
Submitted:
12 July 2024
Posted:
12 July 2024
You are already at the latest version
Abstract
The fulfillment of rights to maternal healthcare is a key factor for wellbeing of woman. However, there is a lack of instrument to know the experience of women during maternity to bind the monitoring. The aim of this study was to validate an instrument to measure the woman’s perception of the fulfillment of rights during healthcare in pregnancy, childbirth and immediate postpartum. The instrument consist in 50 items was screening by an exploratory factor analysis. Additionally, the final version of the instrument consists in 29 items which was validate by confirmatory factor analysis and know-group validity. The instrument was applied in 185 Spanish women. The global Aiken’s V of initial instrument proposal was 0.89. Process resolves an instrument with 5 factors (information, privacy, consent, support, and participation) that explained the 60% of the total variance. The score of the instrument was correlated with resilience, maternity beliefs, and positive and negative affect. External validation showed relations with age, gravida, and number of labors. Additionally, the reliability Cronbach´s was 0.93 [0.91; 0.94]. In conclusion, the instrument developed is consistent and has appropriate psychometric properties for assess the fulfillment rights maternity healthcare.
Keywords:
Maternity rights
; Healthcare during pregnancy
; Vulnerability
; Perception of fulfillment
1. Introduction
The maternal health is one of the rights recognized in the United Nations Human Rights Council. The WHO highlight the importance of addressing the mistreatment of women during childbirth to reduce mortality and morbidity in maternal and neonatal care [1]. However, conventional approaches to maternity do not adequately address quality care that are highly valued by mothers. The mostly described consequences has been unintentional harm, dehumanization, bodily remembrance, mental illness, and sexual issue [2,3]. Therefore, women continue to experience mistreatment during childbirth [4].
Maternal and neonatal well-being are affected by how women are treated during pregnancy, childbirth and postpartum. From European countries, around the 20% of women reported abuse during her antenatal care [5]. In addition, in low/middle-income countries, close to 42% of women attending during postpartum had experienced physic-verbal abuse or discrimination [6]. The maternity vulnerability is defined by devoid of care, suffering and loss of value as a human being [7]. The factors that contributed to the experience of vulnerability have been described as young women, economic difficulties or unemployed, and illiterate [8]. Among others, the characteristics that could modulate the perception of abuse are negative life events in previous pregnancy or childbirth, and the lack of social support.
The perceived fulfillment of women’s rights during maternity plays a key role in the vulnerability during the health care process. In an observational study was showed that women preferred woman-centered and continuity of care models, not only during pregnancy and childbirth, but also during postpartum period [9,10]. The data support that perceived compliance with rights, such as the birth plan, improved clinical maternity outcomes.
The perception of poor quality of healthcare is a powerful determinant of use of maternity services [11,12]. The universal rights of women and newborns described in the respectful maternity care charter of the White Ribbon Alliance [13] described that everyone has the right: 1) to information, informed consent, and respect their choices during maternity care; 2) to privacy and confidentiality; 3) to be treated with dignity and respect; 4) to equality, freedom from discrimination and equitable care; 5) to highest attainable level of health; 6) to liberty, autonomy, self-determination; and 7) every child, to be with their parents or guardians. Therefore, there are international agreements that support all women having access to a humanized maternity care system in which woman-centered care has a positive impact on birth experiences and outcomes [14]. However, research across countries and cultures need the appropriate instruments, which can provide a benchmark to enable meaningful comparisons [3,15,16].
There are instruments focus on the evaluation of maternal satisfaction with the healthcare received during labor and hospital stay, mostly evaluated in healthy women with low-risk obstetric pregnancies [17]. The Mothers on Respect (MOR) index is an instrument that assess the maternity care experience with providers about healthcare options [16]. However, MOR index does not measure the fulfillment of maternity rights and postpartum period. Further research is needed to improve instruments through psychometric testing, consideration different maternity periods, and joint assessment of perception of fulfillment maternity rights and experience of abuse.
In this article, it describes a women-centered research process to develop and validate an instrument to measure the perception of the fulfillment of women rights during maternity, from pregnancy to immediate postpartum covering also the childbirth situation.
2. Materials and Methods
2.1. Fulfillment in Maternity Rights Instrument
The fulfillment perception in maternity rights (FMR) was measured by 50 items. According to the universal rights of women and newborns [13,18]. The items covering the perception of the women related to adequate health information and request informed consent during medical procedures; privacy and confidentiality of medical data; to be treated integrally with dignity and respect; quality healthcare; autonomy, and participation in self-healthcare decision. The items cover not only the last pregnancy and childbirth but also the early last postpartum (up to 40 days after childbirth). The Spanish version of the original 50-item proposed was showed in Table S1. The response was built in a 5 points Likert scale, being 0=“never” and 4=“always”. The interpretation of the scale would be to higher score, higher perception of the fulfillment right. Consistently, the scale of the items 33, 41, 48 and 49 were inverted.
2.2. Evaluation by Judges
This evaluation was carried out by five expert judges in women’s right and maternity research. The Aiken’s V coefficient (V) was used to analyze the content validity. The possible outcomes ranged from 0−1, where 1 represents a perfect agreement among the judges and 0 is general disagreement. The value of this coefficient was considered acceptable at values >0.7 [19]. For this study, the language clarity, the item relevance, and the item coherence were assessed aspects.
2.3. Pilot Test
The comprehensibility of the scale was carried out in a sample of 27 women, selected by non-probabilistic sampling at the discretion of the research team. This inclusion criteria of this pilot cohort were women ≥18 years; to have undergone a labor or C-section in the last 3 years; to have received healthcare for the last pregnancy, labor and early postpartum (up to 40 days after labor); and good Spanish language understanding. Women were asked to assess the understandability of the questionnaire and to suggest changes if they deemed it appropriate, and therefore, the women could contact the research team to improve their understanding of the items.
2.4. Participants and Study Design
Collection and recruitment sample was done by the social media, an adequate technique to recruitment [20]. In the recruitment, 278 women were contacted. Inclusion and exclusion criteria were applied to the women contacted. The inclusion criteria were equal to the pilot test cohort. The exclusion criteria were inability to read/write in Spanish and home birth. Finally, 185 met the inclusion and exclusion criteria. Data were collected from September 2021 to November 2023.
A self-administered online tool was prepared by Qualtrics (https://www.qualtrics.com/es/). Firstly, it was obtained sociodemographic and obstetric variables, and validated psychometric tests and, secondly the FMR instrument.
The sociodemographic and obstetric variables were women age (years), education level, civil status (single/unmarried vs any type of relationship), employ status (active working vs unemployed), parity (number of labor), type of last labor (vaginal vs C-section), if the last pregnancy was intended (yes/no), gestational age in the last pregnancy (weeks), and adverse outcomes (yes/no) during pregnancy (i.e.; preeclampsia or gestational diabetes), labor (i.e.; premature rupture of membrane or intrapartum hemorrhage) or early postpartum (such as mastitis or sepsis).
To assess divergent validity, women responded to 1) the Resilience scale [21], assessing the ability to cope with daily difficulties by 14-items. The higher score, the greater the woman’s ability to cope with the problems of everyday life. Other studies reported a reliability of 0.88 [22]. 2) The Positive and Negative Affect Schedule (PANAS) [23] to measure emotion by 20 items (10 items measuring positive affect and 10 items measuring negative affect). For the positive score, a higher score indicates more positive emotions. For the negative score, a lower score indicates fewer negative emotions. The PANAS obtained a reliability of 0.87−0.91 [24]. 3) The Maternity Beliefs Scale (MBS), identifying beliefs that women have related to maternity. The MBS has 13 items, clustered in: maternity as a sense of life (MBS-life) and maternity as a social duty (MBS-social). The higher score, the higher the woman’s belief in the domain. The previous reliability was 0.93 [25].
Finally, women responded to FMR instrument, a tool designed to assess the perception that women have of fulfillment in maternity rights during pregnancy, labor or postpartum.
2.5. Statistical Analysis
The descriptive analysis was summarized by mean, median, standard deviation (SD), standard error of mean (SEM), and interquartile range [Q1; Q3]. The skewness and kurtosis were calculated for each item and factor, and the Spearman´s coefficient (Rho) was used to test the correlations.
The data analysis consisted in an Exploratory Factor Analysis (EFA) and was verified by a Confirmatory Factor Analysis (CFA). The EFA was conducted to determine the possible clustering of dimensions. The statistic Kaiser-Meyer-Olkin (KMO) and the Bartlett’s test of sphericity were used to check if the data were suitable for this analysis. In addition, follow the Cattel´s test and parallel plot, it was stablished the number of factors to retain, considering the point where the eigenvalue declines steeply and then levels off. The principal component analysis with varimax rotation was also used, eliminating items with factor loadings <0.3 similar to Amado-Mateus [26]. In addition, it was also excluded the item with complexity (com) >1.9. Basically, com=1 indicated that the item loads only on one factor, being 2 evenly loads on two factors.
The factors of the EFA were used for factor conformation. The CFA was estimated by the maximum likelihood. The CFA extracted indexes and thresholds were minimum discrepancy ratio (χ2/df; MR<5), comparative form index (CFI>0.9), normed fit index (NFI>0.9), Tucker-Lewis’s index (TLI>0.9), adjusted goodness-of-fit- index (aGFI>0.8) and root mean square error of approximation (RMSEA<0.08). The convergent analysis of the factors was carried out by the Average Variance Extracted (AVE), the omega (ω) reliability, and Cronbach’s alpha (α) were determined. The values considered acceptable were AVE>0.5, reliability>0.7, and α>0.8. Finally, the Maximum Shared Variance (MSV) and Average Shared Variance (ASV) statistics were calculated, being considered acceptable when MSV and ASV are <AVE. The direct score of the factors was calculated by sum the items belong the factor and divide by number of items in the factor. The standardized (std) factor score was calculated by multiply the standardized coefficient of CFA of each item and sum each standardized item. The total score (FMR) was calculated by averaging the factor scores. The standardized FMR score was calculated considering the standardized coefficient of the factor in the CFA model.
The validated psychometric scales and subscale scores were standardized by Rho coefficient, considering statistical correlation p-Value (P)<0.05. In addition, an inferential analysis by Mann–Whitney´s U test was conducted to compare groups of women likely to have experienced obstetric vulnerability according to several aspects described in the literature [3]. The p-value(P)<0.05 were considered statistically significant.
The data analyses were performed using R software within the RStudio interface (version 2022.07.1+554, 2022, R Core Team, Vienna, Austria) using rio, dplyr, compareGroups, devtools, corrplot, ggcorrplot, psych, DiagrammeR and lavaan packages. For reliability was also used eRm and TAM packages.
2.6. Ethics Statement
This study was approved by the Research Ethics Committees (CEI-112-2199, January 22, 2021). All women willing to participate were given an online information sheet, describing the aims of the study, and the informed consent form was signed in each case. Data collection was anonymous, and databases were blinded. In addition, this study is adhered to the guidelines Standards for the Reporting of Diagnostic Accuracy Studies (STARD) [27] for assessment scale protocols.
3. Results
3.1. Content Validity
The judges had a high level of agreement for the language clarity (V=0.90), the item relevance (V=0.89), and the item coherence (V=0.89), being the global Aiken’s V coefficient = 0.89. Pilot cohort did not report difficulties in understanding any of the items. Therefore, item modifications were not introduced.
3.2. Descriptive of Sample
The women age was 28.5±0.5 years; being nulliparous the 54.6%, and multiparous the 45.4%. Regarding the education level, the 5.5% had primary education, the 47.2% secondary education and the 47.2% university studies. The 17.8% of the women was unmarried/single, being the 82.2% married or in a sentimental relationship. Related to employ situation, the 55.2% was actively working and the 44.8% was unemployed. In the 76.7% of the women, the last pregnancy was intended. The gestational age was 38.7±0.1. The 48.5% of the women were performed C-section in any gestation. Regarding to the obstetric outcomes, pregnancy complications was presented in the 31.9% women, complications during labor in the 17.2% and during early postpartum period in 16.0%.
3.3. Construct Validity by Factor Analysis
Exploratory factor analysis. EFA was performed based on the initial proposed 50-item FMR instrument (correlation coefficients are showed in the Figure S1). The items shown sphericity (Bartlett’s test: χ2=9468.3; P<0.001) and the KMO values indicated an acceptable fit of the sample (KMO=0.84). In addition, the parallel analysis suggested to be retained 7 components. This solution showed a 56.2% of the explained variance. The items with factor loading <0.3 (items 10, 30, and 41) and complexity>1.9 (items 8, 12, 14, 18, 19, 20, 21, 24, 25, 26, 33, 34, 38, 39, 40, 43, 44, 48) were excluded (Table S2).
The final solution of the instrument included 29 items. The descriptive analysis of these items was show in Table 1.
The parallel analysis retained 5 components that explained the 60% of the total variance. The Table S3 show the standardized loadings based on correlation rotated matrix. According to the EFA, factor 1 gathers items related to receive adequate healthcare information (Factor 1=Information), factor 2 gathers rights related to privacy and confidentiality of health information (Factor 2=Privacy), factor 3 refers to consent to medical procedures (Factor 3=Consent), factor 4 refers to social support during maternity (Factor 4=Support) and factor 5 to participation and active listening in medical treatment (Factor 5=Participation).
Confirmatory factor analysis. CFA was showed in Figure 1 and descriptive analysis of the factors were reported in Table 2.
The standardized MR of the model was 3.4 and the scaled MR was 2.6. The CFI was 0.99 (scaled=0.97) and the TLI was 0.99 (scaled=0.97). The RMSEA was 0.092 [0.085; 0.099], the NFI was 0.66 and the aGFI was 0.55. The global AVE was 0.79 and the Cronbach’s α was 0.93 [0.91; 0.94]. All the indexes indicate the factors acceptable consistence. The MSV and ASV were below AVE indicating acceptable adequacy of the model. The partial reliability index was show in Table 3.
The Figure 2 show the correlations between factors and global score of the FMR instrument. Considering the standardized scores were strongly correlated with the direct score, it was considered the direct score for the further analysis.
3.4. Divergent and Know-Groups Analysis
Divergent analysis. The factor 1 (information) was negatively correlated with PANAS negative affect (Rho=-0.23; P=0.003) and the MBS-social dimension (Rho=-0.18; P=0.019) and positively with PANAS positive affect (Rho=0.23; P=0.003) and resilience (Rho=0.18; P=0.025). The factor 2 (privacy) was positively correlated with resilience (Rho=0.21; P=0.008) and factor 5 (participation) and FMR total score were positively correlated with PANAS positive affect (Rho=0.22; P=0.005 and Rho=0.20; P=0.010, respectively) and resilience (Rho=0.27; P<0.001 and Rho=0.21; P=0.010, respectively). The factor 3 (consent) and 4 (support) was not significantly shown correlation.
Know-groups analysis. The type of labor and complications during labor did not show statistical significance in the factor scores. However, the score in factor 1 (information) was significantly lower in women with non-intended pregnancy than in those with an intended pregnancy. The scores on factor 4 (support), factor 5 (participation) and the overall FMR were significantly lower in women who had postpartum complications compared to women who did not develop these complications (Table 4). In addition, the score of factor 1 was positively correlated with women age (Rho=0.16; P=0.027), gravida (Rho=0.15; P=0.034) and number of labors (Rho=0.20; P=0.005). Furthermore, the score of factor 5 (Rho=0.17; P=0.022) and FMR (Rho=0.15; P=0.044) were also positively and significantly correlated with number of labor.
The final version of the FMR instrument, ordered by factor and stage of maternity, was show in the Appendix A.
4. Discussion
Multiple international conventions protect women against mistreatment during maternity healthcare services [4]. However, to suffer abuse during maternity care is still a globally emerging issue. The FMR instrument is suitability to measure women’s perceptions of the maternity process encompassing pregnancy, childbirth, and immediate postpartum period. The FMR measures the rights of adequate health information, privacy and confidentiality, autonomy, and participation, and social support. Previous data showed the relevance to integrate measures in an instrument of fulfillment healthcare in maternity rights and during different maternal periods [3,12]. The FMR instrument is consistent and has appropriate psychometric properties having been evaluated in a specific sociocultural and health context.
In most cases, the women had stable emotional support, being the last pregnancy intentioned. The gestational age exceeded 37 completed weeks and, overall, the pregnancy, labor or postpartum adverse outcomes did not exceed 35%. Additionally, it was balanced between nulliparous and multiparous women, university education, employment status and type of last delivery (vaginal vs C-section). It is important to consider these characteristics since the perception of the fulfillment of rights may be influenced by the social context [8]. It would be interesting to validate this FMR instrument in other contexts to be able to compare scores.
For the psychometry evaluation, the EFA reveled items that should be excluded from the original proposed as they may jeopardize the construct validity of the instrument. These items showed a low factor loading, indicating that none of them were associated with latent variable [28]. In addition, the complexity represents the number of latent variables needed to account for the observed items. Items with complexity values close to 2 imply that their variance may be distributed in 2 or more factors [29]. These items were excluded to avoid that several dimensions were explained simultaneously for the same item. For example, the original item I8 (“You had sufficient and clear information about the medical procedures performed during childbirth”) was excluded because item I2 (“You had sufficient and clear information about the healthcare procedures that you and your newborn should have for an effective delivery/C-section”) already covered the latent variable. Thus, the final FMR instrument was designed by 29 items covering the dimensions of the respectful maternity care charter [13], the right to be informed and request consent, and respect their choices during maternity care; the right to privacy and confidentiality; the right to request social support necessary during the maternity. All items followed a women-centered proposal.
According to the CFA fit indices, the absolute indices (aGFI) and relative index (NFI) did not pass the cut-off. However, other relative indices (CFI and TLI) show that the 5-factors model was acceptable [30]. In general, the FMR instrument presented a good reliability. All the factors had positive and significant correlations between them. Validation showed that both direct factor and standardized scores can be used. However, we recommend using the direct scores, as they have been the most thoroughly validated in this article.
Moreover, the FMR scores correlated with critical psychological variables during maternity. In Chinese women was demonstrated that the positive affect had a positive correlation with maternal role adaptation, having the opposite trend with the negative affect [31]. Furthermore, the fatigue of the women after labor was negatively associated with her positive affect [32]. Additionally, the resilience during pregnancy can be modulated the association between trait anger in gestation and postnatal depression [33]. According to our data, the resilience and positive affect correlated positively with better perceived fulfillment of rights, but particularly with the right of information, privacy, and participation in maternity healthcare decision. It must be considered that motherhood changes the social role of women. This change of the role can alter life experiences and the perception of an environment that demands more than it offers [34]. Thus, it would be useful to evaluate what feels of the women have about the experience of maternity as a criterion to be met by society. Besides, for maternal adaptation to society, the information and active role of women in care process are relevant factors [10,25,35]. Our data support that the perception of the fulfillment of the right to adequate information increased when the negative affect or belief in motherhood as a social duty were low. Conceding the bidirectional association between better women mental health and better social relationships [36], it is important to promote real and optimal social support during all stages of maternity.
As mentioned above, the analysis of the social context in the rights fulfillment should be central. The observational data showed that expectations and experiences of childbirth vary by maternal age [37]. The FMR instrument support that older women and with previous pregnancies were who expressed greater compliance with information rights. Women around 30s has shown an increase in life satisfaction from pregnancy to postpartum [38], depending the stability based on sociocultural context [39]. Women of advanced maternal age (<35 years) have a higher perception of pregnancy risk than younger, regardless of their medical risk [40]. It seems that to have first newborn older has psychological advantages over younger counterparts, reporting lower symptoms of depression and anxiety during pregnancy [41]. This implies that life experiences are key in the assessment of perceptions. Similarly, having had previous pregnancies and labors made the higher perception of information rights compliance, participation in medical decision making, and overall FMR.
It was demonstrated that the feel of the women related to an inadequate healthcare provision during pregnancy, childbirth, and postpartum was the source of their problems [42]. Many of the women have reported that they had not been taken seriously by health care providers, and some felt seriously neglected [42]. In Italian nulliparous women was revealed that the more fear of childbirth, the worse their maternity´s experience, with no significant effect on C-section [43]. In other observational study was reported that the abuse in healthcare was associated with fear of childbirth (aOR=2.25 in nulliparous and aOR=4.04 in multiparous women) [5]. Therefore, special attention should be paid to the postpartum period since hormonal adjustment and adaptation to the role of motherhood in society can be decisive in the perception of rights violations. In line with our data, the women with lower scores on fulfillment of support rights, participation and overall FMR were those with postpartum complication. This shows that FMR scores are linked to the woman’s postpartum unpleasant experiences. It is important to reflect that the women continue consider the childbirth and postpartum are decisive situations to perceive motherhood as a process in which their rights may be vulnerated.
Another important aspect is the intentionality of the pregnancy. When the pregnancy is unplanned, it may demand major adjustments that exceed the woman’s coping [44]. Thus, the FMR instrument is also sensitive to this aspect. Perceived compliance with the right to adequate health information was lower among women who had an unintended pregnancy. Further research would be necessary to determine the counseling policies and supportive care for women experiencing an unplanned pregnancy.
This psychometric study is an important advance that contributes to the research and monitoring of good practices in maternity care. It also responds to the WHO’s to call for attention to the mistreatment of women during childbirth, and the promoting the improvement of maternal services. The psychometric analysis was rigorous, but the FMR was validated in a Spanish sociocultural context. It would be necessary to know the health background of woman to interpretate the outcomes. It highlights the need to prioritize respectful, woman-centered care during pregnancy, childbirth and postpartum. The findings underscore the importance of ensuring access to clear and adequate information, as well as respect for women’s privacy and autonomy at all stages of maternal care. The current data also highlight the importance of providing adequate social support to women during this critical period. These findings support the need for health policies and clinical practices that promote respectful, informed maternity care focused on women’s individual needs.
5. Conclusions
The fulfillment in maternity rights instrument has exhibited strong psychometric properties for assessing maternal perception on healthcare rights. The instrument assesses dimensions such as adequate health information, right to privacy and confidentiality of medical data, right of autonomy, and participation in yourself healthcare decision, and social support during the maternity process. Cultural and health context is needed to clarify the complexity of the scores. Health institutions can use this instrument to assess and adapt maternity protocols for women users perceive that all their human rights are covered, moving towards more and more humanized models.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: The corplot by Spearman´s rho coefficient of the original items of FMR instrument; Table S1: The original items of fulfillment in maternity rights instrument and exclusion criteria by exploratory factor analysis and principal component analysis; Table S2: Factor loading and complexity of the original of FMR instrument; Table S3: Standardized factor loading, communality and uniqueness extracted from rotated matrix of the final version of FMR instrument.
Author Contributions
Conceptualization, E.G. and D.R.-C.; methodology, C.S.S.-F. and D.R.-C.; software, D.R.-C..; validation, E.G., and D.R.-C.; formal analysis, C.S.S.-F. and D.R.-C.; investigation, C.S.S.-F., M.d.l.C., P.A.C. and S.M.A.; resources, C.S.S.-F.; data curation, C.S.S.-F. and D.R.-C.; writing—original draft preparation, C.S.S.-F., M.d.l.C., P.A.C. and S.M.A.; writing—review and editing, E.G. and D.R.-C.; visualization, D.R.-C.; supervision, E.G. and D.R.-C.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The APC was funded by D.R.-C.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of Universidad Autónoma de Madrid (protocol code CEI-112-2199 on January 22, 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data of this study are available upon request from the corresponding author. The availability of the data is restricted to investigators based in academic institutions.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
The Fulfillment in maternity rights scale (FMR).
Instructions. The following describes your perception related to maternity rights in health services. Following the response scale, mark with an "X" how often did you perceive that the following situations occurred about the healthcare process during your last pregnancy, labor and immediate postpartum (up to 40 days after labor).
0 = Never / 1 = Sometimes / 2 = Half of the time / 3 = Often / 4 = Always
| Item | Factor | During last pregnancy | 0 | 1 | 2 | 3 | 4 |
| I1 | 1 | You had sufficient and clear information about the healthcare procedures that you and your newborn should have for a healthy pregnancy. | |||||
| I4 | 1 | You had sufficient and clear information about the administrative steps you had to take to ensure your healthcare. | |||||
| I7 | 1 | You had sufficient and clear information about the medical procedures performed on you. | |||||
| I42 | 2 | Your privacy or avoidance of exposure of your body (covering intimate parts, regulating the exhibition of your body to persons not involved in the treatment) was respected during healthcare. | |||||
| I45 | 2 | Confidentiality of information about your health was maintained during healthcare. | |||||
| I15 | 3 | Your written consent was requested for healthcare procedures involving the invasion of your body (vaginal examinations or ultrasound). | |||||
| I27 | 4 | If you requested family support or accompaniment during healthcare, they were allowed access. If you never requested it, check option "4". | |||||
| I35 | 5 | During the healthcare, your feelings, emotions, doubts, and opinions were listened. | |||||
| Item | Factor | During last labor | 0 | 1 | 2 | 3 | 4 |
| I2 | 1 | You had sufficient and clear information about the healthcare procedures that you and your newborn should have for an effective delivery/C-section. | |||||
| I5 | 1 | You had sufficient and clear information about the administrative steps you had to take to ensure your healthcare. | |||||
| I46 | 2 | Confidentiality of information about your and your newborn’s health status was maintained during healthcare. | |||||
| I50 | 2 | If your rights were violated during healthcare, you consider that you defended them. If your rights were not violated, answer option "4". | |||||
| I13 | 3 | You were asked for your verbal consent for healthcare processes that involved the invasion of your body (perineal cutting or ultrasounds). | |||||
| I16 | 3 | You were asked for your written consent for healthcare processes involving invasion of your body (perineal cutting or ultrasound). | |||||
| I28 | 4 | If you requested family support or accompaniment during healthcare, they were allowed access. If you never requested it, check option "4". | |||||
| I22 | 5 | They respected your decisions on self-care and newborn care behaviors that were not risky for either of you. | |||||
| I31 | 5 | Health professionals performed or allowed to you to perform pain control (medication, application of compresses, walking, postural control). | |||||
| I36 | 5 | During healthcare, they listened to your feelings, emotions, doubts, and opinions. | |||||
| Item | Factor | During last immediate postpartum (up to 40 days after labor) | 0 | 1 | 2 | 3 | 4 |
| I3 | 1 | You had sufficient and clear information about the healthcare procedures that you and your newborn should have for a healthy postpartum period. | |||||
| I6 | 1 | You had sufficient and clear information about the administrative steps you had to take to ensure your healthcare. | |||||
| I9 | 1 | You had sufficient and clear information about the medical procedures that were performed on you. | |||||
| I11 | 1 | You had sufficient and clear information to initiate and maintain breastfeeding in a correct and painless way. | |||||
| I47 | 2 | Confidentiality of information about your and your newborn’s health status was maintained during healthcare. | |||||
| I49 | 2 | You consider that some of the healthcare practices you received may have been both uncomfortable and unnecessary (application of bandages, among others). | |||||
| I17 | 3 | You were asked for your written consent for healthcare procedures that involved invasion of your body (dressings, tubal ligation, or ultrasound). | |||||
| I29 | 4 | In the case of having requested family support or accompaniment during healthcare, they were you allowed access. If you never requested it, check option "4". | |||||
| I23 | 5 | They respected your decisions on self-care and newborn care behaviors that were not risky for either of you (type of contraception, type of breastfeeding, among others). | |||||
| I32 | 5 | Health professionals performed or allowed to you to perform actions to control pain (medication, application of compresses, etc.). | |||||
| I37 | 5 | During healthcare, they listened to your feelings, emotions, doubts, and opinions. | |||||
| Factor 1 gathers items related to receive adequate healthcare information (Factor 1=Information), factor 2 gathers rights related to privacy and confidentiality of health information (Factor 2=Privacy), factor 3 refers to consent to medical procedures (Factor 3=Consent), factor 4 refers to social support during maternity (Factor 4=Support) and factor 5 to participation and active listening in medical treatment (Factor 5=Participation). | |||||||
References
- Bohren, M.A.; Vogel, J.P.; Hunter, E.C.; Lutsiv, O.; Makh, S.K.; Souza, J.P.; Aguiar, C.; Saraiva Coneglian, F.; Diniz, A.L.A.; Tunçalp, Ö.; et al. The Mistreatment of Women during Childbirth in Health Facilities Globally: A Mixed-Methods Systematic Review. PLoS Med 2015, 12, e1001847. [Google Scholar] [CrossRef]
- Schroll, A.-M.; Kjærgaard, H.; Midtgaard, J. Encountering Abuse in Health Care; Lifetime Experiences in Postnatal Women - a Qualitative Study. BMC Pregnancy Childbirth 2013, 13, 74. [Google Scholar] [CrossRef]
- Silva-Fernandez, C.S.; de la Calle, M.; Arribas, S.M.; Garrosa, E.; Ramiro-Cortijo, D. Factors Associated with Obstetric Violence Implicated in the Development of Postpartum Depression and Post-Traumatic Stress Disorder: A Systematic Review. Nurs Rep 2023, 13, 1553–1576. [Google Scholar] [CrossRef]
- Baumont, M.S.; Dekker, C.S.; Rabinovitch Blecker, N.; Turlington Burns, C.; Strauss, N.E. Every Mother Counts: Listening to Mothers to Transform Maternity Care. Am J Obstet Gynecol 2023, 228, S954–S964. [Google Scholar] [CrossRef]
- Lukasse, M.; Schroll, A.; Karro, H.; Schei, B.; Steingrimsdottir, T.; Van Parys, A.; Ryding, E.L.; Tabor, A. Prevalence of Experienced Abuse in Healthcare and Associated Obstetric Characteristics in Six European Countries. Acta Obstet Gynecol Scand 2015, 94, 508–517. [Google Scholar] [CrossRef]
- Bohren, M.A.; Mehrtash, H.; Fawole, B.; Maung, T.M.; Balde, M.D.; Maya, E.; Thwin, S.S.; Aderoba, A.K.; Vogel, J.P.; Irinyenikan, T.A.; et al. How Women Are Treated during Facility-Based Childbirth in Four Countries: A Cross-Sectional Study with Labour Observations and Community-Based Surveys. The Lancet 2019, 394, 1750–1763. [Google Scholar] [CrossRef]
- Brüggemann, A.J.; Wijma, B.; Swahnberg, K. Abuse in Health Care: A Concept Analysis. Scand J Caring Sci 2012, 26, 123–132. [Google Scholar] [CrossRef]
- Afulani, P.A.; Sayi, T.S.; Montagu, D. Predictors of Person-Centered Maternity Care: The Role of Socioeconomic Status, Empowerment, and Facility Type. BMC Health Serv Res 2018, 18, 360. [Google Scholar] [CrossRef]
- Salter, C.; Wint, K.; Burke, J.; Chang, J.C.; Documet, P.; Kaselitz, E.; Mendez, D. Overlap between Birth Trauma and Mistreatment: A Qualitative Analysis Exploring American Clinician Perspectives on Patient Birth Experiences. Reprod Health 2023, 20, 63. [Google Scholar] [CrossRef]
- Martínez-Mollá, T.M.; Siles, J.; Solano, M. del C. Evitar La Violencia Obstétrica: Motivo Para Decidir El Parto En Casa. MUSAS 2019, 4. [Google Scholar] [CrossRef]
- Bohren, M.A.; Hunter, E.C.; Munthe-Kaas, H.M.; Souza, J.P.; Vogel, J.P.; Gülmezoglu, A.M. Facilitators and Barriers to Facility-Based Delivery in Low- and Middle-Income Countries: A Qualitative Evidence Synthesis. Reprod Health 2014, 11, 71. [Google Scholar] [CrossRef]
- van Roosmalen, J.; van den Akker, T. Continuous and Caring Support Right Now. BJOG 2016, 123, 675–675. [Google Scholar] [CrossRef]
- White Ribbon Alliance Respectful Maternity Care Charter Assets. Available online: https://whiteribbonalliance.org/resources/rmc-charter/ (accessed on 19 April 2024).
- Fontein-Kuipers, Y.; de Groot, R.; van Staa, A. Woman-Centered Care 2.0: Bringing the Concept into Focus. Eur J Midwifery 2018, 2, 5. [Google Scholar] [CrossRef]
- Alghamdi, R.S.; Perra, O.; Boyle, B.; Stockdale, J. Perceived Treatment of Respectful Maternity Care among Pregnant Women at Healthcare Facilities in the Kingdom of Saudi Arabia: A Cross-Sectional Study. Midwifery 2023, 123, 103714. [Google Scholar] [CrossRef]
- Vedam, S.; Stoll, K.; Rubashkin, N.; Martin, K.; Miller-Vedam, Z.; Hayes-Klein, H.; Jolicoeur, G. The Mothers on Respect (MOR) Index: Measuring Quality, Safety, and Human Rights in Childbirth. SSM Popul Health 2017, 3, 201–210. [Google Scholar] [CrossRef]
- Alfaro Blazquez, R.; Corchon, S.; Ferrer Ferrandiz, E. Validity of Instruments for Measuring the Satisfaction of a Woman and Her Partner with Care Received during Labour and Childbirth: Systematic Review. Midwifery 2017, 55, 103–112. [Google Scholar] [CrossRef]
- World Health Organization (WHO) Human Rights. Available online: https://www.who.int/news-room/fact-sheets/detail/human-rights-and-health (accessed on 19 April 2024).
- Aiken, L.R. Three Coefficients for Analyzing the Reliability and Validity of Ratings. Educ Psychol Meas 1985, 45, 131–142. [Google Scholar] [CrossRef]
- Gila-Díaz, A.; Carrillo, G.H.; López de Pablo, Á.L.; Arribas, S.M.; Ramiro-Cortijo, D. Association between Maternal Postpartum Depression, Stress, Optimism, and Breastfeeding Pattern in the First Six Months. Int J Environ Res Public Health 2020, 17. [Google Scholar] [CrossRef]
- Abiola, T.; Udofia, O. Psychometric Assessment of the Wagnild and Young’s Resilience Scale in Kano, Nigeria. BMC Res Notes 2011, 4, 509. [Google Scholar] [CrossRef]
- Surzykiewicz, J.; Konaszewski, K.; Wagnild, G. Polish Version of the Resilience Scale (RS-14): A Validity and Reliability Study in Three Samples. Front Psychol 2018, 9, 2762. [Google Scholar] [CrossRef]
- Crawford, J.R.; Henry, J.D. The Positive and Negative Affect Schedule (PANAS): Construct Validity, Measurement Properties and Normative Data in a Large Non-Clinical Sample. Br J Clin Psychol 2004, 43, 245–265. [Google Scholar] [CrossRef]
- Sandín, B.; Chorot, P.; Joiner, T.E.; Santed Miguel, A.; Valiente, R.M. Escalas PANAS de Afecto Positivo y Negativo: Validación Factorial y Convergencia Transcultural. Psicothema 1999, 11, 37–51. [Google Scholar]
- González, C.; Calleja, N.; Bravo, C.; Meléndez, J. Escala de Creencias Sobre La Maternidad: Construcción y Validación En Mujeres Mexicanas. Revista Iberoamericana de Diagnóstico y Evaluación – e Avaliação Psicológica 2019, 50. [Google Scholar] [CrossRef]
- Amado-Mateus, M.; Cuero-Acosta, Y.A.; Guzman-Rincón, A. Evaluation of Psychometric Properties of Perceived Value Applied to Universities. PLoS One 2023, 18, e0284351. [Google Scholar] [CrossRef]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.W.; et al. STARD 2015 Guidelines for Reporting Diagnostic Accuracy Studies: Explanation and Elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]
- Tavakol, M.; Wetzel, A. Factor Analysis: A Means for Theory and Instrument Development in Support of Construct Validity. Int J Med Educ 2020, 11, 245–247. [Google Scholar] [CrossRef]
- Pettersson, E.; Turkheimer, E. Item Selection, Evaluation, and Simple Structure in Personality Data. J Res Pers 2010, 44, 407–420. [Google Scholar] [CrossRef]
- Kyndt, E.; Onghena, P. The Integration of Work and Learning: Tackling the Complexity with Structural Equation Modelling. In; 2014; pp. 255–291.
- He, S.; Yang, F.; Zhang, H.; Zhang, S. Affective Well-Being of Chinese Urban Postpartum Women: Predictive Effect of Spousal Support and Maternal Role Adaptation. Arch Womens Ment Health 2022, 25, 781–788. [Google Scholar] [CrossRef]
- Dokuhaki, S.; Dokuhaki, F.; Akbarzadeh, M. The Relationship of Maternal Anxiety, Positive and Negative Affect Schedule, and Fatigue with Neonatal Psychological Health upon Childbirth. Contracept Reprod Med 2021, 6, 12. [Google Scholar] [CrossRef]
- Tobe, H.; Kita, S.; Hayashi, M.; Umeshita, K.; Kamibeppu, K. Mediating Effect of Resilience during Pregnancy on the Association between Maternal Trait Anger and Postnatal Depression. Compr Psychiatry 2020, 102, 152190. [Google Scholar] [CrossRef]
- Arghavanian, F.E.; Roudsari, R.L.; Heydari, A.; Bahmani, M.N.D. Pregnant Women’s Experiences of Social Roles: An Ethnophenomenological Study. Iran J Nurs Midwifery Res 2020, 25, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Barcelar, L.; Jonas, E.; Rute, L. Obstetric Violence in Public Maternity Wards of the State of Tocantins. Revista de Estudios Feministas 2018, 26, e43278. [Google Scholar]
- Davis, E.P.; Narayan, A.J. Pregnancy as a Period of Risk, Adaptation, and Resilience for Mothers and Infants. Dev Psychopathol 2020, 32, 1625–1639. [Google Scholar] [CrossRef]
- Zasloff, E.; Schytt, E.; Waldenstrom, U. First Time Mothers’ Pregnancy and Birth Experiences Varying by Age. Acta Obstet Gynecol Scand 2007, 86, 1328–1336. [Google Scholar] [CrossRef] [PubMed]
- Aasheim, V.; Waldenström, U.; Rasmussen, S.; Espehaug, B.; Schytt, E. Satisfaction with Life during Pregnancy and Early Motherhood in First-Time Mothers of Advanced Age: A Population-Based Longitudinal Study. BMC Pregnancy Childbirth 2014, 14, 86. [Google Scholar] [CrossRef] [PubMed]
- Quick, A.D.; Tung, I.; Keenan, K.; Hipwell, A.E. Psychological Well-Being across the Perinatal Period: Life Satisfaction and Flourishing in a Longitudinal Study of Black and White American Women. J Happiness Stud 2023, 24, 1283–1301. [Google Scholar] [CrossRef]
- Bayrampour, H.; Heaman, M.; Duncan, K.A.; Tough, S. Comparison of Perception of Pregnancy Risk of Nulliparous Women of Advanced Maternal Age and Younger Age. J Midwifery Womens Health 2012, 57, 445–453. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.A.; Boivin, J.; Gibson, F.L.; Hammarberg, K.; Wynter, K.; Saunders, D.; Fisher, J. Age at First Birth, Mode of Conception and Psychological Wellbeing in Pregnancy: Findings from the Parental Age and Transition to Parenthood Australia (PATPA) Study. Human Reproduction 2011, 26, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Semasaka, J.P.S.; Krantz, G.; Nzayirambaho, M.; Munyanshongore, C.; Edvardsson, K.; Mogren, I. “Not Taken Seriously”-A Qualitative Interview Study of Postpartum Rwandan Women Who Have Experienced Pregnancy-Related Complications. PLoS One 2019, 14, e0212001. [Google Scholar] [CrossRef]
- Fenaroli, V.; Molgora, S.; Dodaro, S.; Svelato, A.; Gesi, L.; Molidoro, G.; Saita, E.; Ragusa, A. The Childbirth Experience: Obstetric and Psychological Predictors in Italian Primiparous Women. BMC Pregnancy Childbirth 2019, 19, 419. [Google Scholar] [CrossRef]
- Mohammadi, E.; Nourizadeh, R.; Simbar, M.; Rohana, N. Iranian Women’s Experiences of Dealing with the Complexities of an Unplanned Pregnancy: A Qualitative Study. Midwifery 2018, 62, 81–85. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The confirmatory factor analysis model. The value shown the standardized estimates variance of each factor and global fulfillment in maternity rights (FMR) global score.
Figure 1.
The confirmatory factor analysis model. The value shown the standardized estimates variance of each factor and global fulfillment in maternity rights (FMR) global score.
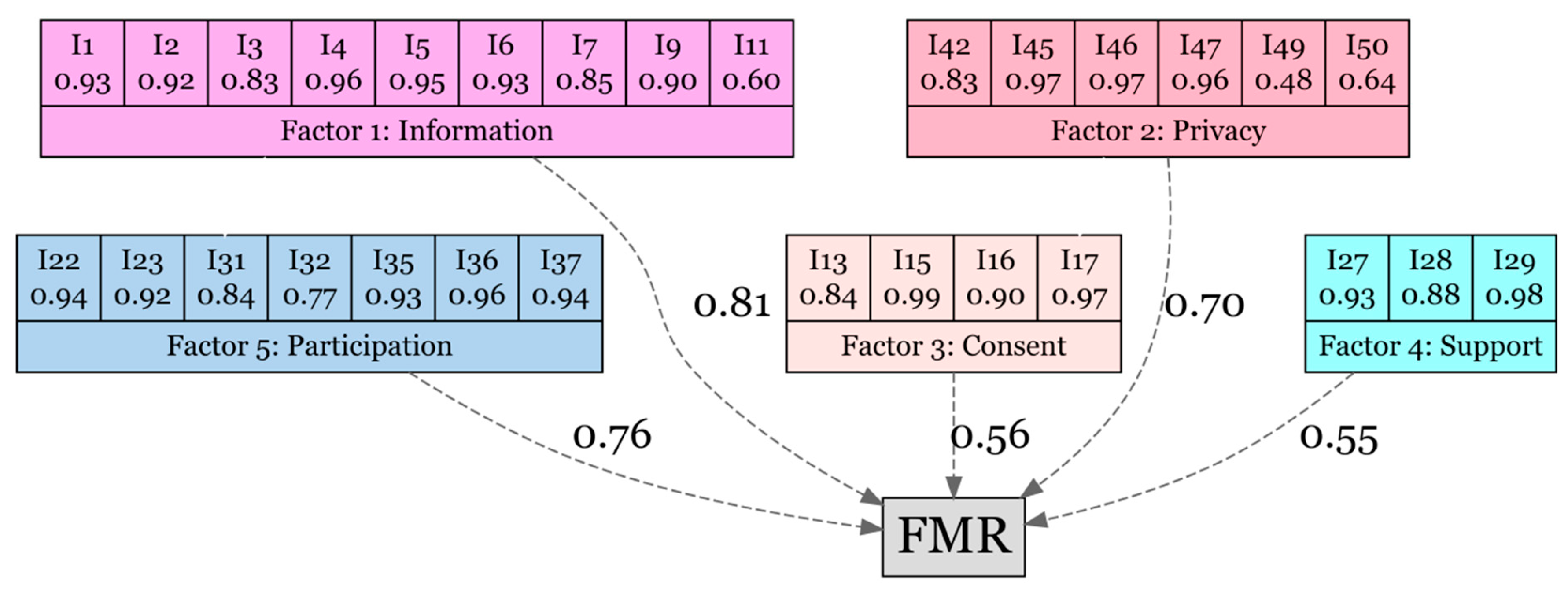
Figure 2.
The Spearman´s Rho coefficient matrix between factors and global direct and standardized score of the fulfillment in maternity rights (FMR) instrument. Standardized (std), Factor 1=Information, Factor 2=Privacy, Factor 3=Consent, Factor 4=Support, Factor 5=Participation.
Figure 2.
The Spearman´s Rho coefficient matrix between factors and global direct and standardized score of the fulfillment in maternity rights (FMR) instrument. Standardized (std), Factor 1=Information, Factor 2=Privacy, Factor 3=Consent, Factor 4=Support, Factor 5=Participation.
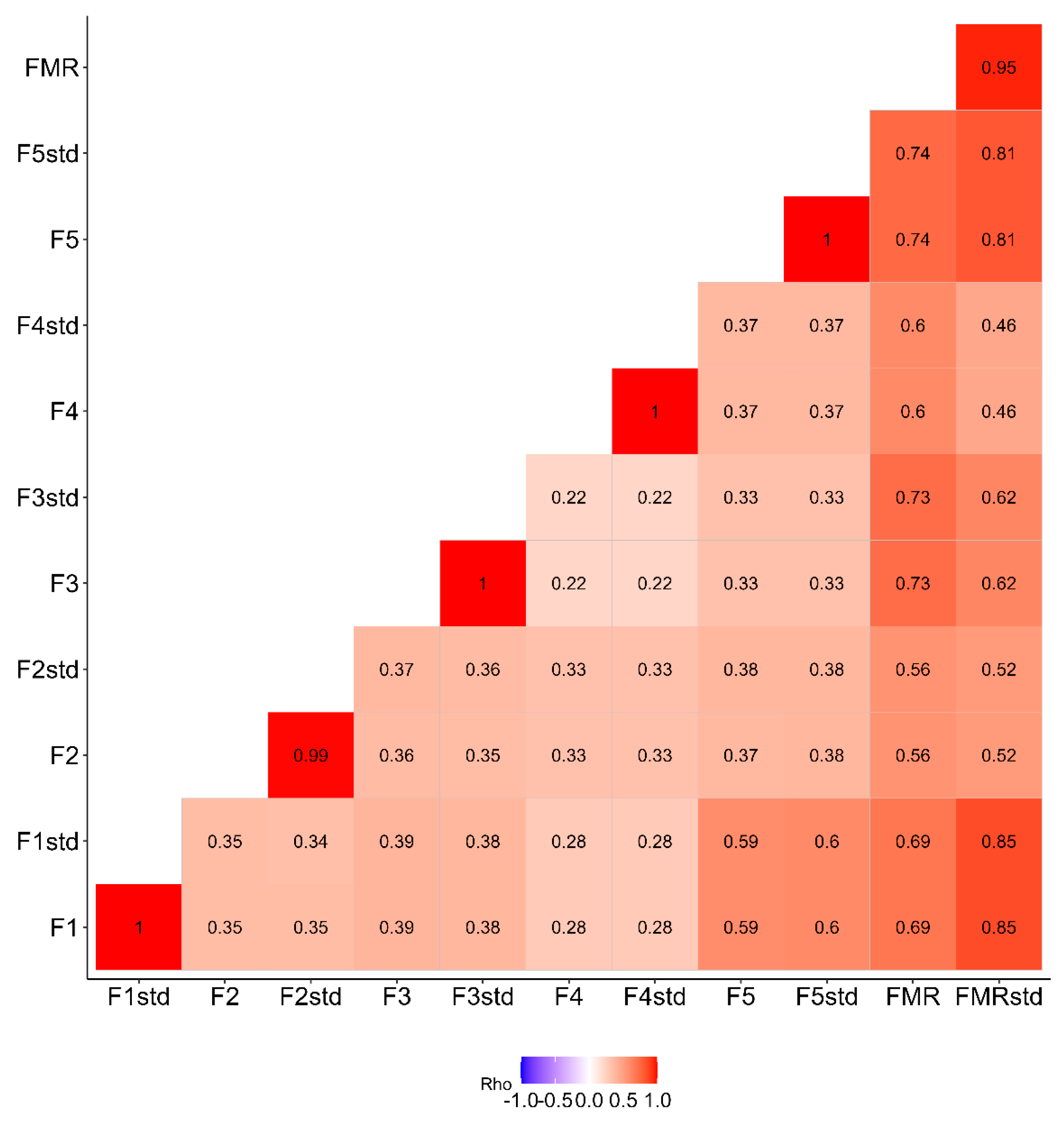

Table 1.
Descriptive analysis of final items included in the FMR instrument.
| Item | Mean | SD | SEM | Median | Q1 | Q3 | Range | Skew | Kurtosis |
|---|---|---|---|---|---|---|---|---|---|
| I1 | 3.19 | 1.28 | 0.09 | 4.00 | 3.00 | 4.00 | 4 | -1.37 | 0.42 |
| I2 | 2.96 | 1.41 | 0.10 | 4.00 | 2.00 | 4.00 | 4 | -1.05 | -0.40 |
| I3 | 2.90 | 1.38 | 0.10 | 4.00 | 2.00 | 4.00 | 4 | -0.90 | -0.66 |
| I4 | 2.91 | 1.42 | 0.10 | 4.00 | 2.00 | 4.00 | 4 | -1.01 | -0.46 |
| I5 | 2.81 | 1.46 | 0.11 | 3.00 | 2.00 | 4.00 | 4 | -0.87 | -0.76 |
| I6 | 2.72 | 1.47 | 0.11 | 3.00 | 1.00 | 4.00 | 4 | -0.74 | -0.97 |
| I7 | 3.23 | 1.28 | 0.09 | 4.00 | 3.00 | 4.00 | 4 | -1.50 | 0.78 |
| I9 | 3.06 | 1.37 | 0.10 | 4.00 | 3.00 | 4.00 | 4 | -1.21 | -0.03 |
| I11 | 2.97 | 1.42 | 0.10 | 4.00 | 2.00 | 4.00 | 4 | -1.05 | -0.44 |
| I13 | 3.03 | 1.41 | 0.10 | 4.00 | 2.00 | 4.00 | 4 | -1.12 | -0.27 |
| I15 | 2.57 | 1.69 | 0.12 | 4.00 | 1.00 | 4.00 | 4 | -0.58 | -1.43 |
| I16 | 2.63 | 1.67 | 0.12 | 4.00 | 1.00 | 4.00 | 4 | -0.63 | -1.37 |
| I17 | 2.48 | 1.74 | 0.13 | 3.00 | 0.00 | 4.00 | 4 | -0.50 | -1.55 |
| I22 | 3.48 | 1.04 | 0.08 | 4.00 | 3.00 | 4.00 | 4 | -2.02 | 3.05 |
| I23 | 3.48 | 1.01 | 0.07 | 4.00 | 3.00 | 4.00 | 4 | -2.02 | 3.19 |
| I27 | 3.06 | 1.48 | 0.11 | 4.00 | 2.00 | 4.00 | 4 | -1.15 | -0.37 |
| I28 | 3.08 | 1.51 | 0.11 | 4.00 | 3.00 | 4.00 | 4 | -1.23 | -0.25 |
| I29 | 3.27 | 1.31 | 0.10 | 4.00 | 3.00 | 4.00 | 4 | -1.51 | 0.71 |
| I31 | 3.01 | 1.45 | 0.11 | 4.00 | 2.00 | 4.00 | 4 | -1.10 | -0.40 |
| I32 | 3.11 | 1.39 | 0.10 | 4.00 | 3.00 | 4.00 | 4 | -1.28 | 0.09 |
| I35 | 2.95 | 1.38 | 0.10 | 4.00 | 2.00 | 4.00 | 4 | -1.04 | -0.37 |
| I36 | 2.75 | 1.49 | 0.11 | 3.00 | 1.00 | 4.00 | 4 | -0.78 | -0.95 |
| I37 | 2.78 | 1.49 | 0.11 | 3.00 | 2.00 | 4.00 | 4 | -0.84 | -0.85 |
| I42 | 3.58 | 1.00 | 0.07 | 4.00 | 4.00 | 4.00 | 4 | -2.67 | 6.23 |
| I45 | 3.73 | 0.75 | 0.05 | 4.00 | 4.00 | 4.00 | 4 | -3.35 | 11.57 |
| I46 | 3.66 | 0.88 | 0.06 | 4.00 | 4.00 | 4.00 | 4 | -3.03 | 8.71 |
| I47 | 3.68 | 0.83 | 0.06 | 4.00 | 4.00 | 4.00 | 4 | -3.12 | 9.77 |
| I49 | 3.66 | 0.92 | 0.07 | 4.00 | 4.00 | 4.00 | 4 | -3.02 | 8.52 |
| I50 | 3.63 | 0.99 | 0.07 | 4.00 | 4.00 | 4.00 | 4 | -2.72 | 6.30 |
Standard deviation (SD); Standard error of mean (SEM); Quartile (Q).
Table 2.
Descriptive analysis of the factor and global scores (direct and standardized) of the FMR instrument.
Table 2.
Descriptive analysis of the factor and global scores (direct and standardized) of the FMR instrument.
| Mean | SD | SEM | Median | Q1 | Q3 | Range | Skew | Kurtosis | |
|---|---|---|---|---|---|---|---|---|---|
| Factor 1 | 2.97 | 1.09 | 0.08 | 3.22 | 2.56 | 3.89 | 4.00 | -1.12 | 0.30 |
| Factor 2 | 3.66 | 0.66 | 0.05 | 4.00 | 3.50 | 4.00 | 4.00 | -3.26 | 12.22 |
| Factor 3 | 2.68 | 1.41 | 0.10 | 3.00 | 1.00 | 4.00 | 4.00 | -0.57 | -1.23 |
| Factor 4 | 3.14 | 1.28 | 0.09 | 4.00 | 2.33 | 4.00 | 4.00 | -1.24 | 0.16 |
| Factor 5 | 3.08 | 0.96 | 0.07 | 3.43 | 2.43 | 4.00 | 4.00 | -0.98 | 0.30 |
| FMR | 15.53 | 3.86 | 0.28 | 16.48 | 13.52 | 18.55 | 17.67 | -1.13 | 0.82 |
| Factor 1 std | 23.37 | 8.71 | 0.64 | 25.96 | 20.12 | 30.88 | 31.48 | -1.11 | 0.23 |
| Factor 2 std | 17.76 | 3.33 | 0.24 | 19.40 | 17.48 | 19.40 | 19.40 | -3.28 | 11.91 |
| Factor 3 std | 9.86 | 5.27 | 0.39 | 11.32 | 3.83 | 14.80 | 14.80 | -0.56 | -1.26 |
| Factor 4 std | 8.76 | 3.57 | 0.26 | 11.16 | 6.61 | 11.16 | 11.16 | -1.25 | 0.18 |
| Factor 5 std | 19.34 | 6.06 | 0.45 | 21.52 | 14.76 | 25.12 | 25.12 | -0.97 | 0.28 |
| FMR std | 56.40 | 14.41 | 1.06 | 61.37 | 49.18 | 66.39 | 63.53 | -1.19 | 0.79 |
Standardized (std); Standard deviation (SD); Standard error of mean (SEM); Quartile (Q). Factor 1=Information, Factor 2=Privacy, Factor 3=Consent, Factor 4=Support, Factor 5=Participation.
Table 3.
Internal consistence of factors and FMR instrument.
| Factor 1. Information | Factor 2. Privacy | Factor 3. Consent | Factor 4. Support | Factor 5. Participation | FMR | |
|---|---|---|---|---|---|---|
| AVE | 0.78 | 0.69 | 0.86 | 0.87 | 0.81 | 0.79 |
| MSV | 0.41 | 0.17 | 0.12 | 0.12 | 0.41 | - |
| ASV | 0.57 | 0.50 | 0.72 | 0.70 | 0.49 | - |
| Omega | 0.95 | 0.86 | 0.94 | 0.90 | 0.94 | 0.97 |
| Alpha | 0.95 | 0.90 | 0.93 | 0.95 | 0.90 | 0.93 |
Average Variance Extracted (AVE); maximum shared variance (MSV); average shared variance (ASV); omega (ω) reliability; Cronbach’s alpha (α).
Table 4.
External validation by known groups of factors and global score of the FRM instrument.
|
Non-intended pregnancy |
Intended pregnancy |
P | Vaginal | C-section | P | |
| Factor 1 | 2.89 [1.56; 3.33] | 3.33 [2.64; 4.00] | 0.048 | 3.33 [2.67; 3.89] | 3.11 [2.44; 3.89] | 0.350 |
| Factor 2 | 3.83 [3.33; 4.00] | 4.00 [3.67; 4.00] | 0.117 | 3.83 [3.50; 4.00] | 4.00 [3.67; 4.00] | 0.113 |
| Factor 3 | 3.00 [1.75; 4.00] | 3.25 [1.00; 4.00] | 0.523 | 3.00 [1.00; 4.00] | 3.00 [2.00; 4.00] | 0.395 |
| Factor 4 | 4.00 [3.00; 4.00] | 4.00 [2.58; 4.00] | 0.408 | 3.00 [1.00; 4.00] | 4.00 [2.42; 4.00] | 0.460 |
| Factor 5 | 3.29 [2.14; 3.71] | 3.50 [2.39; 4.00] | 0.250 | 3.43 [2.43; 4.00] | 3.29 [2.29; 4.00] | 0.961 |
| FMR | 16.0 [12.1; 17.2] | 16.7 [13.8; 18.7] | 0.157 | 16.4 [13.1; 18.5] | 16.7 [13.8; 18.6] | 0.682 |
|
Uncomplicated pregnancy |
Complicated pregnancy |
P |
Uncomplicated postpartum |
Complicated postpartum |
P | |
| Factor 1 | 3.33 [2.67; 4.00] | 3.22 [2.25; 3.78] | 0.340 | 3.33 [2.67; 4.00] | 2.89 [2.11; 3.67] | 0.103 |
| Factor 2 | 4.00 [3.50; 4.00] | 4.00 [3.50; 4.00] | 0.654 | 4.00 [3.50; 4.00] | 3.83 [3.50; 4.00] | 0.238 |
| Factor 3 | 3.00 [1.00; 4.00] | 3.12 [2.00; 4.00] | 0.429 | 3.50 [1.25; 4.00] | 2.25 [1.00; 3.75] | 0.084 |
| Factor 4 | 4.00 [2.33; 4.00] | 4.00 [2.42; 4.00] | 0.774 | 4.00 [2.92; 4.00] | 3.00 [2.00; 4.00] | 0.012 |
| Factor 5 | 3.57 [2.43; 4.00] | 3.07 [2.29; 3.71] | 0.078 | 3.57 [2.43; 4.00] | 2.86 [2.14; 3.57] | 0.002 |
| FMR | 16.6 [13.8; 18.7] | 16.4 [13.3; 18.1] | 0.505 | 16.7 [13.9; 18.7] | 14.7 [12.7; 17.1] | 0.005 |
|
Uncomplicated labor |
Complicated labor |
P | ||||
| Factor 1 | 3.22 [2.50; 4.00] | 3.17 [2.67; 3.67] | 0.539 | |||
| Factor 2 | 4.00 [3.50; 4.00] | 4.00 [3.50; 4.00] | 0.739 | |||
| Factor 3 | 3.00 [1.00; 4.00] | 3.12 [1.44; 4.00] | 0.968 | |||
| Factor 4 | 4.00 [2.33; 4.00] | 4.00 [2.25; 4.00] | 0.605 | |||
| Factor 5 | 3.43 [2.43; 4.00] | 3.07 [2.32; 3.71] | 0.495 | |||
| FMR | 16.6 [13.5; 18.6] | 16.4 [14.1; 18.1] | 0.618 |
Data shown median and interquartile range [Q1; Q3]. The P-value (P) was extracted from Mann-Whitney´s U test. Factor 1=Information, Factor 2=Privacy, Factor 3=Consent, Factor 4=Support, Factor 5=Participation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



