Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Background Sugaya type III rotator cuff re-tears are defined by a supraspinatus tendon thickness reduced to 50% or less of normal. These patients often experience prolonged pain and functional impairment. When considering reoperation, the burden of a long-term rehabilitation process and high risk of re-tear poses significant challenges for both patients and surgeons. Bioinductive collagen implants possess a mechanism that promotes the formation of new tendon tissue, holding potential to accelerate recovery and reduce re-tears. However, studies applying this technique in patients with Sugaya type III re-tear have not yet been reported. This study aimed to evaluate the clinical and radiologic outcomes of applying this procedure in patients with Sugaya type III re-tear. Method: This retrospective case series (Level IV) study included 15 patients (mean age 61.7 years) with Sugaya type III re-tears confirmed by MRI. All patients underwent arthroscopic rotator cuff repair combined with biologically induced collagen implant augmentation. Clinical outcomes were assessed at preoperative, 6-month, and 12-month postoperative time points using VAS, ASES, SANE, and WORC scores. Imaging findings were assessed via MRI, measuring supraspinatus thickness, and evaluating joint range of motion (ROM) and implant failure. Thickness measurements were performed twice each by an orthopedic surgeon (15 years' experience) and a radiologist (9 years' experience), with mean values used and intra- and inter-observer reliability (ICC) calculated. Results: The average VAS score decreased significantly from 6.5 ± 1.0 to 2.1 ± 0.8 (p < 0.001), and the ASES score improved from 45.2 ± 8.5 to 78.5 ± 8.9 (p < 0.001). SANE and WORC scores also showed significant improvement from 41.0 ± 12.1 to 81.4 ± 9.8 and from 39.6 ± 10.7 to 83.3 ± 10.1 respectively (p < 0.001). Supraspinatus thickness on MRI recovered from 4.5 ± 2.2 mm to 6.9 ± 2.5 mm (p < 0.001). At the final follow-up, all patients’ recovery of full or near-full range of motion was observed, and no implant failure were observed at either 6-month or 12-month follow-ups (0%). For MRI measurements, the inter-observer ICC was 0.93 (95% CI 0.85–0.97), and the intra-observer ICC ranged from 0.94 to 0.95. This indicates a high level of reliability. Conclusion: This study represents the first application of arthroscopic reattachment combined with bioengineered collagen implant augmentation in patients with Sugaya type III rotator cuff re-tears. Short-term follow-up confirmed significant improvement in pain and function, restoration of tendon thickness, and a 0% graft failure rate. This procedure is considered a useful method for treating patients with Sugaya type III re-tear, minimizing rehabilitation periods and avoiding the risk of re-tear.
Keywords:
rotator cuff injuries
; reoperation
; arthroscopy
; collagen
; bioprosthesis
1. Introduction
Rotator cuff tears are one of the primary causes of shoulder pain and functional impairment, and their incidence is gradually increasing due to an ageing population [1]. For this condition, arthroscopic rotator cuff repair is widely practised as a standard clinical treatment. However, postoperative re-tears are still reported at a high rate have a negative impact on patient prognosis [2]. In the Sugaya classification, type III is defined as a state that the supraspinatus tendon maintains continuity but has thinned to less than 50% of its normal thickness [3]. This condition is structurally vulnerable, carrying a risk of progression to complete rupture. Indeed, patients often experience prolonged pain and functional impairment [4].
Particularly when considering reoperation for patients with incomplete healing or thinned tendons, such as those with Sugaya type III, previous studies report that the risk of re-rupture after reoperation is approximately more than 1.75 times higher at 6 months and 2.5 times higher at 2 years compared to the primary surgery group [5]. Moreover, the long-term rehabilitation program is a major burden on both patients and surgeons. Therefore, seeking effective treatment strategies for patients with Sugaya type III is clinically very crucial.
The bioinductive collagen implant (REGENETEN®) is an absorbable collagen scaffold that improves the biological healing environment in a way that induces fibroblast proliferation and the formation of a neo-tendon, rather than directly reinforcing mechanical strength [6,7]. In clinical studies on partial-thickness tears and full-thickness tears, pain reduction, functional improvement, and tendon thickness recovery effects have been reported [8,9,10], and complication rates have been found to be low. However, there are no reports to date on the application in patients with Sugaya type III re-tear.
In this study, we hypothesized that the simultaneous application of arthroscopic re-suturing and augmentation with bio-engineered collagen implants would significantly improve clinical and radiologic outcomes by reduced pain, enhancing function, and restoring supraspinatus thickness in patients with Sugaya type III rotator cuff re-tears.
Therefore, the objective of this study is to evaluate the clinical and radiologic outcomes in the short-term follow-up period following the application of bio-engineered collagen implant augmentation in patients with Sugaya type III rotator cuff re-tears.
2. Methods
Inclusion criteria were: (1) adults aged 18 years or older, (2) Sugaya type III re-tear with persistent pain for over 2 years post-surgery, (3) ability to undergo at least 12 months of follow-up.
Exclusion criteria were: (1) Sugaya type IV or V, (2) shoulder joint arthrosis classified as Hamada grade III or higher, (4) concomitant infection.
2.1. Surgical Technique
All procedures were performed by a single surgeon, utilizing only an interscalene block for anesthesia without general anesthesia. The patient underwent surgery in the beach-chair position.
First, diagnostic arthroscopy was performed via a posterior approach to assess the rotator cuff condition and associated pathology, followed by the creation of standard anterior and lateral access points. Should arthroscopic observation reveal that the coracoacromial (CA) ligament was not released, or that the inferior border of the acromion was irregular or rough, CA ligament release and acromioplasty were additionally performed to prevent impingement.
The suture knots and fiber wires used in the previous surgery were loosened in multiple areas, which not only failed to provide mechanical stability but could also cause collision and irritation. Therefore, all loosened fiber wires and unnecessary suture knots were removed as far as possible (Figure 1).
Subsequently, the bioengineered collagen implant (REGENETEN®, Smith & Nephew, USA) was inserted through the lateral insertion port using the manufacturer’s dedicated delivery system. Prior to insertion, the bleeding tissue on the cuff surface (bursal surface bleeding bed) was cleared using a shaver and RF probe to ensure the scaffold could adhere closely to the tendon.
The implant was positioned to fully cover the thinned and heterogeneous region of the supraspinatus tendon, and made to extended medially to the musculotendinous junction and laterally to the greater tuberosity footprint. And in the anterior and posterior directions, after securing a margin of at least 5 mm beyond the border of the thinned tendon, the graft was made to overlap the healthy tendon sufficiently (Figure 2A).
Fixation was achieved using a combination of bioabsorbable staples and tendon anchors. Staples were inserted at regular intervals (approximately 5–7 mm) along the medial and anteroposterior edges of the implant to ensure the scaffold adhered evenly to the cuff surface (Figure 2B, 2C). In this process, precautions were taken to prevent staple protrusion or implant wrinkling.
At the final arthroscopic examination, the implant was observed to be securely attached to the cuff surface. During joint movement, neither displacement nor lifting of the graft was observed. After confirming that the implant was evenly positioned, securely fixed, and stable on the cuff surface, the surgery was completed.
2.2. Postoperative Rehabilitation
Following surgery, the patient wore a shoulder abduction sling for 48 hours, and thereafter was instructed to wear it as required for up to two weeks. During the initial two weeks, shoulder joint movement was restricted, permitting only light movement of the wrist, fingers, and elbow joints. From two weeks onwards, passive range of motion (ROM) exercises commenced under the guidance of a physiotherapist, with external rotation and forward elevation beyond 90° restricted. From four weeks onwards, the range of external rotation was progressively increased within pain-free limits.
From the 6-week mark, active-assisted range of motion (ROM) exercises and scapular stabilisation exercises commenced, alongside isometric muscle contraction exercises to maintain baseline strength in the rotator cuff and surrounding muscles. Subsequently, depending on the patient’s recovery progress, this transitioned to active ROM exercises, with the goal for most patients being full restoration of joint range of motion within 12 weeks.
After three months, progressive muscle strengthening exercises using elastic bands and light dumbbells commenced. This phase focused on strengthening the rotator cuff muscle group and scapular stabilising muscles. Depending on the patient’s condition, light domestic activities and a return to work were permitted.
After six months, patients were gradually permitted to resume daily activities and sports. High-intensity resistance training and overhead sports activities were progressively allowed between nine and twelve months. Ultimately, all patients resumed activities based on pain-free joint movement, restored muscle strength, and functional stability.
2.3. Clinical and Radiologic Outcomes Evaluation
Clinical evaluation was conducted at preoperative, 6-month, and 12-month postoperative time points. Pain was assessed using the visual analogue scale (VAS) from 0 (no pain) to 10 (extreme pain). Functional evaluation utilised the American Shoulder and Elbow Surgeons (ASES) score, the Single Assessment Numeric Evaluation (SANE) score, and the Western Ontario Rotator Cuff (WORC) index. Furthermore, the range of motion (ROM) was measured for forward flexion, external rotation at the side, and internal rotation at the spinal level. The ROM assessment was performed by the same surgeon, and all measurements were recorded at the maximum pain-free range.
Radiologic evaluation was performed using MRI at preoperative, 6-month, and 12-month postoperative time points. All MRI scans were acquired using the same equipment and protocol (T2-weighted fat-suppressed coronal oblique sequence). Supraspinatus tendon thickness was measured at the proximal mid-substance of the greater tuberosity footprint, perpendicular to the tendon fibre orientation. Sugaya type III was defined as a reduction in thickness to 50% or less relative to the contralateral side, or an absolute thickness of 4.0 mm or less when no image was available on the affected side. MRI measurements were independently repeated twice by an orthopedic surgeon (15 years’ experience) and a radiologist (9 years’ experience), with the mean value used for analysis. Intra-observer and inter-observer reliability were assessed by calculating the intraclass correlation coefficient (ICC). Graft failure was defined as graft loss, re-rupture, or patch detachment on MRI. The presence of complications (infection, stiffness, nerve injury, etc.) was also investigated in all patients.
3. Results
3.1. Demographics
This study included 15 patients totally, and their average age was 61.7 years (range, 55–70 years). They consisted of 8 males (53.3%) and 7 females (46.7%), and their average BMI was 24.6 ± 1.7 kg/m2. Dominant-side lesions appeared in 9 cases (60.0%). The average symptom duration was 2.7 ± 0.4 years, and all patients were in the state of Sugaya type III re-tears which had caused persistent pain for over 2 years post-surgery. Diabetes was observed in 4 cases (26.7%), and smoking history was found in 6 cases (40.0%). Preoperative supraspinatus thickness was measured as an average of 3.55 ± 0.27 mm on MRI, and all these cases satisfied the criteria of being 50% or less of the contralateral thickness or having an absolute thickness of 4 mm or less (Table 1).
3.2. Clinical Outcomes
The average VAS score decreased significantly from 6.5 ± 1.0 before surgery to 2.8 ± 0.9 at 6 months and 2.1 ± 0.8 at the 12-month follow-up, as the final stage (p < 0.001). The ASES score improved from 45.2 ± 8.5 to 71.8 ± 9.3 (6 months) 78.5 ± 8.9 (12 months) (p < 0.001), and the SANE score improved from 41.0 ± 12.1 to 70.2 ± 11.5 (6 months) and 81.4 ± 9.8 (12 months) (p < 0.001). The WORC index also showed a significant increase from 39.6 ± 10.7 to 72.1 ± 12.3 (6 months) and 83.3 ± 10.1 (12 months) (p < 0.001, Table 2).
3.3. Range of Motion
Anterior elevation range of motion recovered from 162.0 ± 12.3° to 176.0 ± 6.5°, and external rotation improved from 60.5 ± 8.1° to 71.4 ± 6.2° (p = 0.041). Internal rotation improved from an average level of L2–L3 before surgery to T11–T12 (p = 0.049). At the final follow-up, all patients had recovered either full or near-full joint range of motion (Table 2).
4. Discussion
The hypothesis of this study was that when a surgery with arthroscopic re-suturing concurrently with bio-engineered collagen implant augmentation was performed in patients with Sugaya type III rotator cuff re-tears, it would significantly improve clinical and radiologic outcomes through pain reduction, functional improvement, and restoration of supraspinatus thickness. In fact, the results of this study supported this hypothesis. VAS, ASES, SANE, and WORC scores significantly improved in all patients, and supraspinatus thickness increased from an average of 3.55 mm to 5.6 mm at MRI follow-up examination. Moreover, all patients had recovered either full or near-full range of motion at the final follow-up, and no single graft failure was observed. This suggests that our surgical procedure can provide positive effects on both clinical symptoms and radiologic structural improvement in patients with Sugaya type III.
Sugaya type III is defined radiologically as a state that tendon continuity is maintained but the thickness is decreased by less than 50% relative of normal [3]. This type of pathology can be interpreted not simply as a form of healing, but rather an indication of tendon elongation, which is commonly seen after rotator cuff repair surgery. According to prior studies, the tendon undergoes an average static retraction or dynamic elongation of approximately 10 mm within several months after surgery, and this may merely represent scar healing with loss of tension [11,12]. Thus, Sugaya type III often presents with persistent pain and poor function clinically, even if continuity is preserved on MRI. In fact, some patients complain severe sensation of discomfort in daily life for a prolonged time [7,11].
On the other hand, Sugaya type IV–V is regarded as a clear re-tear, and reoperation is typically considered when symptoms are present [3,15,22]. In the case of type III, however, the situation is more complex. A long rehabilitation period is required during the process of re-releasing and suturing the adhered tendon, and a high re-tear rate has been reported caused by tissue quality deterioration [5,8,22,24]. For these reasons, it is not easy to determine the indications for surgery or to select the proper surgical technique is not easy.
Recent studies applying bioengineered collagen implants (onlay augmentation) in patients with partial-thickness rotator cuff tears (PTRCT) have reported favourable outcomes. Bokor et al. demonstrated significant improvements in pain and function, increased thickness, and a low failure rate at 2-year follow-up in patients with bursal-side PTRCT treated with the implant alone, without suturing [19]. Yoo and Lee also reported 0% implant failure and early clinical improvement at one-year follow-up in bursal-side PTRCT patients treated with implant alone [10]. These studies support that the bioinductive onlay approach is characterised by rapid rehabilitation, high survival rates, and low failure rates [6,7,9,14,19].
Sugaya type III shares significant similarities with high-grade lesions in PTRCT due to its pathological characteristics. Both lesions maintain tendon continuity but exhibit loss of thickness and tension, placing them on the same pathophysiological continuum [4,16]. It is recognised that partial tears with more than 50% loss of tendon thickness have a low likelihood of spontaneous recovery and carry a high risk of persistent symptoms and progression to complete rupture [4,16,17]. Therefore, the authors applied bioinductive collagen implant augmentation in patients with Sugaya type III, based on evidence established in PTRCT.
The advantages of this technique over conventional reattachment are clear. First, by providing a scaffold over the tendon surface without forcing tendon-to-bone reattachment, it induces neotendon formation and enables rapid rehabilitation [6,7,14]. Second, the low graft failure rate reduces burden for both surgeon and patient [8,9,19]. Third, it avoids the high risk of re-rupture associated with revision surgery and the burden of prolonged rehabilitation [5,22,24,25]. The clinical and radiologic improvements observed in this study, along with a 0% graft failure rate, support these advantages.
In other words, the core issue with Sugaya type III lies in its state of “continuity being present, yet tension and thickness being lost”. Therefore, the aim of treatment is not merely to achieve structural continuity, but on restore functional tension and improve tendon quality. The findings of this study align with this aim and suggest that bioinductive collagen implant augmentation can be a useful treatment strategy with lower burden compared to conventional reattachment techniques in patients with Sugaya type III.
This study has some limitations. First, the sample size is limited to 15 cases, and there is a possibility of selection bias since this is a retrospective case series study conducted at a single institution by a single surgeon. Second, this study did not include a control group, so it cannot directly prove if the surgical procedure used in this study has a relative advantage compared to conventional re-suturing or conservative treatment. Third, the follow-up period of 12 months is relatively short, so it is not sufficient to evaluate long-term re-rupture rates and functional outcomes.
Fourth, there still remains certain inherent limitations of radiologic assessment itself and the possibility of observer bias cannot be entirely excluded, although high reliability was verified in the thickness measurements using MRI through repeated assessments by experienced orthopedic and radiology specialists independently.
Lastly, the survey tools used for pain and functional assessment can be affected by subjective bias, as they are designed based on patient-reported outcome.
Despite these limitations, this study is significant as it introduced the first application of bioengineered collagen implants in patients with Sugaya type III rotator cuff re-rupture, and suggests positive clinical and radiologic outcomes in the short-term follow-up.
5. Conclusions
This study represents the first case series to have performed arthroscopic bio-guided collagen implant augmentation in Sugaya type III rotator cuff re-tear patients experiencing persistent pain for over two years post-surgery. The results showed significant improvement in pain and function compared to pre-operative levels. MRI assessment indicated recovery of supraspinatus tendon thickness, and no graft failure was observed up to final follow-up.
Such results suggest that this procedure is a potential treatment strategy for patients with Sugaya type III, since it provides clinical improvement and reduces the burden on both patients and surgeons compared to conventional revision surgery methods. In future research, a prospective design with a larger number of patients, long-term follow-up, and comparative studies with control groups are needed.
Author Contributions
Conceptualization, Jaesung Yoo; Methodology, DauHee Lee, Jae-Wook Park and Jaesung Yoo; Resources, DauHee Lee and Jae-Wook Park; Data curation, DauHee Lee and Jae-Wook Park; Writing – original draft, Jaesung Yoo; Visualization, Jaesung Yoo; Supervision, Jaesung Yoo.
Funding
There is no funding source.
Institutional Review Board Statement
This article does not contain any studies with human participants or animals performed by any of the authors. This study was reviewed and accepted by the Dankook University medical center Institutional Review Board (DKUH-2026-01-030).
Informed Consent Statement
All of authors agree to publication.
Data Availability Statement
It is available when reviewers request.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Abbreviations
VAS: Visual Analog Scale, ASES; American Shoulder and Elbow Surgeons, MRI; Magnetic Resonance Imaging
References
- Yamamoto, A.; Takagishi, K.; Osawa, T.; Yanagawa, T.; Nakajima, D.; Shitara, H.; Kobayashi, T. Prevalence and risk factors of a rotator cuff tear in the general population. J. Shoulder Elbow Surg. 2010, 19, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Galatz, L.M.; Ball, C.M.; Teefey, S.A.; Middleton, W.D.; Yamaguchi, K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J. Bone Joint Surg. Am. 2004, 86, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, H.; Maeda, K.; Matsuki, K.; Moriishi, J. Repair integrity and functional outcome after arthroscopic double-row rotator cuff repair: A prospective outcome study. J. Bone Joint Surg. Am. 2007, 89, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Matthewson, G.; Beach, C.J.; Nelson, A.A.; Woodmass, J.M.; Ono, Y.; Boorman, R.S.; Thornton, G.M.; Lo, I.K. Partial thickness rotator cuff tears: Current concepts. Bone Joint J. 2015, 97-B, 28–35. [Google Scholar] [CrossRef]
- Ting, R.S.; Wajswelner, H.; Scadding, C.; Cook, J.; Cass, B.; Krishnan, J. Revision rotator cuff repair with versus without an arthroscopically inserted onlay bioinductive implant. Orthop. J. Sports Med. 2023, 11, 23259671221148105. [Google Scholar] [CrossRef]
- Thangarajah, T.; Pendegrass, C.J.; Shahbazi, S.; Lambert, S.; Alexander, S.; Blunn, G.W.; Carr, A.J. Augmentation of rotator cuff repair with soft tissue scaffolds. JBJS Essent. Surg. Tech. 2022, 12, e21.00050. [Google Scholar] [CrossRef]
- Camacho-Chacon, S.; Sanz-Herrera, J.A.; Mora, G.; Cuéllar, R.; Vaquero, J.; Vidal, J.; Vaquero-Martín, J. Histologic evidence of neotendon formation after bioinductive implant application in rotator cuff tears. J. Exp. Orthop. 2022, 9, 20. [Google Scholar] [CrossRef]
- Bushnell, B.D.; Creighton, R.A.; Hovis, W.D.; Tokish, J.M. Retear rates and clinical outcomes after repair of full-thickness rotator cuff tears augmented with a bioinductive collagen implant: A multicenter study. JSES Int. 2021, 5, 381–388. [Google Scholar] [CrossRef]
- McIntyre, L.F.; Bishai, S.K.; Brown, P.B.; Bushnell, B.D.; Trenhaile, S.W. Patient-reported outcomes after use of a bioinductive collagen implant to facilitate healing of partial- and full-thickness rotator cuff tears. Arthrosc. Sports Med. Rehabil. 2021, 3, e1137–e1148. [Google Scholar] [CrossRef]
- Yoo, J.S.; Lee, J.H. Clinical outcomes of a bioinductive collagen implant in bursal-sided partial-thickness rotator cuff tears. Medicina 2025, 61, 988. [Google Scholar] [CrossRef]
- Lawrence, C.; Gulotta, L.; Dines, D.; Rodeo, S.; Warren, R.; Dines, J. Tendon elongation with continuity after rotator cuff repair: An important predictor of structural failure. Orthop. J. Sports Med. 2022, 10, 23259671221083905. [Google Scholar]
- Lawrence, C.; et al. Failure with continuity: Dynamic elongation after rotator cuff repair. Orthop. J. Sports Med. 2022, 10, 23259671221083915. [Google Scholar]
- Ridley, T.J.; et al. Regeneten bioinductive implant rehabilitation protocol. In Univ. Minnesota Orthopaedics; (White Paper/Protocol); 2021. [Google Scholar]
- Micheloni, G.M.; et al. Bio-inductive implant in rotator cuff tears: Our experience and technical notes. Acta Biomed. 2020, 91, 153–160. [Google Scholar] [CrossRef]
- Chona, D.V.; et al. Clinical and structural outcomes of revision rotator cuff repair. J. Shoulder Elbow Surg. 2017, 26, 1889–1895. [Google Scholar] [CrossRef]
- McElvany, M.D.; McGoldrick, E.; Gee, A.O.; Neradilek, M.B.; Matsen, F.A. Rotator cuff repair: Published evidence on factors associated with repair integrity and clinical outcome. Am. J. Sports Med. 2015, 43, 491–500. [Google Scholar] [CrossRef]
- Petri, M.; Greenspoon, J.A.; Millett, P.J. Surgical management of rotator cuff tears: An evidence-based review of the literature. Arthroscopy 2016, 32, 1866–1877. [Google Scholar]
- Sclamberg, S.G.; Tibone, J.E.; Itamura, J.M.; Kasraeian, S. Six-month magnetic resonance imaging follow-up of arthroscopic rotator cuff repairs: Initial results and correlation with clinical outcome. J. Shoulder Elbow Surg. 2004, 13, 570–574. [Google Scholar] [CrossRef]
- Bokor, D.J.; Sonnabend, D.; Deady, L.; Cass, B.; Young, A.; van Kampen, C.; van der Merwe, W.; Visser, J.D.; van den Hoorn, B. Evidence of healing of partial-thickness rotator cuff tears following arthroscopic augmentation with a bioinductive collagen implant: 2-year MRI and clinical outcomes. J. Shoulder Elbow Surg. 2019, 28, 2427–2436. [Google Scholar] [CrossRef]
- Barfod, K.W.; et al. The influence of smoking and diabetes on rotator cuff repair outcomes. J. Shoulder Elbow Surg. 2018, 27, 580–587. [Google Scholar] [CrossRef]
- Abrams, G.D.; et al. Arthroscopic repair of full-thickness rotator cuff tears with and without acromioplasty: Randomized prospective trial. Am. J. Sports Med. 2014, 42, 1296–1303. [Google Scholar] [CrossRef]
- Park, J.Y.; et al. Revision rotator cuff repair: Risk factors for retear and clinical outcomes. Am. J. Sports Med. 2018, 46, 157–165. [Google Scholar]
- Holtby, R.; Razmjou, H. Relationship between clinical and radiologic outcomes after arthroscopic rotator cuff repair: A prospective study. J. Shoulder Elbow Surg. 2010, 19, 573–579. [Google Scholar] [CrossRef]
- Lo, I.K.; Burkhart, S.S. Arthroscopic revision of failed rotator cuff repairs: Technique and results. Arthroscopy 2004, 20, 250–267. [Google Scholar] [CrossRef] [PubMed]
- Mall, N.A.; Lee, A.S.; Chahal, J.; Sherman, S.L.; Romeo, A.A.; Verma, N.N.; Cole, B.J. An evidenced-based examination of the epidemiology and outcomes of traumatic rotator cuff tears. Arthroscopy 2013, 29, 366–376. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Arthroscopic findings of the right shoulder showing loosening of previously used FiberWire sutures. Multiple suture knots and fiber wires appear loosened and displaced around the rotator cuff footprint, failing to maintain mechanical stability and potentially causing subacromial irritation. All loosened FiberWire strands and unnecessary knots were carefully removed during revision surgery.
Figure 1.
Arthroscopic findings of the right shoulder showing loosening of previously used FiberWire sutures. Multiple suture knots and fiber wires appear loosened and displaced around the rotator cuff footprint, failing to maintain mechanical stability and potentially causing subacromial irritation. All loosened FiberWire strands and unnecessary knots were carefully removed during revision surgery.
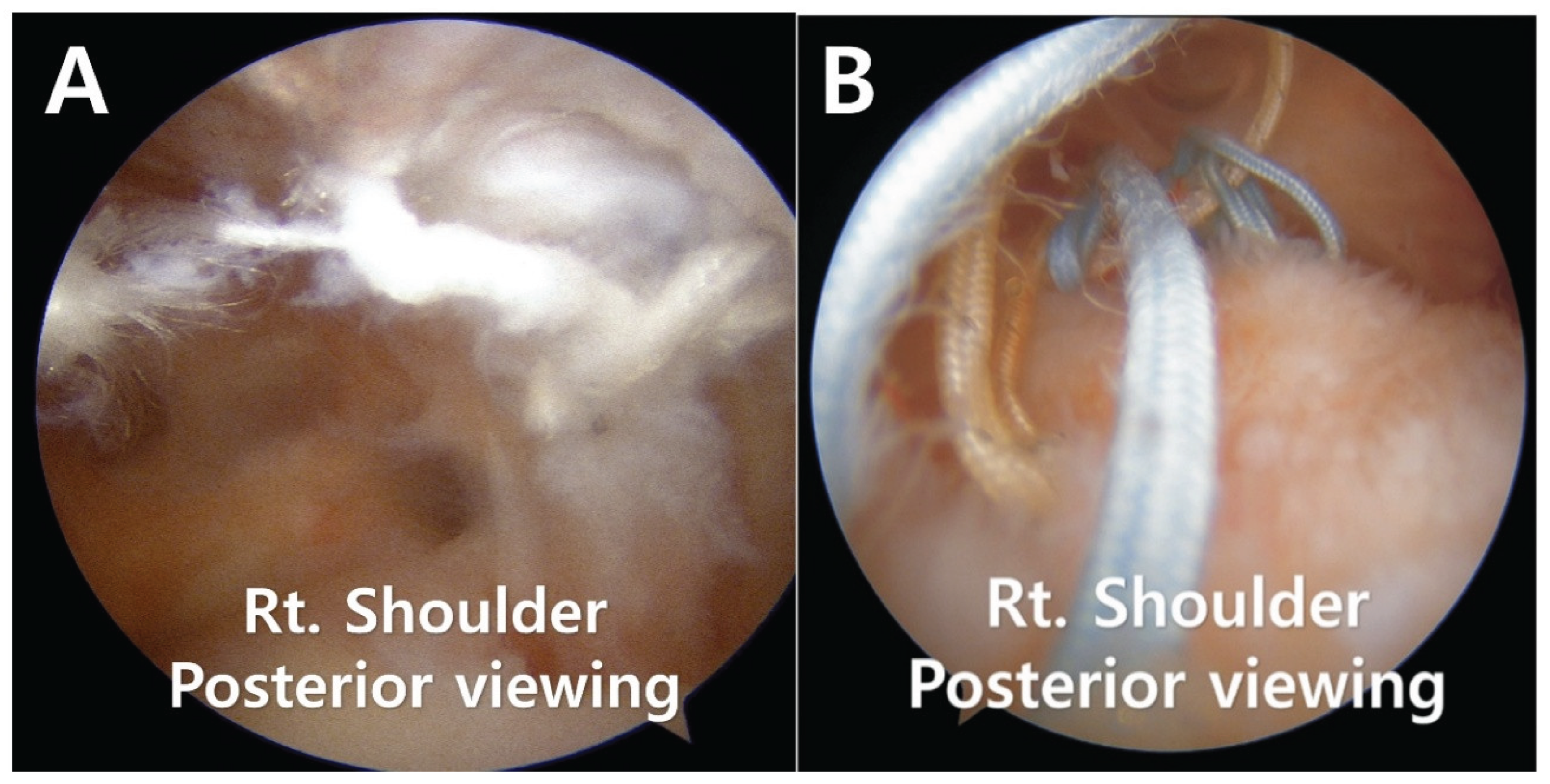
Figure 2.
Arthroscopic views demonstrating the placement and fixation of the REGENETEN bioinductive collagen implant. (A) The implant was positioned to completely cover the thinned and heterogeneous supraspinatus tendon, extending medially to the musculotendinous junction and laterally to the greater tuberosity footprint, with at least a 5 mm overlap beyond the anterior and posterior tendon margins.(B) Arthroscopic image after fixation of the REGENETEN implant using tendon anchors, showing stable adaptation of the graft to the underlying cuff surface. (C) Final arthroscopic appearance after completion of bone anchor fixation at the greater tuberosity, demonstrating.
Figure 2.
Arthroscopic views demonstrating the placement and fixation of the REGENETEN bioinductive collagen implant. (A) The implant was positioned to completely cover the thinned and heterogeneous supraspinatus tendon, extending medially to the musculotendinous junction and laterally to the greater tuberosity footprint, with at least a 5 mm overlap beyond the anterior and posterior tendon margins.(B) Arthroscopic image after fixation of the REGENETEN implant using tendon anchors, showing stable adaptation of the graft to the underlying cuff surface. (C) Final arthroscopic appearance after completion of bone anchor fixation at the greater tuberosity, demonstrating.
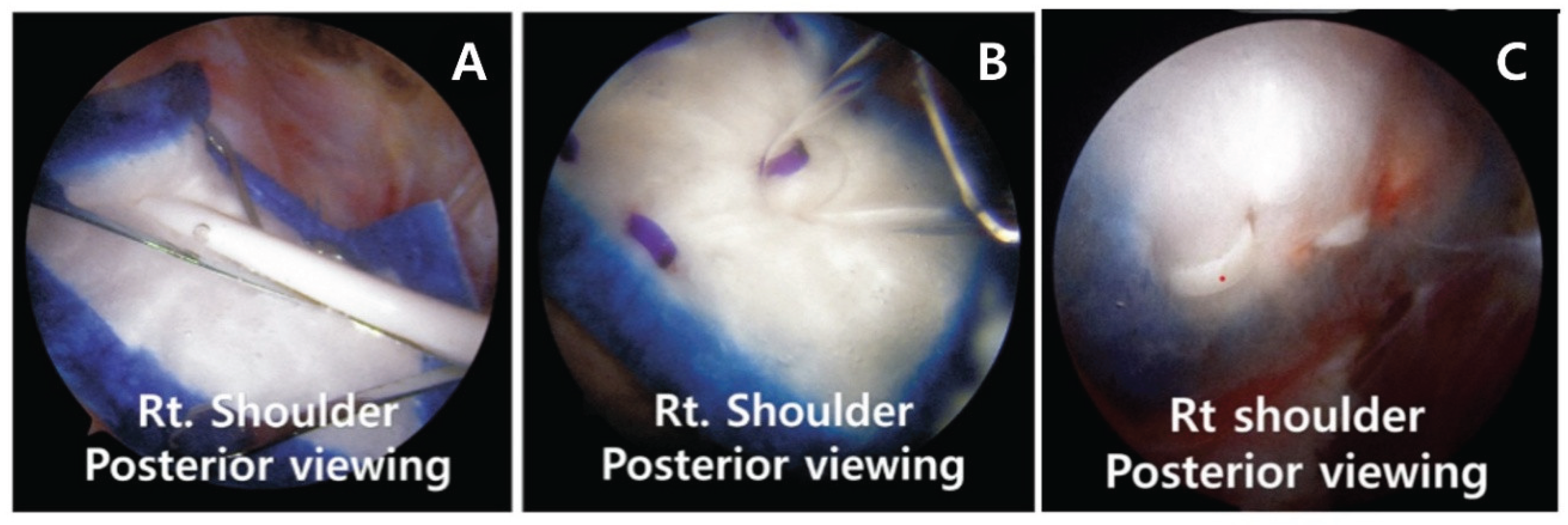
Figure 3.
T2-weighted magnetic resonance imaging (MRI) of a 57-year-old male patient who underwent rotator cuff repair at another institution 3 years earlier. (A) Preoperative MRI demonstrating more than a 25% reduction in supraspinatus tendon thickness compared with the contralateral side, with a measured thickness of 5.059 mm. (B) Postoperative MRI obtained 1 year after surgery showing an increased supraspinatus tendon thickness of 9.49 mm.
Figure 3.
T2-weighted magnetic resonance imaging (MRI) of a 57-year-old male patient who underwent rotator cuff repair at another institution 3 years earlier. (A) Preoperative MRI demonstrating more than a 25% reduction in supraspinatus tendon thickness compared with the contralateral side, with a measured thickness of 5.059 mm. (B) Postoperative MRI obtained 1 year after surgery showing an increased supraspinatus tendon thickness of 9.49 mm.
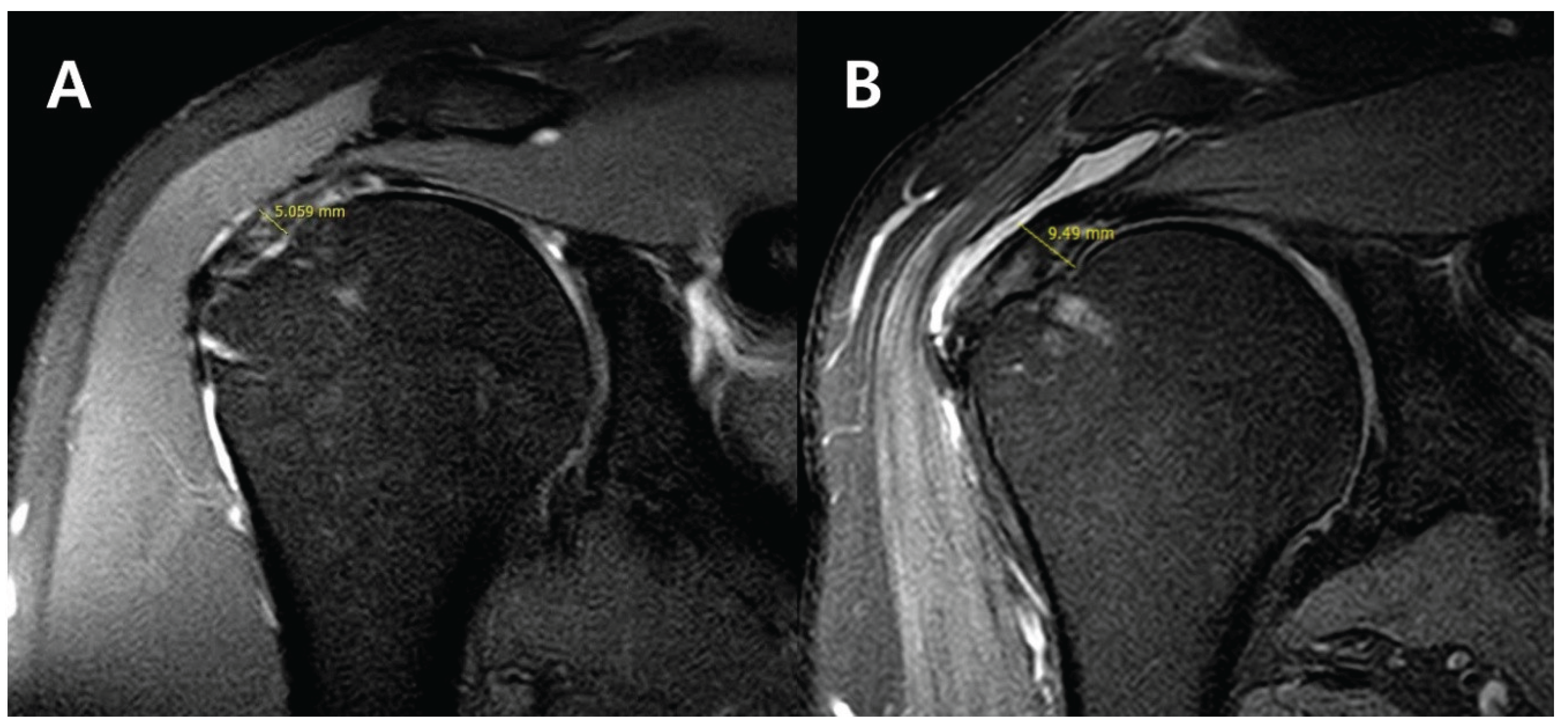

Table 1.
Demographic Characteristics
| Case | Age (years) | Sex | BMI (kg/m2) | Dominant side involved | Symptom duration (years) | Diabetes | Smoking | Supraspinatus thickness (mm, MRI) |
| 1 | 62 | M | 24.8 | Yes | 2.5 | No | No | 2.1 |
| 2 | 58 | F | 22.5 | No | 2.1 | No | No | 2.8 |
| 3 | 67 | M | 26.3 | Yes | 3.0 | Yes | Yes | 3.0 |
| 4 | 55 | F | 23.4 | Yes | 2.3 | No | No | 3.7 |
| 5 | 63 | M | 25.6 | No | 2.6 | No | Yes | 4.2 |
| 6 | 60 | F | 21.8 | Yes | 2.4 | No | No | 4.3 |
| 7 | 70 | M | 27.1 | No | 3.2 | Yes | No | 4.8 |
| 8 | 61 | M | 24.2 | Yes | 2.8 | No | Yes | 5.1 |
| 9 | 57 | F | 23.7 | Yes | 2.2 | No | No | 5.2 |
| 10 | 65 | M | 26.9 | No | 3.1 | Yes | Yes | 5.5 |
| 11 | 59 | F | 22.1 | Yes | 2.5 | No | No | 5.7 |
| 12 | 62 | M | 25.0 | Yes | 2.7 | No | Yes | 5.9 |
| 13 | 64 | F | 23.5 | No | 2.9 | No | No | 5.8 |
| 14 | 68 | M | 27.3 | Yes | 3.3 | Yes | Yes | 5.9 |
| 15 | 56 | F | 22.9 | No | 2.4 | No | No | 4.4 |
All patients met the criteria for Sugaya type III retear, defined as ≥50% thinning of the supraspinatus tendon thickness compared to the contralateral side on MRI. Values are presented as mean ± SD or number (%). BMI = body mass index; M = male; F = female.
Table 2.
Clinical and radiologic outcomes of the study population (n = 15).
| Outcome measure | Preoperative |
Postoperative (6 months) |
Postoperative (12 months) |
p-value (preop vs POD 1Y) |
| VAS pain score | 6.5 ± 1.0 | 2.8 ± 0.9 | 2.1 ± 0.8 | <0.001 |
| ASES score | 45.2 ± 8.5 | 71.8 ± 9.3 | 78.5 ± 8.9 | <0.001 |
| SANE score (%) | 41.0 ± 12.1 | 70.2 ± 11.5 | 81.4 ± 9.8 | <0.001 |
| WORC index (%) | 39.6 ± 10.7 | 72.1 ± 12.3 | 83.3 ± 10.1 | <0.001 |
| Supraspinatus thickness (mm, MRI) |
4.5 ± 2.2 | 6.9 ± 2.5 | <0.001 | |
| Forward flexion ROM (°) | 162.0 ± 12.3 | 172.5 ± 8.4 | 176.0 ± 6.5 | n.s. |
| External rotation at side (°) | 60.5 ± 8.1 | 68.2 ± 6.5 | 71.4 ± 6.2 | 0.041 |
| Internal rotation (spinal level) | L2–L3 (T12–L4) |
T12–L1 (T11–L2) |
T11–T12 (T10–L1) |
0.049 |
| Graft failure rate (MRI) | – | 0% | – |
Values are presented as mean ± standard deviation. ROM = range of motion; VAS = visual analog scale; ASES = American Shoulder and Elbow Surgeons score; SANE = Single Assessment Numeric Evaluation; WORC = Western Ontario Rotator Cuff Index. All patients demonstrated full or near-full ROM at final follow-up. No graft failure was detected on MRI at either 6 or 12 months.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



