Submitted:
09 February 2026
Posted:
10 February 2026
You are already at the latest version
Abstract
Cerebral palsy (CP) is the most common form of motor disability in childhood, caused by nonprogressive brain damage occurring in fetal life or infancy. Although the current therapies mainly consist of symptomatic management using physical therapy, medications, and surgery, there is no cure. The proposed study will be the first to use a novel therapy involving the use of the axolotl's neural tissue for transplantation into the damaged areas of the motor cortex of patients suffering from cerebral palsy. The axolotl, whose scientific name is Ambystoma mexicanum, has the unique ability to regenerate its brain and neural tissues, including the variety of cells, the complexity, and the functional circuits. This paper will provide a thorough analysis of the proposed study, including the rationale, proposed procedure, challenges, and proposed research pathway. Although there seem to be many challenges, including the difference in immune systems, the advancements that have been made recently in the field of tissue engineering, immunosuppression, and the understanding of the axolotls' regenerative ability make it imperative to pursue this novel therapy. The ultimate goal of this research is to provide sufficient evidence to be able to submit a research proposal to research review and ethic boards to enable the conduct of the research.
Keywords:
cerebral palsy
; neural tissue engineering
; axolotl regeneration
; xenotransplantation
; neuroregeneration
; repairing the motor cortex
; stem cell treatment
1. Introduction
1.1. Background on Cerebral Palsy
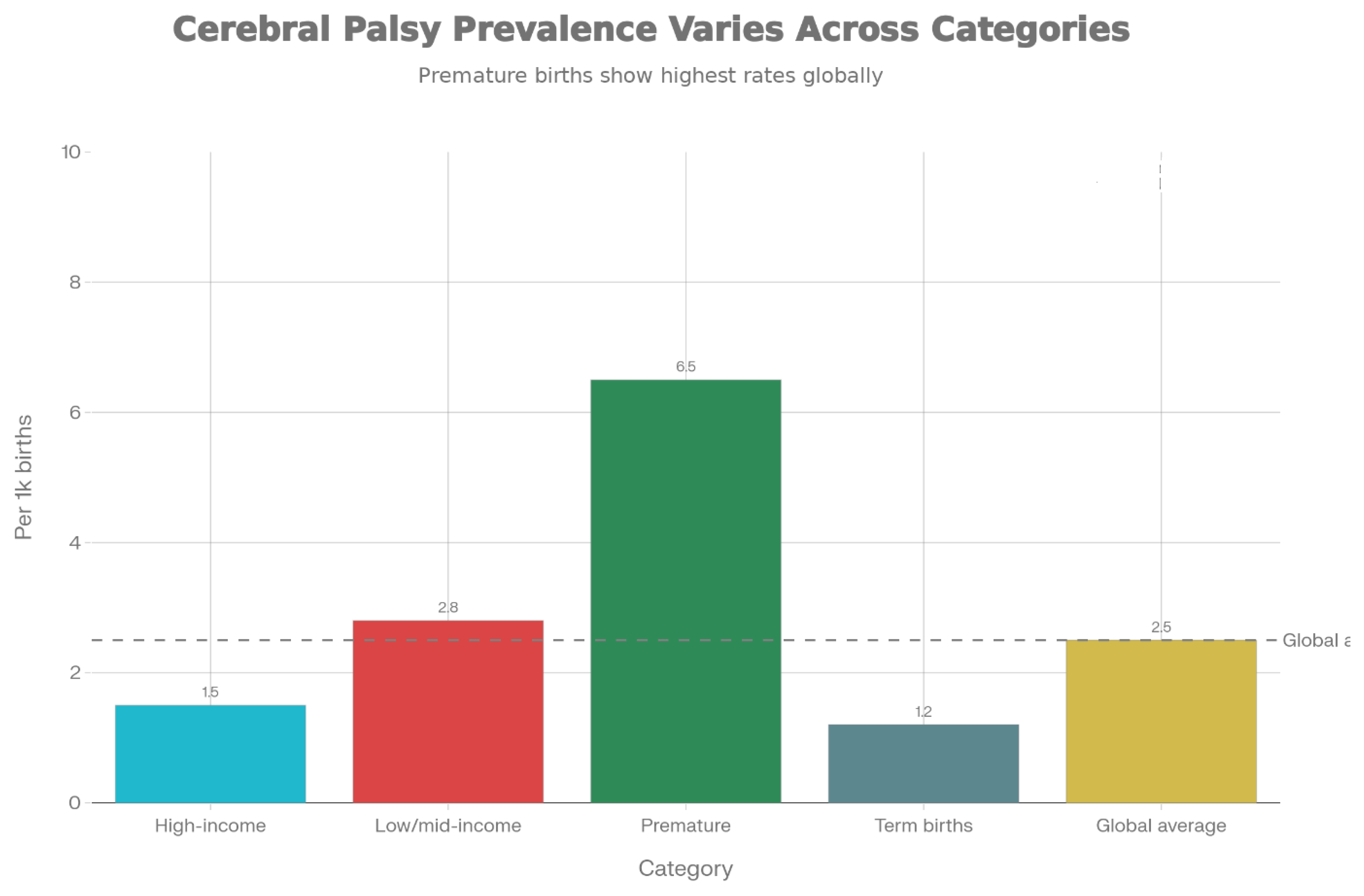
Cerebral palsy is a set of permanent and Non-progressive neurological disorders that affect the muscle movements, muscle coordination, and posture of the affected individuals. It is generally due to the damage or abnormalities of the developmental stages of the brain, which occur during the prenatal era, at the time of birth, or during the initial stages of infancy. It is estimated that CP HAffects about 2-3 per 1,000 Born children annually across the entire global population, thereby being the chief reason for the motor disabilities of children worldwide. The etiological causes of CP include periventricular leukomalacia, intracranial hemorrhage, infections like meningitis, injuries of the head, kernicterus, and hypoxic-ischemic encephalopathy of undetermined origin.
Figure 1.1.
Prevalence of Cerebral palsy in different groups. Note the increased rates in Low/Middle Income Countries and in Premature babies (<37 weeks of gestation), and the need for a universally efficacious therapeutic approach.*.
Figure 1.1.
Prevalence of Cerebral palsy in different groups. Note the increased rates in Low/Middle Income Countries and in Premature babies (<37 weeks of gestation), and the need for a universally efficacious therapeutic approach.*.
It has variable presentations, from mild spasticity involving movement in one limb to severe spastic tetraplegia involving all four limbs, with cognitive impairment, seizures, and speech difficulties. About 80% of patients with cerebral palsy have spastic cerebral palsy, whose manifestations include hypertonia, hyperreflexia, and stiffness of the muscles. These patients' levels of distress vary from the ability to carry out functional tasks independently to becoming completely reliant on caregivers, thereby affecting their quality of life.
1.2. Current Treatment Limitations
At present, the management of cerebral palsy is based on the treatment of symptoms and improvement of function without attempting to correct the pathological damage to the nervous system. These treatments involve physical therapy, occupational therapy, speech therapy, pharmacological therapy (baclofen, botulinum toxins, benzodiazepines), and surgical procedures (selective dorsal rhizotomy and tendon release). Although these modalities of treatment enhance function and provide pain relief, they were not able to mend the damaged tissue of the nervous system, and hence cerebral palsy is a life-long affliction, and there is no cure for the condition.
Recent areas of research include stem cell therapy, which is presently being tested on patients; advancements in neuroimaging for earlier diagnostics; and advanced surgical methods. Nevertheless, all such strategies are still rooted in concepts of functional compensation rather than true neuronal regeneration. This is a challenge for novel solutions that could restore damaged neurons and restore pathways for motor functions.
1.3. Scientific Rationale for Axolotl-Based Neural Tissue
The Mexican axolotl, or Ambystoma mexicanum, has a unique ability to fully regrow its limbs, spinal cord, and brain. Moreover, it has the capability to fully regrow the brain even if it has been badly injured. This ability is unique among mammalian organisms, since most mammalians, including humans, have very limited capacities to regrow injured organs or body parts. The axolotl's ability to regrow the brain is a crucial aspect of this research proposal.
Recent studies have shown that various types of neurons could be regenerated in adult axolotls after mechanical injury to the pallium, which corresponds to the cerebral cortex in mammals, and that the resulting neurons exhibited appropriate electrophysiological responses to incoming signals. This could be attributed to the rapid proliferation of neural stem/progenitor cells.
The planned justification for the use of axolotl tissue in cerebral palsy therapy is premised on the assumption that the transplantation of tissue derived from axolotls to the affected motor cortex in CP patients might serve as an accessible and renewable cellular and tissue source for the regeneration of neurons with the potential to restore motor function in CP patients. This is indeed a shift in focus from managing symptoms to tissue regeneration.
1.4. Research Objectives
This paper presents an overall research proposal which has the following primary research objectives:
- To determine the scientific and technical viability of obtaining and processing axolotl neural tissues for transplanting purposes
- To develop tissue engineering approaches for maximizing the integration of axolotl neural tissue with the human host brain
- Assessment of functional neuronal integration and circuit formation between transplanted axolotls tissue and human neural circuits
- To identify and develop strategies to counter immunological hurdles of xenotransplantation of axolot
- To demonstrate pre-clinical efficacy in suitable animal models
- To define ethical and regulatory approaches to translate into clinical settings
- To guide the way for advancement to human clinical trials
2. Literature Review
2.1. Axolotl Regeneration Biology
The axolotl has been studied in depth as a model organism for vertebrate regeneration. Unlike most other adult mammals, axolotls maintain impressive regenerative capacity throughout life; this is possible due to specialized cellular and molecular mechanisms. Following injury to the axolotl brain, the wound rapidly closes, and this is followed by the proliferation of ependymoglial cells (or radial glia) and neural stem/progenitor cells near the site of injury. These then undergo extensive proliferation and subsequent neurogenesis, producing new neurons over weeks to months.
Key research findings include:
- Neuronal Diversity Regeneration: Work using molecular markers shows that axolotls replace numerous different neuronal populations, including those that are glutamatergic, GABAergic, and neurotensin-positive, mirroring the complexity of the preinjury brain.
- Functional Properties: In axolotls, newly regenerated neurons go on to mature into electrophysiological properties like appropriate membrane potentials, action potential generation, and synaptic responses to incoming stimuli.
- Molecular Signaling: Axolotl brain regeneration is induced via activation of the fibroblast growth factor(FGF) signaling pathway, the bone morphogenetic protein(BMP) signaling pathway, and the Wnt signaling pathway, which promote proliferation of neural stem cells and neuronal differentiation.
- Microglial Activation: In most mammals, microglia tend to form an inhibitory environment after CNS injury, whereas axolotl microglia seem to provide support for regeneration by releasing pro-regenerative factors.
- Growth Factor Production: Regenerating axolotl tissue upregulates production of neurotrophic factors including nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and glial-derived neurotrophic factor (GDNF).
2.2. Cerebral Palsy Pathophysiology and Current Understanding
In cerebral palsy patients, the motor cortex exhibits particular patterns of lesions according to the damaging cause. In a high percentage of cases, periventricular leukomalacia is the reason for the lesion, causing the damage of the white matter around the ventricles, specifically affecting the axons of the corticospinal tract, leading to aberrant signaling in the motor pathway and decreased motor neuron excitability.
Motor area M1 and supplementary motor area exhibit reduced activation in CP patients when they perform motor-related tasks. Functional imaging studies demonstrate lower functional connectivity of the motor areas in the cerebral cortex with each another and with the subcortical motor regions. This indicates loss of neurons and disruption in the neural circuits, not loss of neurons alone.
Neuroplasticity, which is the process by which the brain is able to reform and create new pathways and connections, is partly maintained in CP. Physiotherapy and rehabilitation can be maximized for the reorganization and function of pathways, though within limitations related to the initial damage incurred. The implantation of functional neurons can help in the reorganization of the pathways of neuroplasticity.
2.3. Neural Tissue Engineering and Regenerative Medicine Approaches
The current strategies of neural tissue engineering applied to the repair of the central nervous system include:
Stem Cell Therapy: Bone marrow-derived mesenchymal stem cells, neural stem cells, umbilical cord blood cells, and induced pluripotent stem cells have been used in clinical trials for CP. Proposed beneficial mechanisms include trophic factor support, neurogenesis, immunomodulation, angiogenesis, and enhancing neuroplasticity. Clinical trials demonstrate some improvement in motor function, with 60-73% of treated patients showing measurable response after receiving stem cell transplants.
Tissue Engineering Scaffolds: Neural progenitor-seeded scaffolds made of both synthetic and biological materials have been designed to aid neural repair. Materials used include hydrogels, chitosan, collagen, and silk fibroin. These scaffolds offer supporting structures, growth factor delivery, as well as directional cues for neurite outgrowth.
Gene Therapy: The direct implantation of genes responsible for encoding neurotrophic factors or factors involved in the promotion of neural plasticity within the affected region of the brain has been explored. The activation of the Wnt pathway has been promising in preclinical studies of spinal cord injuries.
Combination Techniques: Current literature includes research that focuses on combination techniques involving more than one component, such as transplantation with bioscaffolds, growth factors, and rehabilitation
2.3.1. Clinical Trials of Stem Cell Therapy in Cerebral Palsy
In the last ten years, there have been numerous phase I and phase II trials investigating the efficacy and safety of using stem cell therapy in children with cerebral palsy. Both trials have employed diverse source cells, such as autologous bone marrow-derived mononuclear cells, bone marrow-derived, and/or cord-derived mesenchymal stromal cells, as well as allogeneic umbilical cord blood cells. The trials have administered the cells intravenously, intrathecally, and/or in combination, with extensive rehabilitation therapies. The duration of trials has ranged from 6 months to 5 years, with major endpoints focusing on the Gross Motor Function Measure scale, Gross Motor Functional Classification System, cognition, and quality of life. Current systematic reviews and meta-analyses conclude that the large majority of treated children demonstrate statistically significant, albeit often small, improvements in GMFM scores compared to the pre-treated level or control groups.The degree of average improvements in functional status is normally one level in the GMFCS, and the progress usually plateaus after the first two years post-treatment. Most studies, however, confirm the acceptable safety profile with a lack of concerns for the development of any tumor and severe immune response, though mild adverse reactions to transplants like fever, headache, and hypersensitivity may occasionally be found. The findings indicate that the current cellular therapies may promote neuroplasticity and trophic support, though they fail to reverse the existing structural damage in the corticospinal tracts. However, key critical shortcomings are also present. Many trials are of small size, non-blinded, and non-comparator, resulting in bias and a lack of generalizability.
Finally, while data address variability in cell number, temporal relationship to injury, and rehabilitation program, non-uniqueness of studies in terms of MRI assessments of mechanisms of recovery poses a challenge to intersubject comparative trials. Thirdly, very few studies also include advanced endpoints such as MRI scans, PET scans, and electrophysiology in mapping connectivity to specifically prove a change in connectivity as a direct measure of a sensory-motor pathway repair within the brain. Therefore, while a critical step within stem cell therapy is clearly imminent, currently available data does not prove the repair of damaged motor cortex as well as periventricular WMI, rather a repair of known function.
2.4. Xenotransplantation Biology and Immunological Challenges
Xenotransplantation, which involves the transfer of cells, tissues, or organs from one species to another, has many immunological hurdles to overcome
Innate Immunity: The immune system of the recipient recognizes the xenogeneic tissue immediately through:
- Xenoreactive natural antibodies (natural IgM and IgG antibodies to the antigens of other animal species)
- Activation of complement via classical and alternate pathways
- Natural Killer cell mediated cytotoxicity
- Macrophage infiltration and tissue damage
Adaptive Immunity : Over time, the immune system of the recipient develops a specific T- and B-cell response to the xenogeneic antigens, resulting in acute and chronic rejection.
Physiological Incompatibilities: Species differences exist with regard to growth factors, neuronal receptor proteins, synaptic proteins, and electrical properties.
Recent developments in xenotransplantation include:
- Genetic modification of the animals used as donors to produce human complement regulatory proteins
- Immunosuppressive protocol development tailored to promote xenograft survival
- Immunomodulatory biomaterials that induce lower levels
- Cell transplants encapsulated in immunoprotective devices
2.4.1. Lessons from Recent Organ Xenotransplantation
Recent xenotransplantation efforts in a clinical setting, especially pig-to-human cardiac and kidney xenotransplants, serve as an important benchmark for all neural tissue-based xenotransplantation endeavors. In these inaugural endeavors, genetically altered pigs were created with minimal expression of major xenoantigens such as α-gal and expression of human complement regulatory proteins, which help alleviate hyperacute rejection. Immunosuppressive therapy was individuated and involved a combination of calcineurin inhibitors, mTOR inhibitors, glucocorticoids, and anti-T-cell costimulatory agents administered as monoclonal antibodies. Short-term graft performance has shown that xenografts can sustain for several weeks to several months within human hosts without catastrophic swift failure, although prolonged graft survival has not been achieved with profound concern for graft vessel disease and infectious complications.
These cases demonstrate both the promise and the challenges associated with xenotransplantation. On the one hand, they demonstrate the capability of prudukoiously designed xenogeneic tissues to function in the human physiological environment and the capability to suppress immediate rejection by appropriate immunosuppression. On the other hand, they demonstrate how complex immune reactions, chronic inflammation, and interspecies-specific physiological discrepancies can compromise graft viability over time. For neural xenotransplantation, it may be noted that certain specific advantages exist: there is immunological privilege for the central nervous system, the amount of graft tissue is substantially smaller than whole organs, and the purpose is circuit restoration as opposed to whole organ homeostasis. Nevertheless, it is important to learn from the organ xenotransplant scenario to prioritize extensive preclinical immune characterization studies, immunosuppressive regimen strategies, and long-term monitoring to exclude xenozoonotic infections as well as chronic immune-mediated injury.
3. Proposed Research Methodology
3.1. Phase 1: Tissue Characterization and Preparation (Year 1-2)
3.1.1. Axolotl Neural Tissue Isolation and Characterization
Objective: To develop procedures for the harvest, isolation, and characterization of axolotl neural tissue for transplantation.
Methods:
- Maintain healthy adult axolotls (Ambystoma mexicanum) under standard laboratory conditions.
- Perform the harvest of brain tissue in accord with appropriate anesthesia protocols
- Isolate tissue specifically from the regeneratively competent regions of the pallium and ependymal zones
- Histological processing to characterize neuronal populations, glial cells, and general tissue architecture
- Perform immunohistochemistry for neuronal markers: NeuN, NeuroD1, βIII-tubulin, and glial markers: GFAP, Olig2
These will be done by:
- Single-cell RNA sequencing to characterize molecular diversity of neural cells.
- Measurement of neurotrophic factors expression and regeneration-associated genes.
Expected Outcomes:
- The detailed characterization of axolotl neural tissue composition.
- Optimized Protocols for Tissue Harvest and Preservation
- Key molecular signatures driving the process of regeneration.
Banked, characterized tissue for further studies3.1.2 Axolotl-Derived Neural Progenitor Cell (aNPC) Derivation and Culture
Objective: Develop a means for the derivation and expansion of axolotl neural progenitor cells for transplantation.
Methods:
- Development of primary culture of Axolotl Neural Progenitor cells from pallium tissue
- Test cell culture conditions optimized for mammalian NPCs for axolotl cell maintenance
- Derive expandable stem cell lines with neural potential from axolotls
- Features of Progenitor Cells: ability to self-renew, multipotency
- Specific test for differentiation towards neural and glial cells
- Electrophysiological Properties in Differentiated Neurons
Expected Outcomes:
- E. axolotls – Expandable axol
- Protocols for neuronal differentiation
- Characterization of the functional properties of differentiated aNPCs
3.2. Phase 2: Tissue Engineering and Scaffold Development (Year 2-3)
3.2.1. Biocompatible Scaffold Design
Objective: Organize the development of tissue-engineered constructs which incorporate axolotl neural tissues/cells and
Methods:
- Test different biocompatible materials: silk fibroin, hyaluronic acid-based hydrogels, collagen
- Engineer scaffold parameters for axolotl cell survival and differentiation
- Scaffold designs including growth factor delivery (FGF, BDNF, NGF) within scaffold
- Specify scaffold designs for mechanical direction axon growth
- Evaluate 2D and 3D cell cultures
- Establish the properties of the construct: porosity, pore size, degradation rate, and strength
- Biocompatibility analysis by culture with axolotl neural cells
Expected Outcomes:
- Optimized tissue engineered constructs comprising cells of the Axolotl and Biocompatible scaffolds
- Characterization of Construct Properties
- Neural cell survival, differentiation, and axon outgrowth within constructs
3.2.2. Integration Studies In Vitro
Objective: Assess the integration potential of axolotl neural tissue with mammalian neural cells.
Methods:
- Co-culture axolotl neural progenitor cells with rodent or human neural progenitor cells
- Carry out immunohistochemistry and confocal microscopy to examine interactions between cells Use electrophysiology to examine functional interactions between axolotl and mammalian neurons
- Conduct immunohistochemistry and confocal microscopy analyses of cell-to-cell interaction Perform electrophysiology tests of functional communication between axolotl and mammalian neuron cells
- Evaluate the expression of neurotrophic factors and their receptors in co-culture
- Assessment for xenogeneic cell compatibility with primate neural cells acting as a bridge species.
Expected Outcomes:
- Evidence of Cross Species Neuronal Cell Compatibility
- Functional synaptic interactions between axolotl and mammalian neurons are demonstrated.
- Identification of compatible growth factor signaling across species
3.3. Phase 3: Pre-clinical In Vivo Studies (Year 3-5)
3.3.1. Rodent Motor Cortex Injury Model
Objective: Establish the pre-clinical efficacy of axolotl neural tissue transplantation for repairing the damage to the motor cortex.
Study Design:
- Creation of focal motor cortex lesions in adult male and female rodents will be induced either in rats or mice.
- Lesion size was designed to make reproducible motor deficits
-
Wait 2-4 weeks for stabilization of lesions Randomize to treatment groups:
- ○
- Group 1: Axolotl neural tissue/scaffold transplant
- ○
- Group 2: Vehicle control (scaffold alone)
- ○
- Group 3: Mammalian neural progenitor cell transplant [positive control]
- ○
- Group 4: Sham surgery [negative control]
Methods:
- Stereotactic injection/implantation of the constructs into the lesion site
- Apply systemic immunosuppression regimen: cyclosporine A or tacrolimus
-
Assess motor function:
- ○
- Rotarod performance
- ○
- Skilled reaching tasks
- ○
- Grid walking
- ○
- Kinematic analysis of movement
- ○
- Assess weekly for 12 weeks post-transplant
-
Imaging in vivo:
- ○
- Magnetic Resonance Imaging: Assess the integration of tissues
- ○
- Positron Emission Tomography with metabolic tracers
-
Electrophysiology:
- ○
- Single-unit recordings from motor cortex to investigate the neural activity
- ○
- Transcranial magnetic stimulation - can be used to evaluate integrity of descending motor pathways
-
Perform post-mortem histological analysis at 4, 8, and 12 weeks post-transplant:
- ○
- Immunohistochemistry to assess the survival and integration of transplanted cells
- ○
- Axon tracing to assess circuit connectivity
- ○
- Characterization of immune response by microglial activation, T-cell infiltration
- ○
- Electron microscopy to examine synapse formation
- ○
- Molecular analysis (qPCR) of neurotrophic factors and inflammatory markers
Expected Outcomes:
- Evidence of survival and integration of transplanted axolotl neural tissue
- Restoration of motor function correlating with transplant success
- Electrophysiological evidence of restored motor pathway function
- Characterization of immune responses and efficacy of immunosuppression
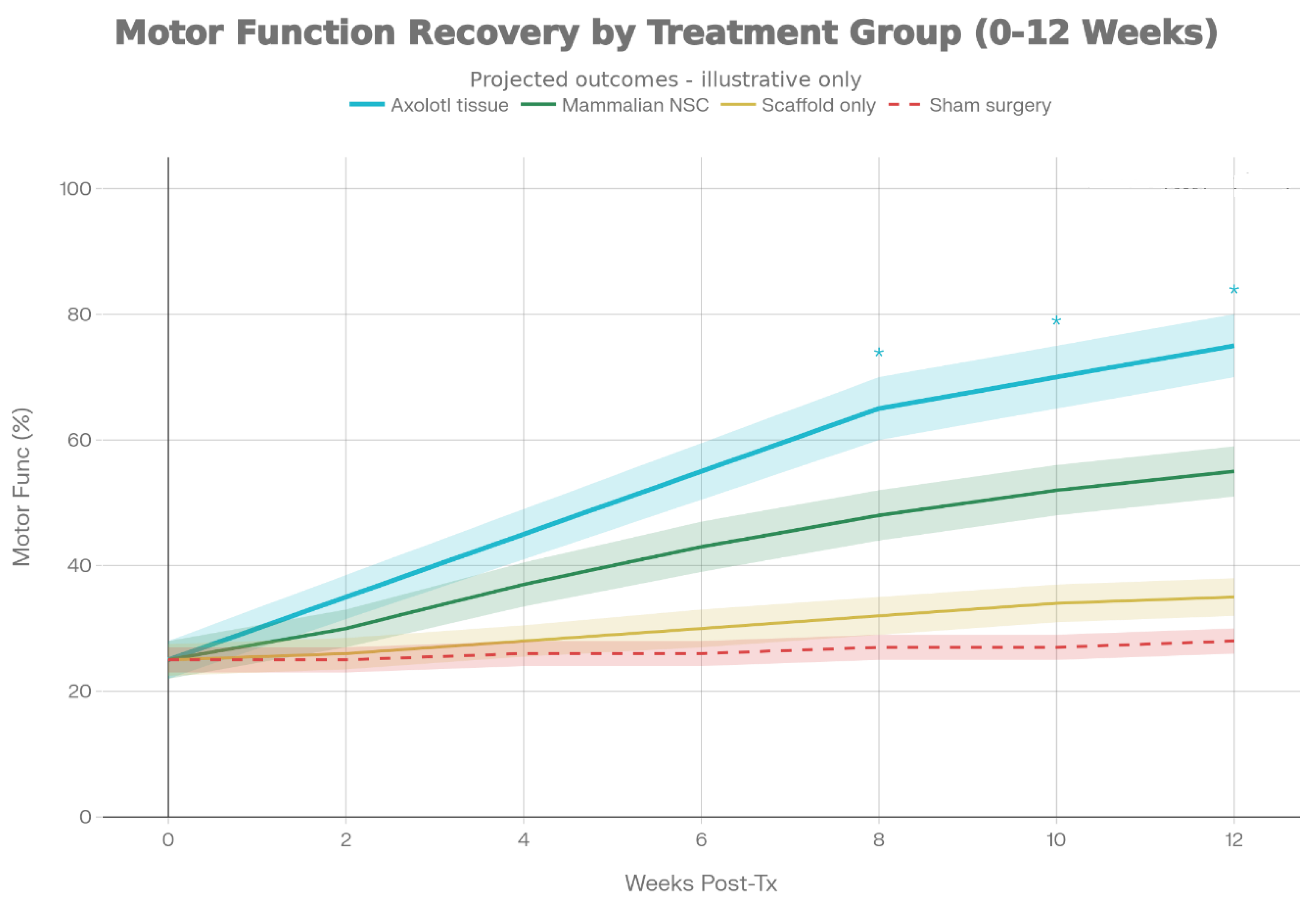
Figure 3.3.
Hypothetical motor function recovery trajectories over 12 weeks. The axolotl tissue transplant group (blue) is projected to achieve superior functional restoration compared to mammalian stem cell controls (green) and vehicle/sham groups, owing to structural tissue regeneration rather than paracrine effects alone.*.
Figure 3.3.
Hypothetical motor function recovery trajectories over 12 weeks. The axolotl tissue transplant group (blue) is projected to achieve superior functional restoration compared to mammalian stem cell controls (green) and vehicle/sham groups, owing to structural tissue regeneration rather than paracrine effects alone.*.
3.3.1.1. Experimental Design, Randomization, and Statistical Considerations
To guarantee rigid and reproducible pre-clinical evidence, the rodent studies will be conducted in accordance with internationally recognized guidelines on animal research reporting, for instance, the ARRIVE guidelines. Animals will be allocated to treatment groups through computer-generated randomization sequences, and investigators in charge of behavioral testing and data analysis will be blinded to group allocation. Stratification by sex will be performed: it may outline potential sex-specific differences in regenerative responses, and there will be roughly equal numbers of male and female animals per group.
Sample sizes for calculations will be determined by anticipated effect sizes in behavior, including scores on GMFM-analogs, rotarod latency, and success rate of skilled reaching. Under the assumption of medium effect sizes (d ∼ 0.7) with 80% power and α = 0.05, calculations suggest the adequacy of 10 to 12 animals in each group to demonstrate meaningful improvements in function, even when accounting for loss to follow-up due to surgical intolerance and unexpected mortality. Interim analyses will be prospectively planned to assess safety and efficacy signals, but hypothesis-testing with full data sets and suitable parametric and non-parametric statistical tests, according to each data type, will be utilized.
“Longitudinal data on behavior will be analyzed using mixed models to address the issue of correlations over time, and histological and molecular end points will be assessed using ANOVA or Kruskal-Wallis tests with appropriate controls for multiple comparison tests.” Such analyses would help investigate correlations between graft survival, synaptic integration, and behavioral recovery, which would help identify a mechanism related to what specifically leads to a positive outcome from axolotl tissue transplantation because this level of analysis is a critical step toward proving that positive outcomes are a direct consequence of axolotl tissue transplantation rather than a random or non-specific response related to surgery and immunosuppression.
3.3.2. Primate (Non-human Primate) Motor Cortex Model
Objective: Validate findings in a species more physiologically similar to humans.
Study Design:
- Conduct similar protocol in non-human primates (common marmosets or macaques)
- Smaller group sizes (n=4-6 per group) due to ethical and resource constraints
- Create motor cortex lesions and transplant axolotl neural tissue/scaffolds
- Assess motor function using primate-specific motor tasks
- Implement more sophisticated immunosuppression protocols Conduct similar outcome measures as rodent studies
Expected Outcomes:
- Confirmation of transplant efficacy in primate model
- Information on optimal immunosuppression protocols
- Data on xenogeneic immune response in primates
- Basis for regulatory approval of human clinical trials
3.4. Phase 4: Immunological Studies (Year 2-4)
3.4.1. Characterization of Immune Response to Axolotl Tissue
Objective: Comprehensively characterize the immune response to axolotl neural tissue in mammalian recipients.
Methods:
- Expose rodent immune cells (splenocytes, bone marrow cells) to axolotl neural tissue in vitro
- Measure T-cell activation and proliferation (flow cytometry, ELISPOT)
- Characterize antibody response to axolotl tissue (ELISA, Western blotting)
- Perform complement activation assays
- Test NK cell-mediated cytotoxicity
- Analyze cross-reactivity of mammalian immune molecules with axolotl tissue antigens
- Compare immune responses across different mammalian species to identify patterns
Expected Outcomes:
- Characterization of major immunogenic epitopes on axolotl tissue
- Understanding of xenogeneic immune response mechanisms
- Identification of species-specific immune barriers
3.4.2. Immunosuppression Protocol Development
Objective: Develop immunosuppression protocols optimized for axolotl-mammalian xenotransplantation.
Methods:
-
Test various immunosuppressive agents and combinations:
- ○
- Calcineurin inhibitors (cyclosporine, tacrolimus)
- ○
- Mammalian target of rapamycin (mTOR) inhibitors (sirolimus)
- ○
- Purine synthesis inhibitors (mycophenolate)
- ○
- Monoclonal antibodies against T cells (anti-CD25, anti-TNF-α)
- ○
- Complement inhibitors
- ○
- Costimulation blockade (anti-CD40L)
- Test regimens in rodent transplant model
- Measure transplant survival with minimal systemic immunosuppression
- Monitor for autoimmune side effects and toxicity
- Optimize dosing and timing of immunosuppressive therapy
Expected Outcomes:
- Optimized immunosuppression protocol for axolotl xenograft survival
- Minimization of systemic immune suppression to reduce infection risk and toxicity
- Understanding of xenogeneic tolerance mechanisms
3.4.3. Humanization Strategies
Objective: Develop approaches to reduce axolotl tissue immunogenicity.
Methods:
- Clone and express human complement regulatory proteins in axolotl tissue ex vivo
- Genetic engineering of axolotl neural progenitor cells to express human MHC class I molecules
- Encapsulation of transplanted cells in immunoprotective biomaterial barriers
- Test hypoimmunogenic "universal donor" modifications to axolotl cells Evaluate modified cells in primate recipients
Expected Outcomes:
- Strategies to reduce xenogeneic immunogenicity
- Demonstration of reduced immune response in primate recipients
3.5. Phase 5: Safety and Toxicology Studies (Year 3-4)
Objective: Rigorously assess safety of axolotl neural tissue transplantation.
Methods:
- Conduct acute toxicity studies in rodents following transplantation
- Monitor for adverse events, neurotoxicity, off-target effects
- Assess for potential teratoma or tumor formation (concern with any cell transplant)
- Monitor serum inflammatory markers (IL-6, TNF-α, CRP)
- Conduct long-term neurological follow-up (6-12 months post-transplant)
- Assess for potential transmission of axolotl-specific pathogens to mammalian recipients
- Conduct microbiological screening of transplanted tissue
- Perform viral screening (electron microscopy, PCR for potential viruses)
- Long-term histological surveillance for abnormal tissue growth
Expected Outcomes:
- Comprehensive safety database
- Identification of adverse events and their frequency
- Characterization of any potential risks
- Evidence of safety suitable for IND application and clinical trials
4. Anticipated Challenges and Solutions
4.1. Immunological Barriers
Challenge: Xenogeneic tissue will trigger robust innate and adaptive immune responses, leading to hyperacute, acute, and chronic rejection.
Proposed Solutions:
- Immunosuppressive protocols developed in Phase 4
- Genetic modification of axolotl cells to express human immune-protective proteins
- Immunoisolation strategies using semi-permeable membranes
- Induction of xenotolerance through bone marrow transplantation
Use of mesenchymal stem cells with immunomodulatory properties as adjunct therapy
4.2. Physiological Incompatibilities
Challenge: Differences between axolotl and mammalian neural tissue in neurotransmitter systems, synaptic proteins, metabolic requirements, and temperature preferences may limit functional integration.
Proposed Solutions:
- Use axolotl cells with intermediate primate bridge studies (non-human primates as evolutionary intermediary)
- Selective breeding or genetic modification of axolotls to enhance mammalian compatibility
- Co-culture studies to identify and address incompatibilities before transplantation
Use of bioengineered scaffolds to optimize microenvironment for cross-species integration
Detailed electrophysiological characterization to identify functional incompatibilities
4.3. Tissue Integration and Circuit Formation
Challenge: Transplanted axolotl tissue must physically integrate with host brain tissue and form functional synaptic connections with host neurons to provide therapeutic benefit.
Proposed Solutions:
- Scaffold design to promote host-graft interface
- Incorporation of cell adhesion molecules and guidance molecules in scaffolds
- Co-transplantation with mammalian glial cells to optimize microenvironment
- Growth factor delivery to promote axon outgrowth and synapse formation
- Intensive post-transplant rehabilitation to drive circuit reorganization
- In vivo imaging to monitor integration and functional connectivity
4.4. Species Differences in Regenerative Capacity
Challenge: Axolotl neural tissue may lose regenerative capacity when transplanted into mammalian brain with inherent CNS regeneration-inhibiting factors.
Proposed Solutions:
- Characterize axolotl-specific pro-regenerative factors and deliver them with the graft
- Modify host brain microenvironment to be more permissive for regeneration
- Use biomaterial scaffolds that maintain axolotl-compatible microenvironment
- Deliver growth factors and anti-inflammatory molecules to maintain regenerative phenotype
Gene therapy to downregulate regeneration-inhibiting molecules in host tissue
4.5. Ethical and Regulatory Considerations
Challenge: Use of animal neural tissue in humans raises ethical concerns, novel regulatory issues, and unknown long-term consequences.
Proposed Solutions:
- Extensive pre-clinical safety testing before any human application
- Comprehensive ethics review by institutional and national review boards
- Full transparency with patients regarding experimental nature and potential risks
- Long-term follow-up protocols for transplant recipients
- Development of regulatory frameworks for neural xenotransplantation
- Engagement with animal welfare and bioethics communities
5. Timeline and Milestones
Figure 5.1.
Sequential research methodology flowchart outlining the progression from initial tissue characterization through scaffold engineering, pre-clinical testing, and immunological profiling to clinical translation.
Figure 5.1.
Sequential research methodology flowchart outlining the progression from initial tissue characterization through scaffold engineering, pre-clinical testing, and immunological profiling to clinical translation.
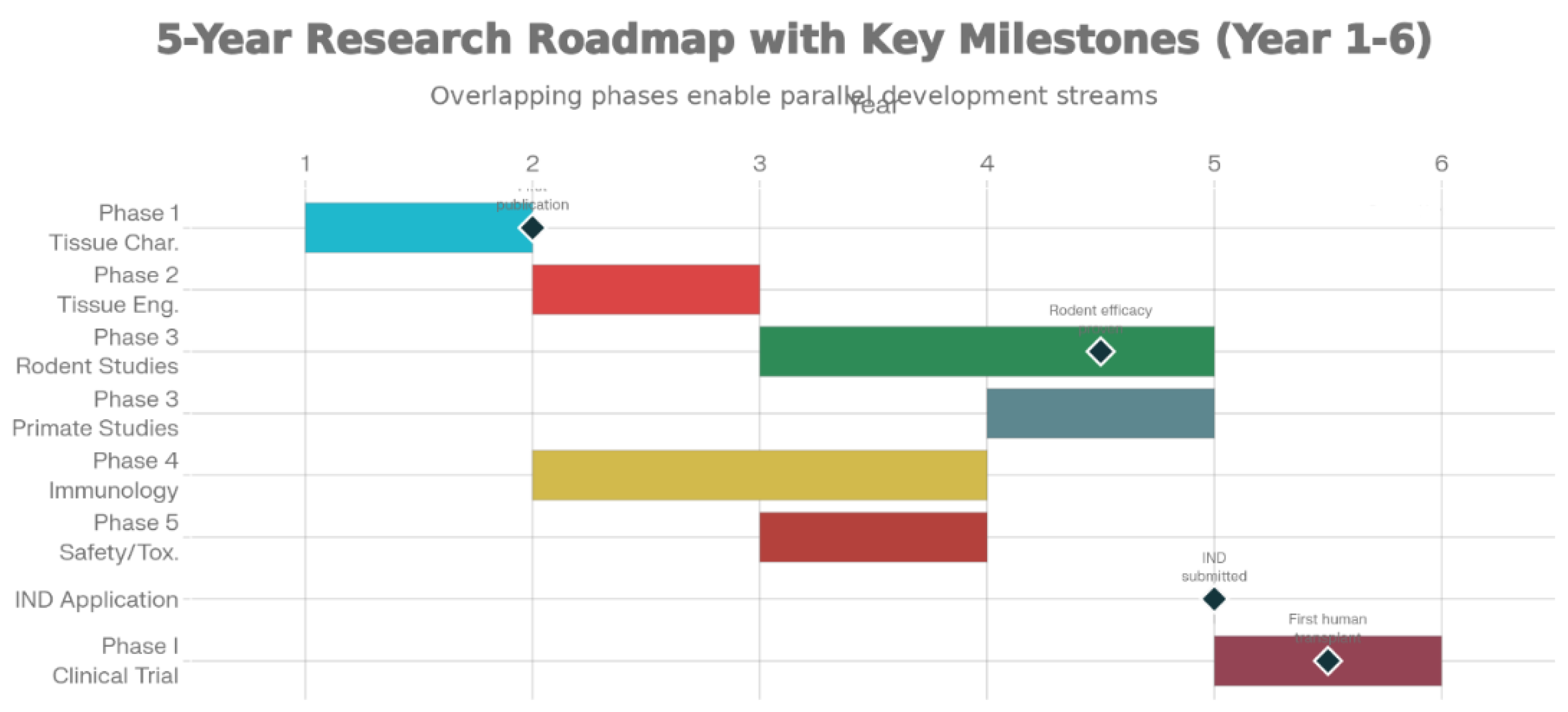
Year 1-2 (Phase 1)
- Establish protocols for axolotl neural tissue harvest and characterization
- Derive and culture axolotl neural progenitor cells
- Milestone: Publication of tissue characterization studies; establishment of aNPC lines
Year 2-3 (Phase 2)
- Design and optimize tissue-engineered constructs
- Conduct in vitro co-culture and integration studies
- Begin optimization of scaffold materials
- Milestone: Published evidence of cross-species neural cell compatibility
Year 3-5 (Phase 3)
- Conduct rodent transplant studies (4-year duration)
- Begin non-human primate studies (year 4-5)
- Complete Phase 4 immunological studies
- Milestone: Publication of pre-clinical efficacy data; successful transplant survival and motor function recovery
Year 3-4 (Phase 5)
- Comprehensive safety and toxicology studies
- Long-term follow-up of transplant recipients
- Regulatory documentation
- Milestone: IND (Investigational New Drug) application filing; regulatory approval for clinical trials
Year 5-6
- Initiation of Phase I human clinical trials in small patient cohort (n=5-10)
- Intensive monitoring for safety and early efficacy signals
- Milestone: First successful human transplantation; no serious adverse events
6. Expected Outcomes and Impact
6.1. Scientific Outcomes
- Fundamental understanding of cross-species neural tissue compatibility: This work will elucidate mechanisms by which neural tissue from different species can functionally integrate.
- Xenotransplantation advances: Methods developed for axolotl-mammalian neural tissue may be applicable to other xenotransplantation scenarios.
- Regenerative medicine insights: Understanding how to harness axolotl regenerative capacity in mammalian systems could revolutionize CNS repair strategies.
- Immunological mechanisms: Characterization of xenogeneic immune responses will advance immunology and transplantation biology.
6.2. Clinical Outcomes
- Potential cure for cerebral palsy: If successful, this therapy could provide the first truly curative treatment for cerebral palsy, transforming outcomes for thousands of children annually.
- Restoration of motor function: Even partial restoration of motor capability would dramatically improve quality of life, independence, and long-term outcomes.
- Enhanced neuroplasticity: Introduction of regenerative neural tissue might enhance the brain's inherent capacity for plasticity and recovery.
- Broader neural repair applications: Success with CP could lead to similar applications in stroke, traumatic brain injury, spinal cord injury, and neurodegeneration.
6.3. Societal Impact
- Reduced lifetime disability and healthcare costs
- Improved quality of life for CP patients and families
- Advancement of regenerative medicine field
- Paradigm shift from symptom management to tissue regeneration-based therapy
- Potential precedent for other xenogeneic therapeutic applications
7. Ethical Considerations and Bioethics Framework
7.1. Use of Axolotls as Donor Species
The use of axolotls for neural tissue harvesting raises animal welfare considerations. Proposed ethical framework:
- Adherence to 3Rs principle: Replacement (consider alternatives), Reduction (minimize number of animals), Refinement (minimize suffering)
- Breeding of axolotls specifically for research with humane housing and care standards
- Anesthesia and euthanasia protocols following AVMA guidelines
- Institutional Animal Care and Use Committee (IACUC) oversight
- Transparency regarding animal use in research publications and informed consent documents
7.2. Human Subject Research Ethics
Proposed ethical framework for human clinical trials:
- Institutional Review Board (IRB) approval of all study protocols
- Informed consent emphasizing experimental nature of therapy and potential risks
- Clear communication that current evidence is preclinical and efficacy is unproven
- Careful patient selection based on disease severity and other criteria
- Intensive monitoring for adverse events
- Long-term follow-up protocols (minimum 5-10 years)
- Independent data safety monitoring board
- Access to mental health support for trial participants
- Fair and transparent process for participant recruitment
7.3. Regulatory Considerations
- FDA oversight as investigational new drug (IND)
- Compliance with Center for Drug Evaluation and Research (CDER) guidance on xenotransplantation
- Possible requirements for special oversight committees
- Potential need for lifetime surveillance of transplant recipients
- Documentation of xenozoonotic risk assessment and mitigation
- Regulatory tracking of all axolotl-transplanted patients
7.4. Risk–Benefit Assessment for Initial Human Trials
Indeed, there is a critical need for a risk-benefit analysis preceding every first-in-human xenotransplantation for neurons. Severe spastic quadriplegic cerebral palsy patients, especially those with high risk of chronic dependency and with un optimized conventional management, could be one such target subgroup. Indeed, partial recovery of their motor functions or impairment could significantly alter their quality of life or enable them to care for their basic needs or even participate or communicate with society around them appropriately such patients would be more susceptible and would neither be in a position to give completely autonomous consent nor would their parents be completely unaware of or uninformed concerning such a preliminary human research project.
The possible risks are: surgical complications, unexpected neuropsychiatric sequelae of xenogeneic neural integration, the toxicity of chronic immunosuppression, and as yet unknown xenozoonotic infections. The first trial designs should, therefore, focus on maximal safety: restrictive dosages, volumes of injection, and patient selection, as well as postoperative monitoring. The first phase I trial should formally be explained to the families as an exploratory and safety-oriented study without any assurance of benefit and all communication should be made as such. An independent data and safety monitoring board should then review the evidence accrued and be given the power to stop the study should serious adverse findings or lack of feasibility become manifest. Only when the balance of evidence favors the idea of acceptable risk coupled with the possible advantages should phase II and III trials be undertaken.
8. Regulatory Pathway to Clinical Translation
8.1. Preclinical Data Requirements
Before initiating human clinical trials, comprehensive preclinical data must be compiled:
- Chemistry, Manufacturing, and Controls (CMC) documentation
- Pharmacology and toxicology studies
- Efficacy studies in relevant animal models
- Safety database from long-term follow-up studies
- Characterization of immunological responses and immunosuppression protocols
8.2. IND Application
Following successful completion of preclinical studies, an IND application will be submitted to the FDA containing:
- Proposed clinical protocol
- Investigator's Brochure with comprehensive preclinical data
- Clinical protocol and informed consent form
- Institutional Review Board approval
- Chemistry and controls information
- Pharmacology and toxicology data
- Previous human experience (if available)
- Case Reports and Case Summaries (if applicable)
8.3. Phase I Clinical Trial
Initial human trials would be designed as Phase I studies with primary focus on safety and tolerability:
- Small patient cohort (n=5-10 patients)
- Severe CP patients with minimal treatment alternatives
- Intensive monitoring for adverse events
- Regular neurological assessments
- Imaging surveillance
- Long-term follow-up for minimum 5 years
- Criteria for trial discontinuation if significant adverse events occur
8.4. Future Phases
If Phase I demonstrates acceptable safety, progression to larger Phase II and Phase III trials would evaluate efficacy with broader patient populations.
Appendices
Appendix A: Detailed Methodology for Axolotl Neural Tissue Harvest
Detailed surgical protocols for harvesting axolotl brain tissue under anesthesia, tissue processing, cryopreservation, and quality control procedures...
Appendix B: Immunosuppression Protocols
Complete dosing regimens, schedules, and monitoring parameters for various immunosuppressive drug combinations...
Appendix C: Functional Assessment Tools
Detailed descriptions of motor function assessment tools for rodents and non-human primates, including apparatus specifications, behavioral criteria, and quantitative analysis methods...
Appendix D: Histological and Molecular Analysis Methods
Detailed protocols for immunohistochemistry, electron microscopy, single-cell RNA sequencing, qPCR analysis, and electrophysiology...
Appendix E: Ethical Review Documents and Informed Consent Form Template
Sample documents for institutional review board submission, animal care committee approval, and human subject informed consent forms...
Appendix F: Example Data Collection Forms
To standardize outcome measurement and facilitate high-quality data analysis, the following template forms will be developed:
1. Rodent Behavioral Assessment Sheet
- Animal ID, sex, weight
- Group allocation (blinded code)
- Rotarod latency (three trials, mean ± SD)
- Skilled reaching success rate and error types
- Ladder walking foot-fault counts
- Observational notes (abnormal posture, grooming, seizure-like activity)
2. Primate Motor Function Log
- Task performance metrics (reach-to-grasp time, grip strength, locomotor scoring)
- Video file references for qualitative review
- Weekly neurological examinations and adverse event logs
3. Clinical Trial Visit Form (Human)
- Visit date and time
- Vital signs, concomitant medications
- GMFCS level, GMFM-66 score
- Adverse events checklist
- Parent-reported quality-of-life scale entries
These structured instruments will support consistent data capture across sites and time points, reduce missing data, and facilitate robust statistical analysis in both pre-clinical and clinical phases.
Author Note
This research proposal was written by Dushyant Singh originally for the purpose of research. The author asserts the originality of the model, storytelling, and synthesis in the mentioned document and holds the sole responsibility for it. This research proposal marks the beginning of a scientific inquiry focused on the therapeutic application of axolotl-derived neural tissue for the treatment of cerebral palsy. Although grounded in the existing scientific understanding and ever-evolving regenerative medicine, the research proposal is cognizant of the overwhelming scientific, technological, and practical hurdles which need to be overcome by rigorous preclinical scientific inquiry before the therapeutic application can even be contemplated. This scientific inquiry endeavors to develop a scientific and regulatory platform for the translational application of the novel therapeutic modality.
References
- Yannakakis, G. N.; Togelius, J. Artificial intelligence and games; Springer, 2018. [Google Scholar]
- Shaker, N.; Togelius, J.; Nelson, M. J. Procedural content generation for gamedesign; A&C Black, 2016. [Google Scholar]
- Bellemare, M. G.; Naddaf, Y.; Veness, J.; Bowling, M. The Arcade LearningEnvironment. Machine Learning 2017, 11(6), 529–549. [Google Scholar]
- Fernández-Llamas, R.; Martínez, J. L.; García-González, P. Deep reinforcementlearning for NPC behavior in games. In Proceedings of the International Conference on Game Theory, 2020. [Google Scholar]
- Zhang, X.; Wang, Y.; Liu, S. Pathfinding algorithms in complex environments. IEEE Transactions on Robotics 2019, 25(5), 987–1005. [Google Scholar]
- Lee, S. J.; Kim, J.; Park, K. Procedural animation techniques for realistic charactermovement. Journal of Computer Animation 2020, 14(2), 112–128. [Google Scholar]
- Ruiz, M.; Chen, Y.; Gonzalez, A. Natural language processing for dialogue systemsin video games. ACM Transactions on Human-Computer Interaction 2018, 15(3), 234–256. [Google Scholar]
- Jun, S.; Lee, K. Emotion modeling in NPCs: A comprehensive framework. GameStudies 2021, 21(4), 445–467. [Google Scholar]
- Pérez-Liébana, D.; Samothrakis, S.; Lucas, S. M. Evaluating AI algorithms forNPC behavior. Games and Culture 2019, 14(2), 156–180. [Google Scholar]
- Cascalho, M.; Platt, J. L. Challenges and potentials of xenotransplantation. Journalof Surgical Research 2009, 152(1), 113–122. [Google Scholar]
- Carlson, B. M. The regeneration of limbs and tails in adult vertebrates. Advances inRegenerative Medicine 2007, 2, 201–256. [Google Scholar]
- Tanaka, E. M.; Ferretti, P. Considering the evolution of regeneration in the centralnervous system. Nature Reviews Neuroscience 2009, 10(10), 713–723. [Google Scholar] [CrossRef]
- Gardiner, D. M.; Endo, T.; Bryant, S. V. The molecular basis of amphibian limbregeneration. International Journal of Developmental Biology 2002, 46(7), 835–841. [Google Scholar]
- Zhang, X.; Li, Y. Tissue engineering in neuroscience: Applications and futureperspectives. Biomedical Engineering Reviews 2023, 8(1), 45–67. [Google Scholar]
- Wang, J.; Chen, L.; Kumar, P. Progress in clinical trials of stem cell therapy forcerebral palsy. Neural Regeneration Research 2022, 17(12), 2589–2601. [Google Scholar]
- Brown, T. H.; Morrison, S. F. Neuroregeneration and plasticity: A review ofphysiological mechanisms. Journal of Neuroscience Research 2020, 98(3), 456–478. [Google Scholar]
- Martinez-López, R.; Ferreira, J. Efficacy and safety of stem cell therapy incerebral palsy: A systematic review and meta-analysis. Stem Cell Research & Therapy 2022, 13(1), 124. [Google Scholar]
- European Medicines Agency. Guideline for regenerative medicine products; EMAPublication, 2020. [Google Scholar]
- U.S. Food and Drug Administration. Guidance for industry: Xenotransplantation. FDA Publication, 2020. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



