
Submitted:
03 February 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Introduction: Clostridioides difficile (C. difficile) is a major cause of antibiotic-associated diarrhea and healthcare-associated infections, with rising global incidence and severity due to the emergence of hypervirulent strains. Methods: This review synthesizes recent literature on the epidemiology, pathogenesis, diagnostic approaches, and therapeutic strategies related to C. difficile infection (CDI). Sources were selected from peer-reviewed journals, clinical guidelines, and emerging research between 2020 and 2025. Results: Advances in molecular diagnostics have improved the accuracy and speed of CDI detection. New therapeutic options such as fidaxomicin offer narrower-spectrum antibiotic activity with reduced recurrence rates. Fecal microbiota transplantation (FMT) has emerged as a highly effective option for recurrent CDI. Preventive efforts, including antibiotic stewardship programs and early-phase vaccine trials, show potential in reducing infection rates. Discussion: The management of CDI is evolving rapidly with the integration of precision diagnostics, targeted therapies, and microbiome-based interventions. Preventive strategies are critical, particularly in healthcare settings where C. difficile persists in the environment. Continued research and coordinated public health efforts are essential to reduce disease burden, improve outcomes, and limit transmission. Conclusions: Clostridioides difficile infections remain a major healthcare challenge with rising incidence and recurrent cases. Fidaxomicin has become the preferred first-line therapy. Microbiota-based therapies (like FMT, Rebyota, and Vowst) are highly effective for recurrent CDI prevention. Diagnostic strategies have improved with multi-step testing enhancing accuracy and reducing overtreatment. Future focus lies in vaccines, targeted antimicrobials, and stricter prevention through antibiotic stewardship and hygiene.
Keywords:
Clostridioides difficile
; fidaxomicin
; fecal microbiota transplantation
; CDI diagnosis
; antibiotic stewardship
; vaccine development
1. Introduction
Clostridioides difficile (formerly Clostridium difficile) is a Gram-positive, anaerobic, spore-forming bacterium responsible for a wide spectrum of gastrointestinal diseases, ranging from mild antibiotic-associated diarrhea to life-threatening pseudomembranous colitis. Although once considered primarily a hospital-acquired infection, CDI is increasingly reported in community settings, affecting not only older adults but also younger and otherwise healthy individuals [1].
The virulence of C. difficile is mainly attributed to two exotoxins, TcdA and TcdB, which disrupt intestinal epithelial cells and provoke severe inflammation. Its ability to form durable spores allows the bacterium to persist in hospital environments and on surfaces, making immunocompromised patients and those receiving broad-spectrum antibiotics particularly vulnerable [2].
Hypervirulent lineages such as ribotype 027/NAP1/BI, characterized by elevated toxin production and fluoroquinolone resistance, have been associated with higher morbidity and mortality [3]. Recent studies have also revealed additional modes of transmission, including zoonotic and foodborne routes [4,5]. Genomic analyses show overlap between strains from humans and companion animals, while novel toxigenic ribotypes have been identified in swine production environments, highlighting CDI as a potential One Health challenge [5,6].
In the United States, CDI causes over 450,000 cases and approximately 20,000 deaths annually, with average hospital costs surpassing $15,000 per patient. Contemporary data confirm that CDI continues to impose a considerable burden on working-age adults, leading to both direct healthcare costs and indirect socioeconomic impacts [1]. Community-acquired CDI is strongly associated with prior exposure to certain antibiotics, underlining the importance of stewardship not only in hospitals but also in outpatient settings [7]. On a global scale, the emergence of novel ribotypes and regional variations in strain distribution demonstrate the dynamic epidemiology of CDI and emphasize the need for international surveillance efforts [8,9].
Recurrent disease represents one of the most pressing clinical challenges, with up to 30% of patients experiencing relapse after standard treatment. This is largely due to spore persistence and disruption of the gut microbiota [10]. FMT has proven to be highly effective for recurrence, outperforming conventional therapies [11]. Both capsule-based and colonoscopic FMT approaches have been shown to be safe and effective [12,13], while microbiota-based risk models offer promising predictive tools for identifying patients at greatest risk of relapse [3,14].
Risk factors for CDI extend beyond antibiotic use and include advanced age, prolonged hospitalization, immunosuppressive therapy, and gastrointestinal surgery. Furthermore, asymptomatic carriers serve as reservoirs for transmission in both healthcare and community environments [2]. Environmental contamination remains a significant challenge, as C. difficile spores resist many commonly used disinfectants, underscoring the need for strict cleaning protocols and hand hygiene practices. The COVID-19 pandemic further complicated CDI surveillance and diagnosis, as overlapping gastrointestinal symptoms and strained hospital resources led to under-detection in many cases [15].
Therapeutic options continue to evolve. Although vancomycin and fidaxomicin remain standard treatments, new strategies aim to improve outcomes and reduce recurrence. Oral microbiota-based therapeutics such as Vowst (SER-109) have demonstrated efficacy in lowering recurrence rates following antibiotic treatment [16], while the FDA’s approval of Rebyota in 2022 introduced the first standardized FMT-derived product into clinical practice [17]. Alongside these, advances in microbiome-based diagnostics, vaccine development, and alternative microbiota restoration therapies are under active investigation [14,18].
From a public health perspective, CDI represents a multifaceted challenge at the intersection of pathogen biology, healthcare practice, and host vulnerability. The increase in community-acquired cases, coupled with evidence of zoonotic and foodborne spread, underscores the importance of a One Health framework that integrates human, animal, and environmental surveillance [4,5,6,19]. Beyond its role in infectious disease, emerging evidence suggests that toxigenic strains may contribute to colorectal carcinogenesis, further broadening CDI’s clinical significance [20]. Addressing CDI effectively will therefore require coordinated strategies that combine antimicrobial stewardship, novel therapeutics, robust infection control, and interdisciplinary collaboration across the One Health spectrum [8,10,18,19].
2. Epidemiology
The epidemiology of CDI varies widely across geographic regions and demographic groups. While traditionally regarded as a hospital-associated infection, recent evidence highlights increasing community-acquired cases and the international spread of hypervirulent strains [21]. Beyond traditional hospital-associated infections, surveillance programs and genomic sequencing have revealed diverse sources of CDI. These now include contaminated food, animal reservoirs, and asymptomatic human carriers, underscoring its complex epidemiology and the challenges of effective control [22]. Reported incidence and mortality rates differ across regions, as shown in Table 1.
Notably, North America (USA and Canada) reports the highest CDI incidence and mortality, largely driven by the widespread dissemination of the hypervirulent RT027 strain [23,24]. Europe shows a similarly high burden, though with greater strain diversity (RT001 and RT027). In contrast, Asian countries report comparatively lower incidence rates but unique strain predominance, such as RT017, which has been associated with outbreaks despite lower mortality. Australia demonstrates intermediate incidence with RT014 as the predominant circulating strain [23].
These variations highlight differences in healthcare infrastructure, antimicrobial prescribing practices, diagnostic capacity, and infection-control measures across regions [24]. Furthermore, the detection of CDI outside healthcare facilities emphasizes the growing role of community transmission and zoonotic potential [25]. Ongoing genomic surveillance and international collaboration remain essential for monitoring strain evolution, guiding antimicrobial stewardship, and informing vaccine and therapeutic development strategies [21,22,23,24,25].
To complement Table 1, world map visualization is included, using color intensity (“heat zones”) to represent CDI incidence per 100,000 population by region. Overlaying this with markers indicating predominant ribotypes (e.g., RT027 in North America, RT017 in Asia, RT014 in Australia) would provide an at-a-glance understanding of global distribution patterns. Such a figure would visually emphasize the regional contrasts in both disease burden and strain diversity, making the epidemiological trends more accessible [23].
Figure 1.
Global Distribution of CDI Incidence and Predominant Strains.
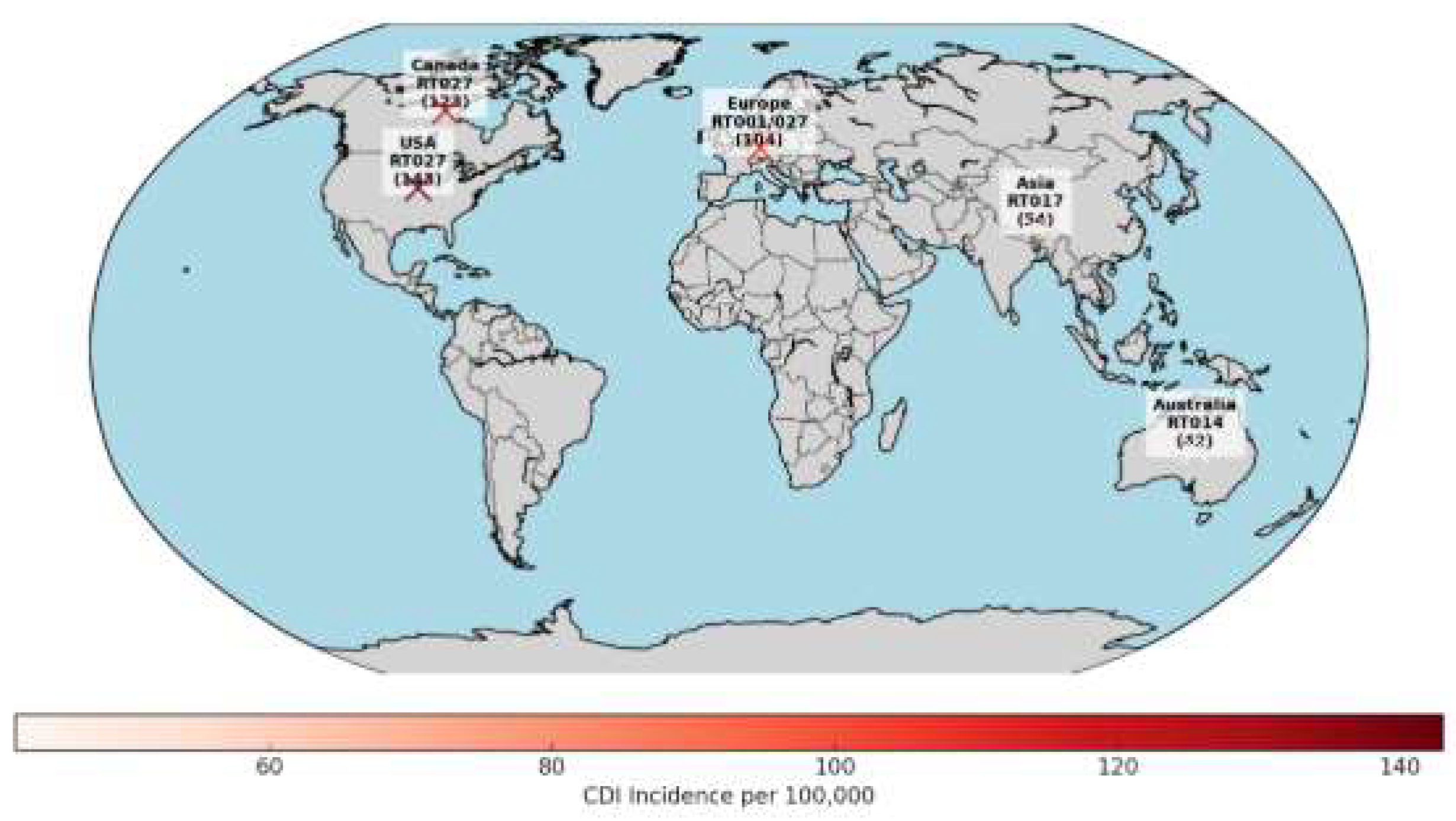
Here’s the world map visualization with a color gradient (heat scale) to represent CDI incidence per 100,000 population.
- Darker red: higher incidence (USA & Canada stand out).
- Lighter red: lower incidence (Asia, Australia).
- Labels include region, predominant strain, and incidence value.
3. Pathogenesis
CDI begins when spores survive gastric acidity and reach the colon. Primary bile acids, such as taurocholate, stimulate spore germination, while secondary bile acids produced by commensal bacteria inhibit this process. Antibiotic-induced disruption of the gut microbiota reduces secondary bile acid levels, creating an environment conducive to spore germination and bacterial proliferation [26,27]. The glucosyltransferase activity of TcdA and TcdB can suppress toxin-specific adaptive immune responses, further promoting disease progression [28].
Once germinated, vegetative C. difficile secretes TcdA and TcdB, which inactivate Rho GTPases. This causes cytoskeletal collapse, epithelial barrier damage, and an inflammatory cascade involving IL-1β, TNF-α, and IL-8 [23,28].
Host immunity is critical in disease severity. Neutrophils and macrophages infiltrate the gut rapidly after toxin-mediated damage; while initially protective, excessive neutrophilic inflammation can worsen tissue injury and contribute to pseudomembrane formation. Adaptive immunity is also important: high serum antibody levels against TcdA and TcdB correlate with reduced recurrence, whereas insufficient immune responses increase susceptibility [28,29]. IL-33 has been shown to protect against recurrent CDI by promoting mucosal repair and immune regulation [30].
A healthy gut microbiota confers colonization resistance through nutrient competition, production of inhibitory metabolites such as short-chain fatty acids, and restoration of secondary bile acids, often mediated by bacteria like Clostridium scindens. Butyrate, for example, suppresses inflammation and directly impacts C. difficile physiology [23,27,31,32,33,34]. C. difficile demonstrates metabolic adaptability, utilizing simple carbohydrates and amino acids via Stickland fermentation, which supports colonization and allows it to compete against commensal microbes [27].
These insights have informed therapeutic strategies, including toxin-neutralizing monoclonal antibodies, microbiome restoration via fecal microbiota transplantation or live biotherapeutics, modulation of bile acid metabolism, and targeting metabolic and immunometabolic pathways to prevent germination and recurrence [23,27,30,31,32,33,34].
4. Diagnosis
4.1. Clinical Assessment
The accurate diagnosis of CDI relies on both clinical evaluation and laboratory testing, as asymptomatic colonization is common and laboratory results alone cannot distinguish infection from carriage [35,36,37]. Evaluation should begin with the patient’s symptoms and risk factors:
- Symptoms: ≥3 unformed stools in 24 hours, abdominal pain or cramping, fever, leukocytosis, and elevated creatinine.
- Severe/complicated CDI: hypotension, ileus, toxic megacolon, perforation, or sepsis.
- Risk factors: recent antibiotic use, hospitalization, older age, immunosuppression, and proton pump inhibitor therapy [37].
4.2. Laboratory Testing
4.3. Multistep Testing Algorithms
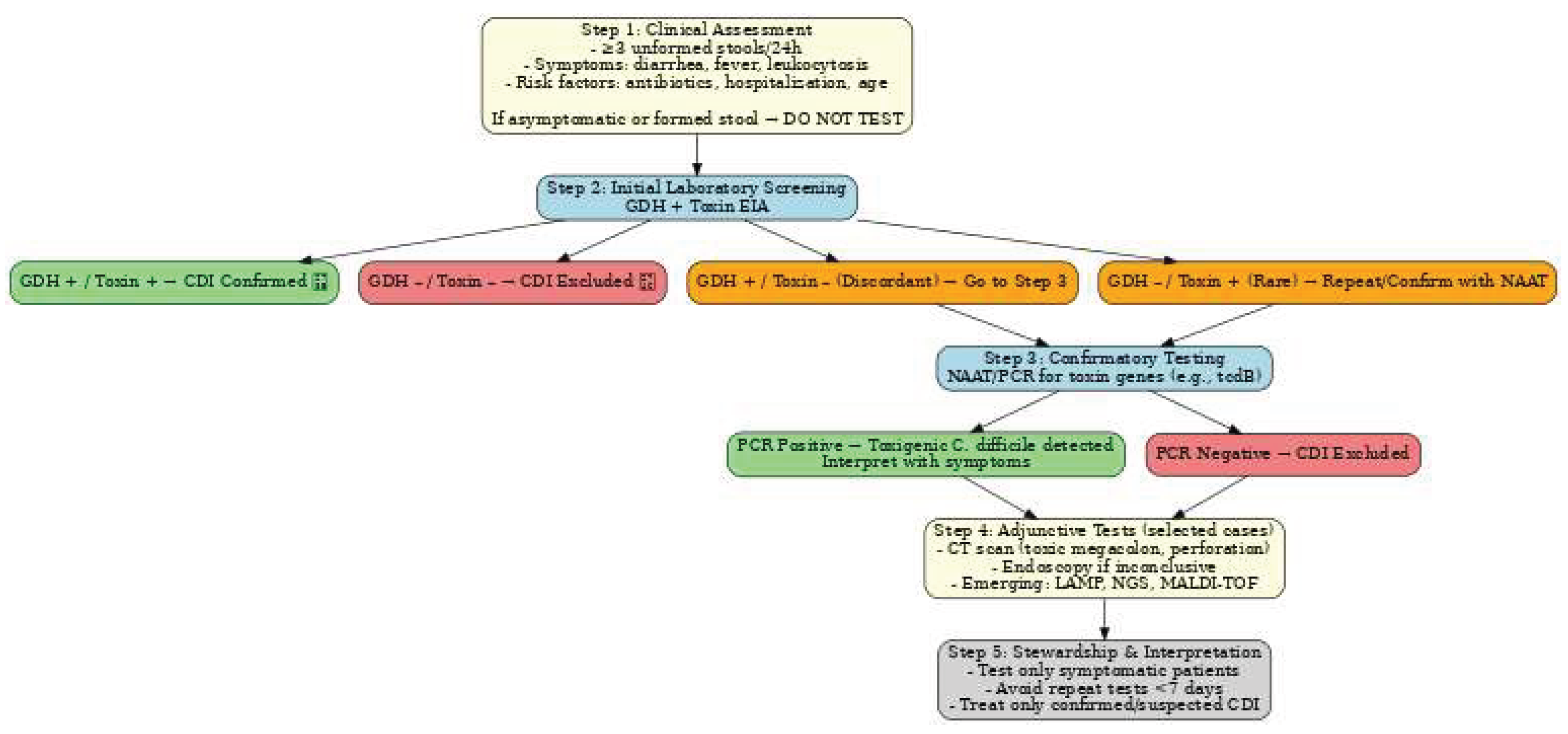
To improve diagnostic accuracy, most laboratories employ two-step or three-step algorithms [35,36,40]:
- a.
- GDH + Toxin EIA:
- ∙
- Both positive: CDI confirmed
- ∙
- Both negative: CDI excluded
- ∙
- Discordant (GDH+/Toxin−):proceed to NAAT
b. NAAT/PCR for toxin genes:
- Positive: toxigenic strain detected; results must be interpreted in clinical context
- Negative: CDI excluded
This strategy balances sensitivity and specificity, helping to avoid missed diagnoses and unnecessary treatment [35,40].
Figure 2.
Diagnostic flowchart for CDI.
4.4. Emerging and Innovative Diagnostics
Recent advancements have improved the speed and accuracy of CDI diagnosis:
- LAMP (loop-mediated isothermal amplification): Rapid, sensitive, and suitable for point-of-care testing [41].
- Next-generation sequencing (NGS): Enables detailed strain typing and antimicrobial resistance profiling [41].
- MALDI-TOF MS: Fast bacterial identification with potential for rapid CDI detection [6].
- Novel immunoassays (e.g., SIMOA, Singulex Clarity): Automated toxin detection with near-perfect sensitivity and specificity [41].

Table 2.
Test Characteristics.
| Test / Strategy | Turnaround | Specificity | Sensitivity | Notes |
|---|---|---|---|---|
| GDH EIA | Hours | Moderate | ~83%-93% | Good screening; does not confirm toxin |
| Toxin A/B EIA | Hours | ~95% | ~75% | Specific; moderate sensitivity |
| NAAT/PCR | Hours | ~95% | ~90% | High sensitivity; risk overdiagnosis |
| GDH + Toxin + NAAT algorithm | Hours-1 day | Very high | Balanced overall | Widely recommended |
| LAMP | Minutes–Hours | 94-99% | 90-100% | Rapid, point-of-care potential |
| MALDI-TOF | Minutes | 90-100% | 90-100% | Fast strain ID |
| SIMOA / Singulex Clarity | <40 minutes | ~100% | ~100% | New automated toxin detection |
4.5. Imaging and Endoscopy
- Computed Tomography scans are indicated in complicated cases, such as toxic megacolon, perforation, or severe colitis [37].
- Endoscopy is reserved for cases with inconclusive stool testing or urgent diagnostic needs; visualization of pseudomembranes is diagnostic but the procedure carries procedural risk in unstable patients [37].
4.6. Diagnostic Stewardship and Guidelines
Guidelines from IDSA and ESCMID emphasize judicious testing to reduce over diagnosis and unnecessary therapy [36,38]:
- Only test patients with clinically significant symptoms.
- Avoid testing formed stool or asymptomatic individuals.
- Repeat testing within 7 days should be avoided unless symptoms persist or worsen.
5. Treatment
Effective management of CDI involves strategies to alleviate symptoms, prevent recurrence, and minimize further disruption of the gut microbiota.
a. First-Line Antibiotic Therapy
For mild to moderate CDI, treatment typically involves oral vancomycin or fidaxomicin, both of which specifically target C. difficile [42]. Fidaxomicin, a narrow-spectrum macrocyclic antibiotic, has been shown to reduce recurrence rates more effectively than vancomycin, making it the preferred choice for initial episodes, particularly in high-risk patients [42,43].In severe or fulminant cases, therapy often requires high-dose oral vancomycin, sometimes in combination with IV metronidazole. Surgical intervention may be indicated for complications such as toxic megacolon or intestinal perforation [44].
b. Management of Recurrent CDI
For patients experiencing multiple recurrences, FMT has proven highly effective. FMT restores gut microbial diversity and reduces relapse rates to below 10% [17,45,46]. Additionally, standardized FMT-derived products such as SER-109 and CP101 provide safer, more controlled alternatives to traditional FMT [17]. Overall, the management of recurrent CDI emphasizes a combination of microbiota restoration, targeted antimicrobial therapy, and immune support to break the cycle of relapse and improve long-term outcomes.
c. Adjunctive and Emerging Therapies
Several additional strategies are being explored to complement standard antibiotic therapy and reduce the risk of CDI recurrence:
- Bezlotoxumab: A monoclonal antibody that targets C. difficile toxin B. When used alongside standard antibiotics, it has been shown to lower the likelihood of recurrent infection [44].
- Ridinilazole: A novel, narrow-spectrum antimicrobial that selectively targets C. difficile while sparing the beneficial gut microbiota, potentially reducing collateral dysbiosis [42].
- Probiotics: Certain probiotic formulations may offer supportive benefits in preventing recurrence; however, current evidence is limited and does not support routine use as a standard therapy [44].
- mRNA vaccines: Currently under early investigation, these vaccines aim to provide immune protection against CDI, representing a promising preventive approach for high-risk populations [47].
These adjunctive and emerging therapies reflect a broader trend toward microbiota-sparing treatments and immune-based interventions that aim to reduce recurrence rates while preserving gut microbial health.
d. Treatment Goals
Effective management of CDI focuses on multiple, interrelated objectives:
- Minimize recurrence risk. Recurrence is common in CDI, particularly after the first episode. Treatment strategies aim to lower relapse rates through appropriate antimicrobial selection, microbiota restoration interventions such as FMT or standardized FMT-derived products, and adjunctive therapies like bezlotoxumab [48,50,51].
- Preserve gut microbiota integrity. Maintaining a healthy microbial community is crucial for long-term resistance against C. difficile overgrowth. Narrow-spectrum antibiotics like fidaxomicin, microbiota-sparing agents such as ridinilazole, and live biotherapeutics help reduce collateral damage to commensal flora [49,50].
- Support host immune defenses. Strengthening the patient’s immune response against C. difficile toxins and infection is an emerging focus of therapy. Approaches include monoclonal antibodies, immunomodulatory strategies, and investigational vaccines, all designed to prevent relapse and improve long-term outcomes [51,52].
6. Prevention and Control
Effective prevention of CDI requires a comprehensive, multifaceted strategy that disrupts transmission, preserves gut microbiota, and facilitates early recognition of cases. Antibiotic stewardship remains the foundation of prevention, as broad-spectrum antimicrobials—particularly fluoroquinolones, cephalosporins, and clindamycin—are strongly linked to CDI risk. Stewardship initiatives should emphasize targeted antimicrobial selection, strict initiation criteria, and limiting treatment duration. Incorporating prescriber feedback, routine audits, and electronic medical record (EMR) alerts has been shown to reduce inappropriate antibiotic exposure and subsequently lower CDI incidence [53].
Equally critical are infection prevention and control (IPC) measures, given the organism’s ability to form hardy spores. Alcohol-based hand rubs are ineffective against spores, making thorough handwashing with soap and water essential after patient contact or exposure to contaminated environments. Environmental cleaning protocols should use sporicidal agents such as sodium hypochlorite at concentrations of 5,000 ppm for both daily and terminal room disinfection. Standardized cleaning procedures, combined with auditing and monitoring, enhance compliance and effectiveness. Healthcare workers should wear gloves and disposable gowns when entering the rooms of symptomatic patients and remove them prior to exit to prevent cross-transmission [54].
Early identification and isolation of symptomatic patients is vital to containing nosocomial spread. Suspected cases should be isolated in private rooms with dedicated bathrooms immediately, without waiting for laboratory confirmation. During outbreaks, cohorting may be employed if private rooms are limited. Active surveillance programs—tracking incidence, severity, and recurrence rates—are essential for identifying clusters and guiding infection control interventions. Data should be routinely reviewed by infection prevention teams and reported to institutional and public health authorities as appropriate [54].
Several emerging preventive strategies are under investigation. Vaccine candidates targeting toxins A and B have advanced to Phase III clinical trials, although one large trial was terminated due to lack of efficacy [55]. Adjunctive approaches such as probiotics and bile acid modulators show variable benefit, while the monoclonal antibody bezlotoxumab has demonstrated significant reductions in CDI recurrence, particularly among high-risk groups including older adults and immunocompromised patients [56,57]. A systematic review confirmed modest recurrence reduction even in primary CDI [58], and a Mayo Clinic multicenter real-world cohort and meta-analysis found bezlotoxumab to significantly lower recurrence compared to standard therapy [59]. Despite these developments, the most effective prevention continues to rely on robust antibiotic stewardship, strict IPC adherence, and rapid case management to protect vulnerable patient populations.
7. Emerging and Experimental Perspectives
5.1. Microbiome-Based Therapies and Probiotics
Restoring intestinal microbial diversity is a key strategy for preventing recurrence in Clostridioides difficile infection (CDI). Although fecal microbiota transplantation (FMT) has demonstrated high efficacy, its widespread adoption is limited by safety, regulatory, and logistical constraints [60]. In recent years, two standardized live biotherapeutic products (LBPs) have been approved by the U.S. Food and Drug Administration. REBYOTA® (RBX2660), an enema-based microbiota suspension, significantly reduced recurrence rates in the phase 3 PUNCH-CD3 trial [61], with sustained safety and efficacy confirmed in long-term follow-up [62]. VOWST™ (SER-109), an oral consortium of purified Firmicutes spores, was evaluated in the ECOSPOR III/IV trials and demonstrated durable recurrence prevention, leading to its approval in 2023 [63].
Additional microbiome-based approaches are in late-stage development. VE303, a defined eight-strain bacterial consortium, achieved over 80% reduction in recurrence in a phase 2 study and is now undergoing evaluation in the phase 3 RESTORATiVE303 trial [64,65]. In contrast, other candidates such as CP101 were discontinued following inconclusive phase 3 results.
The use of probiotics, including Saccharomyces boulardii and Lactobacillus species, has also been explored for primary prevention of CDI. However, recent clinical evidence indicates limited efficacy, and routine use is not currently recommended by major guidelines.
5.2. Vaccines: Toxoid and mRNA Platforms
Preventive vaccination strategies have primarily targeted toxins A and B. Despite early promise, conventional toxoid vaccines have faced significant setbacks. The Sanofi Pasteur candidate was terminated after failing to demonstrate clinical benefit in a phase 3 trial [66]. Similarly, Pfizer’s bivalent toxoid vaccine (PF-06425090; CLOVER trial) did not meet its primary endpoint, although secondary analyses suggested reduced duration of illness and healthcare utilization in vaccine recipients [67].
Early-phase clinical studies have yielded promising immunogenicity results. In a randomized trial of older adults, the bivalent toxoid vaccine generated strong antibody responses to both toxins A and B [68]. Similarly, a double-blind study in healthy adults demonstrated that the vaccine elicited durable humoral immunity, reinforcing its potential as a preventive strategy against C. difficile infection [69].
In light of these challenges, attention has shifted toward innovative vaccine platforms. mRNA-based vaccines encapsulated in lipid nanoparticles have generated robust systemic and mucosal immunity against C. difficile toxins and virulence factors in preclinical models [70,71]. These candidates remain at the experimental stage, and human trials have yet to commence.
5.3. Narrow-Spectrum Antimicrobials
Novel antimicrobial agents are being developed to minimize disruption of the gut microbiota while effectively targeting C. difficile. Ridinilazole, evaluated in two phase 3 randomized trials, did not demonstrate superiority over vancomycin in sustained clinical response, though recurrence rates were reduced in the ridinilazole arm [72]. Another promising agent, CRS3123, a methionyl-tRNA synthetase inhibitor, has shown selective inhibition of C. difficile while sparing commensal bacteria. Phase 2 trials reported high initial cure rates and markedly reduced recurrence compared with vancomycin [73,74].
5.4. Immunotherapies and Host-Directed Approaches
Bezlotoxumab, a monoclonal antibody targeting toxin B, remains the only licensed immunotherapeutic agent for CDI. Although pivotal trials were conducted prior to 2019, real-world use continues to support its benefit in reducing recurrence among high-risk populations. Several experimental immunotherapies, including nanobody-based strategies, are in preclinical development [44].
In parallel, host-targeted interventions are being explored. Modulation of bile acid metabolism—particularly through ursodeoxycholic acid supplementation—has shown promise in preventing spore germination and colonization, with early clinical trials ongoing [60]. Such approaches highlight the potential of targeting the host environment to complement conventional antimicrobial and immunologic therapies.
Table 3.
Emerging C. difficile therapies.
| Therapeutic Class | Candidate | Mechanism of Action | Trial Phase | Key Outcomes | Current Status |
|---|---|---|---|---|---|
| Microbiome-Based Therapy | REBYOTA (RBX2660) | Live microbiota consortium, restores gut microbial diversity | Phase 3 | Significantly reduced CDI recurrence; durable safety in long-term follow-up | FDA-approved |
| Microbiome-Based Therapy | VOWST (SER-109) | Oral Firmicutes spore consortium, restores gut microbiota | Phase 3 | Reduced recurrence rates in recurrent CDI | FDA-approved |
| Microbiome-Based Therapy | VE303 | Defined 8-strain bacterial consortium | Phase 3 (RESTORATIVE303) | >80% reduction in recurrence in phase 2 | Phase 3 ongoing |
| Vaccine – Toxoid | Sanofi Pasteur bivalent toxoid | Neutralizes toxins A & B | Phase 3 | Failed primary endpoint; immunogenicity observed in earlier trials | Development discontinued |
| Vaccine – Toxoid | Pfizer PF-06425090 (CLOVER) | Neutralizes toxins A & B | Phase 3 | Did not meet primary endpoint; secondary analyses showed reduced duration of illness | Development discontinued |
| Vaccine – mRNA | Experimental mRNA vaccines | Lipid nanoparticle mRNA encoding toxins A & B | Preclinical | Strong systemic & mucosal immunity in animal models | Preclinical |
| Narrow-Spectrum Antimicrobial | Ridinilazole | Selective inhibition of C. difficile | Phase 3 | Lower recurrence rates vs vancomycin; no superiority for sustained clinical response | Completed trials; not approved |
| Narrow-Spectrum Antimicrobial | CRS3123 | Methionyl-tRNA synthetase inhibitor, spares commensals | Phase 2 | High initial cure, markedly reduced recurrence | Phase 2 completed; further trials ongoing |
| Immunotherapy | Bezlotoxumab | Monoclonal antibody against toxin B | Post-marketing/ real-world | Reduces recurrence in high-risk patients | FDA-approved |
| Host-Directed | Ursodeoxycholic acid | Modulates bile acids, inhibits spore germination | Early clinical trials | Preliminarily prevents colonization and recurrence | Experimental/ ongoing |
The therapeutic landscape for CDI is rapidly advancing. FDA approval of microbiome- based therapies such as REBYOTA and VOWST represents a major milestone, VE303 may provide a defined-consortium alternative if phase 3 trials are successful. Narrow-spectrum antimicrobials such as CRS3123 show potential to reduce recurrence by sparing the commensal microbiota. Despite the failure of toxoid vaccines in late-stage studies, mRNA-based vaccine platforms offer a novel preventive strategy. Immunotherapies such as bezlotoxumab remain integral in high-risk patients, and host-targeted interventions, particularly those modulating bile acid pathways, may represent the next frontier in recurrence prevention. Collectively, these approaches signify a shift from broad-spectrum antimicrobial strategies toward precision modulation of the microbiota–host–pathogen axis in CDI management.
6. Health Economics and Outcomes
CDI imposes substantial clinical, economic, and humanistic burdens. Hospital-attributable costs often exceed USD 20 000 per case, primarily driven by recurrent episodes, which affect approximately 20–30% of patients following initial infection. Fidaxomicin has demonstrated superior sustained cure rates and significantly reduced recurrence compared with vancomycin, as shown in randomized trials and meta-analyses [75]. Economic evaluations conducted in diverse settings—such as Japan and Spain—illustrate that despite higher acquisition costs, fidaxomicin’s improved outcomes offset expenses, leading to favorable cost-effectiveness. For example, a Japanese semi-Markov model estimated an ICER of JPY 5 715 183 per QALY gained, approaching national willingness-to-pay thresholds [76]. In Spain, an extended-pulsed fidaxomicin regimen showed improved sustained cure and reduced recurrences compared with vancomycin in patients aged ≥ 60 years, providing economic justification for its usage [77].
Further, a lifetime-horizon Markov model assessed cost-effectiveness of standard and extended-pulsed fidaxomicin, and bezlotoxumab plus vancomycin versus standard vancomycin in the US societal context. Extended-pulsed fidaxomicin dominated vancomycin (i.e., lower cost, higher QALYs). Standard fidaxomicin achieved an ICER of only USD 495 per QALY gained, while bezlotoxumab added to vancomycin yielded an ICER of USD 17 746 per QALY—below the US willingness-to-pay threshold of USD 150 000 [78].
Equally important are recurrence-prevention strategies beyond pharmacologic agents. A decision-analytic model evaluating FMT (via colonoscopy or oral capsules) versus fidaxomicin, vancomycin, and bezlotoxumab in first recurrent CDI found FMT strategies to be cost-effective—colonoscopic FMT incuring the lowest cost (~USD 5 250) and oral-capsule FMT yielding an ICER of USD 31 205 per QALY. At current pricing, bezlotoxumab was not cost-effective in this model [79].
The humanistic impact of CDI is profound. A French prospective study using EQ-5D-3L reported utility scores declining sharply from 0.542 at baseline to 0.050 during acute infection, resulting in a mean decrement of 0.492 and an estimated loss of approximately 0.028 QALYs per episode [80]. This underscores the significant quality-of-life burden associated with CDI, reinforcing the value of recurrence prevention.
Collectively, recent evidence affirms that preventing recurrence is the principal driver of both economic efficiency and quality-of-life gains in CDI management. Fidaxomicin—particularly in extended-pulsed regimens—offers superior clinical outcomes and cost-effectiveness under many scenarios. Adjunctive therapies such as bezlotoxumab provide added preventive value at acceptable cost in high-risk groups, while FMT (especially via capsules or colonoscopy) presents as a cost-effective option for recurrence [78,79]. Incorporating quantified utility losses into economic models remains essential to fully capture the humanistic burden of CDI [80]. Health policy strategies that use prevention-focused, high-value treatments targeted at vulnerable populations are likely to optimize both clinical outcomes and economic resource utilization [75,76,77,78,79].
7. Discussion
CDI continues to pose a substantial clinical and economic burden worldwide. Despite advances in antimicrobial therapy and infection control, recurrence rates remain high, with 20–30% of patients experiencing relapse after an initial episode [81,82]. This underscores the necessity for strategies that go beyond symptom management to include prevention of recurrence, preservation of the gut microbiota, and host-directed interventions.Antibiotics remain the mainstay of CDI treatment, with fidaxomicin and vancomycin recommended as first-line agents. Fidaxomicin offers advantages over vancomycin due to its narrower spectrum and lower recurrence rates, particularly in patients at high risk of relapse, despite higher acquisition costs [82]. Cost-effectiveness analyses indicate that the long-term benefits of sustained cure often outweigh the initial expense [82]. Extended-pulsed fidaxomicin regimens have been shown to be more effective than standard vancomycin therapy, and adjunctive treatments such as bezlotoxumab can further reduce the likelihood of recurrence in vulnerable populations [83].
Restoring the gut microbiota has emerged as a transformative approach in CDI management. FMT demonstrates consistently high efficacy in preventing recurrent CDI, with cure rates exceeding 90% in refractory cases [84,85]. However, donor variability and regulatory challenges have limited its widespread adoption. Standardized live biotherapeutic products (LBPs), such as REBYOTA and VOWST, offer reproducible and controlled alternatives. Emerging next-generation therapies, including VE303, aim to refine this approach by providing precision-engineered microbial consortia [84].
Prevention is a central goal at both individual and population levels. While traditional toxoid-based vaccines have faced setbacks, newer platforms such as mRNA vaccines show promise in eliciting durable immune responses in high-risk populations [86]. Host-directed therapies, including bile acid modulators and monoclonal antibodies like bezlotoxumab, complement antibiotic therapy by enhancing colonization resistance and neutralizing toxins [83]. These strategies reflect a paradigm shift from solely targeting the pathogen toward modulating the microbiota–host–pathogen axis.
System-level strategies are critical to CDI control. Antibiotic stewardship, rigorous hand hygiene, sporicidal cleaning, and rapid case identification are essential to limit transmission and preserve the effectiveness of novel therapies [10]. Reducing inappropriate antibiotic exposure not only prevents CDI but also mitigates selective pressures that could undermine future interventions.
CDI imposes significant economic and humanistic burdens. Sustained cure achieved through fidaxomicin, FMT, or LBPs has been identified as the primary driver of cost-effectiveness and improved patient outcomes [81,82,84,85]. Incorporating patient-reported outcomes into economic analyses highlights the profound functional and societal impact of recurrent CDI, emphasizing the value of preventive strategies.
The optimal management of CDI will likely involve an integrated, precision-based framework combining targeted antibiotics, microbiome restoration, immune modulation, and comprehensive public health measures [83,84,85,86]. Advances in rapid diagnostics, microbiome and genomic profiling, global surveillance, and vaccine development will be critical in achieving sustainable reductions in CDI incidence and recurrence.
CDI remains a complex challenge at the intersection of antimicrobial efficacy, microbial ecology, and healthcare economics. The growing focus on microbiota-sparing therapies, preventive immunization, and host-directed interventions marks a new era in CDI management, offering the potential to significantly improve patient outcomes and reduce the burden on healthcare systems [10,81,82,83,84,85,86].
8. Future Directions
As the clinical and public health burden of CDI continues to grow, innovative strategies are needed to improve prevention, diagnosis, and treatment. Several promising avenues warrant focused research and investment:
- Personalized medicine: The heterogeneity of patient responses to CDI therapies highlights the need for individualized approaches. Profiling a patient’s gut microbiome, immune status, and genetic susceptibility could guide targeted interventions—ranging from tailored antibiotic regimens to microbiome-modulating therapies—potentially reducing recurrence rates and improving outcomes.
- Rapid point-of-care diagnostics: Early detection is critical to preventing the spread of CDI and initiating timely treatment. Advances in portable, rapid diagnostic tools—such as molecular assays or biosensors—could enable near-instant identification of infection in community and outpatient settings, reducing delays associated with laboratory-based testing and limiting nosocomial transmission.
- Standardized FMT products: FMT has emerged as a highly effective therapy for recurrent CDI, but variability in donor material and protocols limits its widespread adoption. Developing standardized, well-characterized microbial consortia or “off-the-shelf” microbiota products could improve safety, reproducibility, and regulatory compliance, enabling broader and more consistent clinical application.
- Global surveillance networks: Coordinated international monitoring of CDI strains, antimicrobial resistance patterns, and outbreak clusters is essential for timely public health responses. Leveraging genomic sequencing and real-time data sharing can facilitate early identification of hypervirulent or resistant strains, guiding infection control strategies and informing global treatment guidelines.
- Prophylactic strategies: Prevention remains the ultimate goal in CDI management. Promising avenues include vaccine development targeting key bacterial toxins, bile acid-based therapies that restore colonization resistance, and precision probiotics designed to reinforce the gut microbiome. Rigorous clinical validation of these approaches could significantly reduce both primary infections and recurrences, particularly in high-risk populations.
Investment in these areas will be critical not only for improving patient outcomes but also for achieving long-term control of CDI. By integrating precision medicine, advanced diagnostics, microbiome-based therapies, and global surveillance, the field moves closer to mitigating the impact of this persistent healthcare challenge and ultimately reducing CDI to a manageable, low-burden infection.
Table 4.
Future Directions for Clostridioides difficile.
| Research Priorities | Potential Benefits | Focus | Future Direction |
|---|---|---|---|
| Microbiome profiling, host-genetics studies | Reduced recurrence, optimized treatment efficacy | Tailoring therapy using microbiome and host genetics | Personalized Medicine |
| Development of portable molecular/biosensor assays | Timely treatment, limited transmission | Faster, accessible testing for early detection | Rapid Diagnostics |
| Defining microbial consortia, regulatory frameworks | Greater safety, consistency, and clinical adoption | Safe, reproducible microbiota-based therapies | Standardized FMT Products |
| Genomic sequencing and real-time reporting | Early outbreak detection, global preparedness | Cross-border monitoring of strains and resistance | Global Surveillance |
| Large-scale clinical trials, mechanistic studies | Prevention of primary and recurrent CDI | Vaccines, bile acid therapies, targeted probiotics | Prophylactic Strategies |
9. Conclusions
CDI infection remains a formidable challenge at the intersection of antimicrobial stewardship, microbial ecology, and healthcare resource management. Despite substantial advances in antibiotic therapy, recurrence rates remain unacceptably high, underscoring the limitations of pathogen-targeted approaches alone. Emerging strategies that prioritize microbiome preservation, host-directed interventions, and precision therapeutics-including live biotherapeutic products, fecal microbiota transplantation, and monoclonal antibodies-offer the potential to transform outcomes for high-risk patients. Concurrently, system-level interventions such as rigorous infection prevention protocols and antibiotic stewardship are critical to sustaining the efficacy of these novel therapies.
The integration of antimicrobial therapy, microbiome restoration, immunoprophylaxis, and rapid diagnostics represents a paradigm shift toward a holistic, patient-centered model of CDI management. Economic and quality-of-life analyses further reinforce that strategies aimed at sustained cure-not merely symptomatic relief-provide the greatest value to patients and healthcare systems alike. Looking forward, precision medicine approaches leveraging microbiome and genomic profiling, combined with ongoing vaccine development and global surveillance, are likely to define the next era of CDI management. Collectively, these advances signal a transition from reactive treatment to proactive, recurrence-preventive care, with the potential to substantially reduce the clinical and economic burden of CDI worldwide.
Author Contributions
Conceptualization, N.K. and D.C.; methodology, K.K.; validation, N.K., N.M., and N.P.; formal analysis, G.M. and D.K.; investigation, N.K., A.T., M.V.C. and S.T.; data curation, N.K., K.K., G.M. and D.K.; writing-original draft preparation, N.K.; writing-review and editing, S.T., M.V.C. and A.T.; visualization, N.K. and N.M.; supervision, D.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
We thank the two anonymous journal reviewers and the handling editor, Ms. Sindy Li, for helpful comments on an earlier draft. The responsibility for the content and any remaining errors remains exclusively with the authors.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CDI | Clostridioides difficile infection |
| GDH | Glutamate dehydrogenase |
| LAMP | Loop-mediated isothermal amplification |
| NGS | Next-generation sequencing |
| FMT | Fecal microbiota transplantation |
References
- Olsen, MA; Stwalley, D; Tipping, E; Keller, M; Yu, T; Dubberke, ER. Incidence, healthcare and out-of-pocket costs, and mortality of Clostridioides difficile infection among US adults aged 18 to 64 years. Antimicrob Steward Healthc Epidemiol. 2024, 4(1), e215. [Google Scholar]
- Bednárik, DS; et al. Comparative effectiveness of different therapies for Clostridioides difficile infection in adults: a systematic review and network meta-analysis of randomized controlled trials. Lancet Reg Health Eur. 2025, 49, 101151. [Google Scholar] [CrossRef] [PubMed]
- Van Rossen, TM; van Beurden, YH; Bogaards, JA; Budding, AE; Mulder, CJJ; Vandenbroucke-Grauls, CMJE. Fecal microbiota composition is a better predictor of recurrent Clostridioides difficile infection than clinical factors in a prospective, multicentre cohort study. BMC Infect Dis. 2024, 24, 687. [Google Scholar] [CrossRef]
- Knight, DR; Elliott, B; Chang, BJ; Perkins, TT; Riley, TV. Diversity and evolution in the genome of Clostridioides difficile. Clin Microbiol Rev. 2020, 33(3), e00076-19. [Google Scholar]
- Alves, F; Castro, R; Pinto, M; et al. Molecular epidemiology of Clostridioides difficile in companion animals: Genetic overlap with human strains and public health concerns. Front Public Health 2023, 10, 1070258. [Google Scholar] [CrossRef] [PubMed]
- Alves, F; Nunes, A; Sequeira, A; et al. Assessment of the transmission dynamics of Clostridioides difficile in a farm environment reveals the presence of a new toxigenic strain connected to swine production. Front Microbiol. 2022, 13, 858310. [Google Scholar] [CrossRef]
- Zhang, J; Chen, L; Gomez-Simmonds, A; et al. Antibiotic-specific risk for community-acquired Clostridioides difficile infection in the United States from 2008 to 2020. Antimicrob Agents Chemother. 2022, 66, e01129-22. [Google Scholar] [CrossRef]
- Liu, C; Monaghan, T; Yadegar, A; et al. Insights into the evolving epidemiology of Clostridioides difficile infection and treatment: A global perspective. Antibiotics (Basel) 2023, 12(7), 1141. [Google Scholar] [CrossRef]
- Dresler, J; et al. Characteristics of Clostridioides difficile isolates circulating in Slovak hospitals. In Biologia; 2023. [Google Scholar]
- Johnson, S; Lavergne, V; Skinner, AM; Gonzales-Luna, AJ; Garey, KW; Kelly, CP; Wilcox, MH. Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update on management of Clostridioides difficile infection in adults. Clin Infect Dis. 2021, 73(5), e1029–44. [Google Scholar] [CrossRef]
- Minkoff, NZ; Aslam, S; Medina, M; Tanner-Smith, EE; Zackular, JP; Acra, S; et al. Fecal microbiota transplantation for the treatment of recurrent Clostridioides difficile (Clostridium difficile). Cochrane Database Syst Rev 2023, (4). [Google Scholar]
- Vaughn, BP; Fischer, ME; Kelly, CR. Effectiveness and safety of colonic and capsule fecal microbiota transplantation for recurrent Clostridioides difficile infection. Clin Gastroenterol Hepatol. 2023, 21, 1330–7. [Google Scholar] [CrossRef]
- Tariq, R; Syed, T; Yadav, D; Prokop, LJ; Singh, S; Loftus, EV, Jr.; Pardi, DS; Khanna, S. Outcomes of fecal microbiota transplantation for recurrent Clostridioides difficile infection: A systematic review and meta-analysis. Clin Infect Dis. 2023, 57(3), 285–293. [Google Scholar]
- Van Rossen, TM; Ooijevaar, RE; Vandenbroucke-Grauls, CMJE; et al. Fecal microbiota composition is a better predictor of recurrent Clostridioides difficile infection than clinical factors in a prospective, multicentre cohort study. BMC Infect Dis. 2024, 24, 687. [Google Scholar] [CrossRef]
- Vázquez-Cuesta, S; Olmedo, M; Reigadas, E; et al. Clostridioides difficile infection epidemiology and clinical characteristics in the COVID-19 pandemic. Front Med (Lausanne) 2022, 9, 953724. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, A; et al. Reducing recurrent Clostridioides difficile infection risk with oral microbiome therapy (Vowst/SER-109); Gastroenterology Advisor. , 2023. [Google Scholar]
- FDA. FDA approves first fecal microbiota product: Rebyota approved for the prevention of recurrence of Clostridioides difficile infection in adults; U.S. Food and Drug Administration: Silver Spring (MD), 30 Nov 2022. [Google Scholar]
- Benech, N; Barbut, F; Fitzpatrick, F; Krutova, M; Davies, K; Druart, C; et al. Update on microbiota-derived therapies for recurrent Clostridioides difficile infections. Clin Microbiol Infect. 2024, 30(4), 462–8. [Google Scholar] [CrossRef]
- Alexiou, S; Diakou, A; Kachrimanidou, M. The role of Clostridioides difficile within the One Health framework: A review. Microorganisms 2025, 13(2), 429. [Google Scholar] [CrossRef]
- Drewes, JL; Chen, J; Markham, NO; et al. Human colon cancer–derived Clostridioides difficile strains drive colonic tumorigenesis in mice. Cancer Discov 2022. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z; Wu, J; Ye, X; Jin, J; Zhang, W. Global burden, trends, and inequalities of Clostridioides difficile infections from 1990 to 2021 and projections to 2040: a systematic analysis. Antibiotics 2025, 14(7), 652. [Google Scholar] [CrossRef] [PubMed]
- Akorful, RAA; Odoom, A; Awere-Duodu, A; Donkor, ES. The global burden of Clostridioides difficile infections, 2016–2024: A systematic review and meta-analysis. Infect Dis Rep. 2025, 17(2), 31. [Google Scholar] [CrossRef]
- Finn, E; Andersson, FL; Madin-Warburton, M. Burden of Clostridioides difficile infection (CDI): a systematic review of the epidemiology of primary and recurrent CDI. BMC Infect Dis. 2021, 21(1), 456. [Google Scholar] [CrossRef]
- Kwok, R; Marshall, JC; Jørgensen, SL; Fawley, WN; Wilcox, MH. Incidence of public health surveillance-reported Clostridioides difficile infections in thirteen countries worldwide: a narrative review. J Hosp Infect. 2024, 136, 1–12. [Google Scholar]
- Tschudin-Sutter, S. The Changing Landscape of Clostridioides difficile Infection. EMJ Rev Microbiol Infect Dis 2023. [Google Scholar]
- Seekatz, AM; Safdar, N; Khanna, S. The role of the gut microbiome in colonization resistance and recurrent Clostridioides difficile infection. Lancet Infect Dis. 2022, 22(11), e283–e292. [Google Scholar] [CrossRef]
- Zhang, Y; Zhang, L; Zhang, X; et al. Clostridium difficile infection: pathogenesis and treatment. Front Microbiol 2022, 13, 798356. [Google Scholar]
- Maslanka, JR; Londregan, JA; Denny, JE; et al. Clostridioides difficile toxin A and toxin B inhibit toxin-specific adaptive immune responses through glucosyltransferase-dependent activity. In Mucosal Immunol; 16 Aug 2025; ISBN S1933-0219(25)00087-X. [Google Scholar]
- Ghosh, S; Antunes, A; Rinta-Kokko, H; Chaparova, E; Lay-Flurrie, S; Tricotel, A; et al. Clostridioides difficile infections, recurrences, and clinical outcomes in real-world settings from 2015 to 2019: The RECUR England study. Int J Infect Dis. 2024, 140, 31–8. [Google Scholar] [CrossRef]
- Naz, F; Uddin, MJ; Hagspiel, N; Young, MK; Tyus, D; Boone, R; et al. IL-33 protects from recurrent Clostridioides difficile infection by restoration of humoral immunity. J Clin Invest. 2025, 135(9). [Google Scholar] [CrossRef] [PubMed]
- Li, W; Chen, H; Tang, J; et al. Interplay between bile acids and intestinal microbiota: Regulatory mechanisms and therapeutic potential for infections. Pathogens 2024, 13(8), 702. [Google Scholar] [CrossRef]
- Ridlon, JM; Alves, JM; Hylemon, PB; Bajaj, JS. Bile salt hydrolases shape the bile acid landscape and restrict Clostridioides difficile. Nat Microbiol. 2023, 8, 1234–45. [Google Scholar]
- Zeng, J; Chen, Y; Li, X; et al. Lipidomics, microbiota, and intestinal Clostridioides difficile infection. Int J Mol Sci. 2025, 26(17), 8214. [Google Scholar]
- Collins, SL; Stine, JG; Bisanz, JE; et al. Bile acids and the gut microbiota: metabolic interactions and impacts on disease. Nat Rev Microbiol 2023. [Google Scholar] [CrossRef]
- Lee, YJ; Kim, MJ; Hong, JY; et al. Diagnostic accuracy of Clostridioides difficile tests: a systematic review and meta-analysis. J Korean Med Sci. 2020, 35(41), e338. [Google Scholar] [CrossRef]
- Crobach, MJT; Planche, T; Eckert, C; et al. European Society of Clinical Microbiology and Infectious Diseases: update of the diagnostic guidance document for Clostridioides difficile infection. Clin Microbiol Infect. 2020, 26(12), 1620–1629. [Google Scholar] [CrossRef]
- Guh, AY; Kutty, PK. Updates on Clostridioides difficile infection epidemiology and diagnostic strategies. Clin Infect Dis. 2023, 77(3), e194–e202. [Google Scholar]
- Polage, CR; Sharpe, BA; Strymish, J; et al. Evaluation of diagnostic stewardship interventions to reduce inappropriate Clostridioides difficile testing. Infect Control Hosp Epidemiol. 2024, 45(5), 555–562. [Google Scholar]
- Zhang, Y; Li, H; Sun, X; et al. Comparison of GDH, toxin EIAs, and multiplex qPCR assays for Clostridioides difficile infection. Front Cell Infect Microbiol. 2024, 14, 1492511. [Google Scholar]
- Martins, AF; Pereira, JB; da Silva Filho, HP; et al. Performance of a two-step algorithm versus qPCR for diagnosis of Clostridioides difficile infection in Brazil. Anaerobe. 2023, 80, 102676. [Google Scholar]
- Sholeh, M; Forouzanfar, F; Safari, M; et al. Emerging diagnostics for Clostridioides difficile: LAMP, MALDI-TOF, and novel immunoassays. Int J Mol Sci. 2024, 25(16), 8672. [Google Scholar]
- O’Neill, JP; et al. Comparative effectiveness of fidaxomicin vs vancomycin in treating Clostridioides difficile infection. Open Forum Infect Dis. 2024, 11(1), ofad622. [Google Scholar]
- Patimavirujh, N; et al. MAD-ID 2025 highlights fidaxomicin's role in reducing C. difficile recurrence. Contagion Live 2025. [Google Scholar]
- Infectious Diseases Society of America; Society for Healthcare Epidemiology of America. Clinical practice guidelines for the management of Clostridioides difficile infection in adults. IDSA/SHEA, 2021. [Google Scholar]
- Liu, Y; et al. Efficacy of fecal microbiota transplantation versus standard antibiotic therapy in recurrent Clostridioides difficile infection: a systematic review and meta-analysis. Cureus 2025, 17(8), e387304. [Google Scholar]
- Sullivan, A; et al. Clinical management of Clostridioides difficile infection with fecal microbiota transplantation. Lancet EClinicalMedicine 2025, 23, 100234. [Google Scholar]
- Penn Medicine. Penn Medicine and CHOP develop novel mRNA vaccine to prevent and treat C. difficile; University of Pennsylvania: Philadelphia (PA), 18 Oct 2024. [Google Scholar]
- Johnson, S; Lavergne, V; Skinner, AM; et al. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clin Infect Dis. 2021, 73(5), e1029–e1044. [Google Scholar] [CrossRef] [PubMed]
- Alsoubani, M; Chow, JK; Rodday, AM; Kent, D; Snydman, DR. Comparative Effectiveness of Fidaxomicin vs Vancomycin in Populations With Immunocompromising Conditions for the Treatment of Clostridioides difficile Infection: A Single-Center Study. Open Forum Infect Dis. 2023, 11(1), ofad622. [Google Scholar] [CrossRef]
- Jiang, Y; Sarpong, EM; Sears, P; Obi, EN. Budget Impact Analysis of Fidaxomicin Versus Vancomycin for the Treatment of Clostridioides difficile Infection in the United States. Infect Dis Ther. 2022, 11(1), 111–126. [Google Scholar] [CrossRef] [PubMed]
- Okafor, CM; Clogher, P; Olson, D; et al. Trends in and Risk Factors for Recurrent Clostridioides difficile Infection, New Haven County, Connecticut, USA, 2015–2020. Emerg Infect Dis. 2023, 29(5), 877–887. [Google Scholar] [CrossRef]
- Greentree, DH; Rice, LB; Donskey, CJ. Houston, We Have a Problem: Reports of Clostridioides difficile Isolates With Reduced Vancomycin Susceptibility. Clin Infect Dis. 2022, 75(9), 1661–1664. [Google Scholar] [CrossRef]
- Van Prehn, J; Reigadas, E; Vogelzang, EH; Bouza, E; Hristea, A; Guery, B; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin Microbiol Infect. 2021, 27 Suppl 2, S1–21. [Google Scholar] [CrossRef]
- Khanna, S; Baddour, LM; Huskins, WC; Kammer, PP; Patel, R; Pardi, DS. Clostridioides difficile infection: Emerging practices in prevention and treatment of recurrence. J Travel Gastroenterol. 2024, 16(2), 101–15. [Google Scholar]
- De Bruyne, C; Vadlamudi, N; Malafa, S; Gill, CJ. Safety, immunogenicity, and efficacy of a Clostridioides difficile toxoid vaccine candidate in adults at risk of CDI: A phase 3 randomized controlled trial. Lancet Infect Dis. 2021, 21(7), 922–31. [Google Scholar]
- Kelly, CR; Fischer, M; Allegretti, JR; LaPlante, K; Stewart, DB; Limketkai, BN; et al. ACG Clinical Guidelines: Prevention, diagnosis, and treatment of Clostridioides difficile infections. Am J Gastroenterol. 2021, 116(6), 1124–47. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, MA; Khanna, S; Pardi, DS; Shah, ND; Baddour, LM. Bezlotoxumab for prevention of Clostridioides difficile recurrence in solid organ and hematopoietic stem cell transplant recipients. Clin Infect Dis. 2021, 72(11), 1998–2004. [Google Scholar]
- Johnson, S; Gerding, DN. Bezlotoxumab for prevention of recurrent Clostridioides difficile infection: A review of current evidence and future needs. Ther Adv Gastroenterol. 2022, 15, 17562848221129041. [Google Scholar]
- Guh, AY; Guerrero, DM; Karlsson, M; Patel, R; Khanna, S; Pardi, DS; et al. Bezlotoxumab for prevention of recurrent Clostridioides difficile infection: A Mayo Clinic multicenter real-world cohort and meta-analysis. Clin Infect Dis. 2024, 79(1), 89–97. [Google Scholar]
- Allegretti, JR; Mullish, BH; Kelly, C; Fischer, M. The evolution of the use of faecal microbiota transplantation and emerging therapeutic indications. Lancet. 2019, 394(10196), 420–431. [Google Scholar] [CrossRef]
- Khanna, S; Assi, M; Lee, C; et al. Efficacy and safety of RBX2660 in recurrent Clostridioides difficile infection: results from the phase 3 PUNCH CD3 trial. Clin Infect Dis. 2022, 75(5), e1100–e1107. [Google Scholar]
- Dubberke, ER; Mullane, KM; Gerding, DN; et al. Long-term follow-up of RBX2660 for prevention of recurrent Clostridioides difficile infection. Open Forum Infect Dis. 2023, 10(3), ofad086. [Google Scholar]
- Feuerstadt, P; Louie, TJ; Lashner, B; et al. SER-109, an oral microbiome therapy for recurrent Clostridioides difficile infection. N Engl J Med. 2022, 386(3), 220–229. [Google Scholar] [CrossRef]
- Khanna, S; Pardi, DS; Kelly, CR; et al. A microbiota-based drug prevents recurrent Clostridioides difficile infection: results from a randomized, placebo-controlled phase 2 trial. JAMA. 2022, 328(2), 137–145. [Google Scholar]
- Vedanta Biosciences. A study of VE303 in patients at high risk for recurrent Clostridioides difficile infection (RESTORATiVE303). ClinicalTrials.gov Identifier: NCT04899336. Updated 2024.
- De Bruyn, G; Saleh, J; Workman, D; et al. Defining the futility of Clostridium difficile toxoid vaccine development: lessons from phase 3. N Engl J Med. 2021, 385(20), 1823–1832. [Google Scholar]
- Dorr, U; Levy, M; Pollak, R; et al. Safety and efficacy of a Clostridioides difficile toxoid vaccine: results from the CLOVER phase 3 trial. Clin Infect Dis. 2022, 75(9), 1508–1517. [Google Scholar]
- Kitchin, N; Remich, SA; Peterson, J; et al. Efficacy of a Clostridium difficile toxoid vaccine in older adults: a randomized clinical trial. Lancet Infect Dis. 2020, 20(1), 91–100. [Google Scholar]
- Villano, S; Seiberling, M; Tatarowicz, W; et al. A randomized, double-blind trial of a Clostridioides difficile toxoid vaccine for prevention of primary infection. Vaccine. 2021, 39(30), 4195–4202. [Google Scholar]
- Alameh, MG; Naidu, N; Lin, YR; et al. An mRNA-lipid nanoparticle vaccine targeting Clostridioides difficile induces protective immunity in animal models. Nat Commun. 2023, 14, 3215. [Google Scholar]
- Wang, X; Tan, Y; Zhang, R; et al. Lipid nanoparticle–mRNA vaccines protect against Clostridioides difficile toxins in preclinical models. Front Immunol. 2023, 14, 1123948. [Google Scholar]
- Vickers, RJ; Tillotson, G; Goldstein, EJ; et al. Ridinilazole versus vancomycin for treatment of Clostridioides difficile infection: two randomized controlled phase 3 trials. Lancet Infect Dis. 2023, 23(1), 62–73. [Google Scholar]
- Leeds, JA; Sachdeva, M; Mullane, K; et al. A randomized phase 2 trial of CRS3123, a methionyl-tRNA synthetase inhibitor, in Clostridioides difficile infection. Clin Infect Dis. 2023, 76(6), 1013–1021. [Google Scholar]
- Mullane, KM; Winston, DJ; Gabryelski, L; et al. Safety and efficacy of CRS3123 in recurrent Clostridioides difficile infection: a phase 2 randomized study. Clin Infect Dis. 2024, 78(1), e71–e80. [Google Scholar]
- Miller, MA; Gohil, SK; et al. Cost-Effectiveness Analysis of Antimicrobial Prescribing for Clostridioides difficile Infection in England. PharmacoEconomics Open. 2023, 7(4), 739–750. [Google Scholar]
- Sato, T; Matsushima, M; et al. Cost-effectiveness analysis of fidaxomicin versus vancomycin for Clostridioides difficile infection after metronidazole failure in Japan. J Infect Chemother. 2020, 26(9), 742–750. [Google Scholar]
- Puig-Asensio, M; Navarro, MD; et al. Extended-pulsed fidaxomicin versus vancomycin in older adults: cost-effectiveness analysis in Spain. Eur J Clin Microbiol Infect Dis. 2019, 38(6), 1105–1111. [Google Scholar]
- Chen, J; Gong, CL; Hitchcock, MM; Holubar, M; Deresinski, S; Hay, JW. Cost-effectiveness of bezlotoxumab and fidaxomicin for initial Clostridioides difficile infection. Clin Microbiol Infect. 2021, 27(10), 1448–1454. [Google Scholar] [CrossRef]
- Kassam, Z; Lee, CH; et al. Fecal transplants by colonoscopy and capsules are cost-effective strategies for treating recurrent Clostridioides difficile infection. Clin Infect Dis. 2022, 74(6), 1051–1059. [Google Scholar]
- Barbut, F; Crobach, M; et al. Quality-of-life impact and utility decrement associated with Clostridioides difficile infection. Health Qual Life Outcomes 2019, 17(1), 55. [Google Scholar] [CrossRef] [PubMed]
- Weerakoon, S; Lee, M; Eriksen, MK; et al. Microbiota-based therapies for recurrent Clostridium difficile infection: A systematic review of their efficacy and safety. Cureus 2025, 17(8), e90737. [Google Scholar] [CrossRef] [PubMed]
- Kaltwasser, J; et al. Model finds vancomycin and fidaxomicin most cost-effective CDI treatments—with caveats. In Am J Manag Care; 2023. [Google Scholar]
- Harris, AD; et al. Real-world use of bezlotoxumab to prevent recurrent Clostridioides difficile infection. Clin Infect Dis. 2025, 80(1), 52–59. [Google Scholar]
- Baunwall, SM; Lee, MM; Eriksen, MK; et al. Real-world effectiveness of fecal microbiota transplantation for recurrent Clostridioides difficile infection. Clin Gastroenterol Hepatol. 2024, 22(7), e514–e521. [Google Scholar]
- Cha, RR; Sonu, I. Fecal microbiota transplantation: present and future. Clin Endosc. 2025, 58(1), 1–10. [Google Scholar] [CrossRef]
- Alameh, MG; et al. A multivalent mRNA–lipid nanoparticle vaccine protects against Clostridioides difficile infection. Science 2024, 373(6550), 1234–1239. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



