1. Introduction
Deep neuromuscular relaxation is an essential component of modern general anesthesia, particularly in laparoscopic, robotic, and complex abdominal procedures. Adequate muscle relaxation improves surgical conditions, reduces intra-abdominal pressure, and may decrease postoperative pain and perioperative complications.
Magnesium sulfate has long been used in clinical medicine, most notably in obstetrics and cardiology. In anaesthesiology, magnesium exerts multiple effects relevant to perioperative management, including analgesia, attenuation of sympathetic responses, and modulation of neuromuscular transmission. By blocking voltage-gated calcium channels, magnesium reduces presynaptic acetylcholine release at the neuromuscular junction and enhances the effect of non-depolarizing neuromuscular blocking agents.
Despite accumulating evidence, the clinical significance of magnesium sulfate as an adjuvant to neuromuscular blockers remains a topic of debate, with heterogeneous results reported across studies. The present review summarizes and critically analyzes available clinical evidence regarding the effects of magnesium sulfate on neuromuscular blockade and its potential role in contemporary anaesthetic practice.
2. Materials and Methods
This review included clinical studies investigating the muscle-relaxant effects of intravenous magnesium sulfate in adult patients undergoing general anesthesia. The literature search covered publications from 1978 to 2025 and was conducted using PubMed and DeepDyve databases.
Search terms included magnesium sulfate, neuromuscular block, anesthesia, onset, duration, recovery, reversal, and rapid sequence induction.
Eligible studies comprised randomized controlled trials, systematic reviews with meta-analyses, and retrospective cohort studies evaluating the interaction between magnesium sulfate and depolarizing or non-depolarizing neuromuscular blocking agents. Analyzed outcomes included the onset and duration of neuromuscular blockade, recovery characteristics, intubation conditions, required relaxant doses, adverse effects, and hemodynamic parameters.
3. Results
As early as 1978, Evron S. et al. published a study investigating the effect of magnesium sulfate administration in the treatment of eclampsia and its influence on neuromuscular relaxants used during general anesthesia [
1]. This was one of the first reports suggesting that magnesium may prolong the action of non-depolarizing muscle blockers. In this historical context, researchers proposed that magnesium affects neuromuscular function and subsequently investigated this effect more thoroughly.
3.1. Effect on Depolarizing Neuromuscular Blockers
Several clinical investigations have examined the interaction of MgSO₄ with the depolarizing relaxant succinylcholine.
James MF, Cork RC, and Dennett JE demonstrated in a RCT that magnesium, administered prior to the neuromuscular blocker, did not alter the main characteristics of paralysis, but significantly attenuated the increase in serum potassium levels (
p < 0.01)[
2].
Stacey MR et al. evaluated the effect of magnesium sulfate on succinylcholine-related complications during rapid sequence induction (RSI). They reported a clear reduction in the incidence of fasciculations in the magnesium group, while serum potassium levels and the occurrence of postoperative myalgia remained comparable between groups [
3].
Kumar M et al. investigated pretreatment with magnesium sulfate (40 mg/kg) combined with propofol for induction of anesthesia. In contrast to previous findings, their results revealed a clinically meaningful decrease in both the frequency and severity of fasciculations (
p < 0.001) as well as postoperative myalgia (
p < 0.002) in the magnesium group [
4].
3.2. Effect of Magnesium Sulfate Pretreatment on the Onset of NMB
A significant proportion of the RCTs investigated the effect of pre-administration of MgSO
4 on the onset of NMB induced by various non-depolarizing muscle relaxants. James MF, Schenk PA and van der Veen BW found that pretreatment with MgSO
4 did not lead to a clinically significant change in the onset of action of pancuronium, nor improved intubation conditions [
5].
Similarly, Kussman B et al. reported that MgSO
4 did not substantially speed the onset of NMB induced by rocuronium [
6].
All other RCTs, however, demonstrated a faster onset of NMB induced by various non-depolarizing muscle relaxants after pretreatment with MgSO
4. Fuchs-Buder T, Wilder-Smith OH, Borgeat A and Tassonyi E observed a more rapid onset of vecuronium-induced NMB after MgSO
4 administration [
7].
Wu HL et al. demonstrated that the time to reach maximal NMB after atracurium administration was significantly shorter in the magnesium group compared to control (
p < 0.01) [
8].
Only a year later, Czarnetzki et al. confirmed that pretreatment with MgSO₄ significantly accelerated the onset of rocuronium-induced neuromuscular blockade (by approximately 35%) and reduced variability in onset time [
9].
Subsequent studies reported similar results. Rotava et al. concluded that, in oncology patients older than 60 years, pretreatment with MgSO₄ significantly reduced the onset time of rocuronium-induced neuromuscular blockade [
10].
Sun H et al. confirmed these findings in their RCT [
11].
3.3. Effect of Magnesium Sulfate on the Duration of Neuromuscular Blockade
With respect to the duration of NMB, data from the RCTs are inconsistent. The majority of them demonstrated prolongation after pretreatment with MgSO₄ [
1,
6,
7,
8,
9,
11], whereas only three studies did not find an increased duration [
3,
4,
12].
According to Fuchs-Buder T, Wilder-Smith OH, Borgeat A and Tassonyi E, the duration of vecuronium-induced NMB was nearly doubled (43.3 min vs 25.2 min) with MgSO
4 pretreatment [
7].
Queiroz Rangel Micuci AJ et al. found that MgSO
4 increased both the duration of intense NMB (TOF = 0, PTC = 0) and the period of no response, but the duration of deep NMB (TOF = 0, PTC ≥ 1) was similar in both groups [
13].
3.4. Recovery and Reversal of Neuromuscular Block
Regarding recovery from NMB, half of the studies examining this measure reported prolonged recovery time [
7,
8,
9,
14].
Fuchs-Buder T, Wilder-Smith OH, Borgeat A, Tassonyi E [
7] and Wu HL et al. [
8] found that magnesium sulfate significantly extended the recovery period compared with the control groups.
Czarnetzki C et al. demonstrated that MgSO
4 prolonged the overall time to reversal of the block by about 25%. The average recovery duration was 73.2 min with MgSO
4 vs 57.8 min with placebo (
p = 0.003) [
9].
Fuchs-Buder, Ziegenfuss, Lysakowski, and Tassonyi showed that neostigmine antagonism (0.02 mg/kg) proceeded more slowly in patients pretreated with MgSO₄. After 5 minutes, T1 recovery reached 43% in the MgSO₄ group compared with 66% in controls, and after 10 minutes, 60% versus 83% (p < 0.01). The TOF ratio likewise demonstrated more delayed reversal in the MgSO₄ group. Patients in the MgSO₄ group also exhibited significantly slower spontaneous recovery than controls, with T1 values of 21% versus 38% after 5 minutes and 35% versus 61% after 10 minutes (p < 0.01). Although the maximum assisted recovery between minutes 6 and 10 was similar in both groups, recovery during the first 5 minutes progressed more slowly in the MgSO₄ group. The authors attributed this finding to delayed spontaneous recovery rather than to a reduced effect of neostigmine [
14].
Other RCTs did not observe significant differences between the two groups in recovery time or recovery indices (RI) [
5,
10,
11,
15].
3.5. Intubation Conditions
Some of the studies examined intubation conditions after pretreatment with MgSO4.
James MF, Schenk PA and van der Veen BW found no improvement in intubation conditions when magnesium sulfate preceded pancuronium administration [
5].
Fuchs-Buder T, Wilder-Smith OH, Borgeat A and Tassonyi E found that pretreatment with MgSO
4 improved intubation conditions with vecuronium, making them comparable to those with succinylcholine [
7].
In a clinical study, Kim MH et al. allocated ninety-two patients undergoing general anesthesia to four groups: a control group, a rocuronium priming group (0.06 mg/kg + 0.54 mg/kg), a magnesium pretreatment group (50 mg/kg), and a combined magnesium and rocuronium-priming group. The authors reported that the combination of magnesium sulfate and rocuronium priming provided the best conditions for tracheal intubation compared with the other groups [
12].
Sun H et al. concluded that magnesium sulfate, used as an adjuvant to rocuronium, improved intubation conditions without requiring an increased relaxant dose [
11].
Paul G et al. conducted a double-blind RCT comparing the onset time of paralysis and intubation conditions in three different approaches for RSI: succinylcholine (1 mg/kg), rocuronium (0.9 mg/kg), and rocuronium with prior magnesium sulfate (60 mg/kg). The authors demonstrated that the rocuronium–magnesium combination provided excellent intubation conditions in all patients in that group [
16].
3.6. Dose-Sparing Effect
A limited number of studies have investigated the effect of MgSO₄ administration on the dose of non-depolarizing muscle relaxants.
Fuchs-Buder, Wilder-Smith, Borgeat, and Tassonyi demonstrated that magnesium sulfate reduced the effective doses (ED₅₀ and ED₉₀) of vecuronium by approximately 25% compared with the control group [
7].
Han J et al. conducted an RCT examining the influence of magnesium on the dose of rocuronium required for deep NMB during robot-assisted laparoscopic prostatectomy. They showed that magnesium reduced the dose of rocuronium needed for deep muscle relaxation by approximately 20%, without affecting the recovery time after sugammadex administration [
15].
3.7. Rapid Sequence Induction
Clinical studies have also explored the role of magnesium in RSI.
Czarnetzki C et al. published an RCT investigating the effects of MgSO
4 pretreatment on the onset and recovery of rocuronium-induced neuromuscular block during propofol anesthesia. The results showed that MgSO
4 reduced the onset time of NMB by about 35% (77 s with MgSO
4 vs 120 s with placebo;
p < 0.001). According to the authors, this combination could be a promising alternative to succinylcholine for RSI, offering a shorter and more predictable onset of relaxation. However, they emphasized the need for additional clinical studies to evaluate its practical application and to establish safe limits and optimal dosing for the co-administration of magnesium with muscle relaxants, thereby minimizing unnecessary risk [
9].
Kim MH et al. examined whether a combination of magnesium sulfate and rocuronium priming could accelerate NMB onset during RSI compared to the use of each method alone. The results demonstrated that the combination of magnesium sulfate and rocuronium priming produced the shortest onset time (55 s) and the best conditions for tracheal intubation compared to the other groups [
12].
Ghodraty MR et al. conducted an RCT examining the effects of magnesium on neuromuscular relaxation with cisatracurium during induction of anesthesia. The authors investigated whether magnesium as an adjuvant speeds the onset of muscle relaxation, thereby reducing the risk of aspiration. However, they concluded that the magnesium-shortened onset time was not significant enough to justify its use in combination with cisatracurium for RSI [
17].
Czarnetzki C et al. in a double-blind RCT compared the effect of administering magnesium sulfate before rocuronium versus succinylcholine for RSI. Their data analysis showed no superiority of the magnesium–rocuronium combination over succinylcholine in terms of providing excellent intubation conditions (46% vs 45%). However, the magnesium–rocuronium group had fewer undesirable effects (11% vs 28%). Interestingly, the study noted a higher percentage of excellent intubation conditions in women, especially in those receiving magnesium–rocuronium. Although this combination did not provide better intubation conditions, it may be an appropriate alternative in situations when succinylcholine is contraindicated. According to the authors, this study provides important information for anaesthesiologists, expanding the options for RSI and highlighting the potential safety advantages of the magnesium–rocuronium combination for patients [
18].
Paul G et al. conducted a double blind RCT comparing the onset time of paralysis and intubation conditions in three different RSI approaches: succinylcholine (1 mg/kg), rocuronium (0.9 mg/kg), and rocuronium with prior magnesium sulfate (60 mg/kg). Succinylcholine exhibited the fastest action – on average 65 seconds. Rocuronium with magnesium acted significantly faster (82 seconds) than rocuronium alone (102 seconds). The rocuronium–magnesium combination provided excellent intubation conditions for all patients in this group. Succinylcholine produced the most rapid onset, but the rocuronium–magnesium combination provided better intubation conditions and stable hemodynamics [
16].
3.8. Without Muscle Relaxant
Aissaoui Y et al. published the results of a double-blind RCT titled “Magnesium sulfate: an adjuvant to tracheal intubation without muscle relaxant,” conducted in 60 patients. Before induction of anesthesia with propofol and fentanyl, patients received either 45 mg/kg MgSO
4 in 100 mL saline (Mg group, n = 30) or the same volume of plain saline (control group, n = 30). Intubation conditions were assessed by an anaesthesiologist using the Copenhagen Consensus Conference criteria: ease of laryngoscopy, vocal cord position, and response to intubation or cuff inflation (cough or diaphragmatic movement). Intubation conditions were defined as acceptable (excellent or good) or unacceptable (poor). Clinically acceptable intubation conditions were observed more often in the Mg group compared to control: 25 patients (83%) vs 18 patients (60%) (
p = 0.042). There were no failed intubations. According to the authors, this finding is remarkable since it creates the possibility for “relaxant-free” anesthesia in certain cases by using magnesium to achieve the needed intubation conditions [
19].
3.9. Safety and Hemodynamic Effects
None of the clinical studies reported any serious complications following the administration of MgSO
4 at the doses used (30 to 60 mg/kg). Reports included hot flushes [
7,
12], pain at the injection site, and a single case of bradycardia [
16].
With respect to hemodynamics, the studies reported similar parameters between groups, and only one study noted a suppression of the hemodynamic response to laryngoscopy after MgSO
4 administration [
16].
3.10. Meta-Analysis
Sun H et al. conducted a meta-analysis investigating the efficacy of MgSO4 as an adjuvant to rocuronium in general anesthesia. The aim was to clarify the effects of MgSO4 administration on neuromuscular block parameters and intubation conditions. The authors conducted a systematic review of RCTs using multiple databases up to May 2020. Eleven RCTs with 460 patients were included. The results demonstrated that MgSO4 significantly accelerates the onset and prolongs the clinical duration of rocuronium-induced NMB. The study found no significant difference in the recovery index of neuromuscular blockade between the magnesium and control groups. MgSO4 improves intubation conditions, increasing the percentage of excellent and clinically acceptable conditions. The conclusion is that MgSO4 as an adjuvant to rocuronium can improve NMB and intubation conditions without requiring an increased relaxant dose. However, the authors emphasized that clinical heterogeneity and limited evidence quality require cautious interpretation of the results [
11].
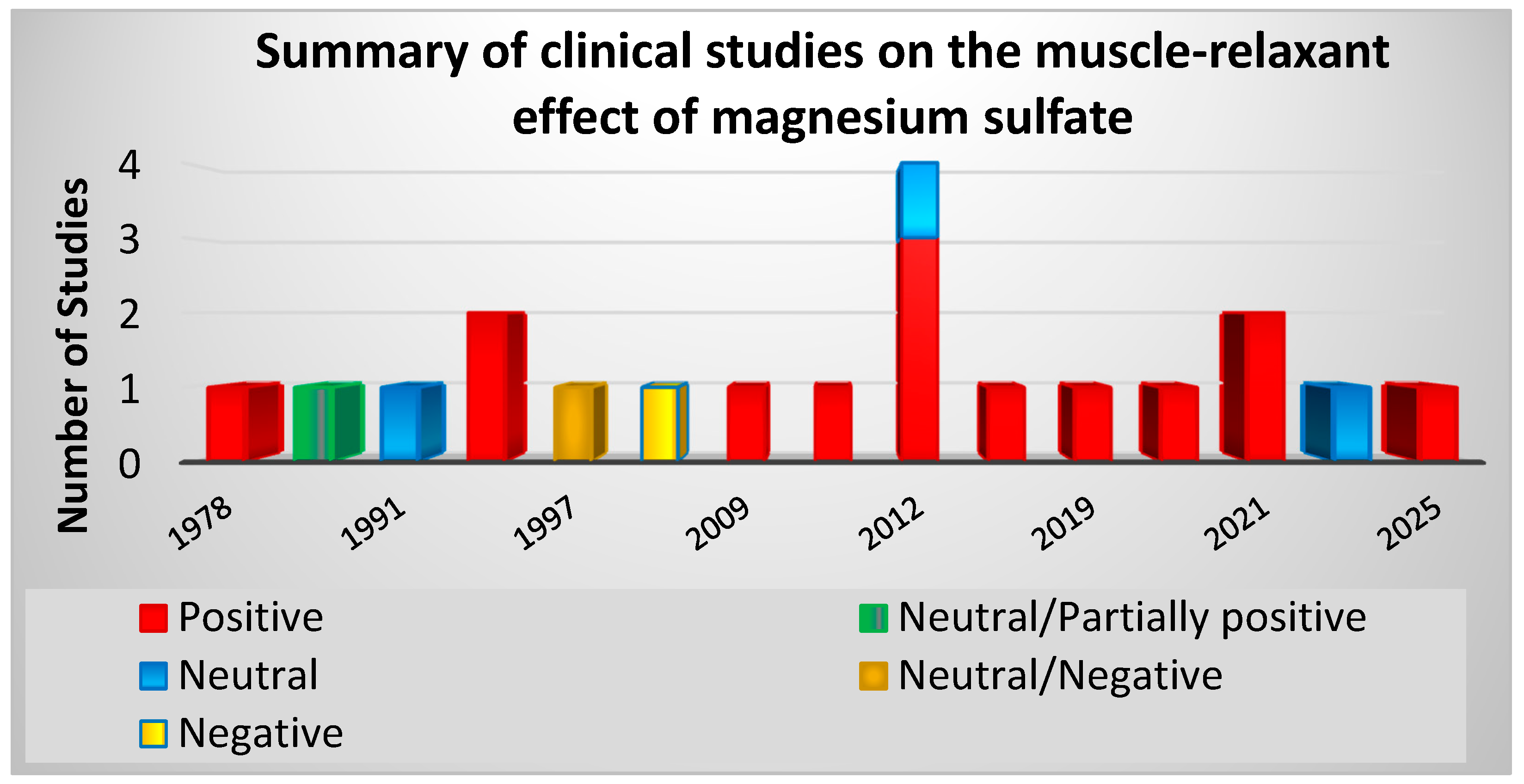
Figure 1 and
Table 1 summarize the evidence from the clinical studies.
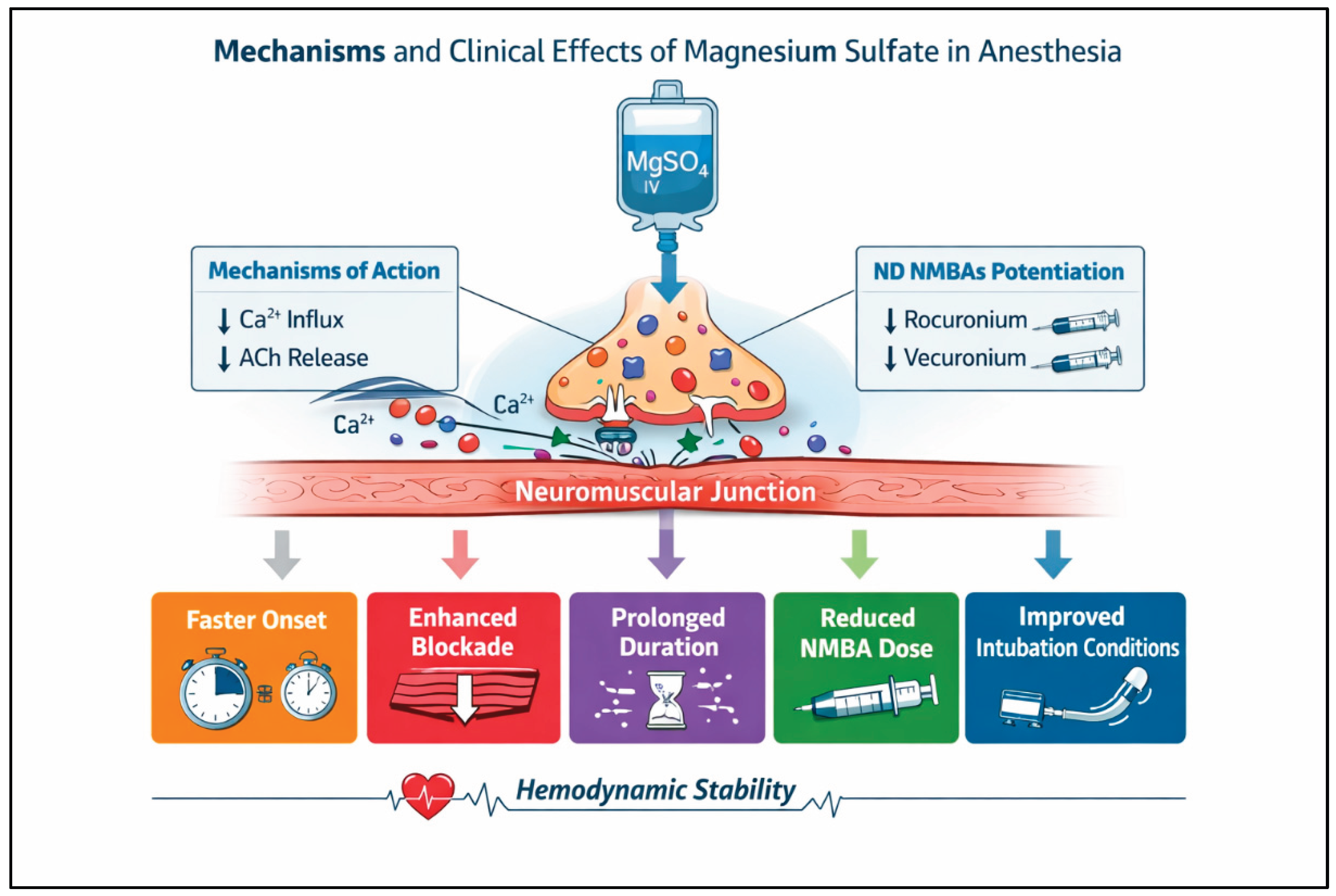
Table 2 and
Figure 2 illustrate the main clinical effects of magnesium sulfate.
4. Discussion
Studies conducted from 1978 to the present have examined the interaction of MgSO₄ with succinylcholine and with the non-depolarizing neuromuscular blockers pancuronium, vecuronium, atracurium, cisatracurium, and rocuronium. These studies analyzed the effects of magnesium pretreatment on fasciculations, postoperative myalgia, serum potassium levels, neuromuscular blockade onset, duration of muscle relaxation and recovery, intubation conditions, and relaxant dose requirements.
Across the analyzed randomized controlled trials, magnesium sulfate was predominantly administered as a single intravenous bolus prior to neuromuscular blocker administration. Continuous infusion was used only in the studies by Rotava P et al. [
10] and Han et al. [
15].
Several studies have explored the use of MgSO₄ in combination with neuromuscular blockers to accelerate the onset of relaxation during rapid sequence induction. Some randomized controlled trials also evaluated potential complications and hemodynamic effects. Although the results across studies are mixed, the majority demonstrate that MgSO₄ shortens the time to onset, prolongs the clinical duration of neuromuscular blockade, improves intubation conditions, and reduces the required doses of neuromuscular blocking agents.
The combination of magnesium and non-depolarizing neuromuscular blockers may serve as an alternative to succinylcholine for RSI. When administered before succinylcholine, MgSO₄ may also reduce the incidence of fasciculations, postoperative myalgia, and elevations in serum potassium levels.
Nearly half of the randomized controlled trials investigating recovery from neuromuscular blockade reported no significant differences in the recovery index between magnesium and control groups. The clinical studies described only minor adverse effects at the administered doses (30–60 mg/kg), including a transient sensation of warmth, injection site discomfort, and a single reported case of bradycardia. No clinically significant changes in hemodynamic parameters were observed. Only one study reported attenuation of the hemodynamic response to laryngoscopy following MgSO₄ administration.
Nevertheless, clinical heterogeneity and the limited quality of evidence warrant cautious interpretation of these findings. Additional high-quality, large-scale randomized controlled trials are required to confirm the observed effects. Although available data indicate no evidence of harm associated with clinically used doses of MgSO₄, long-term safety data remain limited. Most randomized controlled trials highlight the potential benefits of magnesium use in anesthesia while also emphasizing the need for more robust evidence to clarify unresolved issues. Safe clinical application requires strict quantitative neuromuscular monitoring and appropriate dose adjustment of neuromuscular blocking agents.
Overall, the analyzed evidence supports the role of magnesium sulfate as an effective adjuvant in anesthesia, particularly for enhancing non-depolarizing neuromuscular blockade. Its ability to accelerate onset, prolong block duration, and improve intubation conditions is clinically relevant in the context of modern surgical techniques. The observed delay in recovery further underscores the importance of quantitative neuromuscular monitoring when magnesium is incorporated into anaesthetic practice.
Despite the promising evidence, heterogeneity among study designs, dosing regimens and outcome measures limits direct comparisons across trials. Well-designed, large-scale randomized controlled studies are needed to establish standardized protocols and to define optimal dosing strategies for magnesium sulfate in anesthesia.
5. Practical Clinical Implications
The available clinical evidence indicates that intravenous magnesium sulfate can be effectively integrated into contemporary anaesthetic practice as an adjuvant to neuromuscular blocking agents. Its administration before induction of anesthesia may accelerate the onset and enhance the depth of neuromuscular blockade. This effect is clinically relevant in settings requiring rapid and reliable muscle relaxation, including rapid sequence induction, laparoscopic, robotic, and major abdominal surgery.
The dose-sparing effect of magnesium sulfate allows for a reduction in the total amount of non-depolarizing neuromuscular blockers required to achieve adequate surgical conditions. This may contribute to a lower incidence of dose-related adverse effects and supports more individualized dosing strategies. In addition, magnesium pretreatment may reduce succinylcholine-associated complications, such as fasciculations, postoperative myalgia, and potassium release, which is particularly relevant in patients at risk of hyperkalemia.
From a safety perspective, magnesium sulfate appears to be well tolerated at clinically used doses (30–60 mg/kg). Given its potential to prolong neuromuscular blockade and delay spontaneous recovery, routine use of objective monitoring and appropriate dose adjustment of neuromuscular blockers are essential to minimize the risk of residual neuromuscular block.
Overall, magnesium sulfate represents a low-cost, widely available, and clinically useful pharmacological adjuvant that can improve intubation conditions, optimize neuromuscular blockade, and enhance perioperative management when used judiciously and with appropriate monitoring.
These considerations may assist anaesthesiologists in selecting appropriate neuromuscular management strategies adjusted to individual patient and procedural requirements.
6. Conclusions
Analysis of the available data indicates that intravenous magnesium sulfate is a valuable pharmacological adjuvant in anesthesia with a proven effect on neuromuscular transmission, resulting in enhanced muscle relaxation. Evidence from the literature demonstrates that magnesium administration can accelerate the onset and improve the quality and intensity of neuromuscular blockade, leading to improved conditions for tracheal intubation and surgical intervention. Its dose-sparing effect on non-depolarizing neuromuscular blocking agents may reduce dose-related adverse effects and broaden its clinical utility.
The limitations of the existing evidence include small sample sizes, heterogeneity in study designs, and variability in methodologies. Larger, well-designed clinical trials are required to define optimal dosing strategies, clarify indications and contraindications, and establish long-term safety. Although several advantages have been demonstrated, the use of magnesium sulfate remains limited in routine anaesthetic practice.
From a clinical perspective, magnesium sulfate represents a safe and effective adjuvant that may contribute to improved intraoperative and postoperative outcomes through its effects on neuromuscular blockade, analgesia, and hemodynamic stability. Its incorporation into anaesthetic practice should be accompanied by strict quantitative neuromuscular monitoring to ensure optimal dosing, facilitate recovery, and minimize the risk of residual neuromuscular blockade.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Evron, S; Ron, M; Donchin, Y. [Magnesium sulfate in the treatment of toxemia of pregnancy and its influence on muscle relaxants used in general anesthesia]. Harefuah;Hebrew. 1978, 94(2), 90–2. [Google Scholar] [PubMed]
- James, MF; Cork, RC; Dennett, JE. Succinylcholine pretreatment with magnesium sulfate. Anesth Analg. 1986, 65(4), 373–6. [Google Scholar] [CrossRef] [PubMed]
- Stacey, MR; Barclay, K; Asai, T; Vaughan, RS. Effects of magnesium sulphate on succinylcholine -induced complications during rapid-sequence induction of anaesthesia. Anaesthesia 1995, 50(11), 933–6. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M; Talwar, N; Goyal, R; Shukla, U; Sethi, A. Effect of magnesium sulfate with propofol induction of anesthesia on succinylcholine-induced fasciculations and myalgia. J Anaesthesiol Clin Pharmacol. 2012, 28(1), 81–5. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- James, MF; Schenk, PA; van der Veen, BW. Priming of pancuronium with magnesium. Br J Anaesth 1991, 66(2), 247–9. [Google Scholar] [CrossRef] [PubMed]
- Kussman, B; Shorten, G; Uppington, J; Comunale, ME. Administration of magnesium sulphate before rocuronium: effects on speed of onset and duration of neuromuscular block. Br J Anaesth 1997, 79(1), 122–4. [Google Scholar] [CrossRef] [PubMed]
- Fuchs-Buder, T; Wilder-Smith, OH; Borgeat, A; Tassonyi, E. Interaction of magnesium sulphate with vecuronium-induced neuromuscular block. Br J Anaesth 1995, 74(4), 405–9. [Google Scholar] [CrossRef] [PubMed]
- Wu, HL; Ye, TH; Sun, L. Effects of atracurium pretreatment with magnesium on speed of onset, duration, and recovery of neuromuscular blockade. Zhongguo Yi Xue Ke Xue Yuan Xue Bao;Chinese. 2009, 31(1), 73–6. [Google Scholar] [PubMed]
- Czarnetzki, C; Lysakowski, C; Elia, N; Tramèr, MR. Time course of rocuronium-induced neuromuscular block after pre-treatment with magnesium sulphate: a randomised study. Acta Anaesthesiol Scand. 2010, 54(3), 299–306. [Google Scholar] [CrossRef] [PubMed]
- Rotava, P; Cavalcanti, IL; Barrucand, L; Vane, LA; Verçosa, N. Effects of magnesium sulphate on the pharmacodynamics of rocuronium in patients aged 60 years and older: A randomised trial. Eur J Anaesthesiol 2013, 30(10), 599–604. [Google Scholar] [CrossRef] [PubMed]
- Sun, H; Jin, T; Wu, X; Yang, L; Zuo, Y; Liao, R. Efficacy of magnesium sulfate as an adjuvant to rocuronium in general anaesthesia: a meta-analysis. J Int Med Res. 2021, 49(7), 3000605211027736. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, MH; Oh, AY; Jeon, YT; Hwang, JW; Do, SH. A randomised controlled trial comparing rocuronium priming, magnesium pre-treatment and a combination of the two methods. Anaesthesia 2012, 67(7), 748–54. [Google Scholar] [CrossRef] [PubMed]
- Queiroz Rangel Micuci, AJ; Verçosa, N; Filho, PAG; de Boer, HD; Barbosa, DD; Cavalcanti, IL. Effect of pretreatment with magnesium sulphate on the duration of intense and deep neuromuscular blockade with rocuronium: A randomised controlled trial. Eur J Anaesthesiol 2019, 36(7), 502–508. [Google Scholar] [CrossRef] [PubMed]
- Fuchs-Buder, T; Ziegenfuss, T; Lysakowski, K; Tassonyi, E. Antagonism of vecuronium-induced neuromuscular block in patients pretreated with magnesium sulphate: dose-effect relationship of neostigmine. Br J Anaesth 1999, 82(1), 61–5. [Google Scholar] [CrossRef] [PubMed]
- Han, J; Jeon, YT; Ryu, JH; Koo, CH; Nam, SW; Cho, SI; Oh, AY. Effects of magnesium on the dose of rocuronium for deep neuromuscular blockade: A randomised controlled trial. Eur J Anaesthesiol 2021, 38(4), 432–437. [Google Scholar] [CrossRef] [PubMed]
- Paul, G; Naaz, S; Bhadani, UK; Sahay, N; Kumar, R; Kumar, S. Comparison of Succinylcholine, Rocuronium, and Rocuronium with Magnesium on Time of Onset of Paralysis in Adult Patients Undergoing Rapid Sequence Induction: A Double Blinded Randomised Control Trial. Turk J Anaesthesiol Reanim 2025. [Google Scholar] [CrossRef] [PubMed]
- Ghodraty, MR; Saif, AA; Kholdebarin, AR; Rokhtabnak, F; Pournajafian, AR; Nikzad-Jamnani, AR; Shah, A; Nader, ND. The effects of magnesium sulfate on neuromuscular blockade by cisatracurium during induction of anesthesia. J Anesth. 2012, 26(6), 858–63. [Google Scholar] [CrossRef] [PubMed]
- Czarnetzki, C; Albrecht, E; Masouyé, P; Baeriswyl, M; Poncet, A; Robin, M; Kern, C; Tramèr, MR. Rapid Sequence Induction With a Standard Intubation Dose of Rocuronium After Magnesium Pretreatment Compared With Succinylcholine: A Randomized Clinical Trial. Anesth Analg. 2021, 133(6), 1540–1549. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aissaoui, Y; Qamous, Y; Serghini, I; Zoubir, M; Salim, JL; Boughalem, M. Magnesium sulphate: an adjuvant to tracheal intubation without muscle relaxation – a randomised study. Eur J Anaesthesiol 2012, 29(8), 391–7. [Google Scholar] [CrossRef] [PubMed]
- Song, IA; Oh, TK; Do, SH. Trends in Perioperative Magnesium Sulfate Use in Patients Who Underwent Major Cancer Surgery: A Retrospective Population-Based Cohort Study in South Korea. Cancer Control 2023, 30, 10732748231180977. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).