Submitted:
04 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
Background: In many low- and middle-income countries, access to advanced cardiac biomarkers such as B-type natriuretic peptide (BNP) and NT-proBNP remains limited. This constraint poses a challenge for early risk stratification in patients hospitalized with acute heart failure (AHF). Therefore, identifying simple, inexpensive, and universally available laboratory markers with prognostic value is of practical clinical importance. Methods: We retrospectively analyzed consecutive patients hospitalized with AHF between May 2022 and November 2024. After exclusion of patients with incomplete outcome data, in-hospital mortality was assessed using logistic regression analysis. Hemoglobin, serum albumin, lactate dehydrogenase (LDH), neutrophil-to-lymphocyte ratio (NLR), and the C-reactive protein–albumin–lymphocyte (CALLY) index were evaluated as potential predictors of in-hospital mortality. Results: A total of 211 patients were included in the mortality analysis, with an in-hospital mortality rate of 10.0%. Patients were stratified based on anemia and hypoalbuminemia status, revealing significant differences in unadjusted mortality rates across groups (P = 0.04). However, after adjustment for age, sex, and chronic kidney disease, the prognostic impact of anemia and hypoalbuminemia was attenuated. Elevated LDH remained independently associated with in-hospital mortality (adjusted odds ratio 2.84, 95% confidence interval 1.01–8.02). Higher NLR values and lower CALLY index levels showed nonsignificant trends toward adverse outcomes. Conclusions: In this real-world cohort from a resource-limited setting, LDH emerged as a practical and independent predictor of in-hospital mortality in AHF. When access to natriuretic peptides is limited, LDH—supported by routinely available laboratory parameters—may assist early risk stratification and clinical decision-making.
Keywords:
acute heart failure
; lactate dehydrogenase
; low-cost biomarkers
; in-hospital mortality
; risk stratification
; resource-limited settings
Introduction
Acute heart failure (AHF) remains a major global health problem and continues to be associated with substantial morbidity and mortality despite advances in pharmacological and device-based therapies.¹–³ These outcomes are disproportionately worse in low- and middle-income countries, where delayed presentation, limited access to specialized care, and restricted diagnostic resources complicate optimal management.⁴
Risk stratification plays a central role in the early management of AHF. In contemporary practice, natriuretic peptides such as BNP and NT-proBNP are widely used to aid diagnosis and prognostication.⁵ However, in many healthcare systems—including several regions in Africa, the Middle East, and parts of Eastern Europe—routine measurement of these biomarkers is often unavailable due to financial and infrastructural constraints.⁶ In such settings, clinicians must rely on basic laboratory parameters that are readily accessible and inexpensive.
Anemia and hypoalbuminemia are frequently observed in patients hospitalized with AHF and reflect distinct but overlapping pathophysiological mechanisms. Anemia may exacerbate myocardial hypoxia and neurohormonal activation, whereas hypoalbuminemia is associated with systemic inflammation, malnutrition, venous congestion, and impaired hepatic synthesis.⁷–¹¹ Although both conditions have been linked to adverse outcomes in heart failure, their independent and combined prognostic value in acute settings remains inconsistent across studies.¹²–¹⁵
Recently, attention has shifted toward low-cost inflammatory and nutritional biomarkers that are universally available, even in resource-limited hospitals. Among these, the neutrophil-to-lymphocyte ratio (NLR) and the C-reactive protein–albumin–lymphocyte (CALLY) index have been proposed as markers of systemic inflammation and immune dysregulation in cardiovascular disease.¹⁶–²⁰ Lactate dehydrogenase (LDH), a marker of tissue hypoxia and cellular injury, has also emerged as a potential indicator of short-term mortality in AHF, particularly in patients with hemodynamic compromise.²¹–²⁴
Importantly, limitations in access to advanced biomarkers are not confined to a single geographic region. Similar challenges are encountered in several middle-income countries, where pragmatic and reproducible prognostic tools remain clinically relevant.²⁵ Identifying simple laboratory parameters with incremental prognostic value may therefore contribute to more equitable heart failure care across diverse healthcare systems.
Accordingly, this study aimed to evaluate the prognostic significance of commonly available laboratory markers—including hemoglobin, albumin, LDH, NLR, and the CALLY index—for predicting in-hospital mortality among patients hospitalized with AHF in a real-world, resource-limited setting.
Importantly, acute heart failure should not be viewed as an isolated entity, but rather as a critical phase within the continuum of chronic heart failure.¹,² Episodes of acute decompensation often reflect progression of underlying chronic disease and are associated with substantial short- and long-term mortality.¹–³ Early risk stratification during hospitalization may therefore influence not only in-hospital management but also subsequent chronic heart failure care.² In this context, identifying pragmatic and widely available biomarkers with prognostic value during acute presentations remains highly relevant to the broader field of chronic heart failure.³
Materials and Methods
Study Design and Setting
This retrospective observational study was conducted at Mogadishu Somali–Turkey Recep Tayyip Erdoğan Training and Research Hospital, one of the largest tertiary referral centers in Somalia. The hospital serves as a major regional center in a resource-limited healthcare environment, where access to advanced cardiac biomarkers such as B-type natriuretic peptide (BNP) or NT-proBNP is not routinely available due to laboratory and financial constraints.
The study protocol was approved by the local Institutional Review Board (Approval No: MSTH/20379, Date: 07 December 2024). Given the retrospective design and use of anonymized data, the requirement for informed consent was waived. All procedures were conducted in accordance with the Declaration of Helsinki.
Study Population
Consecutive adult patients (≥18 years) hospitalized with a primary diagnosis of acute heart failure (AHF) between May 2022 and November 2024 were screened for eligibility. Acute heart failure was diagnosed based on acute onset or worsening of heart failure symptoms requiring hospital admission, supported by clinical assessment and imaging findings consistent with congestion.
Patients were excluded if:
- in-hospital outcome data were unavailable (n = 9),
- they presented with severe concomitant infections,
- they had acute coronary syndromes requiring immediate revascularization,
- they had active malignancy at the time of admission.
After applying these criteria, 211 patients were included in the final analysis of in-hospital mortality. Subgroup analyses evaluating anemia and hypoalbuminemia were restricted to patients with complete hemoglobin and serum albumin measurements at admission (n = 141) to avoid imputation-related bias. The patient selection process is summarized in Figure 1.
Clinical and Laboratory Data Collection
Demographic characteristics, medical history, comorbid conditions, vital signs, and laboratory data were obtained from electronic medical records. All laboratory measurements were derived from blood samples collected within the first 24 hours of hospital admission as part of routine clinical care. For patients with multiple measurements during this period, the first available laboratory values were used for analysis.
Laboratory parameters included hemoglobin, serum albumin, lactate dehydrogenase (LDH), C-reactive protein (CRP), total leukocyte count, neutrophil count, and lymphocyte count. Due to local laboratory limitations, natriuretic peptide measurements (BNP or NT-proBNP) were not available for assessment.
Definitions
Anemia was defined according to World Health Organization criteria as hemoglobin <13 g/dL in men and <12 g/dL in women. Hypoalbuminemia was defined as a serum albumin concentration <3.5 g/dL at admission.
The neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count. The C-reactive protein–albumin–lymphocyte (CALLY) index was calculated using the following formula, as previously described:
CALLY = (albumin × lymphocyte count) / CRP.
Patients were categorized into four groups based on baseline hemoglobin and albumin levels:
- no anemia and no hypoalbuminemia,
- anemia only,
- hypoalbuminemia only,
- both anemia and hypoalbuminemia.
Outcome Measure
The primary outcome of the study was all-cause in-hospital mortality, defined as death from any cause during the index hospitalization.
Statistical Analysis
Statistical analyses were performed using SPSS software version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality using the Kolmogorov–Smirnov test and are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are expressed as frequencies and percentages.
Between-group comparisons were conducted using Student’s t-test or Mann–Whitney U test for continuous variables and chi-square test or Fisher’s exact test for categorical variables, as appropriate.
Univariable logistic regression analyses were initially performed to identify potential predictors of in-hospital mortality. Variables with clinical relevance or a univariable P value <0.10 were entered into multivariable logistic regression models. Multivariable analyses were adjusted for age, sex, and chronic kidney disease. To minimize model overfitting, the number of covariates included in the final model was limited in relation to the number of outcome events. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs).
A two-sided P value <0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 220 patients hospitalized with acute heart failure were included in the study. The mean age of the cohort was 59.5 ± 14.7 years, and 62.7% of patients were male. Chronic kidney disease was present in 13.2% of the population. Overall in-hospital mortality was 10.0%.
Anemia and hypoalbuminemia were common, observed in 68.7% and 54.6% of patients, respectively. Baseline demographic, clinical, and laboratory characteristics of the study population are summarized in Table 1.
Mortality Across Biomarker Subgroups Overall in-hospital mortality was 10.0% (n = 21). Mortality differed significantly across the hemoglobin–albumin subgroups; Mortality across hemoglobin–albumin subgroups is shown in Table 2
Prognostic Value of Hemoglobin and Albumin
In univariable logistic regression analysis, both anemia and hypoalbuminemia were associated with higher in-hospital mortality. However, after adjustment in the multivariable logistic regression model, neither anemia nor hypoalbuminemia retained independent prognostic significance for in-hospital mortality. These findings indicate that although anemia and hypoalbuminemia are associated with adverse outcomes at a crude level, their prognostic effect is largely attenuated after accounting for relevant clinical covariates.
Prognostic Value of LDH, NLR, and the CALLY Index
Elevated lactate dehydrogenase (LDH) levels were significantly more frequent among patients who died during hospitalization compared with survivors (P < 0.01). In multivariable logistic regression analysis, LDH remained the only laboratory marker independently associated with in-hospital mortality (adjusted odds ratio 2.84, 95% confidence interval 1.01–8.02; P = 0.048).
In contrast, inflammatory–nutritional indices showed only nonsignificant trends toward increased mortality. Patients with a high neutrophil-to-lymphocyte ratio (>3.58) and those with a low C-reactive protein–albumin–lymphocyte (CALLY) index (≤0.03) tended to have worse outcomes; however, these associations did not reach statistical significance (P = 0.09 and P = 0.11, respectively).
Multivariable Model Performance
The final multivariable logistic regression model demonstrated acceptable overall discrimination. After adjustment for age, sex, chronic kidney disease, hemoglobin, albumin, neutrophil-to-lymphocyte ratio, and the CALLY index, LDH remained the only laboratory parameter independently associated with in-hospital mortality. Multivariable logistic regression results are presented in Table 3 and visualized in Figure 2.
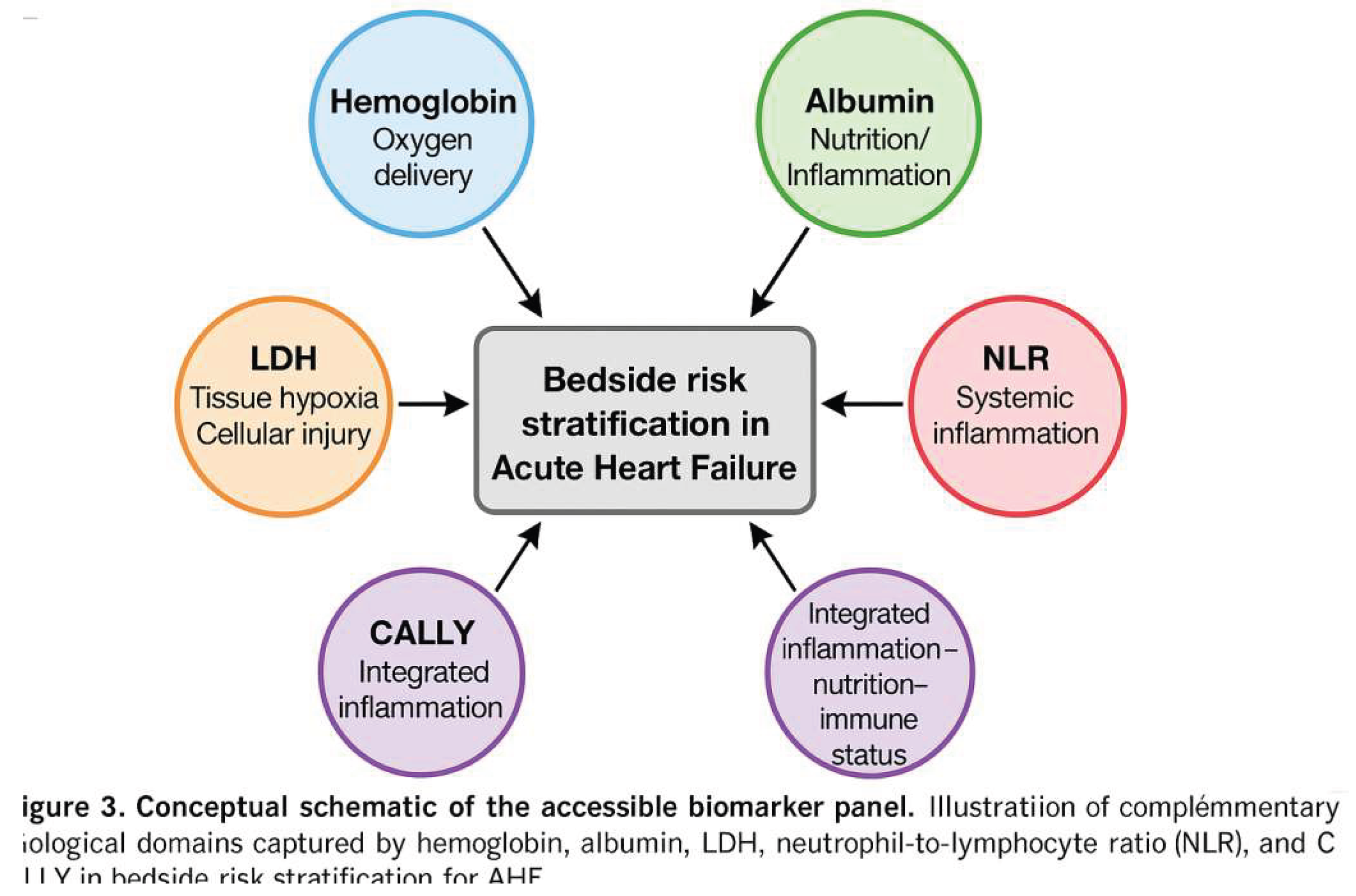
Figure 3.
Conceptual schematic of the accessible biomarker panel. Conceptual schematic illustrating complementary biological domains represented by routinely available biomarkers, including hemoglobin (oxygen delivery), albumin (nutrition and inflammation), lactate dehydrogenase (tissue hypoxia and cellular injury), neutrophil-to-lymphocyte ratio (systemic inflammation), and the C-reactive protein–albumin–lymphocyte (CALLY) index (integrated inflammation–nutrition–immune status), used for bedside risk stratification in acute heart failure.
Figure 3.
Conceptual schematic of the accessible biomarker panel. Conceptual schematic illustrating complementary biological domains represented by routinely available biomarkers, including hemoglobin (oxygen delivery), albumin (nutrition and inflammation), lactate dehydrogenase (tissue hypoxia and cellular injury), neutrophil-to-lymphocyte ratio (systemic inflammation), and the C-reactive protein–albumin–lymphocyte (CALLY) index (integrated inflammation–nutrition–immune status), used for bedside risk stratification in acute heart failure.
Discussion
In this real-world cohort of patients hospitalized with acute heart failure in a resource-limited healthcare setting, our study demonstrates that lactate dehydrogenase (LDH) is independently associated with in-hospital mortality. Although anemia and hypoalbuminemia were common and showed higher crude mortality rates, their prognostic impact did not persist after adjustment for clinical covariates. These findings highlight the potential role of LDH as a simple, low-cost, and widely available biomarker for short-term risk stratification when access to advanced cardiac biomarkers is limited.²³–²⁶
Anemia and hypoalbuminemia are frequently encountered in patients with acute heart failure and have traditionally been associated with adverse outcomes.⁵–⁹ Anemia may impair myocardial oxygen delivery and exacerbate neurohormonal activation, whereas hypoalbuminemia reflects a complex interplay of systemic inflammation, malnutrition, venous congestion, and hepatic dysfunction.⁷–¹² In line with previous studies, both conditions were associated with higher crude mortality in our cohort. However, their lack of independent prognostic significance after multivariable adjustment suggests that they primarily reflect underlying disease severity and comorbidity burden rather than acting as direct drivers of short-term mortality.¹²–¹⁵
In contrast, LDH remained independently associated with in-hospital mortality after adjustment for age, sex, chronic kidney disease, and other laboratory parameters. LDH is a nonspecific but biologically plausible marker of tissue hypoxia, cellular injury, and systemic hypoperfusion—key pathophysiological processes in acute heart failure decompensation.²³–²⁶ Elevated LDH levels may therefore integrate information across multiple organ systems, capturing the severity of acute circulatory compromise more effectively than isolated hematologic or nutritional markers.³¹–³²
Our findings are consistent with prior reports demonstrating an association between elevated LDH levels and adverse outcomes in both acute and chronic heart failure populations.²³–²⁶,³¹ Importantly, the prognostic value of LDH in our cohort was observed in the absence of natriuretic peptide testing, underscoring its potential utility in low-resource healthcare environments where guideline-recommended biomarkers are unavailable or unaffordable.²⁸,³⁶ While the confidence interval around the LDH effect estimate was relatively wide—reflecting the modest number of outcome events—the direction and consistency of the association support its clinical relevance.
Inflammatory–nutritional indices such as the neutrophil-to-lymphocyte ratio (NLR) and the C-reactive protein–albumin–lymphocyte (CALLY) index showed nonsignificant trends toward increased mortality.¹⁴–²⁰,²² These findings suggest that although systemic inflammation and immune–nutritional imbalance contribute to disease severity, their incremental prognostic value beyond established clinical variables may be limited in the acute setting. Larger, adequately powered studies are needed to clarify their role in short-term risk prediction.
From a clinical perspective, our results support a pragmatic approach to risk stratification in acute heart failure. In healthcare systems where access to advanced biomarkers is limited, LDH—interpreted alongside routinely measured parameters such as hemoglobin and albumin—may assist clinicians in identifying high-risk patients, guiding monitoring intensity, and informing early management decisions. This strategy aligns with the need for scalable and equitable diagnostic approaches across diverse healthcare settings.²⁸,³³–³⁷
Although our analysis focused on in-hospital outcomes during acute heart failure hospitalization, the observed association between elevated LDH levels and mortality may also have implications for chronic heart failure care.²³–²⁶ LDH reflects systemic hypoperfusion, tissue injury, and multiorgan stress—pathophysiological processes that are not limited to acute decompensation but are also integral to advanced and progressive chronic heart failure.³⁵ From this perspective, LDH may serve as a marker of overall disease severity along the acute–chronic heart failure spectrum.²³,²⁶
Limitations
Several limitations of this study should be acknowledged. First, its retrospective and single-center design limits causal inference and generalizability. Second, the absence of natriuretic peptide measurements precluded direct comparison with guideline-recommended biomarkers; however, this limitation reflects the real-world constraints faced in many low-resource healthcare systems.³⁶ Third, the number of in-hospital deaths was relatively modest, which may have limited statistical power and contributed to wide confidence intervals. Finally, long-term outcomes were not assessed, restricting conclusions to short-term prognosis.
Conclusion
In this real-world cohort from a resource-limited setting, lactate dehydrogenase emerged as the only laboratory marker independently associated with in-hospital mortality in patients with acute heart failure. Although anemia and hypoalbuminemia were common and associated with crude mortality, they did not retain independent prognostic significance after adjustment for clinical factors. These findings suggest that LDH, a low-cost and universally available biomarker, may provide a practical tool for early risk stratification when access to advanced cardiac biomarkers is limited. Prospective, multicenter studies are warranted to validate these observations.
Highlights
- Lactate dehydrogenase (LDH) was independently associated with in-hospital mortality in acute heart failure.
- Anemia and hypoalbuminemia were associated with crude mortality but did not retain independent prognostic significance.
- Low-cost and routinely available biomarkers may support practical risk stratification across the acute–chronic heart failure spectrum.
- This real-world cohort reflects clinical challenges in resource-limited settings where BNP and NT-proBNP testing is unavailable.
- LDH may provide clinically relevant prognostic information with potential implications for chronic heart failure care.
Declaration of Generative AI and AI-assisted Technologies in the Writing Process
During the preparation of this manuscript, the authors used generative artificial intelligence tools to assist with language refinement, organization of ideas, and improvement of clarity. After using these tools, the authors carefully reviewed and edited the content as needed and take full responsibility for the accuracy, integrity, and originality of the work.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the local Institutional Review Board (Approval No: MSTH/20379, Date: 07 December 2024). Given the retrospective design and use of anonymized data, the requirement for informed consent was waived.
Data Availability Statement
The data supporting the findings of this study are not publicly available due to patient privacy concerns and institutional restrictions. De-identified data may be made available from the corresponding author upon reasonable request and with appropriate institutional approvals.
References
- Ponikowski, P; Voors, AA; Anker, SD; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021, 42(36), 3599–3726. [Google Scholar]
- McDonagh, TA; Metra, M; Adamo, M; et al. The 2021 ESC Heart Failure Guidelines: key updates and clinical implications. Eur Heart J. 2022, 43(4), 221–228. [Google Scholar]
- Savarese, G; Lund, LH. Global public health burden of heart failure. Nat Rev Cardiol. 2017, 14(10), 639–649. [Google Scholar] [CrossRef] [PubMed]
- Dokainish, H; Teo, K; Zhu, J; et al. Heart failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Lancet Glob Health 2017, 5(8), e742–e750. [Google Scholar] [CrossRef] [PubMed]
- Tang, WHW; Yeo, PSD; Hart, R; et al. Anemia in acute decompensated heart failure: prevalence and prognostic significance. Clin Cardiol. 2009, 32(7), E35–E39. [Google Scholar]
- Groenveld, HF; Januzzi, JL, Jr.; Damman, K; et al. Anemia and mortality in heart failure: a systematic review and meta-analysis. J Am Coll Cardiol. 2008, 52(10), 818–827. [Google Scholar] [CrossRef]
- Arques, S; Ambrosi, P; Gelisse, R; et al. Hypoalbuminemia in elderly patients with acute decompensated heart failure. J Am Geriatr Soc. 2003, 51(8), 1229–1230. [Google Scholar]
- Horwich, TB; Kalantar-Zadeh, K; MacLellan, WR; Fonarow, GC. Albumin levels predict survival in patients with advanced heart failure. J Am Coll Cardiol. 2008, 52(11), 1216–1222. [Google Scholar]
- Arques, S; Ambrosi, P. Human serum albumin in the clinical syndrome of heart failure. J Card Fail. 2011, 17(6), 451–458. [Google Scholar] [CrossRef]
- Semba, RD; Nicklett, EJ; Ferrucci, L. Does hypoalbuminemia affect mortality in older persons? Results from the InCHIANTI study. J Gerontol A Biol Sci Med Sci. 2010, 65(8), 795–801. [Google Scholar]
- Liu, M; Chan, CP; Yan, BP; et al. Albumin and mortality in heart failure: a meta-analysis. Eur J Heart Fail. 2012, 14(4), 386–392. [Google Scholar]
- Arques, S; Roux, E; Ambrosi, P. Hypoalbuminemia in heart failure: pathophysiologic mechanisms and clinical significance. Heart Fail Rev. 2019, 24(1), 1–10. [Google Scholar]
- Yancy, CW; Jessup, M; Bozkurt, B; et al. 2017 ACC/AHA/HFSA heart failure focused update. J Am Coll Cardiol. 2017, 70(6), 776–803. [Google Scholar] [CrossRef] [PubMed]
- Zazula, AD; Precoma-Neto, D; Gomes, AM; et al. The neutrophil-to-lymphocyte ratio as an inflammatory marker in acute coronary syndromes. Clin Chim Acta 2008, 395(1–2), 65–70. [Google Scholar]
- Uthamalingam, S; Patvardhan, EA; Subramanian, S; et al. Utility of the neutrophil-to-lymphocyte ratio in predicting long-term outcomes in acute decompensated heart failure. Am J Cardiol. 2011, 107(3), 433–438. [Google Scholar] [CrossRef]
- Bhat, T; Teli, S; Rijal, J; et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther. 2013, 11(1), 55–59. [Google Scholar] [CrossRef]
- Durmus, E; Kivrak, T; Gerin, F; et al. The relationship between NLR and heart failure subtypes. Eur Rev Med Pharmacol Sci. 2015, 19(21), 4331–4338. [Google Scholar]
- Forget, P; Khalifa, C; Defour, JP; et al. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res Notes 2017, 10(1), 12. [Google Scholar] [CrossRef]
- de Jager, CPC; Wever, PC; Gemen, EFA; et al. The neutrophil–lymphocyte ratio in patients with community-acquired pneumonia. Eur J Clin Microbiol Infect Dis. 2010, 29(12), 1501–1507. [Google Scholar] [CrossRef]
- Núñez, J; Miñana, G; Bodi, V; et al. Low lymphocyte count and cardiovascular diseases. Int J Cardiol. 2011, 146(2), 264–270. [Google Scholar]
- Kinoshita, A; Onoda, H; Imai, N; et al. The CRP/albumin ratio as a novel prognostic marker in hepatocellular carcinoma. J Clin Oncol. 2015, 33 (15_suppl), 4105. [Google Scholar]
- Suzuki, K; Imai, N; et al. Prognostic significance of the CALLY index in cancer and cardiovascular disease. Nutrients 2021, 13(7), 2401. [Google Scholar]
- Chen, L; Wu, C; Gao, R; et al. Serum lactate dehydrogenase and outcomes in acute heart failure. Eur J Heart Fail. 2020, 22(5), 898–906. [Google Scholar]
- Liu, T; Li, G; Li, L; et al. Lactate dehydrogenase as a biomarker for mortality in critical illness: a meta-analysis. Crit Care 2021, 25(1), 171. [Google Scholar]
- Niimi, N; Ikeda, Y; Shimizu, M; et al. Association of LDH with in-hospital mortality in acute heart failure: multicenter cohort. Heart Vessels 2023, 38(3), 522–531. [Google Scholar]
- Lu, J; Wang, X; et al. Elevated serum LDH levels and poor prognosis in acute decompensated heart failure. ESC Heart Fail. 2022, 9(1), 356–366. [Google Scholar]
- Shah, KS; Xu, H; Matsouaka, RA; et al. HF with preserved, borderline, and reduced EF: 5-year outcomes. J Am Coll Cardiol. 2017, 70(20), 2476–2486. [Google Scholar] [CrossRef]
- Bhatla, A; Maisel, A. Biomarkers in acute heart failure. Heart Fail Clin. 2019, 15(3), 323–334. [Google Scholar]
- Dhingra, A; Givertz, MM. Interpretation and use of natriuretic peptides. J Am Coll Cardiol. 2019, 73(9), 1184–1201. [Google Scholar]
- Yilmaz, S; Altay, H; Özkan, A; et al. Predictors of mortality in patients hospitalized for AHF. ESC Heart Fail. 2023, 10(2), 1259–1269. [Google Scholar]
- Yao, Y; Zhao, M; et al. Elevated LDH predicts short-term mortality in AHF. Front Cardiovasc Med. 2021, 8, 714485. [Google Scholar]
- Wu, Y; Chen, J; et al. Prognostic significance of LDH in cardiovascular diseases: systematic review. BMC Cardiovasc Disord. 2022, 22, 307. [Google Scholar]
- Mentz, RJ; Greene, SJ; DeVore, AD; et al. Biomarkers in heart failure: implications and challenges. Heart Fail Rev. 2017, 22(6), 725–734. [Google Scholar]
- van der Meer, P; Gaggin, HK; Dec, GW. ACC/AHA/ESC/HFSA recommendations on biomarkers in HF. J Am Coll Cardiol. 2021, 78(5), 494–504. [Google Scholar]
- Harjola, VP; Mullens, W; Banaszewski, M; et al. Organ congestion in HF: assessment and implications. Eur J Heart Fail. 2016, 18(7), 760–771. [Google Scholar]
- Ferreira, JP; Metra, M; Mordi, IR; et al. Heart failure in low-resource settings. ESC Heart Fail. 2020, 7(6), 4213–4224. [Google Scholar]
- Fudim, M; O'Connor, CM; Ahmad, T. Biomarker-guided therapy in HF. Curr Heart Fail Rep. 2018, 15(6), 429–436. [Google Scholar]
- Felker, GM; Mentz, RJ; Teerlink, JR; et al. Serial biomarker measurement in AHF: RELAX-AHF insights. Eur J Heart Fail. 2016, 18(12), 1420–1428. [Google Scholar]
- Ahmad, T; Fiuzat, M; Felker, GM; O'Connor, CM. Novel biomarkers in chronic HF. Nat Rev Cardiol. 2012, 9(6), 347–359. [Google Scholar] [CrossRef]
- Wang, L; Li, Y; et al. Temporal trends in biomarker changes in HF. Front Cardiovasc Med. 2023, 10, 1164325. [Google Scholar]
- Mueller, C; McDonagh, T; et al. Biomarker-based strategies in AHF management. Eur Heart J. 2023, 44(5), 412–427. [Google Scholar]
Figure 1.
Flow diagram of patient selection. Flow diagram illustrating patient selection for the study. A total of 220 consecutive patients hospitalized with acute heart failure between May 2022 and November 2024 were screened. After exclusion of patients with missing in-hospital outcome data (n = 9), 211 patients were included in the primary mortality analysis. Subgroup analyses based on hemoglobin and albumin levels were performed in 141 patients with complete data.
Figure 1.
Flow diagram of patient selection. Flow diagram illustrating patient selection for the study. A total of 220 consecutive patients hospitalized with acute heart failure between May 2022 and November 2024 were screened. After exclusion of patients with missing in-hospital outcome data (n = 9), 211 patients were included in the primary mortality analysis. Subgroup analyses based on hemoglobin and albumin levels were performed in 141 patients with complete data.
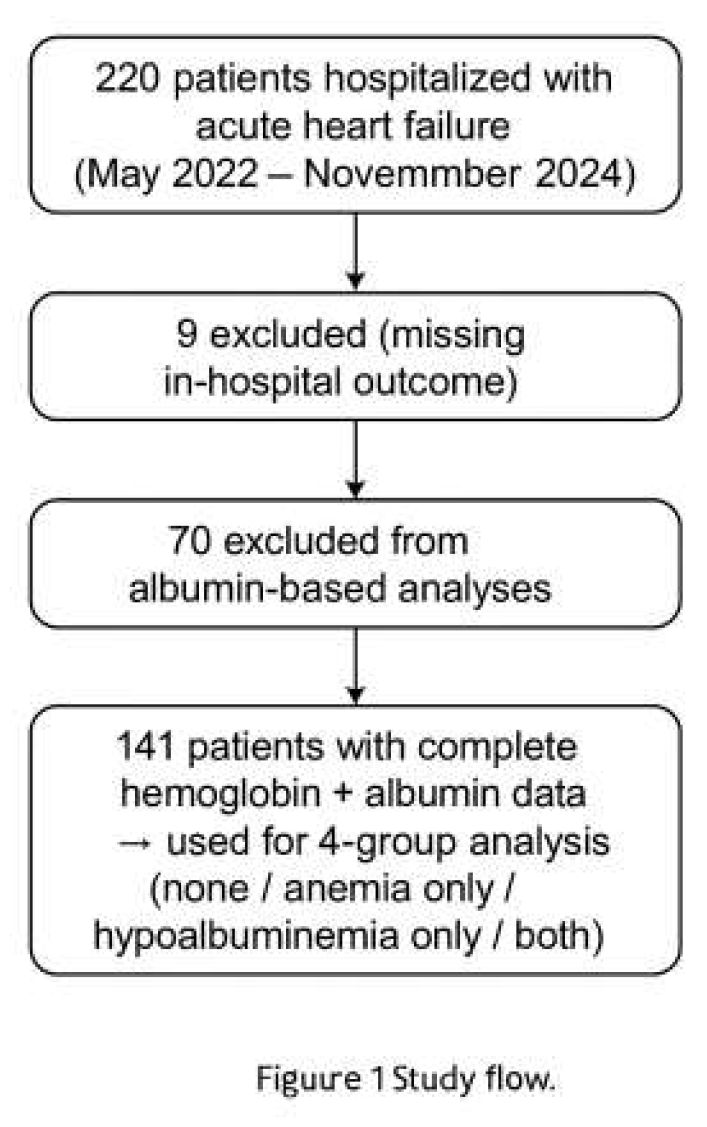
Figure 2.
Multivariable logistic regression analysis for in-hospital mortality. Forest plot showing adjusted odds ratios and 95% confidence intervals for predictors of in-hospital mortality derived from the multivariable logistic regression model. The model was adjusted for age, sex, chronic kidney disease, hemoglobin, albumin, lactate dehydrogenase (LDH), neutrophil-to-lymphocyte ratio (NLR), and the C-reactive protein–albumin–lymphocyte (CALLY) index. LDH was the only laboratory parameter independently associated with in-hospital mortality.
Figure 2.
Multivariable logistic regression analysis for in-hospital mortality. Forest plot showing adjusted odds ratios and 95% confidence intervals for predictors of in-hospital mortality derived from the multivariable logistic regression model. The model was adjusted for age, sex, chronic kidney disease, hemoglobin, albumin, lactate dehydrogenase (LDH), neutrophil-to-lymphocyte ratio (NLR), and the C-reactive protein–albumin–lymphocyte (CALLY) index. LDH was the only laboratory parameter independently associated with in-hospital mortality.
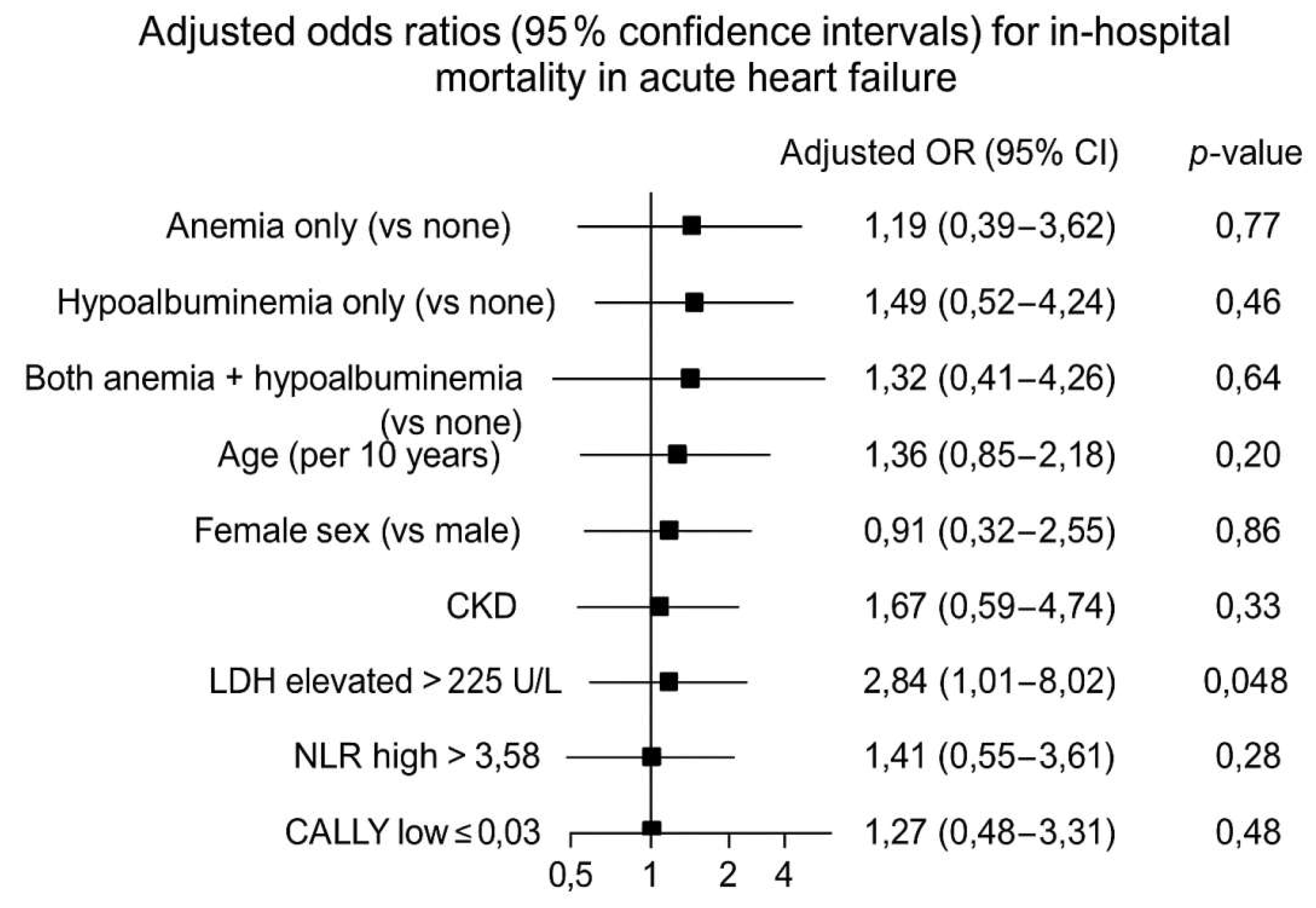

Table 1.
Baseline demographic, clinical, and laboratory characteristics of the study population.
| Variable | Overall cohort (n = 220) |
| Age, years | 59.5 ± 14.7 |
| Male sex, n (%) | 138 (62.7) |
| Diabetes mellitus, n (%) | 129 (58.6) |
| Hypertension, n (%) | 118 (53.6) |
| Chronic kidney disease, n (%) | 29 (13.2) |
| Ischemic heart disease, n (%) | 11 (5.0) |
| Hemoglobin, g/dL | 11.7 (IQR 10.0–13.3) |
| Serum albumin, g/dL | 3.0 (IQR 2.4–3.8) |
| Lactate dehydrogenase, U/L | 54.5 (IQR 20.0–123.0) |
| C-reactive protein, mg/L | 45.0 (IQR 17.0–99.0) |
| Neutrophil-to-lymphocyte ratio | 3.6 (IQR 2.3–6.9) |
Data are presented as mean ± standard deviation or median (interquartile range), unless otherwise indicated. CKD: chronic kidney disease; LDH: lactate dehydrogenase; CRP: C-reactive protein.
Table 2.
In-hospital mortality according to anemia and hypoalbuminemia status.
| Hemoglobin–Albumin subgroup | n | In-hospital mortality, n (%) |
| No anemia / No hypoalbuminemia | 38 | 2 (5.3) |
| Anemia only | 32 | 6 (18.8) |
| Hypoalbuminemia only | 34 | 8 (23.5) |
| Anemia + Hypoalbuminemia | 37 | 5 (14.8) |
| Total | 141 | 21 (14.9) |
P value (overall comparison): 0.04. Data are presented as number (percentage).
Table 3.
Multivariable logistic regression analysis for predictors of in-hospital mortality.
| Variable | Adjusted OR | 95% Confidence Interval | P value |
| Age (per year increase) | 1.03 | 0.99–1.07 | 0.11 |
| Male sex | 1.21 | 0.48–3.05 | 0.68 |
| Chronic kidney disease | 1.89 | 0.72–4.96 | 0.20 |
| Anemia | 1.42 | 0.54–3.71 | 0.47 |
| Hypoalbuminemia | 1.67 | 0.63–4.45 | 0.30 |
| Lactate dehydrogenase | 2.84 | 1.01–8.02 | 0.048 |
| Neutrophil-to-lymphocyte ratio >3.58 | 1.96 | 0.91–4.24 | 0.09 |
| CALLY index ≤0.03 | 1.88 | 0.85–4.13 | 0.11 |
Odds ratios were adjusted for age, sex, and chronic kidney disease. OR: odds ratio; CI: confidence interval; CKD: chronic kidney disease; LDH: lactate dehydrogenase. LDH >225 U/L.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



