Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Centric relation (CR) is a reproducible mandibular reference position that plays a critical role in complex prosthodontic cases. With the advent of digital jaw tracking devices, CR can now be recorded with greater precision through fully digital methods. This study aimed to compare pati-ent-reported outcome measures (PROMs) for the recording of CR determined with conventional and digital techniques. Patients requiring occlusal rehabilitation due to bilateral loss of posterior support in the maxilla were included. Two different jaw relation recording techniques were ap-plied: conventionally determined CR and digitally determined CR. The former was determined using bimanual manipulation, while the latter through multiple mandibular closure recordings performed with an anterior plateau using a jaw-tracking device. PROMs were assessed using Visual Analog Scale (VASs) to evaluate patient experience during jaw relation recording and comfort during restoration try-in. The recording time for both techniques was documented, and the correlation between recording time and VAS scores related to the recording procedure was analyzed. Statistical analyses were performed using the Wilcoxon signed-rank test and Spear-man correlation analysis (α=0.05). Twelve patients were included. No statistically significant difference was found between the two methods in VAS scores assessing patient-reported com-fort and experience. Recording time was significantly shorter for the recording of conventionally determined CR (p=0.002). No statistically significant correlation was found between recording time and patient-reported experience for both techniques (p>0.05). Despite the need for clinician experience and patient compliance, PROMs for digitally determined CR were comparable to those of conventionally determined CR.
Keywords:
PROMs
; jaw relation
; centric relation
; jaw-tracking device
; bimanual manipulation
Introduction
The primary load-bearing components of the masticatory system include posterior teeth and their supporting alveolar bone, temporomandibular joint (TMJ), and anterior teeth. The majority of occlusal support is provided by the posterior teeth and is referred to as posterior support. Loss of posterior teeth may result in impaired masticatory function, esthetic deficiencies, and most importantly, changes in the occlusal vertical dimension (OVD) [1]. OVD is a fundamental parameter in maintaining the neuromuscular (NM) balance of the masticatory system, and failure to reestablish it accurately may lead to adverse effects on the TMJ and the NM system. Therefore, the accurate and predictable reconstruction of OVD in patients with posterior support loss represents a critical step in prosthetic treatment planning [2].
The accurate recording of the jaw relation is one of the fundamental requirements for achieving biologically and mechanically successful prosthetic restorations, particularly in complex cases such as occlusal rehabilitation. Centric relation (CR), defined as a repeatable and clinically stable reference position of the mandible, is widely recommended for full-arch restorations, cases requiring changes in the OVD, and occlusal rehabilitations [3,4,5]. Accurate determination of CR and its proper transfer to restorative procedures are crucial for long-term functional stability and esthetic predictability. The inaccurate determination or transfer of CR and OVD has been associated with TMJ disorders and prosthetic complications. With the increasing use of monolithic zirconia restorations, inappropriate occlusal relationships may result in uneven force distribution and localized stress accumulation, leading to cracks, chipping, or catastrophic failures [6,7,8,9,10]. Recent evidence [11,12,13] suggests that digital approaches enhance the accuracy and reproducibility of restorative procedures, thereby supporting the growing use of digital jaw relation recording methods to help prevent associated clinical complications [14,15,16].
Methods for the determination of CR have been classified in the literature in various ways and are generally described as physiologic, guided, and NM techniques [17,18]. Although differing opinions exist regarding the accuracy and repeatability of these methods, guided techniques have been reported to provide high repeatability when performed by experienced clinicians [19,20,21]. Nevertheless, the reliability of CR determination techniques is highly dependent on clinician experience and patient cooperation, and their relative superiority remains debatable. Axiographic systems allow for the functional assessment of mandibular movements and the dynamic analysis of condylar pathways, thereby contributing to the identification and evaluation of CR as a reproducible mandibular reference position [22,23,24,25]. However, the clinical application of axiographic systems is often considered technique-sensitive and time-consuming, which has limited their routine use and encouraged the adoption of more simplified clinical approaches. In recent years, with the increasing prevalence of digital workflows in prosthodontics, the use of jaw-tracking devices for obtaining and recording jaw relation has increased.
In clinical procedures that require direct patient cooperation, such as jaw relation recording, both the technical accuracy of the method and the patient’s perceived comfort and procedural experience may influence the treatment process. Differences in patient experience between digital and conventional methods have been reported in the literature [26,27,28,29]. In this context, PROMs are regarded as essential assessment tools that complement clinical parameters and incorporate the patient’s perspective into the treatment process [30,31,32]. By focusing on outcomes that are most meaningful to patients, PROMs enable the evaluation of clinical procedures beyond purely technical or clinician-centered measures [33].
Because PROMs directly reflect patient experience, they offer important advantages in evaluating subjective yet clinically meaningful outcomes such as comfort, tolerance, and procedural experience. The current literature indicates that the use of PROMs allows for the quantitative assessment of the patient’s perceived comfort and procedural experience beyond the technical outcomes of clinical procedures, thereby contributing to patient-centered clinical evaluation [34,35,36].
Subjective assessment tools such as the Visual Analog Scale (VAS) allows the quantitative recording of patient experiences and enables clinicians to better balance technical accuracy with patient satisfaction. Accordingly, patient-reported outcomes are increasingly used in the evaluation of jaw relation recording methods, not only to assess patient satisfaction but also to support patient-centered treatment planning [31,32,37].
However, no clinical studies have evaluated the use of jaw-tracking devices in occlusal rehabilitation cases from a PROM perspective. Therefore, the aim of this study was to compare the recordings of conventionally determined centric relation (c-CR) and digitally determined centric relation (d-CR) in patients with posterior support loss requiring occlusal rehabilitation, based on PROMs.
Accordingly, the primary null hypothesis of the study was that there would be no difference in patient-reported outcomes, specifically clinical procedure experience and comfort, between recordings of c-CR and d-CR. The secondary null hypothesis was that there would be no correlation between recording time and patient-reported experience during the jaw relation recording procedure.
2. Materials and Methods
2.1. Study Group
This study included individuals aged 40–55 years who presented to the Faculty of Dentistry, Hacettepe University, for treatment and required bilateral posterior fixed prosthetic treatment and occlusal rehabilitation in the maxilla. The study protocol was approved by the Hacettepe University Clinical Research Ethics Committee (Decision No.: 2024/18-07; Approval Code: KA-24002) and was registered at ClinicalTrials.gov (Identifier: NCT06982898). Written informed consent was obtained from all participants prior to enrollment.
Inclusion criteria:
- Age between 40 and 55 years;
- Bilateral loss of occlusal support involving two premolars and two molars in the maxilla;
- Indication for single-tooth crowns or/and terminal-supported fixed dental prostheses;
- Suitable abutment teeth characteristics (absence of periapical pathology, crown-to-root ratio ≥ 1:1, mobility grade I, probing depth ≤ 4 mm, vital or endodontically treated non-vital teeth) [40];
- Presence of a fixed mandibular dentition with a physiologic occlusal plane (within the limits of the curves of Spee and Wilson) [41];
- No contraindications to dental treatment.
Exclusion Criteria:
- Refusal to sign the informed consent form;
- Use of removable prostheses in the mandible;
- Presence of temporomandibular joint dysfunction, orofacial pain, or acute oral disease;
- History of cervical muscle disorders, cervical disk herniation, or benign paroxysmal positional vertigo.
2.2. Jaw Relation Determination and Recording
In all participants, tooth preparations were completed in a single session during the initial phase of treatment and were performed in accordance with previously described preparation protocols [42,43]. Following this, an intraoral scanner (TRIOS 5; 3Shape A/S, Copenhagen, Denmark) and its corresponding software (3Shape Trios 19.2.0; 3Shape A/S) were used for direct digital recording of the dental arches, and chairside provisional restorations were fabricated using polymethyl methacrylate (PMMA).
At subsequent clinical visits, jaw relations were obtained using two different methods. In the first method, CR was determined via bimanual manipulation and recorded using an intraoral scanner. In the second method, CR was digitally determined from multiple closure recordings obtained with an anterior plateau using a jaw-tracking device. The two jaw relation recording procedures were performed on two separate clinical visits, scheduled two days apart.
Recording of Conventionally Determined Centric Relation (c-CR):
Following completion of the preparations, the occlusal vertical dimension was determined during the second clinical session by considering functional and esthetic determinants. For myofascial relaxation, participants were instructed to perform 10–15 opening and closing movements without tooth contact [44].
During bimanual manipulation, participants were positioned in a fully supine position in the dental unit, with the head stabilized between the clinician’s torso and forearm. This positioning allowed for the controlled guidance of the mandible and prevented involuntary head movements. The clinician placed their thumbs on the patient’s chin and the remaining fingers along the inferior border of the mandible, guiding the mandible gently and continuously in a hinge movement. No sudden or excessive force was applied during manipulation, and the condyles were allowed to sit naturally within the fossae. If muscle response or resistance was perceived during mandibular movement, the procedure was discontinued and repeated after achieving muscle relaxation. When the condyles were perceived to be fully seated in the fossae and the mandible could open and close freely in a hinge movement, this position was accepted as CR [15].
To stabilize the CR position, a layered recording plate was prepared by placing aluminum foil between layers of patterned baseplate wax designed to prevent anterior contact, and the record was positioned intraorally. In the stabilized position, static interocclusal records were obtained from the right and left posterior segments using an intraoral scanner (TRIOS 5; 3Shape, Copenhagen, Denmark) following the manufacturer’s buccal bite scanning protocol. Automatic alignment was performed in the software, and the data were saved after post-processing.
Figure 1.
Stabilization of the centric relation(CR) determined via bimanual manipulation (left); digital jaw relation recording (middle) using an intraoral scanner (right).
Figure 1.
Stabilization of the centric relation(CR) determined via bimanual manipulation (left); digital jaw relation recording (middle) using an intraoral scanner (right).

In this group, CR was clinically determined using a conventional method, and the obtained jaw relation record was digitized. Digitalization of the CR record was achieved using an intraoral scanner, and the record was transferred to prosthetic planning within the digital workflow.
Recording of Digitally Determined Centric Relation (d-CR):
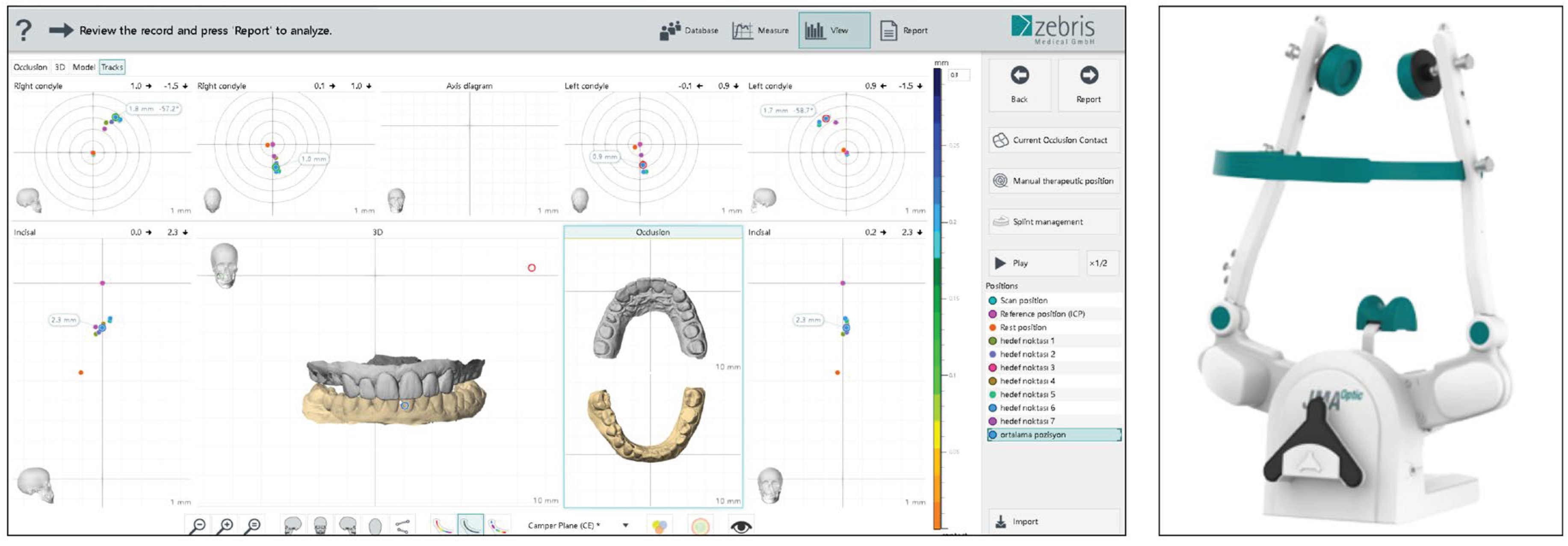
For jaw relation recording, a jaw-motion-tracking and analysis system (zebris JMA Optic; zebris Medical GmbH, Isny im Allgäu, Germany) along with its associated software (WINJAW+; zebris Medical GmbH) was used. The system was configured according to the working protocol of the software’s Function and Digital Occlusion modules. The Camper plane was selected as the reference plane, and the software’s C-arch (condylar reference) tool was used for condylar positioning. To standardize facial references, the subnasal point was marked and reference records related to facial measurements were obtained. A four-point alignment method was used to match intraoral scans in the software. The mandibular static reference position was recorded as a resting position.
Participants were positioned upright in the dental unit, and the electronic facebow was placed parallel to the interpupillary line and the sagittal plane. The porion points and the subnasal reference were determined using the C-arch. Maxillary and mandibular scans were transferred to the software and aligned using four reference points, and the incisal point record was obtained. A customized paraocclusal attachment was used to attach the optical sensor to the mandible. For scan position recording, the CR wax record obtained during the second session was used as a reference position.
For myofascial relaxation, participants were instructed to perform 10–15 opening and closing movements without tooth contact [44]. After intraoral fixation of the customized Reitz anterior plateau [45], participants were instructed to close slowly from maximum opening to approximately 5–10 mm, and subsequently perform a rapid, ballistic closing movement until contact with the anterior plateau was achieved. Each closure was recorded as a target position. This procedure was repeated seven times for each participant. The average of the XYZ coordinates of the seven target positions was calculated within the software and recorded as the “average target position”.
Figure 2.
Digital determination of CR based on multiple mandibular closure recordings obtained using a jaw-tracking system: software interface illustrating the calculation of the average static mandibular position from multiple CR recordings (left), and the jaw-tracking device used in the study (right).
Figure 2.
Digital determination of CR based on multiple mandibular closure recordings obtained using a jaw-tracking system: software interface illustrating the calculation of the average static mandibular position from multiple CR recordings (left), and the jaw-tracking device used in the study (right).
In this group, CR was determined using digital methods, and the obtained jaw relation record was recorded directly in the digital environment. The determination and recording of CR were performed using a digital jaw-tracking system to obtain a static reference position from multiple closure recordings, and the record was transferred to prosthetic planning within the digital workflow.
2.3. PROMs
PROMs were evaluated in two clinical stages. The first evaluation was performed immediately after completion of the recording procedure and aimed to assess the experience of the recording method. The second evaluation was conducted during the try-in of the restorations fabricated based on each jaw relation record and aimed to assess the perceived comfort during restoration try-in.
After completion of the recording procedure with each method, participants were asked to complete an evaluation form. Patient experience during the clinical procedure was assessed using a Visual Analog Scale (VAS) ranging from 0 to 10, where 0 represents an extremely negative experience and 10 represents an extremely positive experience. In addition, participants who experienced both methods were asked the question, “Which method would you prefer for the next procedure?” Responses were recorded as a binary choice (c-CR/d-CR). All evaluations were performed immediately after participants had experienced both methods sequentially, without any operator guidance or reminders. Recording time was documented for both methods.
For the second evaluation, restorations were fabricated based on jaw relation data obtained with each recording method. The datasets were exported in appropriate formats and transferred to computer-aided design (CAD) software. All datasets were transferred to Exocad 3.2 Elefsina software (Exocad GmbH, Darmstadt, Germany) for digital design procedures. To maintain identical occlusal morphology between the two groups, the design created for c-CR was adapted to d-CR, and final adjustments were made according to static occlusion.
The approved digital designs were manufactured using a five-axis milling system (Vhf E5; Vhf GmbH, Germany) with a subtractive manufacturing process from PMMA blocks (Polident Draga, Slovenia). Thus, for each participant, two bilateral posterior restorations based on two different jaw relation records were obtained.
Restorations fabricated based on jaw relation records obtained with both methods were tried intraorally. During the try-in procedure proximal contacts, internal fit, and marginal adaptation were sequentially evaluated. Proximal contacts were assessed using dental floss, and internal and marginal fit were evaluated by verifying the presence of a uniform, thin film of elastomeric disclosing material (Fit Checker Advanced Blue; GC Corporation, Tokyo, Japan) under ×2.5 magnification using a dental loupe. Minor clinical adjustments were performed when necessary to achieve acceptable seating and proximal contacts, as described previously [46]. Restorations requiring major clinical adjustments or exhibiting inadequate fit were excluded from the evaluation. Following clinical approval, participants were asked to score the restorations without performing any occlusal adjustments.
During the try-in procedure, both the participant and the investigator responsible for outcome assessment were blinded, and the restorations were evaluated in a randomized order. All clinical procedures, including jaw relation recordings and try-in appointments, were performed by a single investigator (E.S.K.). Blinding procedures and the evaluation of patient-reported outcomes, including VAS assessments, were conducted by a second independent investigator (K.A.).
At the end of each try-in session, participants were asked to rate both the first-tried and second-tried restorations using a VAS based on perceived comfort. Repetitive opening and closing movements were performed between try-ins to facilitate myofascial relaxation [44].
2.4. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics software (Version 21.0; IBM Corp., Armonk, NY, USA). Statistical power was calculated using G*Power 3.1 software (Universität Düsseldorf, Germany). As VAS scores related to jaw relation recording experience and restoration try-in comfort were considered ordinal data, non-parametric Wilcoxon signed-rank tests were used for intergroup comparisons.
Normality of the recording time variable, calculated in minutes, was evaluated using the Shapiro–Wilk test. Since the data did not show a normal distribution, the Wilcoxon signed-rank test was also applied for the comparison of recording time between the two methods.
Statistical significance was set at p<0.05. The correlation between recording time and VAS scores related to the jaw relation recording procedure was evaluated using Spearman’s rho correlation coefficient. In addition, the association between VAS scores related to jaw relation recording experience and restoration try-in comfort was explored using Spearman’s rho correlation coefficient.
2.5. Sample Size Calculation
The sample size of the study was determined based on a power analysis considering findings from similar studies in the literature and the statistical methods to be used. The analysis indicated that, with a 90% statistical power (1–β = 0.90) and a 5% significance level (α=0.05), a minimum of 13 participants would be required to detect a difference between two dependent measurements.
During the study period, 13 participants were enrolled. One participant was excluded from the analysis due to insufficient cooperation during both clinical procedures. Consequently, data from 12 participants were included in the final analysis.
A post hoc power analysis performed using G*Power software, assuming an effect size of 0.8 and a 95% confidence level, revealed a statistical power of 81%, indicating that the final sample size was acceptable for detecting meaningful differences.
3. Results
A total of 12 patients were included in the study (4 males and 8 females), with a mean age of 45 years. When patient preferences regarding jaw relation determination and recording methods were evaluated, 58% of the participants preferred c-CR, whereas 42% preferred d-CR.
The mean VAS score for c-CR jaw relation recordings was 7.7 ± 1.3 (median: 7.0), whereas the mean VAS score for d-CR recordings was 7.0 ± 1.7 (median: 7.5). No statistically significant difference was observed between the two methods in terms of patient-reported experience during the jaw relation recording procedure (p = 0.296). The mean VAS score for restorations fabricated based on c-CR recordings was 6.6 ± 2.1 (median: 7.0), whereas restorations fabricated based on d-CR recordings had a mean VAS score of 8.0 ± 1.4 (median: 8.0). A difference close to the threshold of statistical significance was observed between the two methods with respect to VAS scores assigned to the restorations (p = 0.051). The mean recording time for c-CR recordings was 10.7 ± 2.2 minutes (median: 10.5), whereas that for d-CR recordings was 20.0 ± 2.2 minutes (median: 19.5). The difference in recording time between the two methods was statistically significant (p = 0.002). Table 1 summarizes the comparison of patient-reported outcome measures (VAS scores) and recording times between c-CR and d-CR.
The correlation between recording time and VAS scores related to patient-reported experience during the jaw relation recording procedure was evaluated using Spearman’s correlation analysis. No statistically significant correlation was found between recording time and VAS scores for either recording method (c-CR: p = 0.619; d-CR: p = 0.697). A moderate, positive association was observed between VAS scores related to jaw relation recording experience and VAS scores assigned to the restorations for both methods. In the c-CR group, this association was ρ = 0.577 (p=0.05), whereas in the d-CR group, the association was ρ = 0.539 (p=0.07).
4. Discussion
In the present study, the recording of CR with conventional and digital techniques was evaluated in patients requiring occlusal rehabilitation, with a specific focus on patient-reported experience during the jaw relation recording stage and patient-reported comfort during restoration try-in. Overall, the findings indicate that both approaches were perceived similarly by patients across the evaluated clinical stages. The primary null hypothesis is not rejected for either the jaw relation recording stage or the restoration try-in stage. Accordingly, the insignificant difference in patient-reported outcomes suggests that the choice between c-CR and d-CR may not substantially influence patient comfort or procedural experience during either jaw relation recording or restoration try-in.
Recording time alone does not provide information regarding patient perception or the qualitative aspects of the clinical procedure. Therefore, the assessment of jaw relation recording methods should not rely solely on time-based metrics but should also incorporate patient-centered outcome measures to achieve a more comprehensive evaluation of clinical performance.
Correlation analyses demonstrated a moderate, positive association between VAS scores related to jaw relation recording experience and VAS scores assigned to the restorations for both methods. However, as these associations remained at a borderline level of statistical significance and restoration evaluations were performed under blinded conditions, a causal relationship between patient experience during the recording stage and restoration assessment cannot be established.
In addition, the absence of a statistically significant correlation between recording time and patient-reported experience during the jaw relation recording procedure indicates that patient perception cannot be explained solely by quantitative time-based measures. Accordingly, the secondary null hypothesis, stating that no correlation exists between recording time and patient-reported experience, was accepted.
PROMs represent a subjective and multidimensional construct that reflects patient perception, comfort, tolerance, and shared decision-making throughout the treatment process, independent of technical clinical success or isolated quantitative parameters such as procedure time. This aspect is particularly relevant in clinical procedures requiring active patient cooperation, such as jaw relation recording, where patient experience may influence both treatment acceptance and clinical feasibility. Previous studies have emphasized that patient perception cannot be fully explained by measurable time-related parameters alone, as it is shaped by contextual, experiential, and individual factors [27,28,29,32]. The absence of a significant correlation between recording time and patient-reported experience observed in the present study is consistent with these findings.
In the c-CR technique, CR is determined using bimanual manipulation, which may be regarded as a more simplified and clinically accessible approach. Although axiographic systems have been proposed for the functional assessment of mandibular movements during centric relation determination, their clinical application is often considered technique-sensitive and highly dependent on clinician experience, which has limited their widespread adoption in routine clinical practice. Consequently, simplified methods for CR determination remain commonly used.
Recording the mandibular position based on a single static registration may necessitate increased occlusal adjustment during the restorative phase and may additionally be associated with the potential development of occlusal adjustment-related clinical and prosthetic complications. Objective clinical parameters commonly used to evaluate restorative outcomes, including occlusal contact distribution, morphological congruence, and prosthetic acceptability, were beyond the scope of the present study and were therefore not assessed [12,47]. The lack of objective restorative evaluations limits the interpretation of prosthetic outcomes associated with single-position digital-centric relation records. Further clinical studies incorporating objective outcome measures are required to clarify the effects of occlusal adjustment and related prosthetic complications.
In contrast, d-CR requires the use of a jaw-tracking device capable of analyzing mandibular movements, introducing additional clinical considerations related to clinician experience and patient tolerance of the tracking system. Despite this increased technological and procedural complexity, the findings of the present study demonstrate that the d-CR approach does not result in a statistically significant difference in patient-reported outcomes when compared with the c-CR approach. This observation suggests that, despite the additional technological complexity of digitally determined centric relation, the method is well accepted by patients and does not negatively influence patient-reported experience.
With the emergence of digital technologies in dentistry, numerous studies have evaluated digital workflows involving intraoral scanners across different clinical scenarios from the perspective of patient-reported outcome measures (PROMs) [12,28,29,48,49,50,51,52,53]. These studies have highlighted the impact of digital impression techniques on patient comfort, procedural experience, and overall perception of clinical procedures, emphasizing the importance of PROM-based evaluations. Similarly, the increasing clinical use of jaw-tracking devices has generated a growing interest in assessing methods of digital jaw relation recording from a PROM perspective. However, despite this growing interest, no clinical studies have directly compared the recordings of conventionally determined CR and digitally determined CR based on PROMs. In this context, the present study provides a PROM-centered approach by incorporating patient perception into the evaluation of digital jaw relation recording methods within routine clinical practice.
In clinical practice, the selection of a jaw relation recording method should not be based solely on scientific validity or procedural simplicity, but should also consider patient-related factors. c-CR and d-CR may exert variable effects across different stages of clinical application and patient perception. Accordingly, the combined evaluation of PROMs and clinical time parameters may support more rational and individualized planning of digital prosthetic workflows.
Although digitally determined centric relation represents a relatively newer technological approach, the findings of the present study indicate that its clinical applicability is predictable and comparable to conventional methods in terms of patient-reported experience.
The lack of objective prosthetic evaluations and long-term follow-up represents the main limitation of the present study.
Author Contributions
Conceptualization, E.S.K. and K.A.; Methodology, E.S.K. and K.A.; Investigation, E.S.K.; Writing—original draft preparation, E.S.K.; Writing—review and editing, E.S.K. and K.A.; Supervision, K.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Hacettepe University Scientific Research Projects Coordination Unit.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Hacettepe University with protocol code KA-24002 and the Ministry of Health, Turkish Medicines, and Medical Devices Agency (No.E.68869993-511).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We thank Dr. Jürgen Reitz for sharing the concept and CAD/STL files of a customized intraoral anterior plateau (using the ‚zebris occlusal alignment fork) for maxillo-mandibular relation recording with the zebris JMA Optic jaw relation module.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gross, M., et al., The science and art of occlusion and oral rehabilitation. Vol. 7. 2015: Quintessence publishing.
- Alhajj, M.N., et al., Determination of occlusal vertical dimension for complete dentures patients: an updated review. Journal of oral rehabilitation, 2017. 44(11): p. 896-907. [CrossRef]
- The Glossary of Prosthodontic Terms: Ninth Edition. J Prosthet Dent, 2017. 117(5S): p. e1-e105.
- Manfredini, D., et al., Centric relation—A biological perspective of a technical concept. Journal of Oral Rehabilitation, 2023. 50(11): p. 1355-1361. [CrossRef]
- Kois, J. and K. Phillips, Occlusal vertical dimension: alteration concerns. Compendium of Continuing Education in Dentistry (Jamesburg, NJ: 1995), 1997. 18(12): p. 1169-74, 1176.
- Nakamura, Y., S. Hojo, and H. Sato, The effect of surface roughness on the Weibull distribution of porcelain strength. Dental materials journal, 2010. 29(1): p. 30-34. [CrossRef]
- Curran, P., et al., Grinding damage assessment for CAD-CAM restorative materials. Dental Materials, 2017. 33(3): p. 294-308. [CrossRef]
- Denry, I. and J.R. Kelly, State of the art of zirconia for dental applications. Dental materials, 2008. 24(3): p. 299-307. [CrossRef]
- Zhang, Y. and B.R. Lawn, Evaluating dental zirconia. Dental Materials, 2019. 35(1): p. 15-23.
- Canneto, J.-J., et al., Grinding damage assessment on four high-strength ceramics. Dental materials, 2016. 32(2): p. 171-182. [CrossRef]
- Zarbakhsh, A., et al., Accuracy of digital impression taking using intraoral scanner versus the conventional technique. Frontiers in Dentistry, 2021. 18: p. 6. [CrossRef]
- Karasan, D., et al., Occlusal adjustment of 3-unit tooth-supported fixed dental prostheses fabricated with complete-digital and-analog workflows: A crossover clinical trial. Journal of Dentistry, 2023. 128: p. 104365. [CrossRef]
- Wang, J., et al., Recent advances in digital technology in implant dentistry. Journal of Dental Research, 2024. 103(8): p. 787-799. [CrossRef]
- Radu, M., D. Radu, and M. Abboud, Digital recording of a conventionally determined centric relation: A technique using an intraoral scanner. The Journal of prosthetic dentistry, 2020. 123(2): p. 228-231. [CrossRef]
- Solaberrieta, E., et al., Determining the requirements, section quantity, and dimension of the virtual occlusal record. The Journal of prosthetic dentistry, 2016. 115(1): p. 52-56. [CrossRef]
- Park, J.H., et al., A digital approach to the evaluation of mandibular position by using a virtual articulator. The Journal of Prosthetic Dentistry, 2021. 125(6): p. 849-853. [CrossRef]
- Neto, C.L.d.M.M., et al., Comparison of techniques for obtaining centric relation based on the reproducibility of the condylar positions in centric relation—A systematic review. European journal of dentistry, 2021: p. 251-257.
- Hellmann, D., et al., Methods of determining centric relation: a comparative study. J Cranio-Mand Func, 2014. 6: p. 193-206.
- Dawson, P.E., Functional occlusion: from TMJ to smile design. 2006: Elsevier Health Sciences. [CrossRef]
- Dawson, P.E., New definition for relating occlusion to varying conditions of the temporomandibular joint. The Journal of prosthetic dentistry, 1995. 74(6): p. 619-627. [CrossRef]
- McKee, J.R., Comparing condylar position repeatability for standardized versus nonstandardized methods of achieving centric relation. The Journal of prosthetic dentistry, 1997. 77(3): p. 280-284. [CrossRef]
- Theusner, J., et al., Axiographic tracings of temporomandibular joint movements. The Journal of prosthetic dentistry, 1993. 69(2): p. 209-215. [CrossRef]
- Posselt, U., Physiology of occlusion and rehabilitation. Blackwell scientific publications, 1962: p. 31-39.
- Parlett, K., et al., Temporomandibular joint axiography and MRI findings: a comparative study. The Journal of Prosthetic Dentistry, 1993. 70(6): p. 521-531. [CrossRef]
- Piehslinger, E., et al., Reproducibility of the condylar reference position. Journal of orofacial pain, 1993. 7(1).
- Wittneben, J.G., et al., Patient-reported outcome measures focusing on aesthetics of implant-and tooth-supported fixed dental prostheses: A systematic review and meta-analysis. Clinical oral implants research, 2018. 29: p. 224-240. [CrossRef]
- Yuzbasioglu, E., et al., Comparison of digital and conventional impression techniques: evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC oral health, 2014. 14(1): p. 10. [CrossRef]
- Gjelvold, B., et al., Intraoral digital impression technique compared to conventional impression technique. A randomized clinical trial. Journal of Prosthodontics, 2016. 25(4): p. 282-287. [CrossRef]
- Pachiou, A., et al., Patient-Reported Outcomes of Digital Versus Conventional Impressions for Implant-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 2025. 15(9): p. 427. [CrossRef]
- Jokstad, A., Patient-reported outcomes (PROs) versus patient-reported outcome measures (PROMs)—Is there a difference? Clinical and Experimental Dental Research, 2018. 4(3): p. 61. [CrossRef]
- Hua, F., Dental patient-reported outcomes update 2022. Journal of Evidence-Based Dental Practice, 2023. 23(1): p. 101802. [CrossRef]
- Hua, F., Dental Patient-Reported Outcomes Update 2024. Journal of Evidence-Based Dental Practice, 2025: p. 102122. [CrossRef]
- Reissmann, D.R., Dental patient-reported outcome measures are essential for evidence-based prosthetic dentistry. 2019, Elsevier. p. 1-6. [CrossRef]
- Aiyegbusi, O.L., et al., Recommendations to address respondent burden associated with patient-reported outcome assessment. Nature medicine, 2024. 30(3): p. 650-659. [CrossRef]
- Lamont, T.J. and J.E. Clarkson, Core outcome sets and dental patient reported outcomes. Journal of Evidence-Based Dental Practice, 2022. 22(1): p. 101659. [CrossRef]
- Hughes, S.E., et al., Opportunities and challenges for patient-reported outcome assessment in multimorbidity research and practice. Nature Medicine, 2024. 30(11): p. 3042-3043. [CrossRef]
- Chander, N.G., Visual analog scale in prosthodontics. 2019, Medknow. p. 99-100. [CrossRef]
- Mariotti, A. and A.F. Hefti, Defining periodontal health. BMC oral health, 2015. 15(Suppl 1): p. S6. [CrossRef]
- Schiffman, E., et al., Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. Journal of oral & facial pain and headache, 2014. 28(1): p. 6. [CrossRef]
- Mühlemann, H.R., Tooth mobility: a review of clinical aspects and research findings. The Journal of Periodontology, 1967. 38(6P2): p. 686-708. [CrossRef]
- Hohmann, A. and W. Hielscher, Foundations of Dental Technology: Anatomy and Physiology. 2014: Quintessence Publishing Company Incorporated. [CrossRef]
- Rosenstiel, S.F., M. Land, and J. Fujimoto, Contemporary Fixed Prosthodontics. 4 [sup] th ed. St. Louis: Mosby, 2006. 223.
- Goodacre, C.J., W.V. Campagni, and S.A. Aquilino, Tooth preparations for complete crowns: an art form based on scientific principles. The Journal of prosthetic dentistry, 2001. 85(4): p. 363-376. [CrossRef]
- Bumann, A. and U. Lotzmann, TMJ Disorders and Orofacial Pain: The Role of Dentistry in a Multidisciplinary Diagnostic Approach. 2002: Thieme.
- Reitz, J., Customized intraoral anterior plateau (using the 'zebris occlusal alignment fork’) for maxillo-mandibular relation recording with zebris JMA Optic (jaw relation module).Personal communication to Kivanc Akca, June 2024.
- Win, T.T., et al., Fit accuracy of complete crowns fabricated by generative artificial intelligence design: a comparative clinical study. The journal of advanced prosthodontics, 2025. 17(4): p. 224. [CrossRef]
- Zhang, Y., et al., Quantitative clinical adjustment analysis of posterior single implant crown in a chairside digital workflow: A randomized controlled trial. Clinical oral implants research, 2019. 30(11): p. 1059-1066. [CrossRef]
- Joda, T., F. Zarone, and M. Ferrari, The complete digital workflow in fixed prosthodontics: a systematic review. BMC oral health, 2017. 17(1): p. 124. [CrossRef]
- Mühlemann, S., et al., Is the use of digital technologies for the fabrication of implant-supported reconstructions more efficient and/or more effective than conventional techniques: A systematic review. Clinical Oral Implants Research, 2018. 29: p. 184-195. [CrossRef]
- Bishti, S., et al., Patient-reported outcome measures (PROMs) of implant-supported reconstructions using digital workflows: A systematic review and meta-analysis. Clinical Oral Implants Research, 2021. 32: p. 318-335.
- Bandiaky, O.N., et al., Comparative assessment of complete-coverage, fixed tooth-supported prostheses fabricated from digital scans or conventional impressions: A systematic review and meta-analysis. The Journal of Prosthetic Dentistry, 2022. 127(1): p. 71-79. [CrossRef]
- Haddadi, Y., G. Bahrami, and F. Isidor, Evaluation of operating time and patient perception using conventional impression taking and intraoral scanning for crown manufacture: a split-mouth, randomized clinical study. International Journal of Prosthodontics, 2018. 31(1). [CrossRef]
- Sakornwimon, N. and C. Leevailoj, Clinical marginal fit of zirconia crowns and patients’ preferences for impression techniques using intraoral digital scanner versus polyvinyl siloxane material. The Journal of prosthetic dentistry, 2017. 118(3): p. 386-391. [CrossRef]

Table 1.
Comparison of Visual Analog Scale (VAS) scores assessing patient-reported experience during jaw relation recording and comfort during try-in, and recording time between conventionally determined centric relation (c-CR) and digitally determined centric relation (d-CR).
Table 1.
Comparison of Visual Analog Scale (VAS) scores assessing patient-reported experience during jaw relation recording and comfort during try-in, and recording time between conventionally determined centric relation (c-CR) and digitally determined centric relation (d-CR).
| Outcome | Method | Mean | SD | MD | Min. | Max. | p |
|---|---|---|---|---|---|---|---|
| Jaw Relation Recording | c-CR | 7.7 | 1.3 | 7.0 | 6 | 10 | 0.296 |
| d-CR | 7.0 | 1.7 | 7.5 | 5 | 10 | ||
| Restoration Try-in | c-CR | 6.6 | 2.1 | 7.0 | 2 | 10 | 0.051 |
| d-CR | 8.0 | 1.4 | 8.0 | 5 | 10 | ||
| Recording Time (minute) | c-CR | 10.7 | 2.2 | 10.5 | 8 | 15 | 0.002* |
| d-CR | 20.0 | 2.2 | 19.5 | 17 | 25 |
(Abbreviations:
SD, standard deviation; MD, median; Min., minimum; Max., maximum. *Statistically significant at p < 0.05.).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



