
Submitted:
06 February 2026
Posted:
09 February 2026
You are already at the latest version
Abstract
Myeloid sarcoma (MS) is a malignant extramedullary tumor that occurs in patients with acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), or chronic myeloid leukemia (CML). The standard first-line treatment for MS is intensive chemotherapy according the AML protocol, regardless of bone marrow involvement. The role of allogeneic hematopoietic stem cell transplantation (alloHSCT) in the treatment of pediatric patients with MS requires further investigation.
The aim of the study was to evaluate treatment outcomes for MS in pediatric patients with a focus on assessing the impact of allogeneic hematopoietic stem cell transplantation (alloHSCT) on treatment efficacy.
The study included 64 patients aged 0 to 19 years from 15 pediatric oncology centers in Poland, who were diagnosed with MS between 1998 and 2024.
The probability of 5-year overall survival (pOS) for the entire cohort was 0.63 ± 0.07, while the 5-year event-free survival (pEFS) and 5-year relapse-free survival (pRFS) were 0.62 ± 0.07 and 0.72 ± 0.07, respectively. Treatment outcomes were compared between patients who underwent allogeneic hematopoietic stem cell transplantation (alloHSCT) in first complete remission (ICR) (n1 = 17/64; 27%) and those who did not receive alloHSCT (n2 = 47/64; 73%). In the alloHSCT group (n1), the estimated survival probabilities were pOS = 0.49 ± 0.13, pEFS = 0.44 ± 0.14, and pRFS = 0.40 ± 0.14. In the non-alloHSCT group (n2), these values were pOS = 0.68 ± 0.08, pEFS = 0.68 ± 0.08, and pRFS = 0.84 ± 0.06. The difference in pRFS between groups n1 and n2 was statistically significant (p = 0.0049). Extramedullary relapse was more frequently observed in patients who had undergone allogeneic hematopoietic stem cell transplantation (alloHSCT) (p = 0.0001). Further research is needed to identify effective strategies for sustaining remission in patients with MS after alloHSCT.
Keywords:
myeloid sarcoma
; myeloid leukemia
; children
1. Introduction
Myeloid sarcoma (granulocytic sarcoma, myeloid tumor, chloroma) is a neoplasm composed of immature or mature myeloid blast cells [1]. Most commonly, it is associated with acute myeloid leukemia, clinically presenting as an extramedullary located mass. However, it may also precede bone marrow infiltration or present as an extramedullary relapse [1,2].The latter one is more frequently observed following allogeneic bone marrow transplantation [2]. MS may also occur in patients with blastic phase of transformed myeloproliferative neoplasms (MPNs), myelodysplastic syndromes (MDS), or MDS/MPNs [1,2,3,4]. The World Health Organisation from 2008 defined myeloid sarcoma as an extramedullary proliferation of myeloid cells which disrupts the surrounding tissue architecture. This distinction clarifies the difference between myeloid sarcoma and extramedullary disease, the latter being a broader entity, including for example central nervous system occupation. According to the latest WHO and International Consensus Classification (ICC) published in 2022, definition of myeloid sarcoma remains unchanged [3].
The incidence of MS in adults varies from 0,2-2,8%, however many authors suggest that the data may be underestimated] as patients with newly diagnosed AML are not routinely screened for extramedullary tumor, unless they exhibit symptoms [2]. There is more data about post- allo-HSCT MS, in which incidence was reported at 5-12%, which is 7-46% of total relapses [3]. In children, the prevalence of MS reported in the literature reaches up to 40% however studies including a large number of pediatric patients are lacking [5,6].
The ,,gold standard” to establish the diagnosis of MS is a biopsy of the tumor and immunohistochemical analysis [5,6]. The panel of antibodies should consist of: MPO, CD14, CD68, lysozyme, CD117, CD11c, CD13, CD33. The inclusion of CD20, CD79a, CD3 and CD45RO helps to exclude B-cell and T-cell lymphomas, which is crucial as T-cell lymphoma is the most common misdiagnosis [5,6,7]. In cases with concomitant bone marrow involvement, the decision to perform a tumor biopsy depends on the patient’s condition and tumor location. If the biopsy is unsafe, the diagnosis may be based on imaging techniques, including positron emission tomography (PET) whose role in the diagnostic approach in MS has been well established [3,8]. The cytogenetics and molecular examination from bone marrow and, if available, from tumor tissue, are also vital to establish an accurate diagnosis, as the genetic abnormalities may influence the treatment strategies [1,6].
The therapy of myeloid sarcoma in children is based on intensive chemotherapy according to the AML Protocol [1]. The role of alloHSCT in children with MS remains a subject of ongoing debate, with conflicting findings reported in various studies. Here, we report the results of the study including a large cohort of pediatric patients with MS, making this report unique within the literature on MS in children, which is predominantly composed of case reports.
2. Material
The study included 64 patients aged 0 to 19 years (29 girls, 35 boys, mean age 7,9, median age 7.5 years), from 15 pediatric oncology centers in Poland, diagnosed with MS between 1998 and 2024. The diagnosis of MS was established in accordance with the World Health Organization (WHO) classification, which defines myeloid sarcoma as an extramedullary proliferation of myeloid cells disrupting the normal tissue architecture (WHO 2008, 2022) [3].
The biopsy and immunohistochemistry were performed on 42 patients. In 22 patients the diagnosis of MS was established based on bone marrow assessment and imaging techniques. Treatment response was assessed primarily using imaging modalities, including positon emission tomography (PET-CT). [5].
3. Methods
An Excel database was created to collect data on clinical features and treatment methods and outcomes. An event was defined as a relapse, progression, death, or second cancer. Complete remission (CR), partial remission (PR), and late remission (LR) were assessed according to the patient’s AML therapeutic protocol. Moreover, PR was reported in the case of partial tumor regression, even if CR in the bone marrow was achieved. Qualitative variables were presented as numbers (N) and percentages (%). For bivariate comparisons, χ² or the Fisher’s exact test was applied. The Kaplan–Meier method was used to determine pOS, pRFS, and pEFS. The influence of MS presentation and alloHSCT on survival times (OS, EFS, RFS) was assessed using the logrank test. A statistical analysis was conducted with MedCalc 20.123 (MedCalc Software, Ostend, Belgium). Statistical significance was considered at p<0.05.
The study protocols were approved by the Ethics Committee of Medical University of Poznań, resolution number 455/15. All of participants have written consent to participate and publish the data. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.Written informed consent for participation and publication was obtained from all participants aged 16–19 years. For participants younger than 16 years, written informed consent was obtained from a parent or legal guardian.
4. Results
4.1. Study Group Characteristics
In the study group, patients with AML predominated (49), thirteen patients had isolated MS without bone marrow involvement, one patient was diagnosed with CML, and one patient was diagnosed with MDS.The distribution of the study group based on the bone marrow disease diagnosis is presented in Table 1.
Clinical presentations of myeloid sarcoma depending on the time relation to bone marrow involvement are illustrated in the Figure 1.
The most frequently affected location was the skin, identified in 22 out of 64 cases (34%). Orbit was the second the most common localization (16/64, 25%). Other anatomical sites of lesions included: central nervous system, kidney, lung, liver, abdominal cavity and pelvis, mediastinum, maxillary, sphenoid, and ethmoid sinuses, pyramid of the temporal bone, soft tissues of the head and face, paraspinal mass, soft tissue of forearm, breast. Twenty patients (20/64, 31%) presented multifocal lesions (more than 1).
Available genetic results of bone marrow in a study group are presented in Supplementary Material S1.
Almost all the patients (63/64, 98%) received systemic chemotherapy. In 27 patients (27/64, 42%) radiotherapy was administered as a part of the treatment, seven patients (7/64, 11%) underwent surgical treatment. Seventeen patients (17/64, 21%) were treated with alloHSCT.
4.2. Treatmen Outcomes
In the study group, CR was achieved in fifty-one patients (51/64, 79%). Among these, thirteen patients relapsed (13/51, 25%). Forty one patients are alive (41/64, 64%) Twenty three patients died (23/64, 36%), the major cause of death was disease progression (19/23, 83%), four patients (4/23, 17%) died due to complications of the treatment. The mean overall survival (OS) was 121.3 ± 12.1 months, and the 5-year overall survival probability was 0.63 ± 0.07. The estimated OS rates were 75.5% at 1 year and 70.3% at 2 years, remaining stable through 30 months. The mean EFS was 119.4 ± 12.3 months, with a 5-year EFS probability of 0.62 ± 0.07. The EFS rates were 76.6% at 1 year and 69.4% at 2 years, with no further decline observed up to 30 months. Relapse occurred in 15 patients. The mean relapse-free survival (RFS) was 140.1 ± 12.3 months, and the 5-year RFS probability was 0.72 ± 0.06. The RFS rates were 87.7% at 1 year, 74.9% at 2 years, and 72.3% at 30 months, indicating a gradual decline over time. Figure 2 shows pOS, pRFS and pEFS curves.
Treatment outcomes were compared between patients who underwent allogeneic hematopoietic stem cell transplantation (alloHSCT) in first complete remission (ICR) (n1 = 17/64; 27%) and those who did not receive alloHSCT (n2 = 47/64; 73%).
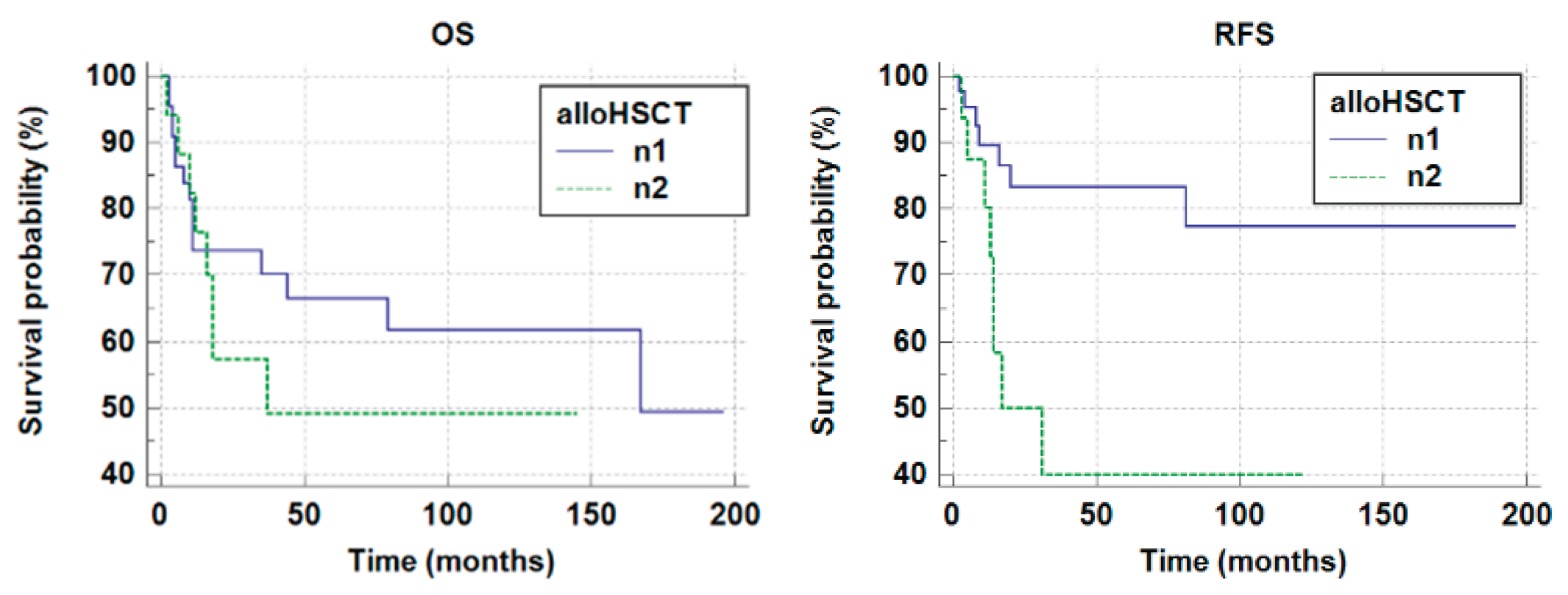
In the n1 group, death occurred in 8 out of 17 patients. The mean survival time was 79.39 ± 16.61 months (Mean ± SE). The 5-year survival probability was pOS = 0.49 ± 0.13. In the n2 group death occured in 15 out of 47 patients. The mean survival time was 128,85±13,95 (months) (Mean±SE). The 5 year survival probability was pOS=0,68±0,08. No statistically significant differences were observed (p = 0.3177, Log-rank test). The 5 year event free survival probability (pEFS) in the group n1 and n2 were n1 pEFS=0,44±0,14 and n2pEFS=0,68±0,08, respectively. No statistically significant difference was observed (p = 0,1974, Log-rank test).
In group n1 relapse occured in 8 out of 17 patients. The mean relapse- free survival time was 57,61±14,97 months (Mean±SE). In group n2 mean relapse- free survival time was 160,14±12,48 months (Mean±SE). The 5-year relapse- free survival probabilities (pRFS) were as follows: n1pRFS=0,40±0,14, n2pRFS=0,84±0,06. A statistically significant difference was observed (p = 0.0049). All relapsed patients in group n1 (8/8) presented extramedullary relapse, in 5/8 cases the relapse was combined with bone marrow relapse. Extramedullary relapse was more frequently observed in patients who had undergone allogeneic hematopoietic stem cell transplantation (alloHSCT) (p = 0.0001).

Table 2.
Outcome of the treatment in group of patients, who received allogeneic hematopoietic stem cell transplantation (alloHSCT) - group n1 and those, who did not received alloHSCT - group n2.
Table 2.
Outcome of the treatment in group of patients, who received allogeneic hematopoietic stem cell transplantation (alloHSCT) - group n1 and those, who did not received alloHSCT - group n2.
| pOS | pEFS | pRFS | |
| n1=17 (with alloHSCT) |
0,49±0,13 | 0,44±0,14 | 0,40±0,14 |
| n2=47 (without alloHSCT) |
0,68±0,08 | 0,68±0,08 | 0,84±0,06 |
Figure 3.
The 5-year overall survival probability and the 5-year relapse free survival probability in the group n1 and n2 (n1 pOS 0,49±0,13; n2 pOS 0,68±0,08, p=0.3177; n1 pRFS=0,40±0,14, n2 pRFS =0,84±0,06, p = 0.0049).
Figure 3.
The 5-year overall survival probability and the 5-year relapse free survival probability in the group n1 and n2 (n1 pOS 0,49±0,13; n2 pOS 0,68±0,08, p=0.3177; n1 pRFS=0,40±0,14, n2 pRFS =0,84±0,06, p = 0.0049).
The outcomes of two clinical presentations of MS were compared - patients with de novo MS (24 patients) and those with MS concurrent with leukemia (33 patients). The 5-year overall survival and event-free survival probabilities were significantly higher in patients with myeloid sarcoma (MS) presenting concurrently with leukemia than in patients with de novo MS (OS: 0.82 ± 0.07 vs 0.50 ± 0.11, p = 0.0037; EFS: 0.79 ± 0.08 vs 0.50 ± 0.10, p = 0.0097).
5. Discussion
The prognosis for adult patients with myeloid sarcoma is poor [3,9].. The prognostic significance of MS in children remains unclear. Some authors demonstrated that myeloid sarcoma in children, except for the cutaneous form, is associated with a better prognosis [1,10,11]. More recent studies have demonstrated that the presence of extramedullary manifestation at diagnosis is associated with poorer outcomes. Li et al. showed that extramedullary infiltration present at diagnosis is an adverse prognostic factor, associated with shorter event-free survival (EFS) and overall survival (OS) [12].Stove et al. analyzed 73 children with extramedullary leukemia (EML). The term EML in their study encompassed both central nervous involvement and myeloid sarcoma. Their findings indicated that 5-year overall survival (OS) was significantly lower in the EML group (64% vs. 73%, P = 0.04) [13].. Treatment results of myeloid sarcoma patients were as follows: 5-year EFS 57%, 5-year OS 68% which is similar to the results presented in our study [13]. In the analysis of Xu LH et al., MS in children was associated with a low complete remission rate, high induction death, poor 5-year EFS, and OS. Interestingly, the authors also showed that KMT2A rearrangement had a negative impact on clinical outcomes in AML patients with MS [14].
In our study, patients with de novo myeloid sarcoma had significantly lower pOS and pEFS, than patients with MS concomitant with bone marrow disease. Little is known about the impact of the clinical presentation of MS on treatment results in children. In Zhao analysis, which included both adults and children, patients with primary MS (without bone marrow involvement) had significantly lower pOS, compared to patients with MS and intramedullary disease [9]. Zipin Xing et al. categorized patients with MS into two subgroups: patients with a hematopoietic location of the tumor (lymph nodes, liver and spleen) and those with tumor in other locations. Patients with non-hematopoietic MS and a clinical presentation of MS as the primary malignancy exhibited a higher survival rate [15].. Better outcome was observed in children than in adults. Interestingly, the authors developed nomograms to predict prognosis in patients with non-hematopoietic locations of MS [15]. Data about the prognostic significance of isolated extramedullary relapse after alloHSCT are also unclear. In Yuda analysis, patients with isolated extramedullary post-transplant relapse presented better 2-year overall survival than those with combined bone marrow and extramedullary relapse or bone marrow relapse [16].
It is well documented that systemic chemotherapy is a frontline treatment for myeloid sarcoma, both in children and adults, regardless of bone marrow involvement. However, there are still a lot of questions about the optimal therapeutic strategy in MS, as treatment results remain insufficient. Data about the role of alloHSCT in myeloid sarcoma are conflicting. Chevalier et al. recommend allogeneic hematopoietic stem cell transplantation after chemotherapy in both isolated myeloid sarcoma and myeloid sarcoma concurrent with leukemia [17]. Shan et al. also reported that alloHSCT improved the outcome of patients with MS, who achieved remission after chemotherapy [18]. In Zhao et al analysis patients who underwent alloHSCT, presented significantly better median survival time than patients treated with local therapy or intensive chemotherapy alone [9]. The authors suggest that maintenance therapy with decitabine after alloHSCT may help to sustain remission in patients with MS [9].. However, some authors demonstrated that alloHSCT had no significant effect on the survival of AML patients with MS [12,14]. In our analysis, patients who underwent allogeneic hematopoietic stem cell transplantation (alloHSCT) had a significantly lower probability of relapse-free survival, compared to those who did not undergo transplantation. It has already been documented that after alloHSCT, the frequency of extramedullary relapse is higher. One potential explanation for the increased risk of extramedullary recurrence following alloHSCT is the reduced graft-versus-leukemia (GvL) effect in extramedullary lesions [3,19]. The reason for that is diminished immunologic surveillance in extramedullary tissues, as patrolling donor T cells and natural killer (NK) cells are mainly concentrated in bone marrow [9,19,20]. This means that the effect of chronic Graft-versus- host disease ( GvHD) does not have a protective effect against relapse in the extramedullary sites, what has been also demonstrated in Hazar et al. Report [19,20,21]. The authors also reported that extramedullary disease before transplantation was an independent risk factor associated with an increased incidence of extramedullary relapse [21].
In this context, a novel therapy approach is needed for patients with MS. Li et al. suggest that gemtuzumab ozogamicin (GO) may improve the outcome of patients with MS, contrary to alloHSCT [12]. Piccaluga et al. also concluded that GO may be an effective agent in the treatment of MS [22]. Xue Zhang et al. reported two cases of adult patients with MS, who underwent microtransplantation. The procedure is the alternative method of allotransplantation, with a low toxicity but it may retain part of graft-versus-leukemia (GVL) effect. Both patients achieved durable disease control [23].
An increasing amount of data in the literature highlights the role of hypomethylating agents and venetoclax in the treatment of myeloid sarcoma [24,25,26].These agents should be also considered as maintenance therapy after alloHSCT is performed as consolidation therapy in patients with MS [1].
In MS associated with AML harboring mutation of fms-like tyrosine kinase 3 (FLT3) gene, FLT3 inhibitors might be effective. There are a few reports of successful treatment with gliteritinib in adult patients with MS [27,28,29]. Some data supporting the use of IDH inhibitors in the treatment of MS exist, as IDH1/IDH2 mutations have been described in MS [3].Sonedeb et al. documented good response in three out of four patients with IDH mutation detected in the tissue of the extramedullary involved site [30].
There is still much to be investigated regarding new drugs used in AML in the context of myeloid sarcoma. Little is known about the efficacy of CPX 351 against extramedullary sites. Gianfelici et al. reported a case of successful treatment with CPX 351 in an adult woman with MS located in the skin [31]. Further research is also needed to determine the role of menin inhibitors in the treatment of myeloid sarcoma with KMT2A rearrangement.
The use of menin inhibitors may represent a breakthrough in the treatment of myeloid sarcoma with KMT2A rearrangement [32].
6. Conclusions
Allogeneic hematopoietic stem cell transplantation (alloHSCT) does not improve the outcome of patients with MS. Moreover, patients who have been transplanted, have a lower 5-year probability of relapse-free survival, indicating a diminished graft-versus-leukemia (GvL) effect in extramedullary sites. Further research is needed to identify effective strategies for maintaining remission in MS patients following allo-HSCT. Additionally, future studies should focus on the genetic characteristics of MS, as this may facilitate the development of novel treatment approaches.
7. Limitations
This study has limitations, as data about the occurence of GvHD, type of conditioning, and type of donor in transplanted patients are lacking. Future research should include analysis with accurate data about transplantation procedure in patients, who underwent alloHSCT.
In addition, due to the multicenter and retrospective design of the study, some cytogenetic and molecular data were unavailable.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
The Authors received no funding for this work.
Authors Contributions
MS and KD designed the study. JW revised critically the manuscript. MS, JS-S, MC, WBal, SK, NB, TO, TU,GW, KK, KM-R, AS-R, IM, PŁ, AMM, BU, AC, AK, MK-R, AS-B, IM, MM, AM-M, RT, TS, AC-G, GK, LM-K, MK, NI-J, KM, WBad, KB, WM, RC, JZ, KDr collected the clinical data. MS drafted the manuscript. KD edited and revised the manuscript. All authors contributed to the article.
Disclosures
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability Statement
The data analyzed in this study is subject to the following licenses/restrictions: The dataset was created by the author on the basis of clinical data and patient’s history available in pediatric oncology centers. The author has access to the data which are not public. Requests to access these datasets should be directed to magdalena.samborska@ump.edu.pl. This retrospective study involved analysis of anonymized patient data and did not require ethical approval, in accordance with institutional and national guidelines.
References
- Zorn, K.E.; Cunningham, A.M.; Meyer, A.E.; et al. Pediatric myeloid sarcoma, more than just a chloroma: a review of clinical presentations, significance, and biology. Cancers (Basel) 2023, 15, 1443. [Google Scholar] [CrossRef]
- Diamantidis, M.D. Myeloid sarcoma: novel advances regarding molecular pathogenesis, presentation and therapeutic options. J. Clin. Med. 2024, 13, 6154. [Google Scholar] [CrossRef]
- Loscocco, G.G.; Vannucchi, A.M. Myeloid sarcoma: more and less than a distinct entity. Ann. Hematol. 2023, 102, 1973–1984. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; et al. International consensus classification of myeloid neoplasms and acute leukemias: integrating morphologic, clinical, and genomic data. Blood 2022, 140, 1200–1228. [Google Scholar] [CrossRef] [PubMed]
- Klco, J.M.; Welch, J.S.; Nguyen, T.T.; et al. State of the art in myeloid sarcoma. Int. J. Lab. Hematol. 2011, 33, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Ye, F.; Zhang, H.; Zhang, W.; et al. Clinical characteristics, pathology features and outcomes of pediatric myeloid sarcoma: a retrospective case series. Front. Pediatr. 2022, 10, 927894. [Google Scholar] [CrossRef] [PubMed]
- Aslam, H.M.; Veeraballi, S.; Saeed, Z.; Weil, A.; Chaudhary, V. Isolated myeloid sarcoma: a diagnostic dilemma. Cureus 2022, 14, e21200. [Google Scholar] [CrossRef]
- Sahu, K.K.; Thakur, K. Role of positron emission tomography imaging in myeloid sarcoma. Indian J. Nucl. Med. 2018, 33, 90. [Google Scholar] [CrossRef]
- Zhao, H.; Dong, Z.; Wan, D.; et al. Clinical characteristics, treatment, and prognosis of 118 cases of myeloid sarcoma. Sci. Rep. 2022, 12, 6752. [Google Scholar] [CrossRef]
- Dusenbery, K.E.; Howells, W.B.; Arthur, D.C.; et al. Extramedullary leukemia in children with newly diagnosed acute myeloid leukemia: a report from the Children’s Cancer Group. J. Pediatr. Hematol. Oncol. 2003, 25, 760–768. [Google Scholar] [CrossRef]
- Johnston, D.L.; Alonzo, T.A.; Gerbing, R.B.; Lange, B.J.; Woods, W.G. Superior outcome of pediatric acute myeloid leukemia patients with orbital and CNS myeloid sarcoma: a report from the Children’s Oncology Group. Pediatr. Blood Cancer 2012, 58, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Shi, M.; Zhou, P.; et al. Extramedullary infiltration in pediatric acute myeloid leukemia: results from the therapeutically applicable research to generate effective treatments (TARGET) initiative. Pediatr. Blood Cancer 2024, 71, e31014. [Google Scholar] [CrossRef] [PubMed]
- Stove, H.K.; Sandahl, J.D.; Abrahamsson, J.; et al. Extramedullary leukemia in children with acute myeloid leukemia: a population-based cohort study from the Nordic Society of Pediatric Hematology and Oncology (NOPHO). Pediatr. Blood Cancer 2017, 64, e26520. [Google Scholar] [CrossRef]
- Xu, L.H.; Wang, Y.; Chen, Z.Y.; Fang, J.P. Myeloid sarcoma is associated with poor clinical outcome in pediatric patients with acute myeloid leukemia. J. Cancer Res. Clin. Oncol. 2020, 146, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Xing, Z.; Zhu, X.; Li, Z.; Wang, H. Incidence, clinical characteristics, and prognostic nomograms for patients with myeloid sarcoma: a SEER-based study. Front. Oncol. 2022, 12, 989366. [Google Scholar] [CrossRef]
- Yuda, S.; Fuji, S.; Onishi, A. Extramedullary relapse of acute myelogenous leukemia after allogeneic hematopoietic stem cell transplantation. Biol. Blood Marrow Transplant. 2019, 25, 1152–1157. [Google Scholar] [CrossRef]
- Chevallier, P.; Labopin, M.; Cornelissen, J.; et al. Allogeneic hematopoietic stem cell transplantation for isolated and leukemic myeloid sarcoma in adults: a report from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Haematologica 2011, 96, 1391–1394. [Google Scholar] [CrossRef]
- Shan, M.; Lu, Y.; Yang, M.; et al. Characteristics and transplant outcome of myeloid sarcoma: a single-institute study. Int. J. Hematol. 2021, 113, 682–692. [Google Scholar] [CrossRef]
- Clark, W.B.; Strickland, S.A.; Barrett, A.J.; et al. Extramedullary relapses after allogeneic stem cell transplantation for acute myeloid leukemia and myelodysplastic syndrome. Haematologica 2010, 95, 860–863. [Google Scholar] [CrossRef]
- Harris, A.C.; Kitko, C.L.; Couriel, D.R.; et al. Extramedullary relapse of acute myeloid leukemia following allogeneic hematopoietic stem cell transplantation: incidence, risk factors and outcomes. Haematologica 2013, 98, 179–184. [Google Scholar] [CrossRef]
- Hazar, V.; Öztürk, G.; Yalçın, K.; et al. Different kinetics and risk factors for isolated extramedullary relapse after allogeneic hematopoietic stem cell transplantation in children with acute leukemia. Transplant. Cell. Ther. 2021, 27, 859.e1–859.e10. [Google Scholar] [CrossRef] [PubMed]
- Piccaluga, P.P.; Martinelli, G.; Rondoni, M.; et al. Gemtuzumab ozogamicin for relapsed and refractory acute myeloid leukemia and myeloid sarcomas. Leuk. Lymphoma 2004, 45, 1791–1795. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, S.; Wang, F. Microtransplantation for myeloid sarcoma: two case reports. Leuk. Res. Rep. 2022, 17, 100326. [Google Scholar] [CrossRef]
- Jian, X.; Cha, J.; Lin, Z.; et al. Real-world experience with venetoclax-based therapy for patients with myeloid sarcoma. Discov. Oncol. 2024, 15, 210. [Google Scholar] [CrossRef]
- Kayser, S.; Sanber, K.; Marconi, G. Outcome of adult acute myeloid leukemia patients with extramedullary disease and treatment with venetoclax/hypomethylating agents. Haematologica 2025, 110, 378–384. [Google Scholar]
- Shatilova, A.; Girshova, L.; Zaytsev, D. The myeloid sarcoma treated by venetoclax with hypomethylating agent followed by stem cell transplantation: rare case report. BMC Womens Health 2021, 21, 184. [Google Scholar] [CrossRef]
- Kim, R.S.; Yaghy, A.; Wilde, L.R.; Shields, C.L. An iridociliochoroidal myeloid sarcoma associated with relapsed acute myeloid leukemia with FLT3-ITD mutation, treated with gilteritinib, an FLT3 inhibitor. JAMA Ophthalmol. 2020, 138, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Kida, M.; Kuroda, Y.; Kido, M.; et al. Successful treatment with gilteritinib for isolated extramedullary relapse of acute myeloid leukemia with FLT3-ITD mutation after allogeneic stem cell transplantation. Int. J. Hematol. 2020, 112, 243–248. [Google Scholar] [CrossRef]
- Kumode, T.; Rai, S.; Tanaka, H.; et al. Targeted therapy for medullary and extramedullary relapse of FLT3-ITD acute myeloid leukemia following allogeneic hematopoietic stem cell transplantation. Leuk. Res. Rep. 2020, 14, 100219. [Google Scholar] [CrossRef]
- Ball, S.; Knepper, T.C.; Deutsch, Y.E.; et al. Molecular annotation of extramedullary acute myeloid leukemia identifies high prevalence of targetable mutations. Cancer 2022, 128, 3880–3887. [Google Scholar] [CrossRef] [PubMed]
- Gianfelici, V.; Levato, L.; Magro, D. PB1822: a case of extramedullary acute myeloid leukemia successfully treated with novel agents. Hemasphere 2022, 6, 1702–1703. [Google Scholar] [CrossRef]
- Cuglievan, B.; Kantarjian, H.; Rubnitz, J.E. Menin inhibitors in pediatric acute leukemia: a comprehensive review and recommendations to accelerate progress in collaboration with adult leukemia and the international community. Leukemia 2024, 38, 2073–2084. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Clinical presentations of myeloid sarcoma depending on the time relation to bone marrow involvement.
Figure 1.
Clinical presentations of myeloid sarcoma depending on the time relation to bone marrow involvement.
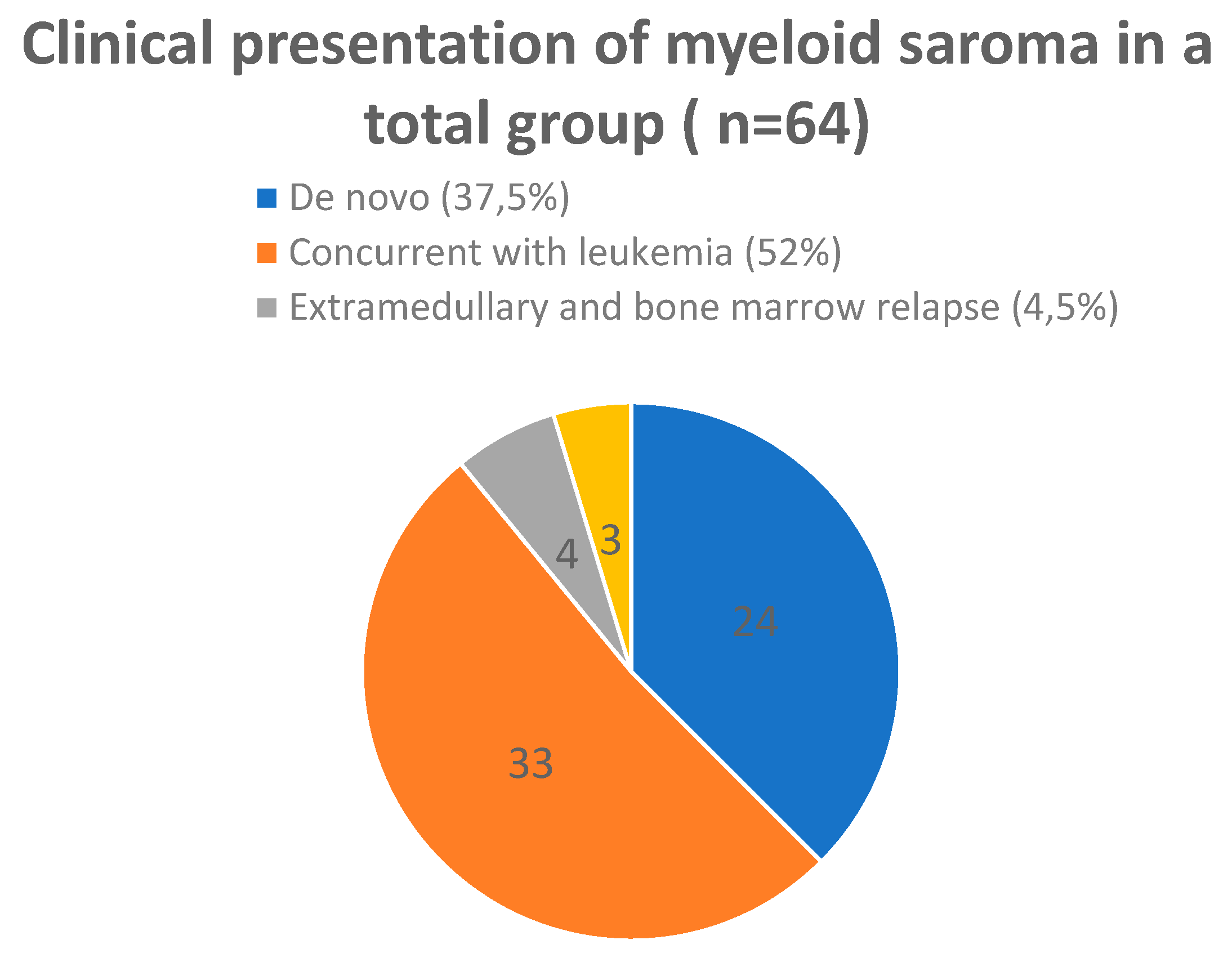
Figure 2.
The 5-year overal survival probability (pOS), relapse free survival (pRFS) and event-free survival probability (pEFS) in a total study group.
Figure 2.
The 5-year overal survival probability (pOS), relapse free survival (pRFS) and event-free survival probability (pEFS) in a total study group.
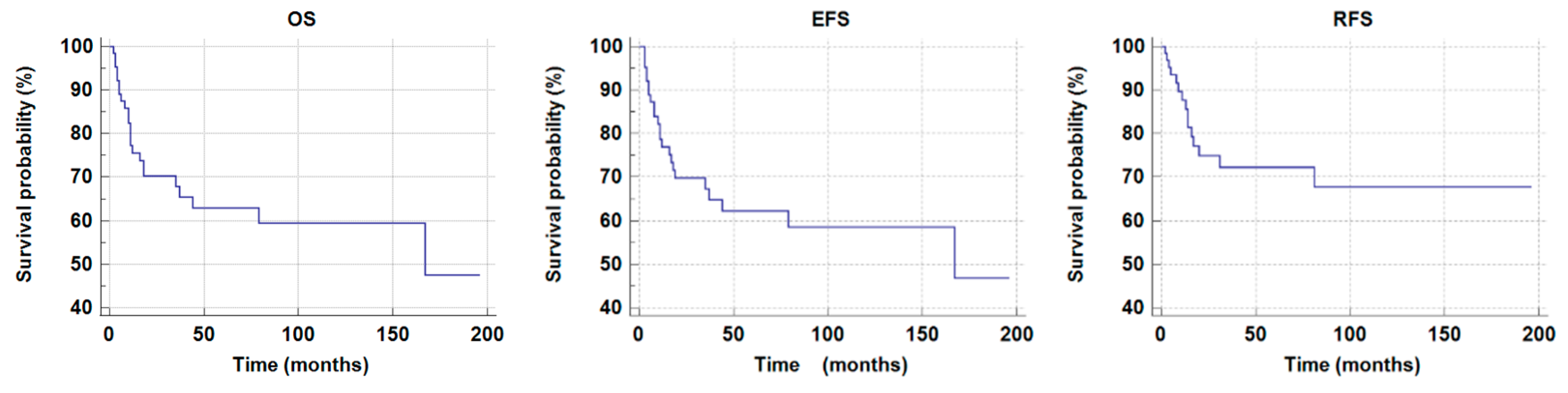
Table 1.
The distribution of the study group based on the bone marrow disease diagnosis.
| Bone Marrow Disease Diagnosis | Number of Patients (n) |
| AML | 49 (77%) |
| CML* | 1 (1,5%) |
| MDS | 1 (1,5%) |
|
Isolated Myeloid Sarcoma (without bone marrow involvement) |
13 (20%) |
*CML - chronic myeloid leukemia.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



