
Submitted:
08 February 2026
Posted:
09 February 2026
You are already at the latest version
Abstract
Background: Breast cancer (BC) diagnostics are undergoing a transformative shift from traditional morphological assessment to a complex multi-omic characterization. While Immunohistochemistry (IHC) remains the clinical bedrock for subtyping, its inherent inability to account for intra-tumoral heterogeneity and the dynamic nature of clonal evolution has necessitated the integration of high-throughput genomic and transcriptomic tools. Main body: This review examines the technological evolution from "gold standard" protein-based assays to precision oncology enabled by Next-Generation Sequencing (NGS) and liquid biopsy. We provide a rigorous analysis of multi-gene expression signatures (Oncotype DX, MammaPrint, Prosigna, EndoPredict) and their impact on clinical decision-making. Furthermore, we explore the clinical utility of circulating tumor DNA (ctDNA) for molecular residual disease (MRD) detection and the identification of acquired resistance mechanisms involving ESR1, PIK3CA, AKT1, and PTEN mutations. We further address the complex bioinformatics challenges, including variant interpretation, the implementation of Unique Molecular Identifiers (UMIs), and the integration of artificial intelligence in analyzing massive multi-omic datasets. Conclusion: The integration of IHC with longitudinal genomic profiling is essential for the future of breast cancer management. This multi-modal approach ensures that therapeutic strategies evolve alongside the tumor's molecular landscape. Future clinical trials must focus on MRD-guided interventions to validate the clinical benefit of early genomic detection.
Keywords:
1. Introduction
1.1. The Evolving Landscape of Oncology
1.2. Aim of the review
2. Search strategy
3. Results and Discussion
3.1. The Foundation and Fragility of the IHC Standard
3.1.1. Technical Nuances and the Challenge of Standardization
3.1.2. The HER2 Spectrum: From Binary to Continuum
3.2. The Transcriptomic Shift: Multi-Gene Expression Assays
3.2.1. Oncotype DX and the TAILORx Trial
3.2.2. MammaPrint and the MINDACT Trial
3.2.3. Prosigna (PAM50) and EndoPredict: Precision in Late Recurrence
3.3. Next-Generation Sequencing (NGS): Mapping the BC Genome
3.3.1. Comparative Analysis: Illumina vs. Ion Torrent Platforms
- Illumina (Sequencing by Synthesis): Dominates the market due to its extremely high accuracy and throughput. It is the gold standard for WES and large targeted panels.
- Ion Torrent (Semiconductor Sequencing): Offers faster turnaround times and requires less starting DNA, making it attractive for small biopsies where tissue is limited. However, its error rate in homopolymer regions (repeated bases like AAAAA) is higher than Illumina.
3.3.2. Targeted Panels vs. Whole Exome Sequencing (WES)
- Targeted Panels: These sequence 300-500 genes known to be relevant in cancer (e.g., FoundationOne). They provide high "depth" of coverage (often >500x), allowing for the detection of mutations present in only 1-2% of cells (Variant Allele Frequency - VAF).
- Whole Exome Sequencing (WES): WES sequences all ~20,000 protein-coding genes. In medical genetics, WES is essential for identifying Tumor Mutational Burden (TMB) and Microsatellite Instability (MSI), which are predictive markers for response to immunotherapy with Pembrolizumab [6].
3.3.3. Actionable Mutations and Resistance Mechanisms
- PIK3CA Mutations: Found in ~40% of HR+ breast cancers, these mutations activate the PI3K/AKT/mTOR pathway, leading to cell proliferation and resistance to endocrine therapy. The SOLAR-1 trial demonstrated that Alpelisib significantly improves progression-free survival in these patients [12].
- ESR1 Mutations (Y537S, D538G): These mutations typically develop under the selective pressure of Aromatase Inhibitors (AI). They cause the Estrogen Receptor to remain "always on" even without estrogen. Detecting these via NGS informs a switch to Selective Estrogen Receptor Degraders (SERDs) like Elacestrant [7].
- BRCA1/2 Mutations: These alterations in DNA repair pathways predict response to PARP Inhibitors, particularly in triple-negative or germline-associated cases [21].
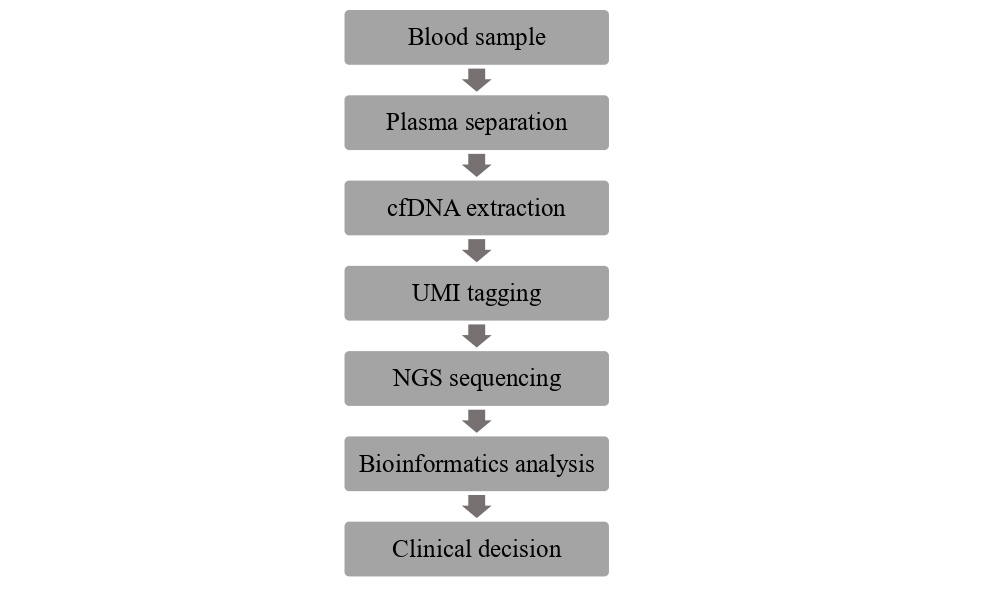
3.4. Liquid Biopsy: The Non-Invasive Diagnostic Revolution
3.4.1. Molecular Residual Disease (MRD) and the "Lead Time"
3.4.2. Clonal Evolution and the "Dynamic Biopsy"
3.5. The Bioinformatics Engine: From Raw Data to Clinical Report
- The Pipeline: Raw data must be aligned to the human reference genome (GRCh38). Sophisticated algorithms like BWA-MEM or Bowtie2 are used for alignment, followed by variant calling with tools like GATK or MuTect2.
- Unique Molecular Identifiers (UMIs): In liquid biopsy, where the signal is very weak, UMIs are used to label each DNA fragment before sequencing. This allows the computer to distinguish between a real mutation and a sequencing error, pushing the sensitivity to unprecedented levels [9].
- Artificial Intelligence (AI) and Machine Learning: AI models are being trained to integrate digital pathology slides (H&E) with NGS data. These "multi-modal" AI tools can predict survival outcomes better than any single test. AI also assists in solving the "Variant of Uncertain Significance" (VUS) problem by simulating the structural impact of a mutation on the protein's fold.
3.6. Socio-Economic Barriers and the Ethical Landscape
- The Genomic Divide: The high cost of NGS (often >$3,000 per test) creates a gap between high-income and low-income healthcare systems. This creates a moral imperative to reduce costs and standardize protocols globally.
- Incidental Findings: Sequencing can reveal germline mutations (e.g., BRCA1/2 or TP53) that have implications for the patient's family [21]. This requires robust genetic counseling services and clear institutional policies on "the right to know."
4. Conclusions and Future Directions
- Interventional Genomics: Clinical trials must now prioritize treating patients based on MRD status rather than waiting for radiological recurrence.
- Multi-modal AI Integration: The future lies in combining "spatial transcriptomics" with serial liquid biopsy to create "digital twins" of patient tumors.
- Equitable Precision Medicine: Standardizing bioinformatics and reducing sequencing costs is vital to bridge the "genomic divide" and ensure global access.
Funding
Authors’ Contributions
Ethics approval and consent to participate
Consent for publication
Availability of data and materials
Competing interests
Abbreviations
| ADC | Antibody-Drug Conjugate |
| BC | Breast Cancer |
| ctDNA | Circulating tumor DNA |
| IHC | Immunohistochemistry |
| MRD | Molecular Residual Disease |
| NGS | Next-Generation Sequencing |
| TMB | Tumor Mutational Burden |
| UMI | Unique Molecular Identifier |
| VAF | Variant Allele Frequency |
| VUS | Variant of Uncertain Significance |
| WES | Whole Exome Sequencing |
References
- Sung, H; Ferlay, J; Siegel, RL; et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021, 71(3), 209–249. [Google Scholar] [CrossRef]
- Wolff, AC; Hammond, MEH; Allison, KH; et al. Human epidermal growth factor receptor 2 testing in breast cancer: ASCO/CAP guideline update. Arch Pathol Lab Med. 2018, 142(11), 1364–1382. [Google Scholar] [CrossRef]
- Allison, KH; Hammond, MEH; Dowsett, M; et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J Clin Oncol. 2020, 38(12), 1346–1366. [Google Scholar] [CrossRef] [PubMed]
- Prat, A; Perou, CM. Deconstructing the molecular portraits of breast cancer. Breast 2015, 24 (Suppl 2), S3–S9. [Google Scholar] [CrossRef]
- Pantel, K; Alix-Panabières, C. Liquid biopsy and minimal residual disease — latest advances and implications for cure. Nat Rev Clin Oncol. 2019, 16(7), 409–424. [Google Scholar] [CrossRef]
- Razavi, P; Chang, MT; Xu, G; et al. The genomic landscape of endocrine-resistant advanced breast cancers. Cancer Cell. 2018, 34(3), 427–438.e6. [Google Scholar] [CrossRef]
- Turner, NC; Swift, C; Kilburn, L; et al. ESR1 mutations are associated with endocrine resistance in advanced breast cancer. J Clin Oncol. 2017, 35(14), 1454–1462. [Google Scholar] [CrossRef]
- Coombes, RC; Page, K; Salari, R; et al. Personalized detection of circulating tumor DNA antedates breast cancer metastatic recurrence. Clin Cancer Res. 2019, 25(14), 4255–4263. [Google Scholar] [CrossRef]
- Murtaza, M; Dawson, SJ; Tsui, DWY; et al. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature 2013, 497(7447), 108–112. [Google Scholar] [CrossRef] [PubMed]
- Sparano, JA; Gray, RJ; Makower, DF; et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med. 2018, 379(2), 111–121. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F; van’t Veer, LJ; Bogaerts, J; et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016, 375(8), 717–729. [Google Scholar] [CrossRef] [PubMed]
- André, F; Ciruelos, E; Rubovszky, G; et al. Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N Engl J Med. 2019, 380(20), 1929–1940. [Google Scholar] [CrossRef]
- Modi, S; Jacot, W; Yamashita, T; et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022, 387(1), 9–20. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M; Turner, NC; Bondarenko, I; et al. Fulvestrant plus ribociclib for advanced hormone receptor-positive breast cancer. Lancet Oncol. 2018, 19(7), 904–915. [Google Scholar] [CrossRef]
- Turner, NC; Ro, J; André, F; et al. Palbociclib in hormone-receptor-positive advanced breast cancer. N Engl J Med. 2015, 373(3), 209–219. [Google Scholar] [CrossRef]
- Johnston, SRD; Harbeck, N; Hegg, R; et al. Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2− breast cancer (monarchE). J Clin Oncol. 2020, 38(34), 3987–3998. [Google Scholar] [CrossRef]
- Tolaney, SM; Saura, C; Krop, IE; et al. Adjuvant abemaciclib in high-risk early breast cancer. N Engl J Med. 2023, 388(5), 395–407. [Google Scholar] [CrossRef]
- Rugo, HS; Bardia, A; Tolaney, SM; et al. Efficacy of sacituzumab govitecan in hormone receptor-positive/HER2-negative metastatic breast cancer. J Clin Oncol. 2022, 40(29), 3365–3376. [Google Scholar] [CrossRef]
- Bardia, A; Hurvitz, SA; Tolaney, SM; et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021, 384(16), 1529–1541. [Google Scholar] [CrossRef]
- Parsons, HA; Beaver, JA; Park, BH. Circulating plasma tumor DNA. Clin Cancer Res. 2016, 22(12), 2843–2850. [Google Scholar] [CrossRef]
- Hunter, DJ; Easton, DF. The genetic architecture of breast cancer. Nature 2021, 594(7862), 41–48. [Google Scholar] [CrossRef]
- Marusyk, A; Janiszewska, M; Polyak, K. Intratumor heterogeneity: the rosetta stone of therapy resistance. Nat Cancer 2020, 1(5), 463–475. [Google Scholar] [CrossRef] [PubMed]

| Assay | Gene Count | Patient Population | Key Trial | Evidence Level | Reference |
|---|---|---|---|---|---|
| Oncotype DX | 21 | HR+/HER2- early BC | TAILORx | Level I | [10] |
| MammaPrint | 70 | Stage I-II BC | MINDACT | Level I | [11] |
| Prosigna | 50 | Postmenopausal HR+ | TransATAC | Level II | [4] |
| Mutation | Pathway | Targeted Therapy | Clinical Utility | Reference |
|---|---|---|---|---|
| PIK3CA | PI3K/AKT/mTOR | Alpelisib | Advanced HR+ BC | [12] |
| ESR1 | Estrogen Receptor | Elacestrant | Endocrine Resistance | [7] |
| BRCA1/2 | DNA Repair | PARP Inhibitors | Triple Negative/Germline | [21] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



