Submitted:
26 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
Maternal satisfaction is a key indicator of the quality of institutional delivery services and plays an important role in improving maternal health outcomes and service utilization. The experiences and perceptions of postpartum women provide valuable insights for strengthening maternity care services. This study assessed maternal satisfaction with institutional delivery services at Mangochi District Hospital and examined the association between selected socio-demographic characteristics and overall satisfaction. A cross-sectional quantitative study was conducted among 125 postpartum women aged 18 years and above at Mangochi District Hospital. Participants were recruited using consecutive sampling. Data were collected using a structured, self-administered questionnaire that assessed socio-demographic characteristics and maternal satisfaction. Satisfaction levels were measured using a 5-point Likert scale. Data were analyzed using SPSS version 20, with descriptive statistics used to summarize satisfaction levels and Chi-square tests applied to examine associations between socio-demographic variables and overall maternal satisfaction. Overall maternal satisfaction with institutional delivery services was high, with 74.4% of respondents reporting being satisfied or very satisfied. The mean overall satisfaction score was 3.9 (SD = 1.0). High satisfaction was observed in interpersonal care, respect and dignity from healthcare providers, emotional support, and cleanliness of labour and delivery rooms. Moderate satisfaction was reported regarding waiting time, involvement in decision-making, and availability of amenities such as beds and water. Chi-square analysis showed that marital status was significantly associated with overall maternal satisfaction (p = 0.043), while age, educational level, and parity were not significantly associated with satisfaction (p > 0.05).The findings indicate that maternal satisfaction at Mangochi District Hospital is generally high, particularly in relation to interpersonal care and provider competence. However, areas such as facility comfort and service organization require improvement. Strengthening respectful maternity care, improving physical amenities, and promoting patient involvement in care decisions may further enhance maternal satisfaction.
Keywords:
institutional delivery services
; Mangochi District Hospital
; maternal satisfaction
; quantitative study
; service quality
1.1. Background of the Study
About 140 million women give birth worldwide every year, according to the World Health Organization (WHO, 2022). Many women have normal pregnancies, but serious complications can occur unexpectedly during labour and delivery. To prevent these complications, the WHO recommends that women give birth in health facilities with skilled health workers. Institutional delivery means giving birth in a properly equipped health facility that can provide safe delivery and emergency care for both mother and baby. In Malawi, maternal and newborn deaths remain a serious public health concern, despite improvements in healthcare services. Although most women in Malawi now deliver in health facilities, the quality of care and women’s experiences during childbirth vary greatly. Maternal satisfaction, how women feel about the care they receive during delivery, strongly influences whether they will use health facilities again. In districts such as Mangochi, challenges such as cultural beliefs, distance to health facilities, and transport difficulties may affect women’s experiences with delivery services. Assessing women’s satisfaction and the factors that influence it is essential for improving maternal healthcare services and promoting safe, facility-based childbirth.
1.2. Problem Statement
Institutional delivery with skilled health workers is widely recognized as the safest way to reduce maternal and newborn deaths. Malawi has achieved a high institutional delivery rate, with about 91% of women giving birth in health facilities (DHS, 2022). Despite this high coverage, many women are not fully satisfied with the delivery services they receive (Bohren et al., 2015). Poor experiences during childbirth, such as disrespectful treatment, poor communication, long waiting times, and lack of privacy, reduce women’s satisfaction. Studies in Malawi have reported cases of neglect, disrespect, and abusive maternity care in health facilities. Maternal dissatisfaction can discourage women from returning to health facilities for future deliveries.
In Mangochi District, home deliveries continue to occur, despite the presence of a district referral hospital (Ólafsdóttir, Munthali, & Gunnlaugsson, 2020). These home deliveries suggest that barriers and dissatisfaction with facility-based delivery services still exist. Women’s satisfaction with delivery services strongly influences their health-seeking behaviour and trust in the health system. Inadequate context-specific evidence on maternal satisfaction at Mangochi District Hospital limits targeted service improvements.
1.3. Research Objectives
1.3.1. Main Objective
Th research was conducted to evaluate the levels of maternal satisfaction with the utilization of institutional delivery services at Mangochi District Hospital.
1.3.2. Specific Objectives
- To assess the levels of maternal satisfaction with institutional delivery services at Mangochi District Hospital.
- To identify the factors associated with maternal satisfaction regarding the utilization of institutional delivery services at Mangochi District Hospital.
1.4. Research Questions
- How satisfied are mothers with the institutional delivery services provided at Mangochi District Hospital?
- What factors determine maternal satisfaction with institutional delivery services at Mangochi District Hospital?
2.1. Study Methodology

Table 1.
Summary presentation of study methodology.
| Component | Description |
|---|---|
| Study Design | Quantitative, cross-sectional |
| Study Setting | Mangochi District Hospital, Southern Malawi; main secondary referral facility |
| Study Population | Postnatal women aged 18-49 years admitted in the postnatal ward |
| Inclusion Criteria | Women aged 18-49, delivered at the hospital, admitted postnatally, provided informed consent |
| Exclusion Criteria | Women under 18, critically ill, or unable to communicate |
| Sampling Method | Consecutive (non-probability) sampling of eligible participants |
| Sample Size | 125 participants (calculated using single population proportion formula; 90% confidence level, 6% margin of error) |
| Data Collection Tool | Structured interviewer-administered questionnaire; pre-tested and translated into Chichewa |
| Data Collection Procedure | Administered in private areas; assistance provided for women unable to read; confidentiality maintained |
| Data Analysis | IBM SPSS v20; descriptive statistics (means, proportions, frequencies), Chi-square tests; significance p < 0.05 |
| Ethical Considerations | Approval from Catholic University Research Ethics Committee & Mangochi District Health Office; informed consent, confidentiality, beneficence, justice |
3.1. Results and Discussion
3.1.1. Demographic Characteristics of the Research Participants
Figure 1.
age distribution of respondents. A total of 125 women who had recently delivered at Mangochi District Hospital participated in the study. Most of the respondents were aged between 20 and 29 years (52%), followed by those aged 30-39 years (28%), while 20% were 40 years or older.
Figure 1.
age distribution of respondents. A total of 125 women who had recently delivered at Mangochi District Hospital participated in the study. Most of the respondents were aged between 20 and 29 years (52%), followed by those aged 30-39 years (28%), while 20% were 40 years or older.
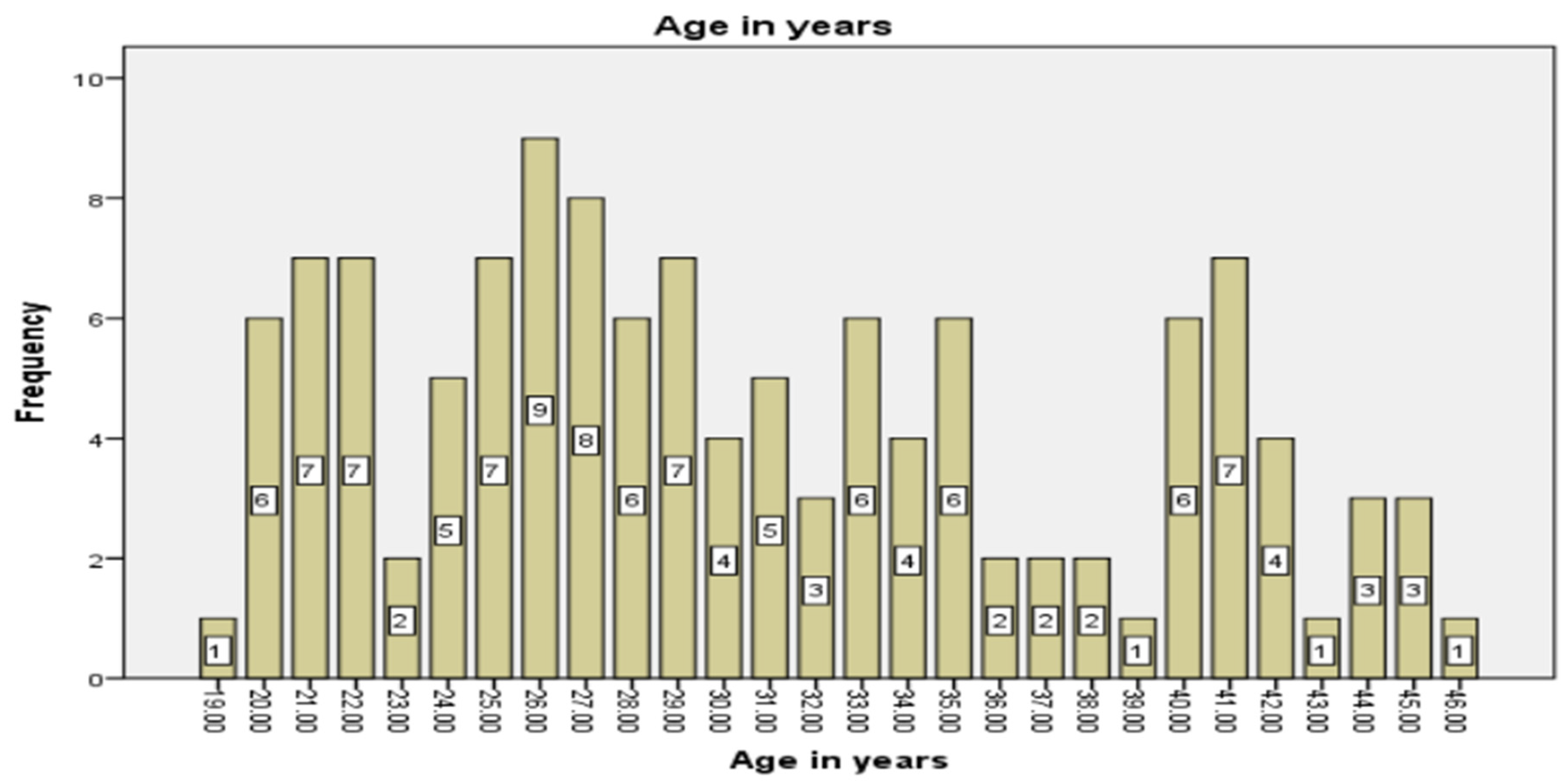
Figure 2.
Marital status of the respondents. Most women were married (70%), 15% were cohabiting, and the remaining 15%were single, divorced, or widowed, reflecting typical marital patterns in the district.
Figure 2.
Marital status of the respondents. Most women were married (70%), 15% were cohabiting, and the remaining 15%were single, divorced, or widowed, reflecting typical marital patterns in the district.
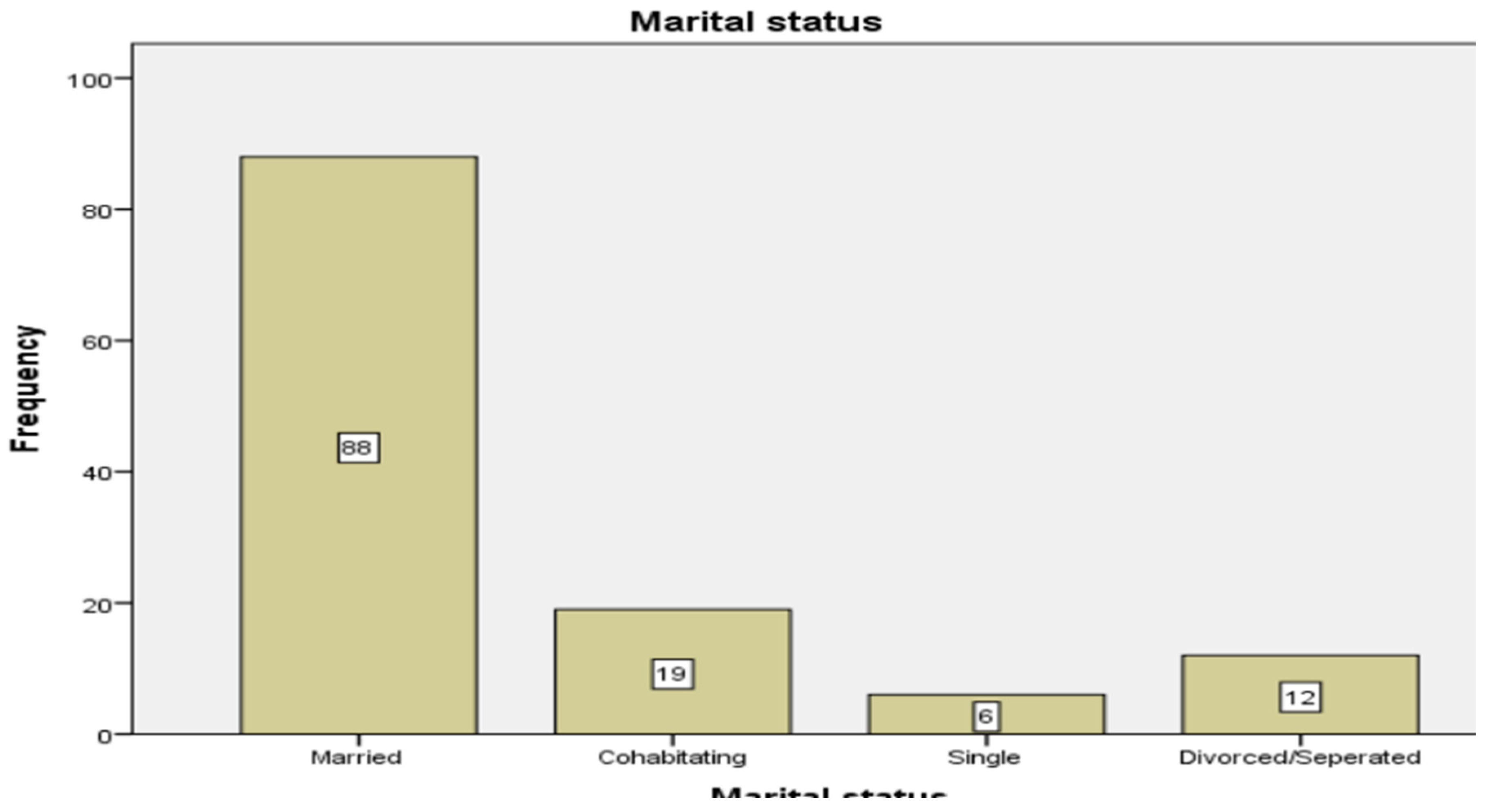
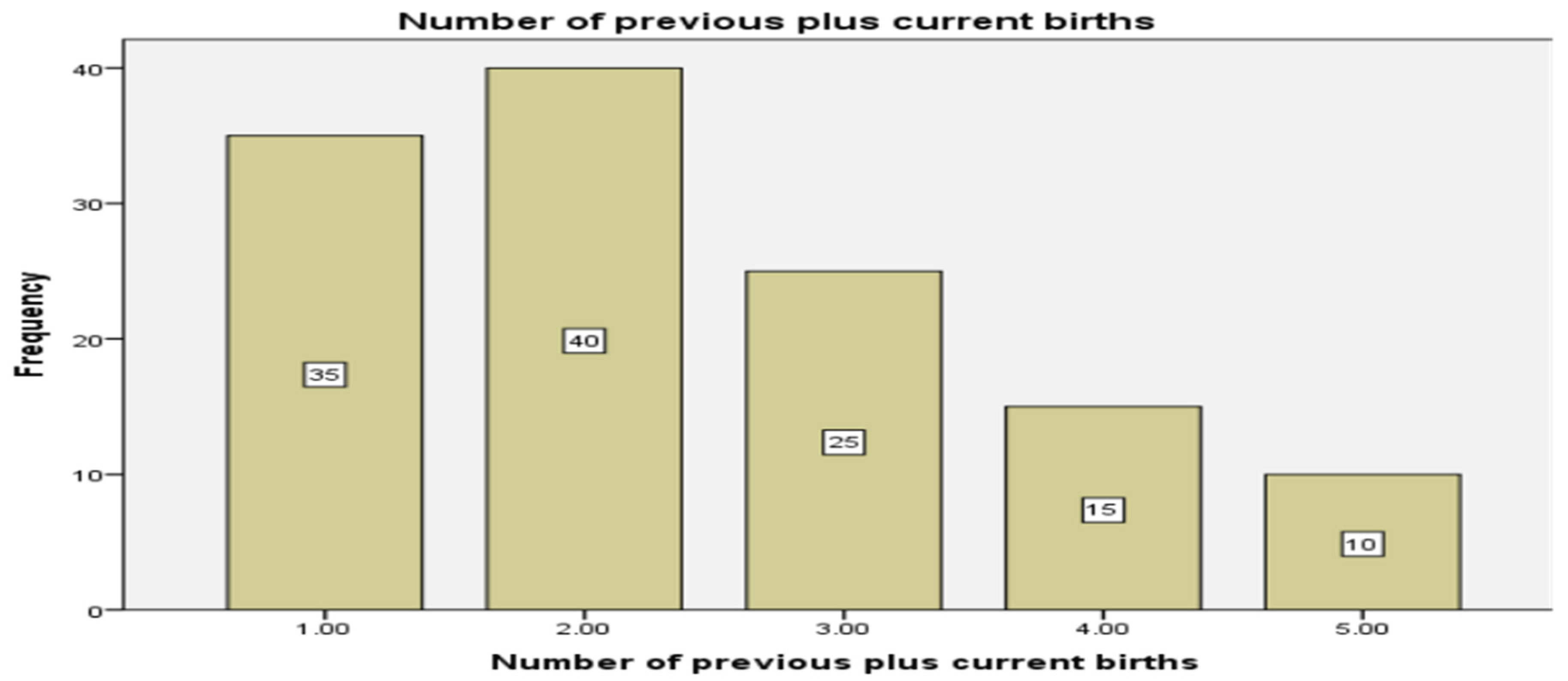
Figure 3.
parity status of the women. The average number of children per woman (parity) was 2.3, indicating that most participants had previous childbirth experience.
Figure 3.
parity status of the women. The average number of children per woman (parity) was 2.3, indicating that most participants had previous childbirth experience.
3.2. Presentation of Results
3.2.1. Satisfaction Across Service Domains
Interpersonal Care & Communication
| Descriptive Statistics | |||
| N | Mean | Std. Deviation | |
| Respect and dignity from nurses/midwives | 125 | 4.1200 | 1.03643 |
| Respect and dignity from doctors | 125 | 4.0880 | 1.03966 |
| Clarity of explanations during labor | 125 | 4.0080 | 1.08134 |
| Staff willingness to listen | 125 | 3.9440 | 1.10937 |
| Emotional support and encouragement | 125 | 3.9360 | 1.10530 |
| Valid N (listwise) | 125 | ||
Women generally felt respected and treated with dignity by nurses and midwives (mean = 4.12) and doctors (mean = 4.09). Most respondents reported that healthcare providers explained procedures clearly (mean = 4.01) and were willing to listen to questions and concerns (mean = 3.94). Emotional support and encouragement during labour was also rated positively (mean = 3.94), though this area may benefit from further attention.
Physical Environment & Amenities
| Descriptive Statistics | |||
| N | Mean | Std. Deviation | |
| Cleanliness of labour/delivery rooms | 125 | 4.1200 | 1.03643 |
| Comfort of bed/beddings | 125 | 4.0400 | 1.11731 |
| Availability of clean toilet/bathroom | 125 | 3.8640 | 1.10237 |
| Availability of clean drinking water | 125 | 3.8640 | 1.10237 |
| Privacy during examinations/delivery | 125 | 3.9680 | 1.09938 |
| Valid N (listwise) | 125 | ||
Cleanliness of labour and delivery rooms was highly rated (mean = 4.12), as was the comfort of beds (mean = 4.04). Availability of clean toilets and drinking water received moderate positive ratings (mean = 3.86), while privacy during examinations was generally satisfactory (mean = 3.97). These findings indicate that the hospital environment is generally acceptable, but some basic amenities could be improved.
Technical Quality & Resources
| Descriptive Statistics | |||
| N | Mean | Std. Deviation | |
| Confidence in midwive's skills | 125 | 3.9840 | .95870 |
| Confidence in doctor's skills | 125 | 3.9440 | 1.01046 |
| Availability of medicines | 125 | 3.8160 | 1.11720 |
| Availability of medical supplies | 125 | 3.7680 | 1.15797 |
| Assistant with pain management | 125 | 3.8800 | 1.07463 |
| Valid N (listwise) | 125 | ||
Confidence in the skills of midwives (mean = 3.98) and doctors (mean = 3.94) was high, showing that women trusted the competence of healthcare providers. Availability of medicines (mean = 3.82) and medical supplies (mean = 3.77) was rated moderately positively, indicating occasional shortages. Pain management support during labour was rated positively (mean = 3.88).
Service Delivery Process
| Descriptive Statistics | |||
| N | Mean | Std. Deviation | |
| Waiting time before being attended | 125 | 3.6800 | 1.20215 |
| Involvement in decisions about care | 125 | 3.7760 | 1.14204 |
| Care and support for newborn | 125 | 4.0560 | .96138 |
| Valid N (listwise) | 125 | ||
Satisfaction with waiting time before being attended was slightly lower (mean = 3.68), indicating some delays. Most women felt involved in decisions about their care (mean = 3.78) and were highly satisfied with care and support for their newborns (mean = 4.06).
Socio-Demographic Factors & Maternal Satisfaction
| Socio-Demographic Variable | χ² (Pearson) | Df | p-value |
| Age group Education level Marital status Parity |
106.699 6.416 21.513 8.615 |
108 12 12 16 |
0.517 0.894 0.043 0.928 |
Age, education, and parity were not significantly associated with overall maternal satisfaction, indicating that women’s satisfaction did not vary significantly across these factors. Marital status, however, was significantly associated with satisfaction (p = 0.043), with married women reporting higher satisfaction compared to single, cohabiting, or widowed women. This suggests that social support and family structure may influence how women perceive and experience maternity care. Overall, these results highlight that while satisfaction is generally high, attention should be paid to improving waiting times, availability of basic amenities, and inclusion in decision-making to enhance women’s experiences further.
3.3. Discussion of Results
The majority of women in the study were aged 20–29 years, reflecting the peak reproductive age and their higher likelihood of using institutional delivery services, as young women are often more aware of the benefits of skilled birth attendance (Jang et al., 2024). Most respondents were married, highlighting the importance of social and economic support in accessing healthcare services. Marriage can facilitate timely decisions, transportation, and overall support during childbirth, influencing maternal satisfaction positively (Zeleke et al., 2025). Educational attainment varied, with most women having completed primary or secondary education. Higher education empowers women to understand health information, navigate healthcare systems, and make informed decisions about their care, which can enhance satisfaction (Srivastava et al., 2015).
Overall, age, parity, and education did not significantly affect maternal satisfaction, suggesting that the hospital provides relatively equitable care across different demographic groups. However, unmarried or adolescent mothers may face unique challenges that require targeted support. Interpersonal care and communication were highly rated, with women reporting that nurses, midwives, and doctors treated them with respect and dignity, listened to their concerns, and provided clear explanations, reinforcing trust in the facility and promoting continued use of services (Srivastava et al., 2015; Jang et al., 2024). Emotional support during labor, while generally positive, showed room for improvement. Providing reassurance, encouragement, and empathetic gestures can reduce anxiety, enhance satisfaction, and strengthen trust in healthcare providers (Ope et al., 2025).
Mothers expressed high satisfaction with the cleanliness of labor rooms and privacy during examinations and delivery, reflecting the importance of these factors in shaping perceptions of care quality. Clean and private environments are essential for both physical safety and emotional comfort (WHO, 2016; Bohren et al., 2019; Afulani et al., 2018). Satisfaction with the availability of basic amenities, such as comfortable beds, clean toilets, and essential supplies, was moderate, indicating that resource limitations can affect overall experience despite high-quality interpersonal care (Srivastava et al., 2015; Banda et al., 2021).
Mothers reported strong confidence in the technical competence of midwives and doctors, which positively influenced feelings of safety and satisfaction. However, occasional shortages of medicines and medical supplies highlighted the need for reliable logistical support to complement skilled care (Srivastava et al., 2015; Turigye et al., 2025).
4.1. Conclusion
Approximately 75% of mothers at Mangochi District Hospital reported satisfaction with delivery care, highlighting generally positive experiences with institutional maternal services. Interpersonal aspects of care, including respect, kindness, and effective communication from healthcare providers, were key factors influencing maternal satisfaction. Confidence in the technical competence and skills of doctors and midwives emerged as a critical pillar of maternal satisfaction, reinforcing the importance of professional expertise in delivery care. While the hospital performed well in clinical care, some environmental and comfort-related aspects, such as hospital bed quality and availability of basic amenities, received lower satisfaction ratings, indicating areas for improvement. The findings underscore the need for ongoing staff training, strengthening interpersonal and technical skills, and improving hospital resources and infrastructure to enhance maternal experiences and overall satisfaction, offering guidance for policymakers and hospital managers.
References
- Abdulraheem, I. S., and D. B. Parakoyi. 2009. Factors affecting mothers’ healthcareseeking behaviour for childhood illnesses in a rural Nigerian setting. Early Child Development and Care 179, 5. [Google Scholar] [CrossRef]
- Ajzen, I. 1991. The theory of planned behavior. Organizational Behavior and Human Decision Processes 50, 2. [Google Scholar] [CrossRef]
- Banda, C., T. Gondwe, and M. Nyirenda. 2021. Factors influencing women’s satisfaction with childbirth services in rural Malawi: A cross-sectional study. BMC Pregnancy and Childbirth 21, 1. [Google Scholar] [CrossRef]
- Banda, H., A. Kazembe, and G. C. Chirwa. 2021. Women’s satisfaction with maternal health services in Malawi: Evidence from health facility surveys. BMC Pregnancy and Childbirth 21, 1. [Google Scholar] [CrossRef]
- Bitew, K., M. Ayichiluhm, and K. Yimam. 2015. Maternal satisfaction with delivery services and associated factors at public health facilities in Debre Markos Town, Northwest Ethiopia. BMC Pregnancy and Childbirth 15, 1. [Google Scholar] [CrossRef]
- Bohren, M. A., J. P. Vogel, E. C. Hunter, O. Lutsiv, S. K. Makh, J. P. Souza, C. Aguiar, F. Saraiva Coneglian, A. L. A. Diniz, Ö. Tuncalp, D. Javadi, O. T. Oladapo, R. Khosla, M. J. Hindin, and A. M. Gülmezoglu. 2015. The mistreatment of women during childbirth in health facilities globally: A mixed-methods systematic review. PLoS Medicine 12, 6: e1001847. [Google Scholar] [CrossRef]
- Chimwaza, W., E. Chipeta, A. Ngwira, and J. Chinkhumba. 2014. Women’s experiences of maternal health care in Malawi. Malawi Medical Journal 26, 3. [Google Scholar]
- Donabedian, A. 1988. The quality of care: How can it be assessed? JAMA 260, 12: 1743–1748. [Google Scholar] [CrossRef]
- Ezo, E. E., A. B. B. Mensah, and W. Agyemang-Duah. 2024. Determinants of maternal satisfaction with facility-based delivery services in sub-Saharan Africa. BMC Health Services Research 24, 1. [Google Scholar] [CrossRef]
- Government of Malawi. 2022. Malawi Health Sector Strategic Plan II (2017-2022). Ministry of Health. [Google Scholar]
- Ijadunola, M. Y., K. T. Ijadunola, O. A. Esimai, T. C. Abiona, and A. B. Adeyemi. 2007. New paradigm, old thinking: The case for emergency obstetric care in the prevention of maternal mortality in Nigeria. BMC Pregnancy and Childbirth 7, 1. Available at. [Google Scholar] [CrossRef]
- Jang, Y., S. Kim, and H. Lee. 2024. Quality of maternal healthcare and women’s satisfaction in low- and middle-income countries: A systematic review. International Journal for Quality in Health Care 36, 1. [Google Scholar]
- Kruk, M. E., S. Kujawski, G. Mbaruku, K. Ramsey, W. Moyo, and L. P. Freedman. 2014. Disrespectful and abusive treatment during facility delivery in Tanzania. Health Policy and Planning 33, 1. [Google Scholar] [CrossRef]
- Kruk, M. E., M. Paczkowski, G. Mbaruku, H. de Pinho, and S. Galea. 2014. Women’s preferences for place of delivery in rural Tanzania. American Journal of Public Health 99, 9. [Google Scholar] [CrossRef]
- Malawi National Statistical Office (NSO). 2018. 2018 Malawi Population and Housing Census: Main report. NSO.
- & ICF, 2022) Malawi National Statistical Office (NSO) & ICF Malawi Demographic and Health Survey 2022, 2022. NSO and ICF.
- Mangochi District Hospital. 2023-2024. Annual delivery statistics report. Health Information Management System (HIMS). [Google Scholar]
- Mehata, S., Y. R. Paudel, M. Dariang, K. K. Aryal, P. Poudel, and S. Barnett. 2017. Factors determining satisfaction among facility-based maternity clients in Nepal. BMC Pregnancy and Childbirth 17, 1: 319. [Google Scholar] [CrossRef] [PubMed]
- Msonthi, J. D. 1983. Traditional birth attendants in Malawi: Their role in primary health care and development. The Society of Malawi Journal 36, 1: 40–44. [Google Scholar]
- Msiska, G., M. K. Kumwenda, and E. Chirwa. 2018. Disrespectful and abusive maternity care in Malawi: A literature review. Malawi Medical Journal 30, 1. [Google Scholar]
- Mugambe, R. K., T. Malinga, and J. Nabunya. 2020. Quality of maternity care in Uganda: A mixed-methods study on patient satisfaction. BMC Health Services Research 20, 1. [Google Scholar] [CrossRef]
- Nyondo, A. L., W. Chimwaza, S. R. Muheriwa, and C. Chitsulo. 2020. Community perceptions and experiences of facility-based delivery in Southern Malawi. BMC Pregnancy and Childbirth 20, 1. [Google Scholar] [CrossRef]
- Schroeder, E., R. Tallarico, and M. Bakaroudis. 2022. The impact of adolescent initiation rites in East and Southern Africa. International Journal of Adolescence and Youth 27, 1: 181–192. [Google Scholar] [CrossRef]
- Shiferaw, K. 2022. Maternal satisfaction and utilization of institutional delivery services: A review. International Journal of Nursing and Midwifery 14, 2: 23–30. [Google Scholar]
- Srivastava, A., B. I. Avan, P. Rajbangshi, and S. Bhattacharyya. 2015. Determinants of women’s satisfaction with maternal health care. BMC Pregnancy and Childbirth 15, 1: 97. [Google Scholar] [CrossRef] [PubMed]
- Turigye, E., T. Nkurunziza, and G. Uwizeye. 2025. Health system supply constraints and maternal satisfaction in East Africa. Health Policy and Planning 40, 2: 145–154. [Google Scholar] [CrossRef]
- UNICEF Malawi. 2019. Access to healthcare in Malawi: The distance challenge. UNICEF Malawi Country Office. [Google Scholar]
- World Bank. 2021. Maternal mortality ratio (modeled estimate, per 100,000 live births) Malawi. Available online: https://data.worldbank.org.
- World Health Organization. 2018. WHO recommendations: Intrapartum care for a positive childbirth experience. WHO. [Google Scholar]
- World Health Organization. 2020. Strategies toward ending preventable maternal mortality (EPMM). WHO. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



