
Submitted:
02 February 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Background: Early identification of small choroidal melanomas is important, as metastatic risk increases with tumor size. However, distinguishing small melanomas from benign choroidal nevi is challenging and may lead to unnecessary referrals and overtreatment. Both the MOLES scoring system and the deep learning algorithm MelAInoma have been developed to support assessment of pigmented choroidal lesions in non-expert settings. This study aims to compare the association between MOLES and MelAInoma scores and to assess their relative association with expert melanoma versus nevus diagnosis. Methods: In this retrospective cohort study, 86 patients with small pigmented choroidal lesions (29 melanomas and 57 nevi) diagnosed at a national ocular oncology referral center were included. MOLES scores were assigned by ocular oncologists based on multimodal examination, whereas MelAInoma scores were generated solely from color fundus photographs. Associations between scores were assessed using linear regression and the Jonckheere–Terpstra test. Univariable and multivariable binary logistic regression was used to evaluate associations with melanoma diagnosis. Results: MelAInoma scores increased monotonically with higher MOLES categories (P=0.0001). Linear regression showed a statistically significant association between MOLES and MelAInoma scores, but with substantial dispersion (R2=0.16). In univariable logistic regression, both MOLES and MelAInoma scores were associated with increased odds of melanoma diagnosis. MelAInoma showed a stronger association with diagnosis than MOLES (R2=0.38 vs. 0.27). In multivariable analysis including both scores, each remained independently associated with melanoma diagnosis. Conclusions: Both MOLES and MelAInoma are effective for differentiating small choroidal melanomas from nevi. Although the scores are statistically associated, they capture partly distinct information. MelAInoma demonstrates slightly stronger association with melanoma diagnosis and provides fully reproducible output, supporting its role as a complementary aid in lesion triage.
Keywords:
choroidal melanoma
; uveal melanoma
; choroidal nevus
; MelAInoma
; MOLES
; artificial intelligence
; deep learning
; fundus photography
; ocular oncology
1. Introduction
The risk of metastasis in uveal melanoma is strongly correlated with tumor size.[1,2] Accurate identification of melanomas when they are as small as possible is therefore likely one of the most effective ways to improve survival in this aggressive disease. However, small choroidal melanomas may be difficult to distinguish from benign pigmented choroidal lesions, which are common in the general population and affect more than 5% of individuals of Caucasian descent.[3,4] Efforts to detect and treat choroidal melanomas at an early stage may therefore result in overdiagnosis and treatment of harmless lesions with potentially severe consequences for visual function.
In Sweden, opticians frequently use optical coherence tomography (OCT) and fundus photography in routine practice.[5] Together with widespread screening for diabetic retinopathy and frequent examinations or treatment for age-related macular degeneration (AMD) or cataract, this has led to detection of an increasing number of incidental pigmented choroidal lesions. As a consequence, a growing number of patients are referred to ocular oncologists, including many false-positive cases. This may pose a challenge, as ocular oncology is a highly specialized field with limited resources, and excessive referrals may delay assessment of patients who truly require intervention.
To support triage of pigmented choroidal lesions in non-expert settings, we have developed a deep learning algorithm, MelAInoma, which estimates the probability that a lesion represents a melanoma based on fundus photographs.[6] In prior evaluations, MelAInoma achieved higher diagnostic accuracy than ocular oncologists, consultant ophthalmologists, and resident ophthalmologists when classifying fundus images, using multimodal expert assessment as reference.[6] When applied by opticians and optometrists, MelAInoma quadrupled the odds of correctly referring a melanoma, reduced false-positive referrals tenfold, and provided net clinical benefit compared with unaided triage.[5]
In contrast, the MOLES system is a well-established, manually applied scoring system designed to support non-expert monitoring of pigmented choroidal lesions and referral decisions.[7,8] MOLES is widely used by opticians and ophthalmologists. By assessing and grading five visual risk factors for growth, lesions are classified as common nevus, low-risk nevus, high-risk nevus, or probable melanoma.[8]
In the present study, we use MOLES scores assigned by ocular oncologists and compare these with MelAInoma scores generated from fundus photographs. We then examine how each of these scores correlates with the true diagnosis, as established by subspecialized ocular oncologists, and assess their relative association with melanoma versus nevus classification.
2. Materials and Methods
2.1. Aim of the Study
The aim of this study is to examine whether MOLES and MelAInoma scores correlate, and to assess which of the two is more strongly associated with a diagnosis of choroidal melanoma versus choroidal nevus.
2.2. Patients and Lesions
This study included a cohort of 86 patients with one pigmented choroidal lesion each, diagnosed as either small choroidal melanoma or choroidal nevus at St. Erik Eye Hospital, Stockholm, Sweden. This study was approved by the Swedish Ethical Review Authority (reference 2025-05054-01) and adhered to the tenets of the declaration of Helsinki.
Inclusion criteria were as follows:
- Age >18 years at the time of examination.
- Fundus photograph obtained after January 1, 2010, corresponding to a period when medical records were fully digitalized, facilitating reliable assessment of follow-up.
- Diagnosis of either choroidal melanoma (International Classification of Diseases, 10th Revision [ICD-10] code C69.3) or choroidal nevus (ICD-10 code D31.3).
- Diagnosis established by a subspecialized ocular oncologist.
- For lesions classified as nevi at the time of photography, a minimum of 5 years of follow-up without reclassification as melanoma was required. Lesions that were diagnosed as melanoma at a later time point (e.g., due to documented growth) were classified as melanomas in the present study. This criterion was applied to facilitate detection of early signs of malignancy at a stage when small melanomas are difficult to distinguish from nevi.
Exclusion criteria were:
- Fundus photographs of insufficient quality, where factors such as poor focus, motion artifacts, over- or underexposure, or reflections prevented reliable assessment of lesion extent or the presence of features such as orange pigment or drusen. Minor image imperfections that did not impede assessment (e.g., focal blur or limited overexposure) were not sufficient for exclusion.
- Photographs in which less than half of the lesion was visible, acknowledging the limitation in accurately estimating the extent of the non-visible portion.
- Lesions obscured by retinal detachment, vitreous hemorrhage, or similar conditions.
The included lesions were imaged using either a standard-field fundus camera (45° field of view; Canon Medical Systems Europe B.V.; n=55) or an ultra-widefield camera (pseudocolor images covering 200°; Optos Inc.; n=31). This cohort has been described in detail previously, including the multimodal diagnostic workup used by ocular oncologists, as it was employed as a test cohort during the development and validation of the MelAInoma algorithm.[6] The cohort was not used for development or training of the MelAInoma deep learning model.
2.3. MOLES
MOLES is a clinical scoring system based on five features: Mushroom shape, Orange pigment, Large size, Enlarging tumor, and Subretinal fluid. Each feature is assigned a score of 0, 1, or 2, reflecting absence, borderline presence, or definite presence.[7,8] Mushroom shape is highly suggestive of choroidal melanoma and is included to ensure referral even in absence of other suspicious features. Orange pigment has been identified as an important risk factor for growth of melanocytic lesions, despite occurring in other choroidal conditions.[9,10] Large size is included because most choroidal nevi are small; in population-based studies, the mean largest basal diameter is approximately 1.25 mm, only a minority exceed 5.5 mm, and increased thickness is associated with a higher risk of future growth.[11] Although choroidal nevi may enlarge slowly over an extended period, more rapid growth is suggestive of malignant transformation.[12] Subretinal fluid is also included, as it has consistently been associated with lesion growth. Based on the total score, lesions are categorized as common nevus (score 0), low-risk nevus (score 1), high-risk nevus (score 2), or probable melanoma (score >2).[8] In this study, all MOLES scores were assigned by ocular oncologists at St. Erik Eye Hospital, with access to multimodal imaging for each lesion to assess the presence of risk factors, such as OCT for detection of subretinal fluid and autofluorescence for identification of orange pigment. In contrast, MelAInoma scores were based solely on analysis of color fundus photographs of the lesion.
2.4. Statistical Analyses
Associations between MOLES score and MelAInoma score were evaluated using linear regression. As MOLES score is an ordinal variable and MelAInoma score is continuous, an ordered trend was additionally assessed using the Jonckheere–Terpstra test, which does not assume normality. To evaluate the association between each score and diagnostic outcome, binary logistic regression was performed with true diagnosis (melanoma vs. nevus) as the dependent variable. Odds ratios (ORs) with 95% confidence intervals (CI) were reported. MelAInoma score and MOLES score were also entered simultaneously as predictors in a multivariable logistic regression model. No interaction terms or variable transformations were included. Model fit was assessed using the Akaike Information Criterion corrected for small sample size (AIC) and by evaluation of calibration with the Hosmer–Lemeshow test. MelAInoma scores were generated by loading fundus photographs into the MelAInoma software (version 0.1; Eyedentity AB, Stockholm, Sweden), which outputs a probability between 0 and 1 that the lesion represents a melanoma. All statistical tests were two-sided, and a significance level of P<0.05 was used. Data management and statistical analyses were performed using R version 4.4.3 (R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism version 10.6.1 (GraphPad Software, San Diego, CA, USA).
3. Results
3.1. Descriptive Statistics
The study included 86 patients with 86 pigmented choroidal lesions, of whom 48 (56%) were female. Of the 86 lesions, 57 (66%) were diagnosed as nevi and 29 (34%) as melanomas. Among melanomas, the mean tumor thickness was 2.8 mm and the mean largest basal diameter (LBD) was 6.6 mm. Further cohort characteristics are summarized in Table 1.
3.2. Distribution of MelAInoma Scores Across MOLES Scores
MelAInoma scores increased monotonically with increasing MOLES categories. The distribution of lesions by MOLES score was as follows: MOLES 0 (n=46), MOLES 1 (n=8), MOLES 2 (n=13), MOLES 3 (n=11), and MOLES ≥4 (n=8). Using the Jonckheere–Terpstra test to evaluate an ordered trend, there was strong evidence for increasing MelAInoma scores with higher MOLES categories (JT=1620, P=0.0001, one-sided test for increasing trend). This association persisted despite substantial ties in MelAInoma score values and unequal group sizes, indicating a consistent monotonic relationship between MOLES score and AI-based risk estimation (Figure 1). In addition, a rank-based one-way ANOVA (Kruskal–Wallis test) showed differences in MelAInoma score distributions across MOLES categories (P=0.0008)
3.3. Linear Regression
In linear regression analysis, increasing MOLES score was associated with higher MelAInoma score (slope 0.09 per MOLES unit, 95% CI 0.05 to 0.14, P<0.0001). However, the association showed considerable dispersion, with MOLES score explaining only 16% of the variability in MelAInoma score (R2=0.16, Figure 2).
3.4. Binary Logistic Regression for MOLES
In binary logistic regression with MOLES score as the sole predictor, higher MOLES score was associated with increased odds of melanoma diagnosis (Figure 3A). Each one-unit increase in MOLES score was associated with a more than twofold increase in the odds of melanoma (OR 2.29, 95% CI 1.59 to 3.50, P< 0.0001, Table 2). Model fit was acceptable, with a Tjur’s R2 of 0.27.
3.5. Binary Logistic Regression for MelAInoma
In binary logistic regression using MelAInoma score as the sole predictor, higher MelAInoma score was associated with increased odds of melanoma diagnosis (Figure 3B). When scaled per 0.1-unit increase, the odds of melanoma increased by a factor of 2.27 (OR 2.27 per 0.1 increase, 95% CI 1.57 to 4.23, P<0.0001, Table 3). Compared to the MOLES model, this model explained a larger proportion of outcome variability (Tjur’s R2=0.38).
3.6. Multivariable Binary Logistic Regression
In multivariable binary logistic regression including both MOLES score and MelAInoma score, both predictors remained associated with melanoma diagnosis. After adjustment for MOLES score, each 0.1-unit increase in MelAInoma score was associated with a 2.82-fold increase in the odds of melanoma (OR 2.82, 95% CI 1.62 to 6.85, P< 0.0001, Table 4). MOLES score also remained associated with melanoma diagnosis after adjustment for MelAInoma score (OR 2.24 per one-unit increase, 95% CI 1.40 to 4.02, P=0.002). The combined model showed substantially improved the fit compared with the intercept-only model (AIC 55.3 vs. 103.2), and there was no evidence of poor calibration based on the Hosmer–Lemeshow test (P=0.86).
3.7. Sensitivity Analysis by Imaging Modality
To determine if the AI algorithm’s performance remained stable across different clinical presentations and imaging hardware, a subgroup analysis was performed. Lesions were categorized based on whether they were captured with standard-field or ultra-widefield systems. It should be noted that while MelAInoma scores were derived solely from these color photographs, MOLES scores were established by ocular oncologists with access to multimodal imaging (e.g., OCT and autofluorescence). In the standard-field subgroup, MelAInoma achieved an AUC of 0.87 (95% CI 0.78–0.96) compared to 0.80 (95% CI 0.67–0.93) for MOLES with no statistically detectable diffrence between the methods (P=0.42, DeLong test). Similarly, in the ultra-widefield subgroup, MelAInoma achieved an AUC of 0.87 (95% CI 0.72–1.00) compared to 0.79 (95% CI 0.61–0.97) for MOLES (P=0.48). These findings indicate that MelAInoma maintains a high and stable diagnostic accuracy across different clinical subgroups, even when compared to an expert scoring system supported by multimodal data.
4. Discussion
In this study, we demonstrate that both the MOLES system and the MelAInoma algorithm were associated with melanoma diagnosis in a cohort of small pigmented choroidal lesions. The two systems demonstrated a statistically significant association, and higher values of either score were linked to higher odds of melanoma. This is clinically relevant, as both approaches are intended for use by non-expert opticians, optometrists, and ophthalmologists in settings where early triage of suspicious lesions is increasingly important.
Despite this overall concordance, there were notable differences between the two systems. Although the association between MOLES and MelAInoma scores was statistically significant, linear regression displayed substantial dispersion, with MOLES explaining only a limited proportion of the variability in MelAInoma score. This suggests that, while related, the two systems capture overlapping but not identical information. In univariable binary logistic regression, MelAInoma showed slightly stronger associations with melanoma diagnosis than MOLES. This difference may partly reflect the distributional properties of the two scores: MOLES values were heavily clustered at low scores, whereas MelAInoma scores were more continuously distributed across lesions, allowing for greater separation in estimated odds across the range of values.
In multivariable logistic regression, both MOLES and MelAInoma scores remained associated with melanoma diagnosis after adjustment for one another, indicating that each score contributed information beyond the other. Although the statistical evidence was slightly stronger for MelAInoma, the results do not suggest that one system renders the other obsolete. Rather, they indicate that the two approaches reflect partly distinct aspects of lesion assessment.
A notable finding of this study is the information efficiency demonstrated by the MelAInoma algorithm. While the expert graders assigned MOLES scores with the benefit of multimodal imaging—including OCT for subretinal fluid and autofluorescence for orange pigment—the AI algorithm achieved a higher point estimate for AUC using only a single color fundus photograph. This suggests that the deep learning model captures diagnostic features from standard photography that are at least as predictive of treatment-requirement as the high-resolution features identified by experts using specialized equipment. In primary care or optometric settings where OCT and AF are often unavailable, this ability to provide high-level risk stratification from a simple photo represents a significant clinical advantage.
An additional practical distinction between the systems is that MelAInoma provides fully reproducible output, yielding the same score each time a given image is analyzed, independent of the user. In contrast, MOLES scoring is subject to human interpretation. In the present study, all MOLES scores were assigned by experienced ocular oncologists, effectively establishing a performance ceiling for the manual scoring system. Because previous research has shown that MOLES performance can vary significantly based on observer expertise, it is probable that the diagnostic gap between the two systems would be even more pronounced in the primary care settings for which they are intended, where the AI’s consistency would remain stable while manual scoring accuracy might decline.[5,6]
Another conceptual difference is that MelAInoma does not explicitly base its classification on predefined clinical risk factors for growth. Although such factors are well established and clinically useful, they do not necessarily reflect underlying tumor biology, including genetic and cytogenetic alterations known to be associated with prognosis.[13,14] Whether image-based AI systems such as MelAInoma capture information related to these biological features remains an open question. Future work should therefore evaluate how MelAInoma scores relate to genetic and cytogenetic markers, such as monosomy 3 and BAP1 mutation status, and aim to identify new image-derived risk features that more accurately reflect tumor biology.[15,16]
4.1. Strengths and Limitations
This study has several limitations. First, it was based on a relatively small cohort from a single national referral center. Although images were acquired using both standard-field and ultra-widefield cameras, patients from Sweden may not be representative of other populations,[17,18] limiting generalizability. Second, genetic and cytogenetic data were not available, precluding analysis of associations with established molecular prognostic factors. Third, both diagnoses and MOLES scores were established by subspecialized ocular oncologists. Results may therefore differ if diagnoses and scoring were performed by non-experts, a scenario that would likely disadvantage MOLES more than MelAInoma. Since the same expert group assigned MOLES scores and established diagnoses, some degree of bias toward stronger associations between MOLES and diagnosis cannot be excluded. Specifically, the high level of clinical expertise in this study may have inadvertently compensated for the inherent subjectivity of the manual MOLES criteria, a factor that might not be present in a real-world triage environment. Fourth, there was an asymmetry in the data available to each system; while MOLES scoring was supported by multimodal imaging, MelAInoma was restricted to color fundus photography. Consequently, this study could not evaluate whether the addition of OCT or autofluorescence data would further enhance the algorithm's performance. Furthermore, while the current results demonstrate the AI's efficacy as a standalone triage tool, its integration with other clinical data remains a subject for future investigation.
The study also has several strengths. The cohort was independent of the datasets used to develop and train the MelAInoma algorithm. Diagnoses were established using multimodal expert assessment, including ultrasonography, OCT, biomicroscopy, and fundus imaging. In addition, classification of lesions as nevi required at least five years of follow-up without reclassification as melanoma, increasing confidence in the correctness of the ground truth diagnoses.
5. Conclusions
Both MOLES and MelAInoma are useful tools for differentiating small choroidal melanomas from nevi. The two systems are statistically associated and both are linked to the odds of melanoma diagnosis. MelAInoma offers practical advantages related to reproducibility and demonstrated slightly stronger associations with melanoma diagnosis in this cohort. These findings support the potential role of MelAInoma as a complementary aid in the assessment and triage of pigmented choroidal lesions.
Author Contributions
Conceptualization, G.S. and M.H.; methodology, G.S. and M.H.; software, G.S and M.H.; validation, K.S., H.C.A., M.H.; formal analysis, G.S.; investigation, G.S. and M.H.; resources, G.S.; data curation, G.S.; writing—original draft preparation, G.S.; writing—review and editing, K.S., H.C.A., and M.H.; visualization, G.S.; supervision, G.S.; project administration, G.S.; funding acquisition, G.S. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: This research was funded by Karolinska Institutet, grant number 2023-02622.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Swedish Ethical Review Authority (reference 2025-05054-01, date of approval September 3, 2025).
Informed Consent Statement
Patient consent was waived as this was a retrospective study that does not affect the treatment or follow-up of the patients. Further, all patient data and images had been previously collected and no new clinical data collection was performed, and no biological tissues were analyzed.
Data Availability Statement
Due to the sensitive nature of the clinical data, including images utilized in this study, the authors are unable to share these materials in compliance with Swedish law. The con dentiality and privacy regulations governing patient information strictly prohibit the distribution of such data.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (version 5.2 for the purpose of improving grammar and language. The authors have reviewed and edited the output and take full responsibility for the content of this publication.”.
Conflicts of Interest
Mats Holmström and Gustav Stålhammar are founders of Eyedentity AB and hold equity in the company, which develops the MelAInoma software evaluated in this study.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial intelligence |
| AIC | Akaike information criterion |
| AJCC | American Joint Committee on Cancer |
| AMD | Age-related macular degeneration |
| AUC | Area under the curve |
| CI | Confidence interval |
| MOLES | Mushroom shape, Orange pigment, Large size, Enlarging tumor, and Subretinal fluid |
| OCT | Optical Coherence Tomography |
| OR | Odds ratio |
| LBD | Largest basal tumor diameter |
| SD | Standard deviation |
References
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of Uveal Melanoma Millimeter-by-Millimeter in 8033 Consecutive Eyes. Archives of Ophthalmology 2009, 127, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Stalhammar, G.; Coupland, S.E.; Ewens, K.G.; Ganguly, A.; Heimann, H.; Shields, C.L.; Damato, B. Improved Staging of Ciliary Body and Choroidal Melanomas Based on Estimation of Tumor Volume and Competing Risk Analyses. Ophthalmology 2023, 131, 478–491. [Google Scholar] [CrossRef] [PubMed]
- Sumich, P.; Mitchell, P.; Wang, J.J. Choroidal nevi in a white population: the Blue Mountains Eye Study. Arch Ophthalmol 1998, 116, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, M.B.; Myers, C.E.; Meuer, S.M.; Klein, B.E.; Cotch, M.F.; Wong, T.Y.; Klein, R. Prevalence and characteristics of choroidal nevi: the multi-ethnic study of atherosclerosis. Ophthalmology 2011, 118, 2468–2473. [Google Scholar] [CrossRef] [PubMed]
- Sabazade, S.; Lumia Michalski, M.A.; Wittskog, S.; Holmstrom, M.; Nilsson, M.; Stalhammar, G. Challenges for Opticians in Evaluating Small Pigmented Choroidal Lesions: Potential Support From the MelAInoma Deep Learning Algorithm. Transl Vis Sci Technol 2025, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Sabazade, S.; Lumia Michalski, M.; Bartoszek, J.; Fili, M.; Holmström, M.; Stålhammar, G. Development and Validation of a Deep Learning Algorithm for Differentiation of Choroidal Nevi from Small Melanoma in Fundus Photographs. Ophthalmology Science 2024, 4. [Google Scholar] [CrossRef] [PubMed]
- Al Harby, L.; Sagoo, M.S.; O’Day, R.; Hay, G.; Arora, A.K.; Keane, P.A.; Cohen, V.M.L.; Damato, B. Distinguishing Choroidal Nevi from Melanomas Using the MOLES Algorithm: Evaluation in an Ocular Nevus Clinic. Ocular Oncology and Pathology 2021. [Google Scholar] [CrossRef] [PubMed]
- Roelofs, K.A.; O'Day, R.; Harby, L.A.; Arora, A.K.; Cohen, V.M.L.; Sagoo, M.S.; Damato, B. The MOLES System for Planning Management of Melanocytic Choroidal Tumors: Is It Safe? Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Shields, J.A.; Kiratli, H.; De Potter, P.; Cater, J.R. Risk factors for growth and metastasis of small choroidal melanocytic lesions. Trans Am Ophthalmol Soc 1995, 93, 259–275; discussion 275–259. [Google Scholar] [CrossRef]
- Shields, C.L.; Furuta, M.; Berman, E.L.; Zahler, J.D.; Hoberman, D.M.; Dinh, D.H.; Mashayekhi, A.; Shields, J.A. Choroidal nevus transformation into melanoma: analysis of 2514 consecutive cases. Arch Ophthalmol 2009, 127, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Cater, J.; Shields, J.A.; Singh, A.D.; Santos, M.C.; Carvalho, C. Combination of clinical factors predictive of growth of small choroidal melanocytic tumors. Arch Ophthalmol 2000, 118, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Stalhammar, G.; Hagstrom, A.; Ermedahl Conradi, M.; Williams, P.A. Choroidal nevi and melanoma doubling times and implications for delays in treatment: A systematic review and meta-analysis. Surv Ophthalmol 2025, 70, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Stalhammar, G.; Kalirai, H.; Coupland, S.E.; Grisanti, S.; Sonntag, S.R.; Tura, A.; Eleuteri, A.; Hussain, R.N.; Heimann, H.; Coude Adam, H. Metastatic potential of small posterior uveal melanomas. Acta Ophthalmol 2025. [Google Scholar] [CrossRef] [PubMed]
- Stalhammar, G. A Word of Caution regarding Risk Factors for Malignant Transformation of Choroidal Nevi. Ocul Oncol Pathol 2021, 7, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Harbour, J.W.; Onken, M.D.; Roberson, E.D.; Duan, S.; Cao, L.; Worley, L.A.; Council, M.L.; Matatall, K.A.; Helms, C.; Bowcock, A.M. Frequent mutation of BAP1 in metastasizing uveal melanomas. Science 2010, 330, 1410–1413. [Google Scholar] [CrossRef] [PubMed]
- Prescher, G.; Bornfeld, N.; Hirche, H.; Horsthemke, B.; Jockel, K.H.; Becher, R. Prognostic implications of monosomy 3 in uveal melanoma. Lancet 1996, 347, 1222–1225. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Yavuzyigitoglu, S.; Brosens, E.; Ramdas, W.D.; Kilic, E.; Rotterdam Ocular Melanoma Study, G. Worldwide Incidence of Ocular Melanoma and Correlation With Pigmentation-Related Risk Factors. Invest Ophthalmol Vis Sci 2023, 64, 45. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.N.; Yu, G.P.; McCormick, S.A.; Schneider, S.; Finger, P.T. Population-based incidence of uveal melanoma in various races and ethnic groups. Am J Ophthalmol 2005, 140, 612–617. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Distribution of MOLES and MelAInoma scores. Each point represents one lesion. (A) Distribution of MOLES scores across the included lesions, shown with horizontal jitter to reduce overlap. The horizontal line indicates the mean, and whiskers indicate the standard deviation (SD). (B) Distribution of MelAInoma scores across the included lesions. (C) Distribution of MelAInoma scores stratified by MOLES score (0, 1, 2, 3, and ≥4).
Figure 1.
Distribution of MOLES and MelAInoma scores. Each point represents one lesion. (A) Distribution of MOLES scores across the included lesions, shown with horizontal jitter to reduce overlap. The horizontal line indicates the mean, and whiskers indicate the standard deviation (SD). (B) Distribution of MelAInoma scores across the included lesions. (C) Distribution of MelAInoma scores stratified by MOLES score (0, 1, 2, 3, and ≥4).
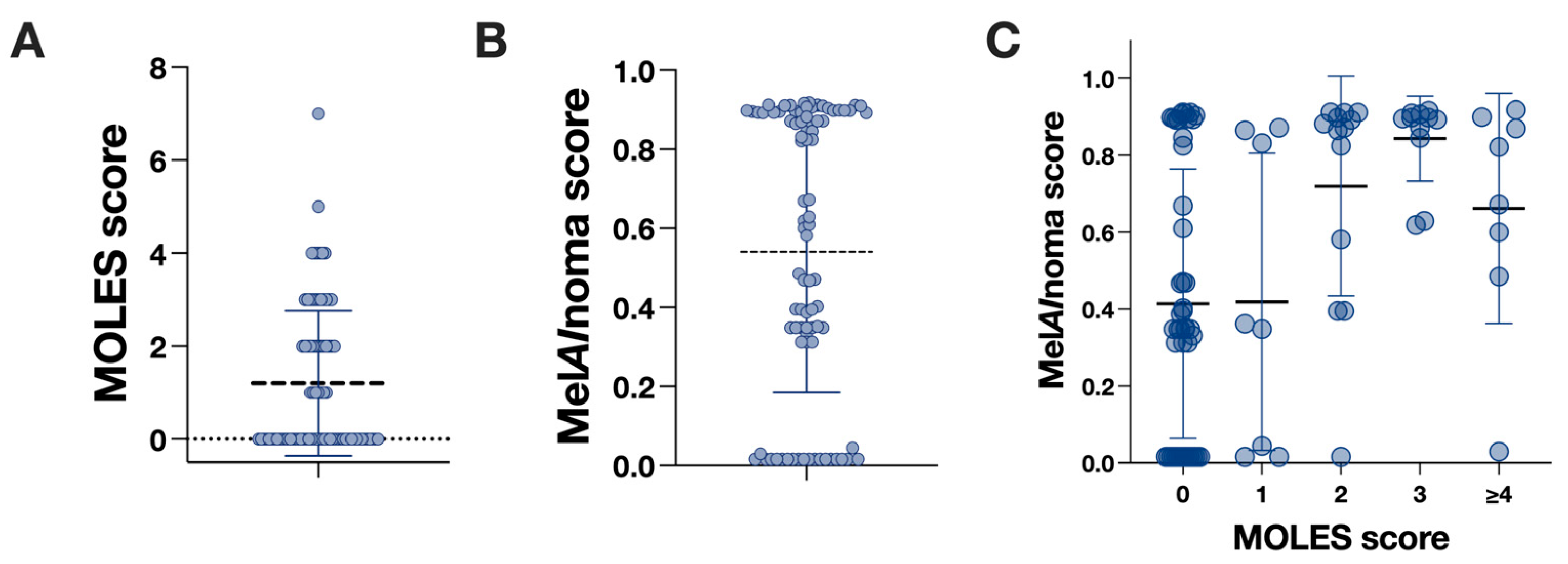
Figure 2.
Association between MOLES score and MelAInoma score. Scatter plot showing MelAInoma score as a function of MOLES score. The solid line represents the fitted linear regression (slope 0.09 per MOLES unit; P<0.0001), and the shaded area indicates the 95% confidence interval (CI).
Figure 2.
Association between MOLES score and MelAInoma score. Scatter plot showing MelAInoma score as a function of MOLES score. The solid line represents the fitted linear regression (slope 0.09 per MOLES unit; P<0.0001), and the shaded area indicates the 95% confidence interval (CI).
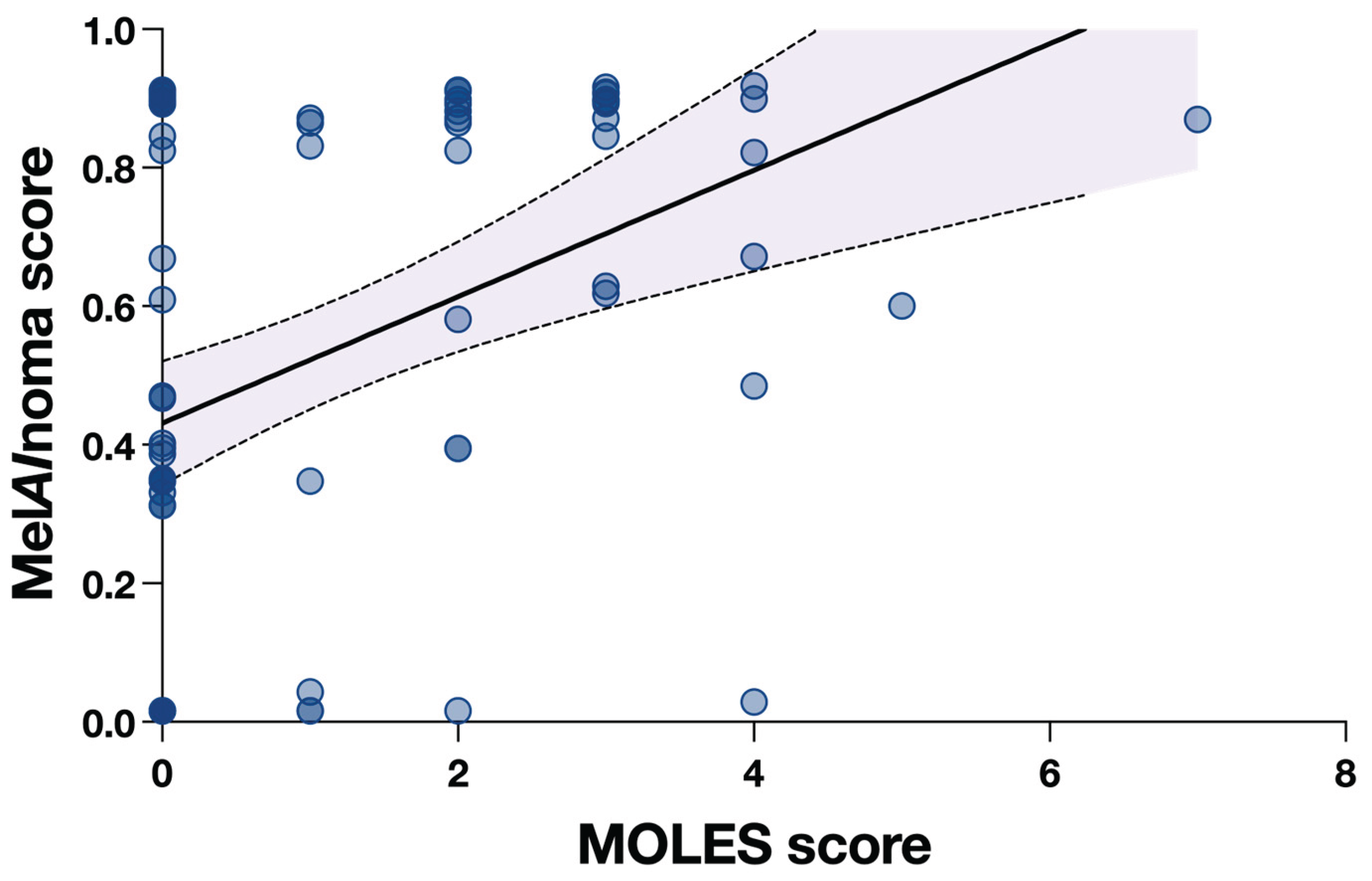
Figure 3.
Binary logistic regression models. (A) Predicted probability of melanoma as a function of MOLES score from a binary logistic regression model. (B) Predicted probability of melanoma as a function of MelAInoma score from a binary logistic regression model. In both panels, the solid line represents the fitted model, and the shaded area indicates the 95% confidence interval (CI).
Figure 3.
Binary logistic regression models. (A) Predicted probability of melanoma as a function of MOLES score from a binary logistic regression model. (B) Predicted probability of melanoma as a function of MelAInoma score from a binary logistic regression model. In both panels, the solid line represents the fitted model, and the shaded area indicates the 95% confidence interval (CI).
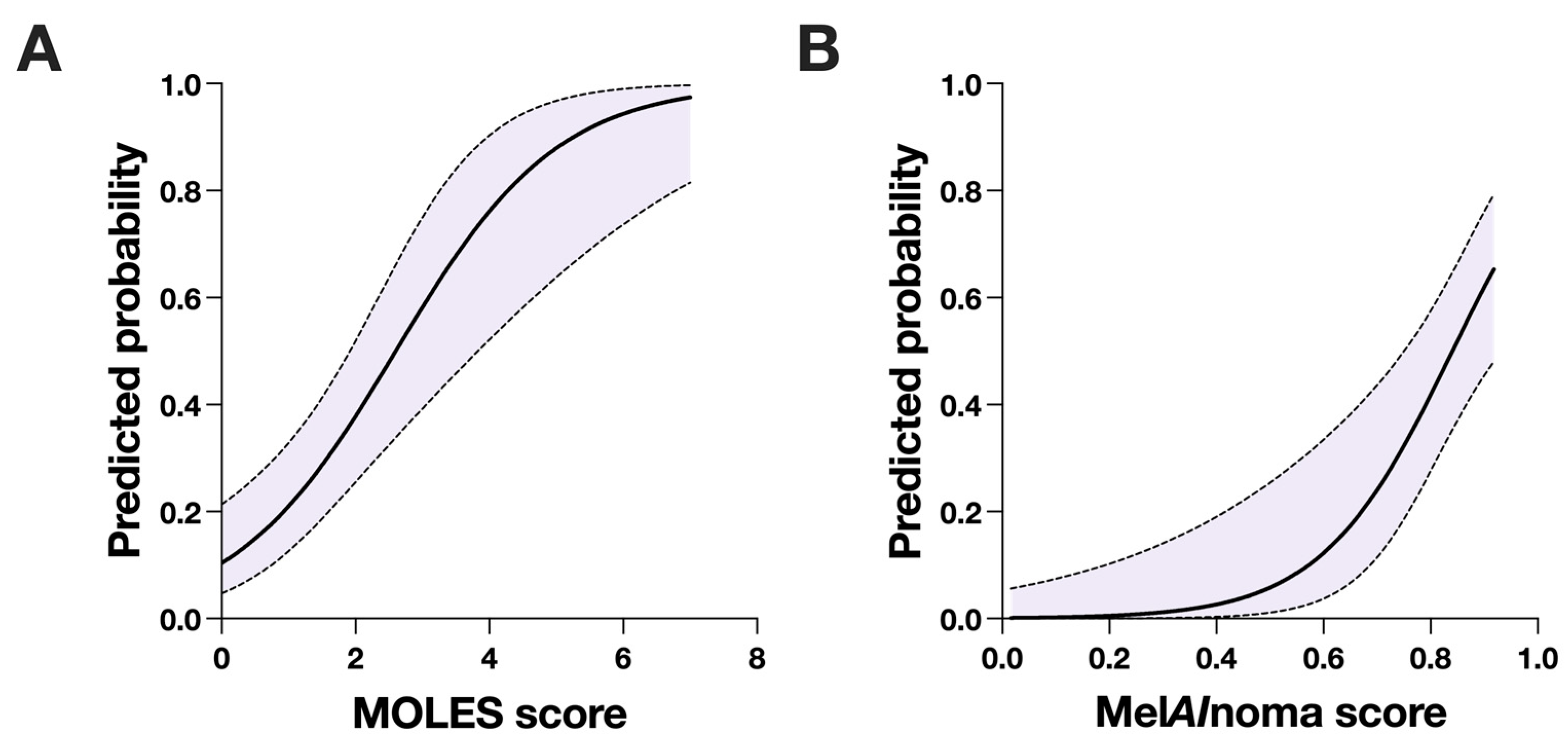

Table 1.
Characteristics of included patients and lesions.
| nimages | 86 |
| nunique patients | 86 |
| Sex,n(%) | |
| Male | 38 (44) |
| Female | 48 (56) |
| Age, mean years (SD) | 58 (14) |
| Fundus photography type,n(%) | |
| Wide field | 31 (36) |
| Standard field | 55 (64) |
| Nevi,n(%) | 57 (66) |
| Melanomas,n(%) | 29 (34) |
| Nevus LBD, mean mm (SD) | 4.4 (1.6) |
| Nevus thickness, mean mm (SD) | 1.6 (0.4) |
| Melanoma LBD, mean mm (SD) | 6.6 (2.1) |
| Melanoma thickness, mean mm (SD) | 2.8 (1.5) |
| Mean MOLES score (SD) | |
| Overall | 1.6 (2.2) |
| For nevi | 0.7 (1.2) |
| For melanomas | 3.9 (2.4) |
| LBD, largest basal diameter. SD, standard deviation. MOLES assigns a score of 0, 1, or 2 for Mushroom shape, Orange pigment, Large size, Enlarging tumor, and Subretinal fluid, based on their absence, borderline presence, or presence. Lesions are classified as common nevi, low-risk nevi, high-risk nevi, or probable melanoma, based on their total score being 0, 1, 2, or more than 2, respectively, as described by Roelofs et al. 2020. | |
Table 2.
Univariable binary logistic regression for MOLES score and melanoma diagnosis.
| Predictor | Scale | OR | 95% CI | P |
| MOLES score | Per 1-unit increase | 2.29 | 1.59 to 3.50 | <0.0001 |
Binary logistic regression with true diagnosis as outcome. CI, confidence interval. OR, odds ratio.
Table 3.
Univariable binary logistic regression for MelAInoma score and melanoma diagnosis.
| Predictor | Scale | OR | 95% CI | P |
| MelAInoma score | Per 0.1 increase | 2.27 | 1.57 to 4.23 | <0.0001 |
Binary logistic regression with true diagnosis as outcome. CI, confidence interval. OR, odds ratio.
Table 4.
Multivariable binary logistic regression for melanoma diagnosis.
| Predictor | Scale | OR | 95% CI | P |
| MelAInoma score | Per 0.1 increase | 2.82 | 1.62 to 6.85 | <0.0001 |
| MOLES score | Per 1-unit increase | 2.24 | 1.40 to 4.02 | 0.002 |
Binary logistic regression including both MOLES score and MelAInoma score as predictors. No interaction terms or variable transformations were included. CI, confidence interval. OR, odds ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



