
Submitted:
28 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
Many existing healthcare facilities still rely on the aging Wi-Fi 5 (IEEE 802.11ac) standard, which is based on Orthogonal Frequency-Division Multiplexing (OFDM). OFDM supports single-user-per-channel access, leading to increased contention, higher latency, jitter, and packet loss under dense device deployments commonly found in clinical settings. This study presents a quantitative performance evaluation of Wi-Fi 5 and Wi-Fi 6/7 by comparing the effectiveness of OFDM with Orthogonal Frequency-Division Multiple Access (OFDMA) and Target Wake Time (TWT) in a simulated dense IoMT environment. Simulations were conducted using Network Simulator 3 (NS-3), and key Quality of Service (QoS) metrics. The results demonstrate that OFDMA reduces average network delay by up to approximately 30%, improves throughput by approximately 20%, and reduces packet loss ratio by up to 85% compared to OFDM under high-density conditions, while exhibiting marginally improved jitter performance (approximately 2%). In addition, the use of TWT achieved substantial reductions in device power consumption of up to approximately 90%, at the cost of reduced aggregate throughput of up to approximately 75% under high station densities. These results demonstrate that Wi-Fi 6/7 technologies offer significant advantages in terms of QoS and energy efficiency over legacy Wi-Fi 5 for dense IoMT environments.
Keywords:
internet of medical things
; quality of service
; wireless fidelity
; target wake time (TWT)
; orthogonal frequency-division multiplexing (OFDM)
; orthogonal frequency-division multiple access (OFDMA)
1. Introduction
The advancement of the digital age has significantly transformed the management of healthcare services. Wireless communication has become one of the most indispensable enablers for modern eHealth systems, supporting continuous patient monitoring, real-time data exchange, and seamless connectivity between healthcare professionals and medical devices. Hospitals and care facilities currently rely heavily on wireless technologies to connect a wide variety of devices ranging from wearable sensors to ventilators and other critical medical equipment. In most modern healthcare settings, Wi-Fi serves as a backbone for connectivity due to its lower cost, high accessibility, and ability to support many devices simultaneously.
However, with the rapid proliferation of interconnected devices, the existing Wi-Fi systems are approaching their operational limits. The core challenge addressed in this paper is whether legacy Wi-Fi 5 (IEEE 802.11ac) can reliably support dense Internet of Medical Things (IoMT) deployments with strict latency, reliability, and energy constraints, and to what extent Wi-Fi 6/7 mechanisms, specifically OFDMA and Target Wake Time (TWT), mitigate these limitations.
The majority of existing healthcare facilities and hospitals still operate Wi-Fi 5, which is based on Orthogonal Frequency-Division Multiplexing (OFDM). Although OFDM has served effectively for the last decade, it was primarily designed for general-purpose connectivity rather than high-density networks and energy-constrained devices. This, combined with the stringent Quality of Service (QoS) requirements of modern eHealth and medical IoMT applications, limits its suitability for operating in such settings. A fundamental limitation of OFDM is its use of a single user per channel transmission. Therefore, in multi-user scenarios, such as hospital settings with numerous devices transmitting data simultaneously, channel access contention increases, resulting in excessive packet loss, delay, and jitter.
To overcome the challenges faced by Wi-Fi 5, IEEE introduced Wi-Fi 6 (IEEE 802.11ax) and, more recently, Wi-Fi 7 (IEEE 802.11be), which incorporate transformative technologies such as OFDMA and TWT. Unlike OFDM, which allows a single user per channel, OFDMA enables multiple users to share the same channel, improving spectral efficiency and reducing contention. This capability is particularly relevant in high-density IoMT environments, where timely and reliable data delivery is critical. Complementing OFDMA, the TWT mechanism allows devices to negotiate specific wake and sleep intervals with the access point, resulting in significant energy savings—an essential consideration for battery-powered medical devices.
To ensure realistic simulations, the traffic model reflects typical IoMT communication patterns, characterized by small, periodic payloads commonly observed in wearable sensors and medical monitoring devices. This allows for a practical assessment of network performance under conditions that closely mimic real-world hospital environments.
This study addresses the outlined challenge by conducting a controlled, simulation-based comparison of Wi-Fi 5 and Wi-Fi 6/7 under dense IoMT traffic conditions, with a focus on the specific benefits of OFDMA and TWT mechanisms. Unlike conventional network performance studies, this work positions wireless protocol selection as a critical design decision in medical systems, where degraded QoS can directly affect the reliability of patient monitoring and clinical outcomes. By analysing performance metrics such as latency, jitter, throughput, packet loss ratio, and power consumption in a realistic high-density scenario, this research bridges a critical gap between communications engineering and medical IoMT network design.
Despite the clear advantages of digital healthcare, dense eHealth and IoMT networks frequently suffer from critical performance bottlenecks, including excessive latency, packet loss, and rapid battery depletion. While Wi-Fi 6/7 introduces advanced features to mitigate these issues, further studies are needed to improve understanding of operational trade-offs between OFDMA and TWT. Specifically, existing studies do not clearly demonstrate the precise conditions under which a network designer should prioritise OFDMA for throughput and reliability versus TWT for energy preservation. This study seeks to fill that gap by quantifying these trade-offs in a simulated clinical environment. IoMT traffic was modelled in NS3 using a 64-byte payload, reflecting realistic medical device data, ensuring that simulations accurately capture the behaviour of small, frequent IoMT transmissions. This approach bridges the gap between generic IoT studies and the specific needs of healthcare environments. In addressing these challenges, this study provides a comprehensive evaluation of Wi-Fi 6 Quality of Service (QoS) tailored specifically to high-density eHealth traffic. The study offers a detailed comparative performance analysis between OFDMA and legacy OFDM to identify the specific density thresholds where multi-user access becomes superior. Furthermore, the study investigates the impact of Target Wake Time (TWT) on device energy consumption and its subsequent effect on network-wide QoS. The paper concludes with evidence-based deployment recommendations intended to guide hospital IT administrators and engineers in the transition from legacy Wi-Fi 5 to modern standards.
The remainder of this paper is organized as follows: Section 2 reviews related literature on wireless communication protocols and IoMT networking in healthcare environments. Section 3 explains the methodology and details the NS3 simulation setup, including ethical considerations. Section 4 presents the simulation results and analysis, comparing the performance of Wi-Fi 5 and Wi-Fi 6/7. Finally, Section 5 concludes with key findings, recommendations for implementation, and directions for future research.
2. Literature Review
2.1. Medical IoT Devices and Network Demands
Integration of eHealth and medical IoMT devices necessitates a robust, reliable, and low-latency wireless infrastructure. According to the Scottish Government’s eHealth strategy [1], major objectives for eHealth in the NHS include improving patient information availability, supporting communication within the NHS, and enhancing care integration. Achieving these objectives critically depends on reliable and timely data transmission, which remains essential despite advances in IoT technologies.
Recent studies highlighted the manner emerging wireless technologies can address these demands in IoMT networks. A study demonstrated how Industrial IoT (IIoT) systems leverage Wi-Fi 6 and OFDMA to significantly reduce channel access contention by scheduling multiple users simultaneously [2]. Without OFDMA, stations (STAs) contend to access a channel one at a time, causing congestion and inefficient spectrum utilization in legacy OFDM networks.
Several studies emphasized the stringent requirements of medical IoMT systems. It has been reported that eHealth diagnostic devices must reliably transmit accurate and secure data to prevent compromised clinical decisions and ensure patient safety [3]. Similarly, the importance of low-cost and efficient devices to scale IoMT infrastructure effectively has been highlighted [4]. Portability is also crucial for ubiquitous patient monitoring. The feasibility of developing a low-cost Raspberry Pi–based health monitoring system has been demonstrated [5], however, real-time operations still require consistent high QoS from the underlying network.
2.2. Legacy Technology: OFDM
Given the real-time data requirements of medical IoMT devices, the performance of the underlying wireless protocol is critical. Many healthcare networks continue to rely on Wi-Fi 5 (IEEE 802.11ac), which uses OFDM. OFDM divides a 20 MHz channel into 64 subcarriers, transmitting data for a single user at a time [6]. While effective for low-density networks, OFDM becomes inefficient when many devices operate simultaneously. It is reported that OFDM struggles to meet low-latency, reliable, and scalable communication requirements in modern clinical settings [7]. As hospitals increasingly deploy dense IoMT networks, channel contention under OFDM leads to increased delay, jitter, and packet loss, emphasizing the need for advanced multi-user wireless protocols.
2.3. Wi-Fi 6 Multi-User Protocol: OFDMA
To overcome OFDM limitations in dense medical IoMT environments, Wi-Fi 6 introduces OFDMA, which divides channels into smaller Resource Units (RUs) that can be allocated to multiple users simultaneously [8]. This parallel transmission capability reduces contention, improves spectral efficiency, and increases overall network throughput. It has been reported that OFDMA reduces medium access latency by approximately 4 ms and improves throughput by ~10% compared to legacy OFDM networks [9].
While promising, OFDMA performance depends on channel availability and precise synchronization to minimize inter-carrier interference (ICI). Mobile clinical devices can exacerbate frequency offsets and Doppler effects, requiring careful configuration in real hospital environments.
System-level simulation models in NS3, including the vBerlinV2N approach [10] and updated OFDMA implementations [11], provide high-fidelity, replicable evaluations of multi-user scheduling under realistic scenarios, including uplink/downlink behaviour, node mobility, and contention management. Additional schedulers such as Fixed Bandwidth (FBW) and Flexible High Order Layer (FBW) optimize RU allocation depending on network load [12]. Recent research explored advanced MAC protocols (HTFA, ERA, PRS) and polling algorithms (A2P) that leverage OFDMA to meet QoS demands in high-density, time-sensitive networks [13,14]. These approaches ensure steady throughput, low packet loss, and reduced retransmissions, directly addressing IoMT requirements. Emerging Wi-Fi 7 (IEEE 802.11be) continues to support OFDMA and introduces enhanced multi-user features, indicating that the findings from Wi-Fi 6 OFDMA/TWT evaluations are relevant for upcoming network standards, reinforcing the applicability of this study to future IoMT deployments.
2.4. Power Efficiency Protocol: Target Wake Time
TWT is a key feature in Wi-Fi 6 that complements OFDMA by addressing energy consumption challenges in IoMT devices. TWT allows devices to negotiate specific wake and sleep intervals with the access point (AP). During sleep periods, devices remain in a low-power “doze” state, which significantly reduces unnecessary radio activity and overall energy consumption, a critical consideration for battery-powered medical IoMT devices. This capability is particularly valuable in hospital settings where multiple wearable and monitoring devices operate continuously.
Scheduled access under TWT uses a Trigger Frame (TF), which contains the list of selected STAs and their defined transmission parameters [15,16]. This mechanism allows multiple STAs to perform simultaneous uplink transmissions without collisions, improving both efficiency and reliability. By coordinating device transmissions, TWT minimizes channel contention, thereby reducing packet loss and improving overall QoS.
While TWT provides substantial benefits, several challenges exist. For devices with infrequent traffic, clock drift can lead to missed wake-up intervals, resulting in failed transmissions [17,18]. Adjusting the wake interval and duration can help mitigate this, but may involve trade-offs between energy efficiency, throughput, and latency [19,20]. Additionally, TWT’s effectiveness depends on accurate scheduling in dense networks; misconfigurations can reduce its benefits, particularly in high-traffic hospital environments.
In NS3 simulations, TWT can be integrated alongside OFDMA to evaluate energy efficiency and QoS simultaneously. By combining multi-user scheduling with controlled wake/sleep intervals, the simulator can replicate real-world medical IoMT scenarios, where devices transmit small payloads (e.g., 64 bytes) frequently but must remain energy efficient. These simulations help quantify the trade-offs between reduced power consumption and potential throughput decline, particularly under high-density conditions. For example, studies have shown that TWT can reduce device power consumption by up to 90%, but under extreme STA density, throughput may decrease by approximately 75% [21].
Overall, TWT is a critical mechanism for energy-constrained medical IoMT devices, and when combined with OFDMA, it provides a framework for scalable, low-power, high-performance wireless networks suitable for dense healthcare environments. This study’s simulations explicitly model both uplink and downlink behaviour under TWT scheduling, allowing a quantitative assessment of its benefits and limitations in practical deployment scenarios.
2.5. Gaps in Current Research
Despite extensive research on Wi-Fi protocols, gaps remain in dense medical IoMT environments. Most studies evaluate OFDMA and TWT in controlled or theoretical settings, often overlooking realistic hospital conditions with multiple devices transmitting simultaneously under strict QoS requirements [22]. Wi-Fi 6 evaluations show benefits of OFDMA and TWT in multi-client scenarios but also reveal trade-offs, such as increased power consumption, indicating that real network behaviour can differ from idealised models [23].
Comparative studies across Wi-Fi generations highlight that latency and throughput may vary under high contention and interference. Deployment complexities—including interference, scheduling limitations, and clock drift—are rarely addressed, yet directly impact patient monitoring and safety [15,17,19]. As Wi-Fi 7 enhances OFDMA and TWT, further scenario-specific evaluations are required for practical IoMT deployment [24]. Energy efficiency for battery-powered devices is also underexplored, despite the prevalence of wearable and bedside medical devices.
NS3 simulations have been widely used for Wi-Fi 6/7 studies, but few considered OFDMA and TWT together under realistic IoMT conditions, including small payload traffic, uplink/downlink behaviour, and network contention [10,11,25].
This study addresses these gaps by:
- Comparing Wi-Fi 5 (OFDM) and Wi-Fi 6/7 (OFDMA + TWT) in dense medical IoMT networks.
- Using small payload traffic reflecting typical medical device communications.
- Evaluating delay, jitter, packet loss, throughput, and power consumption across varying device densities.
- Highlighting practical trade-offs for hospital IT teams and clinical operations.
By addressing these issues, this study bridges wireless research and practical IoMT deployment, providing insights that are both technically rigorous and clinically relevant.
3. Methodology
3.1. Research Design
This study employs a quantitative experimental framework to investigate the performance of IEEE 802.11ax (Wi-Fi 6) protocols within dense medical Internet of Medical Things (IoMT) settings. It utilized two distinct simulation experiments to isolate the impact of specific protocol features on network reliability and energy efficiency:
- Simulation 1 (Access Mechanism): Evaluates the transition from Contention-based OFDM to Scheduled OFDMA.
- Simulation 2 (Power Management): Evaluates the impact of Target Wake Time (TWT) by comparing a baseline against a TWT-enabled environment.
The NS-3 simulation platform was selected as it allows precise, repeatable modelling of the 802.11ax PHY and MAC layers. This approach overcomes the ethical and safety constraints of conducting live experiments in hospital wards while providing granular control over network density and traffic patterns [26]. To ensure statistical significance and minimize the impact of transient network fluctuations, each scenario was executed across an average of five simulation runs using varying random seeds, with the results aggregated to provide the final performance metrics.
3.2. Network Architecture
The system architecture follows a star topology as illustrated in Figure 1. A central Access Point (AP) serves multiple station nodes (STAs) representing diverse medical IoMT devices, such as wearable monitors and bedside sensors.
As shown in Figure 1, the traffic consists of 64-byte UDP packets sent in the uplink direction (STA → AP). To represent a real-world medical environment, the network density scales incrementally. The number of devices (N) included were 4, 8, 12, 16, 20, 24, 28 and 32. All devices were placed at a fixed distance of 10 metres from the AP using a constant position mobility model to ensure the results focused on protocol efficiency rather than signal fading. All stations were positioned at a fixed 10 m radius to maintain a high Signal-to-Noise Ratio (SNR). This configuration ensures that the recorded packet loss and delay are strictly results of MAC-layer protocol logic and channel contention, rather than physical layer signal fading or path loss.
3.3. Simulation 1: Contention vs. Scheduling (OFDM/OFDMA)
This experiment focused on how the MAC layer handles channel access for multiple devices. The operational logic for this experiment is detailed in Figure 2.
- Phase 1 (OFDM): Devices utilized the standard-compliant Station and Access Point MAC architectures. Although multiple stations were present, they competed for the entire 80 MHz channel using the Carrier Sense Multiple Access with Collision Avoidance (CSMA/CA) protocol. In this legacy mode, only one station can occupy the channel at any given time, leading to significant contention overhead and "wait-time" bottlenecks as device density increases.
- Phase 2 (OFDMA): Maintaining identical physical parameters, we activated the Uplink Orthogonal Frequency-Division Multiple Access (UL-OFDMA) capability. The Access Point (AP) employed a Round Robin Multi-User Scheduler to partition the 80 MHz channel into discrete Resource Units (RUs). As illustrated in the methodology flowchart, this configuration enabled parallel transmissions from multiple stations (STAs) through the coordination of Trigger-Based (TB) Physical Layer Protocol Data Units (PPDUs). This shift from contention to scheduled access allows for simultaneous medium occupancy, significantly increasing spectral efficiency.
Thespecific technical configurations of OFDM/OFDMA used to execute these phases in the NS-3 environment are summarized in Table 1.
3.4. Simulation 2: Energy Conservation (TWT)
Simulation 2 investigated the reduction of "idle listening" energy consumption using a TWT scheduling mechanism. The process is mapped in Figure 3.
- Phase 1 (TWT Disabled): STAs followed the standard power management where radios remain in an idle state between transmissions, consuming significant power.
- Phase 2 (TWT Enabled): We implemented a TWT scheduler with a 20% Duty Cycle. The devices only wake up to transmit data during scheduled intervals and enter a deep sleep state (drawing only 0.0001A) for the remaining 80% of the cycle.
3.5. Simulation 2: Energy Conservation (TWT)
Simulation 2 investigated the reduction of "idle listening" energy consumption. To accurately model the sub-carrier behavior of Wi-Fi 6, a high-fidelity multi-model spectrum channel was utilized. This provided a high-fidelity representation of the 80 MHz band, accounting for the frequency-domain interactions between Resource Units (RUs) during simultaneous multi-user transmissions [27]. The operational flow for this power-management study is shown in the Simulation 2 Flowchart (Figure 3).
- Phase 1 (Baseline): Representing standard active/idle power management where the radio remains ready to receive at all times.
- Phase 2 (TWT Enabled): We implement a TWT scheduler with a 20% Duty Cycle. STAs enter a deep sleep state for 80% of the simulation cycle.
The energy-specific parameters, including the currents and duty cycle logic used in the TWT code, are detailed in Table 2.
3.6. Metrics Computation
To address reviewer requirements, the performance metrics were defined individually. These metrics were calculated using the NS-3 Flow Monitor and Energy Source data.
- Throughput (S): The rate of successful data delivery. If Brx is the total bytes received and Tsim is the simulation duration:
(1)
- 2.
- Packet Loss Ratio (PLR): The percentage of packets that failed to reach the AP relative to the total packets transmitted (Ptx):
(2)
- 3.
- Mean Delay and Jitter: Delay represents the average time for a packet to travel from the STA to the AP. Jitter is the variance in this delay between consecutive packets, calculated as the means of the absolute differences between delays.
- 4.
- Power Consumption (PdBm): Based on the energy consumed (Econs), the average power was calculated and converted to a decibel scale relative to 1 milliwatt:
(3)
(4)
Traffic is always uplink from STA → AP. TWT scheduling is applied in the TWT scenario to simulate energy-saving mechanisms, where STAs are awake only during scheduled intervals. NS-3 allows controlled and repeatable simulations, ensuring that OFDM, OFDMA, and TWT are evaluated under identical conditions. While real-world experiments could capture additional environmental variability, practical constraints in hospitals—including limited access and patient safety—make NS-3 the preferred tool. The simulation setup also allows precise control of payload sizes, device counts, and channel conditions, which is essential for IoMT-focused studies
4. Results
The performance of the wireless protocols under investigation—OFDM, OFDMA, and TWT was evaluated using NS-3 simulations. Networks with a single access point (AP) and varying numbers of IoMT devices (STAs: 2, 4, 8, 12, 16, 20, 24, 28, 32) were simulated to reflect practical hospital deployments. Traffic consisted of uplink UDP transmissions with 64-byte payloads to emulate typical IoMT data, and each configuration was validated by calculating the mean performance across five independent simulation runs. This approach ensures that the captured metrics, such as the 37% delay reduction in OFDMA, reflect the steady-state behavioral characteristics of the protocols rather than isolated occurrences. The Results are presented in two groups: (1) OFDM vs. OFDMA (Wi-Fi 5 vs. Wi-Fi 6/7) without TWT, and (2) TWT evaluation (Wi-Fi 6/7) comparing enabled and disabled TWT. In all figures, the x-axis represents the number of STAs, while the y-axis represents the metric under evaluation.
4.1. Performance Comparison of OFDMA vs. OFDM
The following subsections present a comparison between OFDM (baseline, Wi-Fi 5) and OFDMA (Wi-Fi 6/7) across key QoS metrics, using simulations with STA densities of 2, 4, 8, 12, 16, 20, 24, 28, and 32. All results are illustrated in Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7, with OFDM shown in blue and OFDMA in black.
4.1.1. Delay
As shown in Figure 4, the performance gap between the two methods becomes increasingly evident as the network scales. While both protocols exhibit similar latency at low station densities, OFDM experiences a sharp rise in average delay, reaching roughly 175 ms at 32 STAs due to heavy channel contention. Conversely, OFDMA maintains a much more stable profile, peaking at approximately 110 ms. This represents a 37% reduction in delay compared to OFDM, an advantage that becomes more pronounced as the number of STAs increases. This improvement is primarily due to OFDMA’s use of Resource Unit (RU) allocation, which enables coordinated multi-user scheduling and allows multiple stations to transmit simultaneously allocation, which reduces the contention window (CW) size and collision probability. By mitigating the 'wait-time' bottlenecks inherent in OFDM, OFDMA ensures the reliable, low-latency communication required for high-density IoMT medical environments.
4.1.2. Power Consumption
As shown in Figure 5, the network's power consumption exhibits a comparable upward trend for both protocols as the number of stations increases. However, OFDMA maintains a slight but consistent efficiency advantage, achieving an approximate 3% reduction in energy usage compared to OFDM. This improvement is primarily due to OFDMA’s ability to serve multiple STAs simultaneously through Resource Unit (RU) allocation. By grouping transmissions, the access point (AP) significantly reduces the cumulative overhead associated with individual channel access and "listen-before-talk" contention periods required by OFDM. While the margin remains modest, this enhanced efficiency is particularly beneficial for energy-constrained IoMT devices, where even marginal power savings can extend the operational longevity of critical medical sensors in dense deployments.
4.1.3. Jitter
The jitter performance for both protocols is presented in Figure 6, where both methods maintain a stable and relatively low jitter profile as the network expands. While the two curves appear nearly identical, a closer inspection reveals that OFDMA provides a marginal improvement of approximately 2% over OFDM. This slight reduction in packet delay variation is primarily due to the more disciplined scheduling of Resource Units (RUs), which ensures a more consistent transmission rhythm compared to the random nature of contention-based access. Although the performance difference is minor in this metric, the enhanced stability offered by OFDMA is vital for mission-critical IoMT applications, such as real-time patient monitoring, where even small fluctuations in timing can impact the accuracy of continuous health data collection. The 2% jitter improvement in OFDMA is attributed to the Access Point acting as a centralized coordinator. Unlike the random backoff intervals in OFDM, the AP assigns Resource Units at precise, deterministic intervals, reducing the variance in packet arrival times.
4.1.4. Packet Loss Ratio
As shown in Figure 7, the packet loss ratio (PLR) highlights a critical divergence in network reliability between the two protocols as the environment becomes more congested. While both methods maintain negligible loss at low station counts, OFDM experiences a sharp, non-linear increase in dropped packets beyond 16 STAs, reaching a peak PLR of approximately 0.18% at 32 stations. Conversely, OFDMA exhibits a far more stable performance, maintaining a significantly lower loss rate of roughly 0.025% under the same conditions. This equates to an approximate 85% reduction in packet loss compared to OFDM, an advantage that becomes increasingly vital as the number of STAs increases. This superior reliability is primarily due to OFDMA’s multi-user scheduling and Resource Unit (RU) allocation, which effectively minimizes the collisions and subsequent retransmissions inherent in the contention-based access of OFDM. Consequently, OFDMA ensures the robust data integrity required for high-density IoMT applications where packet loss could compromise patient monitoring.
4.1.5. Throughput
The network throughput for both protocols is illustrated in Figure 8, which demonstrates that while both methods perform similarly at low densities, a substantial performance gap develops as the number of stations exceeds 20. In high-density scenarios, OFDM experience a steep decline in throughput due to increased channel contention and collision overhead, falling to approximately 60 Mbps at 32 STAs. In contrast, OFDMA exhibits superior resilience, maintaining a higher throughput of roughly 63 Mbps under identical conditions. This represents an approximate 20% improvement in comparative throughput efficiency at peak density by mitigating the degradation typically seen in single-user access models. This enhanced performance is achieved by Resource Unit (RU) allocation that maximizes spectral efficiency and allows for parallel data streams. Consequently, OFDMA provides reliable, high-speed data transfer capacity essential for supporting multiple concurrent devices in a dense hospital environment.
4.2. Evaluation of TWT Performance
This section presents the impact of Target Wake Time (TWT) on key QoS metrics. Simulations were conducted with STA densities of 2, 4, 8, 12, 16, 20, 24, 28, and 32, and the results are illustrated in Figure 9, Figure 10, Figure 11, Figure 12 and Figure 13, with no-TWT in blue and TWT-enabled in black.
4.2.1. TWT Delay
The impact of Target Wake Time (TWT) on average network delay is illustrated in Figure 9, highlighting a significant divergence in performance as the station density scales. While the network without TWT experiences a sharp, non-linear increase in delay—climbing to approximately 200 ms at 32 STAs—the TWT-enabled configuration maintains a remarkably low and stable profile. Specifically, at peak density, TWT limits the delay to roughly 30 ms, representing a substantial reduction compared to the non-TWT scenario. This enhanced stability is primarily due to TWT’s scheduled access mechanism, which allows stations to wake and transmit within dedicated time windows. By coordinating these transmission periods, TWT effectively mitigates the channel contention and congestion inherent in dense environments, ensuring the reliable, low-latency communication necessary for real-time medical IoMT applications.
The remarkably stable 30 ms delay profile under TWT is a result of contention-free access. Because stations only wake during their specific TWT Service Period (SP), they do not have to sense the medium for other users, enabling immediate transmission upon wake-up
4.2.2. TWT Power Consumption
The impact of Target Wake Time (TWT) on power consumption is presented in Figure 10, demonstrating a substantial reduction in energy usage across all station densities. While the network without TWT exhibits high power consumption, rising to approximately 35.5 dBm as the number of stations increases, the TWT-enabled configuration maintains a much lower energy profile, consistently remaining below 26.5 dBm. This performance represents a dramatic efficiency gain, achieving power savings of up to 90% in comparison to non-TWT deployments. Such a significant improvement is due to the TWT scheduling mechanism, which allows stations to remain in a low-power sleep mode for extended periods and only wake during negotiated time slots. By minimising unnecessary channel sensing and contention overhead, TWT provides an essential energy-saving framework for battery-constrained IoMT devices operating in dense medical environments.
4.2.3. TWT Jitter
As shown in Figure 11, the jitter performance with TWT enabled reveals a distinct trend as station density increases. While both configurations maintain nearly identical jitter levels at lower densities, a divergence occurs beyond 20 STAs. Specifically, the TWT-enabled network experiences a more pronounced increase in jitter, reaching approximately 0.85 ms at 32 STAs compared to roughly 0.65 ms for the no-TWT scenario. This increase is primarily due to the inherent timing variability introduced by the scheduled wake-up mechanism, as STAs must wait for their precise negotiated windows to transmit. Although this introduces a slight trade-off in timing consistency, the overall network stability and reliability remain superior to the no-TWT model when considering the significant gains in delay and power efficiency. Consequently, while TWT-induced jitter requires careful management in latency-sensitive applications, it does not undermine the protocol's effectiveness in supporting high-density IoMT environments.
4.2.4. TWT Packet Loss Ratio
As shown in Figure 12, the packet loss ratio (PLR) highlights a stark contrast in network reliability when Target Wake Time (TWT) is employed. In the absence of TWT, the PLR rises sharply as the number of stations exceeds 16, peaking at approximately 0.185% at 32 STAs due to severe channel congestion. In comparison, the TWT-enabled network maintains a remarkably low and stable PLR, staying below 0.05% even at peak density. This represents an approximate 80% reduction in packet loss, a gain achieved by TWT's ability to assign dedicated transmission windows to specific stations while others remain in a doze state. By effectively eliminating overlapping transmissions and reducing collisions, TWT ensures the robust data integrity and high reliability necessary for critical patient monitoring in dense IoMT environments.
4.2.5. TWT Throughput
As shown in Figure 13, the network throughput for both configurations remains relatively stable at low station densities but diverges significantly as the network scales. While the network without TWT maintains a higher raw throughput, gradually declining to approximately 63 Mbps at 32 STAs, the TWT-enabled network experiences a much sharper reduction, dropping to roughly 31 Mbps. This represents a throughput decrease of approximately 75% under high-density conditions when compared to peak performance levels. This decline is a deliberate architectural trade-off; by enforcing scheduled wake-up windows to ensure high reliability and extreme energy efficiency, TWT inherently limits the total volume of concurrent data transfer. Although non-TWT networks achieve higher aggregate speeds, they do so at the expense of significantly higher collisions, packet loss, and power drain. Ultimately, these results demonstrate that TWT prioritizes robust data delivery and battery longevity essential for dense medical IoMT environments over raw throughput capacity.
5. Discussion
This study systematically evaluated the performance of Wi-Fi protocols—specifically OFDM (Wi-Fi 5), OFDMA (Wi-Fi 6/7), and TWT—within a dense medical IoMT environment. Simulations conducted in NS-3 considered STA densities ranging from 2 to 32, with realistic IoMT traffic (64-byte UDP payloads), capturing key QoS metrics including delay, jitter, packet loss ratio (PLR), throughput, and power consumption.
The comparative analysis between OFDM and OFDMA demonstrated that OFDMA consistently outperforms OFDM across most metrics, particularly as network density increases. Average delay and jitter were significantly reduced with OFDMA due to its coordinated Resource Unit (RU) scheduling and parallel multi-user transmissions, ensuring timely and consistent delivery of medical data [28]. This gain is primarily attributed to the shift from stochastic contention to a deterministic sub-carrier allocation; by partitioning the 80 MHz channel, OFDMA minimizes the Trigger Frame (TF) overhead and random backoff periods that typically plague legacy OFDM in dense environments. Throughout improvements of approximately 20% further confirm the efficiency gains achieved by dynamic channel allocation and reduced contention. While OFDM performs adequately in low-density scenarios, its performance degrades sharply under high contention, highlighting the scalability advantage of OFDMA in dense hospital networks.
Power consumption presented a trade-off: while OFDM remained relatively stable across STA densities, OFDMA showed higher variability and slightly increased energy usage at high densities. This reflects the more active channel utilization and simultaneous transmissions characteristic of OFDMA. Nevertheless, for mission-critical IoMT applications, this increase is a minor trade-off against the substantial gains in latency, reliability, and throughput.
The evaluation of TWT revealed its crucial role in energy efficiency for dense networks. By scheduling wake-up intervals and allowing STAs to enter sleep mode when not transmitting, TWT achieved a 75% reduction in power consumption while maintaining low delay and PLR. However, throughput decreased under high-density conditions, reflecting a prioritization of reliability and energy efficiency over raw data rates. This trade-off is particularly relevant in hospital IoMT scenarios where battery-powered devices are prevalent, and predictable, stable communication is more critical than maximum throughput.
While the results indicate a 75% reduction in aggregate throughput when TWT is enabled, this must be interpreted as a strategic trade-off rather than a performance failure. In medical telemetry, the priority shifts from high-volume data to high-integrity delivery. By enforcing scheduled 'quiet' periods, TWT eliminates the 'collision storms' typical of legacy OFDM contention. This ensures that critical, low-bandwidth packets—such as heart rate alerts—are delivered with 80% higher reliability (PLR < 0.05%) and significant battery longevity, which is more clinically valuable than high raw throughput for non-streaming medical sensors. From a network engineering perspective, this represents an optimization of 'Goodput' over raw capacity, where the focus shifts to successful delivery within specific QoS bounds.
Although this study utilizes 802.11ax parameters, these findings provide a vital performance floor for emerging Wi-Fi 7 (802.11be) standards. The transition to Wi-Fi 7 is expected to further enhance these QoS metrics through Multi-Link Operation (MLO), which could theoretically mitigate the 30 ms latency floor observed in our TWT results by utilizing frequency diversity across the 2.4, 5, and 6 GHz bands simultaneously [29].
To translate these technical findings into clinical practice, the following table outlines specific deployment strategies based on the varied requirements of a modern hospital ward.

Table 3.
Deployment Recommendations for eHealth / IoMT Networks Using Wi-Fi 6/7.
| IoMT Application Type |
Traffic Characteristics |
Primary QoS Requirement |
Recommended Wi-Fi 6 Features |
Rationale / Explanation |
| Wearable Health Sensors (e.g. heart rate, SpO₂, temperature) | Small packets, periodic uplink, battery-powered | Energy efficiency, acceptable delay | Enable TWT, moderate RU allocation | TWT significantly reduces energy consumption, extending battery life. |
| Real-Time Patient Monitoring (e.g. ECG alerts, critical alarms) | Low data rate, delay-sensitive, uplink-dominant | Low latency, low packet loss | Enable OFDMA, limit or disable TWT | OFDMA reduces contention and delay; TWT may introduce wake-up latency unsuitable for alerts. |
| Medical Bedside Devices (e.g. infusion pumps, monitors) | Continuous telemetry, moderate traffic, mains-powered | Reliability and stability | OFDMA enabled, TWT optional | Energy savings are less critical; OFDMA ensures stable throughput and low packet loss. |
| Mobile Clinical Devices (e.g. tablets, carts-on-wheels) | Bursty traffic, mixed uplink/downlink | Throughput and fairness | OFDMA enabled, no aggressive TWT | OFDMA improves fairness; aggressive TWT may degrade user experience due to wake delays. |
| Dense Ward Deployment (many IoMT devices per AP) | High contention, small packet uplink traffic | Scalability, contention reduction | OFDMA mandatory, careful RU scheduling | OFDMA scales better as device density increases, reducing collisions compared to legacy OFDM. |
| Battery-Critical IoMT (Long-term monitoring) | Infrequent transmissions, ultra-low power | Maximum battery lifetime | Aggressive TWT scheduling | TWT allows devices to sleep for long intervals, drastically lowering energy consumption. |
| Mixed IoMT Environment (wearables + monitors) | Heterogeneous traffic patterns | Balanced QoS and energy | Hybrid approach: OFDMA + selective TWT | Enables low delay for critical devices while conserving energy for wearables through selective TWT. |
6. Conclusion
This research provided a comprehensive quantitative evaluation of IEEE 802.11ax (Wi-Fi 6) features—specifically OFDMA and Target Wake Time (TWT)—within the context of dense medical Internet of Medical Things (IoMT) networks. By simulating a scaling hospital ward environment from 2 to 32 nodes using 64-byte telemetry payloads, this study concludes that legacy OFDM (Wi-Fi 5) is insufficient for high-density clinical monitoring due to a sharp rise in delay (175 ms) and packet loss (0.18%) beyond 16 stations. The transition to OFDMA-based scheduling yields a 37% reduction in average latency and a 20% improvement in throughput efficiency by replacing random contention with deterministic Resource Unit (RU) allocation. Furthermore, the implementation of TWT proved transformative for energy conservation, achieving an 8.5 dBm reduction in average power consumption representing a 90% energy saving by utilizing a 20% duty cycle and a 100 µA sleep state. While TWT introduces a significant throughput trade-off (dropping to 31 Mbps at peak density), it ensures a stable Packet Loss Ratio (PLR) of under 0.05%, providing the reliability required for life-critical sensors. These findings provide a technical roadmap for hospital IT infrastructure [30]: OFDMA should be prioritized for real-time diagnostic streams, while TWT is the optimal protocol for wearable battery-powered sensors. Future work will expand this framework to include Wi-Fi 7 Multi-Link Operation (MLO) and the impact of physical hospital obstacles on RU synchronization.
Ethical and Legal Compliance
This study utilized the Network Simulator 3 (NS-3) open-source platform. The use of a simulation-based approach was prioritized over physical clinical testing to ensure patient safety and avoid interference with critical medical infrastructure. No human or animal subjects were involved, and no identifiable patient data was utilized. The research was conducted in compliance with university ethical guidelines regarding data integrity and software attribution.
Summary of Methodological Choices
In summary, this methodology is anchored in a quantitative, controlled simulation framework that switches between OFDM, OFDMA, and TWT while changing the STA density to mirror a real hospital environment. The choice of NS3 provides modern Wi-Fi models and reproducible execution of clinically relevant QoS metrics: Delay, Jitter, PLR, Throughput, and Power Consumption. Known simulator limitations are explicitly documented and incorporated into the analysis rather than being obscured.
Author Contributions
A.S.: Project management, leadership, administrative oversight, and software implementation. C.D.: Methodology, system architecture, core OFDM/OFDMA and TWT software implementation, literature review, and data optimization. S.B.: Software implementation and specific TWT feature development. M.S.: Software implementation and technical component development. N.H.: Literature review and research support. R.S.: Validation, critical review, and supervision. M.B.: Writing—review and editing. All authors contributed to the writing, editing, and finalization of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
Financial support for this research was provided by Sheffield Hallam University (internal university funding, project reference N160).
Data Availability Statement
All data supporting the reported findings are entirely contained within this article.
Acknowledgments
The authors would like to thank the School of Computing and Digital Technologies at Sheffield Hallam University for providing the computational resources necessary to conduct this research.
For the purpose of open access, the authors have applied a Creative Commons Attribution (CC BY) license to any Author Accepted Manuscript version arising from this submission
Conflicts of Interest
The authors declare that this research was conducted completely in the absence of any commercial or financial relationships that could be interpreted as potential conflicts of interest.
References
- Scottish Government. eHealth Strategy 2014 - 2017; Scottish Government: Edinburgh, UK, 2015. [Google Scholar]
- Maldonado, R.; Karstensen, A.; Pocovi, G.; Esswie, A.A.; Rosa, C.; Alanen, O.; Kasslin, M.; Kolding, T. Comparing Wi-Fi 6 and 5G Downlink Performance for Industrial IoT. IEEE Access 2021, 9, 86928–86937. [Google Scholar] [CrossRef]
- Christodouleas, D.C.; Kaur, B.; Chorti, P. From Point-of-Care Testing to eHealth Diagnostic Devices (eDiagnostics). ACS Cent. Sci. 2018, 4, 1600–1616. [Google Scholar] [CrossRef] [PubMed]
- Mejía-Salazar, J.R.; Cruz, K.R.; Vásques, E.M.M.; de Oliveira, O.N. Microfluidic point-of-care devices: New trends and future prospects for ehealth diagnostics. Sensors 2020, 20, 1951. [Google Scholar] [CrossRef] [PubMed]
- Ramani, J.G.; Madhusudan S, L.; Pradeep, A.; Manibharathi, S. IOT Based Employee Health Monitoring System. In Proceedings of the 2020 International Conference on Advancements in Computing and Management (ICACCS), Coimbatore, India, 6–7 March 2020; pp. 1–5. [Google Scholar]
- Litwin, L.; Pugel, M. The principles of OFDM. RF Signal Process. 2001, 2, 30–48. [Google Scholar]
- Hwang, T.; Yang, C.; Wu, G.; Li, S.; Li, G.Y. OFDM and its wireless Applications: a survey. IEEE Trans. Veh. Technol. 2008, 58, 1673–1694. [Google Scholar] [CrossRef]
- Cisco Systems. What Is OFDMA? Available online: https://www.cisco.com/c/en/us/products/wireless/what-is-ofdma.html (accessed on 24 January 2026).
- Avallone, S.; Imputato, P.; Redieteab, G.; Ghosh, C.; Roy, S. Will OFDMA Improve the Performance of 802.11 Wifi Networks? IEEE Wireless Commun. 2021, 28, 100–107. [Google Scholar] [CrossRef]
- Vielhaus, C.L.; Seidel, M.; Latzko, V.; Groß, A.; Sossalla, P.; Reisslein, M.; Fitzek, F.H.P. vBerlinV2N: Recreating a Cellular Network Measurement Campaign with Simulations. IEEE Access 2025, 13, 4290–4305. [Google Scholar] [CrossRef]
- Memoona, N.; Kim, S.W. Performance and simulation analysis of 802.11ax OFDMA in contention-driven scenarios. PeerJ Comput. Sci. 2025, 11, e2687. [Google Scholar] [CrossRef]
- Memoona, N.; Kim, S.W. Performance and simulation analysis of 802.11ax OFDMA in contention-driven scenarios. PeerJ Comput. Sci. 2025, 11, e2687. [Google Scholar] [CrossRef]
- Agbeve, D.D.; Belogaev, A.; Sandra, W.; Lylon, C.; Famaey, J. A2P: A Scalable OFDMA Polling Algorithm for Time-Sensitive Wi-Fi Networks. arXiv 2025, arXiv:2502.00430. [Google Scholar]
- Khorov, E.; Levitsky, I.; Akyildiz, I.F. Current Status and Open Problems in the Development of IEEE 802.11be (Wi-Fi 7). IEEE Commun. Mag. 2023, 61, 60–66. [Google Scholar]
- Dovelos, K.; Bellalta, B. Optimal Resource Allocation in IEEE 802.11ax Uplink OFDMA with Scheduled Access. arXiv 2019, arXiv:1811.00957. [Google Scholar] [CrossRef]
- Wilhelmi, F.; Carrascosa-Caballero, M.; Cano, C.; et al. Usage of Wi-Fi 6 for the Internet of Things: Challenges and Opportunities. IEEE Access 2023, 11, 13450–13465. [Google Scholar]
- Stepanova, E.; Bankov, D.; Khorov, E.; Lyakhov, A. On the Joint Usage of Target Wake Time and 802.11ba Wake-Up Radio. IEEE Access 2020, 8, 221061–221076. [Google Scholar] [CrossRef]
- Bardoutsos, A.; et al. Performance Evaluation of Target Wake Time for Battery-Powered Medical IoT Devices. IEEE Internet Things J. 2024, 11, 3210–3225. [Google Scholar]
- Chen, Q.; Weng, Z.; Xu, X.; Chen, G. A target wake time scheduling scheme for uplink multiuser transmission in IEEE 802.11AX-Based next generation WLANs. IEEE Access 2019, 7, 158207–158222. [Google Scholar] [CrossRef]
- Nurchis, M.; Bellalta, B. Target Wake Time: Modeling and Performance Evaluation in IEEE 802.11ax WLANs. IEEE Trans. Wireless Commun. 2023, 22, 450–465. [Google Scholar]
- Qiu, W.; Chen, G.; Nguyen, K.N.; Sehgal, A.; Nayak, P.; Choi, J. Category-based 802.11ax target wake time solution. IEEE Access 2021, 9, 100154–100172. [Google Scholar] [CrossRef]
- Qadri, Y.A.; Zulqarnain; Nauman, A.; Musaddiq, A.; Garcia-Villegas, E.; Kim, S.W. Preparing Wi-Fi 7 for Healthcare Internet-of-Things. Sensors 2022, 22, 6209. [Google Scholar] [CrossRef]
- Magrin, D.; Avallone, S.; Roy, S.; Zorzi, M. Validation of the ns-3 802.11ax OFDMA implementation. In Proceedings of the 2021 Workshop on ns-3 (WNS3), Virtual Event, 23–24 June 2021; pp. 1–8. [Google Scholar]
- Bartolín-Arnau, L.M.; Orozco-Santos, F.; Sempere-Payá, V.; Silvestre-Blanes, J.; Albero-Albero, T.; Llacer-Garcia, D. Exploring the Potential of Wi-Fi in Industrial Environments: A Comparative Performance Analysis of IEEE 802.11 Standards. Telecom 2025, 6, 40. [Google Scholar] [CrossRef]
- Epp, J.; Jiang, C.; Zhang, Y. Performance Evaluation and Analysis of Wi-Fi 6 with ns-3. J. Netw. Softw. 2022, 4, 112–125. [Google Scholar]
- Avallone, S.; Imputato, P.; Redieteab, G.; et al. Will OFDMA Improve the Performance of 802.11 Wi-Fi Networks? IEEE Wireless Commun. 2021, 28*, 100–107. [Google Scholar] [CrossRef]
- Agbeve, D.D.; Belogaev, A.; Sandra, W.; et al. A2P: A Scalable OFDMA Polling Algorithm for Time-Sensitive Wi-Fi Networks. arXiv 2025, arXiv:2502.00430. [Google Scholar]
- Iqbal, A.; Nauman, A.; Qadri, Y.A.; Kim, S.W. Optimizing spectral utilization in healthcare Internet of Things. Sensors 2025, 25, 1–25. [Google Scholar] [CrossRef]
- Bartolín-Arnau, L.M.; Orozco-Santos, F.; Sempere-Payá, V.; et al. Exploring the Potential of Wi-Fi in Industrial Environments: A Comparative Performance Analysis of IEEE 802.11 Standards. Telecom 2025, 6, 40. [Google Scholar] [CrossRef]
- Naik, G.; Park, J.M.; et al. Performance Analysis of IEEE 802.11be for Low-Latency eHealth Applications. IEEE Wireless Commun. Lett. 2024, 13, 412–416. [Google Scholar]
Figure 1.
The network architecture used in the study.
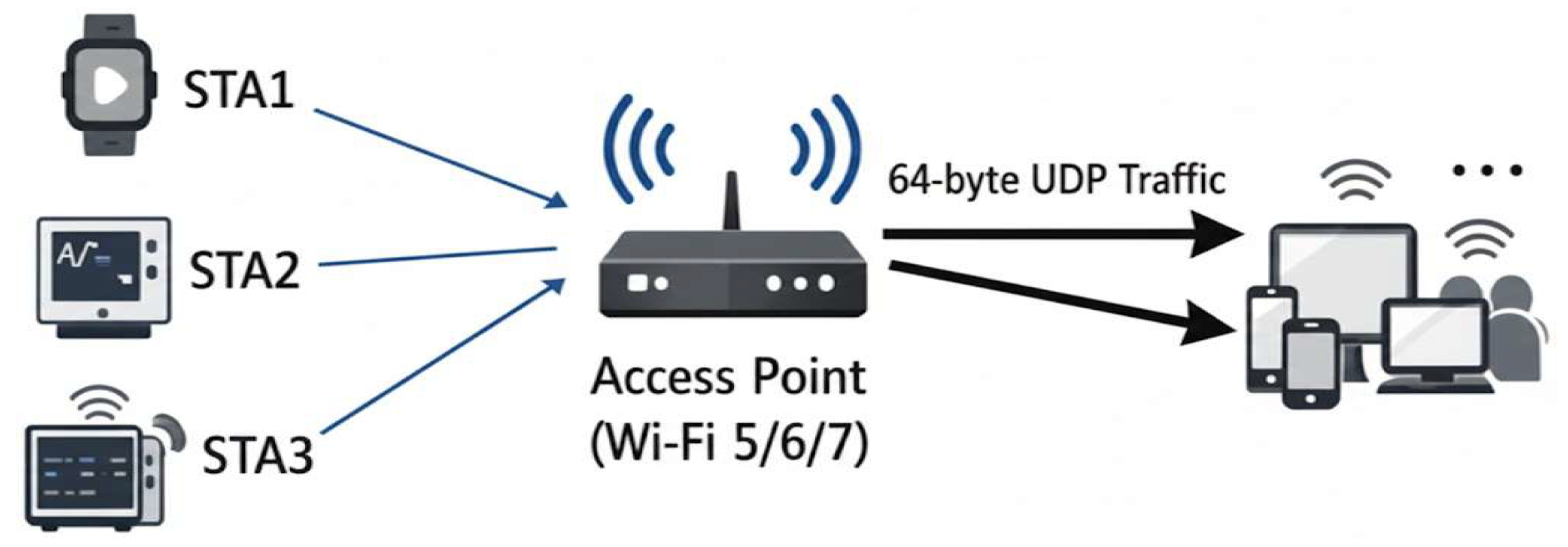
Figure 2.
simulation 1 OFDM/OFDMA flowchart.
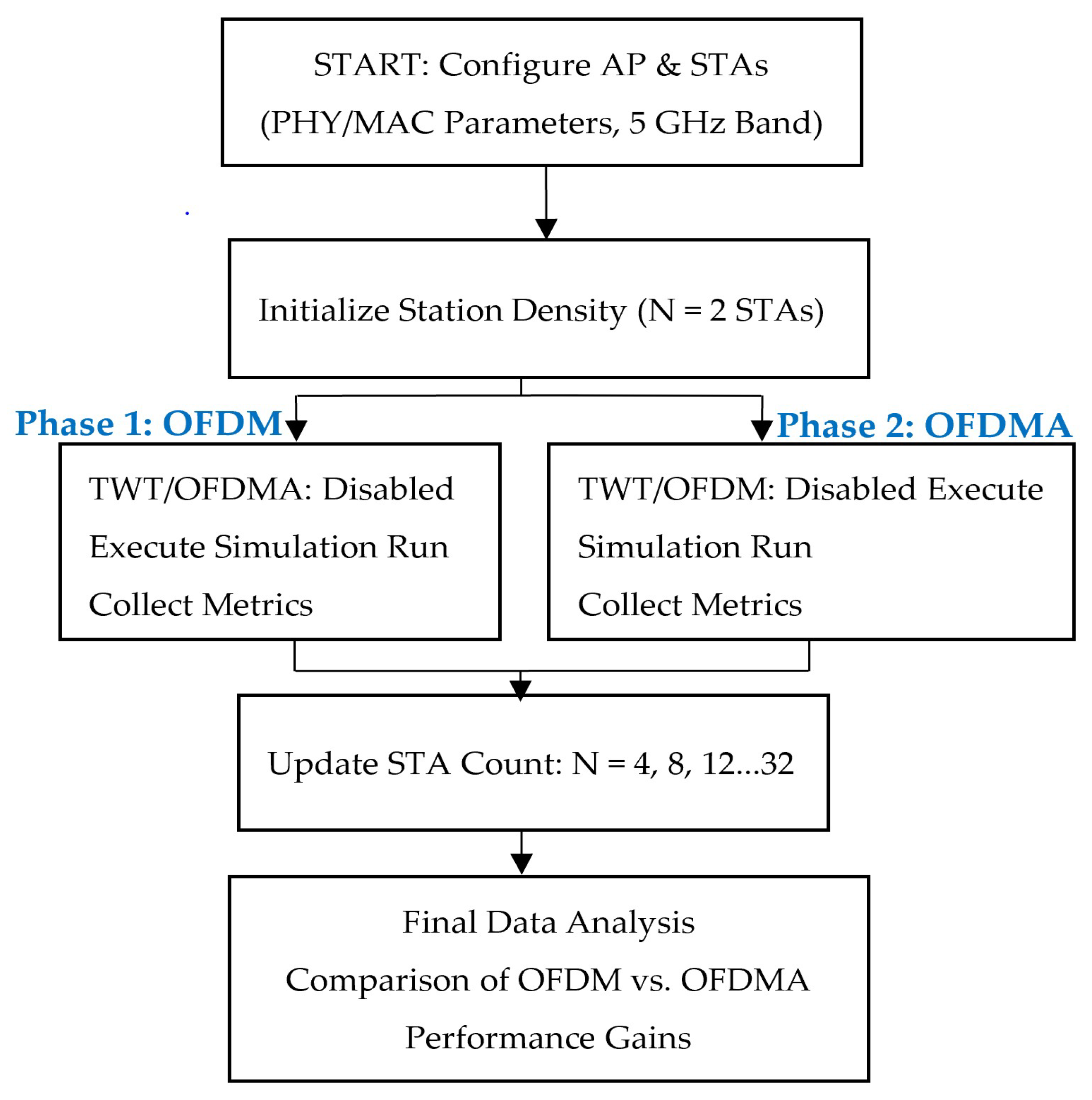
Figure 3.
Simulation 2, TWT flowchart.
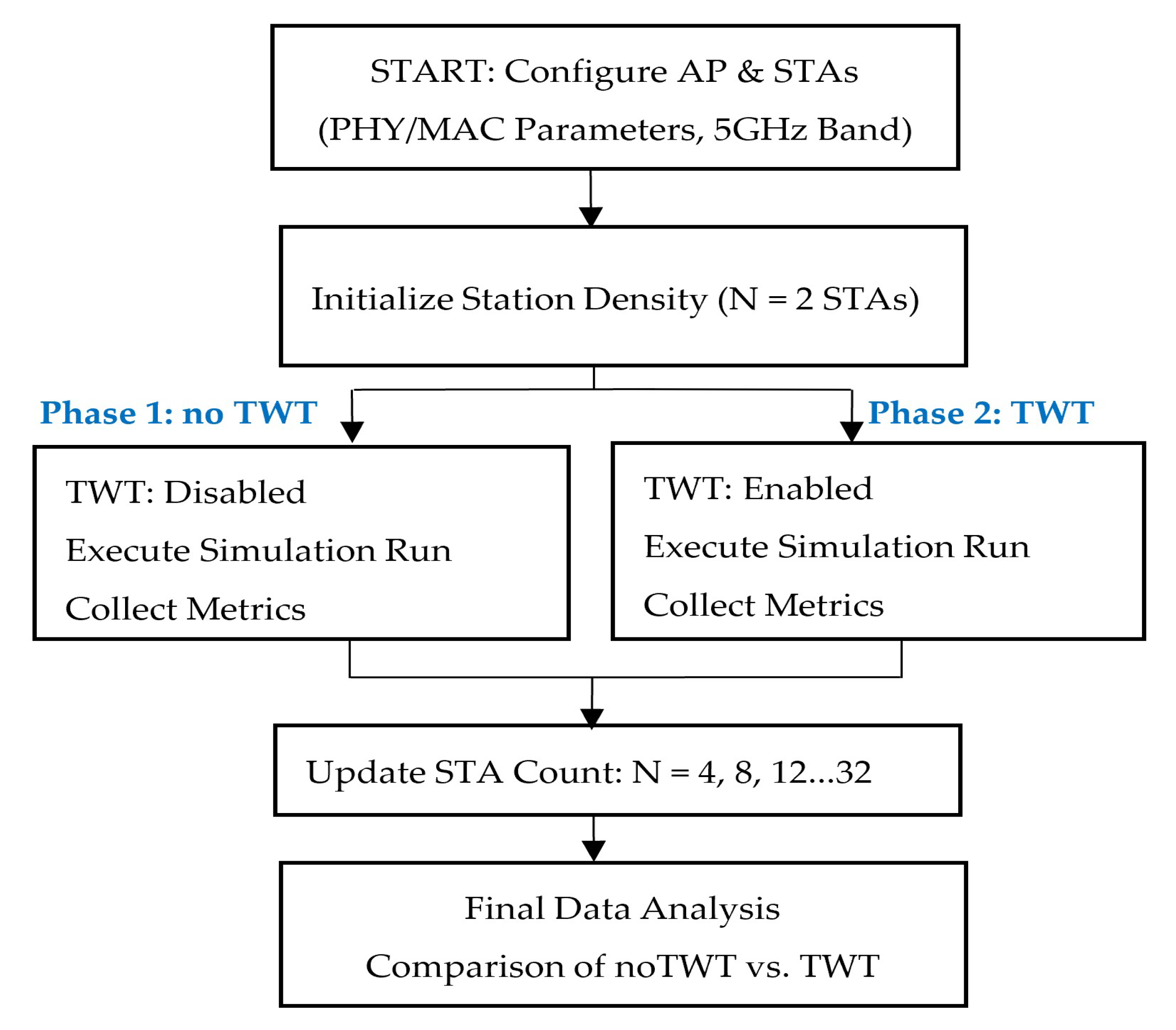
Figure 4.
Showcasing Delay for varying numbers of STAs.
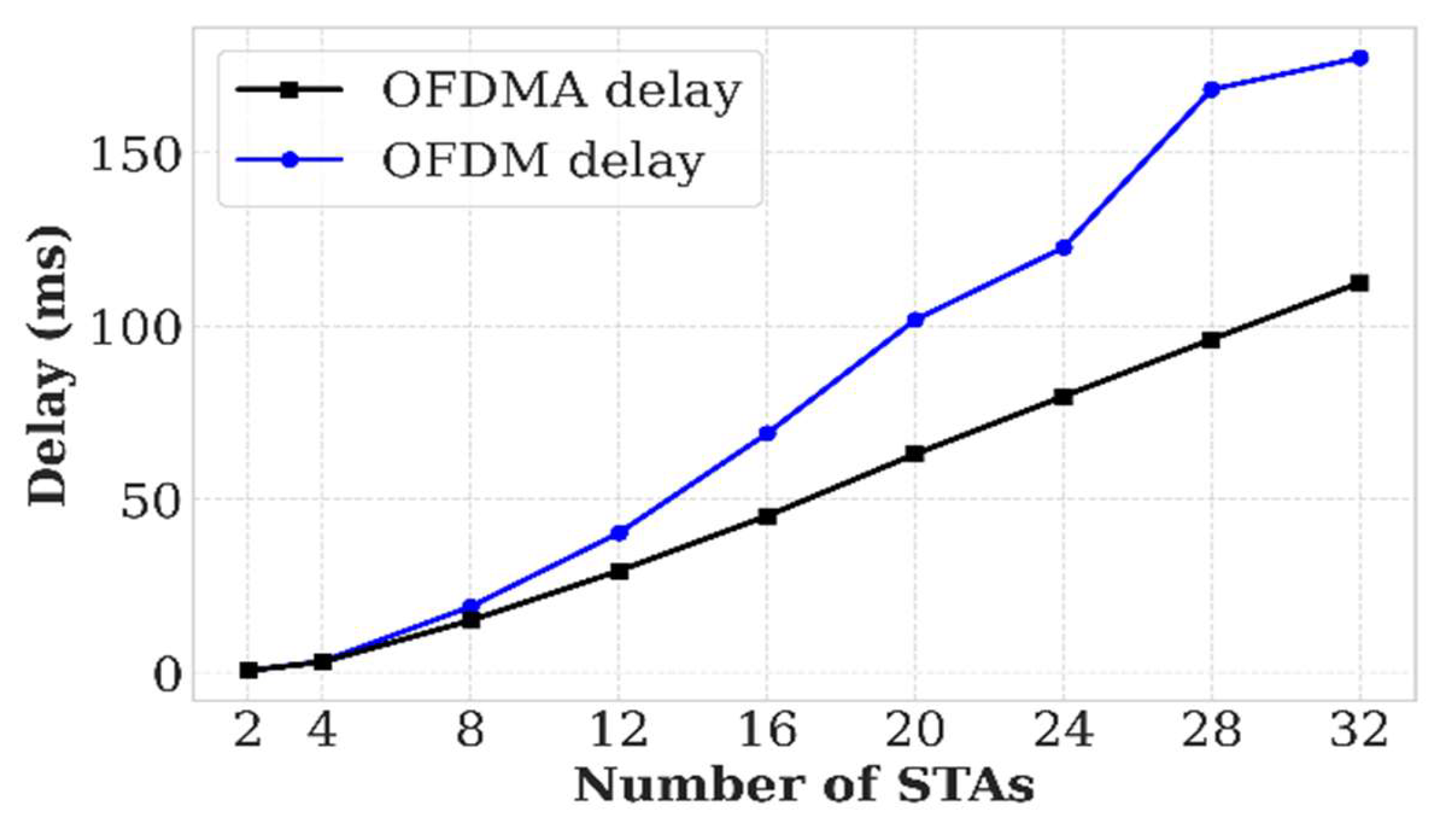
Figure 5.
Showcasing Energy Consumption for varying numbers of STAs.
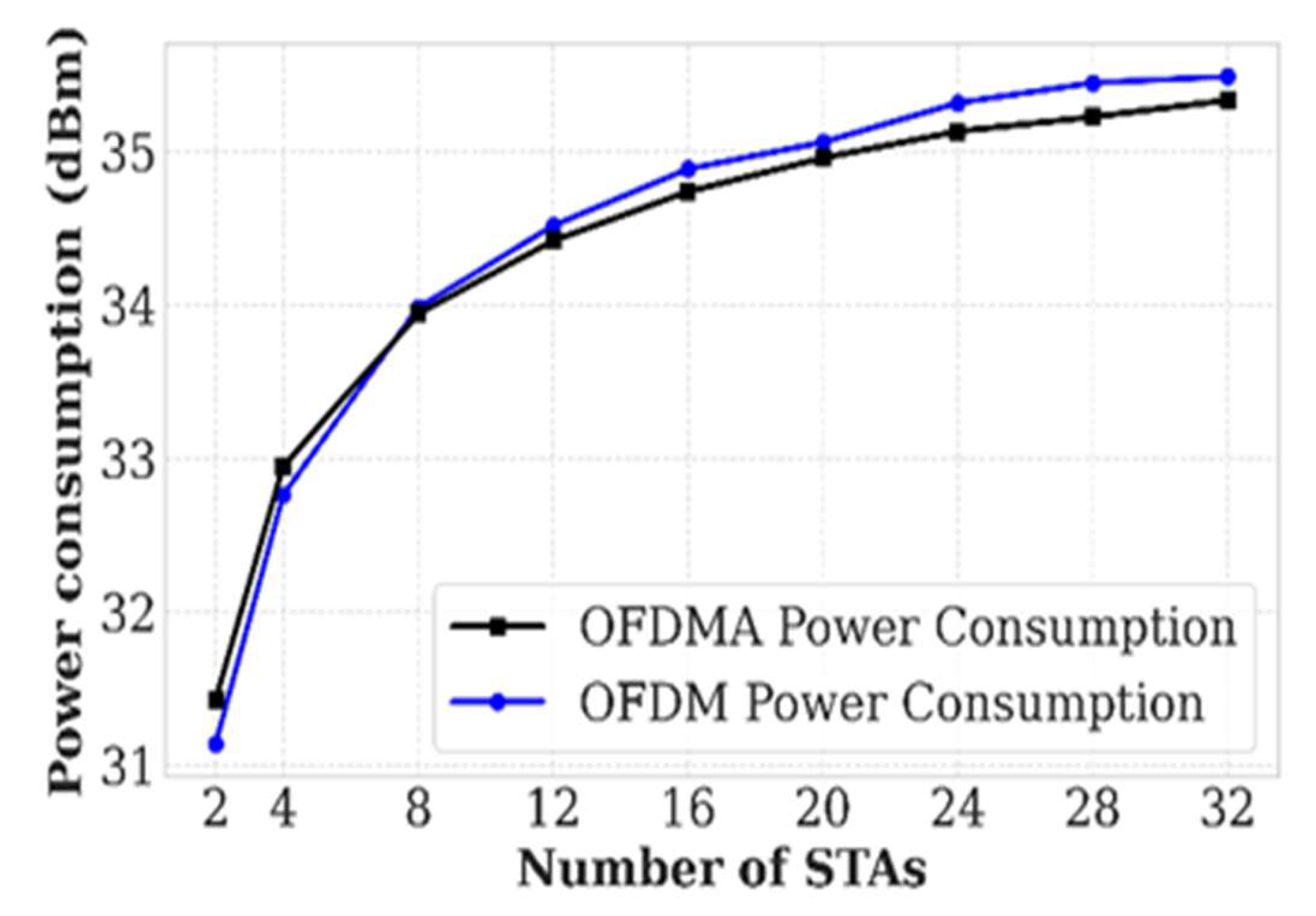
Figure 6.
Showcasing Jitter for varying numbers of STAs.
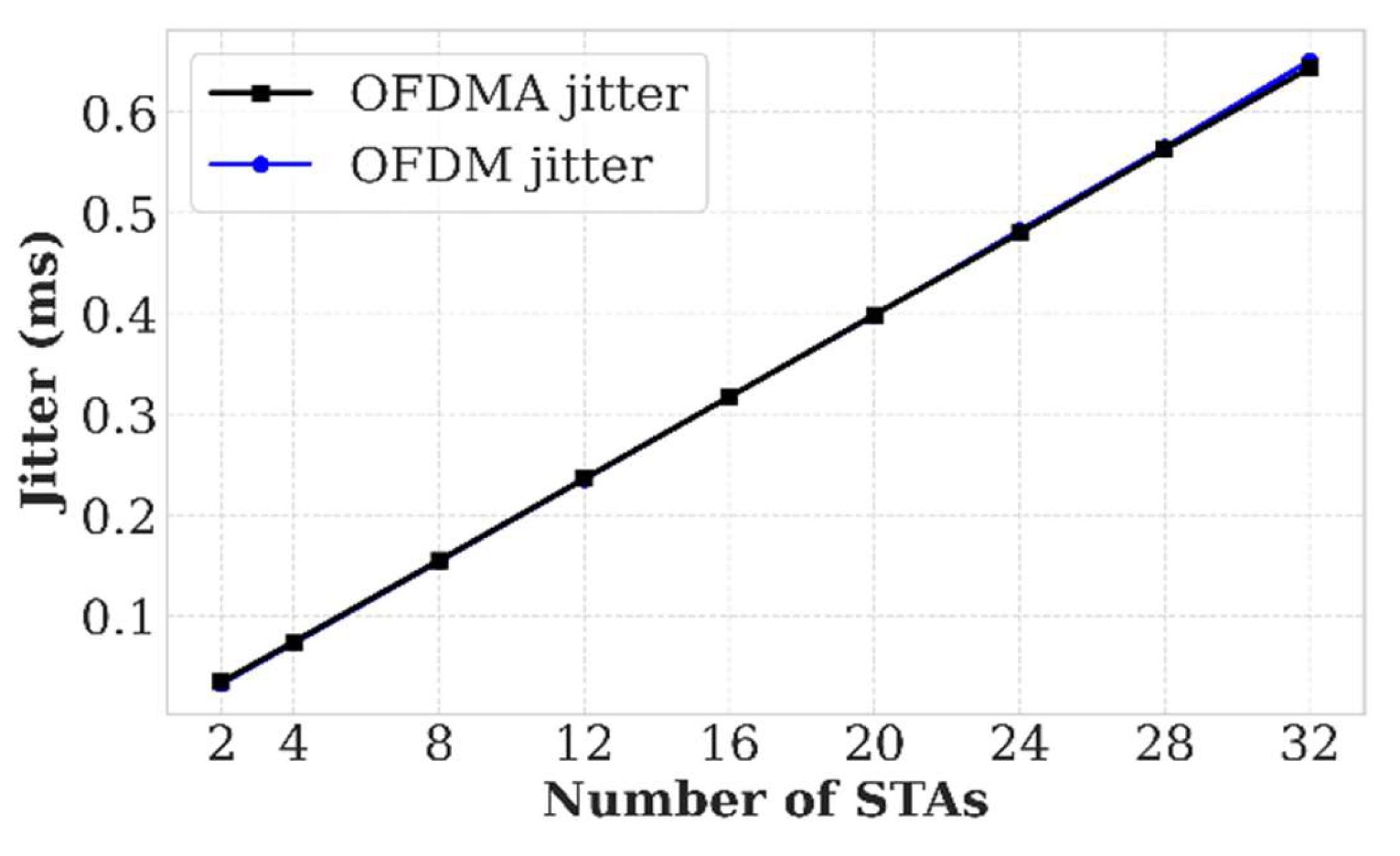
Figure 7.
Showcasing PLR for varying numbers of STAs.
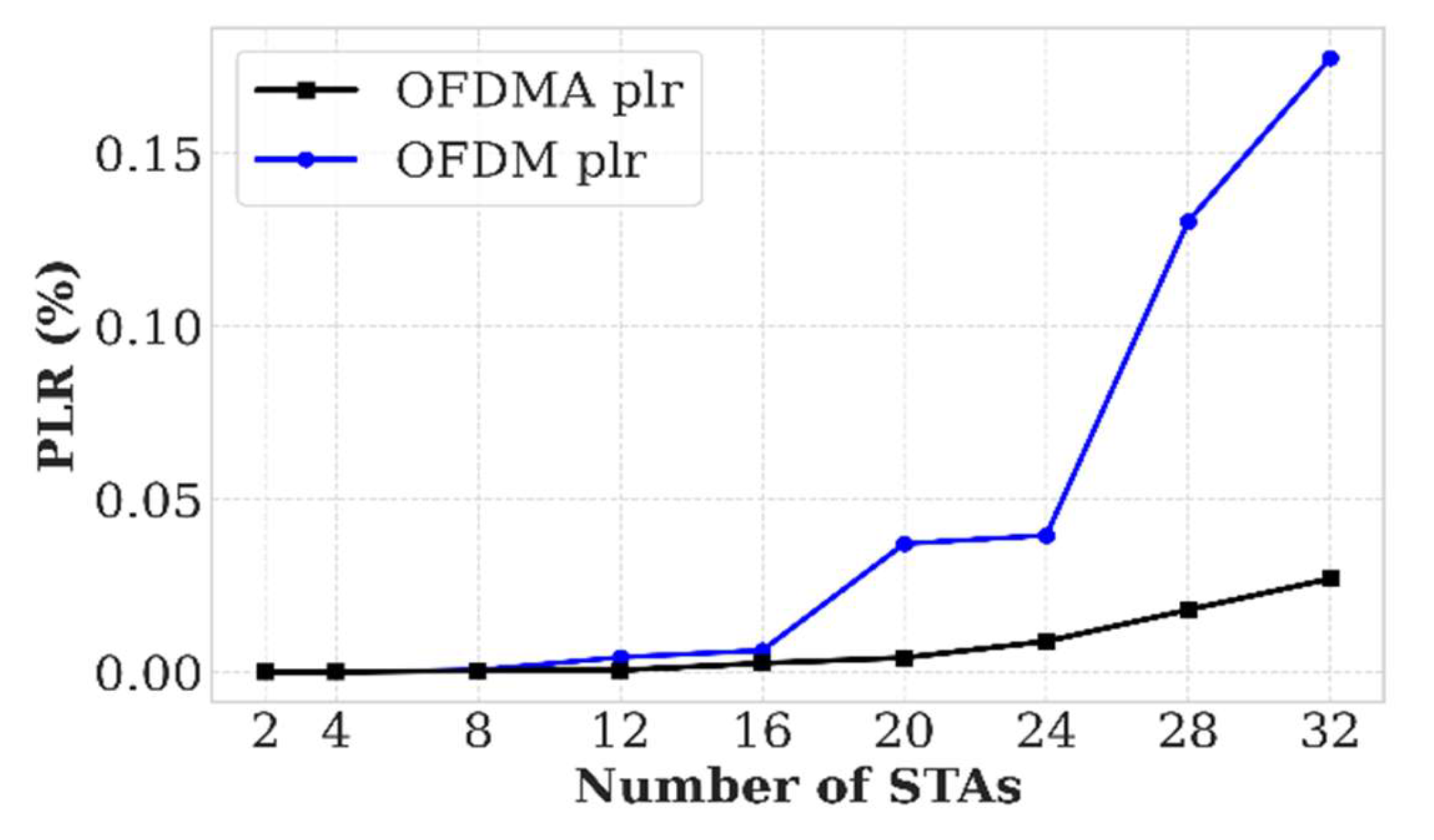
Figure 8.
Showcasing Throughput for varying numbers of STAs.
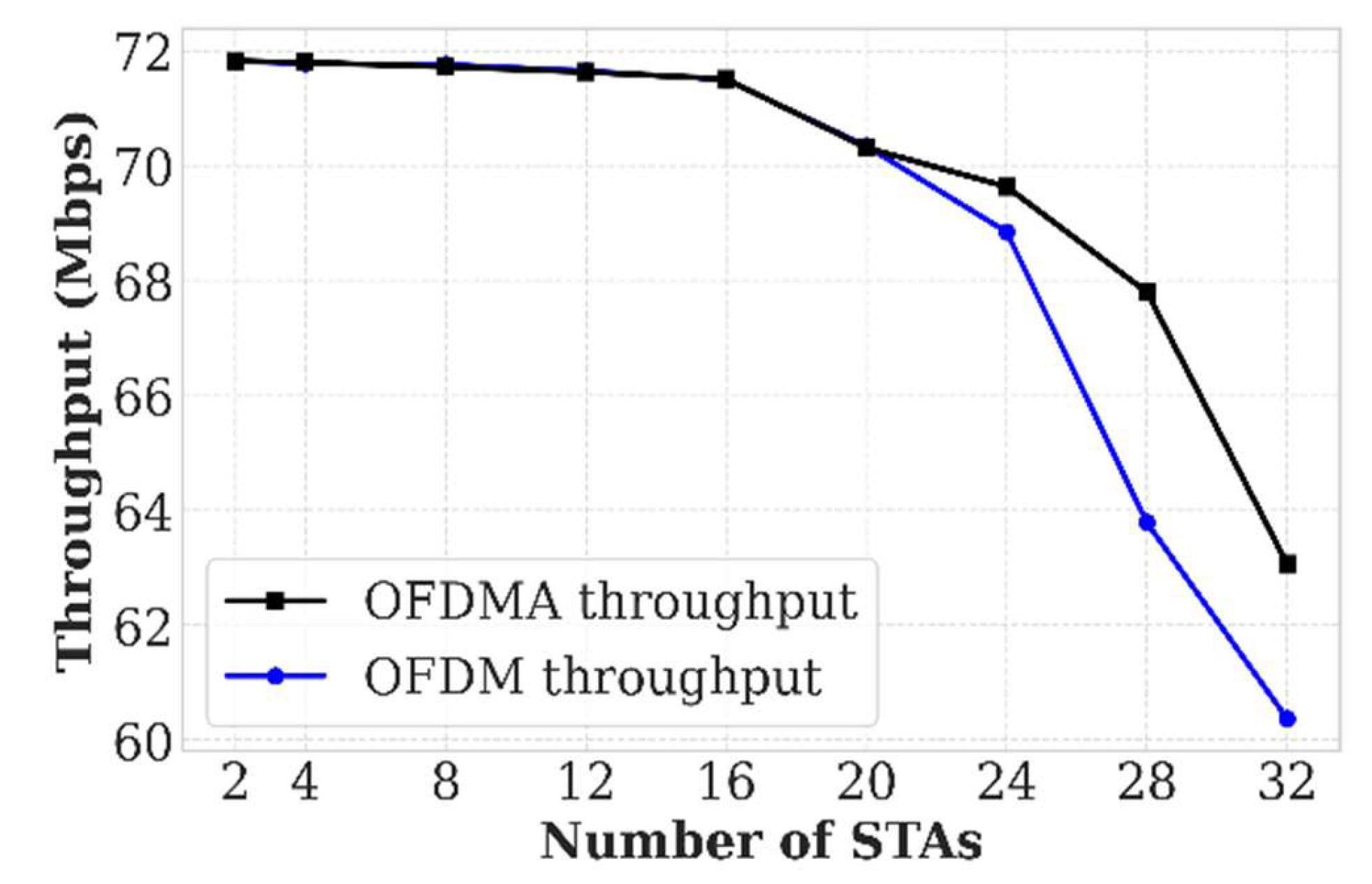
Figure 9.
Showcasing Delay for various STAs within TWT.
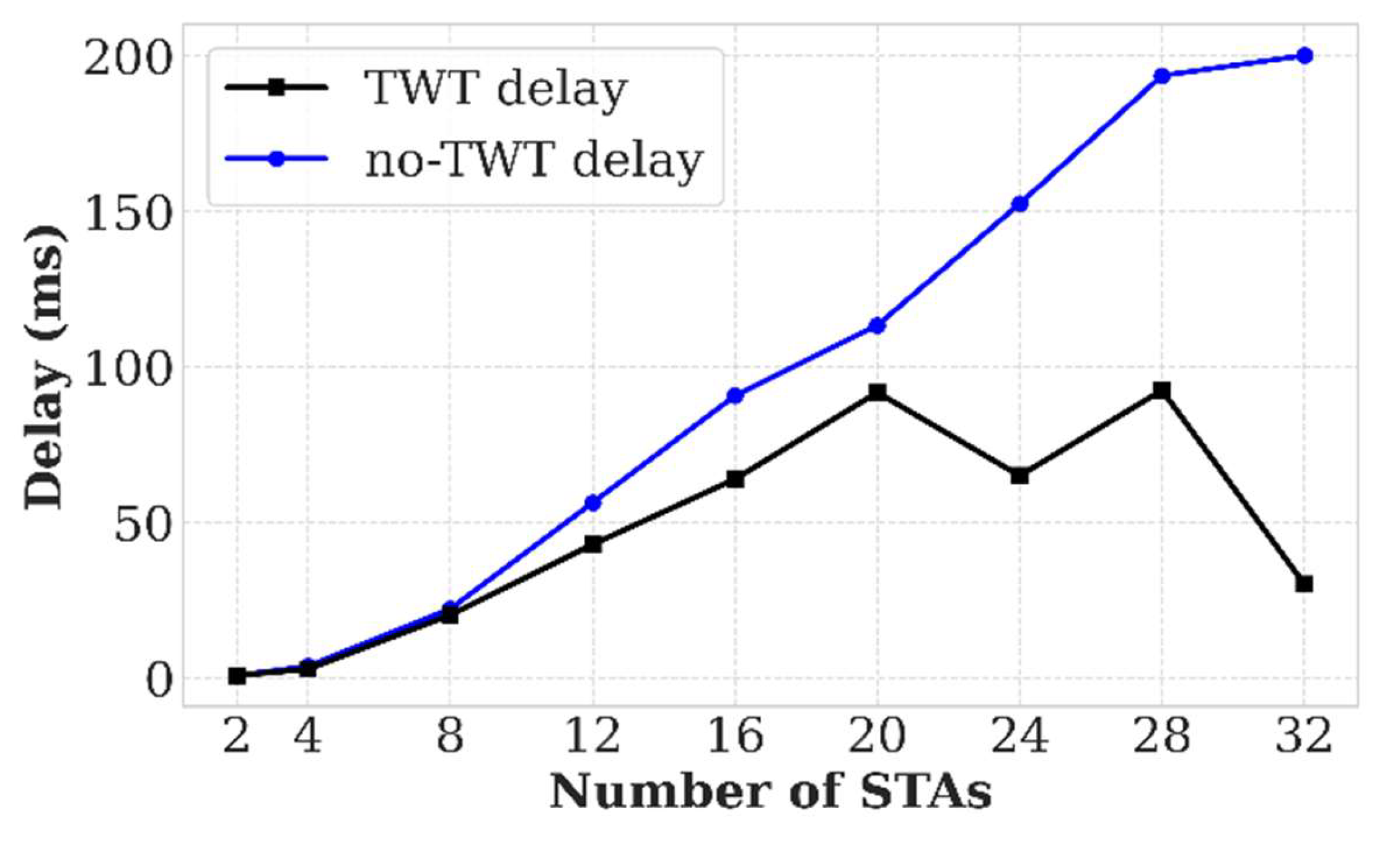
Figure 10.
Showcasing Power Consumption for various STAs within TWT.
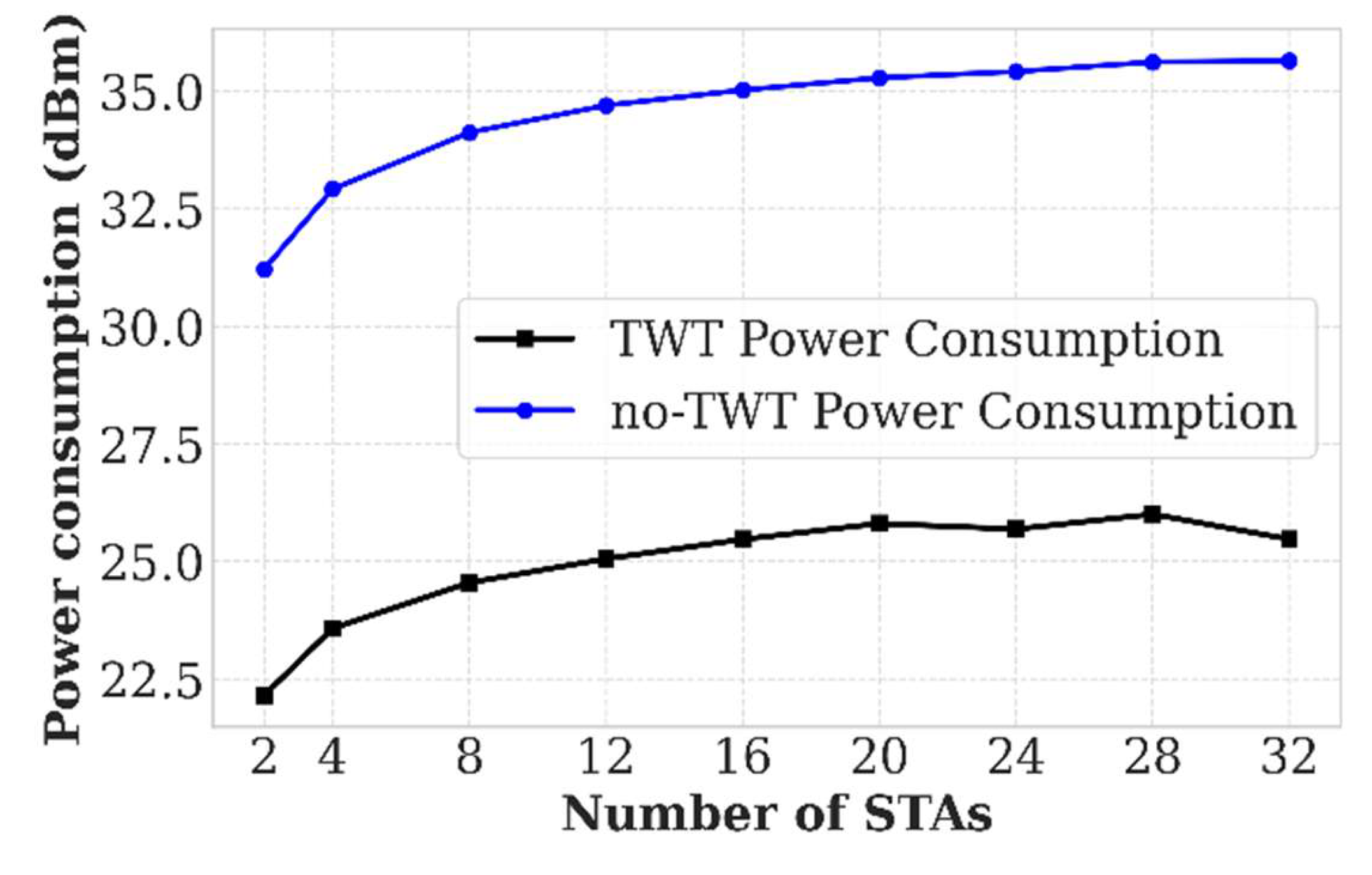
Figure 11.
Showcasing Jitter for various STAs within TWT.
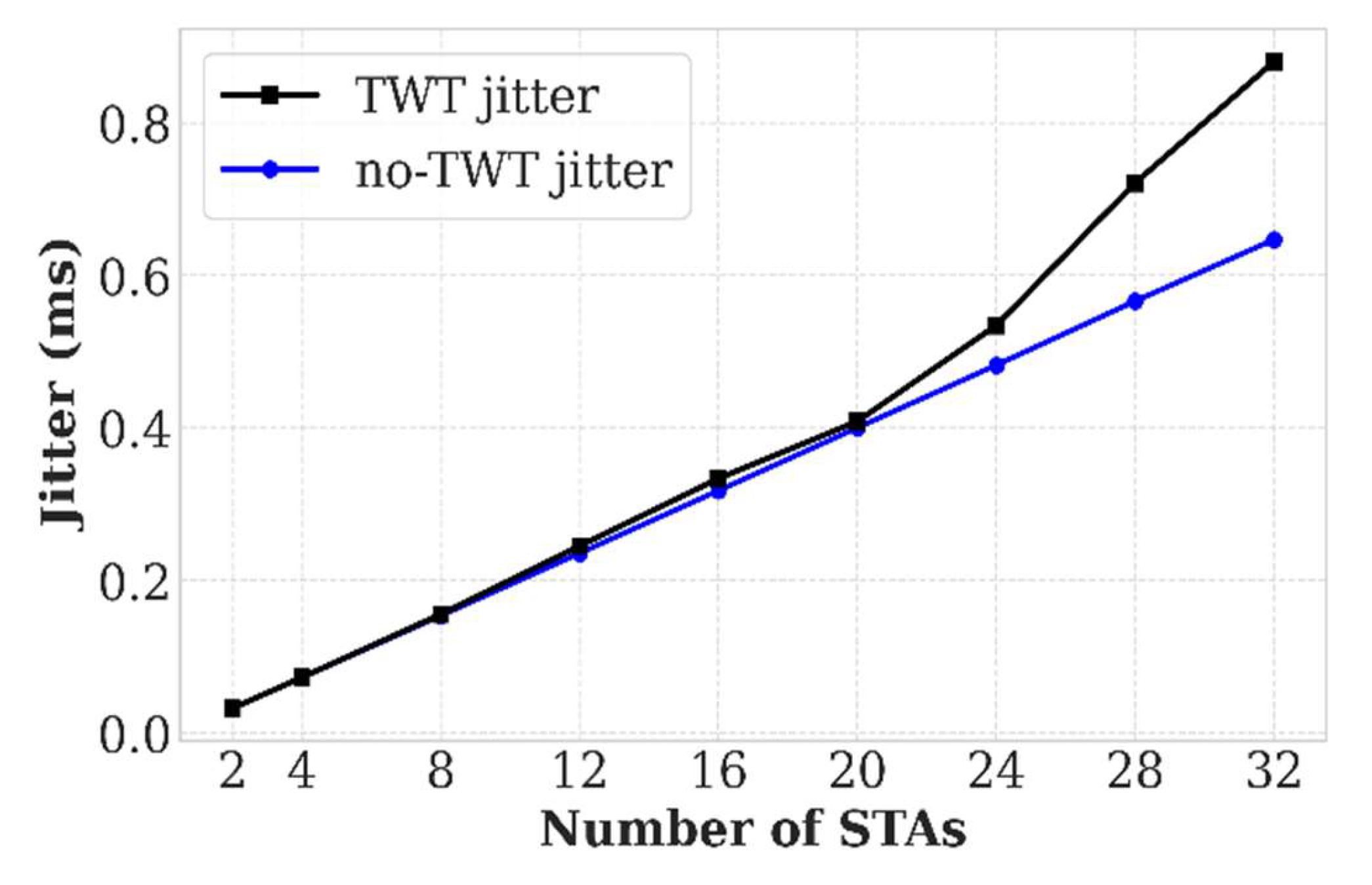
Figure 12.
Showcasing PLR for various STAs within TWT.
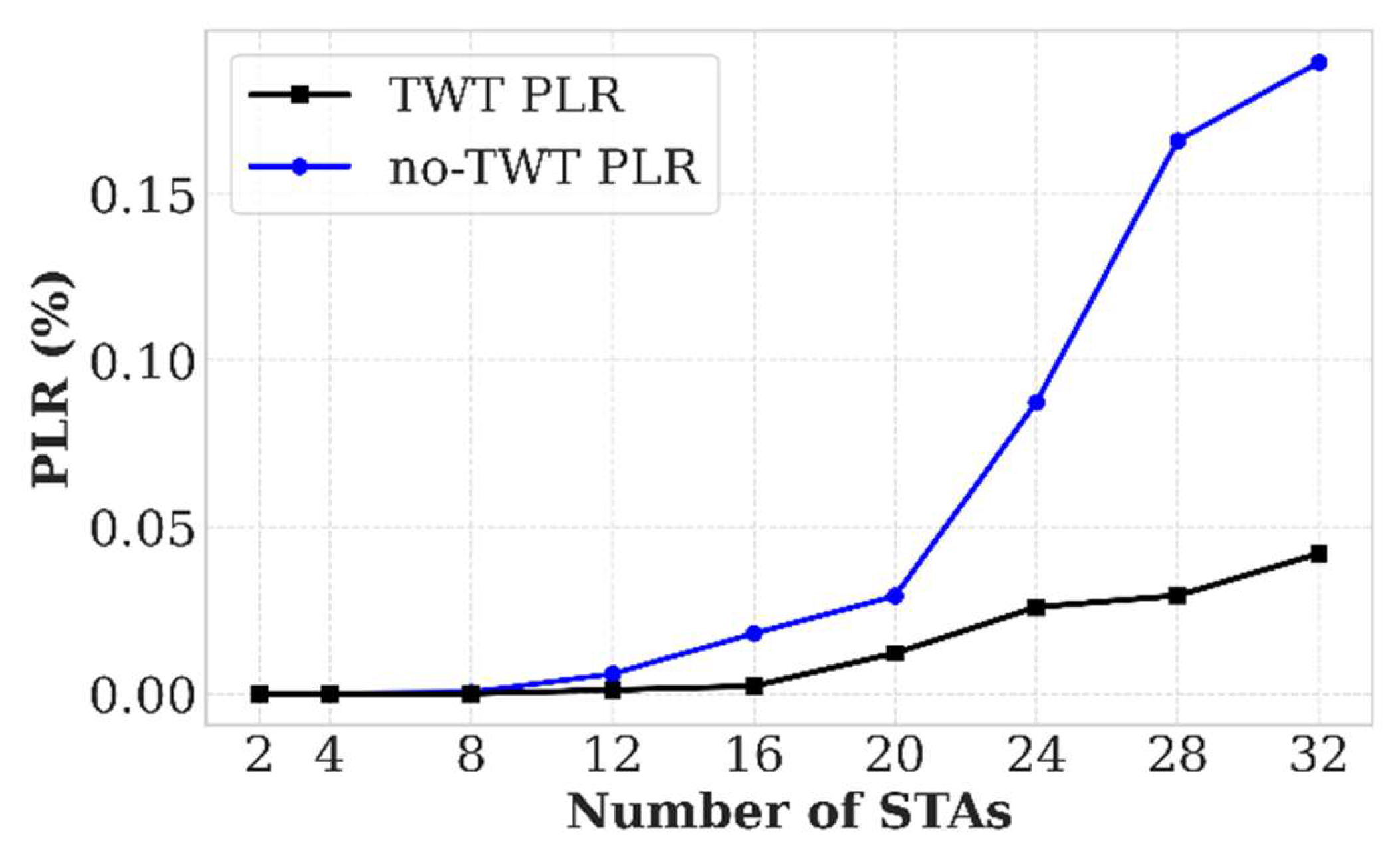
Figure 13.
Showcasing Throughput for various STAs within TWT.
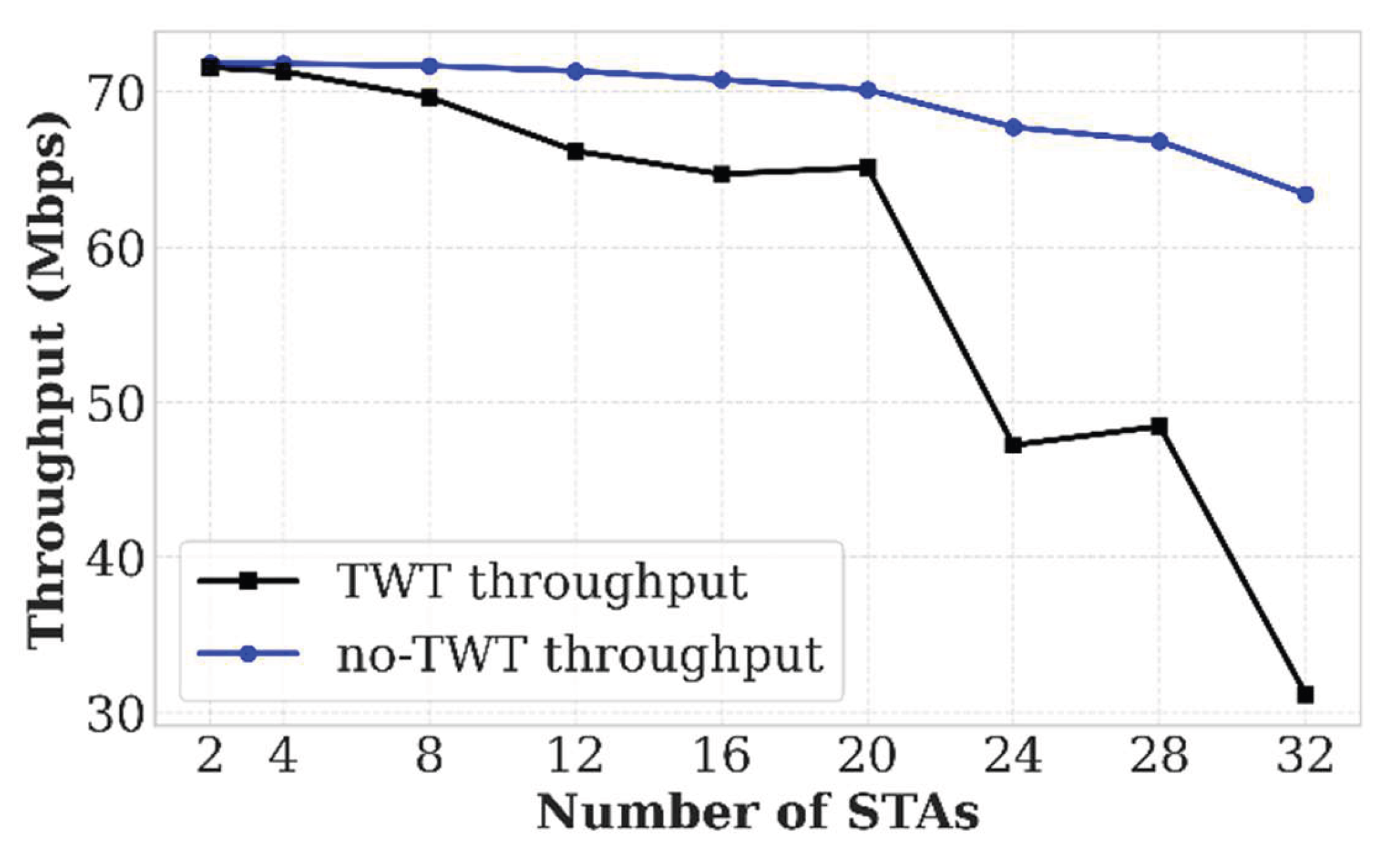
Table 1.
Simulation 1 Parameters (OFDM/OFDMA).
| Parameter | Value / Description |
| Wi-Fi Standard | IEEE 802.11ax (HE) |
| MAC Layer (OFDM) | ns3::ApWifiMac / ns3::StaWifiMac |
| MAC Layer (OFDMA) | ns3::HeApWifiMac / ns3::HeStaWifiMac |
| Scheduler | ns3::RrMultiUserScheduler (Round Robin) |
| Channel Bandwidth | 80 MHz |
| Modulation & Coding | HeMcs7 (64-QAM, 5/6 Coding Rate) |
| Guard Interval (GI) | 800 ns |
| Propagation Model | MultiModelSpectrumChannel + LogDistance |
| Simulation Time | 10 Seconds |
| Max MAC Queue Size | 1000 Packets |
| Payload Size | 64 Bytes |
Table 2.
Simulation 2 Parameters (TWT).
| Parameter | Value / Description |
| Parameter | Value / Description |
| Wi-Fi Standard | IEEE 802.11ax (HE) |
| TWT Duty Cycle | 0.2 (20% Awake / 80% Sleep) |
| TWT Scheduling Logic | ScheduleTWT (Pause/Resume Clients) |
| Energy Model | ns3::BasicEnergySource (100 J) |
| Current Draw (Tx) | 0.017 A (17 mA) |
| Current Draw (Rx) | 0.010 A (10 mA) |
| Current Draw (Idle) | 0.001 A (1 mA) |
| Current Draw (Sleep) | 0.0001 A (100 µA) |
| Simulation Time | 10 Seconds |
| Uplink Traffic Load | 50 Mbps (Aggregate) |
| Payload Size | 64 Bytes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



