
Submitted:
27 August 2025
Posted:
28 August 2025
You are already at the latest version
Abstract
Background: Although Enterococcus domination has been extensively evaluated in the context of allogeneic hematopoietic stem cell transplantation (allo-HSCT), the prevalence and clinical implications of other dominant genera remain poorly understood. Objective: In this study, we sought to determine the dynamics, predictors and clinical implications of intestinal domination in Brazilian patients undergoing allo-HSCT. Methods: In a prospective study of four Brazilian centers, fecal specimens were collected longitudinally from prior to allo-HSCT to six months after. To identify intestinal domination, we performed 16S rRNA gene sequencing using Illumina platform. We then evaluated the impact of intestinal domination on overall survival and acute graft versus host disease (aGvHD) incidence. Finally, to identify predictors of intestinal domination, we performed a logistic regression model. Results: A total of 192 fecal specimens were collected from 69 patients. Among these specimens, 131 (68%) had intestinal domination. The top four dominant genera were Bacteroides, Akkermansia, Phascolarctobacterium, and Escherichia-Shigella. No significant association was identified between intestinal domination by these genera and overall survival and aGvHD incidence. Additionally, we identified that no patient-level characteristic reliably predicts intestinal domination. Conclusion: Our findings suggest that the prognostic significance of intestinal domination may vary according to the dominant genera and to the population being evaluated.
Keywords:
gastrointestinal microbiome
; stem cell transplantation
; prognosis
; intestinal domination
; Enterococcus
1. Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a curative therapy for several malignant and non-malignant diseases [1,2,3,4,5,6]. Despite allo-HSCT potential benefits, life-threatening complications such as neutropenic fever, relapse and acute graft versus host disease (aGvHD) remains major barriers to successful outcomes [1,2,3,4,5,6]. Successful outcomes in allo-HSCT rely on the identification and mitigation of key variables with prognostic significance. Among these prognostic variables that can shape the course of the allo-HSCT, a key player seems to be the intestinal microbiota [7,8,9]. The intestinal microbiota plays a multifaceted role in human physiology, contributing to the preservation of the gut barrier integrity, producing key metabolites to maintain gut homeostasis, and shaping immune responses through complex crosstalk [10]. Through these mechanisms, the intestinal microbiota can shape the development of clinical outcomes over the allo-HSCT. For instance, aGvHD, which is the leading cause of non-relapse mortality, has been linked to specific patterns of intestinal microbiota disruption (“intestinal dysbiosis”) [11,12,13,14,15]. Decreased intestinal diversity (an index that measure intestinal microbiota variety [richness] and balance [evenness]) over the engraftment period has been associated with an approximately eight-fold increase in the risk of aGvHD [12]. Another intestinal dysbiosis feature frequently reported is the decreased abundance of SCFA (short-chain fatty acid)-producing bacteria, which has been associated with infections, transplant-related mortality and overall survival [16,17,18]. These and other studies outline the impact of specific intestinal dysbiosis features over the allo-HSCT.
In patients undergoing allo-HSCT, another key feature of intestinal dysbiosis is the expansion of a single microbiota genus leading to intestinal domination. Intestinal domination is a frequent dysbiosis feature in allo-HSCT, occurring in 28% to 80% of patients [19,20,21,22,23,24]. Although intestinal domination is common, the specific genus driving this event may vary across studies. For example, while Enterococcus was the most common dominant genus in the microbiota of patients from four different centers, Streptococcus and Bacteroides were predominant in other allo-HSCT studies [19,21,24]. Thus, although intestinal domination is consistently present in allo-HSCT studies, distinct domination fingerprints may emerge across different cohorts.
Across different cohorts, understanding how these distinct domination fingerprints may have prognostic significance is a key step to optimizing stratification and intervention strategies. Nevertheless, the available evidence has largely been focused on Enterococcus domination [20,21,22,23,24]. For instance, Enterococcus domination has been linked to significant reduced overall survival, GvHD severity and increased risk of bloodstream infections (BSI) [21,23,24]. However, how other dominant genera may impact clinical outcomes remains poorly understood.
Therefore, in this study, we sought to provide a comprehensive overview of the dynamics, predictors and clinical implications of intestinal domination events in a cohort of Brazilian patients undergoing allo-HSCT. As shown in the subsequent sections of this manuscript, we identified a unique domination fingerprint in our cohort and conclude that the prognostic significance of intestinal domination during allo-HSCT may vary according to the dominant genera and to the population being evaluated.
2. Material and Methods
2.1. Study Design, Ethical Aspects and Sample Collections
This is an ongoing, observational, multi-center, prospective, cohort study of patients undergoing allo-HSCT, which was approved by the Research Ethics Committee from Sao Paulo State University (Process number 5.138.190/2021) and conducted according to the guidelines of the Declaration of Helsinki. All participants signed an informed consent form at the beginning of the study. For patients <18 years old, both the patient and their legal representative agreed to participate in the study and signed consent forms.
Stool samples were collected at four different transplant centers (Hospital de Base of the Fundação Faculdade Regional de Medicina [HB-FUNFARME], Hospital Amaral Carvalho Hospital [HAC], Hospital de Cancer de Barretos [HCB] and Hospital Beneficência Portuguesa de Sao Paulo [BP]) and stored at -80°C. Stool samples were collected longitudinally at 7 time points: Prior to conditioning regimen (D-7), At the day of stem cell infusion (D0), 30 days after stem cell infusion (D+30), D+60, D+90, D+180, and at acute GvHD diagnosis. Although all efforts were made to collect the specimens in these exact time points, some variability occurred due to the timing and frequency of bowel movement patterns. Additionally, some samples were not collected from patients who were discharged from the original institution to continue follow-up in their hometown or, in some cases, when the patient was critically ill.
2.2. Intestinal Microbiota 16S Sequencing and Bioinformatics Pipeline
DNA was obtained from 200 mg from fecal samples by using QIAamp Fast DNA Stool Mini Kit (Qiagen, CA, USA), according to manufacturer protocol. DNA was then quantified by Qubit dsDNA HS Assay Kit (Thermofisher). The 16S sRNA V3-V4 regions were then amplified by PCR using pre-determined primers and sequenced on the Ilumina MiSeq platform. The high-throughput sequencing reads underwent adapter removal using the Cutadapt v2.6 [25]. Then, the reads underwent quality filtering, denoising, chimera removal and amplicon sequence variant (ASV) inference using the DADA2 v.1.26.0 [26]. Taxonomic classification was performed using the Classify-sklearn naive Bayes classifier (q2-feature-classifier plugin), which was trained on the SILVA SSU v138.1 NR 99 database [27]. Tables were then developed to compute the abundance of reads assigned to each operational taxonomic unit (OTU).
2.3. Statistical Analysis
Intestinal domination was defined as the relative abundance ≥ 30% of any specific genera within each stool sample [19,21,23,24,28]. This analysis was focused on genera because this is generally the most specific level at which 16S sequencing can provides reliable classification [17]. We first generated descriptive statistics separated by intestinal domination status. Tests of associations between intestinal domination status and variables were examined by chi-square or Fisher’s exact test for categorical variables and Wilcoxon rank sum test for continuous variable. Consistent with prior studies evaluating intestinal domination, the outcomes of interested were overall survival and cumulative incidence of aGvHD and severe aGvHD (grade 2-4) (17,21,24,29). Overall survival was analyzed using the Kaplan-Meier methodology and survival curves were compared using the log-rank test. The time-to-event was calculated from D0 (day of stem cell infusion) to the date of death by any cause, aGvHD or last follow-up. Acute GvHD was diagnosed clinically, confirmed pathologically by biopsy whenever possible, and graded per the MAGIC criteria [29]. Similar to prior studies, the onset of aGvHD was determined based on the onset of symptoms (clinical suspicion) [15]. A Cox regression analysis was used to evaluate the association between intestinal domination and aGvHD. Univariable logistic regression models were used to identify predictors of intestinal domination (see Supplementary Methods for details). All analysis was performed using the software R. A P-value of <.05 was considered statistically significant.
3. Results
3.1. Included Samples and Prevalence of Intestinal Domination
During the study period, 69 patients undergoing allo-HSCT provided 192 stool samples. The proportion of samples in each timepoint are shown in Supplementary Table S1.
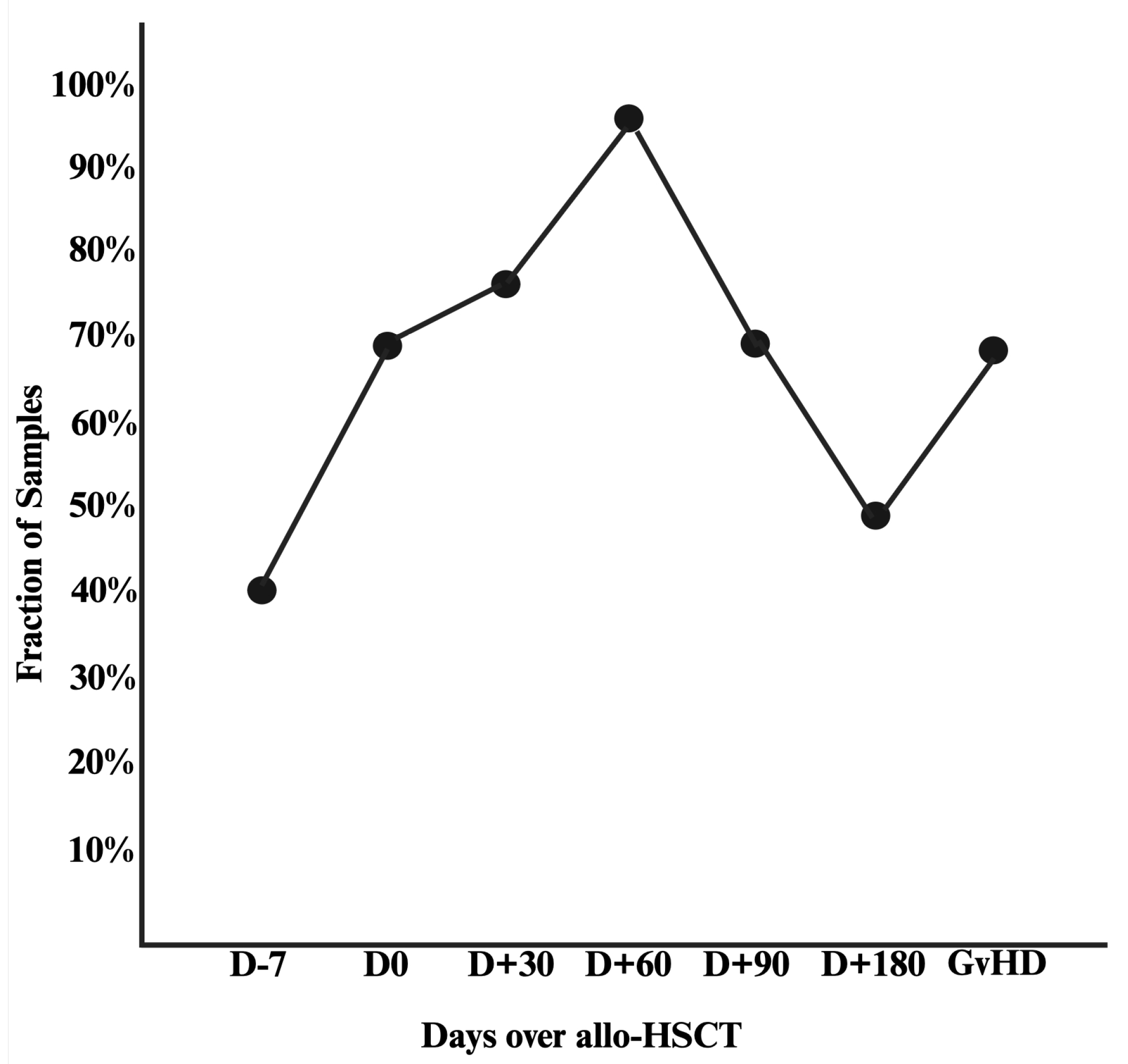
At the patient level, the prevalence of intestinal domination at any time point was 78.2% (n = 54/69). Among the 192 stool samples, 131 (68.2%) had an intestinal domination event in any time point. The prevalence of intestinal domination in each time point is shown in Figure 1. The lowest prevalence occurred in samples collected prior to the conditioning regimen (n = 20/48; 41.6%). The highest prevalence occurred in samples collected 60 days after the allo-HSCT (n = 29/30; 96.6%). At the time of aGvHD diagnosis, 70% of patients had intestinal domination by a single genus. Additionally, among the 131 samples with intestinal domination, 17 (13.9%) had concurrent domination by two distinct genera (see Supplementary Table S2).
Figure 1.
Compositional change of intestinal domination by any genera over the allo-HSCT.
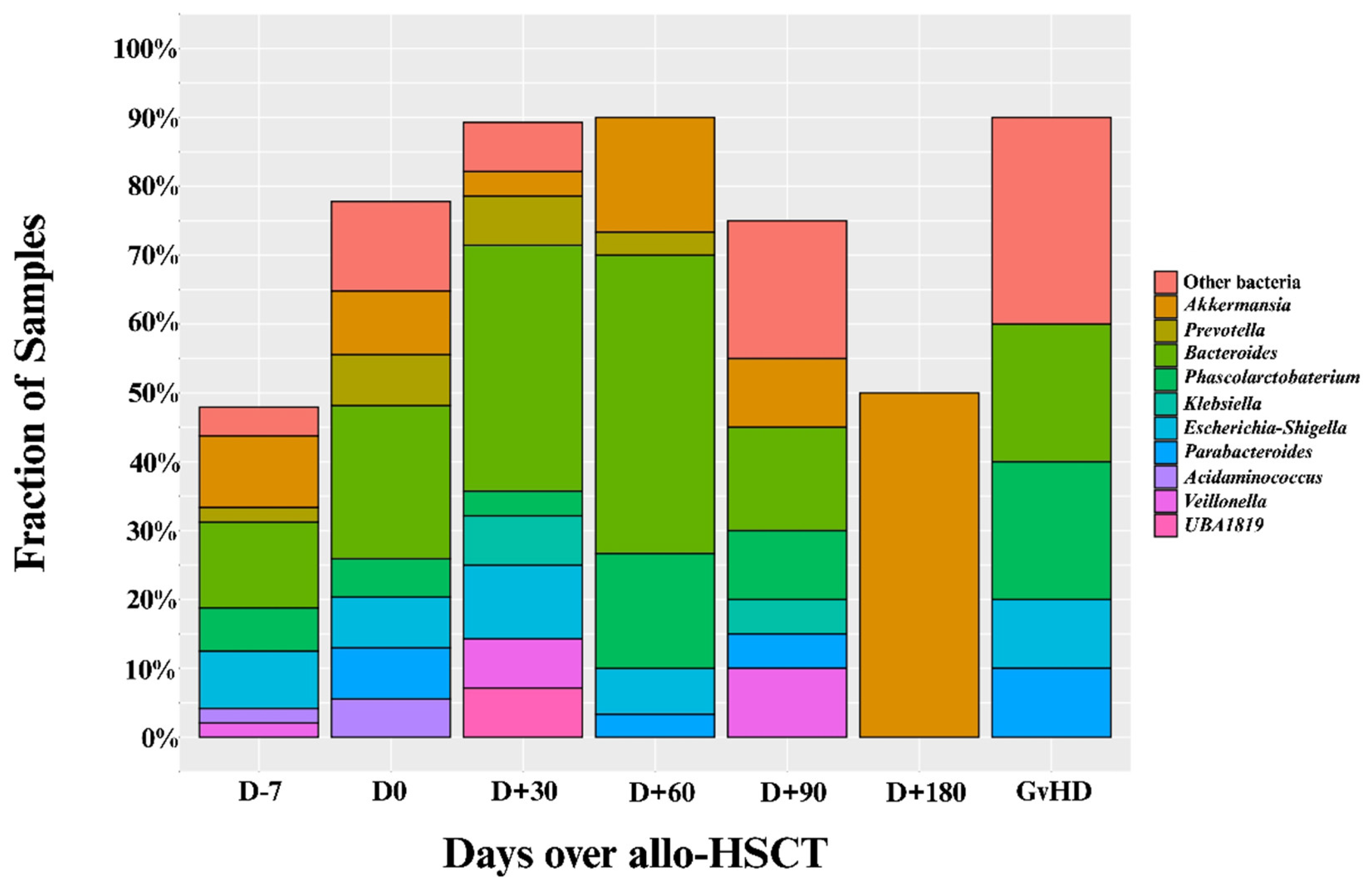
The specific genera responsible for these intestinal domination events are shown in Figure 2. Overall, most of these domination events occurred due to expansion of four genera: 1) Bacteroides (n = 46), 2) Akkermansia (n = 19), 3) Phascolarctobacterium (n = 16), and 4) Escherichia-Shigella (n = 14; see Figure 2). Interestingly, only 1 (0.5%) sample had Enterococcus domination (see Supplementary Table S3).
Figure 2.
Proportion of intestinal domination events by specific genera over the course of allo-HSCT. Allo-HSCT = Allogeneic hematopoietic stem cell transplantation.
Figure 2.
Proportion of intestinal domination events by specific genera over the course of allo-HSCT. Allo-HSCT = Allogeneic hematopoietic stem cell transplantation.
3.2. Patient Characteristics by Intestinal Domination Status
Patient demographic information separated by intestinal domination status is shown in Table 1. No statistically significant differences were found for any of the demographic characteristics (age, weight, height, and sex). Additionally, no statistically significant differences were found for any allo-HSCT-related variable (prior allo-HSCT, stem cell source, donor type and conditioning regimen).

Table 1.
Baseline Demographic Characteristics by Intestinal Domination Status.
| Variable |
No-Intestinal Domination (n=15) |
Yes-Intestinal Domination (n=54) |
Total (N=69) |
P-value |
| Age (years) | 0.6 | |||
| Mean (SD) | 44 (19) | 41 (15) | 40 (16) | |
| Median (IQR) | 40 (27-68) | 42 (31-51) | 40 (28-49) | |
| Range | 18-74 | 12-71 | 12-73 | |
| Weight (kg) | 0.12 | |||
| Mean (SD) | 79 (16) | 72 (17) | 74 (17) | |
| Median (IQR) | 79 (68-87) | 68 (62-82) | 74 (64-82) | |
| Range | 48-110 | 43-130 | 43-130 | |
| Height (cm) | 0.091 | |||
| Mean (SD) | 170 (10) | 166 (10) | 167 (10) | |
| Median (IQR) | 173 (160-178) | 164 (158-174) | 165 (160 – 175) | |
| Range | 150-185 | 146-189 | 146-189 | |
| Center | 0.2 | |||
| HB-FUNFARME | 4 (27%) | 5 (9.3%) | 9 (13%) | |
| HAC | 4 (27%) | 18 (33%) | 22 (32%) | |
| HCB | 0 (0%) | 8 (15%) | 8 (12%) | |
| BP | 7 (47%) | 23 (43%) | 30 (43%) | |
| Sex | 0.2 | |||
| Male | 9 (60%) | 22 (41%) | 31 (45%) | |
| Female | 6 (40%) | 32 (59%) | 38 (55%) | |
| Prior Allo-HSCT | 0 (0%) | 3 (6.4%) | 3 (5.1%) | >0.9 |
| Primary Disease | 0.4 | |||
| Acute Myeloid Leukemia | 6 (40%) | 23 (43%) | 29 (42%) | |
| Acute Lymphoid Leukemia | 1 (6.7%) | 15 (28%) | 16 (23%) | |
| Chronic Myeloid Leukemia | 1 (6.7%) | 2 (3.7%) | 3 (4.3%) | |
| Hodgkin’s Lymphoma | 1 (6.7%) | 1 (1.9%) | 2 (2.9%) | |
| Non-Hodgkin’s Lymphoma | 0 (0%) | 1 (1.9%) | 1 (1.4%) | |
| Aplastic Anemia | 2 (13%) | 5 (9.3%) | 7 (10%) | |
| Sickle Cell Disease | 1 (6.7%) | 2 (3.7%) | 3 (4.3%) | |
| Other | 3 (20%) | 5 (9.3%) | 8 (12%) | |
| Stem Cell Source | 0.4 | |||
| Peripheral Blood | 9 (60%) | 39 (72%) | 48 (70%) | |
| Bone Marrow | 6 (40%) | 15 (28%) | 21 (30%) | |
| Donor Type | 0.11 | |||
| Matched Related | 3 (20%) | 17 (31%) | 20 (29%) | |
| Matched Unrelated | 4 (27%) | 3 (5.6%) | 7 (10%) | |
| Mismatched Related | 0 (0%) | 3 (5.6%) | 3 (4.3%) | |
| Haploidentical | 7 (47%) | 30 (56%) | 37 (54%) | |
| Mismatched Unrelated | 1 (6.7%) | 1 (1.9%) | 2 (2.9%) | |
| Donor Sex | 0.4 | |||
| Male | 7 (47%) | 33 (61%) | 40 (58%) | |
| Female | 8 (53%) | 21 (39%) | 29 (42%) | |
| Intensity of Conditioning Regimen | 0.8 | |||
| Ablative | 4 (27%) | 21 (39%) | 25 (36%) | |
| Reduced Intensity | 7 (47%) | 20 (37%) | 27 (39%) | |
| Nonmyeloablative | 4 (27%) | 12 (22%) | 16 (23%) | |
| TBI-Conditioning Regimen | 6 (40%) | 29 (54%) | 35 (51%) | 0.3 |
| Allo-HSCT = Allogeneic hematopoietic stem cell transplant; BP = Hospital Beneficencia Portuguesa de Sao Paulo; Kg = kilograms; cm = centimeters; SD = Standard deviation; IQR = Interquartile range; TBI = Total body irradiation; HB-FUNFARME = Hospital de Base of Fundacao Faculdade Regional de Medicina; HAC = Hospital Amaral Carvalho; HCB = Hospital de Cancer de Barretos. | ||||
3.3. Analysis of Clinical Outcomes
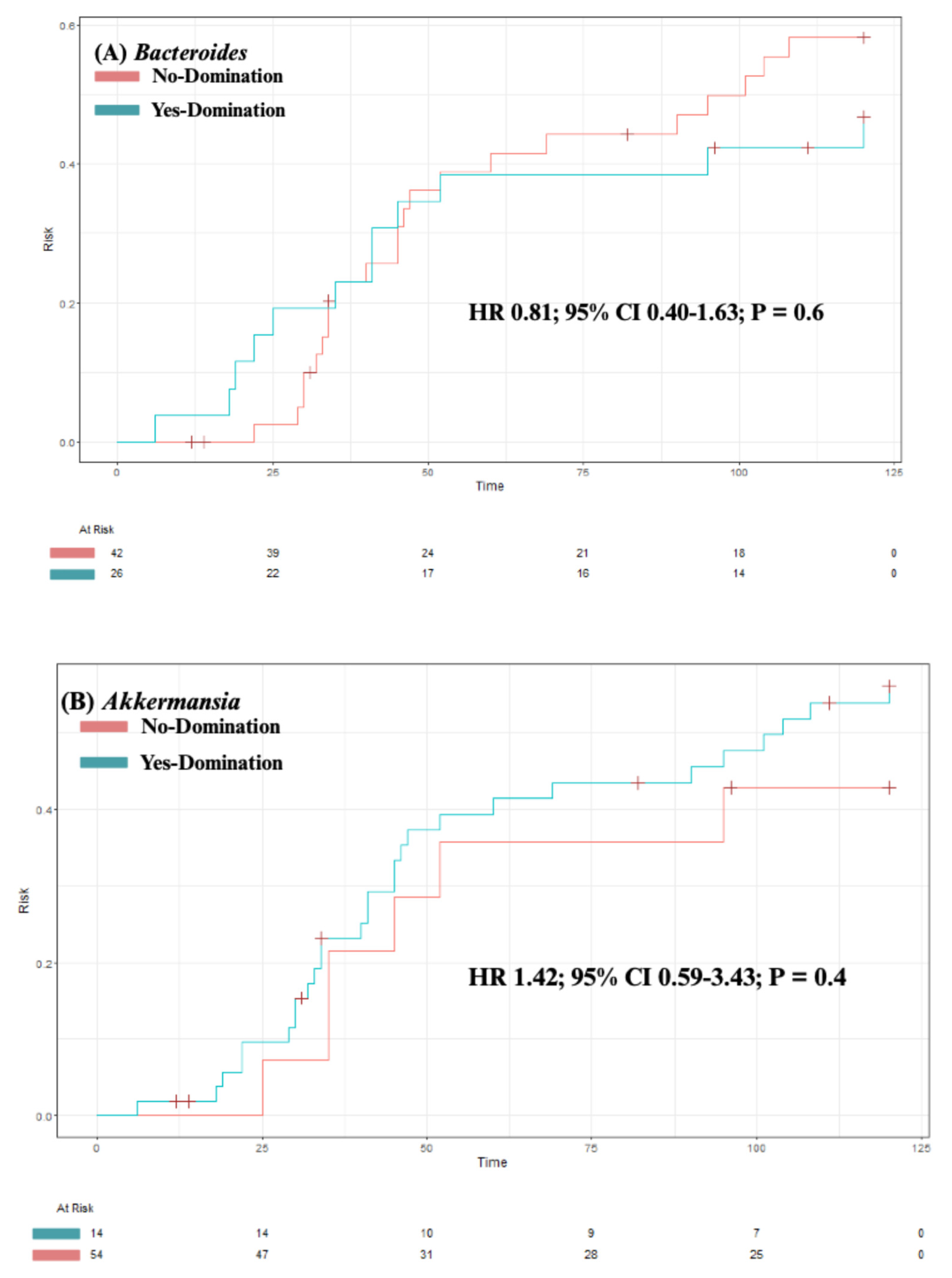
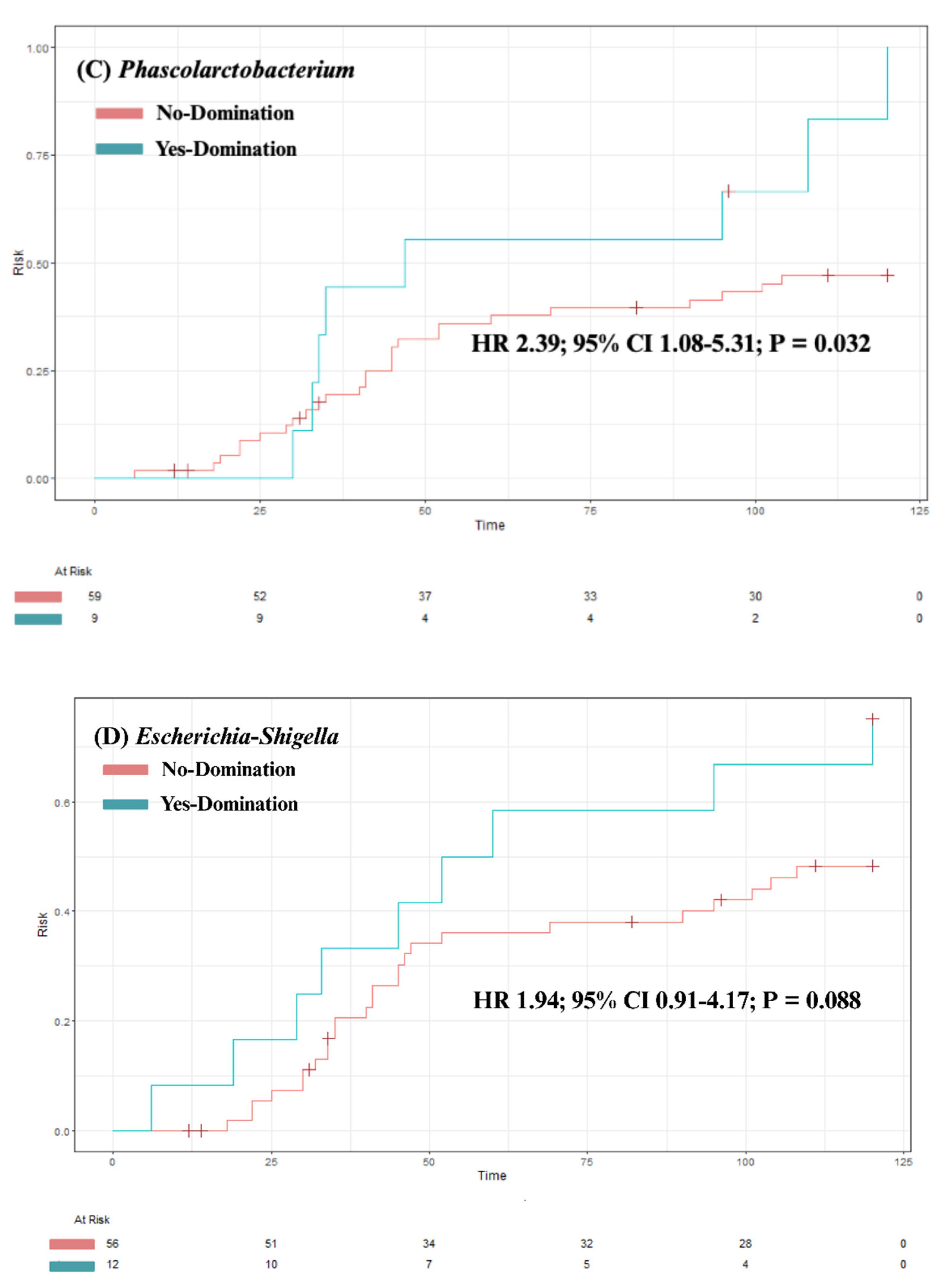
Our analysis identified no significant association between overall survival and intestinal domination by the four most commonly identified genera – Bacteroides (P = 0.84); Akkermansia (P = 0.47), Phascolarctobacterium (P = 0.4) and Escherichia-Shigella (P = 0.98; see Figure 3A-D). Although univariate analysis revealed a significant association between Phascolarctobacterium domination and cumulative incidence of aGvHD (HR 2.39; 95% CI 1.08-5.31; P = 0.032), this was not significant in a multivariable model after adjusting for age, sex, underlying diagnosis, conditioning regimen, donor sex, stem cell source, and donor type (HR 1.75; 95% CI 0.73-4.20; P = 0.2). For the other three genera, no significant associations were found between domination and cumulative incidence of aGvHD (see Figure 4A-D). Finally, domination by any of the four genera was not significantly associated with the cumulative incidence of severe aGvHD (see Supplementary Figure S1A-D).
Figure 3.
The impact of intestinal domination on overall survival. A) Bacteroides. B) Akkermansia. C) Phascolarctobacterium. D) Escherichia-Shigella. HR = Hazard Ratio. CI = Confidence interval.
Figure 3.
The impact of intestinal domination on overall survival. A) Bacteroides. B) Akkermansia. C) Phascolarctobacterium. D) Escherichia-Shigella. HR = Hazard Ratio. CI = Confidence interval.
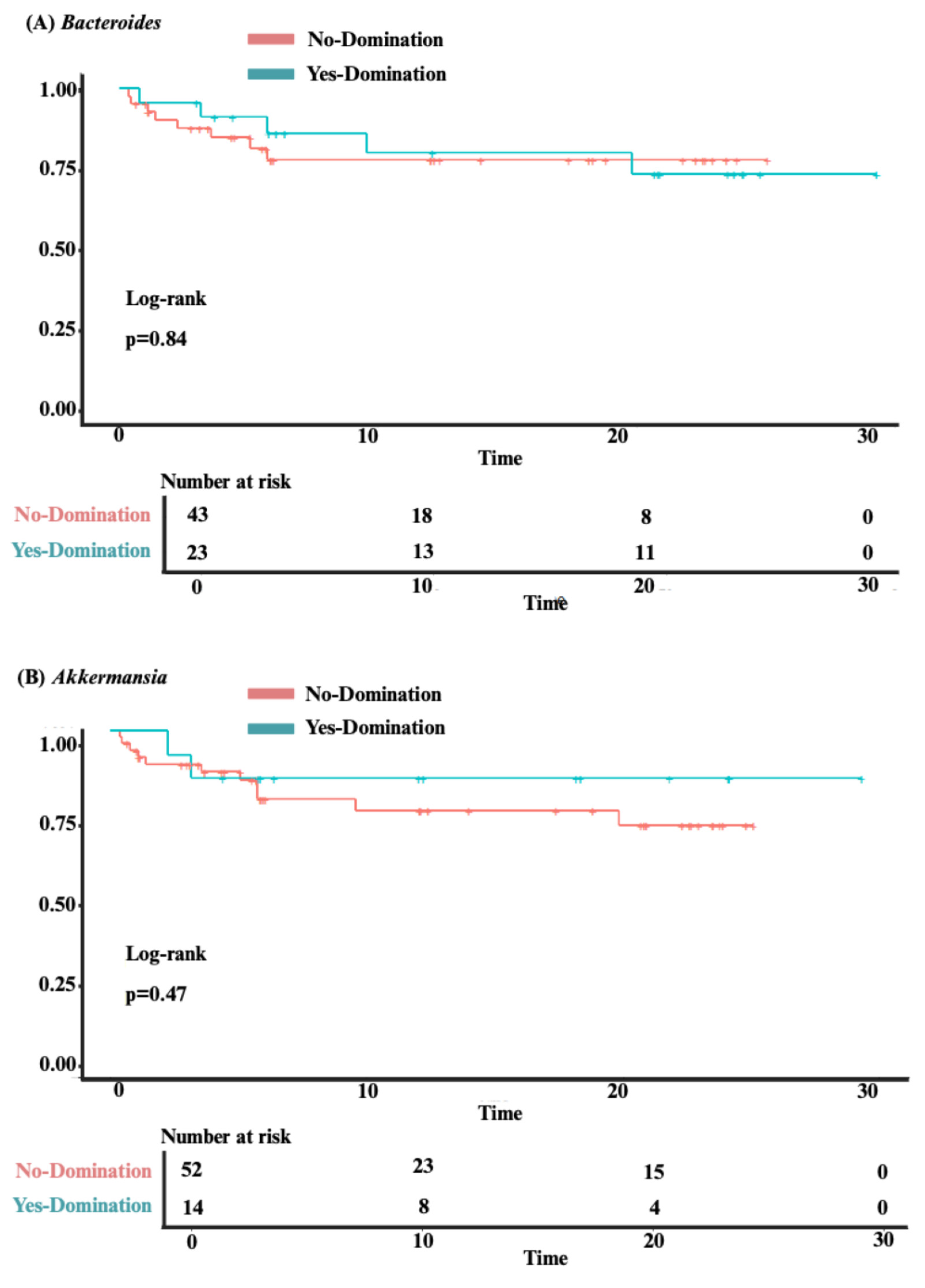
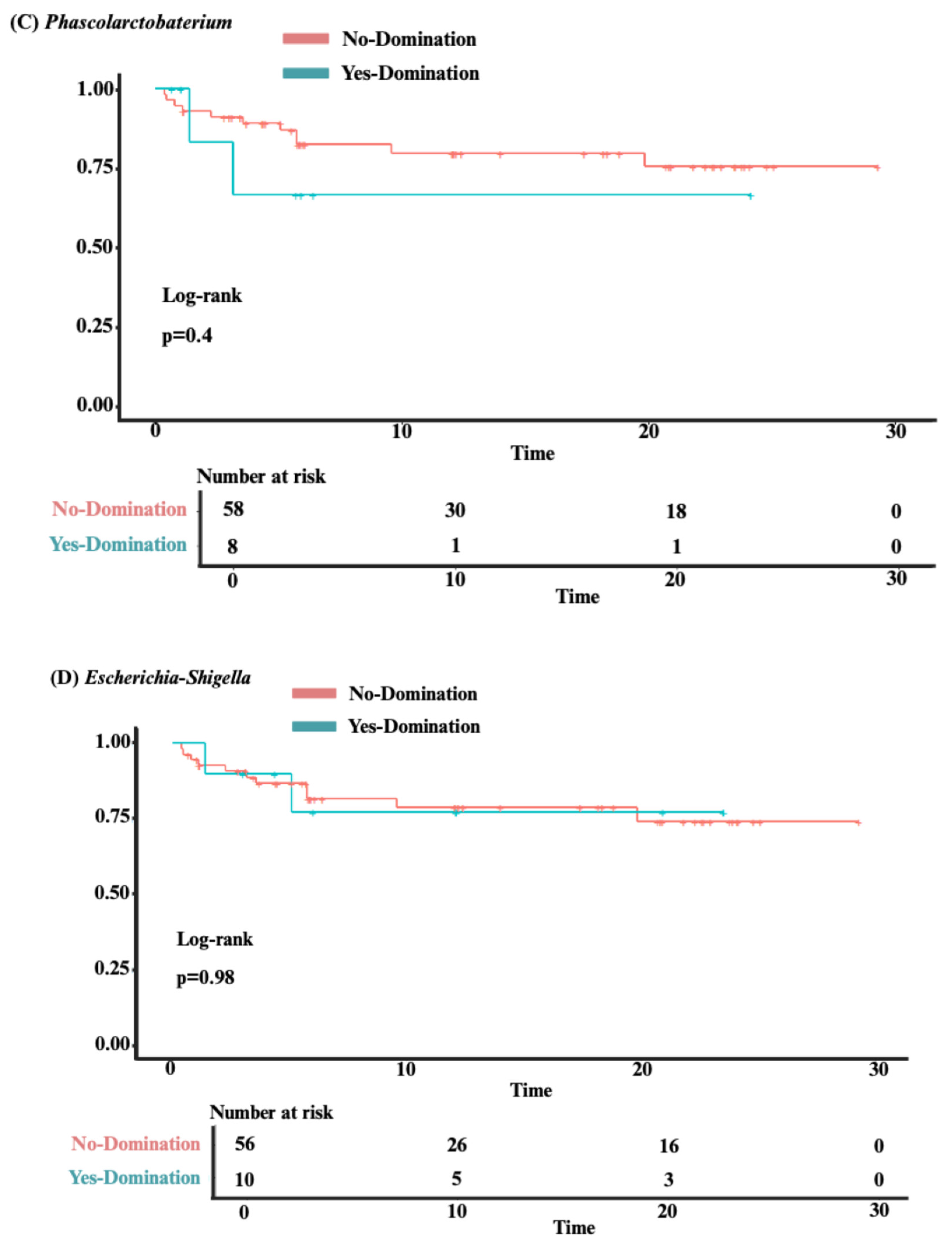
Figure 4.
The impact of intestinal domination on the cumulative incidence of aGvHD. A) Bacteroides. B) Akkermansia. C) Phascolarctobacterium. D) Escherichia-Shigella. HR = Hazard Ratio. CI = Confidence interval.
Figure 4.
The impact of intestinal domination on the cumulative incidence of aGvHD. A) Bacteroides. B) Akkermansia. C) Phascolarctobacterium. D) Escherichia-Shigella. HR = Hazard Ratio. CI = Confidence interval.
3.4. Predictors of Intestinal Domination
The univariable logistic regression model of predictors of intestinal domination by any genera and by Bacteroides, Akkermansia, Phascolarctobacterium and Escherichia-Shigella are shown in Table 2. None of the variables were associated with intestinal domination. Given the absence of statistically significant variables in the univariable model, a multivariable model was not performed.
Table 2.
Univariable Logistic Regression Model of Predictors of Intestinal Domination.
| Any Genus | Bacteroides | Akkermansia | Phascolarctobacterium | Escherichia-Shigella | ||||||
| OR (95%CI) | P value | OR (95%CI) | P value | OR (95%CI) | P value | OR (95%CI) | P value | OR (95%CI) | P value | |
| Age | 0.99 (0.95-1.02) | 0.46 | 0.99 (0.96-1.02) | 0.67 | 0.99 (0.96-1.03) | 0.73 | 1.03 (0.99-1.08) | 0.18 | 1.00 (0.96-1.04) | 0.88 |
| BMI | 0.98 (0.88-1.09) | 0.69 | 1.01 (0.92-1.11) | 0.81 | 0.99 (0.89-1.11) | 0.90 | 1.05 (0.93-1.20) | 0.41 | 0.94 (0.82-1.06) | 0.32 |
| Sex | ||||||||||
| Female | - | - | - | - | - | - | - | - | - | - |
| Male | 0.46 (0.14-1.45) | 0.19 | 0.65 (0.24-1.75) | 0.40 | 0.41 (0.10-1.41) | 0.18 | 0.31 (0.04-1.39) | 0.16 | 0.85 (0.23-2.99) | 0.80 |
| Conditioning regimen | ||||||||||
| Reduced intensity | - | - | - | - | - | - | - | - | - | - |
| Myeloablative | 1.75 (0.46-7.53) | 0.42 | 1.20 (0.39-3.69) | 0.75 | 2.33 (0.61-10.1) | 0.23 | 1.14 (0.19-6.70) | 0.88 | 1.14 (0.24-5.39) | 0.86 |
| Non-myeloablative | 1.00 (0.25-4.47) | >0.99 | 1.08 (0.29-3.85) | 0.91 | 1.38 (0.24-7.24) | 0.70 | 1.92 (0.32-11.7) | 0.46 | 2.00 (0.41-9.87) | 0.38 |
| TBI-Conditioning Regimen | 1.74 (0.55-5.84) | 0.35 | 1.57 (0.59-4.26) | 0.37 | 1.38 (0.43-4.70) | 0.59 | 1.25 (0.30-5.48) | 0.76 | 0.97 (0.27-3.43) | 0.96 |
| Stem cell source | ||||||||||
| Peripheral | - | - | - | - | - | - | - | - | - | - |
| Bone marrow | 0.58 (0.18-1.98) | 0.37 | 1.03 (0.35-2.93) | 0.96 | 1.35 (0.37-4.58) | 0.63 | 0.25 (0.01-1.50) | 0.21 | 1.83 (0.48-6.60) | 0.36 |
| Underlying diagnosis | ||||||||||
| Acute leukemia | - | - | - | - | - | - | - | - | - | - |
| Others | 0.40 (0.12-1.33) | 0.13 | 0.76 (0.25-2.20) | 0.62 | 0.89 (0.22-3.10) | 0.87 | 0.25 (0.01-1.50) | 0.21 | 1.18 (0.28-4.29) | 0.81 |
| BMI = Body mass index; CI = Confidence interval; OR = Odds ratio; TBI = Total body irradiation. | ||||||||||
4.. Discussion
In this multicenter, prospective, observational study we outlined the dynamics, predictors and clinical implications of intestinal domination in Brazilian patients undergoing allo-HSCT. We first identified that intestinal domination is a prevalent dysbiosis fingerprint occurring in 78.2% of patients. Then, we demonstrated that Enterococcus domination is a rare event occurring in only 1.4% of patients. Most of the intestinal domination events in our cohort were due to expansion of Bacteroides, Akkermansia, Phascolarctobacterium, and Escherichia-Shigella. Although intestinal domination by these genera was frequent in our cohort, we observed that it does not significantly impact key clinical outcomes such as overall survival and aGvHD incidence. Finally, we identified that no patient or allo-HSCT characteristics were predictive of intestinal domination.
In our analysis, the most interesting finding is that although intestinal domination occurred in 78.2% of patients, this was rarely driven by Enterococcus expansion (only one patient). This extremely low prevalence of Enterococcus domination (1.4%) differs from the current literature. In prior studies examining intestinal domination in patients undergoing allo-HSCT, Enterococcus has been identified as a key driver of domination events, occurring in 36% to 65% of patients (9,19,21–24). On the higher end of the spectrum of reported Enterococcus domination is a 65% domination prevalence reported in a study including 1,325 patients with 9,049 stool specimens [21]. In this study, Enterococcus genus was the most commonly observed to dominate the microbiota in patients from the four different participating centers [21]. On the lower end of the spectrum is a 36% Enterococcus domination prevalence occurring in a study including 98 patients with 681 stool specimens [24]. In this study, the median time between transplant date and first stool sample with Enterococcus domination was 22 days (IQR 6.75-84.25) [24]. It is important to note, however, that each of these studies used distinct times of sample collection, which may hinder an accurate comparison across studies (9,19,21–24). Nevertheless, compared to these studies, our findings suggest that Enterococcus may not be a key genus driving intestinal domination in Brazilian patients. Therefore, future studies should evaluate which other genera are driving intestinal domination in this cohort.
Our findings identified that important genera driving intestinal domination in Brazilian patients are Bacteroides, Akkermansia, Phascolarctobacterium, and Escherichia-Shigella. In our cohort, these four genera were responsible for most of the domination events. While Bacteroides and Akkermansia have been reported as dominant genera in prior studies, the high frequency of Phascolarctobacterium and Escherichia-Shigella domination is not well demonstrated in the prior literature (9,19–24). The dynamics of intestinal domination was evaluated in 100 patients with 603 stool specimens [19]. This study demonstrated an interesting compositional shift [19]. While Bacteroides was the most common dominant genera before conditioning, at the time of engraftment, intestinal domination occurred predominantly due to pathogenic genera such as Enterococcus, Klebsiella and Escherichia-Shigella [19]. In another study including 98 patients undergoing allo-HSCT, 681 stool specimens were analyzed [24]. The most frequent genera responsible for intestinal domination in decreasing order was as follows: 1) Streptococcus (42%), 2) Enterococcus (36%), and 3) Bacteroides (38%) [24]. Other important dominant genera reported in this study were Akkermansia, Blautia and Lactobacillus, each of which was associated with intestinal domination in approximately 28% of patients [24]. A similar profile was also identified in another study including 94 patients with 439 stool specimens [23]. In this study, Enterococcus was the most frequent dominating genus (40%), followed by Streptococcus (37%) [23]. When compared to these previous studies, our findings suggests that Brazilian patients undergoing allo-HSCT may exhibit a unique intestinal domination fingerprint. This may be partially explained by distinct dietary habits and antibiotics use across countries [19]. Additionally, our findings of persistent Bacteroides domination (a common feature in healthy individuals) over the allo-HSCT, may also suggest a more resilient microbiota in our cohort [24,30,31]. Whether this intestinal domination fingerprint identified in our analysis has prognostic significance was the next question we tried to answer in this study.
In our attempt to evaluate the prognostic significance of this intestinal domination fingerprint, we evaluated overall survival and aGvHD, which are key clinical outcomes that have been linked with Enterococcus domination [20,21,23,24]. For example, in the aforementioned study including 1,325 patients undergoing allo-HSCT, Enterococcus domination was associated with an approximately two-fold decreased in overall survival (HR 1.97; 95% CI 1.45 – 2.66; P < 0.001) [21]. This finding remained significant in a multivariate analysis adjusted for graft source, age, conditioning intensity, gender and underlying disease (HR 2.06; 95% CI 1.50-2.82; P < 0.0001) [21]. In this same study, Enterococcus domination was also significantly associated with GvHD severity in both univariate (HR 1.44; 95% CI 1.10-1.88; P < 0.01) and multivariate (HR 1.32; 95% CI 1.00-1.75; P < 0.05) analysis [21]. It is worth noting that few studies in the literature have specifically analyzed the clinical implications of intestinal domination by some of the genera identified in our cohort. Bacteroides and Akkermansia domination, for example, was not significantly associated with overall survival (P = 0.08 and P = 0.14) in a prior study with 98 patients [24]. This is further corroborated by our findings, demonstrating that intestinal domination by Bacteroides, Akkermansia, Phascolarctobacterium and Escherichia-Shigella may not impact clinical outcomes. Thus, our findings suggest that the prognostic significance of intestinal domination may vary according to the dominant genera and the population being evaluated. Nevertheless, given the relatively low number of patients and stool samples (when compared to prior studies) included in our analysis, future large prospective studies are needed to validate these findings.
Given the potential prognostic significance of intestinal domination, the final planned analysis was to identify predictors of intestinal domination in our cohort. Our findings demonstrated that no patient-level variable can reliably predict intestinal domination during allo-HSCT. This finding is partially supported by previous studies [22,23]. With the aim to identify predictors of Streptococcus domination, a prior study with 94 patients evaluated the following variables: age, sex, underlying diagnosis, prior antibiotic use, conditioning regimen intensity, T-cell depleted graft, stem cell source, and fever [23]. In this analysis, none of the evaluated variables reliably predicted Streptococcus domination [23]. However, in this same study, Enterococcus domination was increased three-fold in patients receiving metronidazole (HR 3.38; 95% CI-6.73; P = 0.01) and in patients with acute leukemia (HR 3.22; 95% CI 1.60-6.94; P = 0.01) [23]. Similar findings were reported by another study with 46 patients undergoing allo-HSCT [22]. Among seven potential predictors (age, sex, donor source, graft type, conditioning regimen intensity, and TBI-containing regimen), only acute leukemia was associated with Enterococcus domination (HR 2.48; 95% CI 1.13–5.45; P = 0.024.) [22]. When combined with our findings, these data suggest that patient-level variables may not be reliable predictors of intestinal domination. Additionally, they suggest that predictors of intestinal domination may vary according on the specific genus involved. Given the prognostic significance associated with some of these dominant genera, future studies evaluating other potential predictors are desired.
The primary strength of this study lies in its comprehensive approach to evaluate the dynamics, predictors, and clinical implications of intestinal domination in Brazilian patients undergoing allo-HSCT. Nevertheless, our study presents some limitations. First, although we had pre-specified time points for stool sample collection, many patients were unable to provide samples at later stages, which significantly reduced the number of samples beyond day +90. Additionally, we have not collected stool samples over the engraftment period, which has been extensively analyzed by prior studies (9,19–24). The lack of samples over this period hinders an accurate comparison with other studies. Furthermore, due to data collection limitations in some centers, we were unable to evaluate: 1) the impact of intestinal domination in BSI, and 2) the role of antibiotics as a predictor of intestinal domination. Finally, all participating centers in our study were located within a single Brazilian state (Sao Paulo), which may limit the generalizability of our findings. Notwithstanding these limitations, our study is an important milestone to define the dynamics and implications of intestinal domination events in Brazilian patients undergoing allo-HSCT.
5. Conclusion
In a cohort of Brazilian patients undergoing allo-HSCT, we identified a unique intestinal domination fingerprint characterized by an extremely low prevalence of Enterococcus expansion. Although intestinal domination was a prevalent dysbiosis feature occurring in 78.2% of patients, our findings showed that intestinal domination by Bacteroides, Akkermansia, Phascolarctobacterium and Escherichia-Shigella was not significantly associated with overall survival and aGvHD incidence. We conclude that the prognostic significance of intestinal domination during allo-HSCT may vary according to the dominant genera and to the population being evaluated. Future prospective multi-center studies are desired to evaluate the factors driving these distinct domination fingerprints.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Proportion of Samples in Each Timepoint; Table S2: Details of Samples with Concurrent Domination by Two Distinct Genera; Table S3. Number of Intestinal Domination Events per Genus; Table S4. Antibiotic Practices in Each Institution; Figure S1. The Impact of intestinal domination on the cumulative incidence of severe aGvHD. Supplementary Methods – Predictors of Intestinal Domination.
Author Contributions
All authors contributed significantly to the development of this study and manuscript. GLVO and ASFJ conceived the study. GLVO, ASFJ and WYH developed the study protocol with input from other authors. WYH developed the statistical analysis with input from GLVO and ASFJ. GLVO gathered funding for this project. GLVO, ASFJ, DANA, LSS, LDM, NLS contributed to project administration. All authors contributed to data interpretation. ASFJ wrote the first full manuscript draft. All authors contributed to the manuscript and critically reviewed.
Funding
This research was funded by the São Paulo Research Foundation (FAPESP), process numbers #2022/12989-6 (Research grant for GLVO); #2023/08142-0 (Fellowship for ASFJ), #2024/02936-8 (Fellowship for DANA), #2023/12271-0 (Fellowship for NLS); by the Brazilian National Council for Scientific and Technological Development (CNPq), process number #313190/2021-6 (Fellowship for GLVO), and by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001. The content in this manuscript is solely the responsibility of the authors and does not in any way represent the official views of the funders.
Institutional Review Board Statement
This study was approved by the Research Ethics Committee from Sao Paulo State University (Process number 5.138.190/2021, date 1 December 2021) and conducted according to the guidelines of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not Applicable.
Acknowledgments
During the preparation of this manuscript, the author(s) used ChatGPT solely for grammatical corrections. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hill GR, Betts BC, Tkachev V, Kean LS, Blazar BR. Current Concepts and Advances in Graft-Versus-Host Disease Immunology. Annu Rev Immunol. 2021 Apr 26;39(1):19–49.
- Ferrara JL, Levine JE, Reddy P, Holler E. Graft-versus-host disease. The Lancet. 2009 May;373(9674):1550–61.
- Jagasia M, Arora M, Flowers MED, Chao NJ, McCarthy PL, Cutler CS, et al. Risk factors for acute GVHD and survival after hematopoietic cell transplantation. Blood. 2012 Jan 5;119(1):296–307.
- Ilett EE, Jørgensen M, Noguera-Julian M, Nørgaard JC, Daugaard G, Helleberg M, et al. Associations of the gut microbiome and clinical factors with acute GVHD in allogeneic HSCT recipients. Blood Advances. 2020 Nov 24;4(22):5797–809.
- Nesher L, Rolston KVI. Febrile Neutropenia in Transplant Recipients. In: Safdar A, editor. Principles and Practice of Transplant Infectious Diseases [Internet]. New York, NY: Springer New York; 2019 [cited 2025 Jun 13]. p. 185–98. Available from: http://link.springer.com/10.1007/978-1-4939-9034-4_9.
- Barrett AJ, Battiwalla M. Relapse after allogeneic stem cell transplantation. Expert Review of Hematology. 2010 Aug;3(4):429–41.
- Wang S, Yue X, Zhou H, Chen X, Chen H, Hu L, et al. The association of intestinal microbiota diversity and outcomes of allogeneic hematopoietic cell transplantation: a systematic review and meta-analysis. Ann Hematol. 2023 Dec;102(12):3555–66.
- Staffas A, Burgos da Silva M, van den Brink MRM. The intestinal microbiota in allogeneic hematopoietic cell transplant and graft-versus-host disease. Blood. 2017 Feb 23;129(8):927–33.
- Peled JU, Gomes ALC, Devlin SM, Littmann ER, Taur Y, Sung AD, et al. Microbiota as Predictor of Mortality in Allogeneic Hematopoietic-Cell Transplantation. N Engl J Med. 2020 Feb 27;382(9):822–34.
- Li Z, Xiong W, Liang Z, Wang J, Zeng Z, Kołat D, et al. Critical role of the gut microbiota in immune responses and cancer immunotherapy. J Hematol Oncol. 2024 May 14;17(1):33.
- Masetti R, Leardini D, Muratore E, Fabbrini M, D’Amico F, Zama D, et al. Gut microbiota diversity before allogeneic hematopoietic stem cell transplantation as a predictor of mortality in children. Blood. 2023 Oct 19;142(16):1387–98.
- Mancini N, Greco R, Pasciuta R, Barbanti MC, Pini G, Morrow OB, et al. Enteric Microbiome Markers as Early Predictors of Clinical Outcome in Allogeneic Hematopoietic Stem Cell Transplant: Results of a Prospective Study in Adult Patients. Open Forum Infectious Diseases. 2017 Nov 20;4(4):ofx215.
- Taur Y, Jenq RR, Perales MA, Littmann ER, Morjaria S, Ling L, et al. The effects of intestinal tract bacterial diversity on mortality following allogeneic hematopoietic stem cell transplantation. Blood. 2014 Aug 14;124(7):1174–82.
- Payen M, Nicolis I, Robin M, Michonneau D, Delannoye J, Mayeur C, et al. Functional and phylogenetic alterations in gut microbiome are linked to graft-versus-host disease severity. Blood Advances. 2020 May 12;4(9):1824–32.
- Golob JL, Pergam SA, Srinivasan S, Fiedler TL, Liu C, Garcia K, et al. Stool Microbiota at Neutrophil Recovery Is Predictive for Severe Acute Graft vs Host Disease After Hematopoietic Cell Transplantation. Clinical Infectious Diseases. 2017 Nov 29;65(12):1984–91.
- Haak BW, Littmann ER, Chaubard JL, Pickard AJ, Fontana E, Adhi F, et al. Impact of gut colonization with butyrate producing microbiota on respiratory viral infection following allo-HCT. Blood. 2018 Apr 19;blood-2018-01-828996.
- Jenq RR, Taur Y, Devlin SM, Ponce DM, Goldberg JD, Ahr KF, et al. Intestinal Blautia Is Associated with Reduced Death from Graft-versus-Host Disease. Biology of Blood and Marrow Transplantation. 2015 Aug;21(8):1373–83.
- Meedt E, Hiergeist A, Gessner A, Dettmer K, Liebisch G, Ghimire S, et al. Prolonged Suppression of Butyrate-Producing Bacteria Is Associated With Acute Gastrointestinal Graft-vs-Host Disease and Transplantation-Related Mortality After Allogeneic Stem Cell Transplantation. Clinical Infectious Diseases. 2022 Mar 1;74(4):614–21.
- Gu Z, Xiong Q, Wang L, Wang L, Li F, Hou C, et al. The impact of intestinal microbiota in antithymocyte globulin–based myeloablative allogeneic hematopoietic cell transplantation. Cancer. 2022 Apr;128(7):1402–10.
- Chhabra S, Szabo A, Clurman A, McShane K, Waters N, Eastwood D, et al. Mitigation of gastrointestinal graft-versus-host disease with tocilizumab prophylaxis is accompanied by preservation of microbial diversity and attenuation of enterococcal domination. haematol. 2022 Sep 15;108(1):250–6.
- Stein-Thoeringer CK, Nichols KB, Lazrak A, Docampo MD, Slingerland AE, Slingerland JB, et al. Lactose drives Enterococcus expansion to promote graft-versus-host disease. Science. 2019 Nov 29;366(6469):1143–9.
- Fujimoto K, Hayashi T, Yamamoto M, Sato N, Shimohigoshi M, Miyaoka D, et al. An enterococcal phage-derived enzyme suppresses graft-versus-host disease. Nature. 2024 Aug 1;632(8023):174–81.
- Taur Y, Xavier JB, Lipuma L, Ubeda C, Goldberg J, Gobourne A, et al. Intestinal Domination and the Risk of Bacteremia in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. Clinical Infectious Diseases. 2012 Oct 1;55(7):905–14.
- Messina JA, Tan CY, Ren Y, Hill L, Bush A, Lew M, et al. Enterococcus Intestinal Domination Is Associated With Increased Mortality in the Acute Leukemia Chemotherapy Population. Clinical Infectious Diseases. 2024 Feb 17;78(2):414–22.
- Martin M. Cutadapt removes adapter sequences from high-throughput sequencing reads. EMBnet j. 2011 May 2;17(1):10.
- Callahan BJ, McMurdie PJ, Rosen MJ, Han AW, Johnson AJA, Holmes SP. DADA2: High-resolution sample inference from Illumina amplicon data. Nat Methods. 2016 Jul;13(7):581–3.
- Bokulich NA, Kaehler BD, Rideout JR, Dillon M, Bolyen E, Knight R, et al. Optimizing taxonomic classification of marker-gene amplicon sequences with QIIME 2’s q2-feature-classifier plugin. Microbiome. 2018 Dec;6(1):90.
- Kusakabe S, Fukushima K, Yokota T, Hino A, Fujita J, Motooka D, et al. Enterococcus: A Predictor of Ravaged Microbiota and Poor Prognosis after Allogeneic Hematopoietic Stem Cell Transplantation. Biology of Blood and Marrow Transplantation. 2020 May;26(5):1028–33.
- Harris AC, Young R, Devine S, Hogan WJ, Ayuk F, Bunworasate U, et al. International, Multicenter Standardization of Acute Graft-versus-Host Disease Clinical Data Collection: A Report from the Mount Sinai Acute GVHD International Consortium. Biology of Blood and Marrow Transplantation. 2016 Jan;22(1):4–10.
- MetaHIT Consortium (additional members), Arumugam M, Raes J, Pelletier E, Le Paslier D, Yamada T, et al. Enterotypes of the human gut microbiome. Nature. 2011 May 12;473(7346):174–80.
- The Human Microbiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature. 2012 Jun;486(7402):207–14.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



