
Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Background: Bovine milk protein-based human milk fortifiers (HMFs) are routinely used in preterm infants in low- and middle-income countries (LMICs) but are associated with potential adverse effects. Plant-derived amino-acid based HMFs are a promising alternative, but comparative data from randomized controlled trials (RCTs) are lacking. This pilot RCT aimed to evaluate the feasibility, safety, and growth outcomes of a novel plant-derived amino-acid based HMF compared to a bovine-derived whole protein based HMF in preterm infants <34 weeks’ gestation. Methods: In this open-label, parallel pilot RCT, preterm infants <34 weeks’ gestation were randomized to a plant-derived amino-acid based HMF (n=66) or a bovine-derived whole protein based HMF (n=70). Primary outcomes were time to reach 180 mL/Kg/day enteral feeds and growth velocities to discharge and 40 weeks’ postmenstrual age (PMA). Feasibility and safety were also assessed. Analysis followed intention-to-treat approach. The trial was registered (CTRI/2025/06/089133). Results: Baseline characteristics were comparable between groups. Time to reach enteral feeds of 180 mL/Kg/day did not differ (adjusted Hazard Ratio 0.93, 95% CI 0.65–1.33; p=0.70). In-hospital weight gain was significantly higher in the plant-derived HMF group (adjusted mean difference 3.20 g/Kg/day, 95% CI 0.46–5.95; p=0.02). This benefit was most evident in exploratory subgroup analyses of infants with birth weight ≥1500g. Length, head circumference growth, and all safety outcomes were similar between groups. Conclusions: The plant-derived amino-acid based HMF was well-tolerated, with a comparable safety profile. Its use was associated with better in-hospital weight gain, indicating it is a potential alternative to bovine-derived whole protein based HMF. These data support the feasibility of definitive trials powered for critical clinical outcomes.
Keywords:
preterm infant
; enteral feed
; human milk fortifier
; amino acids
; plant-based
; bovine HMF
; neonatal nutrition
; randomized controlled trial
Introduction
Optimal nutrition during the neonatal period is crucial for improving both short- and long-term outcomes in preterm infants, including survival, growth, and neurodevelopment [1,2,3,4]. Preterm neonates have markedly higher protein, energy and other micronutrient requirements when compared to term neonates [5,6]. Meeting these nutritional needs is limited by the immaturity of the gastrointestinal tract resulting in inadequate digestion, absorption, and assimilation. Deficiencies in protein and energy intake in the neonatal period in preterm infants are associated with poor outcomes such as extra-uterine growth restriction (EUGR), neurodevelopmental impairment, and metabolic syndrome in later life [3,4,5,6,7].
Mother’s own milk (MoM) is the most appropriate form of milk for very preterm (VPT) and very low birth weight (VLBW) infants due to its protective effects against mortality, necrotizing enterocolitis (NEC), late onset neonatal sepsis (LONS), and other morbidities [2,7]. When MoM is insufficient, pasteurized donor human milk (PDHM) is suggested as a reasonable alternative to preterm formula milk [8]. Since both MoM and PDHM do not meet the high protein, energy, and other nutritional requirements of preterm neonates, they are routinely supplemented with multi-nutrient human milk fortifiers (HMFs) [9,10,11]. A Cochrane review indicated that HMF use is associated with short-term beneficial effects on anthropometric parameters of weight, length, and head-circumference, although evidence for reductions in major morbidities or improved long-term neurodevelopment is uncertain [1].
The protein constituent of routinely used HMFs in neonatal intensive care units (NICUs) is derived from bovine milk and is associated with several limitations [1,12]. Firstly, intact bovine proteins may be poorly digested by preterm neonates due to decreased intestinal proteolytic activity and has been shown to be associated with dysbiosis [13,14]. Secondly, exposure to bovine proteins in early neonatal life has been shown to be associated with intestinal inflammation and higher risk of cow milk protein allergy in childhood [15,16]. Finally, the addition of bovine-derived HMF may result in increased osmolar load on the immature gut perpetuating episodes of feed intolerance [17,18,19]. All of the abovementioned factors could increase the risk of adverse effects such as mortality and NEC with the use of bovine-derived HMF [20,21].
In lieu of the aforementioned limitations of bovine-derived HMF, alternative fortifiers have been evaluated [22]. While one study had evaluated two different types of extensively hydrolyzed bovine protein fortifiers [23], others had studied human milk-derived fortifiers [21,24]. Several recently published meta-analyses have concluded that human milk-based fortifiers may significantly reduce the risk of mortality and NEC when compared to bovine-derived HMFs [22,25,26,27]. However, the beneficial effects of human-milk based fortifiers over bovine-derived HMF on other adverse outcomes such as growth, bronchopulmonary dysplasia (BPD) and retinopathy of prematurity (ROP) are inconclusive [28]. Further, the use of human-milk based fortifiers is limited by higher costs in low- and middle-income countries (LMICs) [29]. Protein supplementation in the form of free amino acids might be a potentially safer and efficacious alternative to bovine-derived whole or hydrolysed protein HMFs [30]. Amino-acid based HMFs are devoid of any bovine proteins and are derived from plant sources through microbial fermentation [31]. Since amino acids do not require luminal proteolysis, their absorption may be more efficient in preterm neonates [14,32].
Recently, a plant-derived amino-acid based multi-nutrient HMF was made available for use in preterm neonates. Small single-centre observational studies have reported it to be efficacious and safe with respect to growth and feed tolerance in preterm neonates [33,34]. An in vitro study found it to be associated with a lower osmolality compared to several bovine-based HMFs [17]. Despite these data, the feasibility, safety and comparative effectiveness of plant-derived amino-acid HMF versus standard bovine-derived whole protein HMFs have not been rigorously evaluated in a randomized controlled trial (RCT). Therefore, we conducted this open label pilot RCT to compare a plant-derived amino-acid HMF with a bovine-derived whole protein HMF in preterm infants born at less than 34 weeks’ gestation. The primary aim was to assess feasibility, safety and short-term growth outcomes to generate preliminary data for a future definitive RCT.
Materials and Methods
This prospective open-label parallel pilot RCT was conducted in two tertiary care NICUs in India from 19th June 2025 to 1st February 2026. The trial was approved by the Institutional Ethics Committee and the protocol was registered in a trial registry (CTRI/2025/06/089133). Written informed consent was obtained from the parents or the caretakers of the neonates before enrolment. The reporting of this RCT adheres to the Consolidated Standards of Reporting Trials (CONSORT) statement for pilot RCTs [35].
Participants
Inclusion criteria: Preterm neonates born at less than 34 weeks’ gestation who were started on MoM or PDHM within 48 hours of life.
Exclusion criteria: Neonates with gross congenital malformations and whose caretakers refused consent.
Intervention (Plant-Derived Amino-Acid Based HMF)
The intervention group received plant-derived amino-acid based HMF (HMF-Advance, Analeptik Biologicals LLP, Bengaluru). Each 1 g sachet provides 4.5 kcal of energy, 0.35 g of protein, 0.24 g of carbohydrates, 0.18 g of fats, essential fatty acids and long-chain polyunsaturated fatty acids namely, linolenic acid (2 mg), alpha-linolenic acid (100 mcg), docosahexaenoic acid (200 mcg), and arachidonic acid (200 mcg). The other relevant constituents (per g) include calcium (20 mg), phosphorus (10 mg), vitamin D (50 IU), Vitamin A (100 IU), Zinc (40 mcg) and other micronutrients.
Comparator (Bovine-Derived Whey Protein Based HMF)
The control group received a bovine-derived whey protein based HMF (Lactodex-HMF, Raptakos, Brett & Co. Ltd., Thane). Each 1 g sachet provides 3.4 kcal of energy, 0.27 g of protein, 0.49 g of carbohydrates and 0.04 g of fats. The other relevant constituents include calcium (16 mg), phosphorus (8 mg), vitamin D (133 IU), Vitamin A (200 IU), Zinc (40 mcg), iron (0.30 mg) and other essential micronutrients.
Enteral Feeding and Other Care Practices
Neonates born at ≥ 30 weeks’ gestation were initiated on total enteral feeding at admission through an orogastric tube or cup depending upon their sickness profile. An enteral feed volume of 60 mL/Kg/d in those with a birth weight of less than 1500 g and 80 mL/Kg/d in others was provided on the first day of life. Neonates of < 30 weeks’ gestation or those with antenatal doppler changes of absent or reversal of end-diastolic blood flow (A/REDF) in the umbilical artery were initiated on trophic feeds (12 mL/Kg/d in neonates of <28 weeks’ gestation and 24 ml/Kg/d in neonates born at 280/7 – 296/7 weeks’ gestation) immediately after admission through an orogastric tube. The volume of the enteral feeds was increased daily by 24 mL/Kg/d in neonates of <28 weeks’ gestation and 36 mL/Kg/d in others till a maximum of 200 mL/Kg/d. MoM was the preferred first choice of milk and if inadequate, PDHM was used to meet the target daily intake. HMF was introduced when an enteral feed volume of 100 mL/Kg/d was reached. Standardized fortification approach (1g of HMF in 25 mL of milk) was used from the day of initiation of HMF. We targeted maximal enteral nutrition doses as per the updated European Society of Pediatric Gastroenterology, Hepatology and Nutrition guidelines in both the groups [36]. Fortification was continued until 40 weeks’ postmenstrual age (PMA). Pre-feed gastric aspiration was done only if the treating clinician or nurse had concerns on clinical examination. Single-strain probiotic supplementation (ProGG, Lactobacillus rhamnosus GG, 5 × 10⁹ CFU, Aristo Pharmaceuticals Pvt. Ltd., Mumbai) was provided from the time of initiation of enteral feeding at a dose of 2.5 × 10⁹ CFU/d till the neonate reached 60 ml/kg/d of enteral feeding and increased to 5 × 10⁹ CFU/d then on. Probiotics were continued until the neonate reached 34 weeks’ PMA. All other care practices were comparable between the two groups.
Those neonates who were born at less than 30 weeks’ gestation or those with antenatal doppler changes of A/REDF in the umbilical artery were initiated on TPN within 6 hours of birth either through an umbilical venous catheter or a peripherally inserted central catheter line based on The American Society for Parenteral and Enteral Nutrition guidelines [37].
Outcomes
Primary outcomes
- Time to reach enteral feed volume of 180 mL/Kg/d.
- Weight gain (g/kg/d), head circumference increment (cm/week) and length increment (cm/week) from enrolment until discharge from the hospital, and at 40 weeks’ PMA.
Secondary outcomes
- Weight gain (g/Kg/d) for different time intervals; birth until discharge, birth until 40 weeks’ PMA, from the day of regaining birth weight until 40 weeks’ PMA and from the day of discharge until 40 weeks PMA (post hoc)
- Days to regain birth weight (post hoc)
- Incidence of feed intolerance (defined as necessity to keep the neonate nil by feeds for at least one day)
- NEC stage ≥ 2 (modified Bells’ staging) [38]
- All-cause mortality
- Late Onset Neonatal Sepsis (LONS) (Blood culture proven sepsis or probable sepsis (clinical signs or symptoms indicative of sepsis with ≥ 2 altered biochemical sepsis parameters with the blood culture being negative))
- Requirement of red blood transfusion (post hoc)
- BPD (defined as oxygen requirement or any other form of respiratory support at 36 weeks’ PMA)
- ROP requiring intervention
- Metabolic bone disease
- Extra uterine growth restriction (EUGR) defined as weight for age of less than 10th centile at 40 weeks’ PMA
- Duration of hospital stay
Randomization Process, Allocation Concealment and Blinding
Neonates were randomized to the two groups in a 1:1 allocation ratio using stratified block randomisation. Randomisation sequence was generated using an online platform by an independent statistician not involved in the trial. Stratification was based on gestational age strata (<28 weeks, 280/7- 31 6/7 weeks and 320/7- 336/7 weeks). A block size of 4 was used within each gestational age category. Blinding of personnel or caretakers was not feasible. Allocation concealment was ensured by using sequentially labelled opaque sealed envelopes. The treating clinician opened the envelope only if the neonate satisfied the inclusion criteria and informed consent was obtained.
Sample Size
As this was a pilot RCT, a convenient sample size of 100 (50 in each group) was considered to be appropriate for evaluating the feasibility (recruitment rate and protocol adherence) and safety of the plant-derived amino-acid based HMF, and estimate the preliminary effect sizes with 95% confidence intervals (CIs) for growth outcomes [39]. To account for a higher than expected lost to follow-up rate after discharge, we enrolled a total of 136 neonates (66 in the intervention group and 70 in the comparator group).
Data Collection and Analysis
Data were entered into pre-specified spreadsheets. Statistical analyses were performed using the R Software Version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was defined as a two-sided p-value < 0.05. Baseline characteristics of the enrolled neonates were compared between the two groups using appropriate statistical tests. While continuous variables are presented as medians with interquartile ranges (IQR) compared using the Mann-Whitney U test, categorical variables were analyzed using the Chi-square test or Fisher’s Exact test. To minimize bias associated with missing data and to adhere to the Intention-to-treat (ITT) approach, missing values for primary and secondary outcomes were handled using Multiple Imputation by Chained Equations (MICE). Predictive Mean Matching (PMM) was used for continuous variables to ensure the imputed values remained within biologically plausible ranges. Fifty imputed datasets were generated. We used Rubin’s Rules to generate valid standard errors and confidence intervals. Growth velocities were analyzed using linear regression and are reported as mean differences (MD) with 95% CI. The primary outcome of time to reach an enteral feed volume of at least 180 mL/kg/day was compared using time-to-event analysis. Kaplan-Meier curves were generated to visualise the probability of reaching the target feed volume over time, and between-group differences were analyzed using the log-rank test. The Cox Proportional Hazards regression model was used to estimate the Hazard Ratio (HR) and 95% CI. To account for potential between-twins clustering, the Cox model utilized a cluster-robust variance estimator, with mother ID as the cluster variable. Multivariate adjusted analyses were performed for all the outcomes to account for the potential confounding factors of gestational age, birth weight, antenatal doppler abnormalities (AEDF or REDF in the umbilical artery) and receipt of antenatal corticosteroids. Exploratory subgroup analyses were performed to evaluate treatment effects in different gestational age and birth weight strata (gestational age, <32 weeks vs. ≥32 weeks and birth weight, <1500 g vs. ≥1500 g) using multivariable linear regression models. Amongst the subgroups in which model convergence was not achieved due to less number of neonates or data sparsity, adjustment was restricted to birth weight and gestational age alone. Per-protocol (PP) analyses for all the primary and secondary growth outcomes were performed to evaluate the robustness of the primary ITT analyses.
Results
A total of 199 preterm neonates were assessed for eligibility from 19th June 2025 to 1st January 2026. Among them, 136 neonates met the inclusion criteria and were randomized; 66 neonates to plant-derived amino-acid HMF group and 70 neonates to bovine-derived protein HMF group. Of the 136 neonates enrolled in the trial, all reached the primary outcome of time to reach enteral feed volume of 180 mL/Kg/d. Eleven neonates in the plant-derived HMF group and 12 neonates in the bovine-derived HMF group either discontinued the intervention, were lost to follow-up or died. While outcomes of all the neonates randomized to the two groups were analyzed in the primary ITT analyses, PP sensitivity analyses for the primary and secondary growth outcomes included 113 neonates (plant-derived HMF, n=55; bovine-derived HMF group, n=58) who fully adhered to the study protocol and completed the study follow-up until 40 weeks’ PMA. Figure 1 illustrates the participant flow of the trial. The baseline demographic and clinical variables were similar between the two groups, provided in Table 1.
Primary Outcomes
Time to Reach Enteral Feed Volume of 180 mL/Kg/d
Neonates in both the groups had a similar rate of progression of enteral feeding with no significant difference in the time to reach an enteral feed volume of 180 mL/Kg/d (log-rank test, p=0.70; HR (95% CI), 0.95 (0.69,1.33), p=0.78)). The Kaplan-Meier survival curves are provided in Figure 2. After accounting for the potential confounding factors of receipt of antenatal corticosteroids, umbilical artery doppler abnormalities, gestational age and birth weight, the adjusted multivariate Cox proportional hazards regression analysis also indicated no significant differences between the two groups (aHR (95% CI), 0.93 (0.65,1.33); p=0.70)).
Anthropometric Parameters from Enrolment Until Discharge and 40 Weeks’ PMA
The weight gain velocity, increments in length and head circumference from enrolment until discharge and 40 weeks’ PMA were similar between the two groups. (Table 2 and Figure 3). Multivariable linear regression adjusting for the aforementioned effect modifiers indicated that the weight gain velocitiy from enrolment until discharge was significantly higher in plant-derived amino-acid HMF group when compared to the bovine-derived HMF group (aMD (95% CI), 3.20 g/Kg/d (0.46, 5.95); p=0.02)). All other growth variables were similar between the two groups. (Table 2 and Figure 3).
Secondary Outcomes
Weight gain velocity was assessed across different epochs namely, birth until discharge and 40 weeks’ PMA, from the day of regaining birth weight until 40 weeks’ PMA and from hospital discharge until 40 weeks’ PMA. Since some neonates were discharged before regaining birth weight, we could not analyse the weight velocity from the day of regaining birth weight until hospital discharge. The aMD in the rate of weight gain for all the different epochs were similar between the two groups (Table 3 and Supplement Figure 1). The other secondary outcomes of days to regain birth weight, number of feed intolerance days, duration of hospital stay, and safety outcomes of mortality and other morbidities were also comparable between the two groups (Table 3 and Supplement Figure 2). The Kaplan-Meier survival curves for days to regain birth weight is provided in Supplement Figure 3.
Sub-Group Analyses (Post Hoc)
Sub-group analyses were performed based on gestational age (<32 weeks vs. ≥32 weeks) and birth weight (<1500 g vs. ≥ 1500 g) for the primary growth outcomes after adjusting for the confounding variables. For the outcome of rate of weight gain from enrolment until discharge, the primary ITT analysis had indicated beneficial effect of plant-derived amino-acid based HMF amongst all the enrolled neonates (aMD (95%CI), 3.20 g/Kg/d (0.48 to 5.92); p=0.02)). Subgroup analyses revealed that this effect was more pronounced in larger infants with birth weight ≥1500 g (aMD (95%CI), 4.47 g/Kg/d (0.09 to 8.84); p=0.04)). No significant subgroup differences were observed between the two groups for the outcomes length or head circumference increments. (Supplement Table 1 and Supplement Figure 4).
Sensitivity Analyses
PP analyses were performed for the primary outcome of weight gain, length increment and head circumference increment from enrolment until discharge. The unadjusted PP analyses showed similar results with no statistically significant differences between the two groups. Similar to the adjusted ITT analysis, the adjusted PP analysis also showed a statistically significant difference in the weight velocity from enrolment until discharge favouring the plant-derived amino-acid HMF group (aMD (95%CI), 3.96 g/Kg/d (1.44 to 6.47); p=0.002)). The robustness of the primary analyses was further established with similar results observed for the outcomes of length and head circumference increments from enrolment until discharge and at 40 weeks’ PMA, and secondary weight outcomes across different time periods (Supplement Table 2 and Supplement Figure 5). PP subgroup analyses showed favourable effects of plant-derived amino-acid HMF for the outcome of rate of weight gain from enrolment until discharge in neonates with birth weight ≥ 1500 g (aMD (95%CI), 5.40 g/Kg/d (1.54 to 9.26); p=0.006)) as seen in the ITT analyses. Additionally, a similar effect favouring plant-derived amino-acid HMF was also seen in neonates born at ≥ 32 weeks’ gestation (aMD (95%CI), 7.47 g/Kg/d (1.63 to 13.31); p=0.01)) (Supplement Table 3 and Supplement Figure 6).
The absolute weight, length, and head circumference from birth through 40 weeks PMA were similar between the two groups for ITT and PP analyses (Supplement Figure 7).
Discussion
In this pilot RCT, we evaluated safety and efficacy of a novel plant-derived amino-acid based HMF compared to the standardly used bovine-derived whole protein HMF in preterm neonates born at less than 34 weeks’ gestation. The results of this trial indicate that plant-derived amino-acid based HMF is well tolerated with similar safety profile when compared to bovine-derived HMF with a possible beneficial effect on in-hospital weight gain.
The efficacy of the plant-derived amino-acid HMF seen in our exploratory trial could be attributed to a multitude of biologically plausible reasons. The primary mechanism likely involves the digestive physiology of the preterm gut. Demers-Mathieu et al. reported that preterm neonates have significantly lower intestinal proteolytic activity compared to term infants [14]. By providing nitrogen in its elemental amino acid form, our intervention likely bypassed the rate-limiting hydrolysis required for bovine protein, thereby enhancing nitrogen retention more effectively. Also, avoidance of exposure to bovine antigens in the plant-derived HMF group might have maintained a balanced oxidant vs. anti-oxidant profile, and promoted a favourable microbiome milieu in the intestinal tract [40,41].
As shown in previous studies, the amino-acid based HMF’s nutritional profile which is higher in protein and essential fatty acids but lower in carbohydrates may also have contributed to better in-hospital weight gain [42,43]. Furthermore, an in vitro study evaluating various HMFs, including those used in our trial, revealed through direct comparison that the amino-acid based fortifier yields a lower reconstituted osmolality compared to the bovine-based protein HMF [17]. This is probably significant as a higher osmolar load has been shown to be associated with altered intestinal mucosal integrity in pre-clinical studies which could adversely affect the nutrient absorption [19,44,45]. We acknowledge that the higher protein content in the plant-derived amino-acid based HMF in conjunction with the use of standardized fortification approach would have possibly contributed to the observed better in-hospital weight gain.
The observed in-hospital weight gain benefit with plant-derived amino-acid based HMF was primarily evident in more mature preterm infants, possibly due to their enhanced metabolic capacity to utilize higher protein intake [46]. These findings should be interpreted as hypothesis-generating as this was a post hoc exploratory sub-group analysis. This subgroup is critically relevant in the context of neonatal care in LMICs, as it represents a large proportion of preterm admissions in LMICs who are often excluded in HMF trials [47]. However, this growth advantage did not extend until 40 weeks’ PMA. While the period from discharge until 40 weeks PMA was uncontrolled, this transient effect is consistent with that reported in literature, where post-discharge cessation of fortification due to non-compliance or other reasons such as transitioning to exclusive breast feeding typically leads to convergence in growth trajectories [11,48].
While an exclusive human milk diet fortified with a human milk-derived fortifier is another promising alternative to bovine-derived HMF, its feasibility, cost, and ethical implications in LMICs remain topics of debate [49]. Moreover, a recent Bayesian meta-analysis has contested the superiority of human milk-derived fortifier over bovine-derived HMF [28]. In this context, the plant-derived amino-acid HMF may be seen as a more scalable and practical alternative to human milk-derived fortifiers in LMICs.
This RCT has several limitations. This was a pilot RCT involving two centres, and hence is underpowered for critical outcomes. Though the trial met the required sample size, high lost to follow-up rate after discharge might have resulted in bias due to missing data. We could not blind the interventions as our follow-up period extended beyond discharge from the hospital, which could have implications related to performance bias. Our results are not generalizable to extremely low gestational age neonates as they constituted only a minor proportion of those enrolled in our trial. Finally, we could not compare the nutrient intake accurately in some neonates after discharge from the hospital as these neonates were transitioned to direct breast feeding with or without variable amounts of formula feeds. There were several strengths as well. To the best of our knowledge, this is the only RCT that had evaluated a plant-derived amino-acid based HMF vs. bovine-derived protein based HMF. Further, the statistical analyses was comprehensive and robust, accounting for lost to follow-up using recommended approaches with adherence to the CONSORT for pilot RCTs guidance. Finally, this trial addressed a critical knowledge gap of use of HMF in relatively mature preterm neonates ≥32 weeks’ gestation from LMICs who were followed up beyond hospital discharge.
Conclusions
In conclusion, this pilot RCT demonstrates the safety, feasibility and efficacy of a novel plant-derived amino-acid based HMF when compared to bovine-derived protein based HMF. The beneficial effects of weight gain until discharge was predominantly seen in the sub-group of neonates born at ≥1500 grams and ≥32 weeks’ gestation. These results provide preliminary data for future multi-centre RCTs that are adequately powered for critical outcomes such as mortality and NEC.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki (2013) and complied with the Indian Council of Medical Research (ICMR) Ethical Guidelines for Biomedical Research on Human Subjects (2017). The study protocol was approved by the Institutional Ethics Committee (IEC) (ANKURA Ethics committee, Ref. No: ANKURA/EC/BMHR/2025/6-02, approved on 10.03.2025). The IEC is registered with the Department of Health Research (DHR), Ministry of Health & Family Welfare, Government of India. All participants provided written informed consent before enrolment.
Consent to Participate in the Study and Publish
Written informed consent was obtained from the legal guardians of the neonates enrolled in the study, and for publication of the study.
Competing Interests
The authors declare no conflict of interest related to this study.
Author Contributions
Conceptualization: NKM, VVR, NBS, LB, AAHA; Methodology: VVR, NBS, VS; Formal analysis and investigation: NKM, VVR, VS; Writing—NKM; Writing—review and editing: VVR, NBS, NKM, AAHA, VS; Funding acquisition: Not applicable; Resources: VVR, NBS, LB, VS; Supervision: VVR.
Funding
No funding was obtained for this study.
Data Availability Statement
Data related to this trial could be provided on request to the corresponding author.
References
- Brown, J.V.; Embleton, N.D.; Harding, J.E.; McGuire, W. Multi-Nutrient Fortification of Human Milk for Preterm Infants. Cochrane Database Syst. Rev. 2016, CD000343.
- Parker, M.G.; Stellwagen, L.M.; Noble, L. Promoting Human Milk and Breastfeeding for the Very Low Birth Weight Infant. Pediatrics 2021, 148, e2021054272.
- Ziegler, E.E. Protein Requirements of Very Low Birth Weight Infants. J. Pediatr. Gastroenterol. Nutr. 2007,45, S170–S174.
- Horbar, J.D.; Ehrenkranz, R.A.; Badger, G.J.; Edwards, E.M.; Morrow, K.A.; Soll, R.F.; Buzas, J.S.; Bertino, E.; Gagliardi, L.; Zampino, G.; et al. Weight Growth Velocity and Postnatal Growth Failure in Infants 501 to 1500 Grams: 2000–2013. Pediatrics 2015, 136, e84–e92.
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral Nutrient Supply for Preterm Infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91.
- Embleton, N.D.; Morgan, C.; King, C. Balancing the Risks and Benefits of Parenteral Nutrition for Preterm Infants: Can We Define the Optimal Composition? Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F351–F354.
- Lucas, A.; Cole, T.J. Breast Milk and Neonatal Necrotising Enterocolitis. Lancet 1990,336, 1519–1523.
- Arslanoglu, S.; Corpeleijn, W.; Moro, G.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; Hojsak, I.; et al. Donor Human Milk for Preterm Infants: Current Evidence and Research Directions. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 535–542.
- Shah, S.D.; Dereddy, N.; Jones, T.L.; Dhanireddy, R.; Talati, A.J. Early versus Delayed Human Milk Fortification in Very Low Birth Weight Infants—A Randomized Controlled Trial. J. Pediatr. 2016, 174, 126–131.e1.
- Rochow, N.; Fusch, G.; Choi, A.; Chessell, L.; Elliott, L.; McDonald, K.; Kuiper, E.; Purcha, M.; Turner, S.; Chan, E.; et al. Target Fortification of Breast Milk with Fat, Protein, and Carbohydrates for Preterm Infants. J. Pediatr. 2013, 163, 1001–1007.
- Arslanoglu, S.; Boquien, C.-Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76.
- Gu, X.; Shi, X.; Zhang, L.; Zhou, Y.; Cai, Y.; Jiang, W.; Zhou, Q. Evidence Summary of Human Milk Fortifier in Preterm Infants. Transl. Pediatr. 2021,10, 3058–3067.
- Li, Y.; Pan, X.; Yuan, S. Human Milk-Based or Bovine Milk-Based Fortifiers for Human Milk-Fed Preterm Infants: A Narrative Review. Front. Pediatr. 2021, 9, 719096.
- Demers-Mathieu, V.; Qu, Y.; Underwood, M.A.; Borghese, R.; Dallas, D.C. Premature Infants Have Lower Gastric Digestion Capacity for Human Milk Proteins than Term Infants. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 816–821.
- Sağır, H.; Çağan Appak, Y.; Aksoy, B.; Kahveci, S.; Onbaşı Karabağ, Ş.; Gülpınar Aydın, Ö.; Alaca, S.; Baran, M. Impact of Using Cow’s Milk Formula During the First Three Postnatal Days and Other Etiological Factors on the Development of Cow’s Milk Protein Allergy. J. Clin. Med. 2025, 14, 8664.
- Abdelhamid, A.E.; Chuang, S.-L.; Hayes, P.; Fell, J.M. Evolution of in Vitro Cow’s Milk Protein-Specific Inflammatory and Regulatory Cytokine Responses in Preterm Infants with Necrotising Enterocolitis. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 5–11.
- Basany, L.; Ali, A.; Gandrakota, N.P.G.; Kulkarni, A.B.; Tabassum, M.; Manjunath, H.; Batthula, V. Balancing Nutrition and Osmolality: Risk of Hyperosmolality During Individualized Fortification With Protein Fortifiers in an In Vitro Study. Cureus 2025, 17, e86602.
- Tang, Q.; Yin, D.; Jin, Z.; Zhang, L.; Zhou, P. Osmolality of Donor Human Milk Rises Dramatically within Minutes of Fortification with Varied Degrees Depending on the Fortifier Used. Front. Pediatr. 2025, 13, 1596255.
- Pearson, F.; Johnson, M.J.; Leaf, A.A. Milk Osmolality: Does It Matter? Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F166–F169.
- Abrams, S.A.; Schanler, R.J.; Lee, M.L.; Rechtman, D.J. Greater Mortality and Morbidity in Extremely Preterm Infants Fed a Diet Containing Cow Milk Protein Products. Breastfeed. Med. 2014, 9, 281–285.
- Sullivan, S.; Schanler, R.J.; Kim, J.H.; Patel, A.L.; Trawöger, R.; Kiechl-Kohlendorfer, U.; Chan, G.M.; Blanco, C.L.; Abrams, S.; Cotten, C.M.; et al. An Exclusively Human Milk-Based Diet Is Associated with a Lower Rate of Necrotizing Enterocolitis than a Diet of Human Milk and Bovine Milk-Based Products. J. Pediatr. 2010, 156, 562–567.e1.
- Feng, Y.; Gao, Y.; Gu, Y.; Liu, Y.; Xu, Y.; Li, S. Impact of Three Mammalian Milk-Derived Fortifiers on Morbidity and Mortality in Preterm Infants: A Systematic Review and Network Meta-Analysis. Int. Breastfeed. J. 2025, 21, 9.
- Kim, J.H.; Chan, G.; Schanler, R.; Groh-Wargo, S.; Bloom, B.; Dimmit, R.; Williams, L.; Baggs, G.; Barrett-Reis, B. Growth and Tolerance of Preterm Infants Fed a New Extensively Hydrolyzed Liquid Human Milk Fortifier. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 665–671.
- O’Connor, D.L.; Kiss, A.; Tomlinson, C.; Bando, N.; Bayliss, A.; Campbell, D.M.; Daneman, A.; Francis, J.; Kotsopoulos, K.; Shah, P.S.; et al. Nutrient Enrichment of Human Milk with Human and Bovine Milk-Based Fortifiers for Infants Born Weighing 1250 <g: A Randomized Clinical Trial. Am. J. Clin. Nutr. 2018, 108, 108–116.
- Galis, R.; Trif, P.; Mudura, D.; Pop, L.; Fufezan, O.; Orășan, R. Association of Fortification with Human Milk versus Bovine Milk-Based Fortifiers on Short-Term Outcomes in Preterm Infants—A Meta-Analysis. Nutrients 2024, 16, 910.
- Ananthan, A.; Balasubramanian, H.; Rao, S.; Patole, S. Human Milk-Derived Fortifiers Compared with Bovine Milk-Derived Fortifiers in Preterm Infants: A Systematic Review and Meta-Analysis. Adv. Nutr. 2020, 11, 1325–1333.
- Grace, E.; Hilditch, C.; Gomersall, J.; Collins, C.T.; Rumbold, A.; Keir, A.K. Safety and Efficacy of Human Milk-Based Fortifier in Enterally Fed Preterm and/or Low Birthweight Infants: A Systematic Review and Meta-Analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 137–142.
- Huizing, M.J.; Vizzari, G.; Bartoš, F.; Cavallaro, G.; Gianni, M.L.; Villamor, E. Absence of Evidence of Beneficial Effects of Human Milk-Based Fortifier: A Bayesian Model-Averaged Meta-Analysis. Acta Paediatr. 2025, 114, 3309–3316.
- Kumar, M.; Upadhyay, J.; Basu, S. Fortification of Human Milk with Infant Formula for Very Low Birth Weight Preterm Infants: A Systematic Review. Indian Pediatr. 2021, 58, 253–258.
- Vanderhoof, J.; Moore, N.; de Boissieu, D. Evaluation of an Amino Acid-Based Formula in Infants Not Responding to Extensively Hydrolyzed Protein Formula. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 531–533.
- Ikeda, M. Amino Acid Production Processes. In Microbial Production of L-Amino Acids; Springer: Berlin/Heidelberg, Germany, 2003; pp. 1–35.
- Bertino, E.; Giribaldi, M.; Cester, E.A.; Coscia, A.; Trapani, B.M.; Peila, C.; Arslanoglu, S.; Moro, G.E.; Cavallarin, L. New Human Milk Fortifiers for the Preterm Infant. J. Pediatr. Neonatal Individ. Med. 2017, 6, e060124.
- Chandra, R.; Singh, P.; Verma, A.; Patel, S.; Sharma, R.; Gupta, N.; Mehta, K.; Joshi, A.; Reddy, S.; Kumar, V.; et al. A Study of Safety and Effectiveness of Amino-Acids Based Multi-Nutrient Fortifier in Premature Infants Admitted in NICU. Int. J. Contemp. Pediatr. 2024, 11, 362–367.
- Karotkar, U.; Sharma, M.; Desai, R.; Mehta, D.; Patel, K.; Nair, S.; Iyer, S.; Choudhary, B.; Agarwal, P.; Kapoor, S.; et al. Effects of Amino-Acids Based Fortifier in Preterm Infants. Int. J. Contemp. Health. 2025, 3, 1–8.
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A.; PAFS Consensus Group. CONSORT 2010 Statement: Extension to Randomised Pilot and Feasibility Trials. Pilot Feasibility Stud. 2016, 2, 64.
- Embleton, N.D.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.P.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Iacobelli, S.; et al. Enteral Nutrition in Preterm Infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and Invited Experts. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 248–268.
- Robinson, D.T.; Calkins, K.L.; Chen, Y.; Cober, M.P.; Falciglia, G.H.; Church, D.D.; Mey, J.; McKeever, L.; Sentongo, T. Guidelines for Parenteral Nutrition in Preterm Infants: The American Society for Parenteral and Enteral Nutrition. J. Parenter. Enter. Nutr. 2023, 47, 830–858.
- Walsh, M.C.; Kliegman, R.M. Necrotizing Enterocolitis: Treatment Based on Staging Criteria. Pediatr. Clin. N. Am. 1986, 33, 179–201.
- Teare, M.D.; Hayman, A.; Dimairo, M.; Shephard, N.; Whitehead, A.; Walters, S.J. Sample Size Requirements for Pilot Randomised Controlled Trials with Continuous Outcomes: A Simulation Study. Trials 2013, 14, P46.
- Aguilar-Lopez, M.; Wetzel, C.; MacDonald, A.; Ho, T.T.B.; Donovan, S.M. Human Milk-Based or Bovine Milk-Based Fortifiers Differentially Impact the Development of the Gut Microbiota of Preterm Infants. Front. Pediatr. 2021, 9, 719096.
- Aydemir, O.; Aydemir, Y.; Surmeli Onay, O. How Does Bovine Milk-Based Fortification Alter the Oxidant-Antioxidant Profile of Breast Milk in Preterm Infants? J. Pediatr. Gastroenterol. Nutr. 2025, 80, 861–869.
- Picaud, J.C.; Reynolds, P.R.; Clarke, P.; van den Hooven, E.; van Weissenbruch, M.M.; van Lingen, R.A.; Goedhart, A.; Botma, A.; Boettger, R.; van Westering-Kroon, E.; et al. A Novel Human Milk Fortifier Supports Adequate Growth in Very Low Birth Weight Infants: A Non-Inferiority Randomised Controlled Trial. Arch. Dis. Child. Fetal Neonatal Ed. 2025, 110, 512–519.
- Bhatt, A.N.; Bingham, R.; Gaillard, P.; Stansfield, B.K. Association between Nonacidified Standard and High-Protein Human Milk Fortifiers and Increased Weight Velocity Relative to Acidified Human Milk Fortifiers in Preterm Infants: A Retrospective Cohort Study. J. Parenter. Enter. Nutr. 2026, 50, 48–55.
- Kreissl, A.; Zwiauer, V.; Repa, A.; Binder, C.; Haninger, N.; Jilma, B.; Berger, A.; Haiden, N. Effect of Fortifiers and Additional Protein on the Osmolarity of Human Milk: Is It Still Safe for the Premature Infant? J. Pediatr. Gastroenterol. Nutr. 2013, 57, 432–437.
- Kreins, N.; Buffin, R.; Michel-Molnar, D.; Chambon, V.; Pradat, P.; Picaud, J.C. Individualized Fortification Influences the Osmolality of Human Milk. Front. Pediatr. 2018, 6, 322.
- Ehrenkranz, R.A.; Das, A.; Wrage, L.A.; Poindexter, B.B.; Higgins, R.D.; Stoll, B.J.; Oh, W.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Early Nutrition Mediates the Influence of Severity of Illness on Extremely LBW Infants. Pediatr. Res. 2011, 69, 522–529.
- North, K.; Marx Delaney, M.; Bose, C.; Lee, A.C.C.; Vesel, L.; Adair, L.; Semrau, K. The Effect of Milk Type and Fortification on the Growth of Low-Birthweight Infants: An Umbrella Review of Systematic Reviews and Meta-Analyses. Matern. Child Nutr. 2021, 17, e13176.
- Young, L.; Embleton, N.D.; McCormick, F.M.; McGuire, W. Multinutrient Fortification of Human Breast Milk for Preterm Infants Following Hospital Discharge. Cochrane Database Syst. Rev. 2013, 2, CD004866.
- Wiechers, C.; Bernhard, W.; Goelz, R.; Poets, C.F.; Franz, A.R. Optimizing Early Neonatal Nutrition and Dietary Pattern in Premature Infants. Int. J. Environ. Res. Public Health 2021, 18, 7544.
Figure 1.
CONSORT Flow Diagram.
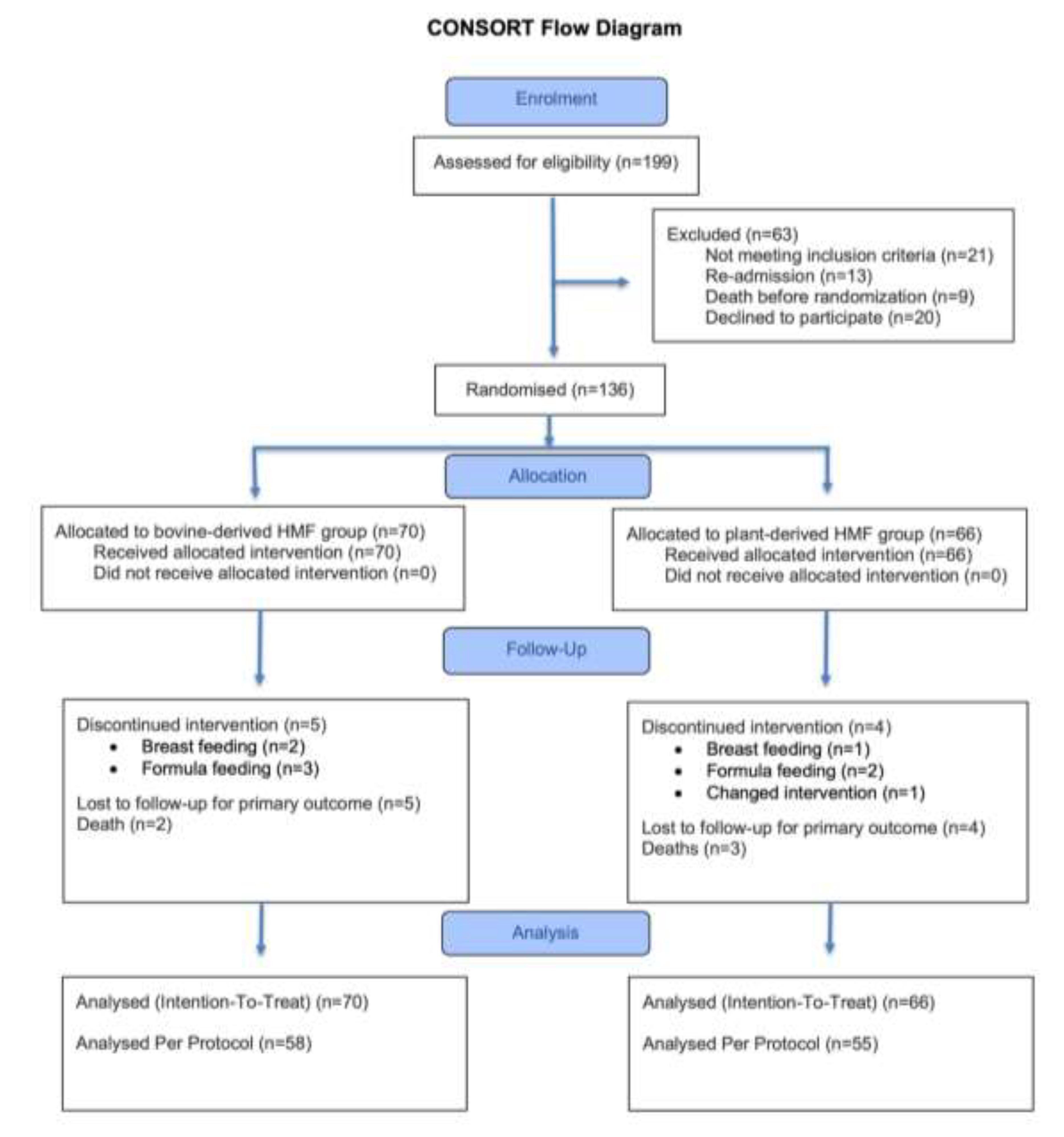
Figure 2.
Intention-to-Treat Analysis for Time to Reach enteral feed volume of 180 mL/Kg/d (Kaplan-Meier Survival Estimates) Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
Figure 2.
Intention-to-Treat Analysis for Time to Reach enteral feed volume of 180 mL/Kg/d (Kaplan-Meier Survival Estimates) Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
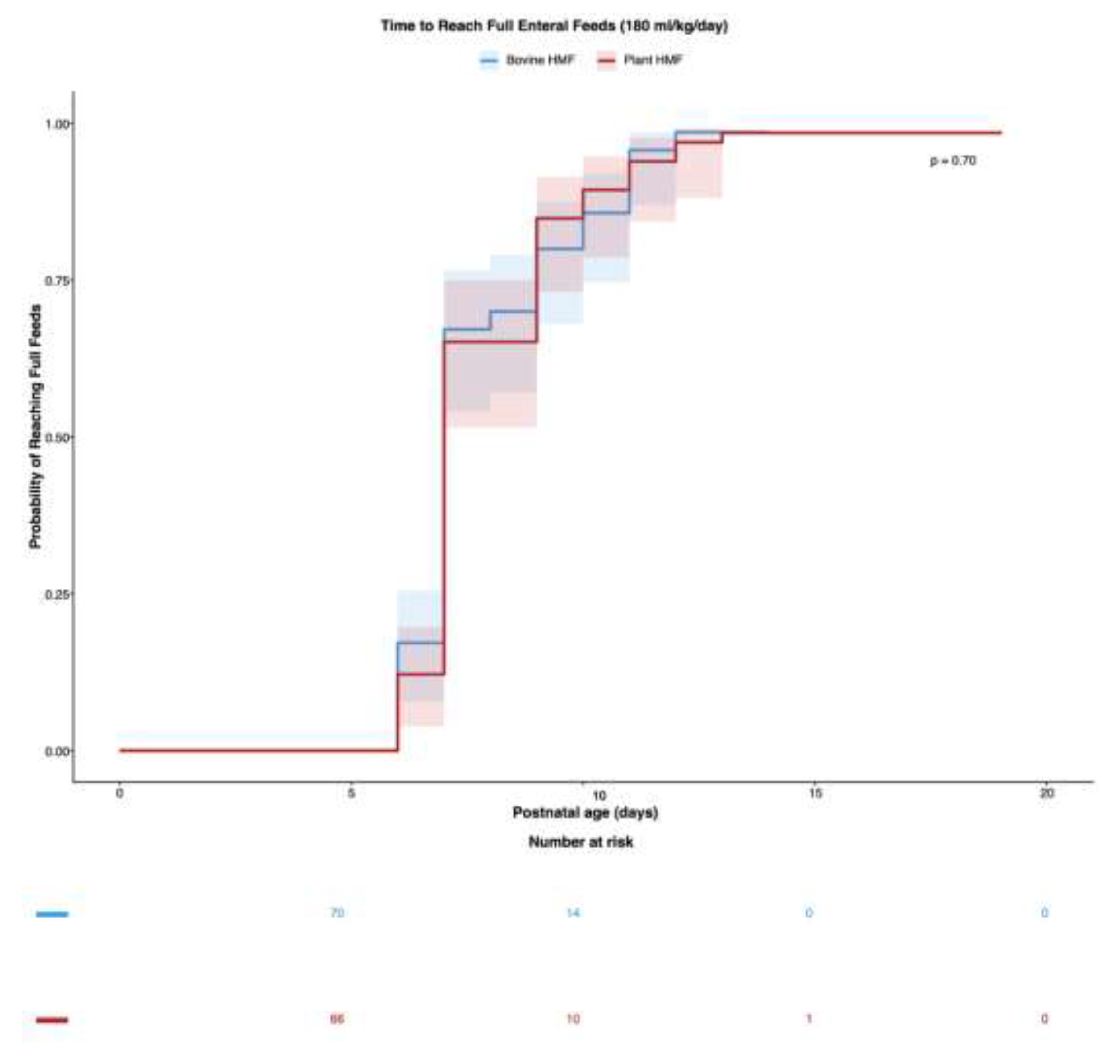
Figure 3.
Unadjusted and Adjusted Intention-to-Treat Analyses of Growth Velocities. (Weight, Length, and Head Circumference) Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
Figure 3.
Unadjusted and Adjusted Intention-to-Treat Analyses of Growth Velocities. (Weight, Length, and Head Circumference) Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
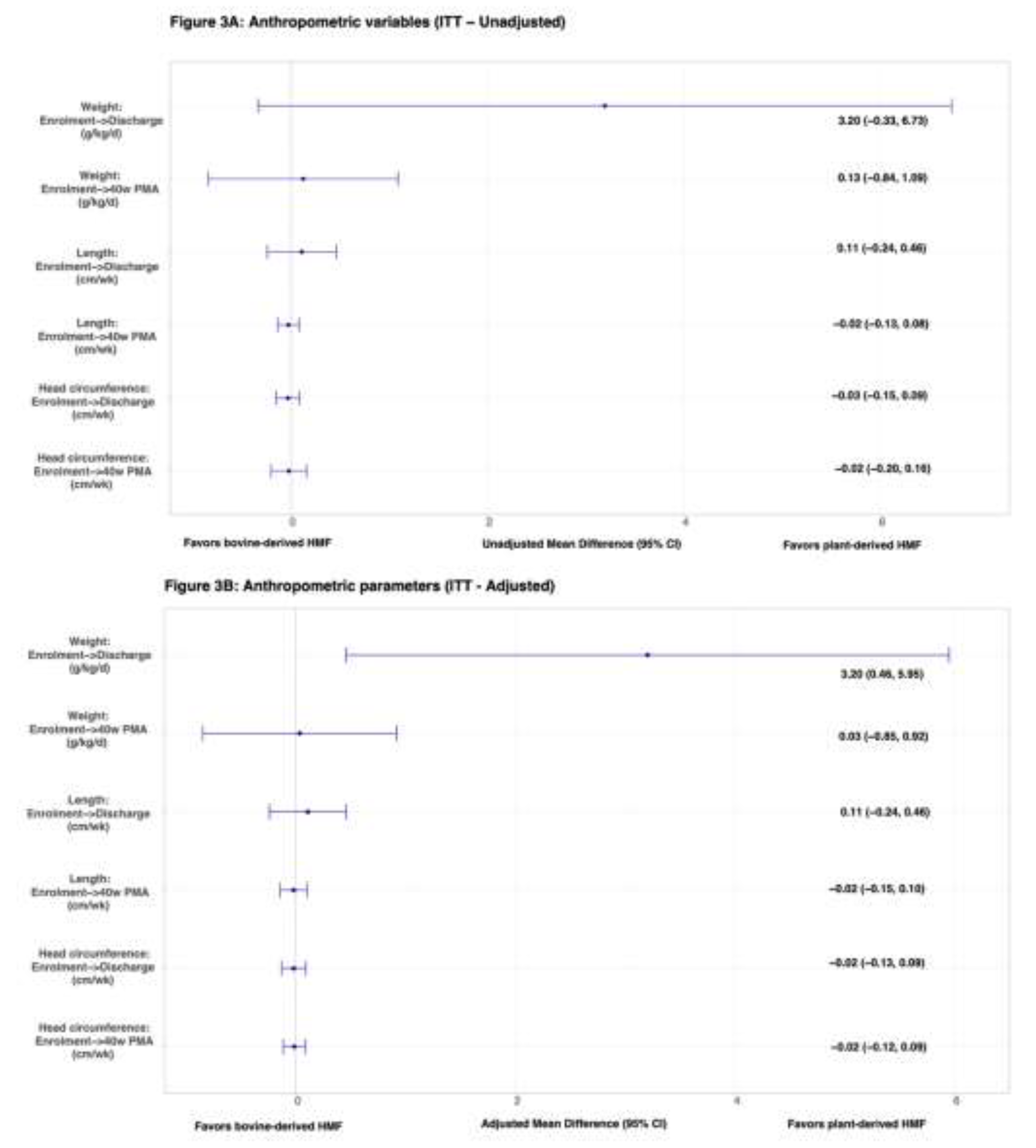

Table 1.
Baseline Demographic and Clinical Variables Between Bovine-Derived Protein Based HMF and Plant-Derived Amino-Acid Based HMF Groups.
Table 1.
Baseline Demographic and Clinical Variables Between Bovine-Derived Protein Based HMF and Plant-Derived Amino-Acid Based HMF Groups.
| Variable | Bovine HMF (n=70) | Plant HMF (n=66) |
| Gestational age (w) | 31.0 [29.0, 32.0] | 31.0 [30.0, 33.0] |
| Birth weight (g) | 1505 [1192, 1769] | 1565 [1200, 1751] |
| Admission temperature (°C) | 36.5 [36.2, 36.6] | 36.5 [36.4, 36.7] |
| Age at enrolment (h) | 48 [48, 96] | 48 [48, 96] |
| Weight at enrolment (g) | 1472 [1142, 1745] | 1515 [1170, 1720] |
| Length at enrolment (cm) | 40.0 [38.0, 42.0] | 41.0 [38.1, 43.0] |
| Head circumference at enrolment (cm) | 29.0 [27.5, 30.0] | 29.0 [28.0, 30.0] |
| Gestational age category | ||
| <28 w | 7 (10.0%) | 3 (4.5%) |
| 28-<32 w | 32 (45.7%) | 35 (53.0%) |
| ≥32 w | 31 (44.3%) | 28 (42.4%) |
| Birth weight category | ||
| <1000 g | 10 (14.3%) | 5 (7.6%) |
| 1000-1499 g | 23 (32.9%) | 24 (36.4%) |
| ≥1500 g | 37 (52.9%) | 37 (56.1%) |
| Weight for age | ||
| AGA or LGA | 65 (92.9%) | 58 (87.9%) |
| SGA | 5 (7.1%) | 8 (12.1%) |
| Multiple gestation | 29 (41.4%) | 22 (33.3%) |
| Gender | ||
| Male | 43 (61.4%) | 40 (60.6%) |
| Female | 27 (38.6%) | 26 (39.4%) |
| Maternal hypertension | 14 (20.0%) | 17 (25.8%) |
| Maternal diabetes | 8 (11.4%) | 7 (10.6%) |
| Maternal fever | 8 (11.4%) | 7 (10.6%) |
| Umbilical artery doppler changes (A/REDF) | 3 (4.3%) | 9 (13.6%) |
| Antenatal steroids | ||
| Complete | 33 (47.1%) | 34 (51.5%) |
| Incomplete | 22 (31.4%) | 23 (34.8%) |
| Not Received | 15 (21.4%) | 9 (13.6%) |
| Deferred cord clamping ≥60 sec | 33 (47.1%) | 32 (48.5%) |
| Mode of delivery | ||
| LSCS | 58 (82.9%) | 60 (90.9%) |
| VD | 12 (17.1%) | 6 (9.1%) |
| Any resuscitation required | 9 (12.9%) | 8 (12.1%) |
| Total parenteral nutrition requirement on day 1 | 16 (22.9%) | 14 (21.2%) |
| Time of Initiation of Enteral Nutrition (h) | 2.0 [2.0, 2.0] | 2.0 [1.0, 2.0] |
| MoM on Day 7 (%) | 100 [65, 100] | 100 [80, 100] |
| Abbreviations: AGA, appropriate for gestational age; A/REDF, absent or reversal of flow in the umbilical artery; C, Celsius; cm, centimetres; g, grams; h, hours; LGA, large for gestational age; LSCS, lower segment caesarean section; MoM, mother’s own milk; sec, seconds; SGA, small for gestational age; VD, vaginal delivery; w, weeks | ||
Table 2.
Unadjusted and Adjusted Intention-to-Treat Analyses of Growth Velocities (Weight, Length, and Head Circumference) Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
Table 2.
Unadjusted and Adjusted Intention-to-Treat Analyses of Growth Velocities (Weight, Length, and Head Circumference) Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
| Anthropometric parameter* | MD (95% CI) (Plant HMF (n=66) vs. Bovine HMF (n=70)) | p-value |
| Rate of weight gain (g/Kg/d) | ||
| Enrolment until discharge | 3.20 (-0.33, 6.73) | 0.08 |
| Enrolment until 40 w PMA | 0.13 (-0.84, 1.09) | 0.80 |
| Length increment (cm/w) | ||
| Enrolment until discharge | 0.11 (-0.24, 0.46) | 0.53 |
| Enrolment until 40w PMA | -0.02 (-0.13, 0.08) | 0.65 |
| HC increment (cm/w) | ||
| Enrolment until discharge | -0.03 (-0.15, 0.09) | 0.63 |
| Enrolment until 40w PMA | -0.02 (-0.20, 0.16) | 0.83 |
| Anthropometric parameter*+ | aMD (95% CI) | p-value |
| Rate of weight gain (g/Kg/d) | ||
| Enrolment until discharge | 3.20 (0.46, 5.95) | 0.02 |
| Enrolment until 40w PMA | 0.03 (-0.85, 0.92) | 0.95 |
| Length increment (cm/w) | ||
| Enrolment until discharge | 0.11 (-0.24, 0.46) | 0.54 |
| Enrolment until 40w PMA | -0.02 (-0.15, 0.10) | 0.75 |
| HC increment (cm/w) | ||
| Enrolment until discharge | -0.02 (-0.13, 0.09) | 0.72 |
| Enrolment until 40w PMA | -0.02 (-0.12, 0.09) | 0.71 |
|
Abbreviations: aMD, adjusted mean difference; CI, confidence interval; cm, centimetres; d, day; g, grams; HC, head circumference; HMF, human milk fortifier; Kg, kilograms; MD, mean difference; w, week *Intention-To-Treat analyses +Multivariable linear regression analyses, adjusted for gestational age, birth weight, receipt of antenatal corticosteroids, antenatal doppler abnormalities | ||
Table 3.
Adjusted Intention-to-Treat Analyses of Secondary and Safety Outcomes Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
Table 3.
Adjusted Intention-to-Treat Analyses of Secondary and Safety Outcomes Between Plant-Derived Amino-Acid Based HMF and Bovine-Derived Protein Based HMF Groups.
| Outcome variables | Bovine HMF (n=70) | Plant HMF (n=66) | aMD/aRR*+ (95% CI) (Plant HMF vs. Bovine HMF) | aRD (95% CI)*+ (Plant HMF vs. Bovine HMF) | p-value |
| Rate of weight gain (g/Kg/d) | |||||
| Birth until discharge | 1.59 [-7.10, 8.29] | 2.49 [-1.00, 8.17] | 3.15 (-0.17, 6.48) | NA | 0.06 |
| Birth until 40w PMA | 10.49 [8.91, 12.09] | 10.32 [8.88, 11.74] | 0.05 (-0.80, 0.90) | NA | 0.91 |
| Day of regaining BW until 40w PMA | 13.12 [11.39, 14.58] | 12.70 [11.21, 14.97] | -0.24 (-1.58, 1.09) | NA | 0.72 |
| Discharge until 40w PMA | 12.58 [11.04, 15.04] | 12.25 [10.78, 14.71] | -0.08 (-1.18, 1.02) | NA | 0.89 |
| Days to regain BW | 12.00 [10.00, 14.00] | 13.08 [9.00, 15.98] | 1.40 (-1.30, 4.09) | NA | 0.31 |
| No. of feed intolerance days | 0.00 [0.00, 0.01] | 0.00 [0.00, 0.01] | 0.22 (-0.31, 0.75) | NA | 0.41 |
| Duration of hospital stay (d) | 14.00 [7.00, 28.00] | 14.00 [9.00, 24.00] | -2.61 (-9.11, 3.89) | NA | 0.43 |
| Receipt of RBC transfusion | 11.4 (16.2%) | 10.8 (16.4%) | 1.01 (0.43, 2.36) | 0.17 (-12.61, 12.94) | 0.98 |
| NEC (≥Stage 2) | 2.1 (3.0%) | 3.0 (4.6%) | 1.56 (0.26, 9.56) | 1.63 (-4.97, 8.24) | 0.63 |
| LONS | 22.1 (31.6%) | 20.0 (30.3%) | 0.96 (0.52, 1.78) | -1.33 (-17.41, 14.76) | 0.89 |
| BPD | 5.1 (7.3%) | 7.1 (10.8%) | 1.48 (0.47, 4.71) | 3.50 (-6.34, 13.34) | 0.50 |
| ROP requiring intervention | 13.4 (19.2%) | 8.8 (13.3%) | 0.69 (0.29, 1.66) | -5.87 (-18.64, 6.90) | 0.41 |
| MBD | 12.3 (17.6%) | 14.7 (22.2%) | 1.26 (0.58, 2.74) | 4.64 (-9.12, 18.40) | 0.55 |
| EUGR at 40w PMA | 9.7 (13.9%) | 11.3 (17.2%) | 1.24 (0.52, 3.00) | 3.32 (-9.23, 15.88) | 0.63 |
| Mortality | 2/70 (2.9%) | 3/66 (4.5%) | 1.59 (0.27, 9.22) | 1.69 (-4.67, 8.05) | 0.67 |
| Mortality or LTFU | 12/70 (17.1%) | 11/66 (16.7%) | 0.97 (0.46, 2.05) | -0.48 (-13.08, 12.13) | 1.00 |
|
Abbreviations: BPD, bronchopulmonary dysplasia; CI, confidence interval; EUGR: extra uterine growth restriction; HMF, human milk fortifier; IQR, interquartile range; LONS, late onset neonatal sepsis; LTFU, lost to follow-up; MBD, metabolic bone disease; aMD, adjusted mean difference; NA, not applicable; NEC, necrotizing enterocolitis; PMA: post-menstrual age; RBC, red blood cell; aRD, adjusted risk difference; aRR, adjusted risk ratio; ROP, retinopathy of prematurity; SD, standard deviation. *Intention-To-Treat analyses +Multivariable linear regression (continuous variables) and modified poisson regression with robust error variance (categorical variables) analyses, adjusted for gestational age, birth weight, receipt of antenatal corticosteroids, antenatal doppler abnormalities | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



