Submitted:
02 February 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Background: Cytomegalovirus (CMV) enteritis can lead to intractable diarrhea, especially when complicated by severe gut dysbiosis, posing a significant therapeutic challenge.
Methods: We present a case of a 40-year-old woman with a history of traumatic brain injury and prolonged broad-spectrum antibiotic use, who developed persistent bloody, mucus-containing diarrhea (up to 40 episodes daily). Colonoscopy with biopsy confirmed CMV enteritis, and 16S rRNA sequencing revealed severe intestinal dysbiosis. Treatment consisted of intravenous ganciclovir combined with multiple sessions of fecal microbiota transplantation (FMT) delivered via jejunal tube, alongside tailored nutritional support.
Results: Despite initial persistence of symptoms, the combined antiviral and FMT regimen led to resolution of diarrhea, normalization of inflammatory markers, and restoration of enteral tolerance. Follow-up colonoscopy showed mucosal healing and negative CMV staining. Microbiota analysis demonstrated restoration of diversity and a shift toward donor-like taxonomic profiles.
Conclusions: This case highlights CMV as an emerging cause of severe enteritis in non-immunosuppressed surgical patients and supports the efficacy of combined antiviral therapy and FMT for refractory diarrhea associated with dysbiosis and CMV infection.
Keywords:
cytomegalovirus enteritis
; fecal microbiota transplantation
; dysbiosis
; multidrug-resistant organisms
; traumatic brain injury
1. Introduction
The introduction
Patients after brain trauma surgery often receive prolonged broad-spectrum antibiotics and remain in a postsurgical stress state, predisposing them to multidrug-resistant infections and intestinal dysbiosis. This cascade can lead to antibiotic-associated diarrhea and may progress to opportunistic enteritis. While cytomegalovirus (CMV) enteritis typically affects immunosuppressed individuals, growing evidence shows it can also cause severe diarrhea in non-classically immunosuppressed postoperative patients. CMV infection may further synergize with gut microbiota disruption to worsen mucosal barrier injury [1,2]. Conventional anti-infective and immunomodulatory therapies often yield poor outcomes in complex enteritis, especially when multidrug-resistant organism (MDRO) colonization is present. Although fecal microbiota transplantation (FMT) is effective for recurrent Clostridioides difficile infection (CDI) [3], its role in concurrent CMV enteritis and gut microbiota dysbiosis remains unclear. This case describes a patient who developed refractory diarrhea after brain trauma surgery and prolonged broad-spectrum antibiotic use, diagnosed with CMV enteritis and gut microbiota dysbiosis. Sequential antiviral therapy and multiple FMT sessions restored the intestinal mucosal barrier and reestablished microbial balance. The case confirms that CMV can trigger enteritis in non-classically immunosuppressed patients and demonstrates a successful treatment strategy for postoperative complex infectious diarrhea. It highlights the essential role of gut microecological regulation amid rising antimicrobial resistance.
2. Case Presentation
A 40-year-old woman (150 cm, 45 kg) was admitted on July 24, 2025, with 17 days of intermittent diarrhea and fever, worsening over the prior 5 days with bloody, mucus-containing stools. She had been hospitalized since July 6 for recovery from traumatic brain injury when she developed diarrhea (3–4 times daily, yellow watery stools), low-grade fever (up to 38℃), and vomiting. On July 18, diarrhea increased to up to 40 times daily (about 50 mL each), accompanied by bloody stools, paroxysmal lower abdominal pain, nausea, vomiting (gastric contents and white foam), and palpitations; no chills or persistent fever occurred. Local hospital treatment with liver protection, anti-infectives, and mesalazine failed. She was transferred on July 22 due to clinical deterioration. Clostridium difficile toxin gene test was negative. Blood tests showed WBC 14.85×10⁹/L, neutrophils 10.43×10⁹/L. Stool analysis revealed red blood cells, elevated white blood cells (3+/HP), and phagocytes (2+/HP), no fungi or parasites—indicative of intestinal inflammation. Diagnosed with intestinal infection, diarrhea, malnutrition, and post-brain trauma status, she was admitted to intensive care unit (ICU). Since onset, she had poor mental status, appetite, and sleep; reduced strength; weight loss of 15 kg; urine output remained normal.
Four months earlier, she developed impaired consciousness and speech disturbances after traumatic brain injury, with irrelevant responses. On March 25, 2025, she underwent intracranial hematoma evacuation, decompressive craniectomy, and intracranial pressure monitor placement. A tracheotomy was performed on March 27 for pulmonary infection. On April 30, a left ventriculoperitoneal shunt was placed for hydrocephalus. On May 16, CSF culture identified Gram-positive cocci, confirming intracranial infection; the shunt was removed and vancomycin (44-day course) and meropenem (39-day course) were initiated.
At admission, she was alert but had deficits in calculation, orientation, and cognition, with occasional irrelevant responses. She appeared underweight and was uncooperative. Nasal oxygen was given at 3 L/min; temperature 36.6℃. Vital signs: HR 95 bpm, RR 15 breaths/min, BP 120/87 mmHg, SpO₂ 100%. No jaundice or lymphadenopathy. A well-healed arc-shaped scar was present in the right frontal-temporal region with bone window depression. Pupils were equal, round, about 2 mm, light-reactive. Neck was supple. Breath sounds were coarse bilaterally, without rales. Cardiac rhythm was regular, no murmurs. Abdomen was flat, soft, non-tender; no edema. Neurological exam: muscle strength grade Ⅳ in right upper limb and left lower limb, approximately grade Ⅱ in left upper limb. Bilateral pathological reflexes were absent.
After admission, stool analysis showed abundant white blood cells (++++). Tests for C. difficile toxin gene, Salmonella, and Shigella were negative. Autoimmune serology (ENA, ANCA 4-panel + GBM) was negative; serum IgE normal. Coxsackievirus B3/B5 IgM, enterovirus RNA, and CMV IgM were negative. Plasma EBV-DNA undetectable; CMV-DNA <4×10² copies/mL. On D6 (July 29), abdominal CT showed mild bowel wall thickening, edema, and irregularity in the colon and distal small intestine, with intraluminal fluid and no obstruction. Colonoscopy on D7 (July 30) revealed hyperemic, edematous terminal ileal mucosa with adherent white exudate; diffuse inflammation from ileocecal junction to rectum with hyperemia, edema, nodular elevations, and dirty coating (Figure 1a). Rectal biopsy showed ulceration with granulation tissue and chronic inflammation, no granulomas. Immunohistochemistry showed focal CMV-positive cells; CD3 (focally positive), CD20 (–), CD56 (–); EBER (–), CMV (sparsely positive); PAS (unremarkable), acid-fast stain (–) (Figure 1b). Diagnosis: CMV-associated infectious colitis. Analysis of intestinal microbiota alterations by 16S ribosomal RNA (rRNA) gene sequencing revealed severe dysbiosis in the patient (Figure 2).
FMT (Meiyitian Biomedical (Wuhan) Co., Ltd.) started on D2 (July 25) via jejunal tube at 50 mL/day, but diarrhea persisted. Intravenous ganciclovir 0.25 g q12h was started on D7. FMT continued daily until D10 (August 2). On D6, commercial enteral formula triggered fever and abdominal pain; it was stopped. She was switched to minimal oral intake (<100 mL/day white rice porridge) with full parenteral nutrition. By D11 (August 3), stool leukocytosis resolved. A customized enteral nutrition plan was initiated via nasogastric tube, with rate and volume adjusted per tolerance scoring.
On D15 (August 7), she developed high fever (39.4℃). Repeat chest CT showed new pulmonary infiltrates, indicating acute lung infection. Empirical therapy: ganciclovir 0.25 g intravenous (i.v.) q12h, cefoperazone-sulbactam 3.0 g i.v. q12h, ornidazole 0.5 g i.v. q12h. On D17 (August 9), sputum culture grew Enterobacter cloacae and Staphylococcus aureus; urine culture grew Escherichia coli. Linezolid 0.6 g i.v. q12h was added. Fever resolved and C-reactive protein (CRP) declined steadily. On D19 (August 11), repeat colonoscopy showed hyperemic terminal ileal mucosa with small round ulcers (3–4 mm, clean bases); ileocecal region largely intact. Ascending colon to rectum showed diffuse congestion, edema, viscous secretions. Scattered superficial ulcers (2–4 mm) in ascending colon; mucosa friable (Figure 1c). Histopathology: (1) Terminal ileum–villous atrophy, mixed lamina propria inflammation, focal cryptitis, apoptotic bodies, localized ulceration; no granulomas or CMV inclusion bodies; CMV IHC and EBER ISH negative; (2) Ileocecal and rectal biopsies–preserved crypt architecture with occasional distortion; focal chronic inflammation, rare apoptotic bodies; (3) Ascending and descending colon–crypt atrophy, reduced goblet cells, diffuse inflammation, small granulation foci. Findings consistent with infectious enterocolitis (Figure 1d). On D20 (August 12), metagenomic next-generation sequencing (mNGS) of intestinal tissue detected 14 reads of CMV and 36 reads of Candida parapsilosis. Antimicrobial regimen was adjusted: cefoperazone-sulbactam and ornidazole discontinued; ganciclovir 0.25 g i.v. q12h, linezolid 0.6 g i.v. q12h, and caspofungin 0.5 g daily continued.
The patient remained afebrile. On D21 (August 13), inflammatory markers showed CRP 2.98 mg/L, WBC 7.54×10⁹/L, and neutrophil percentage 62.8%, indicating effective infection control. Given clinical stability, linezolid was discontinued; intravenous ganciclovir 0.25 g every 12 hours and caspofungin 0.05 g daily were continued for ongoing antiviral and antifungal therapy. From D22 (August 14) to D27 (August 19), FMT was administered daily via jejunal tube with 25 mL of microbial preparation. Stool output gradually decreased and consistency improved; on D25 (August 17), daily volume was 780 mL, yellow and loose with small amounts of semi-solid material. Enteral nutrition was well tolerated, and feeding volume was progressively increased. By D28 (August 20), total enteral intake reached 900 kcal/day.
Repeated FMT significantly reduced severe microbial dysbiosis, as reflected by improvements in both α-diversity and β-diversity metrics (Figure 2a,b). At the phylum level, multiple FMT treatments induced a shift in the relative abundances of key bacterial taxa—specifically Firmicutes, Proteobacteria, and Bacteroidota—toward donor-like configurations. At the genus level, the compositional profiles of several clinically relevant genera, including Enterococcus, Bacteroides, Escherichia-Shigella, Enterobacter, Blautia, Lactobacillus, and Parasutterella, were progressively restored (Figure 2c,d).
On D29 (August 21), the patient was transferred to a rehabilitation facility (Figure 3a). After systematic treatment and close monitoring, symptoms markedly improved, stool frequency declined, and enteral tolerance increased, leading to sustained stability and transition into recovery (Figure 3b). At follow-up on October 20, she had fully resumed oral intake, with 1–2 yellow, pasty bowel movements daily and no gastrointestinal symptoms such as diarrhea or abdominal pain.
3. Discussion
CMV enteritis is typically an opportunistic infection in immunocompromised individuals, including those with HIV/AIDS, cancer, organ transplants, or on immunosuppressive therapy [4,5,6,7,8,9]. However, rare cases occur in immunocompetent hosts, where CMV can cause severe, refractory diarrhea [10,11,12]. Diagnosis is confirmed by histopathology showing viral inclusion bodies or positive CMV staining [13]. In immunosuppressed states, CMV may reactivate locally in the gut without systemic viremia [14]. In this case, postoperative CMV infection likely resulted from physiological stress following traumatic brain injury [2].
Dysbiosis played a central role. It involves gut microbiota imbalance—reduced diversity, loss of butyrate-producing bacteria, pathogen overgrowth, and impaired short-chain fatty acid (SCFA) production—driven by broad-spectrum antibiotics and poor diet [15]. Antibiotics reduce microbial richness, alter composition, and disrupt metabolic profiles [16], promoting dysbiosis and damaging the intestinal barrier via weakened mucus and tight junctions [1]. Dysbiosis is a hallmark of recurrent CDI, IBS, and IBD, contributing to barrier dysfunction and metabolic disturbances. FMT restores microbial balance, SCFA production, and gut barrier integrity; modulates serotonin pathways; and inhibits pathogenic biofilms [17]. After FMT, the patient showed increased beneficial taxa (e.g., Firmicutes, Bacteroidota, Lactobacillus, Blautia, Parasutterella) and reduced pathogens (e.g., Escherichia-Shigella, Enterococcus)—a key mechanism in treating antibiotic-associated diarrhea (AAD). FMT alleviates bloating, pain, and diarrhea, supporting recovery by reshaping the gut environment [18]. Kusakabe et al. reported resolution of Crohn’s-like lesions and CMV enteritis after one FMT in a transplant patient unresponsive to standard therapy, linking mucosal healing to restored microbial diversity following Enterococcus overgrowth [19].
Reported clearance rates of MDRO colonization after FMT range from 37.5% to 87.5%, highlighting its potential in combating antimicrobial resistance by inhibiting resistance gene transfer, restoring barrier function, and suppressing pathogen engraftment [20]. Antibiotic use reduces microbial diversity and alters taxonomic abundance, fostering MDRO emergence [21,22]. Crum-Cianflone et al. documented successful eradication of multiple MDROs with FMT in a recurrent CDI patient [23].
In adults with recurrent CDI and intact immunity, FMT achieves significantly higher cure rates than antibiotics, reaching 95.56% [3,24]. FMT is now a core therapy for dysbiosis-related conditions through microbiota modulation [25]. Rescue FMT is a vital salvage option for critically ill ICU patients with AAD or CDI who fail conventional treatment, especially when complicated by multidrug-resistant infections [26].
5. Conclusions
This case highlights the dynamic clinical course and impact of timely diagnosis and intervention. Initial symptoms mimicked bacterial infection, but CMV enteritis was ultimately diagnosed, emphasizing the need for early recognition in complex diarrheal diseases. Intestinal dysbiosis significantly contributes to severe diarrhea [27]. A combined strategy of prompt antiviral therapy and restoration of microbial homeostasis may offer a more effective, comprehensive treatment approach.
Author Contributions
Conceptualization, X.Z., Z.L., H.L., and J.Z.; methodology, J.Z.; software, X.Z. and J.Z.; validation, H.L., and J.Z.; formal analysis, X.Z. and J.Z.; writing—original draft preparation, X.Z.; writing—review and editing, J.Z.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CMV | Cytomegalovirus |
| FMT | Fecal Microbiota Transplantation |
| MDRO | Multidrug-Resistant Organism |
| ICU | Intensive Care Unit |
| SCFA | Short-Chain Fatty Acid |
| CRP | C-Reactive Protein |
| rRNA | Ribosomal RNA |
| WBC | White Blood Cell |
| AAD | Antibiotic-Associated Diarrhea |
References
- Duan, H.; Yu, L.; Tian, F.; Zhai, Q.; Fan, L.; Chen, W. Antibiotic-induced gut dysbiosis and barrier disruption and the potential protective strategies. Crit. Rev. Food. Sci. Nutr. 2022, 62, 1427–1452. [Google Scholar] [CrossRef]
- Tsai, Y.Y.; Lu, J.W.; Wang, C.C. Cytomegalovirus ileitis in a patient with post-severe trauma: A case report. In. Vivo 2024, 38, 2562–2564. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Luo, X.; Tian, L.; Yue, P.; Li, M.; Liu, K.; Zhu, D.; Huang, C.; Shi, Q.; Yang, L.; et al. The gut microbiome dysbiosis and regulation by fecal microbiota transplantation: Umbrella review. Front. Microbiol. 2023, 14, 1286429. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.K.; Kreiner, L.A.; Walker, P.A.; Klein, K.L.; Bajwa, K.S.; Robinson, E.K.; Millas, S.G.; Souchon, E.A.; Wray, C.J. Cytomegalovirus enteritis manifesting as recurrent bowel obstruction and jejunal perforation in patient with acquired immunodeficiency syndrome: Rare report of survival and review of the literature. Surg. Infect. 2012, 13, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Ebi, M.; Inoue, S.; Sugiyama, T.; Yamamoto, K.; Adachi, K.; Yoshimine, T.; Yamaguchi, Y.; Tamura, Y.; Izawa, S.; Hijikata, Y.; et al. A small bowel ulcer due to clopidogrel with cytomegalovirus enteritis diagnosed by capsule and Double-Balloon endoscopy. Case Rep. Gastroenterol. 2018, 12, 303–310. [Google Scholar] [CrossRef]
- Echenique, I.A.; Penugonda, S.; Stosor, V.; Ison, M.G.; Angarone, M.P. Diagnostic yields in solid organ transplant recipients admitted with diarrhea. Clin. Infect. Dis. 2015, 60, 729–737. [Google Scholar] [CrossRef]
- John, S.G.; Dominguez, C.; Chandiramani, V.; Vemulappalli, T. A rare case intractable diarrhea secondary to Clostridium difficile and cytomegalovirus coinfection. Am. J. Case Rep. 2013, 14, 498–501. [Google Scholar] [CrossRef]
- Bang, S.; Park, Y.B.; Kang, B.S.; Park, M.C.; Hwang, M.H.; Kim, H.K.; Lee, S.K. CMV enteritis causing ileal perforation in underlying lupus enteritis. Clin. Rheumatol. 2004, 23, 69–72. [Google Scholar] [CrossRef]
- Choo, H.; Cher, W.Q.; Kwan, Y.H.; Fong, W. Risk factors for cytomegalovirus disease in systemic lupus erythematosus (SLE): A systematic review. Adv. Rheumatol. 2019, 59, 12. [Google Scholar] [CrossRef]
- Lee, S.W.; Ko, C.W.; Liao, S.C.; Chang, C.S.; Yeh, H.Z.; Chang, C.S. A case with vitamin d Deficiency-Induced cytomegalovirus enteritis presenting as bowel Pseudo-Obstruction. Gasteroenterol. Res. 2017, 10, 193–195. [Google Scholar] [CrossRef]
- Ramos, B.E.; Molina, A.M.; Sarria, O.J.; Larrauri, M.J.; Prieto, B.G. Cytomegalovirus infection causing protracted diarrhea in an immunocompetent child. An. Pediatr. 2009, 70, 582–585. [Google Scholar]
- Telakis, E.; Tsironi, E.; Papatheodorou, K.; Nikolakis, D. Debilitating chronic diarrhea caused by generalized gastrointestinal cytomegalovirus infection in an immunocompetent adult. Case Rep. Gastrointest. Med. 2014, 2014, 260120. [Google Scholar] [CrossRef]
- Kalkan, I.H.; Dagli, U. What is the most accurate method for the diagnosis of cytomegalovirus (CMV) enteritis or colitis? Turk. J. Gastroenterol. 2010, 21, 83–86. [Google Scholar]
- Ninomiya, I.; Nakashima, H.; Gondo, H.; Eto, T.; Seo, M.; Saijyo, K.; Matsuura, T.; Nagafuji, K.; Yao, T.; Harada, M. Local cytomegalovirus infection in patients with diarrhea following allogeneic stem cell transplantation. Fukuoka Igaku Zasshi 2007, 98, 114–123. [Google Scholar] [PubMed]
- Carias, D.A.; de Jesus, R.S.D.; Stefanolo, J.P.; Cruz, S.M.; Casas, I.C.; Zuluaga, P.J. Intestinal dysbiosis: Exploring definition, associated symptoms, and perspectives for a comprehensive understanding - a scoping review. Probiotics Antimicrob. Proteins 2025, 17, 440–449. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Shi, J.; Liu, A.; Xu, Y.J.; Liu, Y. Antibiotic-induced gut microbiota dysbiosis altered host metabolism. Mol. Omics 2023, 19, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Yu, J.; Li, Y.; Zhao, D.; Zhang, Z. Advances in fecal microbiota transplantation for gut Dysbiosis-Related diseases. Adv. Sci. 2025, 12, e2413197. [Google Scholar] [CrossRef]
- Wang, L.; Guo, G.; Xu, Y.; Li, L.; Yang, B.; Zhao, D.; Tian, H.; Ye, C.; Lin, Z.; Cui, J.; et al. The effect of fecal microbiota transplantation on antibiotic-associated diarrhea and its impact on gut microbiota. BMC Microbiol. 2024, 24, 160. [Google Scholar] [CrossRef]
- Kusakabe, S.; Kurashige, R.; Fukushima, K.; Shimizu, K.; Yoshihara, T.; Motooka, D.; Nakamura, S.; Kurashige, M.; Nakata, K.; Hino, A.; et al. Fecal microbiota transplantation for Crohn’s disease-like intestinal lesions arising after allogeneic stem cell transplantation. Int. J. Hematol. 2025. [Google Scholar] [CrossRef]
- Saha, S.; Tariq, R.; Tosh, P.K.; Pardi, D.S.; Khanna, S. Faecal microbiota transplantation for eradicating carriage of multidrug-resistant organisms: A systematic review. Clin. Microbiol. Infect. 2019, 25, 958–963. [Google Scholar] [CrossRef]
- Dethlefsen, L.; Huse, S.; Sogin, M.L.; Relman, D.A. The pervasive effects of an antibiotic on the human gut microbiota, as revealed by deep 16S rRNA sequencing. PLoS Biol. 2008, 6, e280. [Google Scholar] [CrossRef] [PubMed]
- Dethlefsen, L.; Relman, D.A. Incomplete recovery and individualized responses of the human distal gut microbiota to repeated antibiotic perturbation. Proc. Natl. Acad. Sci. U. S. A 2011, 108 Suppl 1, 4554–4561. [Google Scholar] [CrossRef]
- Crum-Cianflone, N.F.; Sullivan, E.; Ballon-Landa, G. Fecal microbiota transplantation and successful resolution of multidrug-resistant-organism colonization. J. Clin. Microbiol. 2015, 53, 1986–1989. [Google Scholar] [CrossRef]
- Minkoff, N.Z.; Aslam, S.; Medina, M.; Tanner-Smith, E.E.; Zackular, J.P.; Acra, S.; Nicholson, M.R.; Imdad, A. Fecal microbiota transplantation for the treatment of recurrent Clostridioides difficile (Clostridium difficile). Cochrane Database Syst Rev. 2023, 4, D13871. [Google Scholar]
- Wang, Y.; Zhang, S.; Borody, T.J.; Zhang, F. Encyclopedia of fecal microbiota transplantation: A review of effectiveness in the treatment of 85 diseases. Chin. Med. J. (Engl). 2022, 135, 1927–1939. [Google Scholar] [CrossRef]
- Dai, M.; Liu, Y.; Chen, W.; Buch, H.; Shan, Y.; Chang, L.; Bai, Y.; Shen, C.; Zhang, X.; Huo, Y.; et al. Rescue fecal microbiota transplantation for antibiotic-associated diarrhea in critically ill patients. Crit. Care 2019, 23, 324. [Google Scholar] [CrossRef]
- Li, Y.; Xia, S.; Jiang, X.; Feng, C.; Gong, S.; Ma, J.; Fang, Z.; Yin, J.; Yin, Y. Gut microbiota and diarrhea: An updated review. Front. Cell. Infect. Microbiol. 2021, 11, 625210. [Google Scholar] [CrossRef]
Figure 1.
(A) Endoscopic examination reveals hyperemia and edema of the terminal ileal mucosa, accompanied by white exudates. Diffuse mucosal inflammation characterized by nodular elevations and fibrinopurulent exudates extends from the ileocecal junction through the ascending, transverse, descending, and sigmoid colon to the rectum. (B) Immunohistochemical staining demonstrates focal and scattered cytomegalovirus (CMV)-positive cells, with in situ hybridization showing sporadic CMV positivity. (C) Follow-up endoscopy shows residual hyperemia in the terminal ileum along with a few small, round ulcers (3–4 mm) without exudate. The colonic mucosa from the ascending colon to the rectum displays persistent hyperemia and edema, with abundant viscous secretions. Scattered shallow ulcers (2–4 mm) are observed in the ascending colon, and the mucosa is diffusely friable. (D) Immunohistochemical analysis indicates no detectable CMV expression, and in situ hybridization for Epstein-Barr virus-encoded RNA (EBER) is negative.
Figure 1.
(A) Endoscopic examination reveals hyperemia and edema of the terminal ileal mucosa, accompanied by white exudates. Diffuse mucosal inflammation characterized by nodular elevations and fibrinopurulent exudates extends from the ileocecal junction through the ascending, transverse, descending, and sigmoid colon to the rectum. (B) Immunohistochemical staining demonstrates focal and scattered cytomegalovirus (CMV)-positive cells, with in situ hybridization showing sporadic CMV positivity. (C) Follow-up endoscopy shows residual hyperemia in the terminal ileum along with a few small, round ulcers (3–4 mm) without exudate. The colonic mucosa from the ascending colon to the rectum displays persistent hyperemia and edema, with abundant viscous secretions. Scattered shallow ulcers (2–4 mm) are observed in the ascending colon, and the mucosa is diffusely friable. (D) Immunohistochemical analysis indicates no detectable CMV expression, and in situ hybridization for Epstein-Barr virus-encoded RNA (EBER) is negative.
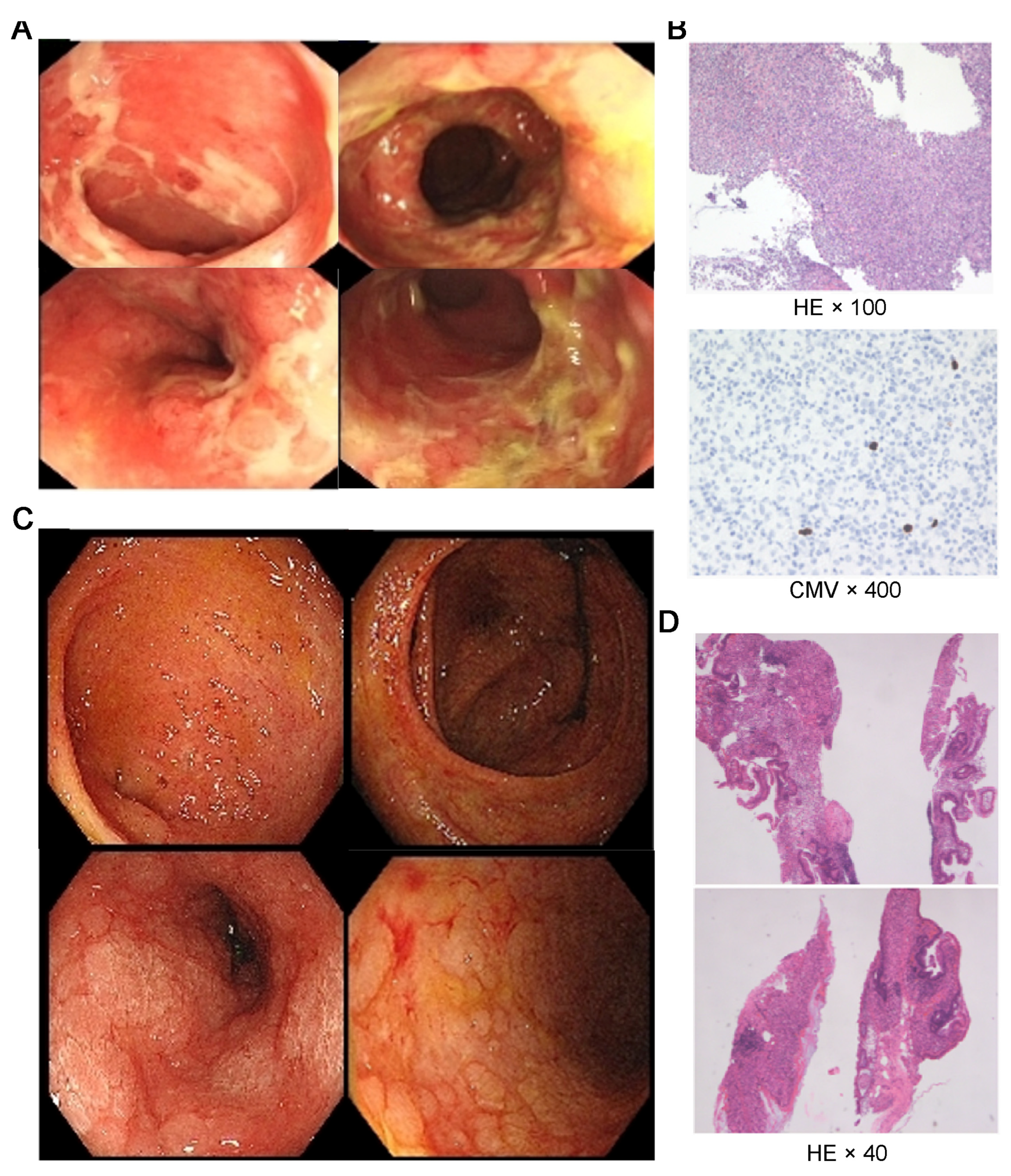
Figure 2.
(A) Alpha-diversity of the gut microbiome, assessed using Faith’s Phylogenetic Diversity, observed ASVs, Shannon index, and Simpson index. (B) Weighted principal coordinates analysis (PCoA). Stacked bar charts illustrating the taxonomic composition of the gut microbiota at the levels of phylum (C) and genus (D), with each taxon represented by a distinct color.
Figure 2.
(A) Alpha-diversity of the gut microbiome, assessed using Faith’s Phylogenetic Diversity, observed ASVs, Shannon index, and Simpson index. (B) Weighted principal coordinates analysis (PCoA). Stacked bar charts illustrating the taxonomic composition of the gut microbiota at the levels of phylum (C) and genus (D), with each taxon represented by a distinct color.
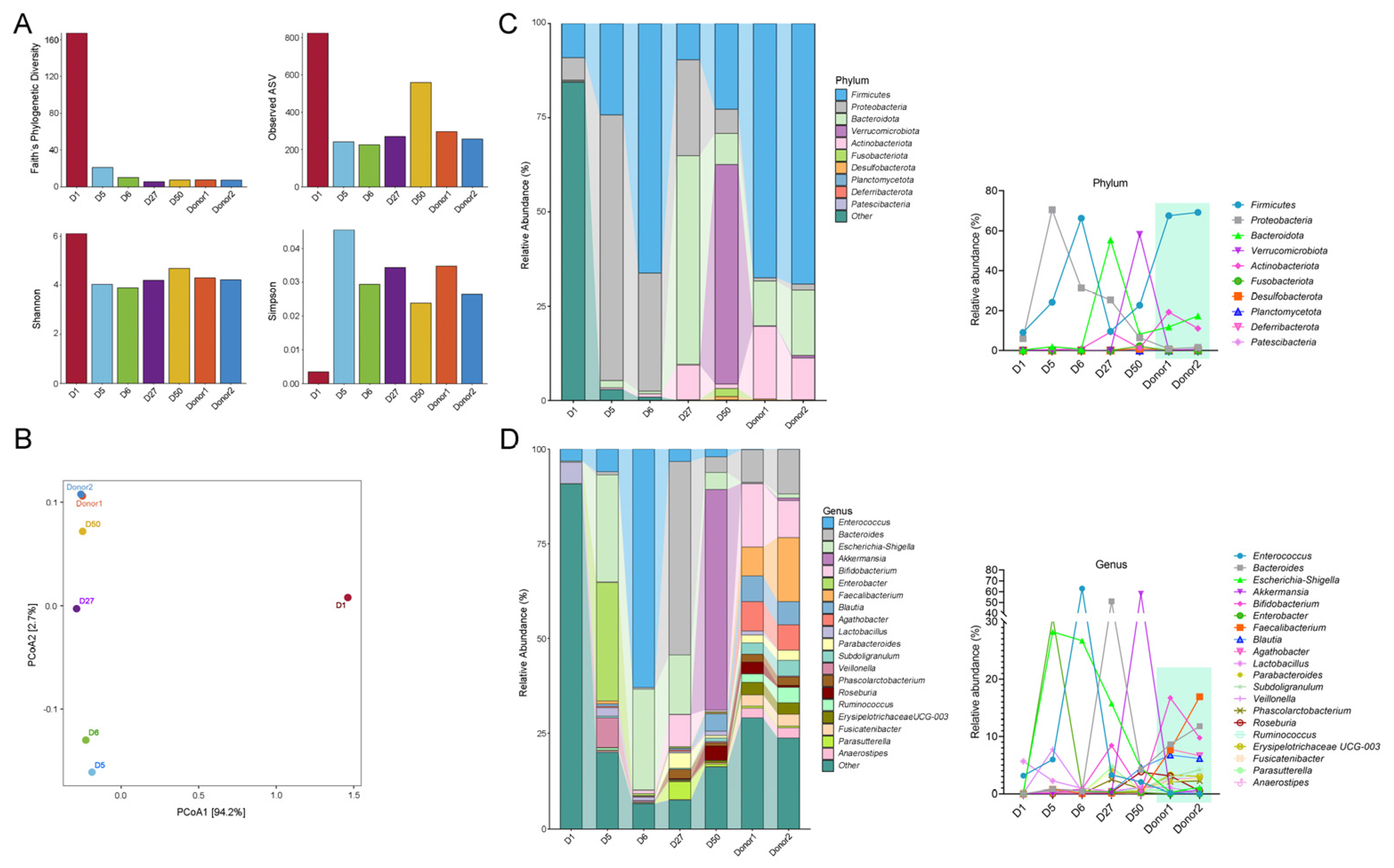
Figure 3.
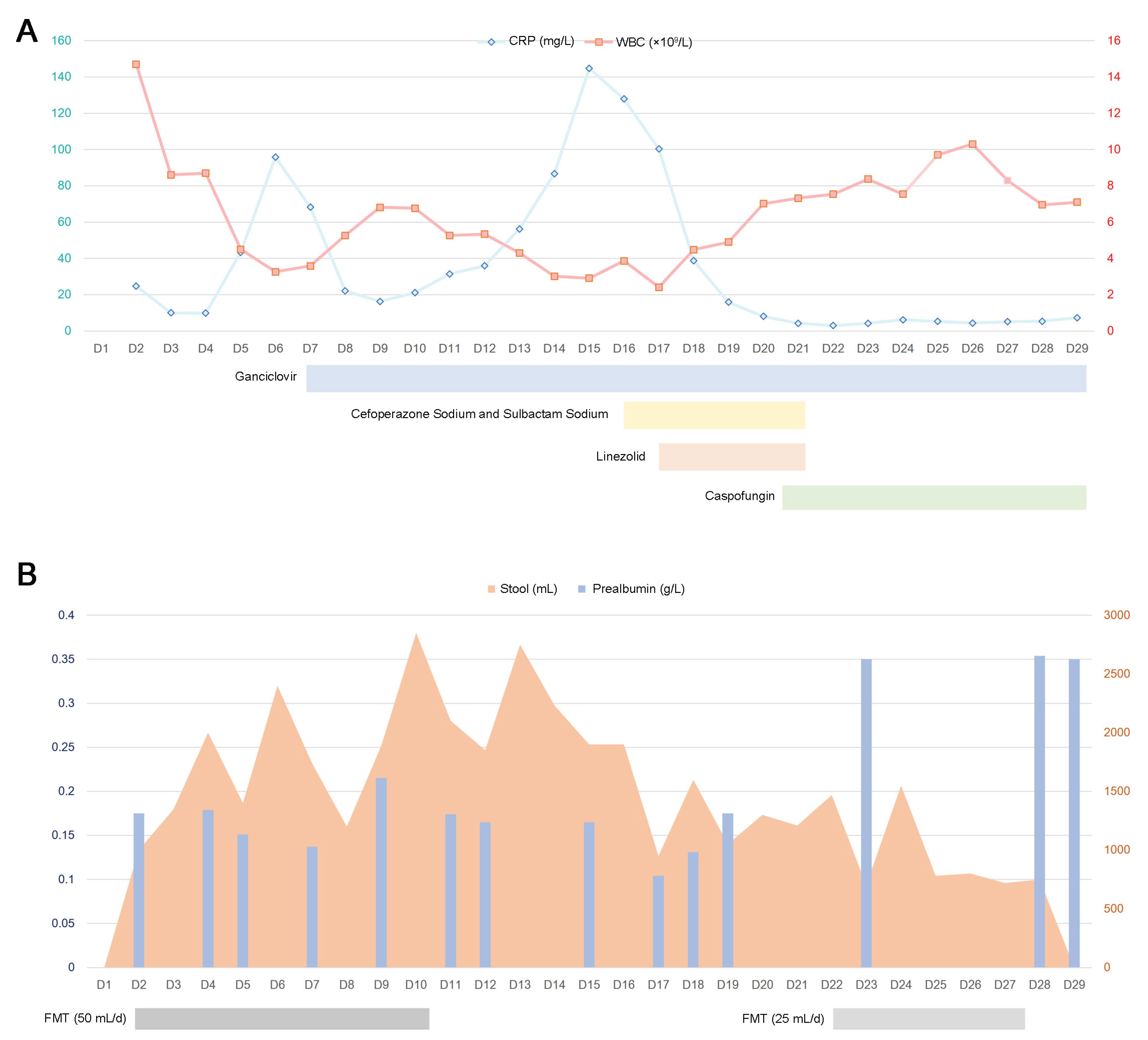
(A) Temporal trends in inflammatory markers, including C-reactive protein (CRP) and white blood cell (WBC) count, along with concomitant antibiotic administration. (B) Clinical course depicting the fecal microbiota transplantation (FMT) regimen, daily stool volume, and serial prealbumin levels over time.
Figure 3.
(A) Temporal trends in inflammatory markers, including C-reactive protein (CRP) and white blood cell (WBC) count, along with concomitant antibiotic administration. (B) Clinical course depicting the fecal microbiota transplantation (FMT) regimen, daily stool volume, and serial prealbumin levels over time.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



