Submitted:
30 January 2026
Posted:
02 February 2026
You are already at the latest version
Abstract
Autistic adults experience high rates of co-occurring mental health conditions. This study sought to explore mental health therapy experiences of recently diagnosed autistic adults in a private mental health clinic, and gauge their interest in, and ideas for, an autism specific mental health group program. Ten adults (20 – 52 years) choose semi-structured qualitative interviews from several participation options. Content analysis of the data was undertaken, and recruitment was concluded after data saturation was reached. Dialectical behaviour therapy variants and art therapy had been most frequently undertaken as previous mental health interventions. Many participants enjoyed the solidarity of group therapy, however some experienced therapists as patronising, impacting on their engagement. Sensory preference mismatches and a tendency for social masking were also cited as impacting engagement. The majority voiced a strong interest in attending an autism specific group mental health program. Participants provided suggestions for group topics and content alongside logistical and group promotion considerations. The results were used to adjust clinical practice at the service and to develop a draft group therapy program outline. This draft group outline was then further refined via consumer focus groups in the next phase of co-production of the broader study project. Limitations of this study included feedback being derived from a cohort of adults recently diagnosed autistic, all who had prior therapy experience, and were engaged with the mental health service undertaking the research.
Keywords:
adults
; autism
; co-production group therapy
; groupwork
; inpatient
; mental health
; therapy
; qualitative
Introduction
Autistic adults experience higher rates of co-occurring mental health conditions. Relative to the general population, lifetime prevalence of depressive disorders (37-77%), anxiety disorders (42-59%), obsessive compulsive disorder (OCD) (24-34%), and attention deficit hyperactivity disorder (ADHD) (40-61%) are elevated (Hollocks et al., 2019; Joshi et al., 2013; Rau et al., 2020; Rong et al., 2021). Ableism, a lack of societal understanding of Autism and required accommodations, alongside explicit and implicit expectations of neuroconformity may contribute to self-esteem and mental health difficulties (Cooper et al., 2017; Crane et al., 2019; Lee et al., 2023). Psychological factors that are also relevant including trauma and invalidation experienced by autistic individuals across many settings, including schools, workplaces, home and community environments, particularly through bullying, stigmatization, and exclusion (Benevides et al., 2020; Crane et al., 2019). Areas of mental health prioritized by autistic adults include improving quality of life and social well-being, alongside addressing societal barriers that contribute to stigma, discrimination and inclusion (Benevides et al., 2020).
When autistic adults do seek support, mixed experiences are reported with mental health systems and professionals. Unmet needs have been uncovered in a variety of areas, including autistic adults being excluded from mental health services and health professionals lacking adequate understanding of autism (e.g., commonly presenting features such as alexithymia and camouflaging behaviors)(Camm-Crosbie et al., 2019). Study findings also indicate that many professionals working with autistic adults appeared unaware of the double empathy problem, including clinician bias in accurately interpreting autistic communication and behavior, leading to problems with rapport building and misperceptions (Camm-Crosbie et al., 2019). To help address this, Pappagianopoulos and colleagues (2024) recently developed a helpful autistic-oriented framework for providing tailored psychological supports. The first of three themes involved cultivating a safe space, informed by building an understanding of autism, developing awareness of personal assumptions and biases, and displaying therapeutic soft skills that validate clients’ experiences. The second was demonstrating a flexible and collaborative approach to therapy that is responsive to clients’ needs. This included considering communication and sensory needs, providing appropriate adaptations, establishing structure and consistency, offering options for therapeutic settings and aligning the therapy context with individualized client goals, including seeking feedback. The third theme considered clients’ preferences regarding talking in session when supporting personal growth and skill development. Suggestions to facilitate this included opportunities to talk and open up emotionally when a client desired, and providing new perspectives and insights on this information, when appropriate (Pappagianopoulos et al., 2024).
These recent findings strongly align with key principles outlined in a Delphi study operationalising neurodiversity affirming psychology practice in Australia for autistic adults (Flower et al., 2025). This paper highlighted the importance of clinician knowledge, in combination with nuanced and adjusted clinical approaches to accommodate client preferences. By modifying therapy approaches and services, with tailored accommodations, in combination with practicing affirming care, interventions become more inclusive, effective and autism-affirming. This also dovetails with autistic self-advocacy and the neurodiversity movement, consistent with ‘nothing about us without us’ in disability rights activism (Kapp, 2020). Autistic self-advocacy promotes full autistic participation in decision-making, and autistic expertise being recognized for the value that it provides in guiding research and practice so services are better fit-for-purpose to meet autistic needs (Kapp, 2020). Rather than attempting to modify, change or ‘improve’ the skills or behavior of autistic individuals through ‘treatment”, therapists themselves need to align their practices to better support autistic individuals (den Houting, 2019; Jellett & Flower, 2024; Mandy, 2022). Neuroaffirming practice should be grounded in an understanding that autistic styles of behaving and relating are healthy differences from neurotypical ‘norms’.
Whilst important advances have been made for practice frameworks in an individual 1:1 therapy context, there is currently a dearth of research exploring autistic adults’ experiences of group-based mental health therapy, and associated group specific recommendations. It is presently not clear whether extra recommendations could be useful when facilitating support in a group-based setting, for autistic adults with mental health challenges. More could be done to involve autistic individuals in the design of ‘fit-for-purpose’ group therapy programs, inclusive of autistic ideas and preferences, via co-production.
A number of studies have reported modifications to standard therapy modalities, in an attempt to make the therapy frameworks, and content delivery, better suited to autistic needs. This includes modifications to Dialectical Behaviour Therapy (DBT), Cognitive Behavioral Therapy (CBT), Modified Acceptance and Commitment Therapy (ACT) and Mindfulness-Based Therapy (MBT) (Bemmer et al., 2021; Bemmouna et al., 2022a; Cooper et al., 2018; Hartmann et al., 2012a; Keenan et al., 2024; McGillivray & Evert, 2014; Pahnke et al., 2019; Ritschel et al., 2022; Spain et al., 2017; Spek et al., 2013). Reported modifications in the above listed studies commonly involve adapted formats for information provision (colour coding, visual information, indexing), avoiding the use of metaphors, use of “plain” language, sensory accommodations and gamification. Many of these studies report improvements in high prevalence mental health symptoms of depression and anxiety in autistic participants. However, few of these modifications have been made on an explicitly described co-production basis, informed by consumer involvement. It remains to be seen whether involving autistic adult consumers, themselves, in the co-production process for group therapy intervention will result in stronger clinical outcomes and consumer satisfaction.
The current study sought feedback from autistic adult mental health service users about their experiences with mental health interventions, and gauged their interest in, and preferential ideas for, a group mental health therapy program for autistic adults. The impetus for this research originated from direct feedback provided by autistic clients of the service about the lack of access to post-diagnostic support and groups specifically designed for autistic adults. The current study represents Phase 2a, of a multi-phase co-production clinical research project. There was intention to use obtained data to inform the development of a mental health group program for autistic clients of the service, if this was indicated as desired and feasible from participant responses, from the co-production process. In Phase 1 qualitative interviews were conducted with adults recently diagnosed with autism, using a strengths-based, neurodiversity-positive neuropsychological framework, to determine the acceptability of this approach (Authors, in press). All participants reported positive sentiments about the assessment, in addition to making suggestions for adjustments to improve the process (including increased modulation of sensory input, improved fatigue management and providing a greater number of feedback sessions). Gaps were identified in opportunities to access autism specific support following diagnosis. The current study (Phase 2a) sought to gauge the interest of adults recently diagnosed with autism in attending a group mental health therapy program. The study sought to gain information on autistic adults’ previous experiences with psychological therapy, their views on what type of content would be helpful in a group therapy program, and any concerns they may have about attending. Ideas were also sought about recommendations for engaging autistic adults in such a program. This study was part of the initial phases of a larger co-production project to design consumer informed mental health support for adults following a diagnosis of autism (if indicated as being desired by consumer stakeholders).1
Method
Research Team and Consultation
The research team is neurodiverse, comprising of autistic and non-autistic members. One clinician-researcher is diagnosed autistic and has both family experience and lived experience of autistic communities. One clinician-researcher has both an autistic parent and child, with other neurodivergent conditions in first-degree family members. The Olga Tennison Autism Research Centre at Latrobe University was consulted during the planning phase, prior to implementing this study. The fundamentals of co-production principles proposed by People with Disabilities Western Australia, and the recommendations for using experience-based co-design (EBCD) suggested by Green, et al., were consulted and implemented, as appropriate, during the phases of the co-production project (Green et al., 2020; People with Disabilities WA Inc, 2018).
Study Design
This study was designed in 2020 and data was collected over an 18-month period in 2021 and 2022. The Consolidated Criteria for Reporting Qualitative Research guidelines were consulted for the reporting of methods and findings (COREQ) (Tong et al., 2007)(Supplement S1). This project was approved by the [insert name] Research Ethics Committee [Project number XX].
Participants
Adult participants (18 years and above) were recruited via an inpatient neuropsychology service at an Australian private mental health hospital, who had a recently been diagnosed autistic (< 24 months) through the service. The diagnostic process, using a strengths-based, neurodiversity-positive neuropsychological framework, has been described elsewhere (Authors, in press). All invited participants met Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) criteria for Autism, with discovery criteria outlined by (Gray & Attwood, 2013) also consulted. Although deficits based, DSM-5 criteria were utilised to align with diagnostic expectations to access relevant healthcare in the country of practice, and support participants if accessing the National Disability Insurance Scheme (NDIS). All participants also had a Social Responsiveness Scale 2nd Edition (SRS-2) self-report total score T-score of 60 or above. As a validated psychometric assessment tool, this measure was also utilised to assist diagnosis; albeit noting that at the time there was not a readily available neuro-affirming psychometric measure (we are aware of several under development). Potentially eligible participants’ treating psychiatrists were contacted first, to check for their suitability to participate. Then, utilising convenience sampling, clients who met criteria were invited in a serial fashion (in chronological order, from date of neuropsychology assessment), and recruitment continued until data saturation was obtained. Eighty-three percent of the eligible clients contacted (10/12) agreed to participate.
Setting
The study was conducted within a private mental health hospital in [City Name], Australia, that provides inpatient, outpatient and outreach (mobile support) services2. Clients need to be receiving care under a hospital accredited psychiatrist and typically have health insurance or funding from the Department of Veteran’s Affairs, WorkCover, or the Transport Accident Corporation to access services (self-funding without insurance is possible although few clients fall into this category). Approximately 55 percent of the Australian population have health insurance according to a recent report (Australian Competition and Consumer Commission, 2023), although this percentage is not known specifically for autistic adults.
Procedures
To minimize the likelihood of coercion, potential participants were contacted inviting them to participate (via email or telephone) by a study researcher not involved in their prior diagnostic assessment. They were explicitly informed both verbally, and in written documentation provided about the study, that participation was voluntary, and that declining to participate would not impact on their relationship with the clinic, in any way. Below is an exert of the written information from the participant information sheet:
Participation in the study is voluntary, you do not have to participate, if you do not want to. If you do not want to participate, this will not affect any current or future treatment you may have at [Name] Clinic. It will not impact on any future review or involvement you may have with the neuropsychology service.
Following consent to participate, the same non-assessing clinician-researcher conducted the research interview with participants, in an attempt to minimise response bias. Beyond diagnostic assessment, feedback and adjustment support, none of the clinician-researchers had previously acted in a mental health therapeutic capacity (as an individual therapist or group facilitator) with any of the study participants. A structured qualitative interview framework was used to conduct the interviews. These were held either online via videoconference, over the telephone or in person (on site at the service), as per participant preference, with only the interviewing clinician-researcher and participant present (i.e. no third parties or observers). The possibility of emailing written responses to interview questions was offered, but this was not chosen by any participants. Five out of six clinician-researchers had acted as the assessing clinician for at least one participant. Four out of the five assessing clinician-researchers completed at least one study interview, all were registered clinical neuropsychologists with Masters or Doctoral level clinical qualifications, two females and two males (CF, ET, NG, JL). The sixth researcher was a registered clinical and counselling psychologist, with a Masters degree, and also a registered mental health nurse. All interviewing clinician-researchers approached the study from a neurodiversity-supportive, diagnosis-affirming care framework, and had experience working with autistic adults. Prior to commencing interviews, participants were informed that questions would be asked about types of psychological therapy they may have undertaken, and if the participant found the therapy(ies) useful. Participants were also informed that questions would ask about their thoughts on group therapy programs and any ideas they had for an autism specific group.
Materials
Utilising principles outlined by (Braun & Clarke, 2013), a qualitative interview guide was developed by members of the research team (five Masters or Doctoral level Clinical Neuropsychologists with four to 20 years clinical experience, three females and two males). The questions were designed to address the research aims described above. The questionnaire collected demographic information and was followed by three open-ended questions, adjunct with a series of prompts to assist the interviewer to elicit further information if required. The questions were:
-
Have you undertaken any psychological therapy before, by yourself or in a therapy group? Can you describe your experiences with this?(Prompts: Do you know what type of therapy it was, e.g. CBT, ACT, DBT, Mindfulness? Do you feel that therapy worked for you?)3
-
The [Name] Clinic has an outpatient Day Program service. This provides different therapy group programs for clients with a range of psychological conditions. Would you have interest in attending an outpatient Day Program for people with Autism4 if one was available? This could be run during the day or at night.(Prompts: How much do group programs interest you? Have you looked for autism specific programs to attend already?)
-
What topics do you think should be covered in an outpatient autism psychological group therapy program?(Prompts: Are there things that you would like to know more about? Are there things that might be important to cover?)
-
Is there anything that would concern you about attending an outpatient autism specific psychological group therapy program?(Prompts: Do you have concerns about therapy in a group? Sensory sensitives that might be an issue?)
-
Do you have any recommendations about engaging people on the autism spectrum4 in a psychological therapy outpatient group program?(Prompts: Is there anything else important that should be considered? Should it be a day or evening program? Do you prefer online or in person? Can you think of any barriers that might affect how well this program runs?)
The interview questions outlined above (constituting Phase 2a) were presented to clients as part of a broader co-production research project. In Phase 1 participants were asked questions about the acceptability of the neuropsychology assessment process (Authors, in press).
Data Analysis
Quantitative
Descriptive analysis was undertaken of the quantitative data, derived from the demographic data collected from participants. This included frequency count, means and ranges of relevant demographic information.
Qualitative
All interviews were audio recorded and transcribed using Otter.ai software, then fully cross-checked by one of two study researchers (JP and CF). All unclear utterances were discussed with the interviewing researcher until consensus of content was reached. All interview data were coded and analysed using conventional content analysis (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005; Kleinheksel et al., 2020). This method was chosen because the principle purpose was to describe a phenomenon, particularly suited for when previous knowledge may be limited. Preconceived categories were avoided, and grouping into categories and labelling of categories were driven by the data in an inductive manner (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005). The major steps of this process included:
- Data elicitation through interviews with open-ended questions and probes (prompts)
- Data analysis commencing with the reading of all of the data, to ensure immersion, by more than one researcher (CF & JP)
- Reading of data word-by-word to derive codes – by highlighting specific words and capturing key thoughts and concepts (CF, NG, JP)
- Initial analysis of codes via the formation of notes of first impressions (NG & JP, cross checked all discrepancies resolved by mutual agreement)
- Sorting of codes into different categories, looking for relationships and links (CF, NG, JP, ET, JL)
- Organisation of emergent “main” categories and sub-categories to group meaningful clusters (CF, NG & JP).
- Identification of exemplars, for categories and sub-categories to add richness to the reporting of the data in the participants own words (CF).
Data saturation within qualitative interview-based research is the juncture at which data set size (e.g. number of interviews) fails to yield any further new information. Acknowledging debate in literature regarding the lack of consistency and variance of data saturation determination criterion, an inductive saturation approach was applied (Saunders et al., 2018). We implemented Guest and colleagues’ (2020), which identified a “base” number of interviews that are then coded to derive categories. A “run” size of additional interviews followed and codes and categories reanalysed to determine if the interviews would yield new information. The chosen base size of eight interviews was more conservative that that proposed by Guest and colleagues (i.e. 6 interviews), due to heterogeneity. A standard run size of two additional interviews was chosen, with a new information threshold was also set conservatively at 0% for any new main categories or subcategories.
Coding and initial early sorting categorisations were discussed as a research team, after the full coding of eight interview transcripts, to determine consistency and clarity. The remaining two interviews were coded and analysed to determine if data saturation had been achieved. Whilst interviews number nine and ten generated new codes, they did not identify any new categories or sub-categories. Thus, based on the above criteria, saturation was achieved after the completion of ten interviews. The categorical grouping and descriptors were discussed, condensed and finalised by three of the authors (CF, JP, NG) in subsequent final data analysis.
Results
Quantitative
Demographic characteristics are provided in Supplement S2 - Table S1. There was a 32-year age span across the cohort (20-52 years); no participants were older adults (>65 years). There was diversity in gender identities, including female, male, non-binary and transgender participants. Variation was seen in the duration of time since the participants’ autism diagnostic assessment, ranging from one month to almost two years. Half of the cohort were in paid employment. There was a high rate of current or lifetime co-occurring mental health conditions, with the most common being Attention Deficit Hyperactivity Disorder (ADHD), Depressive disorders and Anxiety disorders. A range of overall intellectual skills was observed, from the Borderline (3rd percentile) to Superior (95th percentile) ranges; although, all clients had robust verbal skills, with WAIS-IV Verbal Comprehensive Indexes ranging from the 32nd to 96th percentiles. All SRS-2 self-report measures scored in the highest two percent or above, for features of autism. The average interview length was almost 37 minutes, and included questions pertaining to both the Phase 1 and Phase 2a (current) sections of the research project. For more detailed participant information, including neuropsychological assessment results of the participant group, please see [Authors, in press].
Qualitative Results
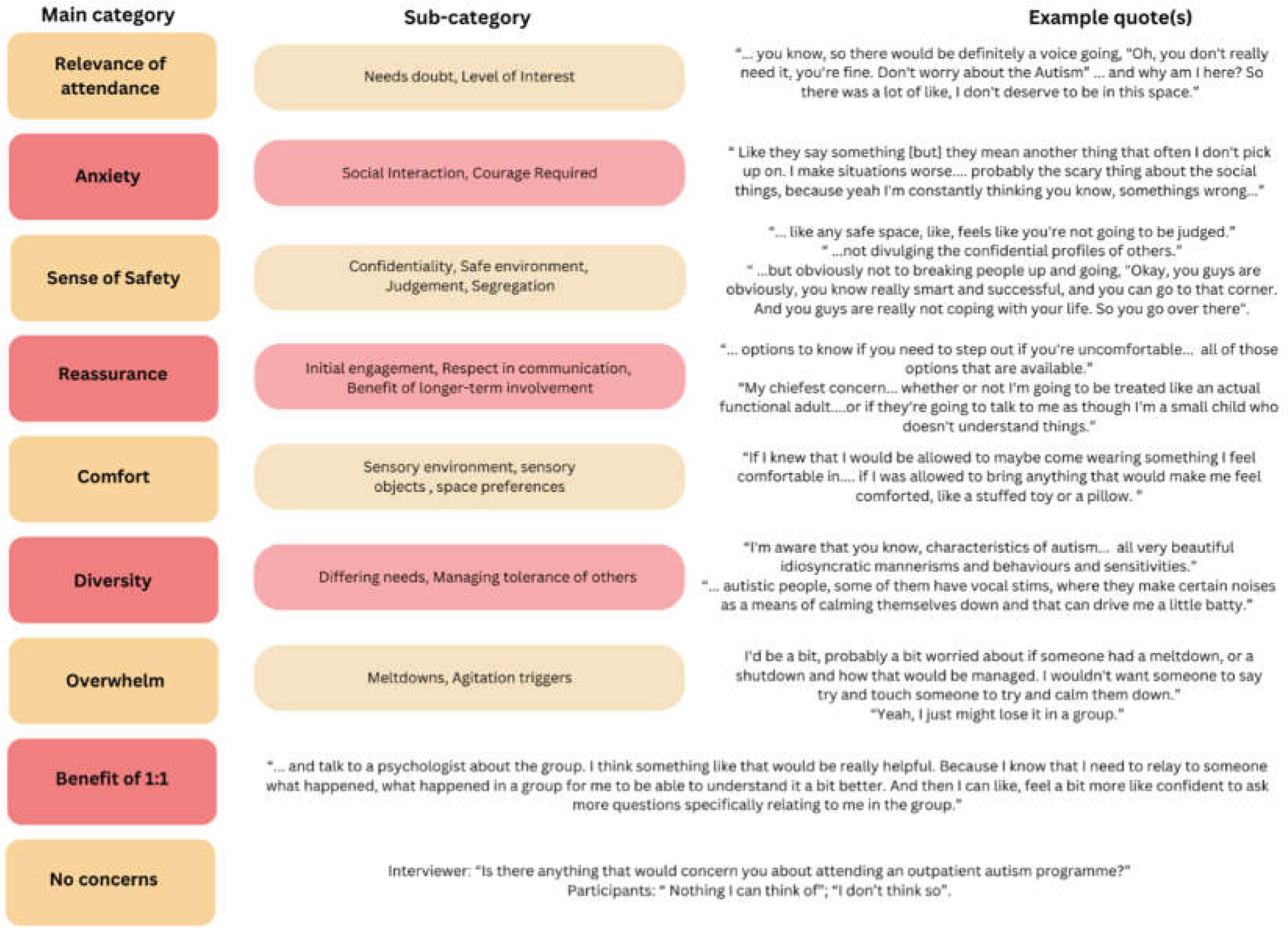
The interview response data was grouped into four key response areas, with main categories, sub-categories and individual codes organised in each of these areas. The four key response areas were: Previous experiences with therapy, Interest in attending an autism group, Topics to cover in an autism group, and Concerns about attending and suggestions to improve attendance and engagement. Each of these four key responses areas, including main categories (capitalised, italics), sub-categories and exemplar quotes, are outlined in Figure 1, Figure 2, Figure 3 and Figure 4. Main category headings are presented in Italics, when described in-text below.
In the key response area of Previous experiences with therapy (see Figure 1) the first main category indicated that participants had undertaken a Broad range of therapies with a variety identified through sub-category analysis. This indicated the participants were a therapy experienced cohort. The three most commonly discussed therapy types were DBT, Emotional Management Programs (EMP- a DBT skills based program) and Art Therapy. Another main category was that participants had undertaken Therapy prior to autism diagnosis with some indicating that their experiences might be different now, given this additional information, and further knowledge about themselves. Some participants also indicated that they experienced their Autism impact on engagement with group therapy, describing masking behaviours and sensory inputs that were not to their preference. Group Experiences were also raised. Sub-categories included the impact of Group Dynamics with many positives aspects discussed, such as shared experiences and group camaraderie. Specific Group Activities that were enjoyable included pairs work and role-plays. Improvements attributed to group therapy included participants’ mental state and social connectedness. Difficulties experienced with group work included groups being too long, and feeling uncomfortable when other people spoke about trauma. Operational group aspects were also discussed as part of previous experiences. These included preferences for groups to start and finish on time, having knowledge of topic outlines before groups commenced, and enjoying groups that built on content presented in previous sessions. There was a variety of preferences for presentation modality. For example, one participant preferred face-to-face groups (rather than online), but also reported there was a lot going on in face-to-face group sessions.
Other categories raised in this key response area were client’s previous experiences with Individual 1:1 Therapy, conducted by a sole practitioner, such as a psychologist or psychiatrist. Positive experiences with individual 1:1 therapy were discussed, whilst some noted it was hard to find a therapist with experience in autism. Others noted they struggled with “small talk” during their individual 1:1 therapy sessions. A preference for having a visual element included in the talk-therapy was also described (e.g., white-boarding topics, drawing, illustration, graphing, mind-mapping and creative activities). The availability and use of Weighted and sensory objects was helpful for several participants. Participants also reflected that the Therapist-client dynamic was important and potentially more so than the mode of therapy, itself. Finally, Negative experiences with professionals were also raised. These included professionals’ limited understanding of autism, condescending and patronising approaches, or being treated/spoken to like a child, particularly when the clinician became aware of a participant’s autism diagnosis.
In the key response area of Interest in Attending an Autism Group (Figure 2), positive Autism group interest was voiced by majority of participants (90%). This included having positive anticipatory regard for a future group, should one be developed, as well as a sense of a safety in a shared autism group environment. Variety and co-conditions in participants were considered as relevant to the running and development of the group. Group Structure was considered important, including the need for breaks, and the capacity to cover topics in detail. Group logistics were also raised as part of running a successful group. This included preparing participants before programs and considering group size, session length and the setting (inpatient versus outpatient). The option of an outpatient group was posed in the anchor question (see above) and was preferred by a number of clients; however the option of, and preference for, an inpatient group was also raised by one client. Attendance challenges were raised that included travel distances, needing to commit for the duration of the program, and that attending a group with people they did not know would be daunting. Suggestions provided for Group Promotion included making brochures, promoting the group with referring doctors, and contacting eligible clients via email. Experiences with Other/external autism groups were also discussed, including that many groups were designed for parents or caretakers of autistic children, and that groups for autistic adults were hard to find.
In the third key response area of Topics to cover in an autism group (Figure 3), Autism as a topic itself, was frequently raised. This included identified sub-categories of information on understanding autism, providing information about autistic traits, the impact and experience of receiving a diagnosis in adulthood, and involving significant others in this education. Suggestions to provide information about Neurodiversity were also received, including an understanding of the neurobiological basis of autism, and coming from a differences, rather than deficits, approach. Emotions and Management also arose as a main category, and included the sub-categories of managing and noticing emotions, alongside specific strategies to assist with emotional regulation. Sensory topics formed another category, including sensory features, soothing, managing preferences, sensation seeking, and interoception.
Under the main category of Interacting with others, were the sub-categories of communication and socialisation. How to manage socialisation across interpersonal relationships and friendships was frequently suggested, as well as skills for both communication and interacting effectively to get a point across. Several participants also indicated that they wanted to be supported to learn skills for how to mask their autism in social settings if they chose to do so, to assist in social interactions with non-autistic people (e.g., including supressing the tendency for “info dumping”). Self-efficacy and advocacy was also a main response category, with sub-categories of self-empowerment and managing self and interpersonal boundaries. This included using self-compassion, resilience, navigating your own path, self-agency and skills for how to say “no” to requests of others. Functional skills were also raised under topics to cover in a group, including executive functioning skills (e.g., planning, organisation, time and energy management), life skills and managing overload. Finally, several participants discussed Specific therapy skills and techniques to include, or not include. This included having art therapy for its non-verbal modality and elements of DBT. Several participants voiced support for mindfulness and mindfulness movement activities, whilst another indicated they found mindfulness practice difficult. CBT was reported to be unfavoured by one participant.
The final key response area was Concerns about attending and suggestions to improve attendance and engagement for an autism group (Figure 4). Some participants indicated that they would, internally, question their Relevance of attendance. Sub-categories included doubting their need to attend, feeling like they did not need to be there, and concerns the content might not relate to, or be of interest to, them. Some voiced Anxiety about attending, due to the social interaction required, potential for misinterpretations, and that it would require courage to attend. Having a Sense of safety was described as important. This included the sub-categories of confidentiality, needing both a safe environment and one that was free of judgement, and not implementing the segregation of clients into ability, or levels of mental health wellness. Ways to foster a sense of safety were suggested under the next main category of Reassurance. This included providing important information during the initial engagement period, facilitators being respectful and empowering in their communication style, and that longer-term therapy involvement may improve working with other group members and engagement with content. Helpful suggestions to increase Comfort were also provided, including modulating sensory input within the environment, allowing and promoting the use of sensory and comfort items and comfort clothing, and managing preferences for personal space and room size.
Participants described an awareness of Diversity within an autistic cohort, including various idiosyncrasies and mannerisms, but also voiced concerns about how they would cope with the mannerisms of other group members (such as vocal stims). Another key category was Overwhelm, which included the sub-categories of meltdowns and managing agitation triggers. This included how staff would manage clients experiencing being overwhelmed, and concern that they, themselves, may not be able to manage agitation triggers in a group environment. Participants also spoke about the Benefit of 1:1 individual therapy with a clinician, in addition to engaging in a group therapy program. Finally, several participants indicated that they had No Concerns about attending an autism group program.
Discussion
The results met the first aim of the project - to gauge the interest of adults recently diagnosed autistic in attending an autism specific mental health group therapy program. The vast majority (90%) of the study participants voiced a positive interest in attending such a group, and provided a wide variety of helpful suggestions for group content, structure and logistics. The second aim of the study was to gain information on autistic adults’ previous experiences with psychological therapy, and any concerns they may have, about attending a group program. Participants had undertaken a wide variety of previous group or one-on-one mental health therapy. Many reported positive experiences in mixed-cohort, unmodified group therapy settings and enjoyed the solidarity experienced in a group dynamic. It was noted that the therapist-client dynamic can be as important as the therapy type itself, and that poor clinician understanding of autism and associated misperceptions and patronising approaches had resulted in negative experiences. Participants also indicated that masking behaviours and sensory preference mismatches impacted their capacity to engage optimally in group therapy, particularly prior to having received their autism diagnosis. The final aim of the project was to gain ideas about engaging autistic adults in a potential future group mental health program. This was achieved, and a number of recommendations were made for modifying existing group programs to support engagement and a sense of safety, and manage attendance anxiety (e.g., increased facilitator numbers and environmental adaptations to promote comfort).
When considering the therapy type best suited for implementation in a mental health program a number of key findings can be derived from the study results. The three most commonly reported previous therapies, DBT, Emotion Management (i.e., a DBT skills-based group program), and art therapy, were described with positive regard from those who had undertaken them. Sensory awareness and modulation groups (provided by occupational therapists at the clinic the study was conducted) were also described positively. Some mixed responses were provided about CBT and mindfulness approaches. When asked about specific group content participants would preference, and skills they may wish to learn, many suggestions also aligned with DBT, art therapy and sensory awareness and modulation approaches. This included topics on emotions and their management, self-efficacy and advocacy, interacting with others, sensory topics and content, and art therapy to allow for non-verbal expression.
These findings are in keeping with the emerging existing evidence base indicating both an efficacy for, and acceptability of, DBT-based therapy interventions with autistic adults (Bemmouna et al., 2022b; Cornwall et al., 2021; Hartmann et al., 2012b; Huntjens et al., 2024; Phillips et al., 2024; Ritschel et al., 2022). Sensory modulation interventions are also growing in awareness and have been used in both mental health settings and with autistic adults (Brown et al., 2018; Kandlur et al., 2023; MacLennan et al., 2022). Although, there is little published research on the efficacy of sensory modulation therapy (as opposed to sensory integration therapy) in autistic adults. There is also emerging evidence that art therapy intervention may be effective at improving mental health issues, particularly symptoms of depression and anxiety in autistic adults (Wang, 2023; Wright, 2023).
Participants were also strongly interested in content about autism being included in the group program. This included features and traits, receiving a diagnosis in adulthood and providing education to significant others. A participant interest in learning more about their neurotype, may be reflective of the characteristics of the cohort – all being newly diagnosed. It aligns with recent research findings that understanding and validation are key concepts of importance for adults with a new diagnosis of a neurodivergence (i.e. autism or ADHD) (Wearn et al., 2025). The broader concept of neurodiversity was also an area of interest, particularly for the diagnosis-affirming, diversity-positive lens provided by this framework.
A number of response categories present in the current study have similarities to those identified in previous qualitative research with autistic adults. Consistent with findings reported by Camm-Crosbie et al. (2019) participants in the current study felt that limited understanding of autism in clinician therapists contributed to negative experiences. Responses also indicated that condescending/patronising approaches of clinicians were problematic. This potentially parallels with the double-empathy problem outlined by Camm-Crosbie et al., (2019), as clinicians may not be aware of how their interpersonal style is received by autistic clients, leaving autistic clients feeling disrespected and infantilised.
Consistent with the framework proposed by Pappagianopoulos et al. (2024) for tailoring psychological interventions to meet the needs of autistic adults, participants felt that having a sense of safety in the group environment, being comfortable, and being provided with reassurance were important for engaging autistic adults in group work. They also reported the need to tailor the environment in a flexible way to meet clients’ needs, particularly from a sensory perspective, and that the diversity of preference needs across clients could be a challenge for therapists and co-participants. This latter point highlights participants’ awareness that preference needs may, at times, be opposing between group members and that participants may need to provide space for accommodations for others, which may not be fully in keeping with their own preferences. The consistency of themes across these three qualitative studies indicated commonalities in experiences of autistic adults when engaging with mental health support. Thus, it is important for therapy providers to be aware of these key themes, as autistic adults themselves have identified that the therapist-client dynamic may have as strong an impact on therapy efficacy, more than the therapy type itself. The findings also suggested that modifying standard therapy practices to accommodate for autistic adults’ sensory, information processing and comfort preferences is likely to yield stronger therapy engagement.
The results indicated that participants had concerns that factors such as social anxiety, sensory concerns, discussing processing of feelings (alexithymia), tolerating others stimming behaviours, and being concerned about themselves or others experiencing overwhelm, were relevant when considering group involvement. However, for the majority of participants, these concerns did not appear or override their interest and desire to be involved in a group mental health therapy program. Thus, if clinicians and therapy teams can assist to reduce or minimise the impact of these concerns, by providing accommodations and adaptations, many autistic adults may be interested in participating in group work (Flower et al., 2025).
This study has a number of limitations. Firstly, the cohort was recruited from a single, private mental health therapy clinic, and all had had previous involvement in a diagnostic capacity, with the study team (but not therapeutic involvement). Attempts were made to reduce power imbalances and influencing biases, by having a non-assessing clinician-researchers contact participants and conduct study interviews. Participants were also asked about any/all of their experiences with previous therapy, and were neither directed nor prevented from discussing their therapy experiences at the clinic. The data obtained indicated that participants spoke about a wide variety of experiences with therapy, including that undertaken at the clinic, and that undertaken at other practices and with other clinicians. Nevertheless, it remains possible that the sampling method impacted on participants’ candidness to speak freely about their experiences.
The participant group sought for this study were all recently diagnosed autistic in adulthood, with time since diagnosis ranging from 1 to 22 months. As such, different ideas may emerge in response to similar questions posed to people with longstanding or childhood autistic diagnoses. The participant group also had robust verbal intellectual skills, with the verbal comprehension abilities of all participants falling in the Average range, or above (32nd to 96th percentiles for WAIS-IV VCIs). Thus, responses may be different for autistic adults with different verbal language skills. Finally, the cohort were also experienced with psychological therapy, with all having previously undertaken, 1:1 individual or group therapy, and a number having participated in multiple types of therapy approaches. This may have contributed to the participants’ willingness to consider engaging in a potential future autism specific group therapy program. These views may differ from autistic adults who have not previously engaged in psychological therapy, have had limited access to mental health services, have had negative experiences engaging in psychological therapy, or do not have a co-occurring mental health condition. However, as the goal of the study was to assist in designing a therapy program for autistic users of the service, the make-up and characteristics of the participant group were appropriate to meet the goals of the study.
These results providing guidance on useful therapy frameworks and approaches, and ideas on how to tailor content, structure and group promotion, led the research team to embark on the next phase of the co-production program. A group program outline was designed based on data obtained in the current Phase 2a section of the project along with that from Phase 2b (clinicians’ ideas for an autism specific group mental health program). This involved a program with 10 active therapy days (2.5 hours active therapy per treatment day), and two primary focus topic content areas:
1) Neuro-affirming approach to identity exploration, education and discussion groups on Understanding Autism. Five topics (two sessions each): Autism and Neurodiversity, Strengths of Autism, Sensory Processing, Communication, Managing Overwhelm.
2) Mental health groups comprising Mindfulness-based practices and DBT Therapy Skills. Eight practical education mindfulness sessions. Four DBT skills topics (two sessions each): Understanding Emotions, Regulating Emotions, Managing Distress, Practical Applications.
See Supplementary Data S3 for further detail on draft program design. This draft program outline was presented for further input and refinement in focus groups with autistic adults (Phase 3). The qualitative data derived from this follow-up phase is currently being prepared for publication. The program pilot has also been launched at the service with data collection for this part of the project (Phase 4) currently underway.
Data Availability
To uphold the conditions of the human research ethics committee approval of this study, the authors are unable to deposit the data into a repository. However, the authors are happy to field any enquiries about the data, and will respond as appropriate on a case-by-case basis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Acknowledgements
We thank Prof. Amanda Richdale, Dr. Lauren Lawson and Dr. Eric Morris of the Olga Tennison Autism Research Centre and Latrobe University for their support and guidance at the inception of this project.
Conflict of Interest
The authors have no conflicts of interest to declare.
References
- Authors (in press). Accepted for publication, currently in the print production phase.
- Australian Competition and Consumer Commission. (2023). Report to the Australian Senate: On anti-competitive and other practices by health insurers and providers in relation to private health insurance.
- Bemmer, E. R., Boulton, K. A., Thomas, E. E., Larke, B., Lah, S., Hickie, I. B., & Guastella, A. J. (2021). Modified CBT for social anxiety and social functioning in young adults with autism spectrum disorder. Molecular Autism, 12(1), 1–15. [CrossRef]
- Bemmouna, D., Coutelle, R., Weibel, S., & Weiner, L. (2022a). Feasibility, Acceptability and Preliminary Efficacy of Dialectical Behavior Therapy for Autistic Adults without Intellectual Disability: A Mixed Methods Study. Journal of Autism and Developmental Disorders, 52(10), 4337–4354. [CrossRef]
- Bemmouna, D., Coutelle, R., Weibel, S., & Weiner, L. (2022b). Feasibility, Acceptability and Preliminary Efficacy of Dialectical Behavior Therapy for Autistic Adults without Intellectual Disability: A Mixed Methods Study. Journal of Autism and Developmental Disorders, 52(10), 4337–4354. [CrossRef]
- Benevides, T. W., Shore, S. M., Palmer, K., Duncan, P., Plank, A., Andresen, M. L., Caplan, R., Cook, B., Gassner, D., Hector, B. L., Morgan, L., Nebeker, L., Purkis, Y., Rankowski, B., Wittig, K., & Coughlin, S. S. (2020). Listening to the autistic voice: Mental health priorities to guide research and practice in autism from a stakeholder-driven project. Autism, 24(4), 822–833. [CrossRef]
- Braun, V., & Clarke, V. (2013). Successful Qualitative Research: A practical guide for beginners. Sage.
- Brown, A., Tse, T., & Fortune, T. (2018). Defining sensory modulation: A review of the concept and a contemporary definition for application by occupational therapists. Scandinavian Journal of Occupational Therapy, 0(0), 1–9. [CrossRef]
- Camm-Crosbie, L., Bradley, L., Shaw, R., Baron-Cohen, S., & Cassidy, S. (2019). ‘People like me don’t get support’: Autistic adults’ experiences of support and treatment for mental health difficulties, self-injury and suicidality. Autism, 23(6), 1431–1441. [CrossRef]
- Cooper, K., Loades, M. E., & Russell, A. (2018). Adapting psychological therapies for autism. Research in Autism Spectrum Disorders, 45, 43–50. [CrossRef]
- Cooper, K., Smith, L. G. E., & Russell, A. (2017). Social identity, self-esteem, and mental health in autism. European Journal of Social Psychology, 47(7), 844–854. [CrossRef]
- Cornwall, P. L., Simpson, S., Gibbs, C., & Morfee, V. (2021). Evaluation of radically open dialectical behaviour therapy in an adult community mental health team: effectiveness in people with autism spectrum disorders. BJPsych Bulletin, 45(3), 146–153. [CrossRef]
- Crane, L., Adams, F., Harper, G., Welch, J., & Pellicano, E. (2019). ‘Something needs to change’: Mental health experiences of young autistic adults in England. Autism, 23(2), 477–493. [CrossRef]
- den Houting, J. (2019). Neurodiversity: An insider’s perspective. Autism, 23(2), 271–273. [CrossRef]
- Elo, S., & Kyngäs, H. (2008). The qualitative content analysis process. Journal of Advanced Nursing, 62(1), 107–115. [CrossRef]
- Flower, R. L., Benn, R., Bury, S., Camin, M., Muggleton, J., Richardson, E. K., Bulluss, E. K., Calabria, B., Curran, A., Giugni, M., Gottliebsen, V., Hodges, H., Lawrence, J., Leung, V., Levy-Knoll, R., Miklosi, K., Mitchelson, M., Nuske, A., Waldie, C., … Jellett, R. (2025). Defining Neurodiversity Affirming Psychology Practice for Autistic Adults: A Delphi Study Integrating Psychologist and Client Perspectives. Autism in Adulthood. [CrossRef]
- Gray, C., & Attwood, T. (2013). The Discovery of Autism by Attwood and Gray.
- Green, T., Bonner, A., Teleni, L., Bradford, N., Purtell, L., Douglas, C., Yates, P., Macandrew, M., Dao, H. Y., & Chan, R. J. (2020). Use and reporting of experience-based codesign studies in the healthcare setting: a systematic review. In BMJ Quality and Safety (Vol. 29, Issue 1, pp. 64–76). BMJ Publishing Group. [CrossRef]
- Hartmann, K., Urbano, M., Manser, K., & Okwara, L. (2012a). Modified dialectical behavior therapy to improve emotion regulation in autism spectrum disorders. In Autism Spectrum Disorders: New Research (Issue May 2017).
- Hartmann, K., Urbano, M., Manser, K., & Okwara, L. (2012b). Modified dialectical behavior therapy to improve emotion regulation in autism spectrum disorders. In Autism Spectrum Disorders: New Research (Issue May 2017).
- Hollocks, M. J., Lerh, J. W., Magiati, I., Meiser-Stedman, R., & Brugha, T. S. (2019). Anxiety and Depression in Adults with Autism Spectrum Disorder: A Systematic Review and Meta-analysis. Psychological Medicine, 49(4), 559–572. [CrossRef]
- Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288. [CrossRef]
- Huntjens, A., Van Den Bosch Wies, L. M. C., Sizoo, B., Kerkhof, A., Smit, F., & Van Der Gaag, M. (2024). The effectiveness and safety of dialectical behavior therapy for suicidal ideation and behavior in autistic adults: A pragmatic randomized controlled trial. Psychological Medicine. [CrossRef]
- Jellett, R., & Flower, R. L. (2024). How can psychologists meet the needs of autistic adults? In Autism (Vol. 28, Issue 2, pp. 520–522). SAGE Publications Ltd. [CrossRef]
- Joshi, G., Wozniak, J., Petty, C., Martelon, M. K., Fried, R., Bolfek, A., Kotte, A., Stevens, J., Furtak, S. L., Bourgeois, M., Caruso, J., Caron, A., & Biederman, J. (2013). Psychiatric comorbidity and functioning in a clinically referred population of adults with autism spectrum disorders: A comparative study. Journal of Autism and Developmental Disorders, 43(6), 1314–1325. [CrossRef]
- Kandlur, N. R., Fernandes, A. C., Gerard, S. R., Rajiv, S., & Quadros, S. (2023). Sensory modulation interventions for adults with mental illness: A scoping review. Hong Kong Journal of Occupational Therapy, 36(2), 57–68. [CrossRef]
- Kapp, S. K. (2020). Autistic Community and the Neurodiversity Movement. In Autistic Community and the Neurodiversity Movement. [CrossRef]
- Keenan, E. G., Gurba, A. N., Mahaffey, B., Kappenberg, C. F., & Lerner, M. D. (2024). Leveling Up Dialectical Behavior Therapy for Autistic Individuals with Emotion Dysregulation: Clinical and Personal Insights. Autism in Adulthood, 6(1), 1–8. [CrossRef]
- Kleinheksel, A. J., Rockich-Winston, N., Tawfik, H., & Wyatt, T. R. (2020). Demystifying content analysis. American Journal of Pharmaceutical Education, 84(1), 127–137. [CrossRef]
- Lee, J. Y. S., Whittingham, K., Olson, R., & Mitchell, A. E. (2023). “Their Happiness, Not Neurotypical Success”: Autistic Adults Reflect on the Parenting of Autistic Children. Journal of Autism and Developmental Disorders. [CrossRef]
- MacLennan, K., O’Brien, S., & Tavassoli, T. (2022). In Our Own Words: The Complex Sensory Experiences of Autistic Adults. Journal of Autism and Developmental Disorders, 52(7), 3061–3075. [CrossRef]
- Mandy, W. (2022). Six ideas about how to address the autism mental health crisis. In Autism (Vol. 26, Issue 2, pp. 289–292). SAGE Publications Ltd. [CrossRef]
- McGillivray, J. A., & Evert, H. T. (2014). Group cognitive behavioural therapy program shows potential in reducing symptoms of depression and stress among young people with ASD. Journal of Autism and Developmental Disorders, 44(8), 2041–2051. [CrossRef]
- Pahnke, J., Hirvikoski, T., Bjureberg, J., Bölte, S., Jokinen, J., Bohman, B., & Lundgren, T. (2019). Acceptance and commitment therapy for autistic adults: An open pilot study in a psychiatric outpatient context. Journal of Contextual Behavioral Science, 13, 34–41. [CrossRef]
- Pappagianopoulos, J., Brunt, S., Smith, J. V., Menezes, M., Howard, M., Sadikova, E., Burroughs, C., & Mazurek, M. O. (2024). ‘Therapy Through the Lens of Autism’: Qualitative exploration of autistic adults’ therapy experiences. Counselling and Psychotherapy Research, April, 1–12. [CrossRef]
- Phillips, M. D., Parham, R., Hunt, K., & Camp, J. (2024). Dialectical behaviour therapy outcomes for adolescents with autism spectrum conditions compared to those without: findings from a seven-year service evaluation. Advances in Autism, 10(3), 185–199. [CrossRef]
- Rau, S., Skapek, M. F., Tiplady, K., Seese, S., Burns, A., Armour, A. C., & Kenworthy, L. (2020). Identifying comorbid ADHD in autism: Attending to the inattentive presentation. Research in Autism Spectrum Disorders, 69(October 2019), 101468. [CrossRef]
- Ritschel, L. A., Guy, L., & Maddox, B. B. (2022). A pilot study of dialectical behaviour therapy skills training for autistic adults. Behaviour and Cognitive Psychology, 50(2), 187–202. [CrossRef]
- Rong, Y., Yang, C.-J., Jin, Y., & Wang, Y. (2021). Prevalence of attention-deficit/hyperactivity disorder in individuals with autism spectrum disorder: A meta-analysis. Research in Autism Spectrum Disorders, 83, 101759.
- Spain, D., Blainey, S. H., & Vaillancourt, K. (2017). Group cognitive behaviour therapy (CBT) for social interaction anxiety in adults with autism spectrum disorders (ASD). Research in Autism Spectrum Disorders, 41, 20–30.
- Spek, A. A., van Ham, N. C., & Nyklíček, I. (2013). Mindfulness-based therapy in adults with an autism spectrum disorder: A randomized controlled trial. Research in Developmental Disabilities, 34(1), 246–253. [CrossRef]
- Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357. [CrossRef]
- Wang, Y. (2023). Art therapy for individuals with autism spectrum disorder and depression: effectiveness and future directions. In Journal of Education, Humanities and Social Sciences RETPS (Vol. 2023).
- Wearn, A., Collier, Z., Jenkins, K., Wearn, L., Carson, N., El Zerbi, C., Shenton, F., Spencer, L., & Pearson, A. (2025). ‘Nothing about us without us’: Developing inclusive and meaningful research collaborations with autistic young people and peers. In Championing Co-production in the Design of Inclusive Practices (pp. 89–100). Routledge.
- Wright, A. C. (2023). Art therapy with an autistic person with learning disabilities: communication and emotional regulation. International Journal of Art Therapy: Inscape, 28(4), 154–166. [CrossRef]
| 1 | In addition to Phase 1, and the current Phase 2a, described above, further extension studies have since been commenced. Phase 2b evaluated the views of mental health clinicians on the implementation and design of an autism specific group mental health therapy program, utilising a constructivist grounded theory approach (N = 18) (in preparation for submission). Phase 3 involved the development of a group mental health therapy program for autistic adults using a consumer co-design framework (N = 4) (in preparation for submission). |
| 2 | The study was conducted by a clinical team, who all have research experience. This was an unfunded study, (i.e. not facilitated by a research grant), but undertaken as a clinical research project to improve the understanding of, and provisions for, therapeutic supports for autistic clients at the service. |
| 3 | This probe covered any experiences with therapy, not just therapy programs run at/by the clinic at which the study was conducted. Participants spoke about a wide range of therapy experience both group and individual 1:1 work, including those run at the clinic, and those run by other practitioners, clinics and services. |
| 4 | Research protocol was designed in 2020. Language used as reported. Since this time neuro-affirming convention has changed such that ‘Autistic people’ would be utilised if designed presently. |
Figure 1.
Key Response Area - Previous Experiences with Therapy.
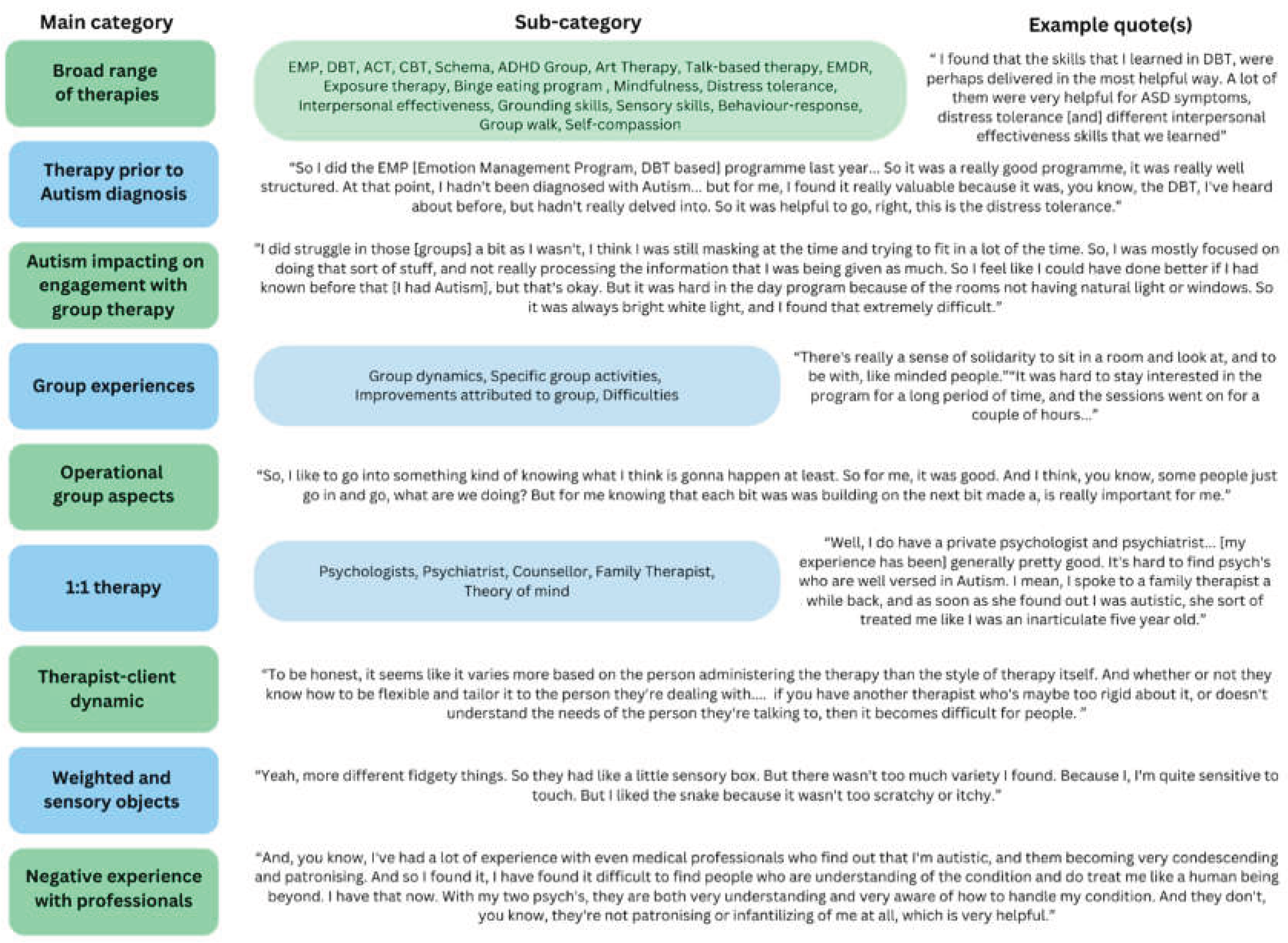
Figure 2.
Key Response Area - Interest in Attending an Autism Group.
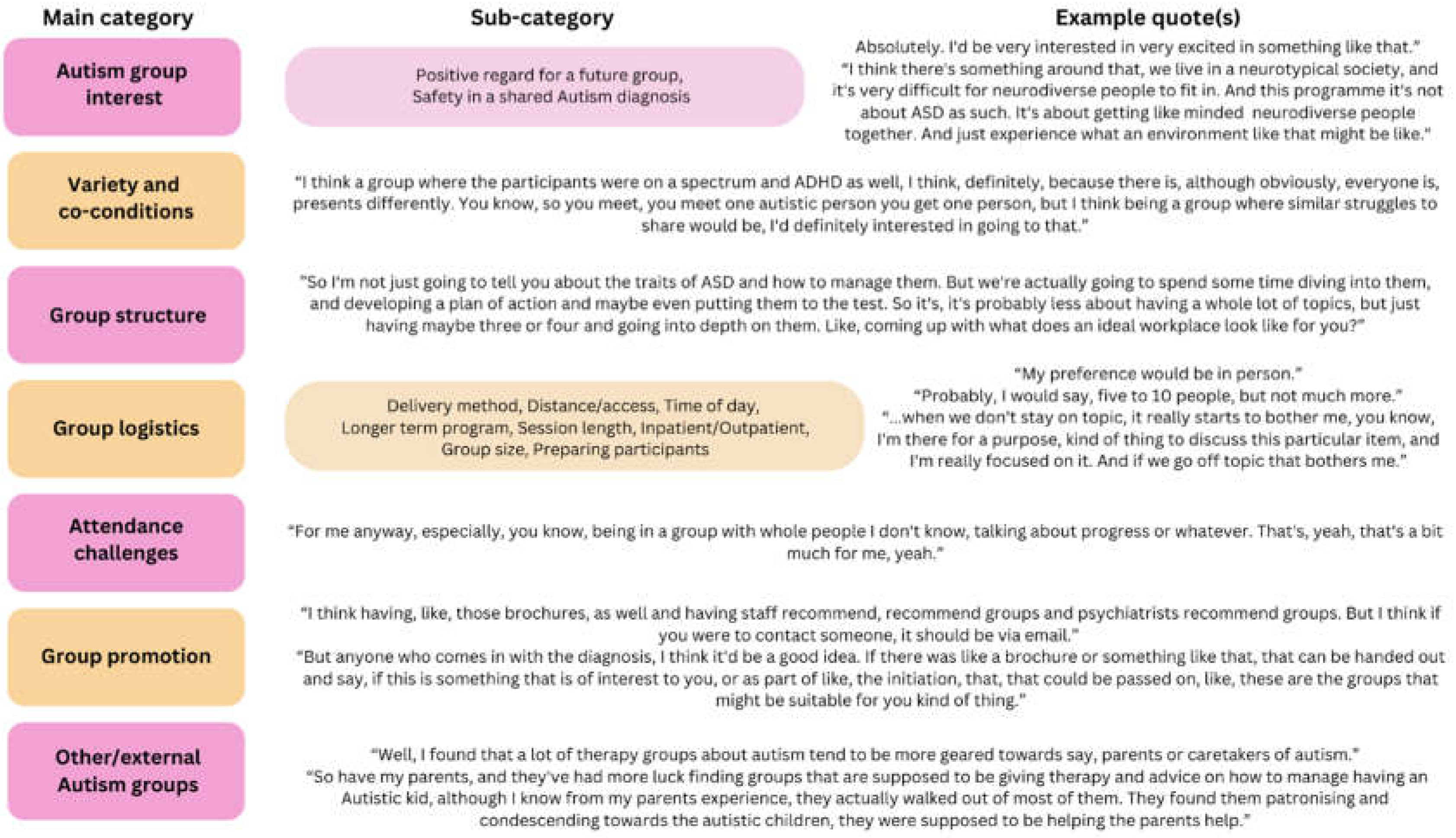
Figure 3.
Key Response Area – Topics to Cover in an Autism Group.
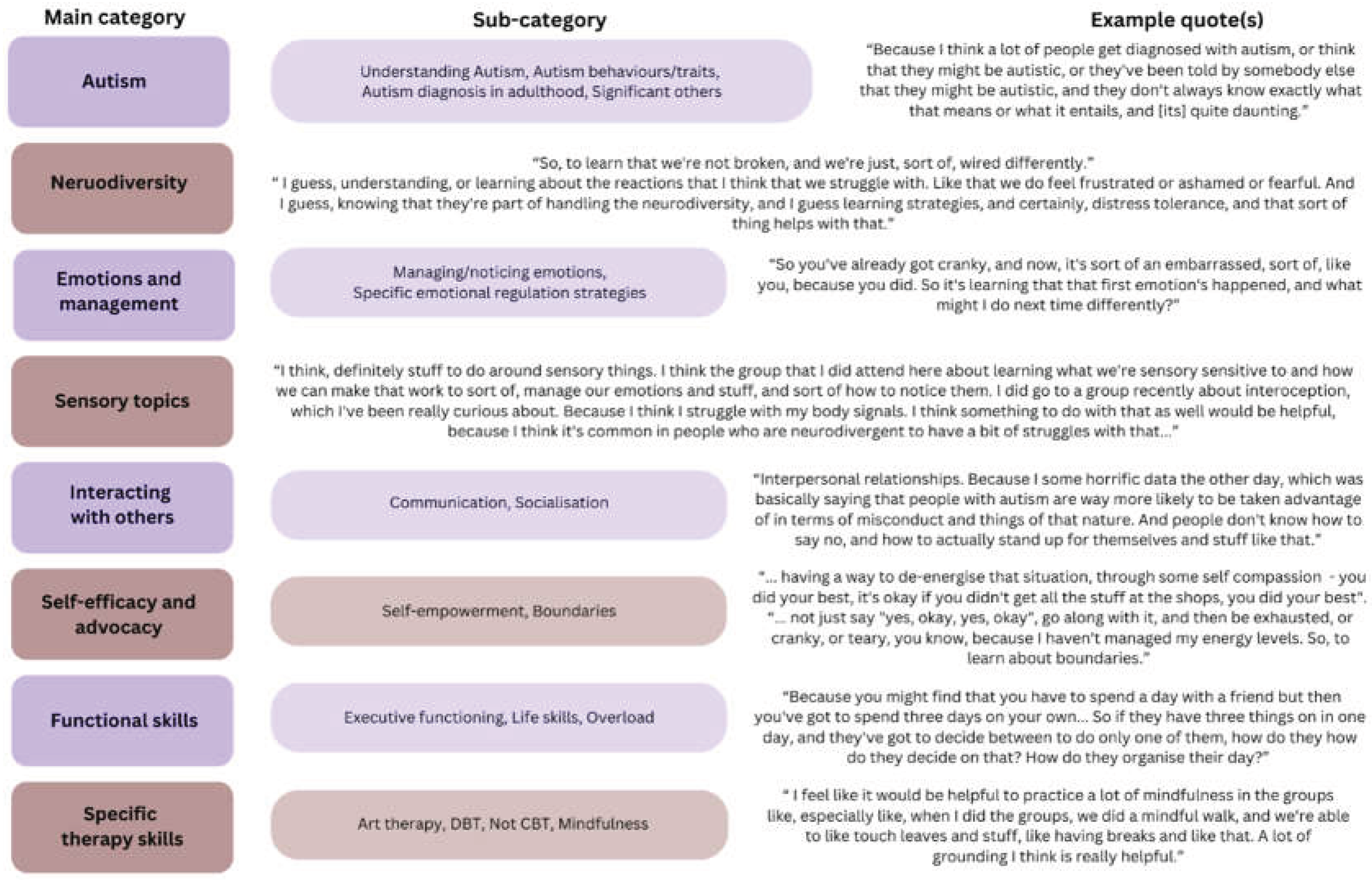
Figure 4.
Key Response Area – Concerns about Attending and Suggestions to Improve Attendance and Engagement.
Figure 4.
Key Response Area – Concerns about Attending and Suggestions to Improve Attendance and Engagement.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



