secretion in the proximal tubule) using perfused epithelial and endothelial interfaces with physiological flow [16,76,77].
Dominant quantitative readouts (typical): transporter-mediated flux/clearance estimates, injury biomarkers, and epithelial function markers under physiological shear [16,76,77].
3.7. Other Organ-on-a-Chip Models
While vascular, pulmonary, intestinal, neural, cardiac, and renal chips represent the most mature platforms, other organs have also been modeled with OOCs:
Liver-on-a-Chip
Dominant quantitative readouts (typical): albumin/urea secretion, CYP activity panels, bile acid handling, and injury/stress-response signatures under perfusion [13,66,78].
- 2022–2024 advances. High-throughput liver chip arrays and refined liver-on-chip designs are enabling larger compound sets, while vascularized liver organoids integrated under flow exhibit superior metabolic fidelity and disease modeling capabilities [42,66,78]. In addition to functional outputs (albumin, urea), panels of CYP isoforms, bile-acid transporters, and stress-response transcripts are increasingly used to define “hepatic fidelity” signatures that can be compared with human liver tissue and clinical DILI phenotypes [13,66,78,79].
Skin-on-a-Chip
Dominant quantitative readouts (typical): barrier integrity surrogates, transepidermal metrics, irritation/inflammation markers, and wound closure/ECM remodeling kinetics [48].
- Recapitulates epidermal barrier function, dermal fibroblasts, and often immune competence in layered constructs, enabling barrier integrity measurements and topical exposure studies [48].
- Used for dermatology drug testing, cosmetic safety, and wound-healing studies, including re-epithelialization and scar formation assays [48].
Tumor-on-a-Chip
Dominant quantitative readouts (typical): invasion/intravasation dynamics, hypoxia/EMT signatures, cytokine/chemokine panels, and therapy-response heterogeneity from live imaging with molecular endpoints [13,42,47,49].
- 2023–2025 advances. Integration of patient-derived tumor organoids with multiplexed readouts (live imaging, secretome, and omics) supports precision-oncology workflows in which therapies are screened directly on patient-matched microtumors, and the resulting high-content datasets are increasingly analyzed with deep learning to predict drug response from baseline morphology and molecular profiles, effectively turning each microtumor into an information-rich training example [18,42,47,49,66,79,80,81]. Hypoxia markers, epithelial–mesenchymal transition signatures, and immune-activation transcripts then serve as molecular endpoints that complement imaging-based invasion and killing assays in these systems [42,47,49,66].
3.8. Organoid-on-Chip Hybrids
Organoids derived from stem cells or patient biopsies provide self-organized, multicellular structures that recapitulate aspects of tissue physiology and disease phenotypes. However, they are limited by the absence of vascularization, immune competence, and controlled microenvironments, leading to variability and restricted scalability [42]. Integrating organoids into microfluidic OOCs addresses these challenges by combining organoid self-organization with the environmental precision of OOCs [31,42,47,70,71].
Dominant quantitative readouts (typical): preservation of tissue architecture and stem-cell niches, perfusion-enabled maturation, functional barrier/transport endpoints (where relevant), and multi-omics concordance with patient samples [31,42,47,70,71].
- Neurodevelopment and brain disease. Cerebral organoids seeded on perfusable chips recapitulate human cortical development and, with vascularization and BBB interfaces, achieve extended viability and advanced neuronal maturation, enabling modeling of neurodevelopmental and neurodegenerative disorders [22,42,68,70,71].
- Metabolic and oncologic models. Pancreatic and liver organoid–on-chip systems enable modeling of diabetes and hepatic disease, while patient-derived tumor organoids incorporated into tumor chips provide precision oncology platforms where therapies can be screened directly on patient-matched microtumors [31,42,66,70,71].
- Vascularized and immune-competent constructs. iPSC-derived vascularized liver and kidney buds perfused on chips improve perfusion and transporter activity, while brain and kidney organoids in microfluidic devices show better nutrient delivery and barrier function. Immune-competent hybrids incorporating myeloid and lymphoid cells model tumor–immune interactions and viral infection, advancing OOCs toward fuller immunophysiology [22,31,42,47,66,67,70,71,77]. Endocrine (e.g., pancreatic islet) and reproductive (e.g., placenta, ovary, testis) OOCs are also emerging and reviewed elsewhere [15,43,82].

Table 4.
Representative Organ-on-a-Chip models, use cases, and assay readouts.
| Organ Model | Context of Use | Key Readouts and Validation Metrics |
|---|---|---|
| Blood-vessel | Thrombosis, angiogenesis, metastasis | Endothelial barrier integrity; platelet adhesion and fibrin formation under defined shear; microvascular dysfunction in diabetes and inflammation. |
| Lung | Inhalation toxicology, viral infection, asthma/COPD | TEER, cytokine release, barrier leakage; aerosol deposition and uptake under cyclic stretch; infection and antiviral response profiling. |
| Gut | IBD, NSAID enteropathy, colorectal cancer, host–microbiome | TEER, mucus production, cytokine panels; microbiome-modulated drug response; organoid- and immune-competent gut chips benchmarked against biopsies. |
| Brain / BBB | BBB permeability, neurodegeneration, neuroinflammation | Apparent permeability and efflux ratios; tight-junction markers; neural activity readouts for CNS exposure and neurotoxicity. |
| Heart | Cardiotoxicity, cardiomyopathies, proarrhythmia risk | Contractile force, field potential duration, conduction velocity, and arrhythmia indices; waveform analysis for torsadogenic risk classification. |
| Kidney | Nephrotoxicity, diabetic nephropathy, renal clearance | Transporter activity, transepithelial flux, and clearance estimates; injury biomarkers under physiological shear; IVIVE of renal function. |
| Liver | DILI, metabolic and cholestatic disease | CYP activity, albumin and urea secretion, bile acid homeostasis; hepatotoxicity biomarkers for acute and chronic DILI prediction. |
| Skin | Wound healing, dermatology, topical/cosmetic safety | Barrier TEER, transepidermal water loss, re-epithelialization and matrix remodeling; immune activation in infection and irritation models. |
| Tumor | Invasion, intravasation, immunotherapy response | Invasion and intravasation metrics, tumor growth and killing assays, cytokine/chemokine panels; tumor–immune interaction profiling. |
| Organoid hybrids | Brain, gut, liver, kidney, tumor models; personalized testing | Preservation of tissue architecture and stem-cell niches; vascularization; multi-omics concordance with patient samples for individualized drug response. |
Advantages of organoid–on–chip integration include improved vascularization and oxygenation, reduced variability via controlled microenvironments, support for multi-lineage co-cultures, and quantitative benchmarking through omics comparisons to patient biopsies [31,42,47,61,62,63,64,65,67,70,71]. These hybrid systems bridge the gap between self-organizing biology and engineered microenvironments, positioning OOCs as powerful tools for personalized medicine and drug discovery pipelines. Their high-content imaging and multi-omics readouts also make them natural substrates for AI-based feature extraction and multi-omics integration, as developed more fully in Section 4.3 [18]. Key design features, cell sources, and representative assay readouts for the Organ-on-a-Chip platforms discussed in this section are summarized above in Table 4.
4. Future Directions: Toward Validation, Integration, and Translation
Organ-on-a-Chip (OOC) technologies have progressed from proof-of-concept devices to platforms increasingly evaluated for decision-making in discovery, safety, and early clinical translation. Recent roadmaps emphasize four intersecting trajectories: (i) deeper biological realism in individual chips, (ii) systemic integration across multiple organs and disease axes, (iii) AI- and multi-omics–enabled analytics that can extract robust, decision-relevant signals from complex datasets, and (iv) validation and regulatory frameworks that treat OOCs as quantitative tools rather than qualitative demonstrations [13,14,15,18,26,27,28,31,32,50,51,52,53,54,73,83,84,85,86,87]. For Biosensors-focused translation, these trajectories are unified by a cross-cutting requirement: OOCs must be paired with an explicit measurement strategy (integrated sensing/imaging and standardized sampling that yield traceable, time-resolved outputs with known performance boundaries) (Section 2.4). A concise, fit-for-purpose checklist is summarized in Table 5, while the broader roadmap from early microfluidics to automated, multi-organ and AI-enabled platforms is depicted in Figure 4. Together, they highlight that technological sophistication alone is insufficient; OOCs must be embedded in a data, validation, and regulatory ecosystem that allows sponsors and regulators to interpret their outputs in parallel with existing in vitro and in vivo standards [17,26,27,28,31,32,50,51,52,53,54,73,83,84,85,86,87,88,89,90,91].
4.1. Enhancing Biological Realism
A central challenge is to increase biological realism without sacrificing robustness and throughput. First-generation OOCs typically recapitulated one or two features of the tissue microenvironment (such as shear stress, basic barrier function, or simple cytoarchitecture) using PDMS-based devices and a limited set of cell types [13,14,15,19,24,25,34,35,36,37]. Newer designs incorporate more complex extracellular matrix (ECM) architectures, stromal and immune components, dynamic mechanical stimulation, and long-term perfusion to more closely emulate native physiology [26,27,34,35,37,38,42,43,61,70,71,85,86,87]. As realism increases, so does the need to define which phenotypes must be measured quantitatively to justify the added complexity; otherwise, more elaborate biology can simply create more variable outputs without improving decision utility [27,28,31,32,50,51,52,53,54,73,83,84,85,86,87].
From a materials perspective, development is moving away from single-material PDMS devices toward hybrid platforms that combine thermoplastics, hydrogels, and ECM-derived biomaterials to fine-tune stiffness, permeability, optical properties, and adsorption [34,35,37,38,40,41,42,43]. Multi-material 3D printing and modular assembly strategies are being used to integrate compliant membranes, porous scaffolds, and vascular-like channels into a single device while maintaining compatibility with optical imaging and plate-based workflows [26,34,35,37,38,42,43,85]. These advances support more physiologically relevant architectures (e.g., villus-like projections in gut chips, anisotropic myocardium, or aligned white-matter tracts), but they also expand the design space. In practice, fit-for-purpose design requires explicit definition of which aspects of native tissue are critical for the intended context-of-use and which can remain simplified [27,28,31,32,50,51,52,53,54,73,83,84,85,86,87].
The convergence of organoids and OOCs is another major opportunity for enhanced realism. Organoid-on-chip systems aim to retain the self-organizing, multi-lineage complexity of organoids while imposing controlled perfusion, mechanical cues, and defined gradients [21,26,27,31,42,61,62,63,64,65,67,70,71,85,86,87]. Brain and neurodevelopmental organoid-on-chip platforms now incorporate vascular surrogates, immune cells, and fluid flow to model neuroinflammation and neurotoxicity, while gut-on-chip platforms integrate microbiota and immune components to investigate barrier function and host–microbe interactions under dynamic conditions [21,26,27,42,61,62,63,64,65,67,70,71,85,86,87]. These hybrid models raise new validation questions: what constitutes acceptable variability in self-organizing systems, and which phenotypic features should be prioritized as anchors for comparison to in vivo benchmarks [26,27,85,86,87]?
Addressing these questions will increasingly require quantitative phenotyping and multi-parametric scoring rather than single-endpoint assays. This creates a direct link to AI-enabled image and signal analysis (Section 4.3), where high-content imaging, time-lapse morphodynamics, and electrophysiological readouts can be converted into composite metrics of “tissue health” or “organotypicity” that are more informative than individual markers [18,26,27,72,85,86,87,99,100,101,102,103]. For Biosensors-facing adoption, an important practical implication is that biological realism should be pursued in parallel with measurement realism: stable acquisition, defined operating ranges, and standardized sampling plans that preserve interpretability as the model’s complexity increases (Section 2.4) [17,26,27,28,85,86,87,88,89,90,91,104,105,106,107].
4.2. From Single Organs to Systemic Models
Many early OOC applications focused on single-organ questions (such as barrier integrity, hepatotoxicity, or cardiotoxicity) that could be addressed by isolated models [13,14,15,19,20,21,22,23,31,32,50,51,52,53,54,73,83,84]. However, key translational questions in drug development and disease biology involve interactions across multiple organs and biological axes (e.g., liver–heart, gut–liver–immune, tumor–stroma–immune), as well as special populations such as pediatrics or pregnancy. Multi-organ and body-on-chip platforms aim to capture these interactions by linking several organ modules through recirculating media, controlled flow splitting, and physiologically inspired scaling rules for volume, surface area, and residence time [14,15,22,26,27,28,31,32,37,47,50,51,52,53,54,73,83,84,85,86,87].
This systemic integration raises several design and analysis challenges. Fluidic scaling must balance physiological relevance against practical constraints such as total media volume, sampling requirements, and compound solubility [14,15,26,27,28,31,32,37,50,51,52,53,54,73,83,84,85,86,87]. Different organ modules may have distinct optimal media, oxygen demands, and mechanical environments, requiring compartment-specific control within a shared circuit. Interpreting outputs from multi-organ models demands clear definitions of system-level biomarkers (e.g., integrated clearance, metabolite fluxes, distributed toxicities) rather than organ-specific readouts alone [26,27,28,31,32,50,51,52,53,54,73,83,84,85,86,87]. From a measurement perspective, this also means prioritizing system-level observables that can be collected reproducibly over time (i.e., readouts that are stable under recirculation and interpretable under changing exposure distributions) rather than only endpoint snapshots (Section 2.4) [17,26,27,28,85,86,87,88,89,90,91,104,105,106,107].
In parallel, in silico modeling of OOC devices and circuits is becoming more common, both for device design and for translational extrapolation. Computational fluid-dynamics and transport models can predict shear stress, concentration gradients, and residence times across complex geometries, while multi-scale models combine chip-level pharmacokinetics with cellular pharmacodynamics to estimate exposure–response relationships [18,31,32,72,82,83,84]. New frameworks such as DigiLoCS explicitly couple OOC data with digital-twin representations of patients, using OOC outputs to calibrate and refine model parameters for specific scenarios [29,31,32,82,83,84]. Digital-twin–enhanced microphysiological systems have already been used to explore drug pharmacokinetics in pregnancy by linking multi-organ chips to maternal–placental–fetal PBPK models, illustrating how OOCs can be embedded in quantitative systems pharmacology workflows [31,32,82,83,84,98].
These trends point toward OOCs not as standalone replacements for animal models, but as modular components in a broader experimental–computational ecosystem. In this ecosystem, device design, flow regimens, sampling schemes, and readouts can be optimized using model-in-the-loop strategies, and chip data are interpreted through the lens of mechanistic models and digital twins that span from cell to organism [18,26,27,28,29,31,32,72,82,83,84,85,86,87,98]. AI and machine-learning (ML) methods can further support multi-organ platforms by guiding experimental design (e.g., active learning for selecting conditions), identifying informative combinations of readouts, and enabling adaptive control strategies in complex circuits (Section 4.3) [18,29,72,82,85,86,87,98,99,100,101,102,103]. For Biosensors translation, a key practical point is that multi-organ “system outputs” must remain measurement-valid: stable acquisition, defined performance limits, and standardized metadata sufficient to compare circuits across sites and lots [17,26,27,28,85,86,87,88,89,90,91,104,105,106,107].
4.3. AI and Multi-Omics Integration
As OOCs increasingly incorporate transcriptomic, proteomic, metabolomic, and secretomic readouts, integrating these data becomes both an opportunity and a challenge. Multi-omics ML frameworks originally developed for patient cohorts (such as similarity-network fusion, multiple-kernel learning, and deep autoencoders) can be adapted to OOC datasets to identify composite signatures of toxicity, efficacy, or disease progression [30,97,108]. These approaches are well suited to high-dimensional, heterogeneous data and can uncover latent factors that distinguish mechanisms of injury or response phenotypes, even when individual readouts are noisy [30,97,108].
In liver chips, for example, a “hepatic stress signature” might integrate CYP down-regulation, mitochondrial stress transcripts, altered bile-acid transport, metabolic flux changes, and secreted cytokines. Once benchmarked against clinical or in vivo datasets, such signatures could serve as translational biomarkers for early detection of idiosyncratic hepatotoxicity or for stratifying compounds by mechanism of liver injury [18,30,31,32,50,51,52,53,54,73,83,84,97,108]. Similar strategies apply to immune-oncology, neurovascular, and gut–liver models, where multi-omics provides insight into cell–cell communication and microenvironmental remodeling [18,30,31,32,50,51,52,53,54,73,83,84,97,108]. In a Biosensors context, these signatures are only as transferable as the underlying measurement pipeline: harmonized sampling windows, consistent preprocessing, and metadata that supports traceability across donors, chips, and sites (Section 2.4) [26,27,28,30,85,86,87,88,89,90,91,97,99,100,101,102,103,104,105,106,107,108,109].
AI for imaging, morphology, and quality control. Deep-learning models have been applied to OOC and organoid imaging for segmentation, tracking of dynamic morphological changes, and classification of treatment responses [18,99,100,101,103]. Curated organ-on-chip image datasets labeled as “acceptable” or “failed” show that convolutional neural networks can detect suboptimal tissue organization and predict downstream experimental failure from early time points [102]. Cross-platform image harmonization further enables multi-site studies by reducing batch effects across microscopes and staining protocols [99,103]. These capabilities are increasingly relevant for routine deployment: automated image-based quality control can flag chips that fall outside predefined morphological envelopes before costly downstream assays, while standardized feature representations support objective comparison across devices, laboratories, and manufacturing lots [18,26,27,28,85,86,87,99,100,101,102,103]. For decision-impact contexts, quality control should be treated as part of the measurement system, with explicitly defined acceptance thresholds and documented failure modes [17,26,27,28,85,86,87,88,89,90,91,104,105,106,107].
Data resources, digital twins, and model-informed decisions. Dedicated databases such as OOCDB, which curate experimental metadata, device designs, cell sources, and assay results, provide a foundation for AI-driven meta-analysis and benchmarking [109]. When linked with imaging and multi-omics repositories, these resources support construction of digital twins (computational representations of patients or subgroups calibrated using mechanistically rich OOC data) [18,26,27,28,29,30,31,32,72,82,83,84,85,86,87,97,98,99,100,101,102,103,108,109]. Recent demonstrations include pregnancy-focused digital twins that combine multi-organ chips with physiologically based pharmacokinetic models to explore drug disposition and safety in populations that are difficult to study in vivo [31,32,82,83,84,98]. More broadly, closed-loop frameworks integrating OOC experiments, ML-based surrogate models, and simulation enable efficient in silico exploration of “what-if” scenarios and experimental design before large-scale laboratory campaigns [18,29,30,31,32,72,82,83,84,97,98,108].
Interpretability & reproducibility. While AI-enabled workflows can increase sensitivity and throughput, they also introduce translational risk if models are not reproducible, interpretable, and robust to dataset shift across donors, sites, instruments, and device lots. In practice, OOC datasets are susceptible to confounding from batch effects (e.g., differences in imaging settings, staining protocols, cell differentiation state, or microfluidic operating conditions), which can inflate apparent performance if not explicitly controlled. For decision-impact contexts, best practices include standardized preprocessing, version-controlled pipelines (data and code), explicit reporting of training/validation splits, uncertainty quantification, and external validation on independent multi-site datasets; where feasible, interpretable representations (e.g., clinically meaningful features or mechanistic proxies) should be prioritized to support auditability and regulatory confidence [18,26,27,28,30,85,86,87,97,99,100,101,102,103,108,109]. Looking forward, AI- and multi-omics–enabled OOCs will be most impactful when embedded in transparent workflows that declare data provenance, preprocessing, model architectures, performance metrics, and limitations. For clinical and regulatory audiences, demonstrating interpretability, reproducibility across sites, and clear links between OOC-derived signatures and clinical outcomes will be as important as predictive accuracy.
4.4. Validation, Standards, and Regulatory Science
As OOCs move closer to regulatory and industrial decision-making, evaluation criteria are shifting from “Does the model look like an organ?” to “Does the model improve decision-making relative to current tools, for a clearly defined context of use?” [17,26,27,28,31,50,51,52,53,54,83,85,86,87,88,89,90,91]. Accordingly, validation efforts increasingly emphasize quantitative concordance with human-relevant endpoints, reproducibility across sites, and transparency of performance boundaries rather than qualitative biomimicry alone. Table 5 summarizes representative organ-specific validation metrics and target performance ranges reported in recent concordance studies and roadmap efforts. In Biosensors-facing implementations, these biological performance targets should be paired with explicit measurement performance expectations (e.g., stability, sampling cadence, and comparability under standardized acquisition), because regulatory confidence depends on both the biological system and the data system that reports its state [17,26,27,28,85,86,87,88,89,90,91,104,105,106,107].
Global regulatory landscape for NAMs. Momentum toward new approach methodologies (NAMs) is increasingly global, but regulatory mechanisms and emphasis differ across jurisdictions. Agencies and consortia are converging on shared expectations: a clearly defined context of use, transparent evidence-generation plans, reproducibility (including cross-site performance where feasible), and interpretable links between assay outputs and decision-relevant endpoints. The FDA Modernization Act 2.0 has further accelerated this shift by explicitly enabling qualified non-animal methods in preclinical safety assessment, strengthening the incentive for standardized validation and reporting practices that can support regulatory confidence across regions [16,17]. Across jurisdictions, this landscape underscores the value of harmonized benchmarks, shared reference-compound panels, and transparent reporting norms to enable cross-comparability and facilitate broader acceptance of OOC-derived evidence.
Industrial surveys indicate that pharmaceutical companies already use OOCs and related microphysiological systems (MPS) for mechanistic studies, compound ranking, and hypothesis generation, but routine deployment at pivotal decision points remains limited [26,27,28,31,50,51,52,53,54,83,85,86,87,88,89,90,91]. Key barriers include uncertainty about inter-laboratory reproducibility, lack of standardized study designs, and incomplete mapping of chip-derived endpoints to regulatory-relevant outcomes such as safety margins and exposure–response relationships [17,26,27,28,31,50,51,52,53,54,83,85,86,87,88,89,90,91].
In response, multiple complementary quality-management and reporting frameworks have been proposed for MPS and related NAMs. The GIVReSt initiative and follow-on guidance define criteria for quality management and reproducibility monitoring across cell sourcing, device manufacturing, assay execution, and data analysis [105,106]. The MDAR (Materials Design Analysis Reporting) framework promotes transparent reporting of study design, reagents, analysis plans, and data availability [104]. Petersen and co-workers outline technical requirements for high-quality measurements in NAMs, including OOCs [88], while Pamies and colleagues propose fit-for-purpose validation and quality strategies specific to microphysiological systems [89]. Reyes and co-workers argue for a shift from animal-centric validation toward in vitro–centric paradigms supported by cross-platform comparisons and shared reference compounds [90]. Omics-reporting standards such as MIAME underscore the importance of structured metadata and data access when transcriptomic and other high-dimensional endpoints are incorporated into OOC studies [107]. Recent position papers further emphasize that AI-based analysis and automated quality control are part of the “system under test” and must themselves be validated, documented, and monitored over time [17,18,26,27,28,31,83,85,86,87,88,89,90,91,99,100,101,102,103,104,105,106,107,109].
Remaining challenges include integrating immune components with acceptable donor-to-donor reproducibility; scaling multi-organ systems with physiologically realistic flows, tissue ratios, and metabolic coupling; establishing consensus reference-compound panels and biomarker benchmarks; developing industrial-scale manufacturing pipelines that balance reproducibility with biological fidelity; and ensuring that AI-driven digital twins and multi-omics frameworks remain interpretable and compatible with regulatory expectations [13,14,15,18,19,20,21,22,23,26,27,28,29,30,31,32,37,47,50,51,52,53,54,61,72,73,82,83,84,85,86,87,88,89,90,91,97,98,99,100,101,102,103,104,105,106,107,108,109]. Addressing these challenges will largely determine whether OOCs achieve mainstream regulatory and industrial adoption over the next decade.
5. Clinical Concordance and Adoption
For Organ-on-a-Chip (OOC) platforms to transition from academic prototypes to regulatory-accepted tools, they must demonstrate clinical concordance, defined as the ability to quantitatively reproduce patient-level outcomes and deliver decision-relevant impact. Clinical concordance goes beyond structural or molecular fidelity and requires direct benchmarking against human pharmacokinetics/pharmacodynamics (PK/PD), toxicology, electrophysiology, and biomarker datasets within clearly defined contexts of use. In a Biosensors context, clinical concordance is only defensible when the measurement layer is characterized (e.g., acquisition stability, drift, sampling cadence, and cross-site comparability), because the “chip + sensor/imaging” system is the source of regulatory-facing evidence [27,28,29,82,88,89,90,91,98,104,105,106,107]. Recent reviews and position papers in the microphysiological systems (MPS) and organs-on-chips field have converged on this translational framing [27,28,29,82,98]. Representative concordance outcomes are aggregated in Table 6, and the overall workflow linking chip readouts to patient data is depicted in Figure 5.
5.1. Defining Clinical Concordance
- Analytical performance, which addresses assay reproducibility, sensitivity, specificity, dynamic range, and limits of detection/quantification, including sensor/electrode performance and imaging acquisition stability (calibration, drift, and lot-to-lot comparability). This tier aligns with traditional bioanalytical validation and is essential to ensure that chip-derived measurements are technically robust across runs, operators, and sites [27,28].
- Biological fidelity, which compares chip-derived gene, protein, metabolic, and functional signatures to native human tissue or high-fidelity ex vivo models. Metrics include transcriptomic similarity, maintenance of tissue-specific markers, stable barrier function, and appropriate responses to positive/negative controls [27,28,82,98].
- Clinical concordance, which requires quantitative agreement between chip-derived outputs and patient-level outcomes, such as permeability coefficients, PK/PD parameters, QT prolongation, biomarker kinetics, and adverse event incidence [29,82,98]. This often involves in vitro–in vivo extrapolation (IVIVE), physiologically based PK/PD (PBPK/PD) coupling, and comparison against historical clinical trial or real-world data [74,80,93,110].
Among these tiers, clinical concordance is the most critical for regulatory and pharmaceutical adoption because it directly addresses whether a given OOC assay improves decision-making relative to incumbent models (2D cultures, organoids, animal studies, or simple in vitro assays) [27,28,29,82,98]. Without decision-relevant alignment, even technically sophisticated platforms risk being deployed only as descriptive tools.
5.2. Case Studies Across Organ Systems
A growing body of work now demonstrates clinical concordance across multiple organ systems, as summarized in Table 6. These examples illustrate how OOCs can reproduce human PK, electrophysiology, toxicity, and barrier function within quantitative error bounds acceptable for decision-making.
- Cardiac chips. Human iPSC-derived cardiac OOCs have been benchmarked against clinical QT prolongation data and torsadogenic risk classification, with international multisite studies reporting AUROC values ≥0.85 and high sensitivity for borderline compounds relative to hERG-only assays [81,92]. Complementary reviews describe deep learning–enabled analytics and related organ-on-chip electrophysiology datasets that support automated waveform and image-based endpoint extraction [99,100,101,102,103]. By integrating field potential duration, contractility, and beat-to-beat variability, these systems better capture integrated cardiac responses and more accurately classify torsadogenic vs. non-torsadogenic drugs.
- Kidney chips. Proximal tubule-on-a-chip platforms quantify active and passive renal clearance, transporter-mediated drug–drug interactions, and nephrotoxicity, with chip-derived clearance estimates typically within 10–20% RMSE of clinical values after IVIVE scaling [74,93]. Physiologic flow and shear stress support more realistic transporter expression (e.g., OATs, OCTs, P-gp) and improve prediction of transporter-mediated clearance compared with static cocultures [74,93].
- Lung chips. Lung-on-chip models reproduce key inflammatory and barrier responses in pulmonary edema, COPD, and viral infection [19,37,47]. Under cyclic stretch and air–liquid interface, they yield TEER and cytokine profiles comparable to human explants, and during COVID-19 were used to model SARS-CoV-2 infection and antiviral responses with patterns that correlated with patient data [19,37,47].
- Liver chips. Liver-on-a-chip platforms that maintain cytochrome P450 activity, albumin secretion, and bile acid homeostasis over weeks improve detection of both dose-dependent and idiosyncratic DILI relative to conventional 2D hepatocyte cultures [30,74,79,97]. Multi-organ MPS linking gut–liver or liver–kidney circuits further show concordance between chip-derived metabolite profiles and clinical PK/DILI outcomes for reference compounds [74,79,105,108].
- Brain chips and blood–brain barrier (BBB) models. Microfluidic BBB chips comprising endothelial cells, pericytes, and astrocytes provide apparent permeability and efflux ratios for CNS-active drugs that correlate well with in vivo microdialysis or PET (R > 0.8; efflux ratios within ±10–20% of in vivo) [61,68,94,95,96]. More complex brain-on-chip systems with neuronal and glial networks recapitulate neuroinflammatory and seizure-like activity, enabling comparison of electrophysiological phenotypes to human EEG and clinical response profiles [67,73].
- Hematologic and retinal models. Bone marrow-on-chip platforms replicate key features of the hematopoietic niche and myelosuppression, allowing longitudinal tracking of leukocyte production and drug-induced marrow toxicity benchmarked against in vivo and clinical data [111]. Retina-on-chip devices that integrate organoid technology with microfluidic perfusion enable multi-layer retinal architectures and gene/cell therapy testing under controlled flow and oxygenation, with structural and functional metrics aligned to patient imaging and ex vivo explants [112].
5.3. Decision Impact and Adoption
Decision impact can be quantified using:
- Discrimination metrics such as AUROC, sensitivity, specificity, and positive/negative predictive values (PPV/NPV).
- Calibration metrics such as Brier scores or calibration curves comparing predicted vs. observed event rates.
In decision-curve analysis, the clinical utility of a model is evaluated across a range of risk thresholds, allowing comparison of how different testing strategies (e.g., animal models alone vs. animal plus OOC) would change the proportion of patients correctly treated or spared unnecessary exposure [27,29,82,98]. Examples include:
Pharmaceutical adoption is accelerating. Major companies have reported internal pilots or broader deployment of OOCs and MPS for safety pharmacology, DILI prediction, and mechanistic de-risking [113,114,115,116,117]. Recent roadmaps and surveys highlight priority use cases, internal barriers to scale-up, and the need for coordinated investment in automation, data infrastructure, and AI/ML capabilities to fully exploit OOC-derived datasets [86,87,118,119,120].
Regulatory agencies and expert consortia now explicitly recognize MPS and OOCs as new approach methodologies (NAMs) for safety and efficacy assessment. Recent reviews and commentaries outline how these platforms can feed into weight-of-evidence frameworks, support mechanism-based read-across, and reduce reliance on animal models within defined contexts of use [17,91,105,119,121,122,123,124]. National and regional position papers emphasize that OOCs and related NAMs will only achieve regulatory impact if aligned with formal qualification processes, transparent reporting standards, and clearly defined performance targets for specific contexts of use [17,31,83,122,123,124].
AI- and omics-enabled OOC pipelines are increasingly positioned as key enablers of such decision impact. Integrative frameworks that couple intelligent OOC devices, high-content analytics, and multi-organ PBPK/PD models aim to move OOCs from exploratory tools to routine decision-support systems in both human and veterinary drug development [18,32,72,84,115,118,119,125].
5.4. Limitations and Barriers to Widespread Adoption
Despite rapid progress, several barriers still limit full regulatory acceptance and widespread industrial deployment of OOC platforms. These limitations span the evidence base used for benchmarking, cross-site reproducibility, study designs that demonstrate decision impact, industrial-scale manufacturing, and the integration of complex data streams (including AI-enabled analytics) into regulatory-facing workflows.
- Inter- and intra-laboratory variability. Outcome variability persists due to differences in cell sources, media formulations, flow rates, chip geometries, and readout analysis pipelines. Recent work on standardized reporting frameworks and comparability metrics for microfluidic systems is beginning to address this but has not yet been universally adopted [33,105,108,111,114,115,124].
- Limited decision-impact studies. Most publications remain descriptive, focusing on demonstrating biological relevance rather than comparative performance vs. incumbent assays. Rigorous, hypothesis-driven studies that prospectively compare OOC-informed vs. standard decision paths (e.g., using historical pipelines or simulation studies) are still relatively rare [27,29,82,93,95,96,98,111,112,119,120,122,123].
- Industrial scaling and manufacturability. Robust, high-throughput production of OOC devices requires scalable thermoplastic manufacturing, integrated sensing, automation, and quality systems that meet Good Laboratory Practice (GLP) expectations [80,105,108,114,126]. Many current platforms rely on PDMS or bespoke fabrication workflows that are difficult to scale or qualify.
- Data/model integration and AI transparency. To fully leverage clinical concordance, chip data must be integrated with PBPK/PD models, digital twins, multi-omics pipelines, and AI-driven analytics. Best practices for model validation, uncertainty quantification, and regulatory submission of model-informed evidence are still evolving, particularly for complex, high-dimensional OOC datasets; in addition, AI-enabled pipelines must remain reproducible and sufficiently interpretable to support confidence in high-stakes decisions [18,32,72,84,93,95,115,118,125].
- Equity and access (cost and infrastructure constraints). Broader translational impact will also depend on whether OOC platforms can be made affordable and operationally practical beyond highly resourced settings. Low-cost microfluidic strategies and simplified platforms (e.g., paper- or textile-inspired approaches) highlight possible pathways toward wider accessibility and neglected-disease relevance without requiring fully automated, high-instrumentation workflows [44,45].
Clinical concordance thus represents the highest tier of OOC validation, defined by quantitative agreement between chip-derived readouts and patient-level outcomes. Demonstrating this alignment establishes confidence that OOCs can replace or supplement animal and static in vitro assays within defined regulatory contexts of use. As summarized in Table 6, concordance has now been shown across heart, kidney, lung, liver, brain, and emerging hematologic and retinal systems [30,74,79,80,81,89,90,91,92,94,97,99,100,101,102,103,106,107,108,109,110,111,112,127]. Continued harmonization of validation standards, expansion of reference drug libraries, cross-laboratory benchmarking initiatives, and integration with AI-enabled, multi-omics-driven modeling frameworks will be essential to sustain this translational trajectory and enable regulatory confidence in OOC-based decision frameworks [29,30,33,93,95,96,98,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126].
6. Conclusions
Organ-on-a-Chip (OOC) and related microphysiological systems have evolved from proof-of-concept microfluidic devices to data-rich translational platforms that can inform real decisions in drug discovery and development. Advances in materials, fabrication, and microfluidic design now support long-term culture, controlled mechanical cues, and integration of vascular, immune, and organoid components, while multi-sensor chips enable continuous readouts of barrier integrity, metabolism, electrophysiology, and secreted biomarkers. Across vascular, pulmonary, gastrointestinal, neural, cardiac, renal, hepatic, cutaneous, and tumor models, these technologies collectively demonstrate that OOCs can capture human-relevant physiology and disease mechanisms in a reproducible, experimentally tractable format. For Biosensors-relevant translation, the key differentiator is not only physiological fidelity but also measurement validity, namely traceable, time-resolved readouts with defined operating ranges and cross-site comparability that convert biology into decision-grade data.
A growing body of evidence supports quantitative clinical concordance in defined contexts of use. Representative benchmarking studies report cardiac platforms achieving AUROC values exceeding 0.85 for torsadogenic risk classification; other studies show that kidney chips can improve prediction of transporter-mediated clearance and nephrotoxicity; and lung, liver, and brain/blood–brain barrier devices reproduce barrier function, cytokine responses, and permeability in line with patient or high-fidelity ex vivo data. Coupled with physiologically based pharmacokinetic/pharmacodynamic (PBPK/PD) modeling and in vitro–in vivo extrapolation (IVIVE), multi-organ systems are beginning to close the loop between microfluidic readouts and whole-body exposure–response relationships. Collectively, these examples support the view that OOCs can move beyond descriptive biology toward decision-relevant tools in safety pharmacology, ADME, and precision medicine.
At the same time, OOCs are becoming intrinsically computational platforms. High-content imaging, electrophysiology, and multi-omics generate data volumes that require artificial intelligence (AI) and machine learning for harmonization, feature extraction, and prediction. Deep learning models trained on cardiac field potentials, blood–brain barrier permeability data, or tumor/organoid morphologies illustrate how AI can enhance endpoint detection, reduce inter-laboratory variability, and support digital twins that couple chip data to in silico simulations. In this view, embedded sensors, acquisition hardware/software, preprocessing, and AI models form a single measurement chain, and failure to control drift, batch effects, or dataset shift can undermine apparent concordance even when the underlying biology is sound. Realizing this potential will depend on treating AI pipelines, multi-omics workflows, and digital-twin models as integral parts of the assay, subject to the same requirements for transparency, validation, and version control as the physical chips themselves.
Looking ahead, broad adoption of OOC technologies will depend less on incremental technical novelty and more on closing several translational gaps:
- Standardized engineering and manufacturing – harmonized materials, fabrication workflows, and microfluidic parameters that support industrial-scale, quality-controlled production.
- Robust, transparent validation frameworks – fit-for-purpose criteria spanning analytical performance, biological fidelity, and clinical concordance, supported by structured reporting standards and shared reference compound panels.
- Integrated AI and multi-omics that are interpretable and auditable – algorithms and data pipelines that can be explained, benchmarked, versioned, and stress-tested for bias and robustness in regulatory settings.
- Physiologically realistic multi-organ and immune-competent systems – platforms that maintain stable, human-relevant interactions across tissues, immune compartments, and microbiome where appropriate.
- Data and ecosystem infrastructure – curated databases, open benchmarking studies, and cross-site collaborations that enable reproducibility, meta-analysis, and continuous refinement of models and digital twins.
By explicitly linking engineering innovation to quantitative clinical concordance and AI-enabled analysis, OOCs are positioned to reduce reliance on animal testing, de-risk development pipelines, and enable more personalized, mechanism-informed therapy selection. Organs-on-chips now sit at the intersection of engineering, computational modeling, and clinical science; their ultimate success will be measured not by how closely they mimic native tissues in isolation, but by how reliably they improve human outcomes and reduce development risk across the therapeutic lifecycle.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviation | Definition |
| ADME | Absorption–distribution–metabolism–excretion |
| ADME–Tox | Absorption–distribution–metabolism–excretion–toxicity |
| AI | Artificial intelligence |
| ALI | Air–liquid interface |
| AUC | Area under the concentration–time curve |
| AUROC | Area under the receiver operating characteristic curve |
| BAL | Bronchoalveolar lavage |
| BBB | Blood–brain barrier |
| CFD | Computational fluid dynamics |
| Cmax | Maximum plasma concentration |
| CNS | Central nervous system |
| COC | Cyclic olefin copolymer |
| COPD | Chronic obstructive pulmonary disease |
| CYP | Cytochrome P450 |
| DDI | Drug–drug interaction |
| DILI | Drug-induced liver injury |
| DigiLoCS | Digital Liver-on-Chip Simulator |
| ECG | Electrocardiogram |
| ECM | Extracellular matrix |
| EEG | Electroencephalography |
| FDA | U.S. Food and Drug Administration |
| GLP | Good Laboratory Practice |
| GIVReSt | Good In Vitro Reporting Standards |
| hERG | human Ether-à-go-go–related gene |
| IBD | Inflammatory bowel disease |
| iPSC | Induced pluripotent stem cell |
| IVIVE | In vitro–in vivo extrapolation |
| MDAR | Materials Design Analysis Reporting |
| MEA | Multi-electrode array |
| MEMS | Microelectromechanical systems |
| MIAME | Minimum Information About a Microarray Experiment |
| ML | Machine learning |
| MPS | Microphysiological system(s) |
| NAM | New approach methodology |
| NSAID | Nonsteroidal anti-inflammatory drug |
| OAT | Organic anion transporter |
| OCT | Organic cation transporter |
| OOC | Organ-on-a-Chip |
| OOCDB | Organs-on-a-Chip DataBase |
| PBPK | Physiologically based pharmacokinetic modeling |
| PBPK/PD | Physiologically based pharmacokinetic/pharmacodynamic modeling |
| PCL | Polycaprolactone |
| PD | Pharmacodynamics |
| PDMS | Polydimethylsiloxane |
| PEG | Polyethylene glycol |
| P-gp | P-glycoprotein |
| PET | Positron emission tomography |
| PK | Pharmacokinetics |
| PK/PD | Pharmacokinetics/pharmacodynamics |
| PLA | Polylactic acid |
| QC | Quality control |
| QT | QT interval |
| RMSE | Root-mean-square error |
| TEER | Transepithelial electrical resistance |
| VEGF | Vascular endothelial growth factor |
Author Contributions
Nilanjan Roy: conceptualization, literature curation, writing (original draft), writing (review and editing). Luca Cucullo: supervision, critical review and editing, journal targeting guidance. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
Not applicable
Acknowledgments
Figures were created with BioRender.com.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- DiMasi, J.A.; Grabowski, H.G.; Hansen, R.W. Innovation in the Pharmaceutical Industry: New Estimates of R&D Costs. Journal of Health Economics 2016, 47, 20–33. [Google Scholar] [CrossRef]
- Hay, M.; Thomas, D.W.; Craighead, J.L.; Economides, C.; Rosenthal, J. Clinical Development Success Rates for Investigational Drugs. Nat Biotechnol 2014, 32, 40–51. [Google Scholar] [CrossRef]
- Waring, M.J.; Arrowsmith, J.; Leach, A.R.; Leeson, P.D.; Mandrell, S.; Owen, R.M.; Pairaudeau, G.; Pennie, W.D.; Pickett, S.D.; Wang, J.; et al. An Analysis of the Attrition of Drug Candidates from Four Major Pharmaceutical Companies. Nat Rev Drug Discov 2015, 14, 475–486. [Google Scholar] [CrossRef]
- Edmondson, R.; Broglie, J.J.; Adcock, A.F.; Yang, L. Three-Dimensional Cell Culture Systems and Their Applications in Drug Discovery and Cell-Based Biosensors. ASSAY and Drug Development Technologies 2014, 12, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Antoni, D.; Burckel, H.; Josset, E.; Noel, G. Three-Dimensional Cell Culture: A Breakthrough in Vivo. IJMS 2015, 16, 5517–5527. [Google Scholar] [CrossRef]
- Pampaloni, F.; Reynaud, E.G.; Stelzer, E.H.K. The Third Dimension Bridges the Gap between Cell Culture and Live Tissue. Nat Rev Mol Cell Biol 2007, 8, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Van Der Worp, H.B.; Howells, D.W.; Sena, E.S.; Porritt, M.J.; Rewell, S.; O’Collins, V.; Macleod, M.R. Can Animal Models of Disease Reliably Inform Human Studies? PLoS Med 2010, 7, e1000245. [Google Scholar] [CrossRef]
- Seok, J.; Warren, H.S.; Cuenca, A.G.; Mindrinos, M.N.; Baker, H.V.; Xu, W.; Richards, D.R.; McDonald-Smith, G.P.; Gao, H.; Hennessy, L.; et al. Genomic Responses in Mouse Models Poorly Mimic Human Inflammatory Diseases. Proc. Natl. Acad. Sci. U.S.A. 2013, 110, 3507–3512. [Google Scholar] [CrossRef]
- Martignoni, M.; Groothuis, G.M.M.; De Kanter, R. Species Differences between Mouse, Rat, Dog, Monkey and Human CYP-Mediated Drug Metabolism, Inhibition and Induction. Expert Opinion on Drug Metabolism & Toxicology 2006, 2, 875–894. [Google Scholar] [CrossRef]
- Ransohoff, R.M. All (Animal) Models (of Neurodegeneration) Are Wrong. Are They Also Useful? Journal of Experimental Medicine 2018, 215, 2955–2958. [Google Scholar] [CrossRef]
- Russell, W.M.S.; Burch, R.L. The Principles of Humane Experimental Technique; Universities Federation for Animal Welfare (UFAW): Potters Bar, UK, 1992; ISBN 9780900767784. [Google Scholar]
- Tannenbaum, J.; Bennett, B.T. Russell and Burch’s 3Rs Then and Now: The Need for Clarity in Definition and Purpose. J Am Assoc Lab Anim Sci 2015, 54, 120–132. [Google Scholar]
- Bhatia, S.N.; Ingber, D.E. Microfluidic Organs-on-Chips. Nat Biotechnol 2014, 32, 760–772. [Google Scholar] [CrossRef]
- Zhang, B.; Korolj, A.; Lai, B.F.L.; Radisic, M. Advances in Organ-on-a-Chip Engineering. Nat Rev Mater 2018, 3, 257–278. [Google Scholar] [CrossRef]
- Ingber, D.E. Human Organs-on-Chips for Disease Modelling, Drug Development and Personalized Medicine. Nat Rev Genet 2022, 23, 467–491. [Google Scholar] [CrossRef]
- Consolidated Appropriations Act, 2023; Public Law 117–328, Sec. 3209 (FDA Modernization Act 2.0). 29 December 2022. Available online: https://www.govinfo.gov/content/pkg/PLAW-117publ328/html/PLAW-117publ328.htm (accessed on 2 February 2026).
- Petersen, E. Technical Framework for Enabling High-Quality Measurements in New Approach Methodologies (NAMs). ALTEX 2022. [Google Scholar] [CrossRef]
- Deng, S.; Li, C.; Cao, J.; Cui, Z.; Du, J.; Fu, Z.; Yang, H.; Chen, P. Organ-on-a-Chip Meets Artificial Intelligence in Drug Evaluation. Theranostics 2023, 13, 4526–4558. [Google Scholar] [CrossRef]
- Huh, D.; Matthews, B.D.; Mammoto, A.; Montoya-Zavala, M.; Hsin, H.Y.; Ingber, D.E. Reconstituting Organ-Level Lung Functions on a Chip. Science 2010, 328, 1662–1668. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Huh, D.; Hamilton, G.; Ingber, D.E. Human Gut-on-a-Chip Inhabited by Microbial Flora That Experiences Intestinal Peristalsis-like Motions and Flow. Lab Chip 2012, 12, 2165. [Google Scholar] [CrossRef]
- Pediaditakis, I.; Kodella, K.R.; Manatakis, D.V.; Le, C.Y.; Barthakur, S.; Sorets, A.; Gravanis, A.; Ewart, L.; Rubin, L.L.; Manolakos, E.S.; et al. A Microengineered Brain-Chip to Model Neuroinflammation in Humans. iScience 2022, 25, 104813. [Google Scholar] [CrossRef] [PubMed]
- Ronaldson-Bouchard, K.; Ma, S.P.; Yeager, K.; Chen, T.; Song, L.; Sirabella, D.; Morikawa, K.; Teles, D.; Yazawa, M.; Vunjak-Novakovic, G. Advanced Maturation of Human Cardiac Tissue Grown from Pluripotent Stem Cells. Nature 2018, 556, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Nieskens, T.T.G.; Wilmer, M.J. Kidney-on-a-Chip Technology for Renal Proximal Tubule Tissue Reconstruction. European Journal of Pharmacology 2016, 790, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Whitesides, G.M. SOFT LITHOGRAPHY. Annu. Rev. Mater. Sci. 1998, 28, 153–184. [Google Scholar] [CrossRef]
- Qin, D.; Xia, Y.; Whitesides, G.M. Soft Lithography for Micro- and Nanoscale Patterning. Nat Protoc 2010, 5, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Liu, J.; Wang, X.; Feng, L.; Wu, J.; Zhu, X.; Wen, W.; Gong, X. Organ-on-a-Chip: Recent Breakthroughs and Future Prospects. BioMed Eng OnLine 2020, 19, 9. [Google Scholar] [CrossRef]
- Low, L.A.; Mummery, C.; Berridge, B.R.; Austin, C.P.; Tagle, D.A. Organs-on-Chips: Into the next Decade. Nat Rev Drug Discov 2021, 20, 345–361. [Google Scholar] [CrossRef]
- Heringa, M. The Value of Organs-on-Chip for Regulatory Safety Assessment. ALTEX 2019. [Google Scholar] [CrossRef]
- Aravindakshan, M.R.; Mandal, C.; Pothen, A.; Schaller, S.; Maass, C. DigiLoCS: A Leap Forward in Predictive Organ-on-Chip Simulations. PLoS ONE 2025, 20, e0314083. [Google Scholar] [CrossRef]
- Liu, Q.; Song, K. ProgCAE: A Deep Learning-Based Method That Integrates Multi-Omics Data to Predict Cancer Subtypes. Briefings in Bioinformatics 2023, 24, bbad196. [Google Scholar] [CrossRef]
- Serrano, R.; Feyen, D.A.M.; Bruyneel, A.A.N.; Hnatiuk, A.P.; Vu, M.M.; Amatya, P.L.; Perea-Gil, I.; Prado, M.; Seeger, T.; Wu, J.C.; et al. A Deep Learning Platform to Assess Drug Proarrhythmia Risk. Cell Stem Cell 2023, 30, 86–95.e4. [Google Scholar] [CrossRef] [PubMed]
- Fatehullah, A.; Tan, S.H.; Barker, N. Organoids as an in Vitro Model of Human Development and Disease. Nat Cell Biol 2016, 18, 246–254. [Google Scholar] [CrossRef]
- Clapp, N.; Amour, A.; Rowan, W.C.; Candarlioglu, P.L. Organ-on-Chip Applications in Drug Discovery: An End User Perspective. Biochemical Society Transactions 2021, 49, 1881–1890. [Google Scholar] [CrossRef]
- Nahak, B.K.; Mishra, A.; Preetam, S.; Tiwari, A. Advances in Organ-on-a-Chip Materials and Devices. ACS Appl. Bio Mater. 2022, 5, 3576–3607. [Google Scholar] [CrossRef]
- Osório, L.A.; Silva, E.; Mackay, R.E. A Review of Biomaterials and Scaffold Fabrication for Organ-on-a-Chip (OOAC) Systems. Bioengineering 2021, 8, 113. [Google Scholar] [CrossRef] [PubMed]
- Toepke, M.W.; Beebe, D.J. PDMS Absorption of Small Molecules and Consequences in Microfluidic Applications. Lab Chip 2006, 6, 1484. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, Q.; Zourob, M. Organ-on-a-Chip Engineering: Toward Bridging the Gap between Lab and Industry. Biomicrofluidics 2020, 14, 041501. [Google Scholar] [CrossRef]
- Ferreira, M.J.; Colombani, S.; Bernardin, A.; Lacampagne, A.; Pasquié, J.-L.; Costa, P.F.; Charlot, B.; Meli, A.C. Advancing Organ-on-Chip Systems: The Role of Microfluidics in Neuro-Cardiac Research. Current Research in Pharmacology and Drug Discovery 2025, 9, 100227. [Google Scholar] [CrossRef]
- Corral-Nájera, K.; Chauhan, G.; Serna-Saldívar, S.O.; Martínez-Chapa, S.O.; Aeinehvand, M.M. Polymeric and Biological Membranes for Organ-on-a-Chip Devices. Microsyst Nanoeng 2023, 9, 107. [Google Scholar] [CrossRef]
- Giri, K.; Tsao, C.-W. Recent Advances in Thermoplastic Microfluidic Bonding. Micromachines 2022, 13, 486. [Google Scholar] [CrossRef]
- Shakeri, A.; Khan, S.; Jarad, N.A.; Didar, T.F. The Fabrication and Bonding of Thermoplastic Microfluidics: A Review. Materials 2022, 15, 6478. [Google Scholar] [CrossRef]
- Papamichail, L.; Koch, L.S.; Veerman, D.; Broersen, K.; Van Der Meer, A.D. Organoids-on-a-Chip: Microfluidic Technology Enables Culture of Organoids with Enhanced Tissue Function and Potential for Disease Modeling. Front. Bioeng. Biotechnol. 2025, 13, 1515340. [Google Scholar] [CrossRef]
- Cho, Y.; You, J.; Lee, J.H. Natural Polymer-Based Hydrogel Platforms for Organoid and Microphysiological Systems: Mechanistic Insights and Translational Perspectives. Polymers 2025, 17, 2109. [Google Scholar] [CrossRef] [PubMed]
- Yetisen, A.K.; Akram, M.S.; Lowe, C.R. Paper-Based Microfluidic Point-of-Care Diagnostic Devices. Lab Chip 2013, 13, 2210. [Google Scholar] [CrossRef]
- Hanze, M.; Piper, A.; Hamedi, M.M. Stitched Textile-Based Microfluidics for Wearable Devices. Lab Chip 2025, 25, 28–40. [Google Scholar] [CrossRef]
- Pisapia, F.; Balachandran, W.; Rasekh, M. Organ-on-a-Chip: Design and Simulation of Various Microfluidic Channel Geometries for the Influence of Fluid Dynamic Parameters. Applied Sciences 2022, 12, 3829. [Google Scholar] [CrossRef]
- Farhang Doost, N.; Srivastava, S.K. A Comprehensive Review of Organ-on-a-Chip Technology and Its Applications. Biosensors 2024, 14, 225. [Google Scholar] [CrossRef]
- Liu, X.; Fang, J.; Huang, S.; Wu, X.; Xie, X.; Wang, J.; Liu, F.; Zhang, M.; Peng, Z.; Hu, N. Tumor-on-a-Chip: From Bioinspired Design to Biomedical Application. Microsyst Nanoeng 2021, 7, 50. [Google Scholar] [CrossRef]
- Leung, C.M.; De Haan, P.; Ronaldson-Bouchard, K.; Kim, G.-A.; Ko, J.; Rho, H.S.; Chen, Z.; Habibovic, P.; Jeon, N.L.; Takayama, S.; et al. A Guide to the Organ-on-a-Chip. Nat Rev Methods Primers 2022, 2, 33. [Google Scholar] [CrossRef]
- Rogal, J.; Schlünder, K.; Loskill, P. Developer’s Guide to an Organ-on-Chip Model. ACS Biomater. Sci. Eng. 2022, 8, 4643–4647. [Google Scholar] [CrossRef]
- Wysoczański, B.; Świątek, M.; Wójcik-Gładysz, A. Organ-on-a-Chip Models—New Possibilities in Experimental Science and Disease Modeling. Biomolecules 2024, 14, 1569. [Google Scholar] [CrossRef] [PubMed]
- Nunes, G.A.M.D.A.; Da Silva, A.K.A.; Faria, R.M.; Santos, K.S.; Aguiar, A.D.C.; Barreto Mota Da Costa, L.; Luz, G.V.D.S.; Carneiro, M.L.B.; Rosa, M.F.F.; Joanitti, G.A.; et al. State-of-the-Art Organ-on-Chip Models and Designs for Medical Applications: A Systematic Review. Biomimetics 2025, 10, 524. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Mishra, A.; Mathur, A.; Shastri, S.; Nizam, A.; Rizwan, A.; Dadial, A.S.; Firdous, A.; Hassan, H. Advancement of Organ-on-Chip towards next Generation Medical Technology. Biosensors and Bioelectronics: X 2024, 18, 100480. [Google Scholar] [CrossRef]
- Ren, J.; Wang, Z.; Du, N.; Cheng, W.; Ju, L.A. Charting the Course of Blood Flow: Vessel-on-a-Chip Technologies in Thrombosis Studies. Microstructures 2024, 4. [Google Scholar] [CrossRef]
- Shakeri, A.; Wang, Y.; Zhao, Y.; Landau, S.; Perera, K.; Lee, J.; Radisic, M. Engineering Organ-on-a-Chip Systems for Vascular Diseases. ATVB 2023, 43, 2241–2255. [Google Scholar] [CrossRef]
- Kim, S.; Kim, W.; Lim, S.; Jeon, J. Vasculature-On-A-Chip for In Vitro Disease Models. Bioengineering 2017, 4, 8. [Google Scholar] [CrossRef]
- Xu, Y.; Yu, G.; Nie, R.; Wu, Z. Microfluidic Systems toward Blood Hemostasis Monitoring and Thrombosis Diagnosis: From Design Principles to Micro/Nano Fabrication Technologies. VIEW 2022, 3, 20200183. [Google Scholar] [CrossRef]
- Yokoi, F.; Deguchi, S.; Takayama, K. Advancing Intestinal Disease Research Using Gut-on-a-Chip. Regenerative Therapy 2025, 29, 541–550. [Google Scholar] [CrossRef]
- Liu, Y.; Li, J.; Zhou, J.; Liu, X.; Li, H.; Lu, Y.; Lin, B.; Li, X.; Liu, T. Angiogenesis and Functional Vessel Formation Induced by Interstitial Flow and Vascular Endothelial Growth Factor Using a Microfluidic Chip. Micromachines 2022, 13, 225. [Google Scholar] [CrossRef]
- Ofori-Kwafo, A.; Sigdel, I.; Al Mamun, E.; Zubcevic, J.; Tang, Y. Gut-on-a-chip Platforms: Bridging in Vitro and in Vivo Models for Advanced Gastrointestinal Research. Physiological Reports 2025, 13, e70356. [Google Scholar] [CrossRef]
- Guarino, V.; Zizzari, A.; Bianco, M.; Gigli, G.; Moroni, L.; Arima, V. Advancements in Modelling Human Blood Brain-Barrier on a Chip. Biofabrication 2023, 15, 022003. [Google Scholar] [CrossRef]
- Taavitsainen, S.; Juuti-Uusitalo, K.; Kurppa, K.; Lindfors, K.; Kallio, P.; Kellomäki, M. Gut-on-Chip Devices as Intestinal Inflammation Models and Their Future for Studying Multifactorial Diseases. Front. Lab. Chip. Technol. 2024, 2, 1337945. [Google Scholar] [CrossRef]
- Zhang, D.; Qiao, L. Intestine-on-a-chip for Intestinal Disease Study and Pharmacological Research. VIEW 2023, 4, 20220037. [Google Scholar] [CrossRef]
- Thomas, D.P.; Zhang, J.; Nguyen, N.-T.; Ta, H.T. Microfluidic Gut-on-a-Chip: Fundamentals and Challenges. Biosensors 2023, 13, 136. [Google Scholar] [CrossRef] [PubMed]
- Bein, A.; Kim, S.; Goyal, G.; Cao, W.; Fadel, C.; Naziripour, A.; Sharma, S.; Swenor, B.; LoGrande, N.; Nurani, A.; et al. Enteric Coronavirus Infection and Treatment Modeled With an Immunocompetent Human Intestine-On-A-Chip. Front. Pharmacol. 2021, 12, 718484. [Google Scholar] [CrossRef]
- Deguchi, S.; Takayama, K. State-of-the-Art Liver Disease Research Using Liver-on-a-Chip. Inflamm Regener 2022, 42, 62. [Google Scholar] [CrossRef]
- Castiglione, H.; Vigneron, P.-A.; Baquerre, C.; Yates, F.; Rontard, J.; Honegger, T. Human Brain Organoids-on-Chip: Advances, Challenges, and Perspectives for Preclinical Applications. Pharmaceutics 2022, 14, 2301. [Google Scholar] [CrossRef]
- Kim, J.; Yoon, T.; Kim, P.; Bekhbat, M.; Kang, S.M.; Rho, H.S.; Ahn, S.I.; Kim, Y. Manufactured Tissue-to-Tissue Barrier Chip for Modeling the Human Blood–Brain Barrier and Regulation of Cellular Trafficking. Lab Chip 2023, 23, 2990–3001. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Aleman, J.; Arneri, A.; Bersini, S.; Piraino, F.; Shin, S.R.; Dokmeci, M.R.; Khademhosseini, A. From Cardiac Tissue Engineering to Heart-on-a-Chip: Beating Challenges. Biomed. Mater. 2015, 10, 034006. [Google Scholar] [CrossRef]
- Yang, Y.; Sheng, J.; Sheng, F.; Liang, X.; Ma, C.; Chen, R.; Wang, S.; Qian, X. Advances and Applications of Organoid-on-a-Chip in Disease Modeling. Analyst 2025, 150, 4870–4881. [Google Scholar] [CrossRef]
- Wang, Y.; Marucci, L.; Homer, M.E. In Silico Modelling of Organ-on-a-Chip Devices: An Overview. Front. Bioeng. Biotechnol. 2025, 12, 1520795. [Google Scholar] [CrossRef] [PubMed]
- Alver, C.G.; Drabbe, E.; Ishahak, M.; Agarwal, A. Roadblocks Confronting Widespread Dissemination and Deployment of Organs on Chips. Nat Commun 2024, 15, 5118. [Google Scholar] [CrossRef] [PubMed]
- Maoz, B.M. Brain-on-a-Chip: Characterizing the next Generation of Advanced in Vitro Platforms for Modeling the Central Nervous System. APL Bioengineering 2021, 5, 030902. [Google Scholar] [CrossRef] [PubMed]
- Keuper-Navis, M.; Walles, M.; Poller, B.; Myszczyszyn, A.; Van Der Made, T.K.; Donkers, J.; Eslami Amirabadi, H.; Wilmer, M.J.; Aan, S.; Spee, B.; et al. The Application of Organ-on-Chip Models for the Prediction of Human Pharmacokinetic Profiles during Drug Development. Pharmacological Research 2023, 195, 106853. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Gust, M.; Ferrell, N. Kidney-on-a-Chip: Mechanical Stimulation and Sensor Integration. Sensors 2022, 22, 6889. [Google Scholar] [CrossRef] [PubMed]
- Romito, A.; Cobellis, G. Pluripotent Stem Cells: Current Understanding and Future Directions. Stem Cells International 2016, 2016, 9451492. [Google Scholar] [CrossRef]
- Fu, J.; Qiu, H.; Tan, C.S. Microfluidic Liver-on-a-Chip for Preclinical Drug Discovery. Pharmaceutics 2023, 15, 1300. [Google Scholar] [CrossRef]
- Sutterby, E.; Thurgood, P.; Baratchi, S.; Khoshmanesh, K.; Pirogova, E. Microfluidic Skin-on-a-Chip Models: Toward Biomimetic Artificial Skin. Small 2020, 16, 2002515. [Google Scholar] [CrossRef]
- Ribeiro, A.J.S.; Yang, X.; Patel, V.; Madabushi, R.; Strauss, D.G. Liver Microphysiological Systems for Predicting and Evaluating Drug Effects. Clinical Pharmacology & Therapeutics 2019, 106, 139–147. [Google Scholar] [CrossRef]
- Ewart, L.; Dehne, E.-M.; Fabre, K.; Gibbs, S.; Hickman, J.; Hornberg, E.; Ingelman-Sundberg, M.; Jang, K.-J.; Jones, D.R.; Lauschke, V.M.; et al. Application of Microphysiological Systems to Enhance Safety Assessment in Drug Discovery. Annu. Rev. Pharmacol. Toxicol. 2018, 58, 65–82. [Google Scholar] [CrossRef]
- Blinova, K.; Dang, Q.; Millard, D.; Smith, G.; Pierson, J.; Guo, L.; Brock, M.; Lu, H.R.; Kraushaar, U.; Zeng, H.; et al. International Multisite Study of Human-Induced Pluripotent Stem Cell-Derived Cardiomyocytes for Drug Proarrhythmic Potential Assessment. Cell Reports 2018, 24, 3582–3592. [Google Scholar] [CrossRef]
- Isoherranen, N.; Madabushi, R.; Huang, S. Emerging Role of Organ-on-a-Chip Technologies in Quantitative Clinical Pharmacology Evaluation. Clinical Translational Sci 2019, 12, 113–121. [Google Scholar] [CrossRef]
- Sachs, N.; De Ligt, J.; Kopper, O.; Gogola, E.; Bounova, G.; Weeber, F.; Balgobind, A.V.; Wind, K.; Gracanin, A.; Begthel, H.; et al. A Living Biobank of Breast Cancer Organoids Captures Disease Heterogeneity. Cell 2018, 172, 373–386.e10. [Google Scholar] [CrossRef]
- Clevers, H. Modeling Development and Disease with Organoids. Cell 2016, 165, 1586–1597. [Google Scholar] [CrossRef] [PubMed]
- The ORCHID partners; Mastrangeli, M.; Millet, S.; Van Den Eijnden-van Raaij, J. Organ-on-Chip in Development: Towards a Roadmap for Organs-on-Chip. ATLEX 2019, 650–668. [Google Scholar] [CrossRef]
- Marx, U. Biology-Inspired Microphysiological Systems to Advance Medicines for Patient Benefit and Animal Welfare. ALTEX 2020. [Google Scholar] [CrossRef]
- Allwardt, V.; Ainscough, A.J.; Viswanathan, P.; Sherrod, S.D.; McLean, J.A.; Haddrick, M.; Pensabene, V. Translational Roadmap for the Organs-on-a-Chip Industry toward Broad Adoption. Bioengineering 2020, 7, 112. [Google Scholar] [CrossRef]
- Van Der Zalm, A.J.; Barroso, J.; Browne, P.; Casey, W.; Gordon, J.; Henry, T.R.; Kleinstreuer, N.C.; Lowit, A.B.; Perron, M.; Clippinger, A.J. A Framework for Establishing Scientific Confidence in New Approach Methodologies. Arch Toxicol 2022, 96, 2865–2879. [Google Scholar] [CrossRef]
- Pamies, D.; Ekert, J.; Zurich, M.-G.; Frey, O.; Werner, S.; Piergiovanni, M.; Freedman, B.S.; Keong Teo, A.K.; Erfurth, H.; Reyes, D.R.; et al. Recommendations on Fit-for-Purpose Criteria to Establish Quality Management for Microphysiological Systems and for Monitoring Their Reproducibility. Stem Cell Reports 2024, 19, 604–617. [Google Scholar] [CrossRef]
- Reyes, D.R.; Esch, M.B.; Ewart, L.; Nasiri, R.; Herland, A.; Sung, K.; Piergiovanni, M.; Lucchesi, C.; Shoemaker, J.T.; Vukasinovic, J.; et al. From Animal Testing to in Vitro Systems: Advancing Standardization in Microphysiological Systems. Lab Chip 2024, 24, 1076–1087. [Google Scholar] [CrossRef]
- Ouedraogo, G.; Alépée, N.; Tan, B.; Roper, C.S. A Call to Action: Advancing New Approach Methodologies (NAMs) in Regulatory Toxicology through a Unified Framework for Validation and Acceptance. Regulatory Toxicology and Pharmacology 2025, 162, 105904. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.; Loskill, P.; Shao, K.; Huebsch, N.; Hong, S.; Marcus, S.G.; Marks, N.; Mandegar, M.; Conklin, B.R.; Lee, L.P.; et al. Human iPSC-Based Cardiac Microphysiological System For Drug Screening Applications. Sci Rep 2015, 5, 8883. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-Y.; Evangelista, E.A.; Yang, J.; Kelly, E.J.; Yeung, C.K. Kidney Organoid and Microphysiological Kidney Chip Models to Accelerate Drug Development and Reduce Animal Testing. Front. Pharmacol. 2021, 12, 695920. [Google Scholar] [CrossRef]
- Brown, J.A.; Pensabene, V.; Markov, D.A.; Allwardt, V.; Neely, M.D.; Shi, M.; Britt, C.M.; Hoilett, O.S.; Yang, Q.; Brewer, B.M.; et al. Recreating Blood-Brain Barrier Physiology and Structure on Chip: A Novel Neurovascular Microfluidic Bioreactor. Biomicrofluidics 2015, 9, 054124. [Google Scholar] [CrossRef]
- Bang, S.; Lee, S.-R.; Ko, J.; Son, K.; Tahk, D.; Ahn, J.; Im, C.; Jeon, N.L. A Low Permeability Microfluidic Blood-Brain Barrier Platform with Direct Contact between Perfusable Vascular Network and Astrocytes. Sci Rep 2017, 7, 8083. [Google Scholar] [CrossRef]
- Park, T.-E.; Mustafaoglu, N.; Herland, A.; Hasselkus, R.; Mannix, R.; FitzGerald, E.A.; Prantil-Baun, R.; Watters, A.; Henry, O.; Benz, M.; et al. Hypoxia-Enhanced Blood-Brain Barrier Chip Recapitulates Human Barrier Function and Shuttling of Drugs and Antibodies. Nat Commun 2019, 10, 2621. [Google Scholar] [CrossRef]
- Arjmand, B.; Hamidpour, S.K.; Tayanloo-Beik, A.; Goodarzi, P.; Aghayan, H.R.; Adibi, H.; Larijani, B. Machine Learning: A New Prospect in Multi-Omics Data Analysis of Cancer. Front. Genet. 2022, 13, 824451. [Google Scholar] [CrossRef]
- Graf, K.; Murrieta-Coxca, J.M.; Vogt, T.; Besser, S.; Geilen, D.; Kaden, T.; Bothe, A.-K.; Morales-Prieto, D.M.; Amiri, B.; Schaller, S.; et al. Digital Twin-Enhanced Three-Organ Microphysiological System for Studying Drug Pharmacokinetics in Pregnant Women. Front. Pharmacol. 2025, 16, 1528748. [Google Scholar] [CrossRef]
- Li, X.; Wang, H.; You, X.; Zhao, G. Organoids-on-Chips Technology: Unveiling New Perspectives in Rare-Disease Research. IJMS 2025, 26, 4367. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, J.; Bai, H.; Wang, H.; Hao, S.; Ding, Y.; Peng, B.; Zhang, J.; Li, L.; Huang, W. An Overview of Organs-on-Chips Based on Deep Learning. Research 2022, 2022, 2022/9869518. [Google Scholar] [CrossRef]
- Dai, M.; Xiao, G.; Shao, M.; Zhang, Y.S. The Synergy between Deep Learning and Organs-on-Chips for High-Throughput Drug Screening: A Review. Biosensors 2023, 13, 389. [Google Scholar] [CrossRef] [PubMed]
- Movčana, V.; Strods, A.; Narbute, K.; Rūmnieks, F.; Rimša, R.; Mozoļevskis, G.; Ivanovs, M.; Kadiķis, R.; Zviedris, K.G.; Leja, L.; et al. Organ-On-A-Chip (OOC) Image Dataset for Machine Learning and Tissue Model Evaluation. Data 2024, 9, 28. [Google Scholar] [CrossRef]
- Gao, W.; Wang, C.; Li, Q.; Zhang, X.; Yuan, J.; Li, D.; Sun, Y.; Chen, Z.; Gu, Z. Application of Medical Imaging Methods and Artificial Intelligence in Tissue Engineering and Organ-on-a-Chip. Front. Bioeng. Biotechnol. 2022, 10, 985692. [Google Scholar] [CrossRef] [PubMed]
- Macleod, M.; Collings, A.M.; Graf, C.; Kiermer, V.; Mellor, D.; Swaminathan, S.; Sweet, D.; Vinson, V. The MDAR (Materials Design Analysis Reporting) Framework for Transparent Reporting in the Life Sciences. Proc. Natl. Acad. Sci. U.S.A. 2021, 118, e2103238118. [Google Scholar] [CrossRef]
- Hartung, T. Toward Good in Vitro Reporting Standards. ALTEX 2019, 36, 3–17. [Google Scholar] [CrossRef]
- Guidance for Good In Vitro Reporting Standards (GIVReSt) – A Draft for Stakeholder Discussion and Background Documentation. ALTEX 2025, 42. [CrossRef]
- Brazma, A.; Hingamp, P.; Quackenbush, J.; Sherlock, G.; Spellman, P.; Stoeckert, C.; Aach, J.; Ansorge, W.; Ball, C.A.; Causton, H.C.; et al. Minimum Information about a Microarray Experiment (MIAME)—toward Standards for Microarray Data. Nat Genet 2001, 29, 365–371. [Google Scholar] [CrossRef]
- Correa-Aguila, R.; Alonso-Pupo, N.; Hernández-Rodríguez, E.W. Multi-Omics Data Integration Approaches for Precision Oncology. Molecular Omics 2022, 18, 469–479. [Google Scholar] [CrossRef]
- Li, J.; Liang, W.; Chen, Z.; Li, X.; Gu, P.; Liu, A.; Chen, P.; Li, Q.; Mei, X.; Yang, J.; et al. OOCDB: A Comprehensive, Systematic, and Real-Time Organs-on-a-Chip Database. Genomics, Proteomics & Bioinformatics 2023, 21, 243–258. [Google Scholar] [CrossRef]
- Cirit, M.; Stokes, C.L. Maximizing the Impact of Microphysiological Systems with in Vitro – in Vivo Translation. Lab Chip 2018, 18, 1831–1837. [Google Scholar] [CrossRef] [PubMed]
- Torisawa, Y.; Spina, C.S.; Mammoto, T.; Mammoto, A.; Weaver, J.C.; Tat, T.; Collins, J.J.; Ingber, D.E. Bone Marrow–on–a–Chip Replicates Hematopoietic Niche Physiology in Vitro. Nat Methods 2014, 11, 663–669. [Google Scholar] [CrossRef]
- Achberger, K.; Probst, C.; Haderspeck, J.; Bolz, S.; Rogal, J.; Chuchuy, J.; Nikolova, M.; Cora, V.; Antkowiak, L.; Haq, W.; et al. Merging Organoid and Organ-on-a-Chip Technology to Generate Complex Multi-Layer Tissue Models in a Human Retina-on-a-Chip Platform. eLife 2019, 8, e46188. [Google Scholar] [CrossRef]
- Baker, T.K.; Van Vleet, T.R.; Mahalingaiah, P.K.; Grandhi, T.S.P.; Evers, R.; Ekert, J.; Gosset, J.R.; Chacko, S.A.; Kopec, A.K. The Current Status and Use of Microphysiological Systems by the Pharmaceutical Industry: The International Consortium for Innovation and Quality Microphysiological Systems Affiliate Survey and Commentary. Drug Metabolism and Disposition 2024, 52, 198–209. [Google Scholar] [CrossRef]
- Kopec, A.K.; Yokokawa, R.; Khan, N.; Horii, I.; Finley, J.E.; Bono, C.P.; Donovan, C.; Roy, J.; Harney, J.; Burdick, A.D.; et al. Microphysiological Systems in Early Stage Drug Development: Perspectives on Current Applications and Future Impact. J. Toxicol. Sci. 2021, 46, 99–114. [Google Scholar] [CrossRef]
- Hargrove-Grimes, P.; Low, L.A.; Tagle, D.A. Microphysiological Systems: Stakeholder Challenges to Adoption in Drug Development. Cells Tissues Organs 2022, 211, 269–281. [Google Scholar] [CrossRef]
- Yamazaki, D.; Ishida, S. Global Expansion of Microphysiological Systems (MPS) and Japan’s Initiatives: Innovation in Pharmaceutical Development and Path to Regulatory Acceptance. Drug Metabolism and Pharmacokinetics 2025, 60, 101047. [Google Scholar] [CrossRef] [PubMed]
- Levner, D.; Ewart, L. Integrating Liver-Chip Data into Pharmaceutical Decision-Making Processes. Expert Opinion on Drug Discovery 2023, 18, 1313–1320. [Google Scholar] [CrossRef]
- Surina, S.; Chmielewska, A.; Pratscher, B.; Freund, P.; Rodríguez-Rojas, A.; Burgener, I.A. Organ-on-a-Chip: A Roadmap for Translational Research in Human and Veterinary Medicine. IJMS 2025, 26, 10753. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, K.S.; Müller, I.; Malcomber, S.; Carmichael, P.L.; Bouwmeester, H. Implementing Organ-on-Chip in a next-Generation Risk Assessment of Chemicals: A Review. Arch Toxicol 2022, 96, 711–741. [Google Scholar] [CrossRef] [PubMed]
- Gow, A. Scientific Usefulness of New Approach Methodologies. Applied In Vitro Toxicology 2022, 8, 65–66. [Google Scholar] [CrossRef]
- Teixeira, S.G.; Houeto, P.; Gattacceca, F.; Petitcollot, N.; Debruyne, D.; Guerbet, M.; Guillemain, J.; Fabre, I.; Louin, G.; Salomon, V. National Reflection on Organs-on-Chip for Drug Development: New Regulatory Challenges. Toxicology Letters 2023, 388, 1–12. [Google Scholar] [CrossRef]
- European Commission; Joint Research Centre. Organ on Chip: Building a Roadmap towards Standardisation : Putting Science into Standards.; Publications Office: LU, 2021. [Google Scholar]
- Peck, R.W.; Hinojosa, C.D.; Hamilton, G.A. Organs-on-Chips in Clinical Pharmacology: Putting the Patient Into the Center of Treatment Selection and Drug Development. Clinical Pharmacology & Therapeutics 2020, 107, 181–185. [Google Scholar] [CrossRef]
- Tomlinson, L.; Ramsden, D.; Leite, S.B.; Beken, S.; Bonzo, J.A.; Brown, P.; Candarlioglu, P.L.; Chan, T.S.; Chen, E.; Choi, C.K.; et al. Considerations from an International Regulatory and Pharmaceutical Industry (IQ MPS Affiliate) Workshop on the Standardization of Complex In Vitro Models in Drug Development. Advanced Biology 2024, 8, 2300131. [Google Scholar] [CrossRef]
- Sillé, F.C.M.; Smirnova, L.; Hartung, T. Microphysiological Systems as a Pillar of the Human Exposome Project. Journal of Biological Chemistry 2025, 301, 110782. [Google Scholar] [CrossRef] [PubMed]
- Monga, A.; Jain, K.; Popli, H.; Telgote, P.; Kaur, G.; Rizwani, F.; Chauhan, R.; Kaur, D.; Chauhan, A.; Tuli, H.S. Organs-on-Chips: Revolutionizing Biomedical Research. Biophysica 2025, 5, 38. [Google Scholar] [CrossRef]
- Ma, C.; Peng, Y.; Li, H.; Chen, W. Organ-on-a-Chip: A New Paradigm for Drug Development. Trends in Pharmacological Sciences 2021, 42, 119–133. [Google Scholar] [CrossRef]
Figure 1.
Overview of Organ-on-a-Chip technologies. Core fabrication strategies enable representative organ models and multi-organ platforms progressing toward multi-omics integration, clinical concordance, and regulatory adoption. Created with BioRender.com.
Figure 1.
Overview of Organ-on-a-Chip technologies. Core fabrication strategies enable representative organ models and multi-organ platforms progressing toward multi-omics integration, clinical concordance, and regulatory adoption. Created with BioRender.com.
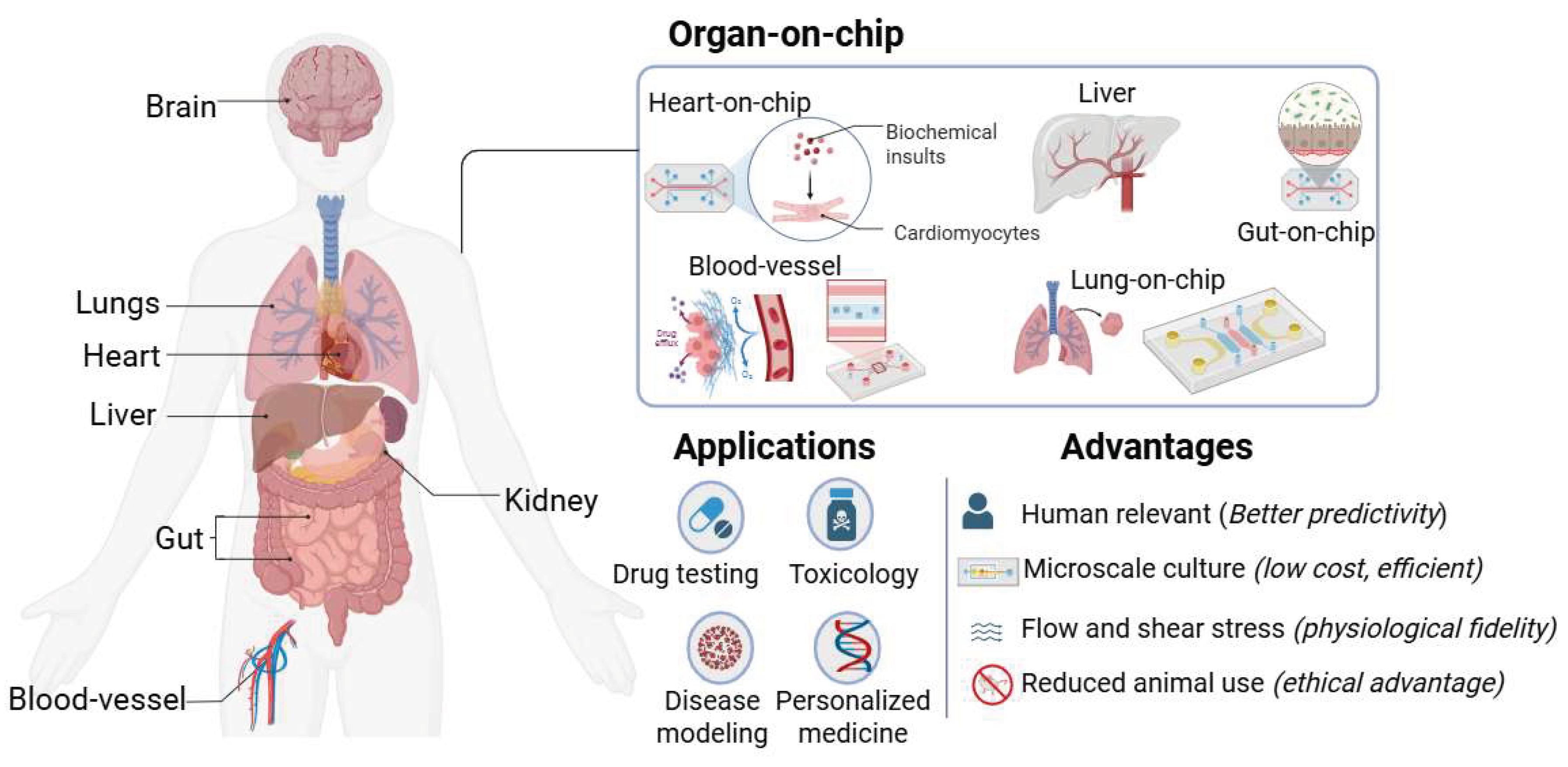
Figure 2.
Three interdependent technological pillars, namely materials, fabrication methods, and microfluidic design, collectively determine the biological fidelity, reproducibility, and translational readiness of Organ-on-a-Chip systems. Created with BioRender.com.
Figure 2.
Three interdependent technological pillars, namely materials, fabrication methods, and microfluidic design, collectively determine the biological fidelity, reproducibility, and translational readiness of Organ-on-a-Chip systems. Created with BioRender.com.
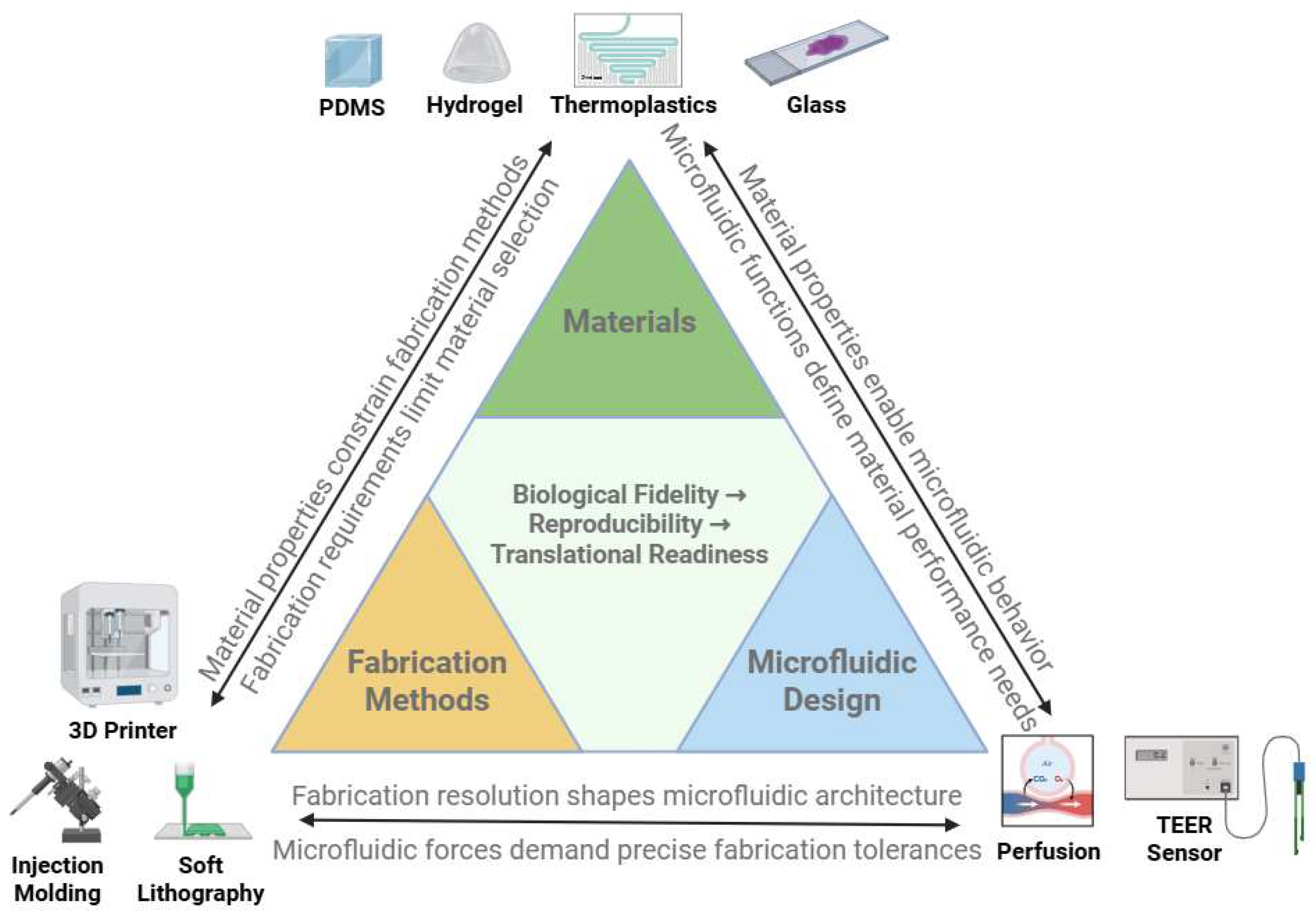
Figure 3.
(A–J). Applications of Organ-on-a-Chip models. (A) blood-vessel, (B) lung, (C) gut, (D) brain/BBB, (E) heart, (F) kidney, (G) liver, (H) skin, (I) tumor microenvironment, (J) organoid-on-chip hybrids. Created with BioRender.com.
Figure 3.
(A–J). Applications of Organ-on-a-Chip models. (A) blood-vessel, (B) lung, (C) gut, (D) brain/BBB, (E) heart, (F) kidney, (G) liver, (H) skin, (I) tumor microenvironment, (J) organoid-on-chip hybrids. Created with BioRender.com.
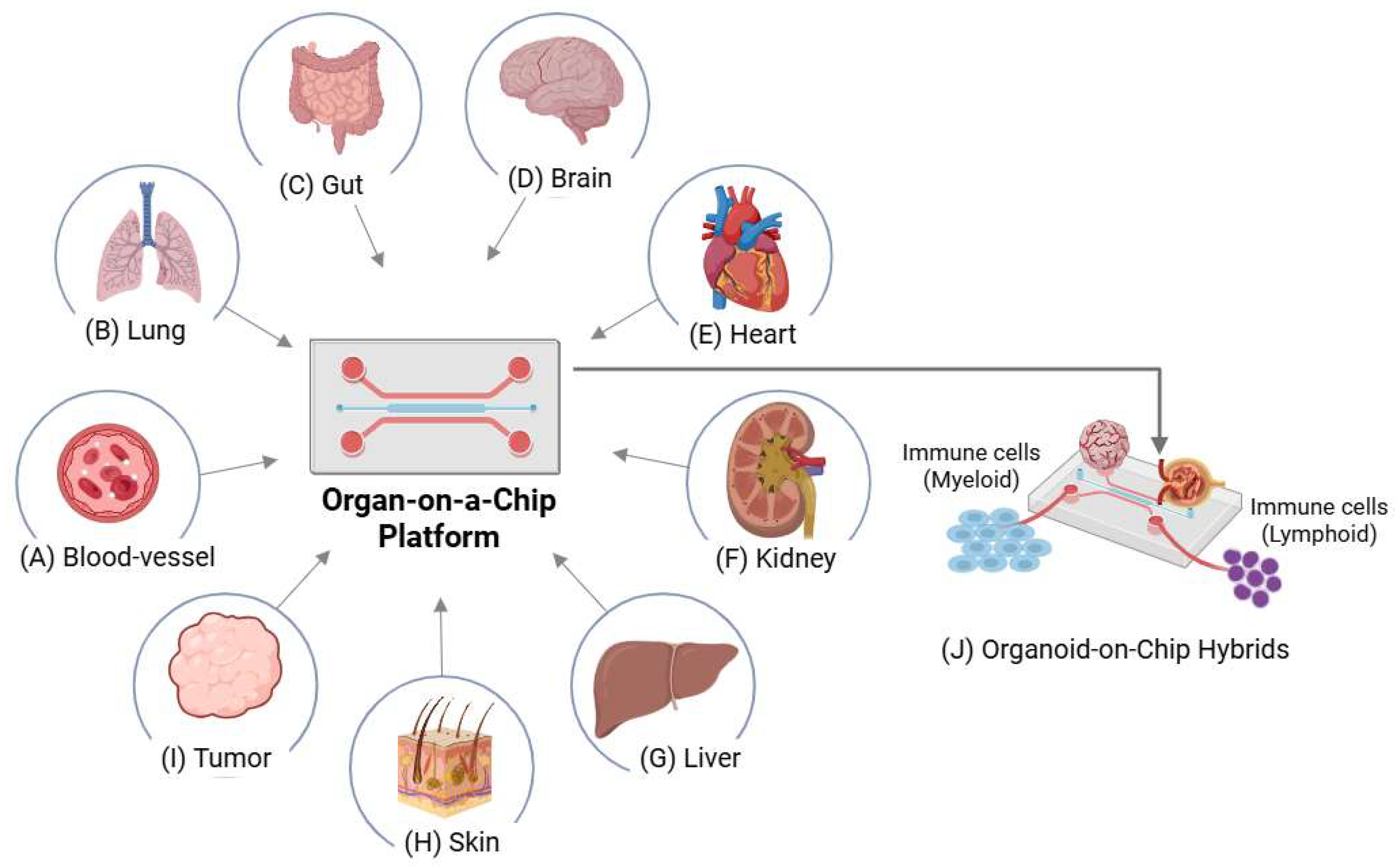
Figure 4.
Conceptual Roadmap for OOC development. Milestones from early microfluidics to automation, regulatory engagement, and multi-organ/AI-enabled platforms (2000–2035). Created with BioRender.com.
Figure 4.
Conceptual Roadmap for OOC development. Milestones from early microfluidics to automation, regulatory engagement, and multi-organ/AI-enabled platforms (2000–2035). Created with BioRender.com.
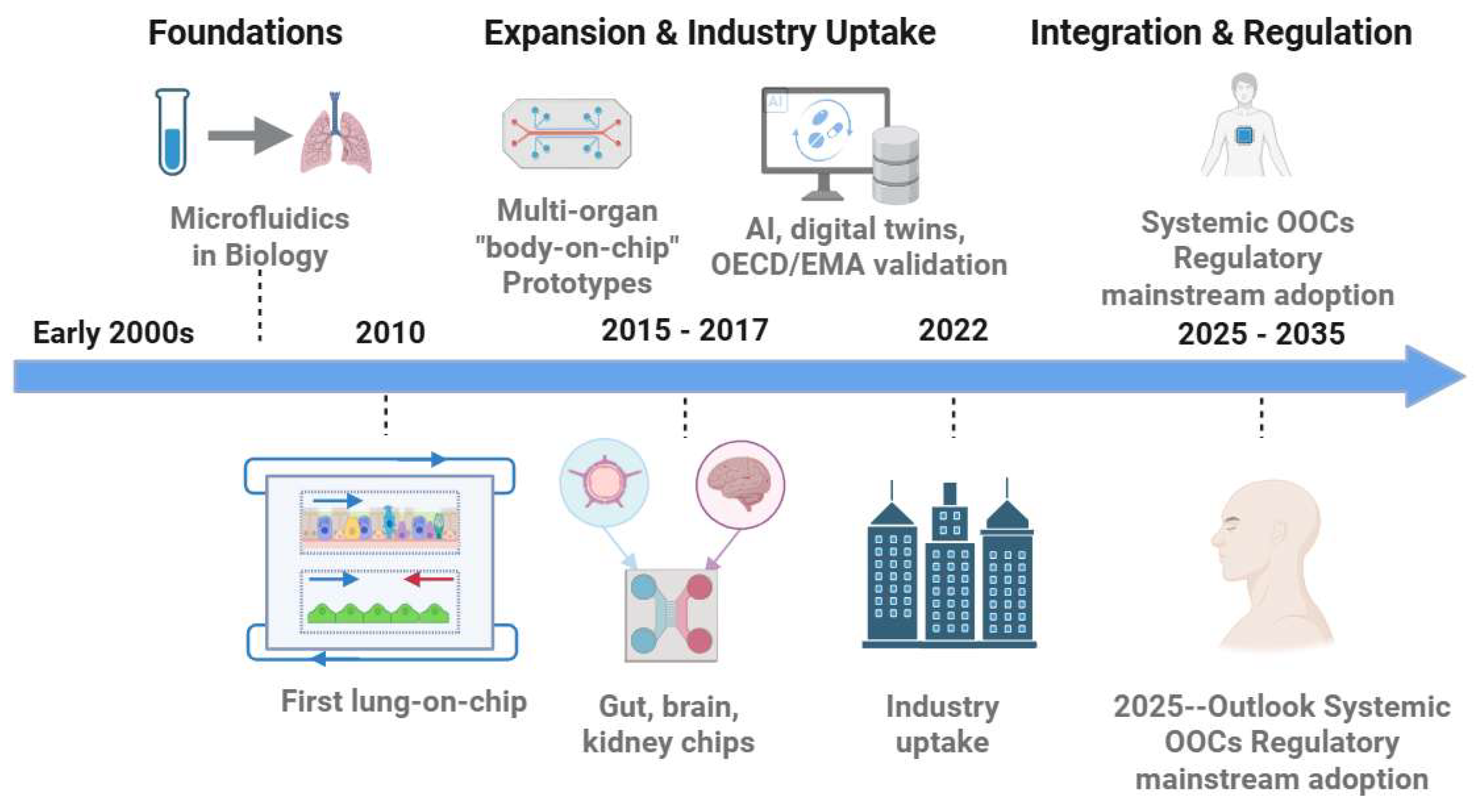
Figure 5.
Clinical concordance workflow. Inputs (human cells, dynamic microenvironment), readouts (barrier integrity, biomarkers, electrophysiology, multi-omics), benchmarking to patient-level datasets, and decision impact. Created with BioRender.com.
Figure 5.
Clinical concordance workflow. Inputs (human cells, dynamic microenvironment), readouts (barrier integrity, biomarkers, electrophysiology, multi-omics), benchmarking to patient-level datasets, and decision impact. Created with BioRender.com.
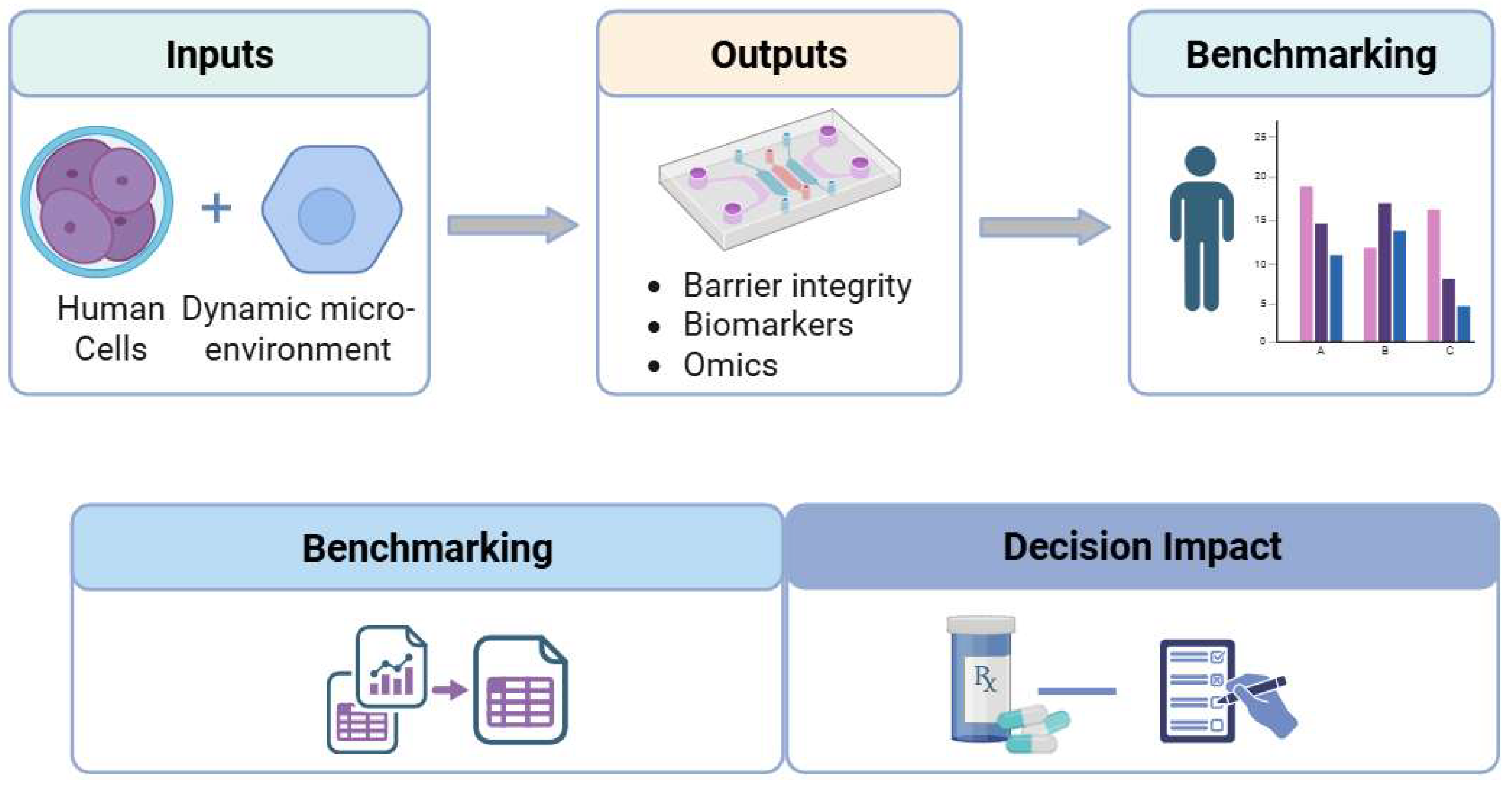
Table 1.
Comparison of preclinical research models.
| Feature | 2D Cell Culture [4,5,6] | Animal Models [7,8,11,12] | Organ-on-a-Chip (OOC) [13,14,15] |
|---|---|---|---|
| Physiological relevance | Low; flat, static monolayers | High systemic complexity but non-human physiology | Medium–high; 3D microenvironments with flow and mechanical cues |
| Human-specific data | Yes, when human cells are used | No; inter-species differences | Yes; primary cells, iPSCs or organoids from human donors |
| Throughput and cost | High throughput; low cost | Low throughput; very high cost | Medium throughput; moderate cost |
| Ethical considerations | Minimal | Significant ethical and welfare concerns | Minimal; potential to reduce animal use |
| Real-time monitoring | Limited; mostly end-point assays | Limited; many assays invasive or terminal | High; compatible with integrated sensors and live imaging |
| Control of variables | High control over media and stimuli | Low; complex whole-organism variability | Very high; precise control of flow, gradients, and co-cultures |
| Translational concordance | Often poor correlation with clinical outcomes | Variable; limited for many human-specific diseases and PK/PD | Growing evidence of quantitative concordance with human PK/PD and clinical biomarkers in defined contexts of use |
Table 2.
Representative milestones in the development of Organ-on-a-Chip (OOC) technology.
| Year | Milestone | Reference |
|---|---|---|
| Early 2000s | Emergence of microfluidics for biology and organ-mimetic microdevices | [13,24,25] |
| 2010 | First lung-on-a-chip (PDMS-based, cyclic strain) demonstrating organ-level breathing functions | [19] |
| 2012–2014 | Expansion to gut, brain and kidney chips, illustrating versatility across multiple organ systems | [20,21,23] |
| 2015–2017 | Development of multi-organ and interconnected OOC platforms enabling systemic PK/PD modeling | [14,15,26,27] |
| 2018–2020 | Growing industrial uptake, early commercialization, and international roadmaps for OOC and MPS adoption | [27,28,29,30] |
| 2022 | FDA Modernization Act 2.0 formally recognizes validated non-animal models, including OOCs, in drug development | [16] |
| 2023–2025 | AI-enabled digital twins, NAM-focused technical frameworks, and standardization efforts supporting quantitative benchmarking and regulatory acceptance | [17,18,31,32,33] |
Table 3.
Organ-specific integration of biosensors in organ-on-chip platforms: analytes, performance limits, and translational readiness.
Table 3.
Organ-specific integration of biosensors in organ-on-chip platforms: analytes, performance limits, and translational readiness.
| Organ system | Sensor modality | Primary analyte(s) / functional endpoint(s) | Key performance limits in OOC context | Translational readiness |
|---|---|---|---|---|
| Barrier organs (gut, lung, kidney, BBB) | TEER / electrical impedance | Barrier integrity; tight junction dynamics; permeability surrogates | Absolute TEER values are highly geometry- and electrode-dependent; sensitive to flow, temperature, and bubble formation; long-term drift due to electrode polarization and fouling | High (within-platform): Widely adopted for dynamic benchmarking; limited cross-platform comparability |
| Spatial or multi-frequency impedance (EIS) | Barrier heterogeneity; capacitive vs resistive components | Increased modeling and instrumentation complexity; interpretation sensitive to electrode placement and analysis assumptions | Moderate: Valuable mechanistic insight; less standardized | |
| Electrochemical pH / ion sensors | Local microenvironment changes affecting barrier function | Reference electrode stability; flow-induced noise; drift under long-term perfusion | Low–Moderate | |
| Cardiac | Microelectrode arrays (MEAs) | Field potentials; beat rate; conduction velocity; arrhythmogenic events | Signal amplitude depends on cell–electrode coupling; noise susceptibility; requires standardized analysis pipelines | High: Increasingly integrated into safety pharmacology workflows |
| Mechanical/contractility sensors (cantilevers, strain gauges, flexible diaphragms) | Contractile force; beat regularity; excitation–contraction coupling | Calibration drift; material fatigue; batch-to-batch variability; mechanical mismatch with tissue | Moderate–High: Strong for cardiac-specific endpoints | |
| Optical Ca²⁺ indicators | Excitation–contraction dynamics | Photobleaching; phototoxicity; reliance on dyes or reporters | Moderate | |
| Neural / brain | MEAs (planar or 3D) | Network activity; firing rate; synchrony; conduction | Long-term signal stability; electrode encapsulation by cells; complex data interpretation | Moderate: Widely used in research; translational benchmarks emerging |
| Neurochemical electrochemical sensors | Neurotransmitters; metabolic markers | Biofouling; selectivity in complex media; limited multiplexing | Low–Moderate | |
| Liver / metabolic organs | Electrochemical metabolite sensors (O₂, glucose, lactate) | Metabolic activity; mitochondrial function; drug-induced stress | Enzyme degradation; recalibration needs; sensitivity to medium composition | Moderate: Robust for core analytes with proper QC |
| Optical oxygen sensors | Oxygen gradients; consumption rates | Photobleaching (intensity-based); sensor aging; spatial averaging effects | High: One of the most mature chemical sensing approaches in OOCs | |
| Affinity biosensors (immuno-/aptamer-based) | Cytokines; secreted injury markers | Non-specific binding; regeneration limits; matrix effects | Emerging | |
| Cross-organ / multi-organ systems | Flow and pressure sensors | Shear stress; perfusion stability | Calibration across viscosities; control-loop instability | High: Essential enablers for credible long-term studies |
| Hybrid on-chip sensing + off-chip analytics | Broad metabolite and proteomic panels | Loss of temporal resolution; dead volume; sampling perturbations | Moderate–High |
Table 5.
Representative validation metrics for OOCs.
| Organ Model* | Context of Use | Key Validation Metrics |
| Heart | Torsadogenic risk prediction | AUROC ≥0.85 reported in multisite benchmarks; sensitivity ≥90% vs clinical QT datasets |
| Kidney | Transporter-mediated clearance; nephrotoxicity | Clearance R² > 0.8; RMSE ~ 10–20% vs clinical clearance |
| Brain / BBB | BBB permeability and efflux | Permeability rank correlation R > 0.8; efflux ratio within ±10–20% of in vivo |
| Lung | Inhalation toxicology; cytokine release; infection | Stable TEER (>95% of baseline); cytokine changes within ex vivo ranges |
| Liver | Drug-induced liver injury (DILI) prediction | CYP activity within ±20% of in vivo; albumin and urea in physiological range |
| Multi-organ (ADME/PBPK) | ADME/PK–PD; digital-twin integration | Plasma C–t R² > 0.85; prediction error < 25% for C_max and AUC |
Table 6.
Clinical concordance of Organ-on-a-Chip models across major organ systems.
| Organ | Clinical endpoint / comparator | Key concordance metrics |
|---|---|---|
| Heart-on-a-chip | Torsadogenic risk, QT prolongation; hERG assay and clinical QT/ECG | Representative studies report AUROC typically ≥0.85 with sensitivity >90% for torsadogenic drugs; improved detection of borderline-risk compounds vs hERG alone. |
| Kidney-on-a-chip | Renal clearance, transporter-mediated DDI, nephrotoxicity; clinical PK and DDI; 2D cocultures | Total and transporter-mediated clearance within ~10–20% RMSE of clinical values after IVIVE; earlier flagging of nephrotoxicity than 2D cocultures. |
| Lung-on-a-chip | Barrier integrity, cytokine release, viral infection; human explants, BAL/biopsy, rodent data | TEER and cytokine responses within roughly two-fold of ex vivo human data; correct ranking of inflammatory stimuli and antiviral candidates under physiological stretch and ALI. |
| Liver-on-a-chip | DILI risk, metabolic function (CYP, bile acids); clinical DILI cases and human PK; 2D hepatocytes | Maintains hepatic function for ≥3–4 weeks; improved sensitivity/specificity for clinical DILI and more accurate classification of high-risk compounds than 2D hepatocytes. |
| Brain / BBB-on-a-chip | BBB permeability and efflux; neurophysiology; microdialysis, PET, and EEG data | Permeability rank correlations R > 0.8 and efflux ratios within ±10–20% of in vivo; seizure-like and neuroinflammatory phenotypes consistent with clinical EEG signatures. |
| Multi-organ / systemic MPS | Plasma concentration–time curves, multi-organ toxicity; clinical PK/PD and reference drugs | Cmax and AUC prediction errors generally <25% vs clinical PK; correct ordering of systemic toxicities and exposure–response profiles in representative compound panels. |
Abbreviations: ALI, air–liquid interface; AUC, area under the concentration–time curve; AUROC, area under the receiver operating characteristic curve; BAL, bronchoalveolar lavage; BBB, blood–brain barrier; Cmax, maximum plasma concentration; CYP, cytochrome P450; DDI, drug–drug interaction; DILI, drug-induced liver injury; ECG, electrocardiogram; EEG, electroencephalography; hERG, human Ether-à-go-go–related gene; IVIVE, in vitro–in vivo extrapolation; MPS, microphysiological system; PET, positron-emission tomography; PK, pharmacokinetics; PK/PD, pharmacokinetics/pharmacodynamics; QT, QT interval; RMSE, root-mean-square error; TEER, transepithelial electrical resistance. Representative references supporting the benchmarks in Table 6 are provided in Section 5; see organ-specific concordance case studies and validation examples cited therein.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



