Submitted:
03 February 2026
Posted:
04 February 2026
You are already at the latest version
Abstract
Approximately 795,000 people experience new or recurrent strokes in the United States each year, and 10 to 20% of these are spontaneous intracerebral hemorrhages (ICH). Uncontrolled hypertension is not only the most common cause of ICH but also a major risk factor for hematoma expansion.
Resistant hypertension, defined as persistently elevated blood pressure despite the use of three or more antihypertensives of different classes, is common in patients with ICH. A long-acting calcium channel blocker, an angiotensin converting enzyme inhibitors (ACEi) or angiotensin receptor blocker (ARB) and a thiazide diuretic are generally considered the mainstay for the treatment of resistant hypertension. However, due to risk of hyponatremia and worsening cerebral edema, thiazide diuretics should be avoided during the first few weeks of ICH. Recent evidence supports the use of a mineralocorticoid receptor antagonist. While resistant hypertension may be idiopathic, workup of secondary causes should be pursued.
Adequate and timely control of elevated blood pressure remains one of the main cornerstones of treatment in patients with ICH. Previous studies have revealed that resistant hypertension in patients with ICH is associated with longer ICU stays, higher risk of recurrent stroke, and can contribute to renal, cardiac, and neurologic complications. This emphasizes the need for early initiation of oral antihypertensives and adequate blood pressure control at hospital discharge.
Landmark studies have shown that early lowering of SBP to 130-150 mm Hg with smooth, sustained BP control is safe and may improve functional outcome in patients with mild to moderate ICH. After initiating oral antihypertensives with a calcium channel blocker, an ACEi or ARB beta-blocker, and a mineralocorticoid receptor antagonist to maximally tolerated doses, the next line of antihypertensive should be tailored to the patient’s co-morbidities, and may include beta blocker, central alpha agonist, hydralazine and minoxidil.
In this review, we will discuss the epidemiology of resistant hypertension in ICH and its molecular basis, diagnostic workup, and acute and long-term treatment. We will also propose a simple algorithm for optimal pharmacological management of resistant hypertension in ICH.
Keywords:
resistant hypertension
; intracranial hemorrhage
; hypertension in intracranial hemorrhage
1. Introduction
Approximately 795,000 people experience new or recurrent strokes each year in the United States, and approximately 10 to 20% of these are hemorrhagic (Tsao / Unnithan / Furie). Intracranial hemorrhage (ICH) may be primary due to small vessel disease in the setting of hypertension and cerebral amyloid angiopathy) or secondary to a lesion or bleeding diathesis (Caplan). Uncontrolled hypertension is not only one of the strongest risk factors for ICH but also a major contributor to hematoma expansion (Zhu et al.).
Globally, an estimated 100-500 million people are affected by resistant hypertension, and a previous meta-analysis revealed that resistant hypertension has a prevalence of 5% amongst patients with hypertension (Buso et al.). It is more often seen in male patients, those with diabetes mellitus and those of black African descent (Buso et al.). A study published by our group found that 31.6% of patients with hypertensive ICH had resistant hypertension (hong et al.).
Clinically, hypertension is defined as a systolic blood pressure greater than 130 mmHg, or a diastolic blood pressure greater than 80 mmHg (Jones et al., AHA 2025 guidelines). Uncontrolled hypertension is commonly attributed to resistant hypertension, which is defined as persistently elevated blood pressure despite the use of three or more antihypertensives of different classes, such as a long-acting calcium channel blocker, ACE/ARB, and a thiazide-like diuretic (biffi, acelajado, carey). Previous studies have revealed that resistant hypertension in patients with ICH is associated with longer lengths of stay in the ICU, as well as higher requirements for ventilator support, hematoma evacuation, hypertonic saline therapy, and nicardipine infusion (hong et al.). Risk of recurrent stroke is also higher in survivors of ICH with resistant hypertension at 3 months post ICH (biffi). Furthermore, refractory hypertension can contribute to systemic (e.g., renal and cardiac) disease and may result in posterior reversible encephalopathy syndrome, hypertensive encephalopathy, and intraocular hemorrhage. These complications emphasize the need for early initiation of oral antihypertensives and adequate blood pressure control at discharge in patients with ICH.
In this paper, we first review the molecular basis of benign and resistant hypertension. We then discuss the acute management of hypertension in patients with ICH, detailing the various classes of antihypertensive medications, followed by the recommended diagnostic workup of secondary causes of hypertension. Finally, we address considerations for long-term management of hypertension in patients with ICH.
2. Molecular Mechanisms in Hypertension
Blood pressure is the lateral pressure on blood vessel walls per unit area during blood flow and is determined by cardiac output and peripheral vascular resistance. By extension of the Bernoulli’s Principle and Poiseuille's Law, the main contributors to blood pressure are intravascular fluid volume and vascular dysfunction. The mechanisms underlying hypertension are the result of a complex interplay between environmental, genetic, neural, and endocrine factors (Padmanabhan). Together, these factors contribute to dysfunction in vascular elasticity, caliber, and reactivity (Ma et al.), which are modulated by changes in signaling pathways of vascular endothelial cells and smooth muscle cells.
Cell signaling underlying vascular function primarily involves interplay between the renin-angiotensin-aldosterone (RAAS), calcium signaling, nitric oxide-nitric oxide sensitive guanylate cyclase – cGMP pathway (NO-NOsGC-cGMP), and vascular remodeling. Calcium and NO-NOsGC-cGMP signaling are reversible while vascular remodeling is less so.
Blood vessels are generally comprised of three layers: the intima, media, and adventitia. Endothelial cells are found in the intima, the innermost layer of the blood vessel. In response to stimuli, these cells secrete signaling molecules to mediate vascular relaxation and contraction. The media is comprised of smooth muscle cells and extracellular matrix. This layer modulates vasoconstriction and vasodilation. The adventitia, the outermost layer of the vessel, is made of fibroblasts and loose collagen extracellular matrix, containing lymphocytes, nerves, and immune cells. (Ma et al.)
Activation of the RAAS results in a rise in blood pressure. Renin is stored in juxtaglomerular cells of the afferent arterioles of the kidney, and released following changes in renal perfusion, activation of beta-1 adrenergic receptors, increased sodium and chloride concentrations at the distal convoluted tubule, and hypokalemia. (Fountain et al. – overview of RAAS) Renin cleaves angiotensinogen, made and secreted by the liver, into angiotensin I. The latter does not have a known biological activity and is converted by angiotensin converting enzyme (ACE) to angiotensin II. Angiotensin II is the main contributor to blood pressure elevation by stimulating contraction of vascular smooth muscle, aldosterone secretion from the adrenal cortex, and release of vasopressin from the hypothalamus. It also causes increased sodium resorption and increased sympathetic outflow. Aldosterone, a mineralocorticoid, acts on the late distal tubule and collecting duct of the nephron, ultimately resulting in sodium and water reabsorption and potassium excretion. (Scott et al.)
When stimulated, vascular smooth muscle cells release intracellular stores of calcium and extracellular calcium enters through high voltage activated L type calcium channels. This results in an increased concentration of intracellular calcium. Calcium binds to calmodulin, and this complex activates myosin light chain kinase, which phosphorylates myosin light chains promoting contraction. (Ma et al.) Activation of the NO-NOsGC-cGMP pathway promotes vasodilation. Nitric oxide is produced in endothelial cells and RBCs and diffuses to vascular smooth muscle cells. It then binds to soluble guanylyl cyclase, which then produces cyclic GMP. Higher concentrations of cGMP results in activation of protein kinase G and phosphorylation of vasodilator-stimulated phosphoprotein. Subsequently, myosin light chain phosphatase de-phosphorylates contracted phosphorylated actin-myosin, resulting in relaxation and vasodilation. NO-NOsGC-cGMP signaling also decreases renin release and promotes natriuresis by modulating sodium transporters. (Ataei)
Vascular remodeling occurs primarily as a consequence of excessive collagen, advanced glycation end-product (AGEs) deposition, degradation of elastic fibers, and calcification within the extracellular matrix. Within the extracellular matrix, matrix metalloproteinases are responsible for degrading collagen and gelatin, but some forms may also promote calcification and collagen accumulation, ultimately resulting in reduced elasticity and “hardening” of vessels. AGEs may accumulate due to diabetes, hyperlipidemia, and smoking. AGEs may deposit in the extracellular matrix and form cross-links, which results in deposition of other macromolecules. Collagen fibers cross-linked to AGEs are stiffer and contribute to vascular dysfunction. Medial arterial calcification and resultant reduced vascular compliance are hypothesized to occur as the result of loss of mineralization inhibition and induction of osteogenesis. (Ma et al.) Furthermore, based on the results of the PATHWAY-2 study, resistant hypertension may be associated with a salt-retaining state, ultimately resulting in high aldosterone-to-renin ratios (Williams B, MacDonald TM, Morant SV, et al. Endocrine and haemodynamic changes in resistant hypertension, and blood pressure responses to spironolactone or amiloride: the PATHWAY-2 mechanisms substudies. Lancet Diabetes Endocrinol. 2018;6(6):464-475. doi:10.1016/S2213-8587(18)30071-8).
Hypertension has been shown to be heritable, with complex polygenic Mendelian inheritance associated with rare genetic mutations (Padmanabhan). Multiple single gene polymorphisms have been identified that are associated with hypertension, the details of which are outside of the scope of this review.
3. Acute Management of Hypertension in ICH Patients
Around 80% of patients with acute ICH present with elevated blood pressure. Persistently uncontrolled blood pressure is a risk factor for hematoma expansion, which has been associated with worse functional outcomes. Two landmark RCTs, INTERACT215 and ATACH II17 (Table 1), were aimed at establishing whether aggressive blood pressure control could prevent hematoma expansion and improve mortality and morbidity after spontaneous ICH. INTERACT215 compared outcomes with early lowering of SBP to <140 mm Hg or to <180 mm Hg; there was no significant difference in adverse events in aggressive early lowering of SBP, and upon ordinal analysis of modified Rankin Scale (mRS) scores, intensive early lowering of SBP was associated with improved functional outcomes at 90 days. Interestingly, early intensive lowering of SBP did not clearly reduce hematoma growth, and on subgroup analysis, there was no significant difference between patients who were randomized to treatment within 4 hours of ICH and those who were randomized later. It was unclear if this was due to limited statistical power, or if the results truly represented an independent effect of the timing of blood pressure lowering. It was hypothesized that intensive SBP lowering could be neuroprotective or reduce perihematomal edema with resultant downstream positive clinical outcomes.
ATACH II17 (Table 1) studied the role of very early and aggressive reduction in patients with acute ICH presenting with SBP 170-200 mmHg. Patients were randomized to standard treatment or intensive treatment within 4.5 hours of symptom onset. Using nicardipine infusion, SBP was maintained around 140-179 mmHg in the standard treatment group, and 110-139 in the intensive treatment group for 24 hours after randomization. While there was no significant difference in neurologic deterioration at 24 hours post randomization, nor in death or disability at 3 months, the intensive treatment group had higher incidence of adverse renal events (9.0%, 4.0%, p=0.002).
The differing conclusions reached by the two trials stem in large part from differences in BP management protocols with ATACH II17 enrolling patients with higher average SBP and achieving the BP targets faster and more frequently than INTERACT215. Importantly, the achieved BP goal in ATACH II17 was lower than in INTERACT215, contributing to a larger reduction in BP. Based on the results of these trials, the AHA guidelines state early lowering of SBP to a target of 130-150 mm Hg with smooth, sustained BP control using regimens that limit BP variability is safe and may improve functional outcome in patients with mild to moderate acute ICH who present with SBP between 150 to 220 (AHA guidelines 2022).
Post-hoc analysis of INTERACT215 data revealed that elevation of baseline SBP, glucose, body temperature, and anticoagulant use were independent predictors of poor functional outcome post ICH. Therefore, INTERACT356 (Table 1) was designed to study the impact of bundled care on outcomes in ICH. The results of INTERACT356 showed bundled care with early intensive lowering of SBP (<140 mmHg), strict glucose control, avoidance of fever (<= 37.5C), and reversal of anticoagulation within 1 hour, improves functional outcomes in patients with acute ICH. While there was no significant difference in death or disability at 90 days, patients who received bundled care had better mRS scores and lower odds of death at 6 months. Therefore, while early and aggressive blood pressure management is paramount, anticoagulation reversal and avoidance of hyperglycemia/fever is also crucial.
It was previously thought that aggressive blood pressure control in the acute period could result in perihematomal ischemia. The RCT, ICH ADAPT, showed that greater blood pressure reduction (SBP <150 mmHg vs <180 mmHg) did not result in more perihematomal ischemia or infarction. Along the same lines, ICH ADAPT2 found that the number and volume of new DWI lesions were not affected by the intensity of blood pressure control after ICH, further confirming that more aggressive blood pressure control approach is unlikely to result in de novo ischemia or infarction.
Given these additional data supporting aggressive blood pressure, INTERACT416 (Table 1) was designed to investigate the utility of strict blood pressure control before arrival at hospital. Patients with suspected acute stroke with SBP >150 mmHg and symptom onset within 2 hours before randomization were assigned to either the intervention group (goal SBP 130-140 mmHg) or usual care group (SBP <220 mmHg or DBP <110 mmHg). This study found that there was no statistical significance between the two groups in terms of functional outcomes (measured by mRS) or serious adverse events. A secondary and subgroup analyses found that among patients later found to have hemorrhagic stroke, early BP lowering was associated with lower odds of poor outcome (OR ~0.75) whereas for those later found to have ischemic stroke, intensive BP lowering was associated with worse outcomes (OR ~1.30). Given these findings, pre-hospital aggressive BP control was not recommended.
4. Initial Choice of Antihypertensives
To maintain sustained blood pressure control with minimal variability, many patients admitted to the neurological intensive care unit are initiated on continuous infusion of an antihypertensive agent.
Typically, in treatment of hypertensive emergency without ICH, patients may receive continuous IV antihypertensive infusion of nicardipine, clevidipine, or nitroprusside. While nitroprusside is a potent antihypertensive, it should be avoided due to its venodilatory effects, increasing cerebral blood volume and potentially worsening ICP. Compared to nicardipine, clevidipine has a faster onset, shorter duration of action and smaller volume of infusion, but it is more costly and can lead to more rebound hypertension when discontinued. Several recent retrospective studies comparing the efficacy of the two have shown no significant difference in time to goal BP (Johnson, Caltagiorone ). One study has shown that early initiation of oral antihypertensives within 24h of event reduces ICU length of stay and hospital cost for patients with hypertensive ICH (Zhu Zhu). Furthermore, given the results of INTERACT, INTERACT2, and ATACH2 showing safety of early aggressive SBP control, once enteric access is obtained, it is reasonable to initiate oral hypertensives.
Based on the 2025 AHA guidelines on the management of high blood pressure in adults, first line antihypertensive therapy should be an angiotensin converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB), a calcium channel blocker, and a thiazide-like diuretic such as chlorthalidone, metolazone or indapamide. Thiazide-like diuretics are more potent than thiazides, and in ICH, they are usually avoided in the acute period due to their potential for causing or worsening hyponatremia and therefore cerebral edema. Based on the PATHWAY-2 trial which concluded that spironolactone was a superior add-on antihypertensive agent compared to doxazosin and bisoprolol in adult patients with resistant hypertension (PATHWAY2), we recommend a mineralocorticoid receptor antagonist (MRA) be added as the next line agent after ACE/ARB and CCB in ICH. If there are contraindications to MRAs, other reasonable next line agents include amiloride, beta blockers, alpha blockers, central sympatholytics, dual endothelin receptor antagonists, or direct vasodilators (Figure 1).
5. ACEi/ARB
ACEi and ARBs inhibit activation of the RAAS signaling cascade and therefore, may also prevent secondary neuronal death following ICH and inhibit atherosclerotic processes (Zhang et al.). Contraindications to ACEi include angioedema (regardless of relation to prior ACE inhibitor or ARB), pregnancy, and renal artery stenosis. ACEi are teratogenic in the second and third trimester of pregnancy. Cough may occur in 5 to 20% of patients (Bicket). ACEi and ARBs are commonly held in patients with acute renal injury in the inpatient setting. However, in patients with chronic kidney disease (CKD), the use of ACEi in patients with creatinine up to 3.0 mg/dL is considered safe. In fact, no level of creatinine level is an absolute contraindication (Bicket). In patients with diabetes and CKD, ACEi and ARBs are recommended by the 2025 AHA guidelines as first-line agents owing to their nephroprotective effects and reduction of urinary albumin excretion. Based on the results of the HOPE trial, the ACEi, ramipril, significantly reduced rates of death, MI, and stroke in diabetic patients aged 55 or older with at least one other cardiac risk factor (Yusuf et al.). In one study comparing ACEi and ARBs, there was no significant difference in efficacy, but ARBs generally had lower risk of GI bleed, pancreatitis, angioedema, and cough (Chen et al.). In patients with non-lobar ICH, ACEi/ARB have been associated with improved 90-day functional outcomes as measured by mRS and Barthel Index compared to other classes of antihypertensives, independent of blood pressure control (Ridha et al.). When further stratified, ARBs showed statistically significant favorable outcomes, while ACEi did not (Ridha et al.).
6. Calcium Channel Blockers (CCB)
Calcium channel blockers prevent calcium influx by binding to L type voltage gated calcium channels in vascular smooth muscle, the heart, and the pancreas (McKeever).
The non-dihydropyridine CCBs, diltiazem and verapamil, inhibit the SA and AV nodes and reduce cardiac conduction and contractility (McKeever). Verapamil and diltiazem are CYP3A isoenzyme inhibitors, and caution should therefore be taken when combined with statins, benzodiazepines, buspirone, sildenafil, and cyclosporin. Due to potential for worsening bradycardia and cardiac output, non-dihydropyridines are contraindicated in HFrEF, second- or third-degree AV block, and sick sinus syndrome.
Dihydropyridine CCBs (amlodipine, felodipine, nimodipine, nicardipine, and nifedipine) have minimal cardiac binding and mostly promote peripheral vasodilation; they are most useful in post ICH vasospasm, hypertension, and migraine.
In part due to its longer half-life (30-50 hours vs 2 hours) and slower onset of action (6-12 hours vs 30-60 minutes), amlodipine is preferred to nifedipine as it has demonstrated a higher rate of adherence, higher absolute and relative therapeutic coverage, more consistent BP control, and lower adverse events and treatment withdrawal (Mounier-Vehier). Especially when concern exists for adherence, amlodipine has shown greater efficacy in overall BP-lowering effect as it has higher plasma concentration compared to that of nifedipine after 24 hours (79% vs 30%) and after 72 hours (61% vs 25%) (Huang et al.). Unlike nifedipine, amlodipine can be crushed, which is important for patients with ICH and dysphagia.
7. Thiazides
Thiazide and thiazide-like diuretics inhibit sodium reabsorption by blocking the sodium-chloride channel in the distal convoluted tubule of the nephron (Anisman et al.). Thiazide diuretics include hydrochlorothiazide (HCTZ), chlorothiazide, and methyclothiazide, while thiazide-like diuretics include indapamide, metolazone, and chlorthalidone. Adverse effects include hypokalemia, hyponatremia, metabolic alkalosis, hypercalcemia, hyperglycemia, and hyperuricemia. In high doses, thiazides may cause hyperlipidemia. Given the risk of hyponatremia and possibility of worsening cerebral edema, thiazides and, even more so, thiazide-like diuretics have limited utility in the acute treatment of hypertension in patients with ICH.
8. Mineralocorticoid Receptor Antagonists (MRAs)
Mineralocorticoid receptors, in addition to mediating the effects of aldosterone in the kidneys, have a role in extra-renal signaling with downstream effects that may affect blood pressure regulation. These include activation of the sympathetic nervous system, endothelial dysfunction, and stimulation of vascular smooth muscle cells (Maiolino et al.). As primary aldosteronism is a frequent cause of secondary hypertension (Maiolino et al.), and patients with resistant hypertension commonly develop secondary aldosteronism because of diuretic-induced sodium depletion and subsequent RAAS activation, MRAs are a good option for next-line treatment of hypertension. As discussed previously, PATHWAY 2 demonstrated that spironolactone was the most effective add-on agent compared to other classes of anti-hypertensives. The results of PATHWAY2 suggested that the benefits of spironolactone seem to be associated with a reduction in baseline plasma renin levels, supporting the hypothesis that increased sodium retention leads to resistant hypertension. Given that MRAs can result in impaired potassium excretion, this class of antihypertensives should be avoided in patients with serum potassium higher than 5.5 mmol/L.
9. Amiloride
Amiloride is a potassium-sparing diuretic that inhibits epithelial sodium channels in the distal nephron, lung, and colon. In the distal convoluted tubule and cortical collecting duct, amiloride decreases potassium, proton, calcium, and magnesium secretion and may result in mild natriuresis. Prolonged use may reduce the excretion of uric acid. While the AHA does not recommend amiloride as an initial agent for management of hypertension, it is approved by the FDA to be used in conjunction with thiazides for treatment of CHF or hypertension to improve hypokalemia (Almajid). In an open-label, blinded endpoint randomized clinical trial in South Korea, amiloride was non-inferior to spironolactone in lowering home blood pressure (Lee et al.).
10. Beta-Blockers
Beta-blockers function by antagonizing beta-1 and beta-2 adrenoreceptors in the heart and smooth muscle to decrease chronotropic and ionotropic effects, which in turn decreases heart rate, blood pressure and cardiac output (Farzamnon-selective beta-blockers (e.g., propranololwhich bind to both beta-1 and beta-2 receptors and beta-1-selective beta-blockers (atenolol, metoprolol, and esmolol) that only bind to beta-1. Carvedilol and labetalol are considered alpha and beta dual receptor blockers, and bind to beta-1, beta-2, and alpha-1 receptors. The use of beta-blockers as monotherapy for hypertension is not generally recommended as other options such as CCB, ACE-I, and ARB have shown greater benefits (Lindholm) (Wiysonge).
However, they cause substantial reduction in blood pressure when combined with drugs of different mechanisms, and are thus recommended as next line agents. A meta-analysis from 2023 showed that adding a beta-blocker to a non-beta-blocker monotherapy significantly decreased both systolic and diastolic blood pressure, and the results were consistent across different non-beta-blocker classes (ACEi/ARBs, CCBs, diuretics) (Guo). In one study of 138 hypertensive ICH patients in Canada, atenolol significantly reduced mortality, rates of SIRS, and pneumonia, but did not show statistically significant improvement in outcomes at 90 days compared to those who did not receive atenolol (Kalita et al.).
11. Alpha-1 Blockers
Alpha-1 adrenergic receptor blockers prevent binding of norepinephrine to receptors on prostatic smooth muscle and vascular smooth muscle. Diminished norepinephrine binding to alpha-1 receptors results in vasodilation, which decreases peripheral vascular resistance, and ultimately lowers blood pressure (Mathur et al.). Commonly prescribed alpha-blockers include doxazosin, terazosin, and prazosin.
Based on the ALLHAT hypertension trial, compared to chlorthalidone, doxazosin had statistically significant increase in decompensated CHF, angina, and stroke and is therefore not typically used as a first-line antihypertensive (Cushman et al.). Alpha-blockers are still used as second or third-line agents, particularly in patients with co-morbid benign prostatic hyperplasia.
In one meta-analysis of 1496 publications evaluating dose-related blood pressure lowering efficacy of alpha-blockers, blood pressure lowering effects of doxazosin and terazosin were similar (Heran et al.). The effect appears modest, on average lowering SBP by approximately 5 to 8 mm Hg (Heran et al.).
12. Central Sympatholytics – Alpha-2 Adrenergic Receptor Agonists
Activation of the centrally located alpha-2a and 2c receptors in the locus coeruleus produces sedation, analgesia, and sympatholytic effects. Alpha-2b receptors are found most often on vascular smooth muscle and agonism of these receptors results in vasopressor effects.
The most commonly used alpha-2 receptor agonist in the management of hypertension is clonidine. Other medications in this class include guanfacine, methyldopa, guanabenz, moxonidine, rilmenidine, and dexmedetomidine (Vongpatanasin et al.). Clonidine is an alpha-2 agonist, available in patch and pill formulations. Abrupt cessation precipitates rebound hypertension within 36 to 72 hours of discontinuation and therefore is not an ideal agent in patients with poor adherence to medical therapy (Vongpatanasin et al.). It can be useful in the management of ICH patients with hypertension who exhibit concomitant paroxysmal sympathetic hyperactivity or hyperactive delirium.
Dexmedetomidine is a selective alpha-2 adrenergic agonist used primarily for sedation. At low doses, it remains selective for central and peripheral alpha-2 receptors, and results in sedation, decreased heart rate, and systemic vascular resistance, thereby reducing blood pressure. Bolus or high-dose infusions diminish alpha-2 receptor selectivity, and result in activation of peripheral alpha-1 and alpha-2b receptors causing systemic hypertension. Caution should therefore be exercised when using high doses of dexmedetomidine as a sedative for patients with ICH (Vongpatanasin et al.).
13. Dual Endothelin Receptor Antagonists
Endothelin-1 mediates vasoconstriction through its action at endothelin-A and endothelin-B receptors. Aprocitentan is a dual endothelin-A and B antagonist which was approved by the FDA in 2024 for the treatment of hypertension. In a multi-center, blinded, randomized, parallel-group phase 3 study, Parallel-Group, Phase 3 Study with Aprocitentan in Subjects with Resistant Hypertension (PRECISION), aprocitentan was superior to placebo in lowering blood pressure by about 4 mm Hg at a dose of 12.5 and 25 mg daily, with sustained effects at week 40. It has a long half-life of about 44 hours and may therefore be helpful in patients where adherence is a concern (Chapman et al.).
14. Direct Vasodilators
Direct vasodilators, such as hydralazine and minoxidil, reduce blood pressure by reducing peripheral vascular resistance. This reduced peripheral resistance is detected by arterial baroreceptors, often resulting in compensatory tachycardia.
Hydralazine is thought to promote vasodilation by inhibiting calcium release from the sarcoplasmic reticulum, which prevents myosin phosphorylation and smooth muscle contraction. Hydralazine is typically dosed three to four times daily and is therefore not an ideal agent if adherence is a concern.
Minoxidil activates adenosine triphosphate-modulated potassium channels in vascular smooth muscle, resulting in reduced concentration of intracellular potassium and smooth muscle relaxation. When combined with a beta-blocker and diuretic, it has been shown to be an effective agent in lowering blood pressure in those with severe or refractory hypertension. Some studies have shown that minoxidil may also be helpful in preventing the progression of renal disease. It can be dosed once daily or divided into multiple doses if the patient has low supine diastolic blood pressure (McComb et al.).
15. Nitrates
Nitrates cause vasodilation through donation of nitric oxide, as previously discussed. This class of drugs includes nitroglycerin, isosorbide mononitrate, and isosorbide dinitrate. These are typically used in treatment of angina and can be used as an adjunct in treatment of hypertension, particularly isosorbide mononitrate. It should be noted that nitrates are not FDA approved for management of hypertension and are not recommended as first line therapy for hypertension (2025 AHA HTN guidelines). However, isosorbide dinitrate in combination with hydralazine is recommended to reduce afterload in HFrEF, particularly in black patients (2025 AHA HTN guidelines). Due to potential for causing severe hypotension, nitrates should not be used in conjunction with sildenafil, tadalafil, vardenafil, and avanafil.
16. Workup of Secondary Hypertension
Resistant hypertension should be differentiated from refractory hypertension (defined as elevated blood pressure despite the use of five or more antihypertensives), and apparent resistant hypertension due to nonadherence, white coat syndrome, or improper blood pressure measurement should be excluded. Once the diagnosis of resistant hypertension has been established, workup of secondary hypertension should be pursued. Patients should be screened for sleep disorders (sleep apnea, restless leg syndrome, etc.), primary aldosteronism, renal parenchymal disease, renal artery stenosis, pheochromocytoma/paraganglioma, and endocrine disorders (Carey et al., AHA resistant hypertension).
Fragmented, poor-quality sleep contributes to elevated blood pressure through heightened sympathetic activity and dysfunction of the RAAS. In patients with obstructive sleep apnea, increased adherence to CPAP therapy modestly and proportionately reduces blood pressure (average 2 to 5 mmHg). Adjunctive antihypertensives are typically required. Polysomnography may not be required in all patients, but patients should be screened for signs and symptoms of OSA.
Primary aldosteronism is a common cause of resistant hypertension, comprising approximately 20% of such patients. Compared to patients with primary hypertension, those with primary aldosteronism have higher risks of cardiovascular disease (4.2-fold increased risk of stroke, 6.5-fold increased risk of myocardial infarction, and 4.2-fold increased risk of atrial fibrillation), owing to toxic effects of aldosterone on the heart and vessels. Screening may be performed by checking the plasma aldosterone to renin ratio (ARR), obtained in the morning with the patient seated for at least 30 minutes prior to sampling. Confirmatory testing should be performed if screening is positive, i.e., the ARR is greater than 20-30.
Renal ultrasound and doppler may be used to evaluate renal parenchymal disease and renal artery stenosis. Renal parenchymal disease, as with chronic kidney disease, contributes to resistant hypertension through impairment of sodium excretion and fluid retention. CKD may also occur as a consequence of untreated hypertension. Renal artery stenosis most commonly occurs because of atherosclerotic disease, but may occur with Takayasu arteritis, fibromuscular dysplasia, or radiation. Chronic renal ischemia from renal artery stenosis results in activation of the RAAS, thereby worsening hypertension.
Pheochromocytoma and paraganglioma are rare but important causes of resistant hypertension, manifesting as paroxysmal episodes of hypertension. Diagnosis of these tumors is often delayed by 3 years, and up to one third of cases are inherited. Screening may be done by measuring circulating catecholamine metabolites: plasma free or urinary fractionated metanephrines. Patients with essential hypertension may also have elevations of metanephrines. Therefore these studies should be repeated if elevated on initial screening. This is often followed by imaging to detect the tumors, using a combination of CT, MRI and nuclear scans such as MIBG (metaiodobenzylguanidine) and PET scans.
Endocrine disorders such as thyroid disease (hyper and hypothyroidism), hyperparathyroidism, congenital adrenal hyperplasia, and acromegaly may also contribute to resistant hypertension. Screening may be performed with TSH/T4/T3, along with measurement of serum calcium, potassium, renin, and aldosterone. If there is high clinical suspicion, patients with acromegaly commonly have elevated serum insulin-like growth factor-1 (IGF-1) levels and may also have elevated serum growth hormone levels that fail to suppress with oral glucose load. When diagnosed or suspected, consultation with Nephrology, Cardiology, Endocrinology and/or Rheumatology may be required to complete the workup and initiate appropriate therapies.
17. Considerations for Long Term Management of Resistant Hypertension
Patients with resistant hypertension have a higher risk of poor outcomes compared to those without. They are 47% more likely to have myocardial infarct, heart failure, stroke, CKD, or death at median 3.8 years of follow up (Carey et al., AHA resistant hypertension). Persistently elevated 3-month blood pressure measurements in survivors of ICH are associated with higher recurrent stroke risk and mortality (Biffi et al.). Therefore, care should be taken to optimize a patient’s antihypertensive regimen to ensure adherence to medical therapy. This can be achieved by selecting medications with less frequent dosing (once or twice daily) and by choosing combination pills when available. (AHA 2025 guidelines).
Lifestyle changes, including regular exercise and weight loss, should be encouraged. Treadmill walking three times weekly for 8 to 12 weeks has been shown to significantly lower daytime ambulatory BP in patients with resistant hypertension (Dimeo et al.). Body mass index greater than 30 kg/m2 is an independent risk factor of resistant hypertension (Carey et al., AHA resistant hypertension). Patients should be counseled to follow a heart-healthy diet (DASH diet, reduce sodium intake, and eliminate alcohol intake).
Once discharged from the hospital, patients should follow up regularly with their primary care physician, neurocritical care team, and vascular neurology. Many patients in this population have not previously established care with a primary care physician; this is paramount. As much of their follow up care relates to the condition for which they were admitted to the critical care unit rather than other primary medical illness, continued care with the critical care team in the clinic setting is an important adjunct (Salasky et al.). There is paucity of literature on optimal frequency of follow up in this population, and further research on the topic should be pursued.
18. Conclusion
Adequate control of blood pressure remains a cornerstone of treatment in ICH. Early reduction of SBP to target 130-150 mm Hg with smooth, sustained BP control may improve functional outcomes and reduce hematoma expansion in patients with mild to moderate ICH. Resistant hypertension is prevalent in patients with acute spontaneous intracerebral hemorrhage. After initiating oral antihypertensives with a calcium channel blocker and an ACEi/ARB to maximally tolerated doses, the next line of antihypertensive(s)n should be tailored to the patient’s co-morbid conditions. Once resistant hypertension is identified, workup for secondary hypertension should be pursued in addition to referrals to appropriate specialists.
References
- Tsao, Connie W., et al. "Heart disease and stroke statistics—2022 update: a report from the American Heart Association." Circulation 145.8 (2022): e153-e639. [CrossRef]
- Unnithan AKA, Das JM. Hemorrhagic Stroke. [Updated 2025 Dec 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
- Furie, Karen. "Epidemiology and primary prevention of stroke." CONTINUUM: Lifelong Learning in Neurology 26.2 (2020): 260-267.
- Caplan, Louis R., ed. Caplan's stroke. Cambridge University Press, 2016.
- Zhu, Z., Bower, M., Stern-Nezer, S., Atallah, S., Stradling, D., Groysman, L., Dastur, C.K., Akbari, Y. and Yu, W. "Early initiation of oral antihypertensives reduces intensive care unit stay and hospital cost for patients with hypertensive intracerebral hemorrhage." Neurocritical care 32.3 (2020): 707-714.
- Buso, Giacomo, et al. "The global burden of resistant hypertension and potential treatment options." European Cardiology Review 19 (2024): e07.
- Hong D, Stradling D, Dastur CK, et al. Resistant Hypertension after Hypertensive Intracerebral Hemorrhage Is Associated with More Medical Interventions and Longer Hospital Stays without Affecting Outcome. Front Neurol. 2017;8:184. Published 2017 May 3. [CrossRef]
- Biffi, Alessandro, et al. "Impact of uncontrolled hypertension at 3 months after intracerebral hemorrhage." Journal of the American Heart Association 10.11 (2021): e020392.
- Padmanabhan, Sandosh, Mark Caulfield, and Anna F. Dominiczak. "Genetic and molecular aspects of hypertension." Circulation research 116.6 (2015): 937-959.
- Ma, Jun, et al. "Signaling pathways in vascular function and hypertension: molecular mechanisms and therapeutic interventions." Signal transduction and targeted therapy 8.1 (2023): 168.
- Ataei Ataabadi, Ehsan, et al. "Nitric oxide-cGMP signaling in hypertension: current and future options for pharmacotherapy." Hypertension 76.4 (2020): 1055-1068.
- Fountain, J. H., and S. L. Lappin. "Physiology, renin angiotensin system. StatPearls." Treasure Island (FL): StatPearls Publishing (2023).
- Scott, J. H., M. A. Menouar, and R. J. Dunn. "Physiology, Aldosterone [internet]." Treasure Island (FL): StatPearls Publishing (2023).
- Anderson, Craig S., et al. "Intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT): a randomised pilot trial." The Lancet Neurology 7.5 (2008): 391-399.
- Anderson, Craig S., et al. "Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage." New England Journal of Medicine 368.25 (2013): 2355-2365.
- Li, Gang, et al. "Intensive ambulance-delivered blood-pressure reduction in hyperacute stroke." New England Journal of Medicine 390.20 (2024): 1862-1872.
- Qureshi, Adnan I., et al. "Intensive blood-pressure lowering in patients with acute cerebral hemorrhage." New England Journal of Medicine 375.11 (2016): 1033-1043.
- Boldt, Joachim. "Clinical review: Hemodynamic monitoring in the intensive care unit." Critical Care 6.1 (2002): 52.
- Klein, Samuel P., Bart Depreitere, and Geert Meyfroidt. "How I monitor cerebral autoregulation." Critical Care 23.1 (2019): 160.
- Acelajado, Maria Czarina, et al. "Treatment of resistant and refractory hypertension." Circulation research 124.7 (2019): 1061-1070.
- Bokhari MR, Bokhari SRA. Renal Artery Stenosis. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430718/.
- Carey, Robert M., et al. "Resistant hypertension: detection, evaluation, and management: a scientific statement from the American Heart Association." Hypertension 72.5 (2018): e53-e90.
- Salasky, Vanessa, et al. "Neurocritical care recovery clinics: an idea whose time has come." Current Neurology and Neuroscience Reports 23.4 (2023): 159-166.
- Williams, Bryan, et al. "Endocrine and haemodynamic changes in resistant hypertension, and blood pressure responses to spironolactone or amiloride: the PATHWAY-2 mechanisms substudies." The Lancet: Diabetes & Endocrinology” 6.6 (2018): 464-475.
- Zhang, Chao, et al. "Usage of angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker in hypertension intracerebral hemorrhage." Neuropsychiatric disease and treatment (2021): 355-363.
- Yusuf, Sleight, et al. "Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients." The New England journal of medicine 342.3 (2000): 145-153.
- Bicket, Daphne P. "Using ACE inhibitors appropriately." American family physician 66.3 (2002): 461-469.
- Chen, RuiJun, et al. "Comparative first-line effectiveness and safety of ACE (angiotensin-converting enzyme) inhibitors and angiotensin receptor blockers: a multinational cohort study." Hypertension 78.3 (2021): 591-603.
- Ridha, Mohamed, et al. "Antihypertensive medication class and functional outcomes after nonlobar intracerebral hemorrhage." JAMA Network Open 8.2 (2025): e2457770-e2457770.
- McKeever, Rita G., Preeti Patel, and Richard J. Hamilton. "Calcium channel blockers." StatPearls [Internet]. StatPearls Publishing, 2024.
- Hong, Daojun, et al. "Resistant hypertension after hypertensive intracerebral hemorrhage is associated with more medical interventions and longer hospital stays without affecting outcome." Frontiers in neurology 8 (2017): 184.
- Dastur, Cyrus K. and Yu, Wengui. "Current management of spontaneous intracerebral haemorrhage." Stroke and vascular neurology 2.1 (2017).
- Greenberg, Steven M., et al. "2022 guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American Heart Association/American Stroke Association." Stroke 53.7 (2022): e282-e361.
- Carey, Robert M., et al. "Resistant hypertension: detection, evaluation, and management: a scientific statement from the American Heart Association." Hypertension 72.5 (2018): e53-e90.
- Jones, D. W., et al. "AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM guideline for the prevention, detection, evaluation and Management of High Blood Pressure in adults: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines." Hypertension 82 (2025): e212-e316.
- Dimeo F, Pagonas N, Seibert F, Arndt R, Zidek W, Westhoff TH. Aerobic exercise reduces blood pressure in resistant hypertension. Hypertension. 2012;60:653–658. [CrossRef]
- Mounier-Vehier C, Bernaud C, Carré A, Lequeuche B, Hotton JM, Charpentier JC. Compliance and antihypertensive efficacy of amlodipine compared with nifedipine slow-release. Am J Hypertens. 1998 Apr;11(4 Pt 1):478-86. [CrossRef]
- Huang QF, Sheng CS, Li Y, Dou Y, Zheng MS, Zhu ZM, Wang JG; Amlodipine Morning Blood Pressure Surge Study (ARMORS) Investigators. A randomized controlled trial on the blood pressure-lowering effect of amlodipine and nifedipine-GITS in sustained hypertension. J Clin Hypertens (Greenwich). 2019 May;21(5):648-657. [CrossRef]
- Anisman, Steven D., Stephen B. Erickson, and Kim M. Fodor. "Thiazide diuretics." bmj 384 (2024).
- Maiolino, Giuseppe, Matteo Azzolini, and Gian Paolo Rossi. "Mineralocorticoid receptor antagonists therapy in resistant hypertension: time to implement guidelines!" Frontiers in cardiovascular medicine 2 (2015): 3.
- Almajid, Ali N., Preeti Patel, and Manouchkathe Cassagnol. "Amiloride." StatPearls [Internet]. StatPearls Publishing, 2024.
- Lee, Chan Joo, et al. "Spironolactone vs amiloride for resistant hypertension: a randomized clinical trial." JAMA (2025).
- Farzam K, Jan A. Beta Blockers. [Updated 2023 Aug 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan.
- Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet. 2005 Oct 29-Nov 4;366(9496):1545-53. [CrossRef]
- Wiysonge CS, Bradley HA, Volmink J, Mayosi BM, Opie LH. Beta-blockers for hypertension. Cochrane Database of Systematic Reviews 2017, Issue 1. Art. No.: CD002003. [CrossRef]
- Guo QH, Zhu ZM, Feng YQ, Lin JX, Wang JG. Blood pressure lowering effects of β-blockers as add-on or combination therapy: A meta-analysis of randomized controlled trials. J Clin Hypertens (Greenwich). 2023 Mar;25(3):227-237. [CrossRef]
- Mathur, R. P., et al. "Role of alpha blockers in hypertension with benign prostatic hyperplasia." J Assoc Physicians India 62.9 Suppl (2014): 40-44.
- Cushman, William C., et al. "Original Papers. Success and predictors of blood pressure control in diverse North American settings: the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT)." The Journal of Clinical Hypertension 4.6 (2002): 393-404.
- Kalita, Jayantee, Usha Kant Misra, and Bishwanath Kumar. "Is beta-blocker (atenolol) a preferred antihypertensive in acute intracerebral hemorrhage?." Neurological Sciences 34.7 (2013): 1099-1104.
- Heran, Balraj S., Brandon P. Galm, and James M. Wright. "Blood pressure lowering efficacy of alpha blockers for primary hypertension." Cochrane Database of Systematic Reviews 8 (2012).
- Vongpatanasin, Wanpen, et al. "Central sympatholytic drugs." The Journal of Clinical Hypertension 13.9 (2011): 658.
- Chapman, Gavin B., and Neeraj Dhaun. "Endothelin Antagonism: A New Era for Resistant Hypertension?." Hypertension 82.4 (2025): 611-614.
- McComb, Meghan N., James Y. Chao, and Tien MH Ng. "Direct vasodilators and sympatholytic agents." Journal of cardiovascular pharmacology and therapeutics 21.1 (2016): 3-19.
- Caltagirone, M., Vandervelde, R., Chase, C., Walton, S., & Khan, J. (2025). 697: COMPARISON OF NICARDIPINE VS CLEVIDIPINE FOR MANAGEMENT OF HYPERTENSION IN INTRACRANIAL HEMORRHAGE. Critical Care Medicine, 53(1).
- Johnson L, Erdman M, Ferreira J. Comparison of clevidipine vs nicardipine in the treatment of hypertensive urgency and emergency in critically ill patients. Am J Health Syst Pharm. 2024 Oct 23;81(21):e668-e676. Erratum in: Am J Health Syst Pharm. 2025 Mar 7;82(6):254. doi: 10.1093/ajhp/zxae402. [CrossRef] [PubMed]
- Ma L, Hu X, et al. INTERACT3 Investigators. The third Intensive Care Bundle with Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT3): an international, stepped wedge cluster randomised controlled trial. Lancet. 2023 Jul 1;402(10395):27-40. Epub 2023 May 25. Erratum in: Lancet. 2023 Jul 15;402(10397):184. doi: 10.1016/S0140-6736(23)01420-4. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Proposed algorithm for the acute blood pressure management in patients with intracerebral hemorrhage and elevated systolic blood pressure. Abbreviations: ACEi = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; ARNi = angiotensin receptor–neprilysin inhibitor; BP = blood pressure; CCB = calcium channel blocker; CHF = congestive heart failure; ICP = intracranial pressure; ICH = intracerebral hemorrhage; IV = intravenous; MRA = mineralocorticoid receptor antagonist; SBP = systolic blood pressure.
Figure 1.
Proposed algorithm for the acute blood pressure management in patients with intracerebral hemorrhage and elevated systolic blood pressure. Abbreviations: ACEi = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; ARNi = angiotensin receptor–neprilysin inhibitor; BP = blood pressure; CCB = calcium channel blocker; CHF = congestive heart failure; ICP = intracranial pressure; ICH = intracerebral hemorrhage; IV = intravenous; MRA = mineralocorticoid receptor antagonist; SBP = systolic blood pressure.
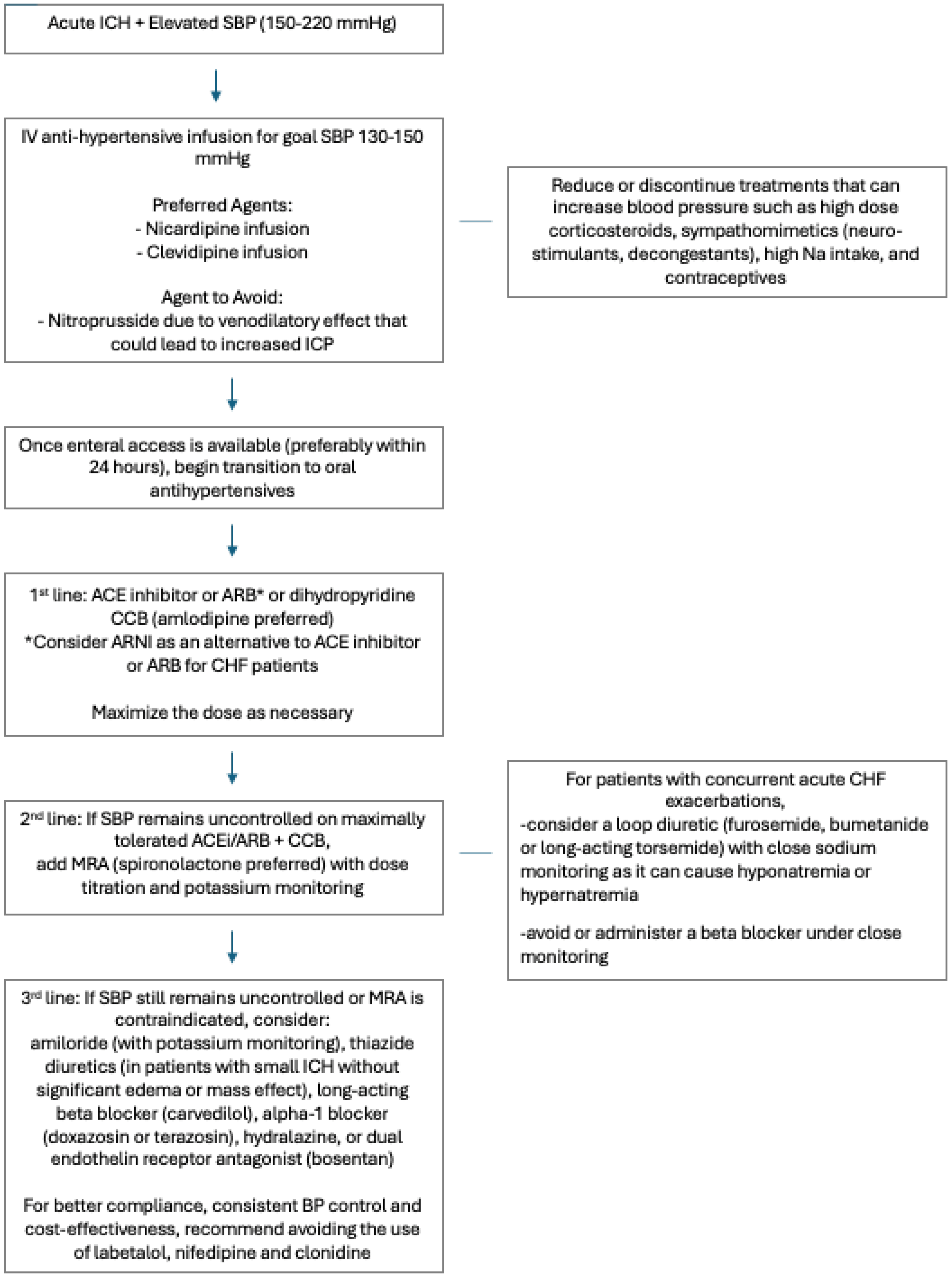

Table 1.
A summary of INTERACT2, ATACH II, INTERACT 3 and INTERACT 4 trials.
| Trial | Timing | Intervention | Major Findings | Safety Outcomes |
|---|---|---|---|---|
| INTERACT 2 (2013)15 | ICH diagnosed within 6 hours of onset | Intensive: SBP < 140 mmHg Standard: SBP < 180 mmHg |
The intensive group had lower modified Rankin scores compared to the standard group (p=0.04). | No significant difference in mortality and nonfatal serious adverse events between the two groups |
| ATACH II (2016)17 | ICH diagnosed within 4.5 hours of onset | Intensive: SBP < 110-139 mmHg Standard: SBP 140-179 mmHg |
No significant difference in primary outcome of death or disability between the two groups | No significant difference in serious adverse events between the two groups The rate of renal adverse events within 7 days was significantly higher in the intensive group compared to the standard group (p=0.002). |
| INTERACT 3 (2023)56 | ICH diagnosed within 6 hours of onset | Care bundle: target SBP < 140 mmHg, strict glucose control, anti-pyrexia and rapid reversal of warfarin-related anticoagulation Usual care: varied depending on hospital practice |
The care bundle group had a lower likelihood of poor functional outcome compared to the usual care group (p=0.015). | The care bundle group had fewer serious adverse events compared to the usual care group (p=0.0098). |
| INTERACT 4 (2024)16 | Presumed acute stroke with elevated SBP (150 mmHg or higher) with the ability to start treatment within 2 hours of symptom onset or last known well | Intervention group: SBP 130-140 mmHg within 30 min until arrival at the hospital Usual care group: SBP < 220 mmHg or DBP < 110 mmHg |
No significant difference in functional outcome between the two groups | No significant difference in the incidence of serious adverse events between the two groups |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



