
Submitted:
09 February 2026
Posted:
10 February 2026
You are already at the latest version
Abstract
Management of ventricular tachycardia (VT) requires an integrated approach combining invasive therapy and cardiac imaging. This article reviews the principal imaging modalities and their integration with electroanatomical mapping systems to plan and guide procedures and to assess the success of VT ablation during follow-up. The central role of imaging in optimizing the efficacy and safety of VT ablation is emphasized. Studies demonstrating that imaging-supported workflows can improve substrate localization, reduce procedural times and radiation exposure, and lower recurrence rates are highlighted. Current limitations and future challenges are also discussed.
Keywords:
ventricular tachycardia
; catheter ablation
; cardiac magnetic resonance
; cardiac computed tomography
; intracardiac echocardiography
; PET
; SPECT
; electroanatomical mapping
; image integration
; myocardial scar
; substrate ablation
1. Introduction
Ventricular tachycardia (VT) is a major cause of morbidity and mortality in patients with structural heart disease, including post-infarction ischaemic cardiomyopathy, non-ischaemic cardiomyopathies and conditions characterized by an arrhythmogenic phenotype. In these settings, VT is frequently associated with appropriate implantable cardioverter-defibrillator (ICD) therapies, recurrent episodes and episodes of “VT storm,” all of which negatively affect quality of life, accelerate heart failure progression and increase hospital readmissions, ultimately leading to higher medium- to long-term mortality [1] (PMID: 36017572; DOI: ).
In recent years, catheter ablation has assumed an increasingly central role in the management of ventricular arrhythmias, particularly when antiarrhythmic drug therapy is ineffective or poorly tolerated, or when arrhythmia recurs despite ICD implantation. Contemporary consensus documents and clinical guidelines support the use of catheter ablation within strategies aimed at reducing arrhythmic burden and ICD shocks in selected patient populations [1,2].
Randomized clinical trials have demonstrated that catheter ablation reduces arrhythmic burden and improves quality of life compared with escalation of pharmacological therapy in patients with ischaemic heart disease and sustained VT, thereby consolidating its role within the therapeutic pathway [3].
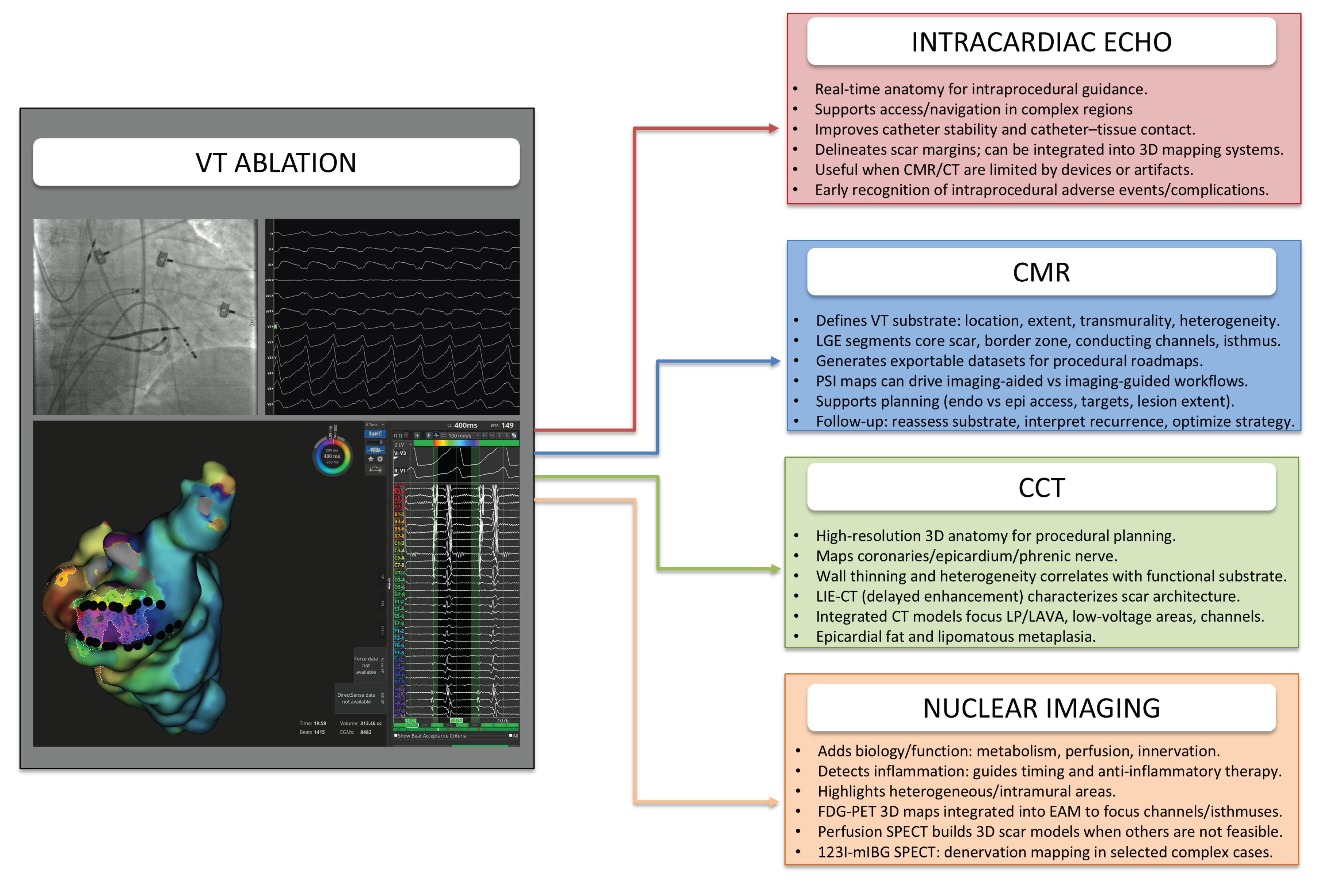
Figure 1.
Multimodality imaging support for ventricular tachycardia (VT) ablation. The left panel shows a typical VT ablation workflow (fluoroscopy, ECG/EGMs and electroanatomical mapping). The right panel summarizes how intracardiac echocardiography, cardiac magnetic resonance (CMR), cardiac computed tomography (CCT) and nuclear imaging (PET/SPECT) provide complementary information to guide mapping, target selection and procedural safety. Abbreviations:CCT: cardiac computed tomography; CCTA: coronary computed tomography angiography; CMR: cardiac magnetic resonance; EAM: electroanatomical mapping; ECG: electrocardiogram; EGM: electrogram; FDG: 18F-fluorodeoxyglucose; ICE: intracardiac echocardiography; LAVA: local abnormal ventricular activities; LGE: late gadolinium enhancement; LIE-CT: late iodine enhancement computed tomography; LP: late potentials; PET: positron emission tomography; PSI: pixel signal intensity; RF: radiofrequency; SPECT: single-photon emission computed tomography; 123I-mIBG: iodine-123 metaiodobenzylguanidine; VT: ventricular tachycardia; 3D: three-dimensional.
Figure 1.
Multimodality imaging support for ventricular tachycardia (VT) ablation. The left panel shows a typical VT ablation workflow (fluoroscopy, ECG/EGMs and electroanatomical mapping). The right panel summarizes how intracardiac echocardiography, cardiac magnetic resonance (CMR), cardiac computed tomography (CCT) and nuclear imaging (PET/SPECT) provide complementary information to guide mapping, target selection and procedural safety. Abbreviations:CCT: cardiac computed tomography; CCTA: coronary computed tomography angiography; CMR: cardiac magnetic resonance; EAM: electroanatomical mapping; ECG: electrocardiogram; EGM: electrogram; FDG: 18F-fluorodeoxyglucose; ICE: intracardiac echocardiography; LAVA: local abnormal ventricular activities; LGE: late gadolinium enhancement; LIE-CT: late iodine enhancement computed tomography; LP: late potentials; PET: positron emission tomography; PSI: pixel signal intensity; RF: radiofrequency; SPECT: single-photon emission computed tomography; 123I-mIBG: iodine-123 metaiodobenzylguanidine; VT: ventricular tachycardia; 3D: three-dimensional.
The objective of VT ablation is to render the arrhythmogenic substrate electrically inert by interrupting slow-conduction pathways and critical isthmuses through the creation of thermal lesions. However, this strategy requires a careful balance between antiarrhythmic efficacy and preservation of myocardial function. A fundamental limitation of approaches based solely on electroanatomic mapping (EAM) is the intrinsically three-dimensional nature of the arrhythmogenic substrate: voltage mapping samples only a surface and may therefore underestimate intramural or epicardial components. Furthermore, the definition of “scar” is influenced by point density, catheter–tissue contact and myocardial fibre orientation [2].
Cardiac imaging plays a pivotal role throughout the VT care pathway, enabling detailed identification and quantification of the arrhythmogenic substrate—including scar location, extent, transmurality and heterogeneity—as well as procedural planning (selection of endocardial versus epicardial approach, and assessment of coronary arteries and structures at risk), intraprocedural guidance (navigation, catheter–tissue contact and safety using echocardiography or intracardiac echocardiography) and post-procedural follow-up [4]. The most relevant imaging modalities include cardiac magnetic resonance (CMR) with late gadolinium enhancement (LGE) for fibrosis characterization and identification of conducting channels; cardiac computed tomography (CT) for high-resolution anatomical definition and procedural risk assessment; intraprocedural echocardiography for real-time guidance and early detection of complications; and positron emission tomography (PET) or single-photon emission computed tomography (SPECT) in selected cases to identify inflammatory substrates or provide complementary biological and functional information.
The integration of imaging data into EAM systems has enabled the development of “imaging-facilitated” workflows, in which preprocedural imaging roadmaps can guide electrical sampling and allow more targeted substrate modification. Available evidence suggests that imaging integration is associated with improved clinical outcomes and greater procedural efficiency, although randomized trials are ongoing to define its incremental benefit and to standardize acquisition protocols and clinical endpoints [5,6,7].
2. Multimodality Imaging in the Context of Ventricular Tachycardia Ablation
In clinical practice the choice of imaging modality depends on the scenario. CMR-LGE is preferred for tissue characterization and identification of border zone and conducting channels. CT is an alternative or complementary option when CMR is limited by devices, artifacts or electrical instability, and is valuable for procedural planning because of its higher anatomic resolution of complex structures, coronaries and the epicardium. Intraprocedural echocardiography is the cornerstone for guiding navigation, catheter–tissue contact and early recognition of complications. Nuclear imaging is reserved for selected cases requiring biological information such as active inflammation or when CMR/CT quality is inadequate [4,8].
Table 1 and Table 2 organize the main imaging modalities according to a temporal workflow framework (pre-procedural, intra-procedural, post-procedural), specifying which anatomical, functional, and tissue information each modality provides and how such information translates into procedural decisions (endo/epi planning, safety constraints, substrate targeting, and integration with EAM). The "Endpoints/metrics" column lists examples of reproducible quantitative parameters that can be used to standardize reporting and integration in planning.
2.1. Echocardiography in Ventricular Tachycardia Ablation: Current Applications
Among cardiovascular imaging modalities, echocardiography represents the first-line noninvasive tool owing to its wide availability, accessibility and cost-effectiveness. Accordingly, it remains the most widely used technique in routine clinical practice for preprocedural assessment and follow-up of patients undergoing complex invasive procedures [9].
Transthoracic 2D echocardiography (TTE) retains a central role in the management pathway of patients undergoing VT ablation, as it enables rapid characterization of ventricular size and function, assessment of right ventricular performance, and identification of structural comorbidities that may influence procedural risk and outcomes [1,10].
Catheter ablation of VT aims to reduce arrhythmic burden by rendering the arrhythmogenic substrate electrically inert through the creation of thermal lesions that induce coagulative necrosis and subsequent scar remodeling. Randomized studies have demonstrated an advantage of ablation over escalation of pharmacological therapy in improving quality of life and reducing clinically relevant endpoints, including death, VT storm and appropriate ICD shocks [3,11].
However, despite its goal of arrhythmic stabilization, VT ablation carries the potential risk of depressing ventricular function by replacing viable contractile myocardium with scar tissue. Heart failure is indeed a recognized complication of recurrent VT, with an incidence that can exceed 10% per year [2,12].
Heart failure and progressive ventricular dysfunction are associated with long-term mortality rates of 10–20% in patients undergoing VT ablation [13,14]. For this reason, systematic monitoring of cardiac function is essential during follow-up. Left ventricular ejection fraction (LVEF) remains a key prognostic indicator, and its reduction is associated with an increased risk of haemodynamic instability and adverse outcomes, including VT recurrence, major procedural complications and mortality [15,16].
Dedicated echocardiographic pre- and post-ablation studies have evaluated the impact of procedural “lesion burden” on left ventricular function and, in selected subgroups, on right ventricular performance. These investigations have shown that changes in echocardiographic parameters carry both clinical and prognostic significance [17,18,19].
Three-dimensional (3D) echocardiography, when available, enables more accurate quantification of ventricular volumes and ejection fraction by reducing geometric assumptions, thereby supporting a more objective and less operator-dependent follow-up, particularly in patients with advanced ventricular remodelling [10,20].
In addition, 3D echocardiography serves as a practical adjunct to the ablation procedure in specific scenarios, such as arrhythmias originating from papillary muscles, mobile intracavitary structures and intrinsically three-dimensional targets. By providing a more intuitive spatial representation of anatomical relationships and complex endocavitary structures, transthoracic 3D echocardiography can assist in localizing arrhythmia origin and monitoring catheter positioning, offering a low-cost intraprocedural orientation tool in laboratories without access to advanced dedicated imaging systems [21]. More recent evidence has confirmed the feasibility of integrating TTE and 3D reconstruction strategies in papillary muscle arrhythmias to support procedural planning and execution [22].
Alongside conventional TTE, speckle-tracking strain analysis extends myocardial mechanical assessment beyond ejection fraction, allowing sensitive detection of subclinical dysfunction and dyssynchrony features that are closely linked to susceptibility to ventricular arrhythmias [23].
In this context, strain parameters have been associated with recurrence-free survival following ventricular arrhythmia ablation, supporting their role in longitudinal follow-up [24]. This association has been confirmed in recent analyses using hard clinical endpoints, identifying strain-derived metrics as predictors of recurrence-free survival (recurrence and mortality) after ablation in patients with structural heart disease [24]. In particular, reduced global longitudinal strain (GLS) is associated with a higher risk of ventricular arrhythmias and appropriate ICD therapies [23,25].
In patients with idiopathic ventricular arrhythmias, longitudinal studies indicate that strain analysis can detect temporal changes in myocardial function even in the absence of a conventional scar substrate [26]. Regional strain assessment may further aid in localizing and quantifying areas of potential arrhythmogenic substrate, showing correlation with regions identified on electroanatomic mapping (EAM) and, in selected cases, assisting procedural planning and identification of ablation targets [23,27].
For VT ablation, intraprocedural echocardiographic imaging can provide direct support to the ablation workflow, complementing electroanatomic mapping and fluoroscopy by defining anatomy in real time, monitoring catheter–tissue contact, and enabling early recognition of procedural complications [2,4].
With respect to transesophageal echocardiography (TEE), its role in VT ablation is primarily related to intraprocedural monitoring during radiofrequency energy delivery. High-resolution visualization enables verification of catheter position and identification of indirect signs of energy-related complications, such as tissue overheating, making it useful in selected scenarios requiring close surveillance [28].
Intracardiac echocardiography (ICE) currently represents the most relevant echocardiographic modality in the electrophysiology laboratory for VT ablation, as it combines procedural guidance with “substrate support.” ICE provides real-time imaging of cardiac anatomy, facilitates access and navigation in anatomically challenging regions (for example, endocavitary structures and papillary muscles), optimizes catheter stability and tissue contact, and enables delineation of scar margins through integration with three-dimensional mapping systems [29,30]. Clinical studies focusing on papillary muscle arrhythmias have demonstrated that protocols combining ICE and image integration allow systematic imaging-guided mapping and ablation—using both radiofrequency and cryoenergy—thereby supporting a more controlled and reproducible approach in anatomically complex substrates [31,32]. Recent reviews have further synthesized the role of ICE in identifying arrhythmogenic substrate and integrating imaging into mapping strategies, particularly when CMR or CT are limited by device-related artifacts or contraindications [33,34].
2.2. Cardiac Magnetic Resonance in Ventricular Tachycardia Ablation: Current Applications
In recent years, CMR has rapidly advanced as a multiparametric technique increasingly integrated into cardiovascular clinical practice and, in many centers, has become a standard of care [35,36].
In electrophysiology, this technological progress has directly impacted the management of VT. CMR is now a pillar of imaging-facilitated pathways, particularly to define the substrate and to guide the procedure via integration with electroanatomic mapping systems [4,8]. Technically, a “VT-oriented” CMR is designed to provide a robust anatomical–functional baseline and an exportable LGE dataset for the lab, creating a procedural roadmap.
In clinical practice, CMR can be integrated into every phase of the ablation pathway: before the procedure it helps define the etiology and the arrhythmogenic substrate (location and extent of scar and heterogeneous tissue); during the procedure, by exporting and integrating data with electroanatomic mapping systems, it supports planning and makes the interventional strategy more efficient (choice of endocardial/epicardial access, target selection, definition of lesion extent); after the procedure, it permits assessment of outcome and detection of possible arrhythmic recurrences [37,38,39]
The protocol acquisition typically begins with cine BSSFP (balanced steady-state free precession) sequences in short-axis and long-axis planes (two, three and four chamber) to assess biventricular volumes and function, segmental wall motion abnormalities, and to identify structural findings relevant to VT such as aneurysms, wall thinning, or remodeling areas [2].
This phase is essential to localize the arrhythmogenic substrate, guide the choice of epicardial versus endocardial approach, and to interpret subsequent LGE assessment. Gadolinium (0.1–0.2 mmol/kg) is then administered and, after about 10–15 minutes, LGE sequences are acquired to define and segment myocardial scar in a manner useful for the procedure. LGE analysis specifically aims to distinguish the core scar, dense, non excitable fibrosis, the border zone, or gray zone, heterogeneous tissue with islands of viable myocardium associated with slow conduction and re-entry circuits, and conduction channels along the scar margins where critical isthmuses are often located [37]. The most commonly used sequences are 2D inversion-recovery gradient-echo (2D IR-GRE) and PSIR (phase-sensitive IR). In the VT setting (arrhythmia, frequent extrasystoles, rhythm variability, unstable patients), a clean, reproducible LGE increases the reliability of subsequent segmentation and integration into mapping, reducing the risk of an incorrect roadmap that could lead to misleading interpretations or procedural decisions. Therefore, PSIR is often preferred because it is more robust when the TI (inversion time) of 2D IR-GRE is not perfectly set [40]. In VT-experienced centers, the use of 3D navigator gated LGE (respiratory navigator) is increasing, as it provides higher resolution and 3D reconstructions useful for integration with mapping and for facilitating identification of critical isthmuses [41].
In patients with limited breath-hold capacity or complex triggering, free-breathing LGE with motion correction (MOCO) is increasingly used; it can improve acquisition robustness in “vulnerable” populations and reduce motion/rhythm instability artifacts [42,43]. In advanced workflows, dark-blood LGE may also be considered to enhance scar-to-blood contrast and sharpen scar borders, which can aid delineation and segmentation—particularly when visualization of the subendocardium is critical [44]. Additional information can be obtained with T1/T2 mapping to characterize the substrate and the stage of the pathological process. T1 mapping and ECV (extracellular volume) are particularly useful in cases of diffuse fibrosis where the substrate may be patchy, intramural, or disorganized as in nonischemic cardiomyopathies (NICM). T2 mapping detects edema and inflammation, so it plays a key role in forms where inflammatory activity may contribute to the arrhythmic phenotype. It is also useful in early post-ablation follow-up to help distinguish acute changes (edema) from more stable lesions (ablation scar). In patients with CIEDs, 1.5T scanners and dedicated wide-band sequences are preferred to minimize device-related artifacts [45].
The practical application of LGE information is integration of preprocedural acquisitions into the mapping to enable a more focused procedure and better outcomes, and its prognostic value because scar characteristics correlate with outcomes and recurrence risk. Pixel signal intensity (PSI) maps convert LGE-CMR into a 3D ventricular map with colors characterizing the arrhythmogenic substrate: signal intensity is quantified and segmented to separate core scar, border zone and relatively healthy myocardium. Within imaging-facilitated workflows, it is useful to distinguish between a CMR-aided and a CMR-guided approach. Nello specifico, le procedure CMR-aided importano i dati nel sistema di navigazione per focalizzare il mapping e migliorare l’interpretazione dell’EGM, ma i target sono definiti prevalentemente da criteri elettrofisiologici; nel caso delle procedure CMR-guided l’imaging definita dalle PSI maps diventa il driver primario della strategia di substrate ablation, con un mapping elettroanatomico potenzialmente più circoscritto alle aree a maggiore probabilità di istmo [46].
Recent studies show that preprocedural PSI maps feasibly and safely guide substrate targeting and are associated with marked reductions in procedural times (procedure, fluoroscopy, and RF), higher post-ablation non-inducibility, and survival rates around 90% with VT recurrence-free survival around 75% [5,46].
Postprocedurally, CMR can be widely used in follow-up to reassess the substrate in cases of recurrence and to plan targeted redo procedures [6,45,47]. In addition, post-ablation CMR may serve as a surrogate procedural endpoint, since reduction of conducting channels identified on LGE has been shown to associate with lower recurrence risk.
In conclution, “VT-oriented” CMR enables preprocedural assessment for etiologic definition, substrate quantification and risk stratification; intraprocedural support to generate roadmaps and color (PSI) maps integrable into EAM and a postprocedural role to evaluate substrate effects, interpret recurrences, and optimize redo strategy [4,5,6].
2.3. Cardiac Computed Tomography CT in Ventricular Tachycardia Ablation: Current Applications
Multidetector cardiac CT (CCT/CCTA) is an increasingly relevant periprocedural imaging modality because it combines high-resolution three-dimensional anatomical reconstruction of cardiac structures with detailed visualization of adjacent anatomy—most notably the coronary arteries—and, using dedicated protocols, characterization of pathological substrate and critical regions such as wall thinning, calcifications and epicardial fat [48]. When integrated with the electrical features derived from electroanatomic mapping (EAM), these anatomical and structural data play an established role in VT ablation procedures [49].
In clinical practice, ECG-gated acquisition with an angiographic phase is performed to enable comprehensive anatomical assessment. Dedicated software allows detailed evaluation of cardiac chambers, endocardial surfaces, great vessels, coronary arteries, epicardial fat and the phrenic nerve. This information supports procedural planning, including selection of an endocardial versus epicardial approach and anticipation of ablation applications in proximity to the coronary arteries [4,50].
In this context, the iodinated contrast load for standard CCTA is commonly expressed as iodine dose (mgI/kg), with recommended ranges of approximately 245–370 mgI/kg and injection durations typically between 10 and 20 s. CT-derived wall thinning and regional thickness heterogeneity correlate with the functional arrhythmogenic substrate and can guide the identification of critical isthmuses and local abnormal ventricular activities (LAVA), supporting the rationale for CT segmentation and registration within EAM systems [51].
A delayed acquisition phase may subsequently be added using late iodine enhancement or delayed enhancement CT (LIE-CT) protocols, which employ a higher iodinated contrast load to highlight fibrotic substrate, in analogy with late gadolinium enhancement CRM imaging (LGE-CMR) [52,53]. In these protocols, iodinated contrast doses of approximately 550–660 mgI/kg are administered, with image acquisition performed 7–15 minutes after injection and processed using dedicated post-processing software. Late-phase images enable characterization of myocardial architecture and delineation of scar substrate [54].
These scar and border-zone models can then be integrated into the mapping system to focus the search for late potentials, LAVA, low-voltage regions and potential conduction channels. This integration supports strategic procedural decisions—including the extent of mapping, the need for combined endocardial–epicardial access and prioritization of ablation targets—with the aim of improving procedural efficiency [6].
Concurrently, CT enables detailed mapping of epicardial fat, facilitating accurate interpretation of epicardial low-voltage areas by distinguishing voltage attenuation due to fat from true scar-related low voltage. CT can also identify lipomatous metaplasia, a pattern increasingly recognized as a relevant imaging marker for localization of functional substrate in scar-related VT and potentially involved in the stabilization of conduction corridors [55,56,57].
Integration of LIE-CT–derived models has been associated with shorter mapping times, reduced fluoroscopy exposure and improved identification of complex intramural and epicardial scar components, facilitating both bipolar and epicardial ablation strategies. However, the impact of this approach on long-term clinical outcomes remains inconclusive and warrants further prospective investigation [54,58].
In post-procedural follow-up, CT is not routinely employed to document ablation lesions. Nevertheless, it represents a highly valuable problem-oriented modality when clarification of complications or structural abnormalities is required and cannot be achieved by echocardiography alone [59].
Specifically, CT can be used to evaluate pericardial complications—including pericardial effusion, hemopericardium and cardiac tamponade—as well as to identify rare structural complications such as myocardial perforation, pseudoaneurysm formation, pleuro-pulmonary complications, phrenic nerve injury and oesophageal lesions. In addition, CT is useful for assessment of vascular access-site complications and for excluding iatrogenic coronary injury (spasm, stenosis, dissection or thrombosis) in the presence of chest pain, electrocardiographic changes or biomarker elevation [60,61].
2.4. Nuclear Imaging (PET/SPECT) in Ventricular Tachycardia Ablation: Current Applications
Within imaging-facilitated pathways for VT ablation, nuclear imaging plays a complementary role alongside echocardiography, CMR and CT. As it is not primarily an anatomical technique, nuclear imaging provides functional and biological characterization of the arrhythmogenic substrate, including myocardial metabolism, perfusion and innervation. Positron emission tomography (PET) and single-photon emission computed tomography (SPECT) enable detection of inflammatory activity, thereby informing the timing of ablation and the initiation or optimization of anti-inflammatory therapy. In addition, these modalities can help characterize heterogeneous or intramural substrate components that may be incompletely sampled by electroanatomic mapping. In this context, nuclear imaging supports a more targeted therapeutic strategy—such as immunosuppression, catheter ablation, or a combined approach—tailored to the underlying pathophysiology [4].
FDG-PET is primarily used in the preprocedural phase when an inflammatory arrhythmogenic substrate is suspected, as in cardiac sarcoidosis, myocarditis or cardiomyopathies with an inflammatory and arrhythmogenic phenotype [62]. The technique relies on the tracer 18F-fluorodeoxyglucose (FDG), whose myocardial uptake reflects glucose transporter activity; focal FDG uptake is interpreted as a marker of active inflammation. This information can assist in determining the underlying aetiology, guiding decisions to intensify or optimize anti-inflammatory therapy, and informing the timing of ablation, thereby avoiding procedures during phases of active inflammation that may be ineffective or excessively injurious [59].
In the specific setting of cardiac sarcoidosis—a high-risk condition—assessment of disease activity is of major clinical importance for diagnosis, risk stratification and longitudinal follow-up. Accordingly, FDG-PET plays a central role in guiding personalized, disease-specific management strategies, including initiation and monitoring of immunosuppressive therapy when indicated [63,64]. Beyond inflammatory assessment, PET imaging can also contribute to definition of the arrhythmogenic substrate through three-dimensional reconstructions that may be integrated into electroanatomic mapping systems to focus the search for border zones, conduction channels and critical isthmuses [65,66]. FDG-PET–based 3D maps have demonstrated spatial correlation with low-voltage regions, conduction channels and VT exit sites, supporting the use of this modality to guide ablation in selected, complex cases [67].
Myocardial perfusion SPECT can similarly be used to generate three-dimensional scar models for integration with electroanatomic mapping [68,69]. Its principal limitation is lower spatial resolution compared with CMR, CT and PET. Consequently, SPECT is generally reserved for situations in which other imaging modalities are contraindicated or unavailable, image quality is suboptimal, implanted devices generate prohibitive artifacts, or when a rapidly accessible assessment of myocardial perfusion is required [68]. A more advanced but less widely available application is 123I-mIBG SPECT, which can be used in specialized centers to identify regions of sympathetic denervation. These regions often extend beyond electrically defined scar and may be implicated in arrhythmia initiation, thereby providing complementary substrate information in complex cases [70].
3. Imaging Integration with Electroanatomical Mapping in Ventricular Tachycardia Ablation: Current Applications
Identifying targets for VT ablation is essential to perform an effective, personalized procedure. Critical areas can be found by creating an activation map during the tachycardia. This approach is the most direct way to locate isthmuses, diastolic signals, and the circuit exit. When the VT is sufficiently stable, the activation map can be combined with entrainment maneuvers, which involve pacing at a slightly faster rate than the tachycardia to “capture” and reset the circuit [71]. However, this approach requires inducing and keeping the arrhythmia stable for the whole mapping phase. In clinical practice this is often limited by hemodynamic intolerance, which can make it difficult or impossible to complete mapping during tachycardia and to reliably interpret entrainment maneuvers [72]. For this reason, ablation is often guided by substrate-mapping strategies performed in sinus rhythm or during pacing. These include voltage mapping, identification of late potentials, and detection of LAVA (local abnormal ventricular activities) [73]. Voltage mapping in sinus rhythm or during pacing, using bipolar signals and, when helpful, unipolar signals, is useful to define the scar by identifying the core scar and the border zone. After that, the operator searches for abnormal electrograms that suggest areas that are still excitable but have slow and disorganized conduction, which can promote reentry.
These electrograms include late potentials, multicomponent signals, and LAVA, which indicate abnormal, high-frequency activity inside or at the edges of the scar [74]. Treatment is then targeted to these areas because eliminating these abnormal activities as an electrophysiological endpoint of substrate inactivation is linked to better outcomes and fewer recurrences when completely removed compared with when they persist [75].
A known limitation of strategies based only on voltage and abnormal electrograms is that they can mix truly critical signals with electrically passive scar. This happens because the arrhythmogenic substrate is inherently three-dimensional and the surface being sampled can miss intramural or epicardial components. Also, scar definition based on voltage thresholds is affected by catheter–tissue contact, fiber orientation, point density, and far-field signals, which can lead to misclassifying regions as “scar” and targeting them, or missing thin but functionally important channels. To overcome these limits and increase targeting specificity, functional approaches have been added to reveal critical channels.
DEEP mapping (decrement-evoked potentials) is a functional approach that uses an extrastimulus to selectively produce decremental behavior in abnormal local potentials. This helps identify, within the scar, signals that are truly related to slow conduction and therefore more likely to be involved in the reentry circuit [76]. A decremental response suggests tissue that is still excitable but has cycle-dependent conduction properties typical of slow-conducting channels; for this reason these signals are more informative and more specific than searching for late potentials alone when guiding identification of critical targets [77].
Along this line, there has been a need to make analysis more reproducible using annotation-independent algorithms based on electrogram features. These tools help automatically detect regions with fractionated or complex signals, reducing operator variability [78]. In intramural or deep substrates, such as septal or midwall regions, even good targeting can fail because unipolar RF lesions are not deep enough or do not cross the full thickness. Therefore, the procedure may require advanced strategies to solve the “reach” problem, including bipolar ablation (endo–epicardial or endo–endo) to increase lesion depth and transmurality, and chemical ablation with ethanol as a bailout in selected refractory cases [79,80].
Although classical strategies are effective, electroanatomic mapping alone can underestimate or incompletely characterize substrates. The practical goal of integrating imaging with EAM is to turn a preprocedural substrate characterization into a 3D roadmap that reduces mapping time, guides electrogram sampling to regions with highest likelihood of isthmus, and makes treatment more targeted when the substrate is heterogeneous, epicardial, or intramural.This need led to imaging-facilitated workflows, where CMR and/or CT are used to reconstruct the substrate in 3D and fuse it with the intraprocedural EAM geometry.
The aim is to focus electrogram sampling and make ablation more targeted [45,81]. In current workflows it is useful to distinguish between imaging-aided procedures—where imaging helps focus mapping and interpret EGM but targets are still mainly defined by electrophysiologic criteria—and imaging-guided procedures—where imaging narrows the field of action and standardizes the procedural workflow [46,82].
Integration involves segmentation of the ventricle and substrate on LGE-CMR or CT, exporting the model, registering it to the EAM model, and applying the roadmap to the navigation system (CARTO/EnSite/Rhythmia) [45,47].
Beyond simple “anatomic overlay,” imaging can influence practical decisions that help plan the procedural strategy before the patient enters the lab: selection of epicardial or endocardial access, prioritization of areas to map, interpretation of low voltages, assessment of complex anatomic structures, and planning of personalized strategies for deep or hard-to-reach substrates [81].
The key point is that roadmap-guided mapping can translate into shorter mean procedure times, reduced fluoroscopy time, more targeted RF delivery, and comparable or better outcomes in terms of procedural success and reduced recurrence [46,83].
Specifically, when the approach is well structured this is reflected in concrete parameters (duration, RF, fluoroscopy) and clinical endpoints that often lie around 70–75% VT-free survival at midterm, even in complex populations [6]. A critical caveat is imaging quality: an inaccurate roadmap can misdirect procedural focus and itself become a source of decision bias.
4. Imaging-Facilitated VT Ablation: Current Evidence, Practical Limitations, and Future Directions
The integration of advanced imaging into VT ablation has progressively shifted from a conceptual adjunct to a clinically relevant component of contemporary workflows. Beyond technical feasibility, its adoption raises critical questions regarding real-world effectiveness, methodological robustness and long-term sustainability across different clinical settings. Accordingly, the following sections synthesize the available real-world evidence supporting imaging-facilitated ablation strategies, critically examine the current methodological and practical limitations that constrain broader implementation, and outline emerging technological paradigms that may shape the future evolution of imaging-guided VT ablation.
4.1. Real-World Evidence Supporting Imaging-Facilitated Workflows
The recognized limitations of conventional VT ablation in fully capturing the complexity of the arrhythmogenic substrate have provided the rationale for systematic integration of advanced imaging into ablation workflows [84].
In this context, imaging-guided VT ablation has been associated with meaningful clinical benefit, enabling more accurate substrate characterization and greater precision in the identification of critical targets [85]. In particular, a systematic review and meta-analysis of observational studies demonstrated that preprocedural integration of scar imaging into the navigation system was associated with superior outcomes compared with procedures performed without imaging guidance, with higher VT-free survival (82% vs 59%) and overall survival (94% vs 82%) [5].
Further supporting these findings, a recent prospective multicentre registry by Penela et al. documented the feasibility of systematic imaging integration and procedural standardization, reporting favourable acute and long-term outcomes. Specifically, survival rates of 94% and arrhythmic recurrences of approximately 20% were observed, findings attributed to comprehensive three-dimensional reconstruction of the arrhythmogenic substrate [6].
Taken together, these real-world data suggest that systematic integration of advanced imaging into VT ablation workflows is associated with improved clinical outcomes. However, the predominantly observational nature of the available evidence, the heterogeneity of patient populations and procedural strategies, and the potential for selection bias underscore the need for prospective randomized studies comparing imaging-facilitated approaches with standard electroanatomic mapping (EAM)-guided ablation to define the true incremental value of imaging. Within this framework, the prospective, randomized, multicentre VOYAGE and PREVENT-VT trials are currently ongoing.
The VOYAGE trial is designed to assess whether a CMR-aided or CMR-guided ablation strategy is superior to standard EAM-guided therapy in terms of efficacy, procedural efficiency and safety, thereby evaluating imaging as an active guiding tool in VT treatment [7]. The PREVENT-VT trial extends the concept of imaging-guided ablation to the identification of high-risk arrhythmogenic substrate using advanced imaging, evaluating a prophylactic CMR-guided ablation strategy for primary prevention following myocardial infarction, based on scar structural features associated with increased arrhythmic vulnerability [86].
4.2. Current Methodological and Practical Limitations of Imaging Integration
Although imaging-facilitated workflows in VT ablation are promising, their widespread adoption remains constrained by technical, methodological and organizational challenges that limit real-world applicability [4]. Despite a growing body of evidence, the generalizability of reported results is affected by heterogeneity in patient populations and imaging protocols, as well as by variability in local technologies and expertise influencing image acquisition, post-processing and integration with EAM systems [4,59].
A major source of variability among imaging-facilitated VT ablation studies lies in cohort heterogeneity. Arrhythmia aetiology (ischaemic versus non-ischaemic) and scar architecture—including extent, transmurality, and intramural or epicardial components—substantially influence both substrate detectability on imaging and the representativeness of electrical sampling.
In non-transmural substrates or those with predominantly intramural or epicardial localization, ablation targets may be less clearly defined by conventional imaging and less completely characterized by endocardial EAM alone. In addition, in haemodynamically unstable patients, activation and entrainment mapping often play a limited role due to practical constraints, making substrate-based strategies performed in sinus rhythm relatively more central [87].
Image quality also represents a critical limitation. In patients with cardiac implantable electronic devices or in the presence of motion or arrhythmia during acquisition, artefacts may impair target definition and reduce the effectiveness of imaging-guided integration [37,88].
A further limitation arises from variability in imaging acquisition and quantification protocols, including differences in LGE sequences and spatial resolution (2D versus 3D), PSIR versus IR-GRE techniques, gating and motion correction strategies, CT reconstruction and delayed-enhancement parameters, as well as segmentation criteria and software platforms. These factors directly affect scar and border-zone estimation and the reconstruction of conduction channels and corridors [89].
Challenges related to image-to-mapping fusion further compound this variability. Registration errors may result from the registration technique itself, from changes in ventricular geometry between imaging and the procedure, or from cardiac and respiratory motion. Given that critical isthmuses may measure only a few millimetres, even small mismatches can have clinically relevant consequences [90].
Moreover, the effectiveness of imaging integration is highly dependent on local expertise and procedural standardization. To generate truly “VT-oriented” datasets suitable for seamless import into EAM systems, a dedicated workflow is required, encompassing tailored acquisition protocols, quality control, segmentation, and iterative alignment using anatomical landmarks and mapping meshes. Differences among imaging software and EAM platforms can introduce further mismatches and increase inter-centre variability, limiting the broader applicability of results reported by highly specialized centres [4,81].
Finally, even when technically feasible, advanced imaging protocols entail non-negligible costs, time investment and organizational burden, including acquisition, post-processing, dedicated personnel, specialized software and in-lab integration. These factors represent a significant barrier to systematic implementation. To promote wider adoption, simplified and reproducible operational pathways are needed, supported by robust cost-effectiveness analyses, to ensure that advanced imaging does not remain confined to a limited number of high-resource centres [4,59].
4.3. Future Challenges and Emerging Paradigms
Current limitations related to data quality, standardization and transferability in imaging-facilitated VT ablation may be mitigated by emerging technologies aimed at making imaging–EAM integration more automated, robust and less operator-dependent. These advances have the potential to substantially improve procedural efficiency and inter-centre reproducibility [4,91].
Artificial intelligence is already reshaping imaging-based workflows. Beyond accelerating segmentation and post-processing, AI is increasingly entering the intraprocedural domain through tools capable of automating geometry generation and anatomical reconstruction directly within the mapping system. A representative example, already established in atrial fibrillation ablation workflows, is CARTOSOUND FAM, which integrates deep-learning modules with intracardiac echocardiography to generate three-dimensional reconstructions without manual segmentation or contour annotation, thereby reducing operator-dependent variability and procedural duration [92,93,94].
In the ventricular setting, clinical evidence supporting analogous AI-driven modules remains limited; however, the potential impact is substantial given the anatomical complexity of the ventricles and the sensitivity of ablation targeting to even small reconstruction or registration errors [95].
In parallel, intracardiac echocardiography is evolving toward four-dimensional solutions and tighter integration with EAM platforms, enabling multiplanar imaging and volumetric acquisition with minimal catheter manipulation. These developments aim to improve navigation and ablation precision in complex three-dimensional structures such as papillary muscles and intracavitary targets. Preclinical studies using NuVision NAV support the feasibility of accurate electroanatomic reconstruction and more controlled energy delivery, suggesting potential gains in procedural safety and efficiency [96].
Another emerging paradigm is the transition from static anatomical roadmaps to predictive tools based on patient-specific models and so-called “digital twins,” which integrate imaging data with computational simulation to estimate arrhythmogenic circuits, vulnerability and optimal ablation targets. This approach may reduce uncertainty in target selection, particularly in non-ischaemic and intramural substrates; however, widespread clinical adoption will require high-quality standardized datasets and rigorous external validation against meaningful clinical endpoints [97].
Real-time intraprocedural CMR represents a potential paradigm shift by enabling direct visualization of anatomy, catheter contact and tissue injury during energy delivery. First-in-human studies have demonstrated feasibility, raising the prospect of monitoring lesion formation in real time and defining tissue-based procedural endpoints rather than relying solely on electrical surrogates [98].
Advances in CT technology, such as late-enhancement photon-counting CT, may further expand access to myocardial tissue characterization when CMR is limited, facilitating substrate models that can be integrated into EAM systems and potentially promoting more homogeneous real-world practice if validated by comparative and outcome-driven studies [99].
Finally, in selected refractory cases, non-invasive radioablation using stereotactic arrhythmia radioablation (STAR/SBRT) is consolidating as an emerging therapeutic option based on multimodal target definition. Further prospective studies are required to clarify optimal timing, patient selection and long-term safety [100].
5. Conclusions
Ventricular tachycardia (VT) in patients with structural heart disease represents a high-impact clinical problem, characterized by recurrences, appropriate ICD therapies, and arrhythmic storms, associated with recurrent hospitalizations, worsening heart failure, and increased mortality risk. Therefore, structured and multidisciplinary management is essential to optimize outcomes [2].
In this scenario, multimodal cardiac imaging serves as a fundamental support in the contemporary management of VT ablation, as it allows for a more comprehensive and three-dimensional characterization of the arrhythmic substrate compared to solely using electroanatomical mapping (EAM). This has an impact on patient selection, planning, intraprocedural safety, and substrate ablation strategy [4].
Available clinical evidence suggests that imaging-facilitated workflows, with the pre-procedural integration of imaging into the navigation system, may reduce procedural times and fluoroscopy exposure while being associated with better clinical outcomes. However, most data comes from observational studies and registries, showing methodological heterogeneity and dependence on acquisition quality, segmentation, and registration.
Assessing the true incremental contribution of imaging compared to standard EAM-guided approaches requires randomized, prospective, multicentric studies and more rigorous standardization of protocols. In this context, ongoing trials (VOYAGE and PREVENT-VT) represent essential steps to clarify the efficacy, safety, and efficiency of imaging-guided workflows [86].
In the near future, automation and artificial intelligence applied to segmentation, registration, integration, and more robust tissue imaging technologies could make imaging-guided pathways more reproducible and accessible, accelerating the transition toward more targeted, safe, and personalized procedures.
Abbreviations
The following abbreviations are used in this manuscript:
| VT | Ventricular tachycardia |
| ICD | Implantable cardioverter-defibrillator |
| EAM | Electroanatomical mapping (o electroanatomic mapping) |
| CMR | Cardiac magnetic resonance |
| LGE | Late gadolinium enhancement |
| CT / CCTA | Computed tomography / Coronary CT angiography |
| PET | Positron emission tomography |
| SPECT | Single-photon emission computed tomography |
| PSI | Pixel signal intensity (PSI maps) |
| TTE | Transthoracic echocardiography |
| TEE | Transesophageal echocardiography |
| ICE | Intracardiac echocardiography |
| FDG | (18)F-fluorodeoxyglucose (FDG-PET tracer) |
| 123I-mIBG | (123)I-metaiodobenzylguanidine (SPECT tracer) |
| LIE-CT / DE-CT | Late iodine enhancement / Delayed enhancement CT |
| LVEF | Left ventricular ejection fraction |
| LVEDV / LVESV | Left ventricular end-diastolic / end-systolic volume |
| RVEF | Right ventricular ejection fraction |
| WMA | Wall motion abnormalities |
| GLS | Global longitudinal strain |
| RF | Radiofrequency |
| BSSFP | Balanced steady-state free precession |
| IR-GRE | Inversion-recovery gradient-echo |
| PSIR | Phase-sensitive inversion recovery |
| MOCO | Motion correction (free-breathing LGE MOCO) |
| T1 / T2 / ECV | T1 mapping / T2 mapping / Extracellular volume |
| CIEDs | Cardiac implantable electronic devices |
| LAVA | Local abnormal ventricular activities |
| DEEP | Decrement-evoked potentials |
| EGM | Electrogram (EGM/EGMs) |
| STAR / SBRT | Stereotactic arrhythmia radioablation / Stereotactic body radiotherapy |
| AI | Artificial intelligence |
| SUV | Standardized uptake value |
| H/M ratio | Heart-to-mediastinum ratio (nel 123I-mIBG) |
References
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Cronin, E.M.; Bogun, F.M.; Maury, P.; Peichl, P.; Chen, M.; Namboodiri, N.; Aguinaga, L.; Leite, L.R.; Al-Khatib, S.M.; Anter, E.; et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Europace 2019, 21, 1143–1144. [Google Scholar] [CrossRef]
- Sapp, J.L.; Wells, G.A.; Parkash, R.; Stevenson, W.G.; Blier, L.; Sarrazin, J.F.; Thibault, B.; Rivard, L.; Gula, L.; Leong-Sit, P.; et al. Ventricular tachycardia ablation versus escalation of antiarrhythmic drugs. N. Engl. J. Med. 2016, 375, 111–121. [Google Scholar] [CrossRef]
- Chery, G.; Khoshknab, M.; Nazarian, S. Imaging to facilitate ventricular tachycardia ablation: Intracardiac echocardiography, computed tomography, magnetic resonance, and positron emission tomography. JACC Clin. Electrophysiol. 2024, 10, 2277–2292. [Google Scholar] [CrossRef]
- Hendriks, A.A.; Kis, Z.; Glisic, M.; Bramer, W.M.; Szili-Torok, T. Pre-procedural image-guided versus non-image-guided ventricular tachycardia ablation-a review. Neth. Heart J. 2020, 28, 573–583. [Google Scholar] [CrossRef]
- Penela, D.; Falasconi, G.; Soto-Iglesias, D.; Fernández-Armenta, J.; Zucchelli, G.; Bisbal, F.; Zaraket, F.; Silva, E.; Parollo, M.; Latini, A.C.; et al. Outcomes of ventricular tachycardia ablation facilitated by pre-procedural cardiac imaging-derived scar characterization: a prospective multi-centre international registry. Europace 2025, 27. [Google Scholar] [CrossRef]
- Lilli, A.; Parollo, M.; Mazzocchetti, L.; De Sensi, F.; Rossi, A.; Notarstefano, P.; Santoro, A.; Aquaro, G.D.; Cresti, A.; Lapira, F.; et al. Ventricular tachycardia ablation guided or aided by scar characterization with cardiac magnetic resonance: rationale and design of VOYAGE study. BMC Cardiovasc. Disord. 2022, 22, 169. [Google Scholar] [CrossRef] [PubMed]
- Di Cori, A.; Pistelli, L.; Parollo, M.; Zaurino, N.; Segreti, L.; Zucchelli, G. Approaching ventricular tachycardia ablation in 2024: An update on mapping and ablation strategies, timing, and future directions. J. Clin. Med. 2024, 13, 5017. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.D.; Mann, R.D.; Kristenson, S.D.; Buck, R.M.; Mendoza, J.D.; Reese, J.M.; Grant, D.W.; Roberge, E.A. Transthoracic echocardiography: Beginner’s guide with emphasis on blind spots as identified with CT and MRI. Radiographics 2021, 41, 1022–1042. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Barkagan, M.; Leshem, E.; Shapira-Daniels, A.; Sroubek, J.; Buxton, A.E.; Saffitz, J.E.; Anter, E. Histopathological characterization of radiofrequency ablation in ventricular scar tissue. JACC Clin. Electrophysiol. 2019, 5, 920–931. [Google Scholar] [CrossRef]
- Calkins, H.; Epstein, A.; Packer, D.; Arria, A.M.; Hummel, J.; Gilligan, D.M.; Trusso, J.; Carlson, M.; Luceri, R.; Kopelman, H.; et al. Catheter ablation of ventricular tachycardia in patients with structural heart disease using cooled radiofrequency energy. J. Am. Coll. Cardiol. 2000, 35, 1905–1914. [Google Scholar] [CrossRef]
- Segal, O.R.; Chow, A.W.C.; Markides, V.; Schilling, R.J.; Peters, N.S.; Davies, D.W. Long-term results after ablation of infarct-related ventricular tachycardia. Heart Rhythm 2005, 2, 474–482. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, P.A.; Poloniecki, J.; Sosa-Suarez, G.; Ruskin, J.N.; McGovern, B.A.; Garan, H. Long-term clinical outcome of patients with prior myocardial infarction after palliative radiofrequency catheter ablation for frequent ventricular tachycardia. Am. J. Cardiol. 2001, 87, 975–979. [Google Scholar] [CrossRef]
- Santangeli, P.; Muser, D.; Zado, E.S.; Magnani, S.; Khetpal, S.; Hutchinson, M.D.; Supple, G.; Frankel, D.S.; Garcia, F.C.; Bala, R.; et al. Acute hemodynamic decompensation during catheter ablation of scar-related ventricular tachycardia: incidence, predictors, and impact on mortality. Circ. Arrhythm. Electrophysiol. 2015, 8, 68–75. [Google Scholar] [CrossRef]
- Santangeli, P.; Frankel, D.S.; Tung, R.; Vaseghi, M.; Sauer, W.H.; Tzou, W.S.; Mathuria, N.; Nakahara, S.; Dickfeldt, T.M.; Lakkireddy, D.; et al. Early mortality after catheter ablation of ventricular tachycardia in patients with structural heart disease. J. Am. Coll. Cardiol. 2017, 69, 2105–2115. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.H.; Maisel, W.H.; Ho, C.; Suzuki, M.; Soejima, K.; Solomon, S.; Stevenson, W.G. Effect of radiofrequency catheter ablation of ventricular tachycardia on left ventricular function in patients with prior myocardial infarction. J. Interv. Card. Electrophysiol. 2002, 7, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Turnbull, S.; De Silva, K.; Bhaskaran, A.; Bennett, R.G.; Campbell, T.G.; Thomas, L.; Kumar, S. Impact of catheter ablation for ventricular tachycardia on left ventricular ejection fraction in patients with structural heart disease. J. Arrhythm. 2025, 41, e70042. [Google Scholar] [CrossRef]
- Ezzeddine, F.M.; Davis, N.E.; Asirvatham, S.J.; Bois, J.P.; Chang, I.C.; Deshmukh, A.; Friedman, P.A.; Giudicessi, J.; Kapa, S.; Kowlgi, G.G.; et al. Cardiac function after catheter ablation of ventricular arrhythmias in patients with arrhythmogenic right ventricular cardiomyopathy. Eur. Heart J. Open 2025, 5, oeaf049. [Google Scholar] [CrossRef]
- Surkova, E.; Muraru, D.; Genovese, D.; Aruta, P.; Palermo, C.; Badano, L.P. Relative prognostic importance of left and right ventricular ejection fraction in patients with cardiac diseases. J. Am. Soc. Echocardiogr. 2019, 32, 1407–1415.e3. [Google Scholar] [CrossRef]
- Leftheriotis, D.; Flevari, P.; Stassinos, V.; Ikonomidis, I. Transthoracic 3D echocardiography used as a low-cost and precise technique to facilitate ablation of ventricular tachycardia from the left posteromedial papillary muscle. Hellenic J. Cardiol. 2019, 60, 261–263. [Google Scholar] [CrossRef]
- Mirzeyeva, G.; Heukäufer, M.; Janschel, S.; Schneppe, D.; Ebrahimi, R.; Dörr, M.; Kiuchi, M.G.; Futyma, P.; Martinek, M.; Pürerfellner, H.; et al. 3D map combined with transthoracic echocardiography for ablation of premature ventricular contractions/ventricular arrhythmia from papillary muscle: A technical report. J. Clin. Med. 2024, 13, 6358. [Google Scholar] [CrossRef]
- Haugaa, K.H.; Smedsrud, M.K.; Steen, T.; Kongsgaard, E.; Loennechen, j.P.; Skjaerpe, T.; Voigt, J.U.; Willems, R.; Smith, G.; Smiseth, O.A.; et al. Mechanical dispersion assessed by myocardial strain in patients after myocardial infarction for risk prediction of ventricular arrhythmia. [CrossRef]
- Trivedi, S.J.; Bennett, R.G.; Byth, K.; Campbell, T.; Turnbull, S.; Stefani, L.; Kumar, S.; Thomas, L. Speckle-tracking echocardiography parameters associated with ventricular arrhythmia recurrence-free survival after ablation in structural heart disease. J. Am. Soc. Echocardiogr. 2025, 38, 820–831. [Google Scholar] [CrossRef]
- Guerra, F.; Malagoli, A.; Contadini, D.; Baiocco, E.; Menditto, A.; Bonelli, P.; Rossi, L.; Sticozzi, C.; Zanni, A.; Cai, J.; et al. Global longitudinal strain as a predictor of first and subsequent arrhythmic events in remotely monitored ICD patients with structural heart disease. JACC Cardiovasc. Imaging 2020, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, S.J.; Campbell, T.; Stefani, L.; Kumar, S.; Thomas, L. Speckle-tracking strain echocardiography in the assessment of myocardial mechanics in patients with idiopathic ventricular arrhythmias: A longitudinal follow-up study. Circ. Arrhythm. Electrophysiol. 2020, 13, e008748. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, S.J.; Campbell, T.; Davey, C.J.; Stefani, L.; Thomas, L.; Kumar, S. Longitudinal strain with speckle-tracking echocardiography predicts electroanatomic substrate for ventricular tachycardia in nonischemic cardiomyopathy patients. Heart Rhythm O2 2022, 3, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Saxon, L.A.; Stevenson, W.G.; Fonarow, G.C.; Middlekauff, H.R.; Yeatman, L.A.; Sherman, C.T.; Child, J.S. Transesophageal echocardiography during radiofrequency catheter ablation of ventricular tachycardia. Am. J. Cardiol. 1993, 72, 658–661. [Google Scholar] [CrossRef]
- Bunch, T.J.; Weiss, J.P.; Crandall, B.G.; Day, J.D.; DiMarco, J.P.; Ferguson, J.D.; Mason, P.K.; McDaniel, G.; Osborn, J.S.; Wiggins, D.; et al. Image integration using intracardiac ultrasound and 3D reconstruction for scar mapping and ablation of ventricular tachycardia. J. Cardiovasc. Electrophysiol. 2010, 21, 678–684. [Google Scholar] [CrossRef]
- Proietti, R.; Rivera, S.; Dussault, C.; Essebag, V.; Bernier, M.L.; Ayala-Paredes, F.; Badra-Verdu, M.; Roux, J.F. Intracardiac echo-facilitated 3D electroanatomical mapping of ventricular arrhythmias from the papillary muscles: assessing the ‘fourth dimension’ during ablation. Europace 2016, euw099. [Google Scholar] [CrossRef]
- Rivera, S.; de la Paz Ricapito, M.; Espinoza, J.; Belardi, D.; Albina, G.; Giniger, A.; Roux, J.F.; Ayala-Paredes, F.; Scazzuso, F. Cryoablation for ventricular arrhythmias arising from the papillary muscles of the left ventricle guided by intracardiac echocardiography and image integration. JACC Clin. Electrophysiol. 2015, 1, 509–516. [Google Scholar] [CrossRef]
- Rivera, S.; Ricapito, M.d.l.P.; Tomas, L.; Parodi, J.; Bardera Molina, G.; Banega, R.; Bueti, P.; Orosco, A.; Reinoso, M.; Caro, M.; et al. Results of cryoenergy and radiofrequency-based catheter ablation for treating ventricular arrhythmias arising from the papillary muscles of the left ventricle, guided by intracardiac echocardiography and image integration. Circ. Arrhythm. Electrophysiol. 2016, 9, e003874. [Google Scholar] [CrossRef]
- Kanawati, J.; De Silva, K.; Bhaskaran, A.; Turnbull, S.; Zhou, J.; Kotake, Y.; Kumar, S.; Campbell, T. Intracardiac echocardiography techniques to identify ventricular arrhythmia substrate. Heart Rhythm O2 2022, 3, 602–612. [Google Scholar] [CrossRef]
- Qian, P.C.; Tedrow, U.B. Intracardiac echocardiography to guide catheter ablation of ventricular arrhythmias in ischemic cardiomyopathy. Card. Electrophysiol. Clin. 2021, 13, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Simkowski, J.; Eck, B.; Tang, W.H.W.; Nguyen, C.; Kwon, D.H. Next-generation cardiac magnetic resonance imaging techniques for characterization of myocardial disease. Curr. Treat. Options Cardiovasc. Med. 2024, 26, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Barison, A.; Timoteo, A.T.; Liga, R.; Borodzicz-Jazdzyk, S.; El Messaoudi, S.; Luong, C.; Mandoli, G.E.; Moscatelli, S.; Ramkisoensing, A.A.; Moharem-Elgamal, S.; et al. Cardiovascular imaging research and innovation in 2023. Eur. Heart J. Imaging Methods Pract. 2024, 2, qyae029. [Google Scholar] [CrossRef]
- Dickfeld, T.; Tian, J.; Ahmad, G.; Jimenez, A.; Turgeman, A.; Kuk, R.; Peters, M.; Saliaris, A.; Saba, M.; Shorofsky, S.; et al. MRI-Guided ventricular tachycardia ablation: integration of late gadolinium-enhanced 3D scar in patients with implantable cardioverter-defibrillators. Circ. Arrhythm. Electrophysiol. 2011, 4, 172–184. [Google Scholar] [CrossRef]
- Sour, A.; Jenni, S.; Ortí-Suárez, A.; Schmitt, J.; Heitz, V.; Bolze, F.; Loureiro de Sousa, P.; Po, C.; Bonnet, C.S.; Pallier, A.; et al. Four gadolinium(III) complexes appended to a porphyrin: A water-soluble molecular theranostic agent with remarkable relaxivity suited for MRI tracking of the photosensitizer. Inorg. Chem. 2016, 55, 4545–4554. [Google Scholar] [CrossRef]
- Mahida, S.; Sacher, F.; Dubois, R.; Sermesant, M.; Bogun, F.; Haïssaguerre, M.; Jaïs, P.; Cochet, H. Cardiac imaging in patients with ventricular tachycardia. Circulation 2017, 136, 2491–2507. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef]
- Andreu, D.; Ortiz-Pérez, J.T.; Fernández-Armenta, J.; Guiu, E.; Acosta, J.; Prat-González, S.; De Caralt, T.M.; Perea, R.J.; Garrido, C.; Mont, L.; et al. 3D delayed-enhanced magnetic resonance sequences improve conducting channel delineation prior to ventricular tachycardia ablation. Europace 2015, 17, 938–945. [Google Scholar] [CrossRef]
- Yan, C.; Hu, J.; Li, Y.; Xie, X.; Zou, Z.; Deng, Q.; Zhou, X.; Bi, X.; Zeng, M.; Liu, J. Motion-corrected free-breathing late gadolinium enhancement combined with a gadolinium contrast agent with a high relaxation rate: an optimized cardiovascular magnetic resonance examination protocol. [CrossRef]
- Yang, K.; Cui, C.; Teng, F.; Yin, G.; An, J.; Yang, X.; Li, J.; Bi, X.; Pang, J.; Chow, K.; et al. Full free-breathing cardiovascular magnetic resonance imaging: enhancing efficiency and image quality in clinical practice. J. Cardiovasc. Magn. Reson. 2025, 27, 101955. [Google Scholar] [CrossRef]
- Holtackers, R.J.; Van De Heyning, C.M.; Chiribiri, A.; Wildberger, J.E.; Botnar, R.M.; Kooi, M.E. Dark-blood late gadolinium enhancement cardiovascular magnetic resonance for improved detection of subendocardial scar: a review of current techniques. J. Cardiovasc. Magn. Reson. 2021, 23, 96. [Google Scholar] [CrossRef]
- Andreu, D.; Berruezo, A.; Ortiz-Pérez, J.T.; Silva, E.; Mont, L.; Borràs, R.; de Caralt, T. Integration of 3D electroanatomic maps and magnetic resonance scar characterization into the navigation system to guide ventricular tachycardia ablation. [CrossRef]
- Soto-Iglesias, D.; Penela, D.; Jáuregui, B.; Acosta, J.; Fernández-Armenta, J.; Linhart, M.; Zucchelli, G.; Syrovnev, V.; Zaraket, F.; Terés, C.; et al. Cardiac magnetic resonance-guided ventricular tachycardia substrate ablation. JACC Clin. Electrophysiol. 2020, 6, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Armenta, J.; Berruezo, A.; Andreu, D.; Camara, O.; Silva, E.; Serra, L.; Barbarito, V.; Carotenutto, L.; Evertz, R.; Ortiz-Pérez, J.T.; et al. Three-dimensional architecture of scar and conducting channels based on high resolution ce-CMR: insights for ventricular tachycardia ablation. [CrossRef] [PubMed]
- Burger, J.C.; Hopman, L.H.G.A.; Kemme, M.J.B.; Hoeksema, W.; Takx, R.A.P.; Figueras I Ventura, R.M.; Campos, F.O.; Plank, G.; Planken, R.N.; Allaart, C.P.; et al. Optimizing ventricular tachycardia ablation through imaging-based assessment of arrhythmic substrate: A comprehensive review and roadmap for the future. Heart Rhythm O2 2024, 5, 561–572. [Google Scholar] [CrossRef] [PubMed]
- Englert, F.; Bahlke, F.; Erhard, N.; Krafft, H.; Popa, M.A.; Risse, E.; Lennerz, C.; Lengauer, S.; Telishevska, M.; Reents, T.; et al. VT ablation based on CT imaging substrate visualization: results from a large cohort of ischemic and non-ischemic cardiomyopathy patients. Clin. Res. Cardiol. 2024, 113, 1478–1484. [Google Scholar] [CrossRef]
- Arya, A.; Di Biase, L.; Bazán, V.; Berruezo, A.; d’Avila, A.; Della Bella, P.; Enriquez, A.; Hocini, M.; Kautzner, J.; Pak, H.N.; et al. Epicardial ventricular arrhythmia ablation: a clinical consensus statement of the European Heart Rhythm Association of the European Society of Cardiology and the Heart Rhythm Society, the Asian Pacific Heart Rhythm Society, the Latin American Heart Rhythm Society, and the Canadian Heart Rhythm Society. Europace 2025, 27. [Google Scholar]
- Maher, T.R.; Freedman, B.L.; Locke, A.H.; Tracey, M.; Waks, J.W.; Litmanovich, D.; d’Avila, A. Correlation between functional substrate mapping and cardiac computed tomography-derived wall thinning for ventricular tachycardia ablation. JACC Clin. Electrophysiol. 2023, 9, 1878–1889. [Google Scholar] [CrossRef]
- Liu, P.; Lin, L.; Xu, C.; Han, Y.; Lin, X.; Hou, Y.; Lu, X.; Vembar, M.; Jin, Z.; Wang, Y. Quantitative analysis of late iodine enhancement using dual-layer spectral detector computed tomography: comparison with magnetic resonance imaging. Quant. Imaging Med. Surg. 2022, 12, 310–320. [Google Scholar] [CrossRef]
- Gatti, M.; De Filippo, O.; Cura Curà, G.; Dusi, V.; Di Vita, U.; Gallone, G.; Morena, A.; Palmisano, A.; Pasinato, E.; Solano, A.; et al. Diagnostic accuracy of late iodine enhancement on cardiac CT for myocardial tissue characterization: a systematic review and meta-analysis. Eur. Radiol. 2025, 35, 3054–3067. [Google Scholar] [CrossRef]
- van den Bruck. Preprocedural substrate visualization and image integration based on late enhancement computed tomography for ventricular tachycardia ablation in non-ischemic cardiomyopathy.
- Xu, L.; Khoshknab, M.; Berger, R.D.; Chrispin, J.; Dixit, S.; Santangeli, P.; Callans, D.; Marchlinski, F.E.; Zimmerman, S.L.; Han, Y.; et al. Lipomatous metaplasia enables Ventricular Tachycardia by reducing current loss within the protected corridor. JACC Clin. Electrophysiol. 2022, 8, 1274–1285. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Zahid, S.; Khoshknab, M.; Moss, J.; Berger, R.D.; Chrispin, J.; Callans, D.; Marchlinski, F.E.; Zimmerman, S.L.; Han, Y.; et al. Lipomatous metaplasia facilitates slow conduction in critical Ventricular Tachycardia corridors within postinfarct myocardium. JACC Clin. Electrophysiol. 2023, 9, 1235–1245. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Khoshknab, M.; Moss, J.; Berger, R.D.; Chrispin, J.; Callans, D.; Marchlinski, F.E.; Zimmerman, S.L.; Han, Y.; Trayanova, N.; et al. Lipomatous metaplasia is associated with ventricular tachycardia recurrence following ablation in patients with nonischemic cardiomyopathy. JACC Clin. Electrophysiol. 2024, 10, 1135–1146. [Google Scholar] [CrossRef]
- Sacristan, B.; Cochet, H.; Bouyer, B.; Tixier, R.; Duchateau, J.; Derval, N.; Pambrun, T.; Arnaud, M.; Charton, J. Imaging-aided VT ablation. Long-term results from a pilot study. [CrossRef]
- Notarstefano, P.; Ciabatti, M.; Marallo, C.; Lazzeri, M.; Fraticelli, A.; Tavanti, V.; Zucchelli, G.; La Camera, A.; Bolognese, L. The role of imaging in ventricular tachycardia ablation. Diagnostics (Basel) 1973, 2025, 15. [Google Scholar] [CrossRef]
- Kuroda, M.; Hiroshima, K.; Ando, K. Epicardial ventricular tachycardia ablation: A contemporary review of indications, techniques, and practical approaches for challenging substrates. Rev. Cardiovasc. Med. 2026, 27. [Google Scholar] [CrossRef] [PubMed]
- Russo, F.; Vella, C.; Cauti, F.M.; Romano, V.; Gamardella, M.; Ancona, M.B.; Chieffo, A.; Montorfano, M. Iatrogenic acute coronary occlusion during epicardial ventricular tachycardia ablation: when intravascular imaging guides the management-a case report. Eur. Heart J. Case Rep. 2025, 9, ytaf358. [Google Scholar] [CrossRef]
- Lameka, K.; Farwell, M.D.; Ichise, M. Positron emission tomography. In Handbook of Clinical Neurology; Handbook of Clinical Neurology; Elsevier, 2016; pp. 209–227. [Google Scholar]
- Al Taii, H.; Saxena, R.; Morcos, R.; Al-Shammari, A.S.; Farhat, K.; Al Sakini, A.S.; Al-Wssawi, A.; Gaalema, D.; Naraynan, A.; Sabayon, D.; et al. Outcomes of catheter ablation in cardiac sarcoidosis patients with ventricular tachycardia: a propensity score-matched retrospective analysis. J. Interv. Card. Electrophysiol. 2025, 68, 1171–1177. [Google Scholar] [CrossRef]
- Hashimoto, K.; Turnbull, S.; Bickley, M.; Bhaskaran, A.; Huang, K.; De Silva, K.; Kumar, S. Clinical outcomes after catheter ablation in cardiac sarcoidosis and idiopathic nonischemic cardiomyopathy. J. Cardiovasc. Electrophysiol. 2025, 36, 1913–1923. [Google Scholar] [CrossRef] [PubMed]
- Dickfeld, T.; Lei, P.; Dilsizian, V.; Jeudy, J.; Dong, J. Integration of three-dimensional scar maps for ventricular tachycardia ablation with positron emission tomography-computed tomography. [CrossRef] [PubMed]
- Fahmy, T.S.; Wazni, O.M.; Jaber, W.A.; Walimbe, V.; Di Biase, L.; Elayi, C.S.; DiFilippo, F.P.; Young, R.B.; Patel, D.; Riedlbauchova, L.; et al. Integration of positron emission tomography/computed tomography with electroanatomical mapping: a novel approach for ablation of scar-related ventricular tachycardia. Heart Rhythm 2008, 5, 1538–1545. [Google Scholar] [CrossRef]
- Ghzally, Y.; Imanli, H.; Smith, M.; Mahat, J.; Chen, W.; Jimenez, A.; Sawan, M.A.; Abdelmegid, M.A.K.F.; Helmy, H.A.E.R.; Demitry, S.; et al. Metabolic scar assessment with18F-FDG PET: Correlation to ischemic ventricular tachycardia substrate and successful ablation sites. J. Nucl. Med. 2021, 62, 1591–1598. [Google Scholar] [CrossRef]
- Tian, J.; Smith, M.F.; Ahmad, G.; Dilsizian, V.; Jimenez, A.; Dickfeld, T. Integration of 3-dimensional scar models from SPECT to guide ventricular tachycardia ablation. J. Nucl. Med. 2012, 53, 894–901. [Google Scholar] [CrossRef]
- Thibault, B.; Richer, L.P.; McSpadden, L.C.; Ryu, K.; Aguilar, M.; Cadrin-Tourigny, J.; Tadros, R.; Mondésert, B.; Rivard, L.; Dyrda, K.; et al. Integration of 3D nuclear imaging in 3D mapping system for ventricular tachycardia ablation in patients with implanted devices: Perfusion/voltage retrospective assessment of scar location. Heart Rhythm O2 2022, 3, 560–567. [Google Scholar] [CrossRef]
- Klein, T.; Abdulghani, M.; Smith, M.; Huang, R.; Asoglu, R.; Remo, B.F.; Turgeman, A.; Mesubi, O.; Sidhu, S.; Synowski, S.; et al. Three-dimensional 123I-meta-iodobenzylguanidine cardiac innervation maps to assess substrate and successful ablation sites for ventricular tachycardia: feasibility study for a novel paradigm of innervation imaging. Circ. Arrhythm. Electrophysiol. 2015, 8, 583–591. [Google Scholar] [CrossRef]
- Josephson, M.E.; Anter, E. Substrate mapping for ventricular tachycardia: Assumptions and misconceptions. JACC Clin. Electrophysiol. 2015, 1, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, M.; Atreya, A.R.; Saggu, D.K.; Yalagudri, S.; Calambur, N. Catheter ablation of ventricular tachycardia: strategies to improve outcomes. Front. Cardiovasc. Med. 2023, 10, 966634. [Google Scholar] [CrossRef]
- Hawson, J.; Al-Kaisey, A.; Anderson, R.D.; Watts, T.; Morton, J.; Kumar, S.; Kistler, P.; Kalman, J.; Lee, G. Substrate-based approaches in ventricular tachycardia ablation. Indian Pacing Electrophysiol. J. 2022, 22, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Ciaccio, E.J.; Hsia, H.H.; Saluja, D.S.; Garan, H.; Coromilas, J.; Yarmohammadi, H.; Biviano, A.B.; Peters, N.S. Ventricular tachycardia substrate mapping: What’s been done and what needs to be done. Heart Rhythm 2025, 22, 2280–2299. [Google Scholar] [CrossRef] [PubMed]
- Jaïs, P.; Maury, P.; Khairy, P.; Sacher, F.; Nault, I.; Komatsu, Y.; Hocini, M.; Forclaz, A.; Jadidi, A.S.; Weerasooryia, R.; et al. Elimination of local abnormal ventricular activities: a new end point for substrate modification in patients with scar-related ventricular tachycardia. Circulation 2012, 125, 2184–2196. [Google Scholar] [CrossRef] [PubMed]
- Jackson, N.; Gizurarson, S.; Viswanathan, K.; King, B.; Massé, S.; Kusha, M.; Porta-Sanchez, A.; Jacob, J.R.; Khan, F.; Das, M.; et al. Decrement evoked potential mapping: Basis of a mechanistic strategy for ventricular tachycardia ablation. Circ. Arrhythm. Electrophysiol. 2015, 8, 1433–1442. [Google Scholar] [CrossRef]
- Bhaskaran, A.; Fitzgerald, J.; Jackson, N.; Gizurarson, S.; Nanthakumar, K.; Porta-Sánchez, A. Decrement evoked potential mapping to guide ventricular tachycardia ablation: Elucidating the functional substrate. Arrhythm. Electrophysiol. Rev. 2020, 9, 211–218. [Google Scholar] [CrossRef]
- Solimene, F.; Speziale, G.; Schillaci, V.; Stabile, G.; Shopova, G.; Arestia, A.; Salito, A.; D’Auria, C.; Coltorti, F.; De Simone, A.; et al. An annotation-independent algorithm based on electrogram characteristics to guide the identification of ventricular tachycardia isthmuses in patients with structural heart disease. J. Interv. Card. Electrophysiol. 2024, 67, 739–750. [Google Scholar] [CrossRef]
- Igarashi, M.; Nogami, A.; Fukamizu, S.; Sekiguchi, Y.; Nitta, J.; Sakamoto, N.; Sakamoto, Y.; Kurosaki, K.; Takahashi, Y.; Kimata, A.; et al. Acute and long-term results of bipolar radiofrequency catheter ablation of refractory ventricular arrhythmias of deep intramural origin. Heart Rhythm 2020, 17, 1500–1507. [Google Scholar] [CrossRef]
- Roca-Luque, I.; Rivas-Gándara, N.; Francisco-Pascual, J.; Rodriguez-Sanchez, J.; Cuellar-Calabria, H.; Rodriguez-Palomares, J.; García-Del Blanco, B.; Pérez-Rodon, J.; Santos-Ortega, A.; Rosés-Noguer, F.; et al. Preprocedural imaging to guide transcoronary ethanol ablation for refractory septal ventricular tachycardia. J. Cardiovasc. Electrophysiol. 2019, 30, 448–456. [Google Scholar] [CrossRef]
- Yamashita, S.; Sacher, F.; Mahida, S.; Berte, B.; Lim, H.S.; Komatsu, Y.; Amraoui, S.; Denis, A.; Derval, N.; Laurent, F.; et al. Image integration to guide catheter ablation in scar-related ventricular tachycardia. J. Cardiovasc. Electrophysiol. 2016, 27, 699–708. [Google Scholar]
- Deneke, T.; Kutyifa, V.; Hindricks, G.; Sommer, P.; Zeppenfeld, K.; Carbucicchio, C.; Pürerfellner, H.; Heinzel, F.R.; Traykov, V.B.; De Riva, M.; et al. Pre- and post-procedural cardiac imaging (computed tomography and magnetic resonance imaging) in electrophysiology: a clinical consensus statement of the European Heart Rhythm Association and European Association of Cardiovascular Imaging of the European Society of Cardiology. Europace 2024, 26. [Google Scholar]
- Berte, B.; Cochet, H.; Dang, L.; Mahida, S.; Moccetti, F.; Hilfiker, G.; Bondietti, J.; Ruschitzka, F.; Jaïs, P.; Scharf, C.; et al. Image-guided ablation of scar-related ventricular tachycardia: towards a shorter and more predictable procedure. J. Interv. Card. Electrophysiol. 2020, 59, 535–544. [Google Scholar] [CrossRef]
- Kawaguchi, M.; Takahashi, M.; Hata, T.; Kashima, Y.; Usui, F.; Morimoto, H.; Izawa, A.; Takahashi, Y.; Masumoto, J.; Koyama, J. Inflammasome activation of cardiac fibroblasts is essential for myocardial ischemia/reperfusion injury. [CrossRef]
- Dudzinski, D.M.; Januzzi, J.L., Jr. The evolving medical complexity of the modern cardiac intensive care unit. J. Am. Coll. Cardiol. 2017, 69, 2008–2010. [Google Scholar] [CrossRef]
- Falasconi, G.; Penela, D.; Soto-Iglesias, D.; Francia, P.; Teres, C.; Viveros, D.; Bellido, A.; Alderete, J.; Meca-Santamaria, J.; Franco, P.; et al. Preventive substrate ablation in chronic post-myocardial infarction patients with high-risk scar characteristics for ventricular arrhythmias: rationale and design of PREVENT-VT study. J. Interv. Card. Electrophysiol. 2023, 66, 39–47. [Google Scholar] [CrossRef]
- Santangeli, P.; Marchlinski, F.E. Substrate mapping for unstable ventricular tachycardia. Heart Rhythm 2016, 13, 569–583. [Google Scholar] [CrossRef]
- Mesubi, O.; Ahmad, G.; Jeudy, J.; Jimenez, A.; Kuk, R.; Saliaris, A.; See, V.; Shorofsky, S.; Dickfeld, T. Impact of ICD artifact burden on late gadolinium enhancement cardiac MR imaging in patients undergoing ventricular tachycardia ablation. Pacing Clin. Electrophysiol. 2014, 37, 1274–1283. [Google Scholar] [CrossRef]
- Bhagirath, P.; Campos, F.O.; Costa, C.M.; Wilde, A.A.M.; Prassl, A.J.; Neic, A.; Plank, G.; Rinaldi, C.A.; Götte, M.J.W.; Bishop, M.J. Predicting arrhythmia recurrence following catheter ablation for ventricular tachycardia using late gadolinium enhancement magnetic resonance imaging: Implications of varying scar ranges. Heart Rhythm 2022, 19, 1604–1610. [Google Scholar] [CrossRef]
- Mukherjee, R.K.; Whitaker, J.; Williams, S.E.; Razavi, R.; O’Neill, M.D. Magnetic resonance imaging guidance for the optimization of ventricular tachycardia ablation. Europace 2018, 20, 1721–1732. [Google Scholar] [CrossRef]
- Canino, G.; Di Costanzo, A.; Salerno, N.; Leo, I.; Cannataro, M.; Guzzi, P.H.; Veltri, P.; Sorrentino, S.; De Rosa, S.; Torella, D. Artificial intelligence in cardiac electrophysiology: A clinically oriented review with engineering primers. Bioengineering (Basel) 2025, 12, 1102. [Google Scholar] [CrossRef]
- Dello Russo, A.; Valeri, Y.; Ciconte, G.; Schiavone, M.; Compagnucci, P.; Di Monaco, A.; Riva, S.; Salerno, R.; Volpato, G.; Cipolletta, L.; et al. AI-assisted 3D intracardiac echocardiography for Pulsed Field Ablation of atrial fibrillation using a novel variable loop circular catheter: A multicenter evaluation. J. Clin. Med. 2025, 14, 7249. [Google Scholar] [CrossRef]
- Di Biase, L.; Zou, F.; Lin, A.N.; Grupposo, V.; Marazzato, J.; Tarantino, N.; Della Rocca, D.; Mohanty, S.; Natale, A.; Alhuarrat, M.A.D.; et al. Feasibility of three-dimensional artificial intelligence algorithm integration with intracardiac echocardiography for left atrial imaging during atrial fibrillation catheter ablation. Europace 2023, 25. [Google Scholar] [CrossRef]
- Akerström, F.; Drca, N.; Jensen-Urstad, M.; Braunschweig, F. Feasibility of a novel algorithm for automated reconstruction of the left atrial anatomy based on intracardiac echocardiography. Pacing Clin. Electrophysiol. 2022, 45, 1288–1294. [Google Scholar] [CrossRef]
- Wang, X.; Dennis, A.; Hesselkilde, E.M.; Saljic, A.; Linz, B.M.; Sattler, S.M.; Williams, J.; Tfelt-Hansen, J.; Jespersen, T.; Chow, A.W.C.; et al. Machine learning approach for automated localization of ventricular tachycardia ablation targets from substrate maps: development and validation in a porcine model. Eur. Heart J. Digit. Health 2025, 6, 645–655. [Google Scholar] [CrossRef]
- Blumenthal, C.J.; Hsue, W.; Chen, T.; Zhang, D.; Brem, E.; Garcia, F.C.; Callans, D.J.; Marchlinski, F.E.; Santangeli, P.; Tschabrunn, C.M. Preclinical experience using 4D intracardiac echocardiography to guide cardiac electrophysiology procedures. J. Cardiovasc. Electrophysiol. 2025, 36, 480–486. [Google Scholar] [CrossRef]
- Qin, D.; Singh, J.P. Digital twins: The future for ventricular tachycardia ablation? Circulation 2025, 151, 534–536. [Google Scholar] [CrossRef]
- Götte, M.J.W.; Hopman, L.H.G.A.; Bhagirath, P.; Kemme, M.J.B.; Nelissen, J.L.; Lindborg, K.; Krafft, A.J.; Sprengers, M.E.S.; Chamuleau, S.A.J.; Allaart, C.P. First-in-human real-time MR-guided ventricular ablation for idiopathic outflow tract premature ventricular complexes. JAMA Cardiol. 2025, 10, 1195–1200. [Google Scholar] [CrossRef]
- Mergen, V.; Reiner, M.F.; Klambauer, K.; Moser, L.J.; Guan, F.; Brunckhorst, C.; Duru, F.; Klotz, E.; Flohr, T.; Ruschitzka, F.; et al. Myocardial characterization using late enhancement photon-counting detector CT in ventricular arrhythmia: comparison with electroanatomical mapping. Insights Imaging 2025, 16, 187. [Google Scholar] [CrossRef]
- Carbucicchio, C.; Jereczek-Fossa, B.A.; Andreini, D.; Catto, V.; Piperno, G.; Conte, E.; Cattani, F.; Rondi, E.; Vigorito, S.; Piccolo, C.; et al. STRA-MI-VT (STereotactic RadioAblation by Multimodal Imaging for Ventricular Tachycardia): rationale and design of an Italian experimental prospective study. J. Interv. Card. Electrophysiol. 2021, 61, 583–593. [Google Scholar] [CrossRef]

Table 1.
Pre-, Intra-, and Post-Procedural Roles of Multimodal Imaging.
| Modality | Pre-procedural Role | Intra-procedural Role | Post-procedural Role |
|---|---|---|---|
| TTE (2D/3D) | Assess biventricular function and volumes; identify structural comorbidities | Support anatomical orientation in selected cases | Monitor function and remodeling |
| Strain (speckle-tracking) | Characterize subclinical dysfunction; assess regional mechanics/dyssynchrony | – | Stratify risk and monitor recovery/deterioration |
| TEE | Selected: exclude thrombi; evaluate anatomy if indicated | Monitor RF in selected scenarios; control position; indirect signs of complications | Selected: assess complications if clinical suspicion |
| ICE | – (possible planning if already available) | Guide access and navigation; optimize contact/stability; recognize early complications | Evaluate immediate complications (e.g., pericardium) if symptomatic |
| CMR cine | Define phenotype; quantify function and remodeling; identify aneurysms | Provide anatomical-functional roadmap (indirect) | Reassess function and remodeling; support redo |
| CMR-LGE (± PSI maps) | Segment 3D scar; distinguish core/border zone; identify conducting channels | Integrate model into EAM; focus mapping; support CMR-aided/guided strategies | Reassess substrate in recurrence; plan targeted redo |
| CMR T1/T2 mapping (± ECV) | Characterize diffuse/infiltrative fibrosis; identify edema/inflammation | – | Distinguish edema vs fibrosis in early follow-up |
| Cardiac CT / CCTA | 3D anatomy reconstruction; coronary evaluation; thickness; epicardial fat | Integrate geometry for navigation and safety; epicardial planning | Problem-oriented use for complications; anatomical updates |
| LIE-/DE-CT | Identify scar/border zone as an alternative or complement to CMR | Integrate scar model in EAM (selected centers) | – |
| FDG-PET | Phenotype inflammatory substrate; guide timing and therapy | Integrate 3D maps (if available) to focus on active regions | Monitor activity and therapeutic response; reassess recurrences |
| SPECT perfusion | Estimate perfusion/scar when CMR/CT not feasible | Integrate perfusion/scar model (less frequent) | Selected follow-up |
| 123I-mIBG SPECT | Assess sympathetic denervation (selected centers) | – | Selected follow-up |
Abbreviations: TTE: transthoracic echocardiography, TEE: transesophageal echocardiography, ICE: intracardiac echo, CMR: cardiac magnetic resonance, LGE: late gadolinium enhancement, CT/CCTA: computed tomography/coronary angiography, LIE-CT: late iodine enhancement CT, PET: positron emission tomography, SPECT: single photon emission computed tomography, EAM: electroanatomical mapping, PSI: pixel signal intensity.
Table 2.
Outputs and Endpoints of Multimodal Imaging.
| Modality | Output for EAM/strategy | Endpoints/metrics (examples) |
|---|---|---|
| TTE (2D/3D) | Define functional baseline; support risk stratification and timing | LVEF; LVEDV/LVESV; RVEF (if possible); 3D volumes; WMA |
| Strain (speckle-tracking) | Suggest regions of dysfunction compatible with substrate | GLS; regional strain; temporal dispersion (dyssynchrony indices) |
| TEE | Enhance safety in high-risk settings | Presence of thrombi; indirect parameters of overheating/complications; effusion |
| ICE | Improve EAM geometry; facilitate mapping; reduce fluoroscopy | Catheter-tissue contact (qualitative); distance from critical structures; effusion |
| CMR cine | Inform endo/epi choice and mapping priorities | LVEF/RVEF; volumes; wall thickness; WMA; aneurysm |
| CMR-LGE (± PSI maps) | Reduce blind mapping; direct targets; recognize reach-problem | Scar extent; transmurality; gray zone; channels/isthmuses |
| CMR T1/T2 mapping (± ECV) | Contextualize substrates in NICM/active conditions; support timing | T1 native; T2; ECV; edema burden |
| Cardiac CT / CCTA | Bind lesions; interpret low voltages (fat vs scar) | Distance from coronaries; epicardial fat; wall thinning; calcifications |
| LIE-/DE-CT | Increase detection of intramural/epicardial components | Extent delayed iodine enhancement; scar/border zone volume |
| FDG-PET | Distinguish active inflammation vs quiescent scar | Uptake pattern; SUV; perfusion mismatch |
| SPECT perfusion | Complementary perfusion information | Perfusion defects; extent and severity |
| 123I-mIBG SPECT | Add neural information on substrate and triggers | H/M ratio; washout rate; extent of denervation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



