
Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Background/Objectives: Incidental gallbladder cancer (IGBC) is an uncommon but clinically important malignancy, typically diagnosed unexpectedly after cholecystectomy performed for benign indications. Despite its incidental nature, IGBC may present with advanced pathological features and unfavorable outcomes. This study aimed to evaluate the incidence, clinicopathological characteristics, surgical management, and prognostic factors of IGBC in a large cholecystectomy cohort from a tertiary referral center. Methods: A retrospective analysis was performed on 19,798 cholecystectomy procedures conducted between January 2010 and December 2025. Patients with a preoperative diagnosis of gallbladder cancer or incomplete clinical or pathological data were excluded. Only cases with invasive incidental gallbladder cancer (IGBC) were included, whereas dysplasia and carcinoma in situ were excluded. Demographic, clinical, surgical, pathological, and survival data were systematically collected. Results: Incidental gallbladder cancer was identified in 43 patients (0.22%). The mean age was 71.4 ± 9.9 years, and 74.4% were female. Gallstones were present in 88.4% of patients. Adenocarcinoma was the predominant histology (90.7%), and pT2 disease was the most common stage (41.9%), while 25.6% had advanced-stage tumors (pT3–T4). Median OS was 26.0 months, and median DFS was 25.5 months in non-metastatic patients. Pathological T stage was significantly associated with both OS and DFS. Advanced T stage, positive surgical margins, perineural invasion, lymphovascular invasion, and increasing tumor size were significantly associated with worse DFS. Re-resection rates were limited, mainly due to advanced age and comorbidities. Conclusion: Although incidental gallbladder cancer is rare, it leads to clinically and oncologically significant outcomes. In this study, pathological T stage emerged as a key prognostic factor influencing both overall survival and disease-free survival. In addition, perineural invasion, lymphovascular invasion, and positive surgical margins were identified as the main pathological factors adversely affecting disease-free survival.
Keywords:
incidental gallbladder cancer
; cholecystectomy
; pathological T stage
; disease-free survival
1. Introduction
Gallbladder cancer (GBC) is an aggressive malignancy characterized by rapid progression, poor prognosis, and high mortality, and it remains difficult to treat [1]. It accounts for approximately 4% of all gastrointestinal cancers and is the most common malignancy of the biliary tract [2,3]. The vast majority of cases consist of highly aggressive adenocarcinomas and are responsible for approximately 3,710 new deaths annually in the United States alone [2,4,5]. GBC is generally associated with an unfavorable prognosis even after treatment, with reported median overall survival ranging from 3 to 22 months [6,7,8]. Multiple factors contribute to disease development, including gallstones, calcified gallbladder wall, adenomatous polyps, obesity, estrogen exposure, choledochal cysts, and chemical carcinogens [9,10]. Among these, gallstones are considered the strongest risk factor, being associated with disease development in 75–90% of cases [9,11].
In patients undergoing cholecystectomy for benign indications witho.ut preoperative suspicion of malignancy, the detection of carcinoma in the gallbladder specimen on histopathological examination is defined as incidental gallbladder cancer (IGBC) [1,2,3,12]. The reported incidence of IGBC ranges from 0.25% to 3.3% [13]. Approximately 27–41% of all gallbladder cancers are reported to be diagnosed incidentally [14]. With the global increase in the number of laparoscopic cholecystectomies, a corresponding rise in the frequency of IGBC cases has also been reported [1,15].
The primary reason IGBC cannot be detected in the preoperative period is the absence of specific clinical or radiological findings. Although certain weakly supported warning signs—such as irregular gallbladder wall thickening, large polyps, nonvisualization of the gallbladder, or lymphadenopathy—have been described, these findings do not reliably direct surgeons toward the presence of IGBC [2,16,17]. The most debated issues in the management of IGBC include whether additional surgery should be performed, the optimal timing if indicated, and the extent of the surgical procedure [1,15]. In most IGBC cases, a second surgical intervention may be required to achieve oncologic adequacy [15]. However, the survival benefit of additional resection across different stages of GBC remains controversial [1].
In this retrospective study, we aimed to evaluate the clinical, surgical, and pathological characteristics of patients diagnosed with incidental gallbladder cancer among cholecystectomy cases performed at our institution between 2010 and 2025, and to compare these findings with the existing literature in order to contribute to contemporary approaches in the management of IGBC.
2. Materials and Methods
2.1. Study Design and Patient Selection
This retrospective study was conducted using the archival records of our Department of General Surgery. A total of 19,798 patients who underwent cholecystectomy between January 2010 and December 2025 were evaluated. Patients with a known preoperative diagnosis of gallbladder cancer (n = 15) and those with incomplete clinical or pathological data (n = 376) were excluded. The remaining 19,407 patients underwent surgery for benign indications. Within this cohort, incidental gallbladder cancer (IGBC) was identified in 43 patients (0.22%). The diagnosis was established intraoperatively in 4 patients and by postoperative histopathological examination in 39 patients.
Only patients with a diagnosis of invasive incidental gallbladder cancer were included in this study. Cases of dysplasia and carcinoma in situ (Tis) were excluded from the analysis. Dysplastic lesions do not represent a patient group comparable to invasive cancer because of their heterogeneous biological behavior and unpredictable course regarding progression to invasive carcinoma. Carcinoma in situ lesions, on the other hand, do not breach the basement membrane and lack invasive potential, thereby being biologically distinct from invasive gallbladder cancers in terms of prognostic analyses. Inclusion of these lesions could have artificially improved survival outcomes and introduced methodological bias; therefore, they were excluded from the study. The patient selection process is summarized in Figure 1.
2.2. Data Collection and Variables
Demographic characteristics, preoperative laboratory results, ultrasonographic evaluations, intraoperative findings, and details of the surgical procedures were recorded for all patients. Preoperative laboratory parameters were obtained prior to the index cholecystectomy, whereas tumor markers were evaluated only after the histopathological confirmation of malignancy. Histopathological assessment included tumor type, anatomical location, histologic grade, and the presence of perineural and lymphovascular invasion; resection margin status was recorded according to pathology reports. Tumor staging was performed in accordance with the 8th edition of the American Joint Committee on Cancer (AJCC) classification.
Because malignancy was incidentally detected after cholecystectomy performed for benign indications in all patients, the initial surgical procedure was limited to cholecystectomy alone. Consequently, lymph node status (N stage) was not included in the analysis. The presence of distant metastasis (M stage) was assessed based on postoperative imaging studies performed after histopathological confirmation of malignancy. Postoperative complications, the need for re-resection, and clinical outcomes were also included in the analysis.
2.3. Surgical Treatment Approach
All patients underwent laparoscopic or open cholecystectomy with a preoperative diagnosis of benign disease. Patients diagnosed with IGBC in the postoperative period were evaluated for the need for additional surgery based on clinical, radiological, and pathological findings. A total of 31 patients underwent simple cholecystectomy alone and were followed without additional surgical intervention. In ten patients, gallbladder bed resection was performed in addition to cholecystectomy. In two patients, anatomical resection of liver segments IVb–V was added to cholecystectomy. The main reasons for not performing additional surgical intervention in patients managed with simple cholecystectomy were early-stage disease and the presence of concomitant comorbid conditions.
2.4. Statistical Analysis
All analyses were performed using IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). Baseline demographic, clinical, operative, pathological, and laboratory characteristics were summarized as mean ± standard deviation (SD) for normally distributed continuous variables and as median [interquartile range (IQR)] for non-normally distributed continuous variables; categorical variables were reported as n (%). Distributional assumptions were assessed using visual inspection of histograms and Q–Q plots in conjunction with the Shapiro–Wilk test.
Overall survival (OS) was defined as the time from the index surgery to death from any cause; patients alive at the last follow-up were censored. Disease-free survival (DFS) was analyzed among baseline M0 patients and defined as the time from surgery to the first documented recurrence or death, whichever occurred first; patients alive and recurrence-free at the last follow-up were censored. Kaplan–Meier methods were used to estimate survival functions, summarized by median and mean survival times (months) with 95% confidence intervals (CIs). In addition, actuarial survival rates at 24, 48, and 72 months were obtained using a life-table approach with 24-month intervals.
Associations between candidate predictors and OS/DFS were evaluated using univariable Cox proportional hazards regression, reporting hazard ratios (HRs) with 95% CIs and two-sided Wald p-values. The proportional hazards assumption was evaluated using log-minus-log survival plots and time-by-covariate interaction checks. Cox models were fitted using a complete-case approach; therefore, OS models typically included n = 42 (SPSS excluded one patient censored before the earliest event). The CA 19-9 model included n = 41 due to one additional missing CA 19-9 value, and DFS models restricted to M0 patients included n = 35. Statistical significance was defined as p < 0.05 (two-sided).
2.5. Ethical Approval
All procedures performed in this study were conducted in accordance with the ethical standards of the institutional and/or national research committees and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This study was approved by the Local Ethical Committee (Approval number: 2025/010.99/21/33; Approval date: 30.10.2025).
3. Results
As summarized in Table 1, the study cohort included 43 patients with IGBC; the mean age was 71.4 ± 9.9 years, and women predominated (32/43, 74.4%). Most patients had at least one comorbidity (39/43, 90.7%). With respect to preoperative biliary history, cholecystitis was common (24/43, 55.8%), and choledocholithiasis (14/43, 32.6%) and pancreatitis (12/43, 27.9%) were also frequently observed. A history of prior abdominal surgery was present in 14 patients (32.6%), whereas approximately two-thirds of the cohort had no previous abdominal surgical history. Smoking history was documented in 12/43 (27.9%), alcohol use in 5/43 (11.6%), and prior ERCP in 9/43 (20.9%).
On preoperative ultrasonography, gallbladder wall thickness was 3–10 mm in 24/43 (55.8%), ≤3 mm in 15/43 (34.9%), and >10 mm in 4/43 (9.3%). The primary ultrasonographic finding was gallstones in 38/43 (88.4%), whereas polyps were reported in 5/43 (11.6%). Among patients with gallstones (N = 38), the largest stone size was most often 1–3 cm (24/38, 63.2%), followed by <1 cm (12/38, 31.6%); stones >3 cm were uncommon (2/38, 5.3%).
Most procedures were performed electively (35/43, 81.4%), with urgent surgery in 8/43 (18.6%). A minimally invasive approach was predominant: laparoscopic in 31/43 (72.1%), with conversion in 5/43 (11.6%) and
initially planned open surgery
in 7/43 (16.3%).
The index surgical procedure was most commonly simple cholecystectomy (31/43, 72.1%). In addition, gallbladder bed resection was performed in 10 patients (23.3%) in conjunction with cholecystectomy, while anatomical segment IVb–V resection was added to cholecystectomy in 2 patients (4.7%).
Postoperative complications were uncommon (41/43, 95.3% had no complication); bile leak and
superficial surgical site infection
occurred in 1/43 (2.3%) each. The diagnosis was primarily postoperative/incidental (39/43, 90.7%), with intraoperative recognition in 4/43 (9.3%).
Pathologically, adenocarcinoma was the dominant histology (39/43, 90.7%). Tumors were most frequently located in the body/corpus (26/43, 60.5%), followed by diffuse involvement (12/43, 27.9%); fundus (3/43, 7.0%) and neck (2/43, 4.7%) locations were less common. Perineural invasion was present in 19/43 (44.2%) and lymphovascular invasion in 17/43 (39.5%). Histologic grade was most often intermediate (20/43, 46.5%), followed by high grade (14/43, 32.6%) and low grade (9/43, 20.9%). Pathologic T stage was centered on T2 disease (18/43, 41.9%); T1a and T1b each accounted for 7/43 (16.3%), while T3 and T4 comprised 8/43 (18.6%) and 3/43 (7.0%), respectively. Distant metastasis was documented in 7/43 (16.3%). Resection margins were negative (R0) in 29/43 (67.4%); positivity involved the cystic duct (5/43, 11.6%) and liver bed (5/43, 11.6%), while margin status was not assessable in 4/43 (9.3%). Tumor size showed substantial variability, with a median of 15 mm [IQR 33].
Baseline laboratory parameters, including complete blood count, liver function tests, coagulation profile, and tumor markers, were evaluated as part of the initial assessment. Overall, these values were largely within expected ranges and comparable to those reported for typical cholecystectomy populations, and none demonstrated a clear association with oncologic outcomes in exploratory analyses.
As presented in Table 2, Kaplan–Meier estimation for the full IGBC cohort (n = 43) demonstrated a median OS of 26.0 months, with a mean OS of 42.37 ± 34.12 months. Actuarial (life-table) estimates at 24-month intervals indicated cumulative OS proportions of 54% at 24 months, 40% at 48 months, and 11% at 72 months. DFS was evaluated in patients without distant metastasis at baseline (M0) and, using a complete-case approach, included 35 patients (14 events; 21 censored). In this cohort, the median DFS was 25.5 months and the mean DFS was 38.14 ± 34.31 months. Life-table estimates showed DFS proportions of 60% at 24 months, 53% at 48 months, and 38% at 72 months. Given the high censoring fraction (21/35), late follow-up estimates should be interpreted cautiously.
As shown in
Table 3
, grouped pathologic T stage was significantly associated with overall survival (OS) (overall Wald p = 0.038). Relative to T1 disease, T2 showed a non-significant tendency toward a lower hazard of death (HR 0.38, p = 0.071), whereas T3–T4 was not significantly different from T1 (HR 2.26, p = 0.200). Resection margin positivity (R1/R2 vs R0) was not associated with OS (HR 1.41, p = 0.524). Similarly, lymphovascular invasion (HR 1.56, p = 0.411) and perineural invasion (HR 1.14, p = 0.807) were not significant predictors of OS. High histologic grade was also not significantly associated with OS (HR 0.46, p = 0.124). For continuous covariates, tumor size (per 10-mm increase) was not associated with OS (HR 0.91, p = 0.551), and age (per 1-year increase) was likewise non-significant (HR 0.99, p = 0.664). Among clinical factors, urgent surgery was associated with higher mortality (HR 3.47, 95% CI 1.08–11.15; p = 0.037). In contrast, any comorbidity (yes vs no) was associated with a lower hazard of death (HR 0.19, 95% CI 0.05–0.71; p = 0.013). Regarding biomarkers and perioperative risk, log-transformed CA 19-9 (model-specific n = 41 due to one missing value) was not associated with OS (HR 0.87, p = 0.345). ASA class III–IV vs I–II (also n = 41) and hypoalbuminemia (<3.5 g/dL) were not significant predictors (ASA: HR 0.53, p = 0.167; albumin: HR 0.50, p = 0.359). Finally, distant metastasis (M1 vs M0) was not significantly associated with OS in univariable analysis (HR 1.70, p = 0.484).
As shown in
Table 4
, in the M0-restricted cohort (complete-case Cox models: n = 35; 14 recurrence/death events), grouped pathologic T stage was significantly associated with disease-free survival (DFS) (overall Wald p = 0.013), demonstrating a graded increase in recurrence/death hazard with advancing T category. Compared with pT1, pT2 disease was associated with substantially worse DFS (HR 9.51, 95% CI 1.19–75.77; p = 0.033), and pT3–pT4 conferred an even higher hazard (HR 27.61, 95% CI 2.91–262.44; p = 0.004). Margin positivity was strongly associated with inferior DFS (HR 5.91, 95% CI 1.81–19.26; p = 0.003). Lymphovascular invasion (HR 6.37, 95% CI 2.00–20.33; p = 0.002) and perineural invasion (HR 15.25, 95% CI 3.26–71.34; p = 0.001) were significant adverse prognostic factors. Tumor size (per 10-mm increase) was also strongly associated with worse DFS (HR 1.92, 95% CI 1.44–2.57; p < 0.001). In contrast, high histologic grade was not associated with DFS (HR 0.72, 95% CI 0.24–2.18; p = 0.559), and neither age (per 1-year increase: HR 1.05, 95% CI 0.99–1.12; p = 0.132) nor hypoalbuminemia (HR 2.68, 95% CI 0.81–8.86; p = 0.106) reached statistical significance.
4. Discussion
The identification of incidental gallbladder cancers (IGBC) within a large cholecystectomy population demonstrates that, despite its rarity, this entity continues to represent a clinically meaningful problem in daily surgical practice [18,19]. The reported incidence of IGBC after cholecystectomy varies geographically and has been shown to range between 0.25% and 3.3% [13]. In addition, approximately 27–41% of all gallbladder cancers are reported to be diagnosed incidentally, and residual disease rates as high as 40–76% have been documented in patients undergoing re-exploration [14]. These findings indicate that an incidental diagnosis does not invariably translate into adequate surgical treatment and that the need for additional surgical intervention is frequently encountered.
From a demographic perspective, advanced age and female sex have consistently been reported as the most common risk factors for IGBC [20]. Gallbladder cancer is known to occur more frequently in women, a phenomenon that has been attributed to the role of estrogen in increasing cholesterol saturation of bile and thereby promoting gallstone formation [21]. In our study, 43 IGBC cases were identified among approximately 19,798 cholecystectomy procedures, yielding an incidence of 0.22%; 74.4% of the patients were female, and the mean age was 71.4 years. These findings are consistent with the series reported by Chaturvedi et al., in which a predominance of female patients was observed [22]. In contrast, Matsuyama et al. reported a female proportion of 48.6%, suggesting that demographic distributions may vary according to geographic region and population characteristics [23]. Moreover, in a systematic review by Kellil et al., age was identified as a significant predictor of IGBC in seven studies, and Alvi et al. demonstrated a significant association between age over 55 years and postoperative cancer detection [24,25]. Similarly, in a multivariable logistic regression analysis by Ahn et al., age ≥65 years was the only factor independently associated with IGBC, underscoring the importance of advanced age as a key predictor (odds ratio: 2.542; 95% confidence interval) [26].
Recent studies have shown that gallstone disease is the most common indication for cholecystectomy in patients ultimately diagnosed with IGBC [27]. Nevertheless, the overall incidence of IGBC among all patients undergoing cholecystectomy remains low, reported at approximately 0.25% (67 of 26,572 patients) [27]. To date, no specific clinical findings or reliable radiological features have been clearly defined to predict early gallbladder cancer or benign premalignant lesions in patients with gallstones [28]. Gallstones, however, are widely recognized as the strongest risk factor for gallbladder cancer and are implicated in disease development in 75–90% of cases [9,11]. In line with these observations, the rate of cholelithiasis in our cohort was 88.4%, demonstrating close concordance with the existing literature.
Pathological evaluations indicate that advanced-stage disease and aggressive biological features cannot be entirely excluded despite an incidental diagnosis. Adenocarcinomas (not otherwise specified, NOS) represent the most common histologic subtype of malignant gallbladder neoplasms, accounting for approximately 90–95% of all cases; in line with this, the adenocarcinoma rate among IGBC cases in our cohort was 90.7% [21]. The literature indicates that the majority of IGBC cases not suspected preoperatively are diagnosed at pT1–pT2 stages, and similarly, pT2 was the most frequently identified stage in our study (41.9%) [14,19]. Nevertheless, the presence of pT3–4 disease in 25.6% of cases demonstrates that an incidental diagnosis does not preclude advanced-stage disease. In the series reported by Chaturvedi et al., 20.8% of patients had pT1 disease, 52% had pT2 disease, and 27.2% had pT3 disease, with pT2 being the most common presentation stage [22]. Likewise, Wu et al. reported advanced-stage disease (pT3–4) in 31.8% of patients. [3] The fact that advanced-stage (T3–T4) tumors are more readily detectable on preoperative imaging and during intraoperative assessment has been proposed as a possible explanation for the relatively higher proportion of early-stage tumors among IGBC cases diagnosed after laparoscopic cholecystectomy [3]. In addition, the rates of perineural invasion and lymphovascular invasion in our cohort were 44.2% and 39.5%, respectively, which are comparable to the rates of 53% and 45% reported by Ethun et al., underscoring that aggressive pathological features should not be overlooked in IGBC [30].
For gallbladder cancer (GBC), surgical resection remains the only potentially curative treatment, with radical cholecystectomy constituting the standard approach [14]. Radical cholecystectomy involves en bloc removal of the gallbladder, a wedge resection of at least 2 cm or more from the gallbladder bed (segments IV and V of the liver), and regional lymph node dissection [14]. Current guidelines recommend re-resection following laparoscopic cholecystectomy (LC) in patients with IGBC staged as T1b, T2, or T3. [31] In our study, re-resection was recommended for patients with appropriate stages, excluding those with T1a disease (n = 7) and those with metastatic disease at diagnosis (n = 8); however, 16 of the 28 eligible patients declined re-resection. Similarly, Wu et al. reported that radical re-resection was recommended for patients with T1b or higher-stage tumors without poor performance status or severe comorbidities, yet only a limited proportion of patients accepted this intervention [3]. In that study, advanced age was identified as the primary determinant for refusal of reoperation (69.2%), likely related to the high mean age of the cohort (66.4 ± 12.5 years) [3]. Owing to the limited number of patients undergoing re-resection, prognosis in this subgroup was considered to largely reflect the natural history of IGBC, and the survival impact of re-resection could not be adequately assessed [3]. Likewise, Ahn et al. reported that the majority of patients with pT2–pT3 disease were treated with cholecystectomy alone because of advanced age (median 75 years) and accompanying comorbidities [26]. Collectively, these findings suggest that advanced age and comorbidity burden are key clinical factors limiting the application of re-resection, despite guideline recommendations.
Pathological T stage is widely regarded as one of the most critical prognostic determinants in gallbladder cancer, as it directly reflects tumor burden and biological aggressiveness [32,33]. Wu et al. reported that advanced T stage was significant in univariable analyses evaluating potential risk factors associated with poor prognosis [3]. Similarly, Mazer et al. demonstrated that T stage was a significant predictor of mortality, with advanced T stage associated with an approximately 7.6-fold increased risk of death [34]. Consistent with these reports, pathological T stage in our study was significantly associated with both disease-free survival (DFS) and overall survival (OS), emerging as one of the strongest prognostic factors. The presence of advanced pathological stage (pT3–4) was associated with an approximately 27.61-fold increased risk for DFS compared with early-stage disease. In addition, perineural invasion was associated with an approximately 15.26-fold increase in DFS risk, lymphovascular invasion with a 6.37-fold increase, and positive surgical margins with a 5.91-fold increase. In the study by Altiok et al., perineural invasion and lymphovascular invasion were detected in 40% and 27.5% of patients, respectively, and both parameters were highlighted as having substantial prognostic importance [20]. Regarding margin status, Vega et al. demonstrated significantly worse OS in patients with positive cystic duct margins at the index cholecystectomy [35]. In contrast, in our cohort, margin positivity was associated with a significant reduction in DFS but did not translate into a statistically significant difference in OS, suggesting that while positive margins increase the risk of early recurrence, their impact on OS may be attenuated in cohorts dominated by advanced age and competing clinical factors. Reported survival outcomes in the literature show that Wu et al. observed a mean OS of 50.5 months for all IGBC patients, with 1-, 3-, and 5-year cumulative OS rates of 79.8%, 49.0%, and 40.8%, respectively [3]. By comparison, the mean OS in our study was 42.37 months, with 2-, 4-, and 6-year cumulative OS rates of 54%, 40%, and 11%, respectively.
When tumor size was analyzed as a continuous variable, each 10-mm increase was associated with an approximately 1.9-fold increase in DFS risk, supporting the prognostic relevance of tumor burden. In contrast, Ahn et al. reported that while advanced pT stage was a significant risk factor for recurrence and survival, tumor size itself was not significantly associated with clinical outcomes [26]. Despite these substantial effect sizes, the wide confidence intervals observed—particularly for advanced pathological stage and perineural invasion—warrant careful interpretation. In our study, the confidence interval for advanced-stage disease ranged from 2.91 to 262.44, indicating biologically consistent effect direction but limited precision attributable to the small number of events.
In OS analyses, the most notable and unexpected finding was the apparent association between the presence of comorbidity and improved OS (HR ≈ 0.19). However, the very high prevalence of comorbidity in our cohort (90.7%) resulted in a small comparator group without comorbidities, complicating interpretation. This observation may be influenced by methodological factors such as selection bias, differences in treatment allocation, and competing risks. Similarly, several clinical and pathological variables did not reach statistical significance in DFS or OS analyses, suggesting that their effects on survival may be modest and characterized by small effect sizes. Korkmaz et al. also emphasized that the rarity of incidental gallbladder carcinoma limits case numbers, reduces statistical power, and increases the risk of type II error [36]. Accordingly, unexpected or statistically non-significant findings in retrospective cohorts with limited patient and event numbers should be interpreted with appropriate caution.
5. Conclusion
This study demonstrates that, although incidental gallbladder cancer is rare within a large cholecystectomy population, it leads to clinically and oncologically meaningful outcomes. Our findings indicate that an incidental diagnosis does not exclude advanced-stage disease or aggressive pathological features, and that pathological T stage represents the strongest prognostic determinant for both disease-free survival and overall survival. Perineural invasion, lymphovascular invasion, and positive surgical margins were significantly associated with an increased risk of recurrence, whereas re-resection rates remained limited despite guideline recommendations, largely due to advanced age and accompanying comorbidities. In addition, differences observed in survival analyses and certain unexpected findings should be interpreted in the context of the retrospective study design, the limited number of events, and imbalances in patient distribution. Collectively, these results underscore the importance of meticulous pathological assessment, appropriate patient selection, and individualized surgical decision-making in incidental gallbladder cancer, and highlight that prognosis may remain heterogeneous even in cases detected at an early stage.
Author Contributions
Conceptualization, G.C. and A.B.; Methodology, G.C. and A.B.; Formal Analysis, G.C. and M.F.B.; Investigation, G.C., A.B. and M.F.B.; Data Curation, A.B. and M.F.B.; Writing – Original Draft Preparation, G.C.; Writing – Review and Editing, G.C., H.F.K.; Visualization, M.F.B.; Supervision, G.C.; Project Administration, H.F.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by The Local Ethical Committee of Kartal Dr. Lutfi Kirdar City Hospital (Approval number: 2025/010.99/21/33; Approval date: 30.10.2025). Ethical statement of human rights: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Informed Consent Statement
This study was approved by the local ethics committee. In addition, preoperative informed surgical consent was obtained from all patients included in the study. As the study was retrospective in design, no separate informed consent for study participation was required.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Jin, K.; Lan, H.; Zhu, T.; He, K.; Teng, L. Gallbladder carcinoma incidentally encountered during laparoscopic cholecystectomy: how to deal with it. Clinical and Translational Oncology 2011, 13, 25–33. [Google Scholar] [CrossRef]
- Goussous, N.; Maqsood, H.; Patel, K.; Ferdosi, H.; Muhammad, N.; Sill, A.M.; Kowdley, G.C.; Cunningham, S.C. Clues to predict incidental gallbladder cancer. Hepatobiliary & Pancreatic Diseases International 2018, 17, 149–154. [Google Scholar] [CrossRef]
- Wu, X.; Li, B.; Zheng, C.; Liu, W.; Hong, T.; He, X. Incidental gallbladder cancer after laparoscopic cholecystectomy: incidence, management, and prognosis. Asia-Pacific Journal of Clinical Oncology 2020, 16, 158–164. [Google Scholar] [CrossRef]
- Carriaga, M.T.; Henson, D.E. Liver, gallbladder, extrahepatic bile ducts, and pancreas. Cancer 1995, 75, 171–190. [Google Scholar] [CrossRef]
- Duffy, A.; Capanu, M.; Abou-Alfa, G.; Huitzil, D.; Jarnagin, W.; Fong, Y.; D'Angelica, M.; Dematteo, R.; Blumgart, L.; O'Reilly, E. Gallbladder cancer (GBC): 10-year experience at memorial Sloan-Kettering cancer centre (MSKCC). Journal of surgical oncology 2008, 98, 485–489. [Google Scholar] [CrossRef]
- Alarabiyat, M.; Raza, S.S.; Isaac, J.; Mirza, D.; Marudanayagam, R.; Roberts, K.; Abradelo, M.; Bartlett, D.C.; Dasari, B.V.; Sutcliffe, R.P. Incidental gallbladder cancer diagnosis confers survival advantage irrespective of tumour stage and characteristics. World journal of gastroenterology 2022, 28, 1996. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Yang, J.D.; Peeraphatdit, T.; Roberts, L.R. The incidence rates and survival of gallbladder cancer in the USA. European Journal of Cancer Prevention 2019, 28, 1–9. [Google Scholar] [CrossRef]
- Chen, C.; Geng, Z.; Shen, H.; Song, H.; Zhao, Y.; Zhang, G.; Li, W.; Ma, L.; Wang, L. Long-term outcomes and prognostic factors in advanced gallbladder cancer: focus on the advanced T stage. PloS one 2016, 11, e0166361. [Google Scholar] [CrossRef]
- Jha, V.; Sharma, P.; Mandal, K.A. Incidental gallbladder carcinoma: Utility of histopathological evaluation of routine cholecystectomy specimens. South Asian journal of cancer 2018, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, P.; Yogi, N.; Shrestha, B. Incidence of incidental carcinoma gall bladder in cases of routine cholecystectomy. Kathmandu University Medical Journal 2011, 9, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Shih, S.P.; Schulick, R.D.; Cameron, J.L.; Lillemoe, K.D.; Pitt, H.A.; Choti, M.A.; Campbell, K.A.; Yeo, C.J.; Talamini, M.A. Gallbladder cancer: the role of laparoscopy and radical resection. Annals of surgery 2007, 245, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Kumar N, P.; Gupta, Y.; Nag, H.H. Incidental gallbladder cancer: A comprehensive review. Journal of Gastrointestinal Cancer 2025, 56, 94. [Google Scholar] [CrossRef]
- Kanlioz, M.; Ekici, U.; Ayva, Y. Analysis of incidental gallbladder cancer in cholecystectomies. Cureus 2019, 11. [Google Scholar] [CrossRef]
- Rathanaswamy, S.; Misra, S.; Kumar, V.; Chintamani; Pogal, J.; Agarwal, A.; Gupta, S. Incidentally detected gallbladder cancer-the controversies and algorithmic approach to management. Indian Journal of Surgery 2012, 74, 248–254. [Google Scholar] [CrossRef]
- Panebianco, A.; Laforgia, R.; Volpi, A.; Mancarella, R.; Carbotta, G.; Punzo, C.; Lozito, C.; Tucci, R.; Minafra, M.; Delvecchio, A. Predictive factors for incidental gallbladder cancer (IGBC) in patients undergoing cholecystectomy for presumed benign disease. Annali Italiani di Chirurgia 2018, 89, 118–127. [Google Scholar]
- Isambert, M.; Leux, C.; Métairie, S.; Paineau, J. Incidentally-discovered gallbladder cancer: When, why and which reoperation? Journal of visceral surgery 2011, 148, e77–e84. [Google Scholar] [CrossRef] [PubMed]
- Pitt, S.C.; Jin, L.X.; Hall, B.L.; Strasberg, S.M.; Pitt, H.A. Incidental gallbladder cancer at cholecystectomy: when should the surgeon be suspicious? Annals of surgery 2014, 260, 128–133. [Google Scholar] [CrossRef]
- Lundberg, O.; Kristoffersson, A. Port site metastases from gallbladder cancer after laparoscopic cholecystectomy. Results of a Swedish survey and review of published reports. European Journal of Surgery 1999, 165, 215–222. [Google Scholar]
- Paolucci, V.; Schaeff, B.; Schneider, M.; Gutt, C. Tumor seeding following laparoscopy: international survey. World journal of surgery 1999, 23, 989–995. [Google Scholar] [CrossRef]
- Altiok, M.; Özdemir, H.G.; Kurt, F.; Gul, M.O.; Gumus, S. Incidental gallbladder cancer: a retrospective clinical study of 40 cases. Annals of Surgical Treatment and Research 2022, 102, 185–192. [Google Scholar] [CrossRef]
- Bhalla, S.; Shabbir, N.; Yadav, K.; Kumar, M.; Gupta, N.; Chaudhary, S.; Sharma, A.; Agarwal, P.; Shabbir, N., Sr. Evaluating the Incidence of Incidental Gallbladder Carcinoma in a Tertiary Care Centre: A Retrospective Analysis in North India. Cureus 2024, 16. [Google Scholar] [CrossRef]
- Chaturvedi, A.; Misra, S.; Chaudhary, S.; Gupta, S.; Prakash, P.; Kumar, V.; Akhtar, N.; Rajan, S. Treatment Outcomes of Incidental Gallbladder Cancer–Results from a High-Volume Tertiary Care Centre in North India. Indian Journal of Surgical Oncology 2024, 15, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, R.; Matsuo, K.; Mori, R.; Sugita, M.; Yamaguchi, N.; Kubota, T.; Kameda, K.; Mochizuki, Y.; Takagawa, R.; Kadokura, T. Incidental gallbladder cancer on cholecystectomy: strategy for re-resection of presumed benign diseases from a retrospective multicenter study by the Yokohama Clinical Oncology Group. in vivo 2021, 35, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Kellil, T.; Chaouch, M.A.; Aloui, E.; Tormane, M.A.; Taieb, S.K.; Noomen, F.; Zouari, K. Incidence and preoperative predictor factors of gallbladder cancer before laparoscopic cholecystectomy: a systematic review. Journal of Gastrointestinal Cancer 2021, 52, 68–72. [Google Scholar] [CrossRef]
- Alvi, A.R.; Siddiqui, N.A.; Zafar, H. Risk factors of gallbladder cancer in Karachi-a case-control study. World journal of surgical oncology 2011, 9, 164. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Park, C.-S.; Hwang, S.; Jang, H.-J.; Choi, K.-M.; Lee, S.-G. Incidental gallbladder cancer after routine cholecystectomy: when should we suspect it preoperatively and what are predictors of patient survival? Annals of surgical treatment and research 2016, 90, 131. [Google Scholar] [CrossRef]
- Koshenkov, V.P.; Koru-Sengul, T.; Franceschi, D.; DiPasco, P.J.; Rodgers, S.E. Predictors of incidental gallbladder cancer in patients undergoing cholecystectomy for benign gallbladder disease. Journal of surgical oncology 2013, 107, 118–123. [Google Scholar] [CrossRef]
- Cha, B.H.; Bae, J.-M. Comparison of clinical outcomes of incidental and non-incidental gallbladder cancers: a single-center cross-sectional study. Asian Pacific Journal of Cancer Prevention 2014, 15, 1281–1283. [Google Scholar] [CrossRef]
- Wakai, T.; Shirai, Y.; Hatakeyama, K. Radical second resection provides survival benefit for patients with T2 gallbladder carcinoma first discovered after laparoscopic cholecystectomy. World journal of surgery 2002, 26, 867. [Google Scholar] [CrossRef]
- Ethun, C.G.; Le, N.; Lopez-Aguiar, A.G.; Pawlik, T.M.; Poultsides, G.; Tran, T.; Idrees, K.; Isom, C.A.; Fields, R.C.; Krasnick, B.A. Pathologic and prognostic implications of incidental versus nonincidental gallbladder cancer: a 10-institution study from the United States extrahepatic biliary malignancy consortium. The American Surgeon 2017, 83, 679–686. [Google Scholar] [CrossRef]
- Aloia, T.A.; Járufe, N.; Javle, M.; Maithel, S.K.; Roa, J.C.; Adsay, V.; Coimbra, F.J.; Jarnagin, W.R. Gallbladder cancer: expert consensus statement. Hpb 2015, 17, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.S.; Zywot, A.; Mahendraraj, K.; Chamberlain, R.S. Gallbladder carcinoma in the United States: a population based clinical outcomes study involving 22,343 patients from the surveillance, epidemiology, and end result database (1973–2013). HPB Surgery 2017, 2017, 1532835. [Google Scholar] [CrossRef]
- Shukla, S.K.; Singh, G.; Shahi, K.; Bhuvan; Pant, P. Staging, treatment, and future approaches of gallbladder carcinoma. Journal of gastrointestinal cancer 2018, 49, 9–15. [Google Scholar] [CrossRef]
- Mazer, L.M.; Losada, H.F.; Chaudhry, R.M.; Velazquez-Ramirez, G.A.; Donohue, J.H.; Kooby, D.A.; Nagorney, D.M.; Adsay, N.V.; Sarmiento, J.M. Tumor characteristics and survival analysis of incidental versus suspected gallbladder carcinoma. Journal of Gastrointestinal Surgery 2012, 16, 1311–1317. [Google Scholar] [CrossRef]
- Vega, E.A.; Vinuela, E.; Sanhueza, M.; Mege, R.; Caracci, M.; Diaz, C.; Diaz, A.; Okuno, M.; Joechle, K.; Goumard, C. Positive cystic duct margin at index cholecystectomy in incidental gallbladder cancer is an important negative prognosticator. European Journal of Surgical Oncology 2019, 45, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, Y.Y.; Aydin, O.; Karatay, H.; Korkmaz, M.S.; Peker, S.; Gungor, F.; Kinaci, E. Preoperative Advanced Lung Cancer Inflammation Index as a Potential Marker for Incidental Gallbladder Carcinoma: A Matched Case–Control Study. Medicina 2026, 62, 269. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of patient selection and inclusion process for incidental gallbladder cancer (IGBC).
Figure 1.
Flowchart of patient selection and inclusion process for incidental gallbladder cancer (IGBC).
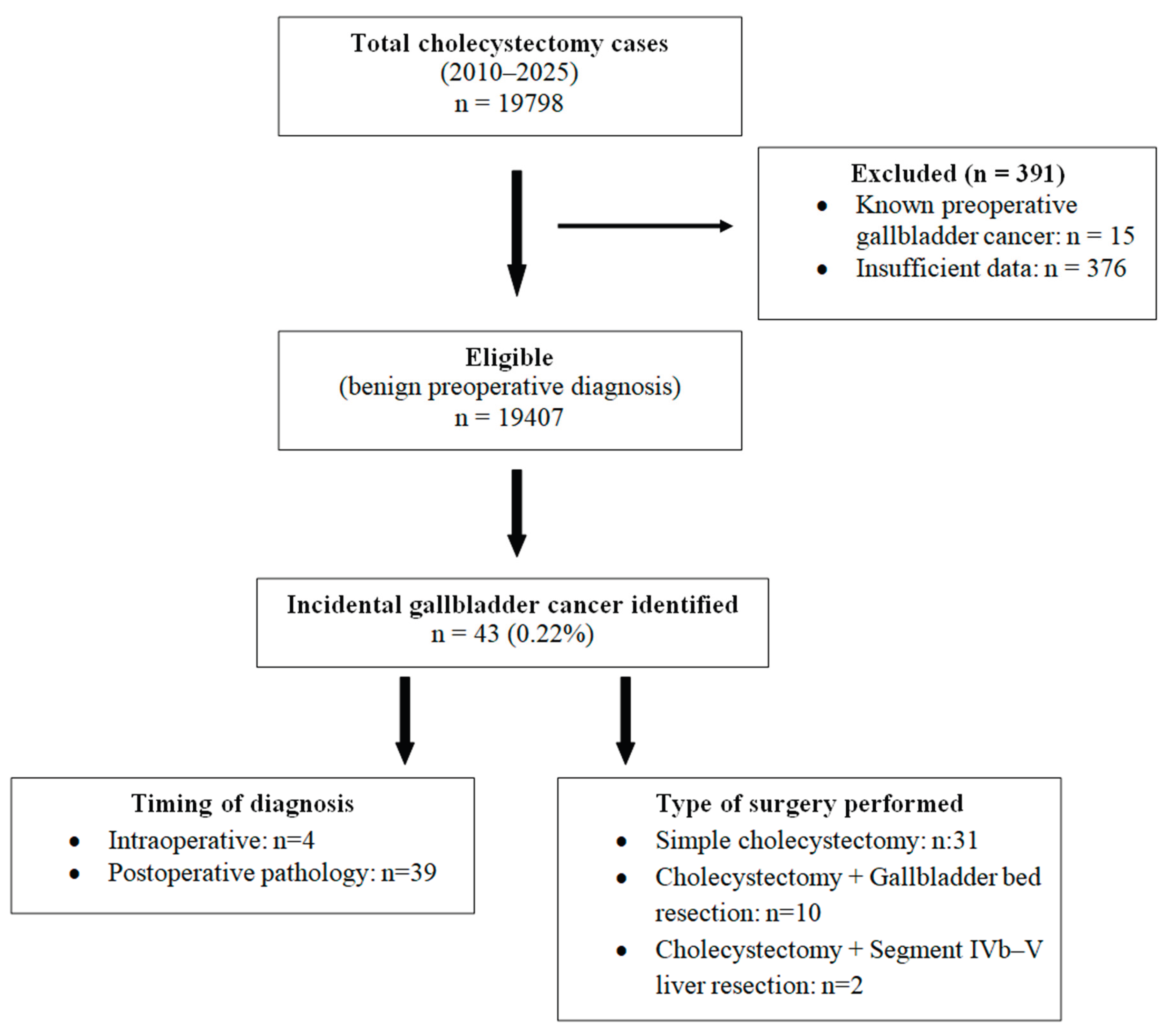

Table 1.
Baseline demographic, clinical, operative, and pathological characteristics of patients with incidental gallbladder cancer (IGBC) (n = 43).
Table 1.
Baseline demographic, clinical, operative, and pathological characteristics of patients with incidental gallbladder cancer (IGBC) (n = 43).
| Characteristic | Overall |
|---|---|
| Demographics and preoperative clinical status | |
| Age, years, mean ± SD | 71.4 ± 9.9 |
| Female sex, n (%) | 32 (74.4) |
| Body mass index category, n (%) | Low 7 (16.3); Normal 21 (48.8); High 15 (34.9) |
| ASA physical status, n (%) | I 1 (2.3); II 20 (46.5); III 15 (34.9); IV 7 (16.3) |
| Any comorbidity, n (%) | 39 (90.7) |
| Hepatitis history, n (%) | 1 (2.3) |
| Cholecystitis history, n (%) | 24 (55.8) |
| Choledocholithiasis history, n (%) | 14 (32.6) |
| Pancreatitis history, n (%) | 12 (27.9) |
| Smoking history, n (%) | 12 (27.9) |
| Alcohol use, n (%) | 5 (11.6) |
| ERCP history, n (%) | 9 (20.9) |
| Preoperative ultrasonography and gallstone profile | |
| Gallbladder wall thickness on US, n (%) | <3 mm 15 (34.9); 3–10 mm 24 (55.8); >10 mm 4 (9.3) |
| Primary US finding, n (%) | Stone 38 (88.4); Polyp 5 (11.6) |
| Largest stone size*, n/N (%) | <1 cm 12/38 (31.6); 1–3 cm 24/38 (63.2); >3 cm 2/38 (5.3) |
| Operative characteristics | |
| Surgical urgency, n (%) | Urgent 8 (18.6); Elective 35 (81.4) |
| Surgical approach, n (%) | Laparoscopic 31 (72.1); Open 7 (16.3); Conversion 5 (11.6) |
| Procedure type, n (%) | Cholecystectomy 31 (72.1); Cholecystectomy+gallbladder bed resection 10 (23.3); Cholecystectomy+segment IVb–V resection 2 (4.7) |
| Postoperative complications, n (%) | None 41 (95.3); Bile leak 1 (2.3); Superficial surgical site infection 1 (2.3) |
| Timing of diagnosis, n (%) | Intraoperative 4 (9.3); Postoperative 39 (90.7) |
| Pathology and tumor characteristics | |
| Histology, n (%) | Adenocarcinoma 39 (90.7); Other 4 (9.3) |
| Tumor location, n (%) | Fundus 3 (7.0); Body (corpus) 26 (60.5); Neck 2 (4.7); Diffuse 12 (27.9) |
| Perineural invasion, n (%) | 19 (44.2) |
| Lymphovascular invasion, n (%) | 17 (39.5) |
| Histologic grade, n (%) | Low 9 (20.9); Intermediate 20 (46.5); High 14 (32.6) |
| Pathologic T stage, n (%) | T1a 7 (16.3); T1b 7 (16.3); T2 18 (41.9); T3 8 (18.6); T4 3 (7.0) |
| Distant metastasis (M stage), n (%) | M0 36 (83.7); M1 7 (16.3) |
| Resection margin status, n (%) | Negative (R0) 29 (67.4); Cystic duct positive 5 (11.6); Liver bed positive 5 (11.6); Not assessable 4 (9.3) |
| Tumor size, mm, median [IQR] | 15 [33] |
*Largest stone size is reported among patients with gallstones on ultrasonography (N = 38). ASA, American Society of Anesthesiologists physical status; ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range; SD, standard deviation; US, ultrasonography.
Table 2.
Kaplan–Meier–estimated long-term survival outcomes in incidental gallbladder cancer (IGBC).
Table 2.
Kaplan–Meier–estimated long-term survival outcomes in incidental gallbladder cancer (IGBC).
| Endpoint | Analysis cohort | N (events / censored) | Median survival, months (95% CI) | Mean survival, months | 2-year (24 mo) | 4-year (48 mo) | 6-year (72 mo) |
|---|---|---|---|---|---|---|---|
| Overall survival (OS) | Full cohort | 43 | 26.00 [41.00] | 42.37 ± 34.12 | 54% | 40% | 11% |
| Disease-free survival (DFS) | M0 cohort (no distant metastasis) | 35 (14 / 21) | 25.50 [37.50] | 38.14 ± 34.31 | 60% | 53% | 38% |
CI, confidence interval; DFS, disease-free survival; KM, Kaplan–Meier; M0, no distant metastasis; OS, overall survival.
Table 3.
Univariable Cox proportional hazards regression for overall survival (OS) in incidental gallbladder cancer (IGBC).
Table 3.
Univariable Cox proportional hazards regression for overall survival (OS) in incidental gallbladder cancer (IGBC).
| Predictor (unit / contrast; reference) | HR | 95% CI | P value |
|---|---|---|---|
| Pathologic T stage (grouped; overall test) | — | — | 0.038 |
| ├─ T2 vs T1 (T1) | 0.38 | 0.13–1.09 | 0.071 |
| └─ T3–T4 vs T1 (T1) | 2.26 | 0.65–7.81 | 0.200 |
| Resection margin positivity (R1/R2 vs R0; R0) | 1.41 | 0.49–4.04 | 0.524 |
| Lymphovascular invasion (present vs absent; absent) | 1.56 | 0.54–4.49 | 0.411 |
| Perineural invasion (present vs absent; absent) | 1.14 | 0.40–3.29 | 0.807 |
| High histologic grade (high vs low; low/intermediate) | 0.46 | 0.17–1.23 | 0.124 |
| Tumor size (per 10-mm increase) | 0.91 | 0.65–1.25 | 0.551 |
| Age (per 1-year increase) | 0.99 | 0.94–1.04 | 0.664 |
| Any comorbidity (yes vs no; no) | 0.19 | 0.05–0.71 | 0.013 |
| CA 19-9 (log-transformed; per 1-unit increase) | 0.87 | 0.65–1.16 | 0.345 |
| ASA class (III–IV vs I–II; I–II) | 0.53 | 0.22–1.30 | 0.167 |
| Hypoalbuminemia (<3.5 vs ≥3.5 g/dL; ≥3.5) | 0.50 | 0.11–2.21 | 0.359 |
| Urgent surgery (urgent vs elective; elective) | 3.47 | 1.08–11.15 | 0.037 |
| Distant metastasis (M1 vs M0; M0) | 1.70 | 0.39–7.49 | 0.484 |
ASA, American Society of Anesthesiologists physical status; CA 19-9, carbohydrate antigen 19-9; CI, confidence interval; HR, hazard ratio; OS, overall survival.
Table 4.
Univariable Cox proportional hazards regression for disease-free survival (DFS) in incidental gallbladder cancer (IGBC), restricted to the M0 cohort.
Table 4.
Univariable Cox proportional hazards regression for disease-free survival (DFS) in incidental gallbladder cancer (IGBC), restricted to the M0 cohort.
| Predictor (unit / contrast; reference) | HR | 95% CI | P value |
|---|---|---|---|
| Pathologic T stage (grouped; overall test) | — | — | 0.013 |
| ├─ T2 vs T1 (T1) | 9.51 | 1.19–75.77 | 0.033 |
| └─ T3–T4 vs T1 (T1) | 27.61 | 2.90–262.44 | 0.004 |
| Resection margin positivity (R1/R2 vs R0; R0) | 5.91 | 1.81–19.26 | 0.003 |
| Lymphovascular invasion (present vs absent; absent) | 6.37 | 2.00–20.33 | 0.002 |
| Perineural invasion (present vs absent; absent) | 15.26 | 3.26–71.34 | 0.001 |
| High histologic grade (high vs low; low/intermediate) | 0.72 | 0.24–2.18 | 0.559 |
| Tumor size (per 10-mm increase) | 1.92 | 1.44–2.57 | <0.001 |
| Age (per 1-year increase) | 1.05 | 0.99–1.12 | 0.132 |
| Hypoalbuminemia (<3.5 vs ≥3.5 g/dL; ≥3.5) | 2.68 | 0.81–8.86 | 0.106 |
CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; M0, no distant metastasis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



