
Submitted:
06 February 2026
Posted:
10 February 2026
You are already at the latest version
Abstract
Background: High-dose chemotherapy (HDCT) followed by autologous stem cell transplantation (ASCT) is an established salvage therapy for relapsed or refractory (R/R) germ cell tumors (GCTs). Methods: We conducted a retrospective analysis of 9 patients (23-41 years of age) with relapsed/refractory (R/R) GCTs treated according to the Swedish-Norwegian Testicular Cancer Group Clinical Protocol (SWENOTECA), at the Specialized Hospital for Active Treatment of Hematological Diseases (SHATHD) in Sofia, Bulgaria. The study evaluates the efficacy and safety of HDCT followed by ASCT in R/R GCTs eligible for second-line consolidation. Results: The median follow-up was 39.3 months. Following ASCT, the overall response rate (ORR) was 33.3%, consisting entirely of complete responses (CR). The 1-year OS and PFS were both 44.4%. Notably, Kaplan-Meier curves for OS and PFS reached a plateau after 24 months (33.3%), showing that long-term durable remission in these patients is achievable. Although grade 3–4 toxicities were observed, there was no treatment-related mortality. Conclusion: Tandem HDCT followed by ASCT is a safe and effective salvage strategy for R/R GCTs, offering predictable toxicity and curative potential, which is proven by the observed survival plateau. While tandem cycles are the current standard, the upcoming TIGER trial results will determine the future necessity of further intensification.
Keywords:
germ cell tumors
; high dose chemotherapy
; autologous stem cell transplantation
1. Introduction
Germ cell tumors (GCTs) are the most common solid malignancies in young men aged 15–45 years. Diagnosis and disease staging are performed in accordance to the established international guidelines provided by the National Comprehensive Cancer Network (NCCN) [1] and the European Society for Medical Oncology (ESMO) [2]. The clinical prognosis and risk stratification are primarily determined by the International Germ Cell Consensus Classification (IGCCCG) [3], which was validated in a large-scale analysis by Einhorn et al. [3]. More recent updates to this classification continue to refine risk categories for metastatic cases [4].
Published data have shown that the treatment of GCTs is exceptionally successful: the cure rate in early stages often exceeds 95% [5], and even in metastatic forms, it reaches 80–90% [2]. Radical inguinal orchiectomy is the first mandatory step in the treatment of the primary tumor, serving simultaneously for diagnosis and therapy. After the operation, the subsequent treatment depends on the histological variant of the tumor and its stage. For early stage disease (I), the most common approach is active surveillance. Alternatively, adjuvant chemotherapy, usually a single course with carboplatin, can be administered to reduce the risk of relapse. For advanced stage (II and III), the main method is Platinum-based chemotherapy, most often administered through the BEP regimen (bleomycin, etoposide, cisplatin). Radiotherapy is used less frequently today, but it can be effective for certain cases in stage II.
The clinical management of relapsed/refractory (R/R) GCTs remains a subject of active debate, centered on the choice between standard chemotherapy and HDCT followed by ASCT [6]. While GCTs are highly sensitive to cisplatin, the prognosis for primary refractory cases remains dismal, necessitating dose-intensive consolidation strategies like tandem HDCT. Retrospective data, most notably from the Indiana University [7] and large analyses of the Center for International Blood and Marrow Transplant Research (CIBMTR) / European Society for Blood and Marrow Transplantation (EBMT) [8], suggest that HDCT and ASCT provide superior long-term survival, particularly when utilized as an early salvage intervention. Tandem HDCT cycles aim to maximize dose intensity while mitigating cumulative organ toxicity [9].
In Northern Europe and Scandinavia, the SWENOTECA Group [10] has established robust management guidelines that have standardized the approach to GCTs. The SWENOTECA protocols emphasize a risk-adapted strategy, ensuring that patients at high risk of failure receive intensified treatment early in their clinical course.
In Bulgaria, the implementation of such intensive protocols at a single-center level requires significant coordination between oncology, hematology, and transplant units. At the SHATHD in Sofia, we have adopted the HDCT approach as a consolidation strategy for R/R GCT patients. This study aims to provide a detailed analysis of our single-center experience with tandem HDCT/ASCT. By presenting our clinical outcomes and toxicity profiles, we aim to contribute to the growing evidence regarding the feasibility and efficacy of this intensive treatment in Eastern European clinical practice, particularly focusing on long-term survival and the management of treatment-related complications.
2. Materials and Methods
2.1. Study Design and Population
We conducted a retrospective, single-center study, which included nine male patients with R/R GCTs referred to our HSCT center at SHATHD by their treating oncologist between 2019 and 2022. All patients were candidates for tandem cycles of HDCT followed by ASCT after failing at least one line of platinum-based chemotherapy. Eligibility was based on standard institutional protocol. All patients achieved successful PBSC mobilization with a target CD34+ yield of 5–7 × 10⁶/kg (minimum 2 × 10⁶/kg per cycle) and provided signed informed consent. The study was approved by the local Ethics review board.
2.2. Treatment Protocol
The therapeutic strategy followed the SWENOTECA IV protocol. The tandem regimen consisted of two distinct HDCT cycles:
- Cycle 1: Carboplatin 7 x (GFR+25), max 800 mg (Day 1-4), Cyclophosphamide 1500 mg/m² (Day 1-4), and Etoposide 440 mg/m² (Day 1-4).
- Cycle 2: Carboplatin 7 x (GFR+25), max 800 mg (Day 1-4), Cyclophosphamide 1500 mg/m² (Day 1-4) and Thiotepa 120 mg/m² (Day 1-4).
Peripheral blood stem cells (PBSC) were mobilized during second-line salvage therapy by chemo-mobilization (77.8%) or G-CSF alone (22.2%). The target CD34+ cell count was set at 5–7 × 10⁶/kg to ensure sufficient cell dose for both cycles.
2.3. Statistical Analysis
The primary endpoints were OS and PFS, calculated from the date of the first ASCT. Survival probabilities were estimated using the Kaplan-Meier method. Statistical analysis was performed using Python (version 3.10) utilizing the lifelines library for survival modeling. Toxicities were graded according to the NCI Common Terminology Criteria for Adverse Events (CTCAE) v5.0 [11].
3. Results
3.1. Patient Characteristics and Mobilization
A total of nine male patients with relapsed or refractory (R/R) germ cell tumors were included in this analysis. The median age at the time of the first ASCT was 34 years (range 23–41). Patient characteristics are summarized in Table 1. At initial diagnosis, 66.7% of patients presented with metastatic disease (T2N2M1). All patients had previously undergone radical inguinal orchiectomy and received first-line BEP/EP regimens. Unfortunately, only 2 (22.3%) of patients achieved an objective response – 1 (11.15%) complete response (CR) and 1 (11.15%) partial response (PR), while 6 (77.7%) had a stable or progressive disease. Consequently, the patients proceeded to second line therapy according to TIP (Paclitaxel, Ifosfamide, Cisplatin) or PEI (Cisplatin, Etoposide, Ifosfamide) protocols, followed by HDCT and ASCT. The only one patient in CR1 experienced a rapid morphological relapse prior to ASCT. Half of patients (55.5%) achieved partial or complete response to second-line salvage (TIP/PEI), while 44.5% had stable or progressive diseases. Stem cell mobilization was successful in all patients with a mean CD34+ yield of 8.38 × 10⁶/kg. Mobilization was primarily achieved using chemotherapy plus G-CSF (77.7%), while 22.3% of patients required G-CSF alone.
3.2. Survival and Response
With a median follow-up of 39.3 months, the median OS was 8.4 months and the median PFS was 5.9 months. The ORR post-ASCT was 33.3%, with all responders achieving CR. Kaplan-Meier analysis (Figure 1A, 1B) demonstrated a 1-year OS and PFS of both 44.4% with the majority of events concentrated in the early post-transplant period. Notably, the survival curve reached a stable plateau after the initial 18-month high-risk window, suggesting that patients, who remain progression-free at this time point achieve durable long-term remission.
3.3. Safety and Engraftment
Hematopoietic recovery was comparable after both ASCT. Mean neutrophil engraftment occurred on day 14 for both Cycle 1 and Cycle 2. Platelet recovery (>20 × 10⁹/L) was achieved on days 18 and 16, respectively.
The cumulative safety profile was evaluated by documenting adverse events from both transplantation cycles, as shown in Table 2. The toxicity profile was significant, but manageable. Hematological toxicity was universal, with all patients reaching Grade 4 neutropenia and thrombocytopenia. Febrile neutropenia occurred in 88.9% of cases but was successfully resolved with standard antibiotic treatment protocols. Grade 2-3 mucositis and diarrhea were frequently reported. Cumulative renal toxicity from prior heavy cisplatin exposure was a significant consideration for patient eligibility and management in our cohort. In our series, Grade 3–4 nephrotoxicity (according to CTCAE v5.0) was observed in one patient (11.1%), who required temporary hemodialysis. This underscores the necessity for rigorous monitoring of glomerular filtration rate (GFR) and aggressive hydration protocols during tandem ASCT to mitigate the risks of irreversible renal failure. Most importantly, there was no treatment-related mortality (TRM), with 100% of patients surviving the treatment. These findings demonstrate that, despite the intensive nature of the regimen, the associated toxicities are predictable and can be effectively managed by multidisciplinary teams.
4. Discussion
The management of R/R GCTs remains a clinical challenge, particularly in patients who show limited response to initial salvage chemotherapy. Our study confirms that the tandem HDCT approach, established by the SWENOTECA group, is a feasible and safe strategy even in a heavily pre-treated cohort.
4.1. Comparative Efficacy and Population Risk
Our observed 2-year OS of 33.3% is lower than the 63–66% reported by the Indiana University group [7]. However, this discrepancy is likely attributable to the high-risk nature of our small cohort; 44.4% of our patients entered ASCT with stable or progressive disease (SD/PD), whereas the best outcomes in literature are typically seen in patients who are “platinum-sensitive” or at least in partial remission before HDCT [12]. Nevertheless, the survival plateau we observed at 24-month aligns with international data, suggesting that HDCT has curative potential in a subset of
Our observed complete response (CR) rate of 33.3% is consistent with several international reports, although it is on the lower end compared to high-volume centers of excellence. For instance, the landmark study by Einhorn et al., which utilized tandem HDCT as a second-line or later salvage treatment, reported a long-term remission rate of approximately 60%. Similarly, the TICE protocol (Paclitaxel, Ifosfamide followed by High-dose Carboplatin and Etoposide) has demonstrated impressive durable response rates.
The discrepancy between our results and these major trials can likely be attributed to the high proportion of patients with primary refractory disease in our cohort. Specifically, over 55% of our patients exhibited progressive disease (PD) during or immediately after first-line BEP therapy. According to the International Prognostic Factors Study Group (IPFSG) criteria, these patients fall into the high-risk or very high-risk categories, where survival outcomes are significantly compromised regardless of the salvage strategy employed.
4.2. The Safety of the Tandem Approach
The most striking finding in our study is the absence of TRM. In larger multicenter series, TRM for HDCT typically ranges from 3,5% to 7% [7,13]. Our results demonstrate that with rigorous supportive care and a multidisciplinary team, the significant toxicities of high-dose Carboplatin and Thiotepa (including febrile neutropenia and mucositis) can be effectively mitigated. The stability of engraftment between the first and second cycles also proves that the bone marrow microenvironment is not prohibitively damaged by the initial high dose burst.
4.3. Biological Rationale for Tandem Transplantation and Future Trends (The TIGER Trial) [14]
The choice of a tandem (double) transplant approach, as advocated by the SWENOTECA guidelines and implemented in our center, is based on the biological principle of maximizing the cumulative dose of platinum agents while allowing for hematological recovery between cycles. This “dose-intensive” strategy is specifically designed to eradicate chemoresistant clones that might survive a single cycle of high-dose therapy. However, the high mortality observed in our cohort (6 out of 9 patients) underscores that even the most intensive consolidation cannot always overcome the aggressive biology of primary refractory germ cell tumors (GCTs).A key point of current debate is the optimal number of HDCT cycles. While our institutional protocol utilizes a tandem (2-cycle) approach, the international community is closely monitoring the ongoing Phase III TIGER trial. This trial is evaluating a 3-cycle TI-CE (Paclitaxel, Ifosfamide, Carboplatin, Etoposide) regimen as a first-line salvage treatment. The 3-cycle approach theoretically increases dose intensity but also raises concerns regarding cumulative toxicity, increased demand for CD34+ stem cells, and longer hospital stays.
Our data show that a tandem approach provides a robust yield of CD34+ cells and a manageable toxicity profile, making it a viable option in a real-world clinical setting. If the TIGER trial results eventually demonstrate a significant survival advantage for three cycles of HDCT, a shift in international protocols may be warranted. However, for centers treating highly refractory patients with limited physiological reserves, the tandem approach remains a validated, potent, and potentially safer standard.
4.4. The Bulgarian Context and Single-Center Limitations
To our knowledge, this is one of the few reports detailing the use of tandem ASCT for GCTs in Eastern Europe. The implementation of such protocols in Bulgaria faces unique challenges, including access to specialized salvage agents and the logistical burden of stem cell cryopreservation for multiple cycles.
The primary limitations of this study are its retrospective nature and the small sample size (N=9). However, as a single-center experience in a specialized setting, it provides valuable real-world data on the implementation of intensive SWENOTECA protocols outside of Scandinavian populations.
4.5. Future Directions
Moving forward, better patient selection is paramount. Emerging biomarkers, such as serum microRNA-371a-3p (miR-371) [15], may in the future help clinicians identify earlier those patients who are likely to fail conventional salvage therapy and who should be fast-tracked to HDCT. Additionally, for patients with platinum-refractory disease, exploring the role of novel agents or immunotherapy in combination with HDCT remains a promising area for clinical research [16].
5. Conclusions
Tandem HDCT followed by ASCT is an intensive but safe salvage therapy for patients with recurrent or refractory germ cell tumors. The procedure is characterized by predictable toxicities and excellent hematopoietic recovery. While long-term survival is lower in highly refractory cases, the achievement of a survival plateau confirms the curative potential of this treatment. Future results from the TIGER trial will further refine whether intensification to three cycles of HDCT and ASCT should become the new international standard.
In conclusion, our single-center experience confirms that tandem HDCT with ASCT is a feasible and potentially curative salvage strategy for patients with relapsed and refractory germ cell tumors in Bulgaria. Despite the small cohort, the observed survival plateau after 24 months suggests that long-term remission is achievable even in heavily pre-treated patients. Future efforts should focus on early identification of high-risk patients using molecular biomarkers to optimize the timing of this intensive intervention.
Author Contributions
Conceptualization, K.K.; methodology, I.T.; validation, K.V.; formal analysis, K.K.; investigation, M.M and I.T.; resources, K.V.; data curation, K.V.; writing—original draft preparation, K.K.; writing—review and editing, A.B.; supervision, G.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Any research article Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ASCT | Autologous Stem Cell Transplantation |
| BEP | Bleomycin, Etoposide, Platinum |
| CIBMTR | Center for International Blood and Marrow Transplant Research |
| CR | Complete Response |
| CTCAE | Common Terminology Criteria for Adverse Events |
| EBMT | European Society for Blood and Marrow Transplantation |
| EP | Etoposide, Platinum |
| ESMO | European Society for Medical Oncology |
| GCTs | Germ Cell Tumors |
| HDCT | High-Dose Chemotherapy |
| HSCT | Hematopoietic Stem Cell Transplantation |
| IGCCCG | International Germ Cell Consensus Classification |
| NCCN | National Comprehensive Cancer Network |
| ORR | Overall Response Rate |
| OS | Overall Survival |
| PBSC | Peripheral Blood Stem Cells |
| PEI | Cisplatin, Etoposide, Ifosfamide |
| PFS | Progression-Free Survival |
| PR | Partial Response |
| R/R | Relapsed or Refractory |
| SD/PD | Stable Disease / Progressive Disease |
| SHATHD | Specialized Hospital for Active Treatment of Hematological Diseases |
| SWENOTECA | Swedish-Norwegian Testicular Cancer Group |
| TI-CE | Paclitaxel, Ifosfamide, Carboplatin, Etoposide |
| TIP | Paclitaxel, Ifosfamide, Cisplatin |
| TRM | Treatment-Related Mortality |
References
- National Comprehensive Cancer Network (NCCN). Testicular Cancer (Version 1. 2024. Available online: https://www.nccn.org/guidelines/category_1.
- Oldenburg, J.; Fosså, S.D.; Nuver, J.; Heidenreich, A.; Schmoll, H.-J.; Bokemeyer, C.; Horwich, A.; Beyer, J.; Kataja, V. Testicular seminoma and non-seminoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi125–vi132. [Google Scholar] [CrossRef] [PubMed]
- International Germ Cell Consensus Classification: a prognostic factor-based staging system for metastatic germ cell cancers. International Germ Cell Cancer Collaborative Group. J. Clin. Oncol. 1997, 15, 594–603. [CrossRef] [PubMed]
- Gillessen, S.; Sauvé, N.; Collette, L.; Daugaard, G.; de Wit, R.; Albany, C.; Tryakin, A.; Fizazi, K.; Stahl, O.; Gietema, J.A.; et al. Predicting Outcomes in Men With Metastatic Nonseminomatous Germ Cell Tumors (NSGCT): Results From the IGCCCG Update Consortium. J. Clin. Oncol. 2021, 39, 1563–1574. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, T; Seidenfeld, J. Testicular Cancer: Diagnosis, Staging, and Treatment. ASCO Educational Book 2012, 32, e54–e59. [Google Scholar] [CrossRef]
- Honecker, F.; Aparicio, J.; Berney, D.; Beyer, J.; Bokemeyer, C.; Cathomas, R.; Clarke, N.; Cohn-Cedermark, G.; Daugaard, G.; Dieckmann, K.-P.; et al. ESMO Consensus Conference on testicular germ cell cancer: diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, 1658–1686. [Google Scholar] [CrossRef] [PubMed]
- Einhorn, L.H.; Williams, S.D.; Chamness, A.; Brames, M.J.; Perkins, S.M.; Abonour, R. High-Dose Chemotherapy and Stem-Cell Rescue for Metastatic Germ-Cell Tumors. New Engl. J. Med. 2007, 357, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Kilari, D.; D'SOuza, A.; Fraser, R.; Qayed, M.; Davila, O.; Agrawal, V.; Diaz, M.A.; Chhabra, S.; Cerny, J.; Copelan, E.; et al. Autologous Hematopoietic Stem Cell Transplantation for Male Germ Cell Tumors: Improved Outcomes Over 3 Decades. Biol. Blood Marrow Transplant. 2019, 25, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Nichols, C.R.; Andersen, J.; Lazarus, H.M.; Fisher, H.; Greer, J.; A Stadtmauer, E.; Loehrer, P.J.; Trump, D.L. High-dose carboplatin and etoposide with autologous bone marrow transplantation in refractory germ cell cancer: an Eastern Cooperative Oncology Group protocol. J. Clin. Oncol. 1992, 10, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Haugnes, H.S.; Laurell, A.; Stierner, U.; Bremnes, R.M.; Dahl, O.; Cavallin-Ståhl, E.; Cohn-Cedermark, G. High-dose chemotherapy with autologous stem cell support in patients with metastatic non-seminomatous testicular cancer – a report from the Swedish Norwegian Testicular Cancer Group (SWENOTECA). Acta Oncol. 2011, 51, 168–176. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. 2017. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf.
- The International Prognostic Factors Study Group Prognostic Factors in Patients With Metastatic Germ Cell Tumors Who Experienced Treatment Failure With Cisplatin-Based First-Line Chemotherapy. J. Clin. Oncol. 2010, 28, 4906–4911. [CrossRef] [PubMed]
- Pico, J.-L.; Rosti, G.; Kramar, A.; Wandt, H.; Koza, V.; Salvioni, R.; Theodore, C.; Lelli, G.; Siegert, W.; Horwich, A.; et al. A randomised trial of high-dose chemotherapy in the salvage treatment of patients failing first-line platinum chemotherapy for advanced germ cell tumours. Ann. Oncol. 2005, 16, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Randomized Phase III Trial of TIP vs. High-Dose Chemotherapy (TI-CE) as First-Line Salvage Treatment for GCT (TIGER). 2015. Available online: https://clinicaltrials.gov/ct2/show/NCT02375204.
- Dieckmann, K.-P.; Radtke, A.; Geczi, L.; Matthies, C.; Anheuser, P.; Eckardt, U.; Sommer, J.; Zengerling, F.; Trenti, E.; Pichler, R.; et al. Serum Levels of MicroRNA-371a-3p (M371 Test) as a New Biomarker of Testicular Germ Cell Tumors: Results of a Prospective Multicentric Study. 70th Congress of the German-Society-of-Urology; LOCATION OF CONFERENCE, COUNTRYDATE OF CONFERENCE; pp. 1412–1423.
- Adra, N.; Einhorn, L.; Althouse, S.; Ammakkanavar, N.; Musapatika, D.; Albany, C.; Vaughn, D.; Hanna, N. Phase II trial of pembrolizumab in patients with platinum refractory germ-cell tumors: a Hoosier Cancer Research Network Study GU14-206. Ann. Oncol. 2017, 29, 209–214. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A. Overall Survival (OS); B. Progression-Free Survival (PFS).
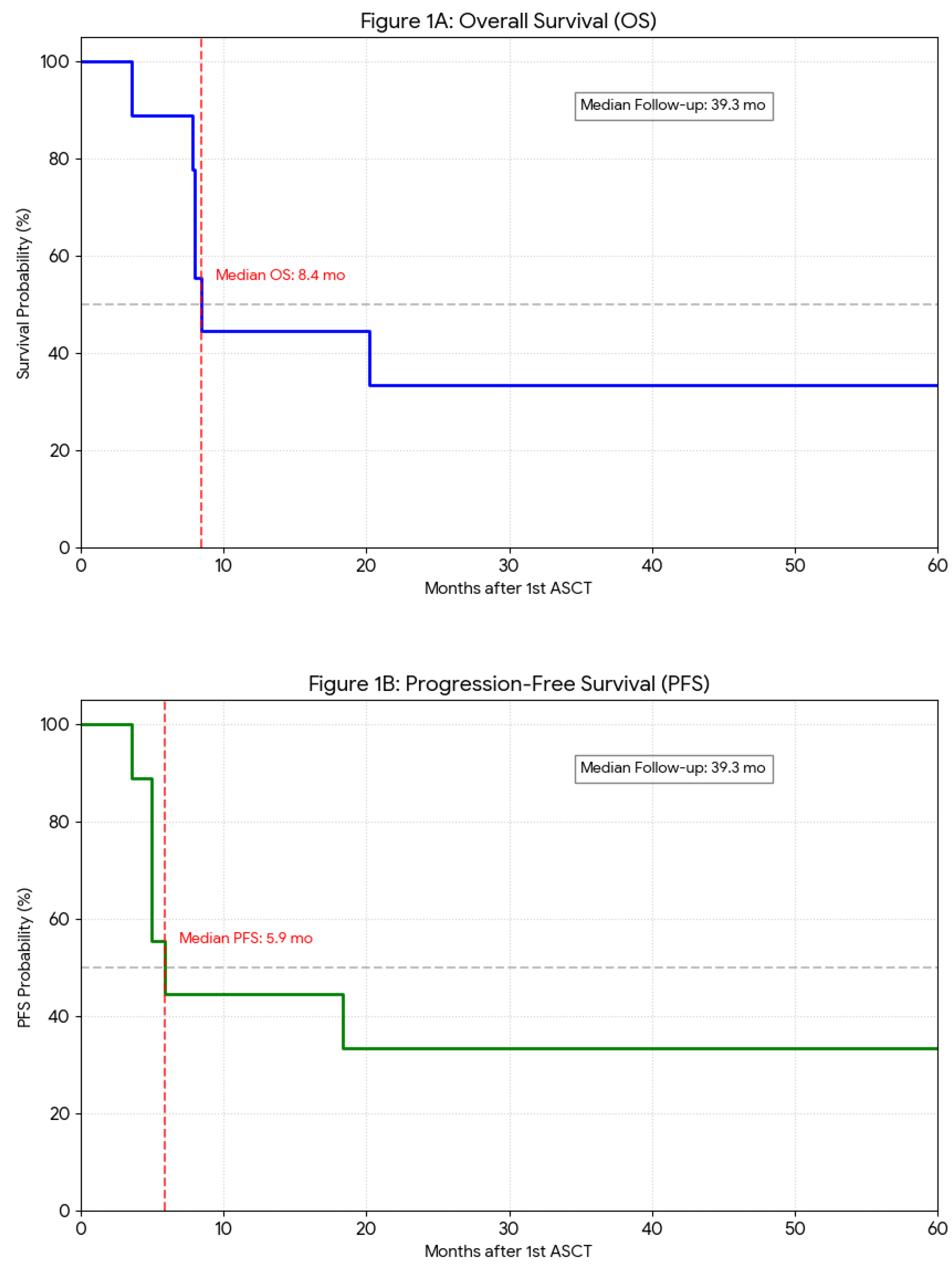

Table 1.
Treatment characteristics and outcomes.
| Characteristics First Line Therapy BEP PEI |
Patients, N=9 5 (55.5) 4 (44.5) |
| Response assessment after 1st line therapy, n (%) | |
| CR+PR | 2 (22.3) |
| SD+PD Second Line Therapy TIP PEI |
7 (77.7) 8 (88.8) 1 (11.1) |
| Mobilization regimen, n (%) | |
| CT + G-CSF | 7 (77.7) |
| G-CSF | 2 (22.3) |
| Response assessment before HSCT, n (%) | |
| CR+PR | 5 (55.5) |
| SD | 3 (33.3) |
| PD | 1 (11.1) |
| Response assessment after HSCT, n (%) | |
| CR | 3 (33.3) |
| PD | 5 (55.5) |
| NA | 1 (11.1) |
Table 2.
Cumulative Adverse Events observed during the first and second ASCT cycles (N=9).
| Adverse Event | All Grades, n (%) | Grade 3–4, n (%) |
| Gastrointestinal (GI) | ||
| Mucositis | 9 (100%) | 2 (22.2%) |
| Nausea/Vomiting | 9 (100%) | 2 (22.2%) |
| Erosive gastritis | 2 (22.2%) | 1 (11.1%) |
| Toxic colitis | 1 (11.1%) | 1 (11.1%) |
| Systemic & Organ Toxicities | ||
| Febrile neutropenia | 8 (88.9%) | 1 (11.1%) |
| Infections | 7 (77.8%) | 2 (22.2%) |
| Hepatotoxicity | 2 (22.2%) | 0 (0%) |
| Nephrotoxicity | 2 (22.2%) | 1 (11.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



