
Submitted:
29 January 2026
Posted:
30 January 2026
You are already at the latest version
Abstract
Background/Objectives: An effective inferior alveolar nerve block (IANB) is critical for mandibular third molar surgery, especially for novice student operators who face steep learning curves. This study compared the clinical efficacy and safety of 4% articaine, 2% lidocaine, and 2% mepivacaine in an undergraduate setting. Methods: A prospective observational study was conducted with 189 patients undergoing third molar surgery performed by dental students. Patients received either 4% articaine (n=69), 2% lidocaine (n=61), or 2% mepivacaine (n=59). Anesthetic efficacy was evaluated using a two-stage assessment comprising Vincent’s sign (Stage 1) and profound surgical anesthesia (Stage 2). Intra- and postoperative pain, anesthetic volume, surgical duration, and postoperative complications were recorded and compared among anesthetic groups. Results: Baseline demographics, impaction patterns, and difficulty indices did not differ significantly among groups. Stage 2 profound success rate was significantly higher with articaine (76.8%) than with lidocaine (55.7%) and mepivacaine (61.0%) (p=0.031). Articaine was also associated with a longer duration of anesthesia (261.7 vs. 164.6 and 192.6 min; p < 0.001), a lower total anesthetic volume (2.1 vs. 2.4 and 2.3 mL; p = 0.007), and significantly lower intraoperative pain scores (14.3 vs. 31.0 and 29.8 mm on the HPS; p < 0.001). Postoperative pain through Day 7 and complication rates were comparable among anesthetics, with no serious adverse events reported. Conclusions: Four percent articaine appeared to be superior to 2% lidocaine and 2% mepivacaine in student-led third molar surgery. Its high efficacy and enhanced tissue diffusion may partially compensate for technical inexperience and prolonged surgical duration, supporting its routine use to improve patient comfort and student confidence in the dental education setting.
Keywords:
local anesthesia
; articaine
; undergraduate student
; third molar surgery
; dental education
1. Introduction
Mandibular third molar surgery requires effective inferior alveolar nerve block (IANB) anesthesia for pain control [1,2,3]. The current knowledge indicates that this method of administering local anesthesia has a failure rate of up to 35% due to the diverse physical characteristics of patients [4,5,6]. Undergraduate clinical training in lower third molar surgery is commonly undertaken during the penultimate or final year of dental school, at a stage when operator competence in anesthetic administration and surgical skills is still developing [7,8,9]. Undergraduate settings face heightened risks: residents report 14.6% complication rates (pain, trismus, dry socket) versus experienced surgeons. Novice operators may experience IANB failure rates up to two to three times higher than those of experienced clinicians, attributed to imprecise needle positioning and an increased likelihood of repeat injections and neurotoxicity [10,11,12]. Local anesthetics commonly used for third molar surgery—2% lidocaine, 2% mepivacaine, and 4% articaine—are often combined with vasoconstrictors to prolong anesthetic effects and improve hemostasis, both of which are critical for surgical efficacy [13,14]. Several studies have compared the efficacy of local anesthetic agents in various dental procedures [15,16]. Recent meta-analyses support the superiority of 4% articaine (1:100,000 epinephrine) over 2% lidocaine for third molar surgery, with higher success rates, reduced onset time, better intraoperative pain control, and prolonged duration [17], attributes compensating for novice technical variability. A 2024 randomized controlled trial reported a significantly lower need for supplemental injections with articaine compared with lidocaine in third molar extractions (p < 0.05) [18]. Nonetheless, gaps in knowledge persist concerning the optimal anesthetic agent for the mandibular third molar surgery in undergraduate clinics. However, randomized controlled trial (RCT) in this setting face significant logistical and ethical hurdles; the high number of participating students and the inherent lack of standardized surgical experience make strict variable control difficult to achieve without disrupting the educational process. Therefore, the objective of this prospective observational cohort study was to compare two-stage IANB success and efficacy among 4% articaine, 2% lidocaine, and 2% mepivacaine in an undergraduate oral surgery clinical setting.
2. Materials and Methods
2.1. Study Setting and Operators
This was a prospective observational cohort in the undergraduate oral surgery clinic, Department of Oral Surgery, Faculty of Dentistry, Naresuan University. The observational design was selected to reflect the authentic clinical environment of undergraduate training, where strict randomization is often impractical due to the high volume of diverse student operators. The operators were 5th-6th year dental students on clinical rotations, which all of the students had experience with third molar surgery fewer than ten cases. The difficulty level of the cases was determined to be appropriate for the pre-graduate level according to the department’s criteria (the slightly to moderately difficult Pederson difficulty index) [19]. This research was conducted in accordance with the Helsinki Declaration and was approved by the ethics committee of Naresuan University, Thailand (approval COA No. 306/2024). The study protocol was registered at the Thai Clinical Trials Registry (TCTR Identification Number: TCTR20260110004)
Inclusion Criteria:
- Presence of at least one mandibular third molar requiring surgical extraction, with the diagnosis and surgical necessity confirmed by a supervising oral surgeon.
- Case difficulty met the criteria for undergraduate student management and was defined as slightly to moderately difficult according to the Pederson Difficulty Index (Class I–II ramus relationship; mesioangular, horizontal, or vertical impaction; Level A–B depth).
- Age 18–45 years.
- Provided written informed consent after reviewing the study information.
Exclusion Criteria:
- Presence of local pathology, including periodontitis, pulpitis, apical periodontitis, or pericoronitis.
- Preoperative pain at the surgical site.
- Use of analgesic medications within 2 weeks prior to surgery.
- Known allergy to ibuprofen or any local anesthetic agent.
- Behavioral or psychiatric conditions impairing pain assessment, or communication barriers.
- Inability to attend the Day 7 postoperative follow-up.
Discontinuation Criteria:
- Terminated from research due to supervising faculty intervention; required manual/physical assistance from the supervisor beyond verbal guidance to ensure patient safety or successful extraction
- Intraoperative emergency threatened safety, or participant withdrew consent.
2.2. Sample Size Calculation
The sample size was determined a priori using G*Power software (version 3.1.9.7; Franz Faul, University of Kiel, Kiel, Germany). For a three-group chi-square comparison of Stage 2 profound IANB success, a minimum of 57 participants per group (total n=171) was required to achieve 80% power (1-β = 0.80) at a significance level of α = 0.05. The final analysis included 189 patients (n=69 for articaine, n=61 for lidocaine, and n=59 for mepivacaine). A post-hoc analysis confirmed that this final sample size provided sufficient power to detect the observed significant difference in profound success rates (76.8% vs. 55.7% and 61.0%; p = 0.031).
2.3. Clinical Procedure Protocol
Following informed consent, patients received detailed study explanations. Patients were instructed to rate the pain experienced via the 170 mm line Heft-Parker VAS pain scale (HPS) [20]. All patients signed approval after Q&A, medical histories were reviewed for comorbidities, allergies, and third molar symptoms while confirming inclusion/exclusion criteria. Under close faculty supervision, 5th or 6th year students administered the initial 1.5 ml of the local anesthetic solution to anesthetize the inferior alveolar nerve and lingual nerve, and the 0.3 ml remaining solution was administered to anesthetize the long buccal nerve. The injection speed was performed at 2 mL/min (~100 sec) using a standard syringe with a 27-gauge 30-mm-long needle (Disposable Dental Needles, J Morita, Connecticut, United States). The prepackaged 1.8 mL local anesthetics utilized in this study include:
- 2% lidocaine hydrochloride with epinephrine 1:100,000 (Lignospan standard, Septodent, France);
- 2% mepivacaine hydrochloride with epinephrine 1:100,000 (Scandonest 2%, Septodent, France);
- 4% articaine hydrochloride with epinephrine 1:100,000 (Artinibsa 4%, Inibsa, Spain).
Onset was assessed from injection start to subjective Vincent’s sign (lower lip numbness). After 10 min of full anesthesia verification (lip numbness + buccal mucosa), surgery proceeded if profound; otherwise, the same-anesthetic supplementation occurred: buccal deficiency via local infiltration of 0.3 mL, incomplete IANB via repeat of 1.2 mL (adjusted position), or intraoperative failure (tooth sectioning/elevation pain) via intraligamentary/intrapulpal injection of 0.6 mL. The sulcular full-thickness mucoperiosteal flap was elevated from the distal line angle of the lower first molar. Bone undercut removal or tooth splitting was done when necessary. The primary closure was performed using 4/0 silk suture. To mitigate operator-related bias and the inherent technical variability of the novice operators, all participating 5th- and 6th-year dental students underwent a standardized didactic and preclinical simulation workshop before the clinical rotation. Under faculty supervision, students were restricted to verbal guidance only; any case requiring physical faculty intervention (n = 24) was excluded from the final analysis to ensure that the reported success rates reflected purely student performance. Clinical photographs illustrating the basic procedure for mandibular third molar surgery by undergraduate students are shown in Figure 1.
Intraoperative HPS was recorded immediately post-extraction, the participants placed a mark on the 170 mm scale where it best described their pain level. Total volume measured post-procedure via syringe markings. Standard surgical extractions followed with faculty oversight. Post-operatively, patients were administered ibuprofen 400 mg as needed (discontinue medication when HPS=0). Amoxicillin 500 mg entire regimen, including documentation for post-operative pain onset at 24 h (D1), 72 h (D3), and 168 h (D7). Day 7 suture removal assessed complications (infection, swelling, dry socket, trismus <35 mm) with coded data entry. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement guidelines for prospective cohort studies [21]. Figure 2 shows the STROBE flow diagram representing participant recruitment and study progression. The chart details the standardized surgical protocol performed by 117 novice operators, the predefined rescue anesthesia steps, and the exclusion of 24 cases requiring faculty intervention to maintain the integrity of the novice-performance data. Final analysis was conducted on 189 cases across the three anesthetic cohorts
2.4. Primary and Secondary Outcomes
The primary outcome was IANB success, categorized into two clinical levels:
- Objective Sensory Blockade (Stage 1 success): Presence of Vincent’s sign and no pain upon sharp probing of the labial mucosa near the lower canine at 10 minutes post-injection.
- Complete Surgical Anesthesia (Stage 2 success): Successful completion of the entire surgical procedure without the need for any supplemental anesthetic injections, which was defined as the ability to perform the surgery with no or weak pain (HPS rating ≤36 mm)
Secondary outcomes obtained in this study include:
- Onset (min): documented from the time of injection to the start of ipsilateral lip anesthetic as subjective symptoms.
- Surgical duration (min): recorded from the time the incision was made until the last stitch was applied.
- Anesthetic duration (min): recorded the start of ipsilateral lip anesthetic as subjective symptoms to the return of normal sensation in the lower lip, tongue, and alveolar mucosa.
- Total anesthetic volume (mL): the cumulative volume (mL) of all local anesthetic injections administered during the surgical procedure, including any supplemental injections.
- Intra-operative pain (HPS): the pain intensity during the surgical procedure, assessed immediately after surgery using the Heft–Parker Visual Analogue Scale.
- Post-operative Pain at D1, D3, and D7 (HPS): the pain intensity assessed at 24, 72, and 168 hours after surgery using the Heft–Parker Visual Analogue Scale.
- Post-operative complications: the complications assessed on the seventh day after surgery, including infection, swelling, dry socket, and trismus (maximum mouth opening < 35 mm).
2.5. Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) software version 26.0 (IBM Corp., Armonk, NY, USA) was used for analyzing the data. For continuous variables, we used descriptive statistics including means, standard deviations (SD), and standard errors of the mean (SEM). For categorical variables, we used frequencies and percentages. Specifically, SEM was utilized to present the precision of mean pain intensity at various time points in the pain profile graph to facilitate a clearer visual comparison of anesthetic efficacy. The Shapiro-Wilk test was utilized to verify when the continuous data distribution, such as the onset, duration, surgical time, and pain scores, was normal. The data met the criteria for parametric analysis; therefore, one-way analysis of variance (ANOVA), performed by Tukey’s post-hoc test, was utilized to compare the mean values among the three anesthetic groups (articaine, lidocaine, and mepivacaine. The Pearson’s chi-square test was used for categorical outcomes, including the success rates of Vincent’s sign (Stage 1) and profound anesthesia (Stage 2), and the rates of postoperative complications. Fisher’s exact test was used when the expected number of cells was less than five. Pairwise comparisons between groups for categorical data were performed using chi-square tests with Bonferroni correction to identify specific differences. The p-value for all tests was set at 0.05.
3. Results
3.1. Baseline Demographic Characteristics of the Patients
Based on the inclusion criteria, a total of 189 mandibular third molar surgeries performed by 5th–6th year dental students were included in the final analysis. Participants were recruited between January 2024 and December 2025. Patient baseline characteristics, including age, sex distribution, impaction pattern, and Pederson difficulty index, were comparable among the articaine, lidocaine, and mepivacaine cohorts (Table 1). No significant inter-group differences were observed in demographic or radiographic baseline parameters (p>0.05).
3.2. Anesthetic Efficacy and Success Rates
Regarding the primary outcome, Stage 1 objective sensory block (Vincent’s sign with negative sharp probing at 10 minutes) was achieved in a high proportion of cases across all three anesthetic agents, without a statistically significant difference between groups (p>0.05). Stage 2 complete surgical anesthesia, defined as case completion without any supplemental injections, showed 4% articaine with 1:100,000 epinephrine achieved a significantly higher Profound Success Rate (Stage 2) at 76.8% (53/69), compared to 55.7% (34/61) for lidocaine and 61.0% (36/59) for mepivacaine (Figure 3). Most failures in all cohorts were managed effectively with protocolized rescue strategies, including supplemental IANB, local infiltration, or intraligamentary injections, and did not necessitate case abandonment.
3.3. Anesthesia Duration vs. Surgical Time and Pain Intensity
The onset of anesthesia was similar across all groups, with mean times ranging from 2.1 to 2.2 minutes (p = 0.133). However, the duration of anesthesia was significantly longer for articaine (261.7 ± 34.8 min) compared to lidocaine (164.6 ± 48.3 min) and mepivacaine (192.6 ± 33.0 min) (p < 0.001). The mean surgical duration was 67.6 ± 21.8 minutes for articaine, 73.1 ± 23.1 minutes for lidocaine, and 78.1 ± 27.9 minutes for mepivacaine (p = 0.054). When comparing the “safety buffer” (anesthesia duration minus surgical time), articaine provided the most substantial window for instructional delays and faculty verification (Figure 4).
3.4. Total Anesthetic Volume and Intra-Operative Pain
Articaine achieved superior pain control with a lower volume of anesthetic. The total volume used in the articaine group (2.1 ± 0.5 mL) was significantly lower than in the lidocaine (2.4 ± 0.8 mL) and mepivacaine (2.3 ± 0.8 mL) groups (p = 0.007). Crucially, intra-operative pain scores (HPS) were significantly lower for articaine (14.3 ± 10.8) compared to lidocaine (31.0 ± 12.6) and mepivacaine (29.8 ± 8.8) (p < 0.001). The mean HPS scores in the articaine group were consistently maintained within the “no pain to faint pain” range (0–23 mm) throughout the procedure. Figure 5 shows box-and-whisker plots of the total anesthetic volume and intraoperative pain scores.
3.5. Post-Operative Pain and Complications
The pain intensity profile from the intra-operative phase to postoperative Day 7 is illustrated in Figure 6. Postoperative pain assessed by HPS at Day 1, Day 3, and Day 7 followed the expected temporal decline in all groups, with the highest scores at 24 hours and progressive reduction by Day 7. There were no statistically significant differences in postoperative pain trajectories among articaine, lidocaine, and mepivacaine at any timepoint (p>0.05). Regarding postoperative morbidity, the incidence of complications was low and did not differ significantly between groups (p > 0.05). Dry socket occurred in 1.4%, 3.3%, and 1.7% of patients in the articaine, lidocaine, and mepivacaine groups, respectively. Jaw trismus was reported in 4.3% (articaine), 4.9% (lidocaine), and 5.1% (mepivacaine) of cases. No severe adverse reactions or neurological complications were observed during the follow-up period, indicating similar safety profiles under routine undergraduate supervision.
4. Discussion
This real-world observational study highlights the clinical advantages of 4% articaine over 2% lidocaine and 2% mepivacaine in the context of mandibular third molar surgery performed by undergraduate dental students. Our findings demonstrate that articaine not only provides a higher rate of profound anesthesia but also significantly reduces intraoperative pain despite a lower total volume of anesthetic used. The mean surgical duration in this study (approximately 67–78 minutes) is notably longer than durations reported for general practitioners or oral surgeons, which typically range from 15 to 30 minutes for similar difficulty levels [22,23,24].
This extended duration and the inherent technical challenges faced by students can be explained by the learning curve of third molar surgery. A prospective cohort study identified a critical proficiency milestone after the completion of approximately 10 cases, after which surgical time and complications significantly decrease. As the undergraduate students in this study were in their initial learning phase—often performing their first few clinical cases—they had not yet reached this stability milestone [25]. Beyond surgical dexterity, the educational protocol requires step-by-step verification by supervising faculty at critical stages (e.g., flap design, bone removal, tooth sectioning). Research by Sánchez-Torres et al. supports this, noting that surgical time is greatly prolonged when procedures are conducted by students, owing to both precise technique and the educational necessity for intraoperative evaluation [26]. In this “stop-and-go” environment, the prolonged duration places a premium on the “safety buffer” provided by the anesthetic’s duration. Articaine’s significantly longer duration of action (262 min) compared to lidocaine (165 min) and mepivacaine (193 min) provides students with a larger window to complete the surgery without the stress of waning anesthesia, which often leads to higher intraoperative pain.
The clinical superiority of articaine observed in this study is consistent with a previous finding. Muhammad et al. reported that 4% articaine significantly improved IANB success rates for simple exodontia performed by students [27]. This advantage is particularly crucial for novice operators; articaine’s unique thiophene ring and higher lipid solubility enhance its ability to penetrate dense cortical bone and lipid-rich nerve membranes [1,28,29]. As suggested by a previous study, these superior diffusion properties may compensate for imprecise needle placement, a common technical error among students who may not yet have mastered the precise anatomical localization of the mandibular foramen [27]. Consequently, articaine achieved a higher profound success rate (78.3%) in our study, reducing the need for stressful supplemental injections and enhancing overall operator confidence during the early stages of clinical training.
A key strength of this study is the two-stage assessment, distinguishing subjective nerve blockade (Stage 1) from surgical anesthesia (Stage 2). This reveals that while Stage 1 is often achieved, articaine is significantly more reliable in reaching the pulpal and bone-cutting depth required for Stage 2. Despite its efficacy, the use of 4% articaine in IANB remains a subject of debate due to concerns regarding neurotoxicity and paresthesia. Retrospective studies, such as those by Haas and Lennon, suggested a higher incidence of nerve injury associated with 4% solutions [30]. However, this controversy has been largely mitigated by more recent prospective clinical trials and systematic reviews. Martin et al. and a large-scale meta-analysis by Nogueira et al. found no statistically significant difference in the incidence of permanent nerve damage between articaine and other amides [17,31]. The consensus in contemporary literature suggests that nerve injury is more likely related to mechanical trauma from the needle or the surgical procedure itself rather than the chemical properties of Articaine [32,33]. In our study, no cases of permanent paresthesia were recorded, supporting the safety of 4% articaine when administered with proper technique.
This study has several limitations. First, its observational design could introduce selection bias, as operators chose the anesthetic agent themselves. However, baseline patient characteristics and tooth difficulty were comparable across all groups. Second, pain perception is subjective and may be influenced by patient anxiety, which was not measured. Lastly, the seven-day follow-up period was insufficient to detect rare, long-term neurosensory changes. Future studies should use a double-blind, randomized controlled trial (RCT) with a more standardized selection of operators. To reduce errors, students should be screened and grouped according to their surgical experience or clinical scores.
The findings of this study offer several implications for dental education and clinical practice:
- Managing Educational Delays: 4% articaine should be the first choice for student-led surgeries as it provides them a “safety window” against the longer surgery times that come from faculty verification checkpoints.
- Mitigating Novice Technical Variability: Articaine’s strong pharmacological effects compensate for the imprecise IANB techniques novice operators often utilize.
- Optimizing Patient Comfort: Articaine improves the patient experience and decreases the risk of systemic toxicity by lowering the total volume requirements.
5. Conclusions
In conclusion, 4% articaine is superior to 2% lidocaine and 2% mepivacaine for mandibular third molar surgery performed by undergraduate dental students. Articaine achieved a significantly higher rate of profound anesthesia success and maintained lower intraoperative pain scores despite a lower total volume of anesthetic solution. While all three agents showed similar postoperative pain profiles and complication rates, articaine’s unique pharmacological properties provided a critical margin of safety and predictability that is particularly beneficial during the early stages of clinical training. These results support the routine adoption of 4% articaine to enhance both surgical success and patient experience in dental educational settings.
Author Contributions
Conceptualization, T.S. and T.E.; methodology, T.E., R.T. and K.R.; formal analysis, P.R., P.T. and P.E.; investigation, P.R., P.T. and P.E.; data curation, T.S. and T.E.; writing—original draft preparation, T.S., T.E., R.T. and K.R.; writing—review and editing, T.S., T.E., R.T. and K.R.; supervision, T.S. and T.E.; project administration, T.S. and T.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the faculty of dentistry grant, Naresuan University.
Institutional Review Board Statement
This research was conducted in accordance with the Helsinki Declaration and was ap-proved by the ethics committee of Naresuan University, Thailand (approval COA No. 306/2024). The study protocol was registered at the Thai Clinical Trials Registry (TCTR Identification Number: TCTR20260110004).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are provided within the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ANOVA | Analysis of variance |
| HPS | Heft-Parker VAS pain scale |
| IANB RCT STROBE |
Inferior alveolar nerve block Randomized controlled trial Strengthening the Reporting of Observational Studies in Epidemiology |
References
- Huang, N.-C.; Chang, H.-H.; Lin, C.-P. Efficacy and safety of infiltration anesthesia with 4% Articaine and block anesthesia with 2% Lidocaine in the mandibular third molar extraction. Journal of Dental Sciences 2025, 20, 1139–1147. [Google Scholar] [CrossRef]
- Goyal, R.; Sharma, P.; Bali, R. Comparative Analysis of the Anesthetic Efficacy of 0.5% Ropivacaine Versus 2% Lignocaine Hydrochloride with Adrenaline (1:80,000) for Inferior Alveolar Nerve Block in Surgical Removal of Impacted Mandibular Third Molars. J. Maxillofac. Oral Surg. 2021, 20, 234–239. [Google Scholar] [CrossRef]
- Li, Z.; Yang, M.; Liao, T.; Zhou, Y.; Yue, H.; Piao, Z.; Zhou, L. Combined inferior alveolar nerve block anaesthesia and local infiltration anaesthesia in extraction of impacted mandibular third molars: a randomised controlled trial. Br. Dent. J. 2020. [Google Scholar] [CrossRef]
- Bicsák, Á.; Esser, L.; Hassfeld, S.; Bonitz, L. An in-silico comparison of success rate of different methods for inferior alveolar nerve blockade. Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology 2025, 37, 935–940. [Google Scholar] [CrossRef]
- Chen, H.-S.; Hsu, K.-J.; Chen, P.-J.; Lee, H.-N.; Chen, J.H.; Chen, C.-M. Investigating the relation among the needle insertion plane, occlusal plane, mandibular foramen, and mandibular lingula for inferior alveolar nerve block. Journal of Dental Sciences 2025, 20, 1792–1801. [Google Scholar] [CrossRef]
- Kaya Mumcu, A.; Gündüz, M.; Kiraz, G.; Koldemir Gündüz, M. Effect of dental anxiety on the success of inferior alveolar nerve block in symptomatic irreversible pulpitis: A prospective clinical study. Journal of Dental Sciences 2025. [Google Scholar] [CrossRef]
- Sanchez Jorge, M.I.; Ocana, R.A.; Valle Rodriguez, C.; Peyro Fernandez-Montes, B.; Rico-Romano, C.; Bazal-Bonelli, S.; Sanchez-Labrador, L.; Cortes-Breton Brinkmann, J. Mandibular third molar extraction: perceived surgical difficulty in relation to professional training. BMC Oral Health 2023, 23, 485. [Google Scholar] [CrossRef] [PubMed]
- Sakka, S.; Alqhtani, N.R.; Alqahtani, A.S.; Nabhan, A.B.; Eid, M.K.; Alagla, M.; Alfaifi, K.; Nassani, M.Z. Dental students, interns, and junior dentists’ awareness and attitude toward the inferior alveolar nerve block technique and related failure. Journal of Dental Sciences 2024, 19, 2315–2322. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-L.; Chiu, Y.-W.; Yu, C.-H.; Chang, Y.-C.; Chen, Y.-T. Flipped classroom teaching model with video instruction improves skills in local anesthesia training. Journal of Dental Sciences 2024, 19, 1070–1074. [Google Scholar] [CrossRef]
- de Abreu, J.M.; Cerqueira, É.; Quitério, A.; Nunes, T.; Figueiredo, J.; Corte-Real, A. Assessment of complications in third molar surgery performed by resident surgeons: A comprehensive analysis. Surg Pract Sci 2024, 18, 100256. [Google Scholar] [CrossRef]
- AlHindi, M.; Rashed, B.; AlOtaibi, N. Failure rate of inferior alveolar nerve block among dental students and interns. Saudi Med. J. 2016, 37, 84–89. [Google Scholar] [CrossRef]
- Rizqiawan, A.; Lesmaya, Y.D.; Rasyida, A.Z.; Amir, M.S.; Ono, S.; Kamadjaja, D.B. Postoperative Complications of Impacted Mandibular Third Molar Extraction Related to Patient’s Age and Surgical Difficulty Level: A Cross-Sectional Retrospective Study. Int J Dent 2022, 2022, 7239339. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Hwang, K.G.; Park, C.J. Local anesthesia for mandibular third molar extraction. J Dent Anesth Pain Med 2018, 18, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Govind, S.; Jena, D.; Dash, S.; Jena, S.P.; Yadav, D.; Karan, S.; Kancherla, J.; Jena, A.; Mishra, L.; et al. Local Anesthesia Onset and Pain Perception in Hemophilic and Thalassemic Conditions. Journal of clinical medicine 2023, 12, 3646. [Google Scholar] [CrossRef] [PubMed]
- De Grado Gabriel, F.; Clement, B.; Florence, F.; Anne-Marie, M.; Damien, O. Efficacy of Articaine or Eugenol for Pain Relief after Emergency Coronal Pulpotomy in Teeth with Irreversible Pulpitis: A Randomized Clinical Trial. Dent J (Basel) 2023, 11. [Google Scholar] [CrossRef]
- Manteca-Fernandez, L.; Meniz-Garcia, C.; Fernandez-Caliz, F.; Barona-Dorado, C.; Santos-Marino, J.; Martinez-Rodriguez, N. Influence of Premedication and Dental Anxiety on Anesthetic Efficacy in Patients Undergoing Root Canal for Symptomatic Irreversible Pulpitis in Upper and Lower Molars: A Comparative Study of Articaine and Bupivacaine. Dent J (Basel) 2025, 13. [Google Scholar] [CrossRef]
- Nogueira, E.C.; Almeida, R.A.; de Souza, B.L.; Aguiar, P.L.; Vasconcellos, R.H. Why choose articaine over lidocaine for the removal of third molars? Systematic review and meta-analysis. J Clin Exp Dent 2023, 15, e963–e977. [Google Scholar] [CrossRef]
- Javed, M.; Alam, M.A.; Arooj, Z.; Asghar, H.; Haroon, K.H.; Mustafa, Q. Comparing the Efficacy of Articaine and Lignocaine in Maxillary Irreversible Pulpitis: A Randomized Triple Blind Study. Proceedings 2024, 38, 233–238. [Google Scholar] [CrossRef]
- Achararit, P.; Manaspon, C.; Jongwannasiri, C.; Kulthanaamondhita, P.; Itthichaisri, C.; Chantarangsu, S.; Osathanon, T.; Phattarataratip, E.; Sappayatosok, K. Impacted lower third molar classification and difficulty index assessment: comparisons among dental students, general practitioners and deep learning model assistance. BMC Oral Health 2025, 25, 152. [Google Scholar] [CrossRef]
- Heft, M.W.; Parker, S.R. An experimental basis for revising the graphic rating scale for pain. Pain 1984, 19, 153–161. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. The Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Roca, J.A.; Donoso-Martínez, B.; Ameneiros-Serantes, S.; Martínez-Beneyto, Y.; Salmerón-Martínez, D.; Gay-Escoda, C. Influence of operator’s professional experience in the postoperative course after surgical extrac-tion of the impacted lower third molar: A pilot study. J Clin Exp Dent 2020, 12, e805–e812. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, M.; Fieuws, S.; Jacobs, R.; Politis, C. Surgical experience and patient morbidity after third molar removal. Journal of Stomatology, Oral and Maxillofacial Surgery 2022, 123, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Benediktsdóttir, I.S.; Wenzel, A.; Petersen, J.K.; Hintze, H. Mandibular third molar removal: Risk indicators for extended operation time, postoperative pain, and complications. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 2004, 97, 438–446. [Google Scholar] [CrossRef]
- Komerik, N.; Muglali, M.; Tas, B.; Selcuk, U. Difficulty of Impacted Mandibular Third Molar Tooth Removal: Predictive Ability of Senior Surgeons and Residents. J. Oral Maxillofac. Surg. 2014, 72, 1062.e1061–1062.e1066. [Google Scholar] [CrossRef]
- Sánchez-Torres, A.; Sabreen, E.; Arias-Huerta, X.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellón, E.; Gay-Escoda, C. Learning Curve in the Extraction of Impacted Lower Third Molars: A Prospective Cohort Study. Eur. J. Dent. Educ. 2025, 29, 266–276. [Google Scholar] [CrossRef]
- Muhammad, Z.A.; Abdullah, R.M.; Majid, O.W. Articaine improves anesthetic achievement for exodontia performed by undergraduate dental students: A clinical comparative study. J. Dent. Educ. 2021, 85, 1702–1709. [Google Scholar] [CrossRef]
- Rao, J.K.D.; Alnasser, A.A.; Alotaibi, K.Z.; Altwaijri, A.; Alharbi, G.M.; Aljaber, S.s. Efficacy and Safety of 4% Articaine Versus 2% Mepivacaine After Surgical Removal of Impacted Lower Third Molars: A Double Bind Clinical Trial. J. Maxillofac. Oral Surg. 2025. [Google Scholar] [CrossRef]
- Malamed, S.F.; Gagnon, S.; Leblanc, D. Articaine hydrochloride: a study of the safety of a new amide local anesthetic. J. Am. Dent. Assoc. 2001, 132, 177–185. [Google Scholar] [CrossRef]
- Haas, D.A.; Lennon, D. A 21 year retrospective study of reports of paresthesia following local anesthetic administration. Journal (Canadian Dental Association) 1995, 61, 319-320, 323-316, 329-330. [Google Scholar]
- Martin, E.; Nimmo, A.; Lee, A.; Jennings, E. Articaine in dentistry: an overview of the evidence and meta-analysis of the latest randomised controlled trials on articaine safety and efficacy compared to lidocaine for routine dental treatment. BDJ Open 2021, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Filipe de Carvalho Nogueira, E.; Andrey da Costa Araújo, F.; Faro, T.F.; de Albuquerque Cavalcanti Almeida, R.; José de Holanda Vasconcellos, R. Does the Use of Articaine Increase the Risk of Hypesthesia in Lower Third Molar Surgery? A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2021, 79, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Stirrup, P.; Crean, S. Does articaine, rather than lidocaine, increase the risk of nerve damage when administered for inferior alveolar nerve blocks in patients undergoing local anaesthesia for dental treatment? A mini systematic review of the literature. Br. Dent. J. 2019, 226, 213–223. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Undergraduate Mandibular Third Molar Surgery Protocol. Clinical photographs illustrating key steps of mandibular third molar extraction performed by 5th–6th year dental students under faculty supervision, including (A) injection of local anesthesia, (B) flap design, (C) bone removal/tooth sectioning, and (D) primary closure with 4–0 silk sutures.
Figure 1.
Undergraduate Mandibular Third Molar Surgery Protocol. Clinical photographs illustrating key steps of mandibular third molar extraction performed by 5th–6th year dental students under faculty supervision, including (A) injection of local anesthesia, (B) flap design, (C) bone removal/tooth sectioning, and (D) primary closure with 4–0 silk sutures.
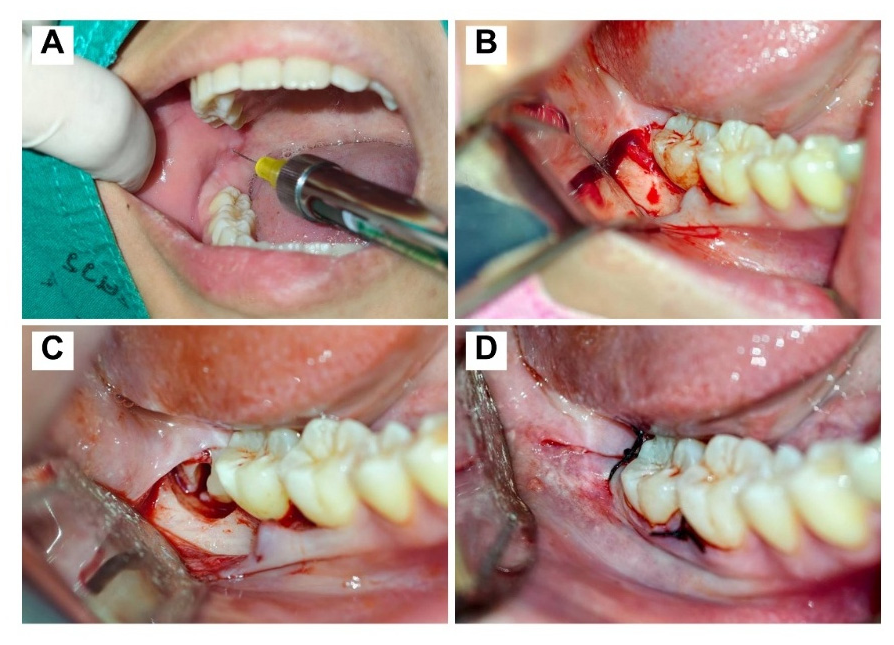
Figure 2.
STROBE Flow Diagram of Study Cohort. Flow diagram illustrating patient recruitment, the standardized surgical and rescue anesthesia protocols, and the final cohort distribution after excluding cases with faculty intervention.
Figure 2.
STROBE Flow Diagram of Study Cohort. Flow diagram illustrating patient recruitment, the standardized surgical and rescue anesthesia protocols, and the final cohort distribution after excluding cases with faculty intervention.

Figure 3.
Comparison of Anesthetic Success Rates Among Three Local Anesthetics. Bar graph comparing Stage 1 objective sensory blockade (Vincent’s sign) and Stage 2 complete surgical anesthesia among articaine, lidocaine, and mepivacaine; Stage 2 profound success is significantly higher with articaine, whereas Stage 1 success is comparable across groups. Data are presented as percentages (%). Statistical significance was determined using Pearson’s chi-square test with Bonferroni correction for multiple pairwise comparisons (asterisk p<0.05; 95% Confidence Interval error bars).
Figure 3.
Comparison of Anesthetic Success Rates Among Three Local Anesthetics. Bar graph comparing Stage 1 objective sensory blockade (Vincent’s sign) and Stage 2 complete surgical anesthesia among articaine, lidocaine, and mepivacaine; Stage 2 profound success is significantly higher with articaine, whereas Stage 1 success is comparable across groups. Data are presented as percentages (%). Statistical significance was determined using Pearson’s chi-square test with Bonferroni correction for multiple pairwise comparisons (asterisk p<0.05; 95% Confidence Interval error bars).
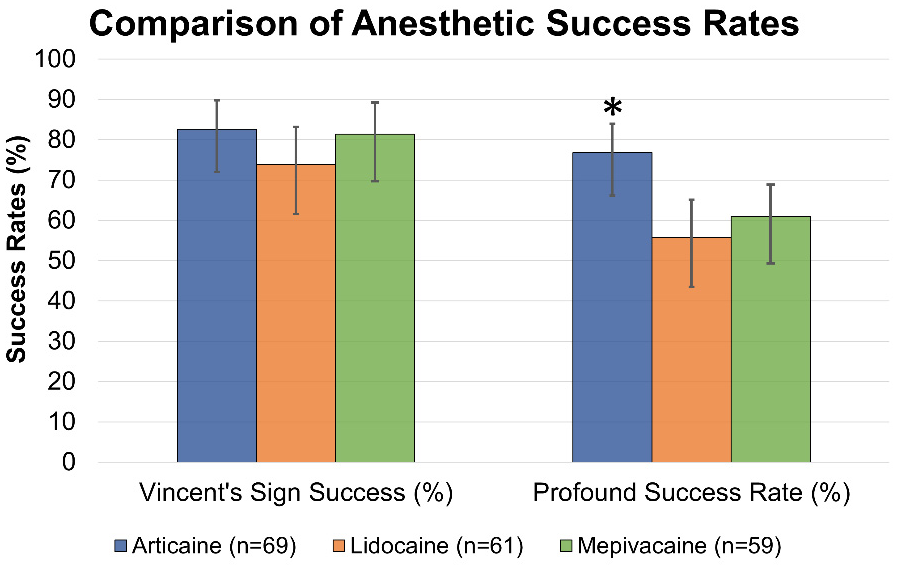
Figure 4.
Anesthesia Duration vs. Surgical Time: The “Pharmacological Buffer”. A plot showing mean anesthesia duration and mean surgical time for each anesthetic; articaine provides a substantially longer pharmacological safety buffer than lidocaine and mepivacaine for prolonged student-led procedures. Statistical comparisons were performed using one-way ANOVA followed by Tukey’s post-hoc test (asterisk p<0.05; SD error bars).
Figure 4.
Anesthesia Duration vs. Surgical Time: The “Pharmacological Buffer”. A plot showing mean anesthesia duration and mean surgical time for each anesthetic; articaine provides a substantially longer pharmacological safety buffer than lidocaine and mepivacaine for prolonged student-led procedures. Statistical comparisons were performed using one-way ANOVA followed by Tukey’s post-hoc test (asterisk p<0.05; SD error bars).
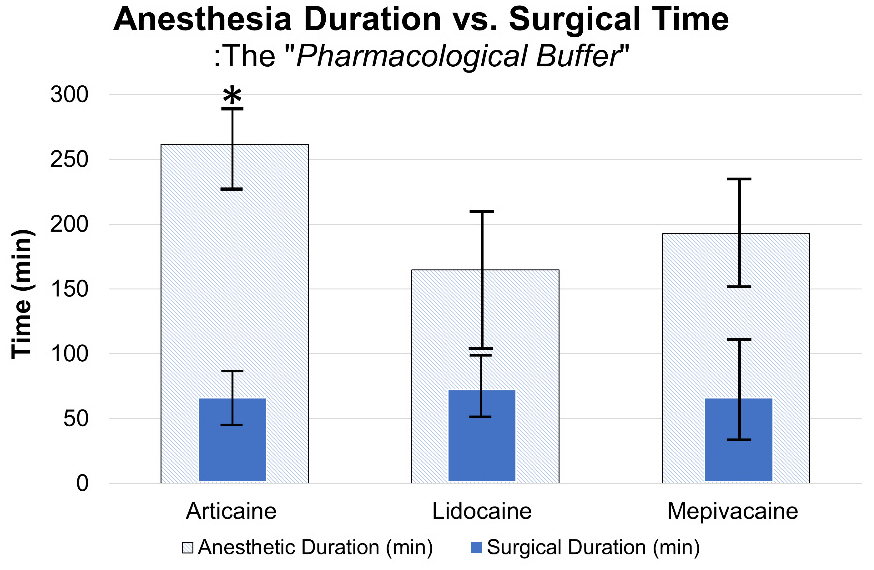
Figure 5.
Distribution of Total Anesthetic Volume and Intraoperative Pain Scores. Box-and-whisker plots illustrating total anesthetic volume and intraoperative Heft-Parker pain scores; (A) articaine requires lower volume and (B) yields pain scores concentrated within the no-to-faint pain range (0–23 mm), with significant differences versus lidocaine and mepivacaine. The box plots represent the median, quartiles, and range of the data. Significant differences were identified using one-way ANOVA and Tukey’s post-hoc test. (asterisk p<0.05).
Figure 5.
Distribution of Total Anesthetic Volume and Intraoperative Pain Scores. Box-and-whisker plots illustrating total anesthetic volume and intraoperative Heft-Parker pain scores; (A) articaine requires lower volume and (B) yields pain scores concentrated within the no-to-faint pain range (0–23 mm), with significant differences versus lidocaine and mepivacaine. The box plots represent the median, quartiles, and range of the data. Significant differences were identified using one-way ANOVA and Tukey’s post-hoc test. (asterisk p<0.05).
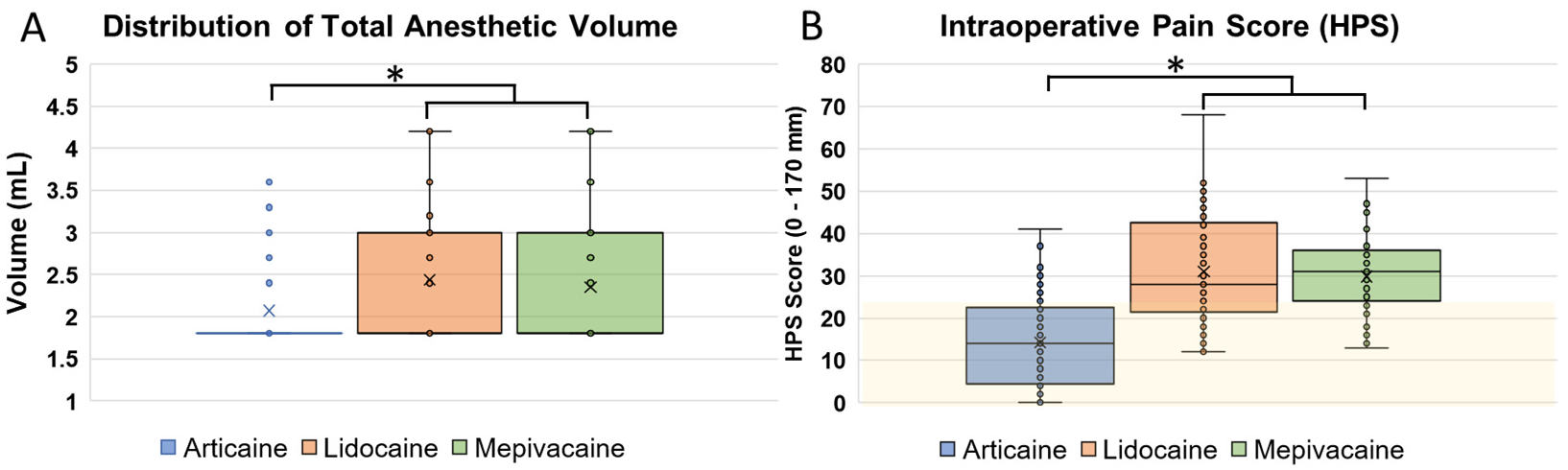
Figure 6.
Pain intensity profile (HPS) from intra-operative to postoperative Day 7. Line graph showing mean pain scores measured by the Heft-Parker Visual Analog Scale (HPS). Error bars represent the Standard Error of the Mean (SEM). Statistical analysis at each time point was conducted using one-way ANOVA with Tukey’s post-hoc test. Articaine demonstrated significantly lower intra-operative pain scores compared to other groups (p < 0.001). No significant differences were observed during the postoperative follow-up period.
Figure 6.
Pain intensity profile (HPS) from intra-operative to postoperative Day 7. Line graph showing mean pain scores measured by the Heft-Parker Visual Analog Scale (HPS). Error bars represent the Standard Error of the Mean (SEM). Statistical analysis at each time point was conducted using one-way ANOVA with Tukey’s post-hoc test. Articaine demonstrated significantly lower intra-operative pain scores compared to other groups (p < 0.001). No significant differences were observed during the postoperative follow-up period.
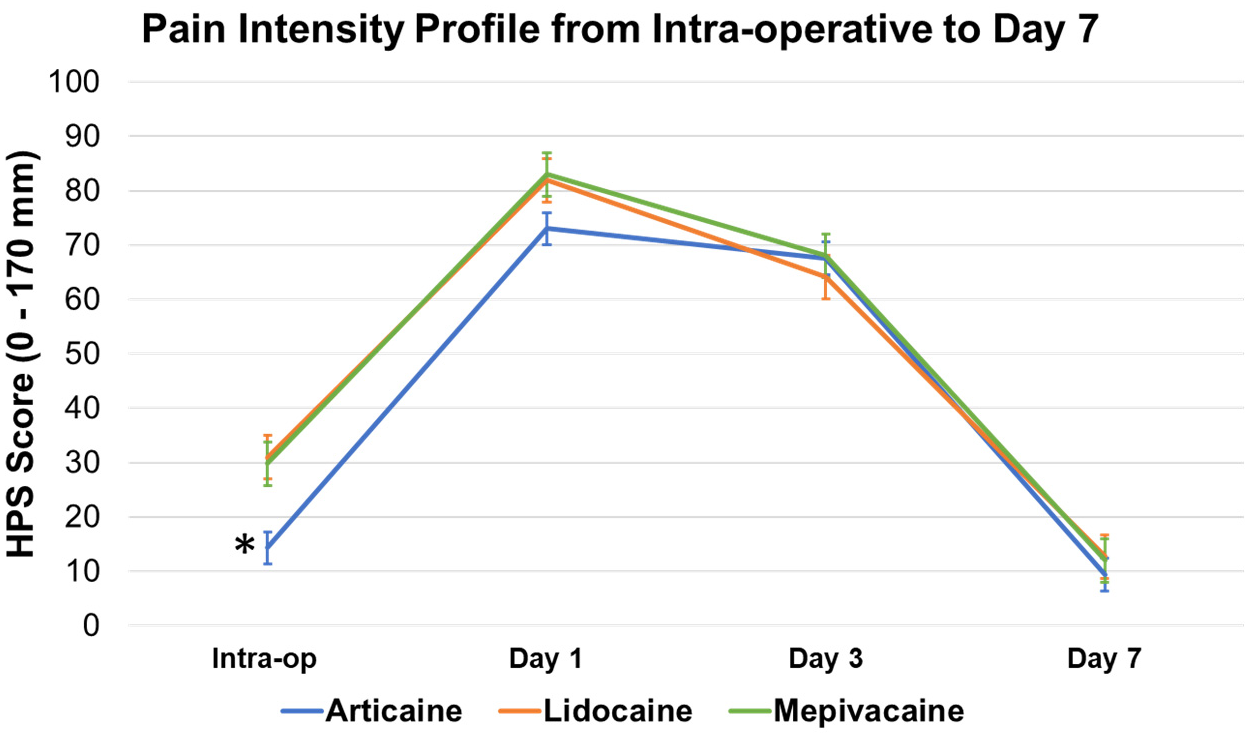

Table 1.
Baseline demographic characteristics of the patients.
| Characteristics | Articaine (n=69) |
Lidocaine (n=61) |
Mepivacaine (n=59) |
p-value |
|---|---|---|---|---|
| Age, mean (SD) | 20.4 (2.1) | 20.7 (2.3) | 20.5 (2.2) | 0.72 |
| Sex, n (%) | 0.45 | |||
| Female | 36 (52%) | 35 (57%) | 31 (53%) | |
| Male | 33 (48%) | 26 (43%) | 28 (47%) | |
| Tooth position, n (%) | 0.76 | |||
| Left third molar | 42 (61%) | 34 (56%) | 29 (49%) | |
| Right third molar | 27 (39%) | 27 (44%) | 30 (51%) | |
| Pederson Difficulty, n (%) | 0.89 | |||
| Slightly | 23 (33%) | 20 (33%) | 19 (32%) | |
| Moderately | 46 (67%) | 41 (67%) | 40 (68%) | |
1 Note: Data are expressed as mean ± standard deviation (SD) for continuous variables and as frequency (n) and percentage (%) for categorical variables. Statistical significance for continuous data (age) was evaluated using one-way analysis of variance (ANOVA). For categorical data (sex, tooth position, and difficulty index), Pearson’s chi-square test or Fisher’s exact test was applied as appropriate. A p-value < 0.05 was considered statistically significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



