
Submitted:
27 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Alzheimer’s disease (AD) is the most common neurodegenerative disease that accounts for 60–80% of all dementia cases and affects millions of people worldwide. At present, standard drug therapies provide only limited symptomatic relief. Therefore, the exploration of novel therapeutic approaches is crucial for improving patient outcomes. Transcranial Magnetic Stimulation (TMS) has emerged as a promising non-invasive neuromodulation technique that may provide benefit in the management of AD. This review discusses the pathophysiological mechanisms by which TMS operates, evaluates its clinical efficacy in AD patients, assesses its safety profile, and suggests future directions for research.
Keywords:
Alzheimer's Disease
; Transcranial Magnetic Stimulation
; neuromodulation
; non-invasive treatment
; cognitive decline
1. Introduction
Alzheimer’s disease (AD) is the most prevalent neurodegenerative disorder and the most common form of dementia, accounting for approximately 60–70% of all dementia cases [1]. It is clinically characterized by progressive cognitive decline that affects memory, executive function, language, and visuospatial abilities, ultimately leading to loss of functional independence. The neuropathological hallmarks of AD are the accumulation of extracellular amyloid plaques that consist of beta-amyloid, and intracellular neurofibrillary tangles composed of hyperphosphorylated tau [2,3,4].
Despite decades of research, therapeutic options for AD remain limited. Current pharmacological treatments, such as acetylcholinesterase inhibitors and NMDA receptor antagonists, offer modest symptomatic relief but don’t substantially alter disease progression [5]. The recent FDA and EMA approval of the amyloid-targeting disease-modifying therapies donanemab and lecanemab, have shown until now limited and often controversial clinical efficacy, highlighting the urgent need for alternative therapeutic approaches that address the complex pathophysiology of AD [6,7].
A growing amount of evidence suggests that AD might be viewed as a disconnection syndrome marked by disrupted synaptic plasticity, impaired excitation–inhibition balance, and large-scale network disruption, particularly within the default mode network (DMN) and hippocampal–prefrontal circuits [8,9,10]. The DMN is a network of interconnected brain regions (hubs) in the medial prefrontal cortex, posterior cingulate cortex or precuneus, and bilateral inferior parietal cortices, as well as supplementary brain regions such as the medial temporal lobes and temporal poles. This network dysfunction precedes structural brain changes and clinical symptoms and is closely associated with cognitive impairment observed in AD [11].
Transcranial magnetic stimulation (TMS) is a non-invasive brain stimulation technique that is capable of directly modulating cortical excitability and inducing long-lasting plastic changes in targeted neural circuits. By generating transient magnetic fields that induce focal electric currents in the cortical tissue, TMS alters brain activity by impacting neuronal firing, synaptic efficacy, and increasing brain network connectivity [12,13]. In particular, repetitive TMS (rTMS), has been shown to induce long-term potentiation (LTP)- or long-term depression (LTD)-like effects and alter network connectivity, likely through modulation of complex mechanisms involving calcium-dependent processes and glutamate receptors. [14].
TMS has received FDA clearance for several neuropsychiatric disorders such as major depression and migraine and is widely investigated in neurodegenerative diseases [15]. rTMS offers several advantages in the case of AD treatment i.e. it directly targets disrupted neural circuits, engages activity-dependent plasticity mechanisms, modulates inflammatory processes, and might influence beta-amyloid and tau protein cascades through network-driven clearance mechanisms and metabolic regulation [16,17,18].
Over the last twenty years, an increasing number of clinical studies have evaluated the use of rTMS as a therapeutic approach in AD, using various stimulation protocols, target regions, and outcome measures. The most common stimulation site for rTMS is the dorsolateral prefrontal cortex (DLPFC); however recent studies have adopted multisite, DMN-based, and personalized targeting strategies, including stimulation of posterior cortical hubs such as the precuneus [19,20,21,22].
Moreover, preclinical and translational studies have started to elucidate the molecular and cellular mechanisms underlying TMS-induced effects in AD animal models. These involve modulation of synaptic plasticity pathways, regulation of neuroinflammatory responses mediated by microglia and astrocytes, enhancement of neurotrophic signaling, and improvements in neurovascular coupling and metabolic function [23,24,25].
The aim of the current literature review is to provide a comprehensive overview of the role of TMS as potential AD treatment, highlighting the molecular and cellular mechanisms and preclinical and clinical studies. Future directions and challenges are proposed for TMS to be widely used in routine clinical practice.
2. Principles of Transcranial Magnetic Stimulation
2.1. Biophysical Basis of TMS
TMS is based on the Faraday’s law of electromagnetic induction. A rapidly changing current passing through a stimulation coil of wire generates a magnetic field that penetrates the scalp and skull and induces an electric field in the underlying neural and non-neural tissues, leading to depolarization or hyperpolarization of neuronal membranes.
The physiological effects of TMS depend on multiple factors, such as stimulation frequency and intensity, coil geometry, number of pulses, and the functional state of the targeted cortex. Although TMS is applied on a specific site, its effects extend to distant inter-connected brain regions through anatomical and functional connectivity, resulting in modulation of large-scale networks. Therefore, the beneficial effects of TMS may be the result of the stimulation of the targeted cortical area, the propagation to inter-connected regions or the combined effect of both, as a function of white matter connectivity. [27]
2.1.1. Magnetic Field Generation and Induced Currents
A circular or figure-of-eight coil in TMS produces strong, transient magnetic fields, typically 1-2 Tesla, with a pulse width of 80 to 300 microseconds. The shape and size of the TMS coil plays an important role in determining focality and depth of the brain stimulation. The pyramidal neurons in the cortex are more easily excited when the stimulating electric currents, flow in parallel to the axons of the pyramidal neurons, compared with the stimulation by currents which are perpendicular to the axons.[28] The induced current is attenuated as a function of distance by bone, air, tissues, and possible structural alterations of cortex. Layer-5 pyramidal neurons are particularly sensitive due to their exceptionally long apical dendrites that reach all six layers of cortex and are aligned with the induced current [29]
2.1.2. Neuronal Activation Mechanisms
TMS pulses mainly stimulate axonal initial segments and dendritic branches, generating action potentials that propagate in both orthodromic and antidromic directions within cortical networks. This depolarization triggers synaptic release of neurotransmitters and initiates downstream neuroplasticity mechanisms. rTMS modulates cortical excitability through activity-dependent synaptic plasticity; in particular intrinsic plasticity mechanisms that include: a) amplification or attenuation of postsynaptic potentials at the dendrites. B) alterations in the resting membrane potentials and c) increase in the threshold required for the generation of action potentials [30]. rTMS may influence GABA and glutamate levels (the principal inhibitory and excitatory neurotransmitter in the CNS respectively), enhancing GABAergic neuron function and GABA expression. In particular, LF-rTMS (1 Hz), intermittent TBS, and continuous TBS were shown to influence the GABAergic circuitry of the rat cortex [31]
2.1.3. Field Orientation and Cortical Geometry
Cortical folding morphology and orientation influences TMS-induced electric fields. Neurons aligned parallel to the induced electrical field (E-field) are preferentially activated, while those perpendicular may require higher stimulation intensity. Computational modeling of individualized head anatomy and cortical gyrification as assessed with brain MRI, has demonstrated that E-field strength and directionality correlate with clinical responsiveness i.e. when the coil orientation is perpendicular to the direction of the sulcus, a greater E-field strength and penetration depth is produced [32]
2.2. TMS Protocols and Their Neurophysiological Effects
TMS protocols are highly variable and can be tailored to specific therapeutic goals in AD, that range from modulation of cortical excitability to network-level reorganization. Protocols are generally classified according to frequency, intensity, pattern, and target area, each of which influences neurophysiological responses and subsequent clinical outcomes.
2.2.1. Frequency-Dependent Effects
• High-frequency TMS (>5 Hz) typically initiates facilitation effects by increasing cortical excitability and inducing long-term potentiation (LTP)-like effects. In AD patients, high-frequency stimulation of the dorsolateral prefrontal cortex (DLPFC) or precuneus enhances synaptic plasticity, functional connectivity, and cognitive performance, particularly in memory and executive domains [23,24,25,26,27,28,29,30,31,32,33]. rTMS studies in AD patients are almost exclusively performed with high-frequency protocols (>10Hz). In a recent review [34] HF-rTMS was found to improve global cognitive function in patients with mild to moderate AD as assessed with MMSE score, ADAS-Cog and P300 latency.
• Low-frequency TMS (≤1 Hz) generally induces inhibitory effects on motor cortical excitability and is associated with long-term depression (LTD)-like effects. LF rtMS of 0.5Hz inhibited the initiation of early action potentials in AD mice [35]. In particular, targeting hyperactive parietal regions, such as the precuneus and the posterior parietal cortex can restore network balance and reduce excitotoxicity. [23,33]
2.2.2. Patterned Stimulation Protocols
Recent developments include theta-burst stimulation (TBS), which delivers pulses in bursts of three, at a frequency of 50 Hz and an inter-burst interval in the theta-frequency range of 200 ms (5 Hz). The two most frequent patterns used are intermittent (iTBS) and continuous (cTBS), that can induce rapid LTP- or LTD-like changes. iTBS has been shown to enhance hippocampal-prefrontal connectivity and memory encoding in mild cognitive impairment and early AD [36]; while cTBS results in inhibitory effects. The advantage of TBS is shorter session duration and lower stimulation intensities, making it clinically feasible for repeated interventions [37].
2.2.3. Intensity and Pulse Number
Stimulation intensity is typically expressed as a percentage of resting motor threshold (RMT) and determines the depth and magnitude of cortical engagement. Studies in AD patients have used 80–120% RMT to achieve adequate excitatory effects without inducing adverse events. Higher cumulative pulses per session are associated with stronger and longer-lasting neuroplastic changes, although tolerability should be monitored, particularly in elderly populations.
2.2.4. Target Selection
The target stimulation area of the brain is another important variable that influences neurophysiological and clinical outcomes:
• Dorsolateral prefrontal cortex (DLPFC): Enhances working memory, attention, and executive function and increases functional connectivity. It is the most commonly targeted cortical region for AD treatment. 20 Hz rTMS applied to the left DLPFC significantly improves cognitive and psychiatric symptoms in AD patients [38]
• Precuneus and posterior cingulate cortex (PCC): Both sites are key nodes of the default mode network (DMN); their stimulation improves episodic memory and network connectivity. In particular, the effects of rTMS in the precuneus might propagate in the hippocampus through synaptic transmission in the precuneus-hippocampal pathway [39].
• Hippocampal network Personalized network-targeted TMS improves hippocampal-precuneus functional connectivity and memory consolidation. In particular, rTMS proved to have significant improvement on ADAS-Cog, particularly in the memory domain, as well as S-IADL and the Clinical Dementia Rating Scale–Sum of Boxes (CDR-SOB) scores. [33]
Network-based targeting is increasingly preferred over single-region stimulation because it engages distributed circuits underlying cognition and may maximize clinical benefit.
2.2.6. Clinical Relevance
Developing TMS protocols for AD treatment requires optimizing frequency, intensity, session duration, and target selection to achieve maximal neuroplasticity while minimizing adverse events. What seems to be more effective is to increase session frequency, target brain networks, and combine TMS with cognitive training or medications to produce lasting improvements in cognition and daily functioning.
3. Molecular and Cellular Mechanisms of TMS Relevant to Alzheimer’s Disease
Evidence indicates that TMS influences multiple biological pathways that are involved in the pathophysiology of AD i.e. enhancement of synaptic plasticity, regulation of inflammation, glial function, network level modulation and beta-amyloid clearance, thus making it promising candidate for modulating the pathophysiology of the disease. These mechanisms are summarized below and are depicted in Figure 1.
3.1. Synaptic Plasticity
Synaptic dysfunction can be detected at the early stages of AD pathology even before neuronal degeneration [40] The induction of brain plasticity requires cell pathways such as ERK/MAPK signaling pathway and the transcription factor response element-binding protein (CREB) [41] The pathways are needed to stimulate plasticity-related genes (PRG1-5) and improve cognitive function. Impairment in CREB-mediated gene transcription is associated with beta-amyloid deposition in AD patients. A reduction in CREB, as well as its activated form, pCREB, was observed in the hippocampus and the prefrontal cortex of mice and AD patients showing the importance of CREB transcription in the pathophysiology of neurodegeneration [42]. A study in a genetic AD mouse model showed that 25 Hz TMS reduced neuronal loss and apoptosis of hippocampal cells due to the activation of PI3K/Akt/GLT-1 pathway, which is associated with decreased excitotoxicity.
Both preclinical and clinical studies demonstrate that rTMS increases Brain-Derived Neurotrophic Factor (BDNF) expression in the cortex and hippocampus, as well as peripheral circulation, suggesting systemic effects. [31,43]. rTMS also enhances BDNF–TrkB signaling [44] by increasing the affinity of BDNF for TrkB receptor [45]. BDNF-TrkB pathway activates intracellular cascades that promote neuronal survival, growth and plasticity; processes that are severely impaired in AD. TMS might increase BDNF and NGF expression regardless of stimulation frequency, because LF and HF-rTMS both improved their reduced levels in an AD mouse model. [46] However Choung et al [47], observed that only HF-rTMS could increase BDNF levels in a mouse model with AD, that was induced by the injection of intracerebroventricular (ICV) Aβ42 oligomer.
The presence of a single nucleotide polymorphism BDNF-Val66Met, has also been associated with smaller hippocampal volumes and reduced grey matter in areas of frontal cortex as well as with the individual variability of TMS effects [48]. This finding underscores the potential value of prior genetic and molecular testing in optimizing individual TMS protocols.
3.2. Large Scale Network Modulation
There is evidence that pathophysiological changes observed in AD are associated with both cortical hyperexcitability and functional brain network disruption, particularly involving early changes within the DMN, suggesting that AD might be a disconnection syndrome [50] TMS can reorganize functional networks such as DMN and hippocampal–prefrontal circuits. In particular, non-invasive stimulation of the precuneus and hippocampal network has been shown to improve connectivity [51,52]
3.3. Neuroinflammation and Glial Modulation
Neuroinflammation is involved in the pathophysiology of AD by contributing to synaptic dysfunction, oxidative stress and as a result neuronal loss, and network disruption. Moreover, chronic neuroinflammation can cause severe neuronal and blood-brain-barrier disruption. Active glial cells that include microglia and astrocytes, release pro-inflammatory cytokines, complement proteins and reactive oxygen species (ROS), which can cause neuronal damage and lead to AD. [53] rTMS has been shown to modulate the activity of glial cells and inflammatory signaling in models of brain injury and neurodegeneration. Specifically, high-frequency rTMS reduces microglial activation in the dentate gyrus of the hippocampus and suppresses the production of pro-inflammatory mediators (IL-1α, IL-6, TNF-α) and pro-oxidative molecules (ROS and malondialdehyde), while increasing the levels of antioxidants like superoxide dismutase and glutathione in 3xTg AD mice [54]. Astrocytic responses, including regulation of IL-33 expression, further support neuroprotective outcomes. These effects suggest that rTMS could prevent the initiation of the cascade leading to the release of neuroinflammatory products that are involved in AD pathology. [55,56]
3.5. Effects on Amyloid Metabolism
TMS can indirectly reduce activity-dependent Abeta production, by enhancing clearance mechanisms including microglial phagocytosis and glymphatic flow. High-frequency rTMS stimulation a) increases expression of BDNF that enhances the activity of a-secretase and reduces Abeta production, and b) reduces levels of Abeta 1-42 in the hippocampus likely through PI3K/Akt pathway activation via the modulation of BACE1-mediated APP cleavage. rTMS reduces serum levels of Abeta 1-40, Abeta 1-42 and total Abeta [57]. Evidence also shows that rTMS modulates GSK-3β and CDK5 activity kinase/phosphatase pathways that control tau phosphorylation [47,58]. Tao et al. [58] applied 20 Hz rTMS to the DLPFC (100% RMT) for 20 minutes; after treatment, the soluble ectodomain of p75NTR — which inhibits Abeta accumulation — increased compared to controls.
3.6. Neurovascular Regulation and Neurotransmission
Vascular pathology that can exacerbate synaptic failure and cognitive decline plays a significant role in AD pathogenesis [59]. TMS has been shown to increase cerebral blood flow and induce angiogenesis [60]. Enhanced perfusion and vascular reactivity may improve neuronal resilience against the accumulation of toxic metabolites. Moreover, rTMS of the prefrontal cortex can induce the release of dopamine, improving metabolic efficiency within the targeted networks [61]. McNerney et al [62]. studied the effects of HF-rTMS (10 Hz, applied daily for 2 weeks or twice weekly for 6 weeks) in 3xTgAD mice and showed that rTMS increases acetylcholine levels by modulating AChE activity. In preclinical models, chronic rTMS treatment was found to modulate cortical serotonergic, adrenergic, and dopaminergic circuits in the rat brains [63]. These vascular and metabolic effects complement synaptic and glial modulation and current evidence shows that specific rTMS protocols can modulate the activity of the various neurotransmitter circuits that are affected in AD.
4. Clinical Evidence for TMS in Alzheimer’s Disease
Over the last years, clinical research on TMS in AD has evolved from promising initial exploratory pilot studies to randomized controlled trials employing network-based and personalized neuromodulation strategies. [21,22,23] These studies indicate that rTMS can improve or stabilize overall cognitive performance, modulate DMN brain networks, and result in neurophysiological and biomarker changes consistent with enhanced neuroplasticity. Although there is variability across centers in study design and stimulation parameters there is accumulating body of evidence that supports the clinical feasibility and therapeutic promise of TMS as an adjunctive intervention in AD.
4.1. Randomized Controlled Trials and Cognitive Outcomes
Randomized controlled trials (RCTs) indicate that rTMS can improve cognitive performance in patients with mild-to-moderate AD. The most widely used protocol is 2 weeks of everyday (5 days/week) treatment, followed by maintenance treatments (either 1 or 2 sessions/week) that could last up to 6 months.
Koch et al., 2025 [23] conducted a 52-week RCT (divided in a 2 week intensive course and a 50-week maintenance phase) in patients with mild-to-moderate dementia due to AD targeting the precuneus, demonstrating slowed cognitive decline measured by several neuropsychometric tests such as: CDR-SB, improved ADAS-Cog, MMSE, and improved functional outcomes (assessed by ADCS-ADL). Functional MRI indicated increased hippocampal–precuneus connectivity, suggesting that rTMS improves cognition by modulating network function.
Jung et al., 2024 [22] studied 30 patients with either MCI due to AD or mild AD dementia by using a personalized hippocampal network-targeted rTMS protocol. They delivered 20 sessions over 8 weeks and stimulated the left parietal area. This approach led to significant improvements in ADAS-Cog and memory performance, with fMRI showing improved hippocampal–precuneus functional connectivity. Effects appeared by week 8, and improvements persisted for at least four weeks after treatment ended.
Earlier trials targeting the DLPFC and temporoparietal regions also reported improvements in memory, language, and executive function. Nguyen, et al [64], combined rTMS with cognitive training (NeuroAD protocol). In the NeuroAD protocol rTMS was targeted over six brain areas that were thought to be impaired in AD: such as right and left prefrontal cortex, right and left parietal cortex, and Broca's and Wernicke's areas. These target areas were identified by the Neuronix neuronavigation system based on the individual patient's brain MRI. According to the results of the study, the cognitive gains (i.e. significantly improved ADAS-Cog score) persisted for up to approximately 8 months post-intervention. Similar results were observed in a recent study by Luo et al., 2026 [65]. Moreoever, a meta-analysis by Menardi et al. [66] compared the effects of cognitive training and found that only the combination of rTMS and cognitive training produced significant results for overall cognitive function, while rTMS alone showed no effectiveness. These results indicate that both cortical stimulation and network-targeted approaches can have clinically meaningful results.
4.2. Meta-Analyses and Systematic Reviews
Meta-analyses consolidate the effects of rTMS across studies. A 2024 meta-analysis of nine randomized controlled trials including 361 patients [67] showed an improvement in MMSE and ADAS-Cog scores immediately after treatment, which persisted one month later. High-frequency protocols (>10 Hz) targeting the DLPFC for ≥20 sessions resulted in better therapeutic results. Stimulation of the DLPFC, the most common stimulation target for improving cognitive function in patients with AD, was found to be most effective. Another meta-analysis including patients with AD and MCI [68] confirmed moderate-to-large effect sizes on global cognitive function, emphasizing the importance of frequency, total sessions and pulses, duration and stimulation site. These analyses underscore the potential of rTMS as a symptomatic intervention while highlighting the need for protocol standardization to optimize efficacy. A summary of randomized control trials on the role of TMS in AD treatment is presented in Table 1
4.3. Network and Neurophysiological Effects
Network-level mechanisms are getting more emphasis in clinical studies. Personalized stimulation of the hippocampus and precuneus enhances functional connectivity within the DMN and the precuneus-hippocampal circuits. DLPFC stimulation was shown to be the most effective stimulation site for improving cognitive impairment in AD patients [64]. Moreover, EEG studies report decreased delta-band activity and normalized theta and gamma oscillations that correlate with improved cognitive function [71]. Targeting networks holds promise; better rTMS outcomes correlate with higher baseline intra-cortical connectivity, suggesting pre-treatment DMN regulation predicts treatment response.[72]
4.4. Safety and Tolerability
rTMS is effective and well tolerated in older adults and people with AD. The most frequently reported adverse effects are transient headaches and local discomfort at the site of stimulation. Seizures are extremely rare, with a rate of roughly <1 per 30,000 sessions, when strictly adhering to established guidelines. When present, they resolve on their own [73]. Long-term follow-up, including the 52-week precuneus trial, found no sustained adverse effects, supporting the safety of repeated and maintenance sessions.
5. Conclusions
TMS offers non-invasive AD neuromodulation, potentially improving cognition and influencing disease networks and pathology. TMS helps restore synaptic plasticity, normalizes network connectivity, and reduces neuroinflammation; it may indirectly influence beta-amyloid and tau protein levels. Neurovascular and metabolic improvements further support neuronal resilience.
Current clinical evidence suggests that rTMS, particularly when delivered in personalized, network-targeted protocols, can improve memory and global cognition in patients with mild-to-moderate AD, with effects lasting up to 3 months [67]. rTMS demonstrates a good safety profile in AD treatment, with multiple studies reporting few adverse events. Biomarker and neuroimaging studies suggest that TMS-induced improvements in connectivity and plasticity correlate with clinical cognitive improvements; this agrees with preclinical findings that TMS improves connectivity and plasticity in animal models. Current guidelines suggest that multisite rTMS together with cognitive training is probably effective (Level C of Evidence) in improving cognitive function in AD patients, especially at a mild/early stage of the disease [16].
Despite the encouraging results, several challenges remain that limit the wider clinical application of TMS. Heterogeneity in stimulation protocols, target selection, session duration, and patient characteristics limits cross-study comparisons and definitive conclusions regarding TMS efficacy in AD. Larger, multicenter trials with extended follow-up and integration of multimodal biomarkers (e.g., resting state connectivity, TMS EEG, PET imaging, fluid biomarkers), genotype stratification (e.g., BDNF, APOE), and longer follow up are required in order to assess the long-term effects and disease-modifying potential of TMS. [73]
Future research should focus on target precision neuromodulation using imaging and physiological markers in order to design individualized TMS protocols. Combining TMS with cognitive training, pharmacotherapy, or other methods of neuromodulation may further enhance therapeutic outcomes. Continued exploration of TMS mechanisms will elucidate how network, glial, and synaptic modulation contribute to disease modification, ultimately bridging preclinical insights with clinical application.
In summary, TMS holds significant promise as a safe, and potentially disease-modifying adjunctive therapy for AD. Ongoing advancements in personalized stimulation protocols and mechanistic understanding are poised to optimize its clinical effectiveness and integrate TMS into new multi-modal therapeutic strategies that will target cognitive impairment and network dysfunction in AD.
Author Contributions
Conceptualization, V.P.; methodology, V.P, V.K.K.; writing—original draft preparation, V.P, K.K.; writing—review and editing, M.M.,M.A, E.K..; supervision V.K.K. All authors have read and agreed to the published version of the manuscript..
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| TMS | Transcranial Magnetic Stimulation |
| AD MCI DMN |
Alzheimer’s Disease Mild Cognitive Impairment Default mode Network |
| DLPFC | Dorsolateral Prefrontal Cortex |
| BDNF ROS |
Brain Derived Neurotrophic Factor Reactive Oxygen Species |
References
- World Health Organization. Dementia. WHO Fact Sheet. 2023. [Google Scholar]
- Long, J.M.; Holtzman, D.M. Alzheimer disease: An update on pathobiology and treatment strategies. Cell 2019, 179, 312–339. [Google Scholar] [CrossRef] [PubMed]
- De Strooper, B.; Karran, E. The cellular phase of Alzheimer’s disease. Cell 2016, 164, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Pozo, A.; Frosch, M.P.; Masliah, E.; Hyman, B.T. Neuropathological alterations in Alzheimer disease. Cold Spring Harb. Perspect. Med. 2011, 1, a006189. [Google Scholar] [CrossRef]
- Birks, J.S.; Harvey, R.J. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database Syst. Rev. 2018, CD001190. [Google Scholar] [CrossRef]
- Knopman, D.S.; Jones, D.T.; Greicius, M.D. Failure to demonstrate efficacy of aducanumab: An analysis of the EMERGE and ENGAGE trials. Alzheimers Dement. 2021, 17, 696–701. [Google Scholar] [CrossRef]
- Cummings, J; Zhou, Y; Lee, G; Zhong, K; Fonseca, J; Cheng, F. Alzheimer's disease drug development pipeline: 2024. Alzheimer's Dement 2024, 10, e12465. [Google Scholar] [CrossRef]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The brain’s default network. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar] [CrossRef]
- Brier, M.R.; Thomas, J.B.; Snyder, A.Z.; et al. Loss of intranetwork and internetwork resting state functional connections with Alzheimer’s disease progression. J. Neurosci. 2012, 32, 8890–8899. [Google Scholar] [CrossRef]
- Palop, J.J.; Mucke, L. Network abnormalities and interneuron dysfunction in Alzheimer disease. Nat. Rev. Neurosci. 2016, 17, 777–792. [Google Scholar] [CrossRef]
- Ereira, S.; Waters, S.; Razi, A.; et al. Early detection of dementia with default-mode network effective connectivity. Nat. Mental Health 2024, 2, 787–800. [Google Scholar] [CrossRef]
- Hallett, M. Transcranial magnetic stimulation: A primer. Neuron 2007, 55, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Wagner, T.; Valero-Cabré, A.; Pascual-Leone, A. Noninvasive human brain stimulation. Annu. Rev. Biomed. Eng. 2007, 9, 527–565. [Google Scholar] [CrossRef] [PubMed]
- Rotenberg, A.; Horvath, J.C.; Pascual-Leone, A. Transcranial Magnetic Stimulation; Springer: New York, NY, USA, 2019. [Google Scholar]
- Hoogendam, J.M.; Ramakers, G.M.; Di Lazzaro, V. Physiology of repetitive transcranial magnetic stimulation of the human brain. Brain Stimul. 2010, 3, 95–118. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.P.; Aleman, A.; Baeken, C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation. Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef]
- Koch, G.; Bonnì, S.; Casula, E.P.; et al. Transcranial magnetic stimulation of the precuneus enhances memory and neural activity in Alzheimer’s disease. Brain 2018, 141, 1961–1974. [Google Scholar] [CrossRef]
- Cirrito, J.R.; Yamada, K.A.; Finn, M.B.; et al. Synaptic activity regulates interstitial fluid amyloid-β levels in vivo. Neuron 2005, 48, 913–922. [Google Scholar] [CrossRef]
- Hampel, H.; Mesulam, M.M.; Cuello, A.C.; et al. The cholinergic system in the pathophysiology and treatment of Alzheimer’s disease. Brain 2018, 141, 1917–1933. [Google Scholar] [CrossRef]
- Bentwich, J.; Dobronevsky, E.; Aichenbaum, S.; et al. Beneficial effect of repetitive transcranial magnetic stimulation combined with cognitive training in Alzheimer’s disease. Alzheimers Dement. 2011, 7, 490–498. [Google Scholar]
- Rabey, JM; Dobronevsky, E; Aichenbaum, S; Gonen, O; Marton, RG; Khaigrekht, M. Repetitive transcranial magnetic stimulation combined with cognitive training is a safe and effective modality for the treatment of Alzheimer's disease: a randomized, double-blind study. J Neural Transm (Vienna) 2013, 120(5), 813–9. [Google Scholar] [CrossRef]
- Jung, YH; Jang, H; Park, S; Kim, HJ; Seo, SW; Kim, GB; Shon, YM; Kim, S; Na, DL. Effectiveness of Personalized Hippocampal Network-Targeted Stimulation in Alzheimer Disease: A Randomized Clinical Trial. JAMA Netw Open 2024, 7(5), e249220. [Google Scholar] [CrossRef]
- Koch, G.; Casula, E.P.; Bonnì, S.; et al. Effects of 52 weeks of precuneus rTMS in Alzheimer’s disease. Alzheimers Res. Ther. 2025, 17, 69. [Google Scholar] [CrossRef]
- Vlachos, A.; Ziemann, U. Metaplasticity in human cortex: Mechanisms and clinical significance. Neuroscientist 2014, 20, 583–597. [Google Scholar]
- Cullen, C.L.; Young, K.M. How does transcranial magnetic stimulation influence glial cells in the central nervous system? Front. Neural Circuits 2016, 10, 26. [Google Scholar]
- Quentin, R; Elkin Frankston, S; Vernet, M; Toba, MN; Bartolomeo, P; Chanes, L; Valero-Cabré, A. Visual Contrast Sensitivity Improvement by Right Frontal High-Beta Activity Is Mediated by Contrast Gain Mechanisms and Influenced by Fronto-Parietal White Matter Microstructure. Cereb Cortex 2016, 26, 2381–90. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, Y.; Chen, L.; Wang, H.; Yuan, H.; Li, K.; Zhang, L. Therapeutic Potential and Mechanisms of Repetitive Transcranial Magnetic Stimulation in Alzheimer’s Disease: A Literature Review. Eur. J. Med. Res. 2025, 30, 233. [Google Scholar] [CrossRef] [PubMed]
- Ueno, S; Sekino, M. Figure-Eight Coils for Magnetic Stimulation: From Focal Stimulation to Deep Stimulation. Front Hum Neurosci. 2021, 15, 805971. [Google Scholar] [CrossRef]
- Aberra, AS; Wang, B; Grill, WM; Peterchev, AV. Simulation of transcranial magnetic stimulation in head model with morphologically-realistic cortical neurons. Brain Stimul. 2020, 13(1), 175–189. [Google Scholar] [CrossRef]
- King, ES; Tang, AD. Intrinsic Plasticity Mechanisms of Repetitive Transcranial Magnetic Stimulation. Neuroscientist 2024, 30, 260–274. [Google Scholar] [CrossRef]
- Antonioni, A; Martorana, A; Santarnecchi, E; Hampel, H; Koch, G. The neurobiological foundation of effective repetitive transcranial magnetic brain stimulation in Alzheimer's disease. Alzheimers Dement. 2025, 21, e70337. [Google Scholar] [CrossRef]
- Gomez-Tames, J.; Hamasaka, A.; Laakso, I.; Hirata, A.; Ugawa, Y. Atlas of optimal coil orientation and position for TMS: A computational study. Brain Stimul 2018, 11, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Jung, YH; Jang, H; Park, S; Kim, HJ; Seo, SW; Kim, GB; Shon, YM; Kim, S; Na, DL. Effectiveness of Personalized Hippocampal Network-Targeted Stimulation in Alzheimer Disease: A Randomized Clinical Trial. JAMA Netw Open. 2024, 7(5), e249220. [Google Scholar] [CrossRef] [PubMed]
- Xiu, H; Liu, F; Hou, Y; Chen, X; Tu, S. High-frequency repetitive transcranial magnetic stimulation (HF-rTMS) on global cognitive function of elderly in mild to moderate Alzheimer's disease: a systematic review and meta-analysis. Neurol Sci. 2024, 45(1), 13–25. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z; Ding, C; Fu, R; Wang, J; Zhao, J; Zhu, H. Low-frequency rTMS modulated the excitability and high-frequency firing in hippocampal neurons of the Alzheimer’s disease mouse model. Brain Research 2024, 1831 148822. [Google Scholar] [CrossRef]
- Aghamoosa, S; Nolin, SA; Chen, AA; Caulfield, KA; Lopez, J; Rbeiz, K; Fleischmann, HH; Horn, O; Madden, K; Antonucci, M; Revuelta, G; McTeague, LM; Benitez, A. Accelerated iTBS-Induced changes in resting-state functional connectivity correspond with cognitive improvement in amnestic MCI. Brain Stimul. 2025, 18(3), 957–964. [Google Scholar] [CrossRef]
- Huang, Y.; Zelmann, R.; Hadar, P.; et al. Theta-burst direct electrical stimulation remodels human brain networks. Nat Commun 2024, 15, 6982. [Google Scholar] [CrossRef]
- Li, X; Qi, G; Yu, C; Lian, G; Zheng, H; Wu, S; et al. Cortical plasticity is correlated with cognitive improvement in Alzheimer’s disease patients after rTMS treatment. Brain Stimul. 2021, 14, 503–10. [Google Scholar] [CrossRef]
- Mancini, M.; Mastropasqua, C.; Bonnì, S.; et al. Theta Burst Stimulation of the Precuneus Modulates Resting State Connectivity in the Left Temporal Pole. Brain Topogr 2017, 30, 312–319. [Google Scholar] [CrossRef]
- Pelucchi, S; Gardoni, F; Di Luca, M; Marcello, E. Synaptic dysfunction in early phases of Alzheimer's Disease. Handb Clin Neurol. 2022, 184, 417–438. [Google Scholar] [CrossRef]
- Zent, Katlin H.; Dell’Acqua, Mark L. Synapse-to-Nucleus ERK→CREB Transcriptional Signaling Requires Dendrite-to-Soma Ca2+ Propagation Mediated by L-Type Voltage–Gated Ca2+ Channels. Journal of Neuroscience 2025, 45(4), e1216242024. [Google Scholar] [CrossRef]
- Pugazhenthi, S; Wang, M; Pham, S; Sze, CI; Eckman, CB. Downregulation of CREB expression in Alzheimer’s brain and in Aβ-treated rat hippocampal neurons. Mol Neurodegener. 2011, 6, 60. [Google Scholar] [CrossRef]
- Bashir, S; Uzair, M; Abualait, T; Arshad, M; Khallaf, RA; Niaz, A; Thani, Z; Yoo, WK; Túnez, I; Demirtas-Tatlidede, A; Meo, SA. Effects of transcranial magnetic stimulation on neurobiological changes in Alzheimer's disease (Review). Mol Med Rep. 2022, 25, 109. [Google Scholar] [CrossRef]
- Riccitelli, G.C.; Gironi, R.; Melli, G.; Kaelin-Lang, A. The Effect of Repetitive Transcranial Magnetic Stimulation Treatment on Plasma BDNF Concentration and Executive Functions in Parkinson’s Disease: A Theoretical Translational Medicine Approach. Int. J. Mol. Sci. 2025, 26, 1205. [Google Scholar] [CrossRef]
- Wang, HY; Crupi, D; Liu, J; Stucky, A; Cruciata, G; Di Rocco, A; Friedman, E; Quartarone, A; Ghilardi, MF. Repetitive transcranial magnetic stimulation enhances BDNF-TrkB signaling in both brain and lymphocyte. J Neurosci. 2011, 27;31(30), 11044–54. [Google Scholar] [CrossRef]
- Pang, Y; Shi, M. Repetitive transcranial magnetic stimulation improves mild cognitive impairment associated with Alzheimer's disease in mice by modulating the miR-567/NEUROD2/PSD95 Axis. Neuropsychiatr Dis Treat. 2021, 17, 2151–2161. [Google Scholar] [CrossRef] [PubMed]
- Choung, JS; Kim, JM; Ko, MH; Cho, DS; Kim, M. Therapeutic efficacy of repetitive transcranial magnetic stimulation in an animal model of Alzheimer's disease. Sci Rep. 2021, 11(1), 437. [Google Scholar] [CrossRef] [PubMed]
- Cheeran, B; Talelli, P; Mori, F; Koch, G; Suppa, A; Edwards, M; Houlden, H; Bhatia, K; Greenwood, R; Rothwell, JC. A common polymorphism in the brain-derived neurotrophic factor gene (BDNF) modulates human cortical plasticity and the response to rTMS. J Physiol. 2008, 586(23), 5717–25. [Google Scholar] [CrossRef] [PubMed]
- Gersner, R; Kravetz, E; Feil, J; Pell, G; Zangen, A. Long-term effects of repetitive transcranial magnetic stimulation on markers for neuroplasticity: differential outcomes in anesthetized and awake animals. J Neurosci. 2011, 31, 7521–7526. [Google Scholar] [CrossRef]
- Ozdemir, RA; et al. Neurophysiological signatures of default mode network dysfunction and cognitive decline in Alzheimer’s disease. Sci. Adv. 2025, 11, eadt8991. [Google Scholar] [CrossRef]
- Millet, B; Mouchabac, S; Robert, G; Maatoug, R; Dondaine, T; Ferreri, F; Bourla, A. Transcranial Magnetic Stimulation (rTMS) on the Precuneus in Alzheimer's Disease: A Literature Review. Brain Sci. 2023, 13, 1332. [Google Scholar] [CrossRef]
- Chen, J; Ma, N; Hu, G; Nousayhah, A; Xue, C; Qi, W; Xu, W; Chen, S; Rao, J; Liu, W; Zhang, F; Zhang, X. rTMS modulates precuneus-hippocampal subregion circuit in patients with subjective cognitive decline. Aging (Albany NY). 2020, 13, 1314–1331. [Google Scholar] [CrossRef] [PubMed]
- Adamu, A; Li, S; Gao, F; Xue, G. The role of neuroinflammation in neurodegenerative diseases: current understanding and future therapeutic targets. Front Aging Neurosci. 2024, 16, 1347987. [Google Scholar] [CrossRef] [PubMed]
- Cao, H; Zuo, C; Gu, Z; et al. High frequency repetitive transcranial magnetic stimulation alleviates cognitive deficits in 3xTg-AD mice by modulating the PI3K/Akt/GLT-1 axis. Redox Biol. 2022, 54, 102354. [Google Scholar] [CrossRef] [PubMed]
- d’Errico, P; Früholz, I; Meyer-Luehmann, M; Vlachos, A. Neuroprotective and plasticity promoting effects of repetitive transcranial magnetic stimulation (rTMS): A role for microglia. Brain Stimulation 2025, 18, 810–821. [Google Scholar] [CrossRef]
- Qian, F; He, R; Du, X; Wei, Y; Zhou, Z; Fan, J; He, Y. Microglia and Astrocytes Responses Contribute to Alleviating Inflammatory Damage by Repetitive Transcranial Magnetic Stimulation in Rats with Traumatic Brain Injury. Neurochem Res. 2024, 49, 2636–2651. [Google Scholar] [CrossRef]
- Nigam, SM; Xu, S; Kritikou, JS; Marosi, K; Brodin, L; Mattson, MP. Exercise and BDNF reduce Aβ production by enhancing α-secretase processing of APP. J Neurochem. 2017, 142, 286–296. [Google Scholar] [CrossRef]
- Tao, Y; Lei, B; Zhu, Y; Fang, X; Liao, L; Chen, D; Gao, C. Repetitive Transcranial Magnetic Stimulation Decreases Serum Amyloid-β and Increases Ectodomain of p75 Neurotrophin Receptor in Patients with Alzheimer's Disease. J Integr Neurosci. 2022, 21(5), 140. [Google Scholar] [CrossRef]
- Li, S; Xiao, Z. Recent Research Progress on the Use of Transcranial Magnetic Stimulation in the Treatment of Vascular Cognitive Impairment. Neuropsychiatr Dis Treat. 2024, 20, 1235–1246. [Google Scholar] [CrossRef]
- Kinney, KR; Hanlon, CA. Changing Cerebral Blood Flow, Glucose Metabolism, and Dopamine Binding Through Transcranial Magnetic Stimulation: A Systematic Review of Transcranial Magnetic Stimulation-Positron Emission Tomography Literature. Pharmacol Rev. 2022, 74(4), 918–932. [Google Scholar] [CrossRef]
- Strafella, AP; Paus, T; Barrett, J; Dagher, A. Repetitive transcranial magnetic stimulation of the human prefrontal cortex induces dopamine release in the caudate nucleus. J Neurosci. 2001, 21(15), RC157. [Google Scholar] [CrossRef]
- McNerney, MW; Heath, A; Narayanan, SK; Yesavage, J. Repetitive transcranial magnetic stimulation improves brain-derived neurotrophic factor and cholinergic signaling in the 3xTgAD mouse model of Alzheimer's disease. J Alzheimer Dis. 2022, 86, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Kanno, M; Matsumoto, M; Togashi, H; Yoshioka, M; Mano, Y. Effects of acute repetitive transcranial magnetic stimulation on dopamine release in the rat dorsolateral striatum. J Neurol Sci. 2004, 217, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.P.; Suarez, A.; Le Saout, E.; et al. Combining cognitive training and rTMS in Alzheimer’s disease. Neurophysiol. Clin. 2018, 48, 1–9. [Google Scholar]
- Luo, J; Tan, Z; Shang, P; Huang, S; Liu, Y; Wang, Y; Xie, H; Chen, Q. Accelerated intermittent theta burst stimulation combined with cognitive training modulates cortical plasticity and brain activation in patients with amnestic mild cognitive impairment. Exp Gerontol. 2026, 213, 113009. [Google Scholar] [CrossRef]
- Menardi, A; Dotti, L; Ambrosini, E; Vallesi, A. Transcranial magnetic stimulation treatment in Alzheimer’s disease: A meta-analysis of its efficacy as a function of protocol characteristics and degree of personalization. J Neurol 2022, 269, 5283–5301. [Google Scholar] [CrossRef]
- Zhang, T; Sui, Y; Lu, Q; Xu, X; Zhu, Y; Dai, W; Shen, Y; Wang, T. Effects of rTMS treatment on global cognitive function in Alzheimer's disease: A systematic review and meta-analysis. Front Aging Neurosci. 2022, 8;14, 984708. [Google Scholar] [CrossRef]
- Li, S; Lan, X; Liu, Y; Zhou, J; Pei, Z; Su, X; Guo, Y. Unlocking the Potential of Repetitive Transcranial Magnetic Stimulation in Alzheimer's Disease: A Meta-Analysis of Randomized Clinical Trials to Optimize Intervention Strategies. J Alzheimers Dis. 2024, 98, 481–503. [Google Scholar] [CrossRef]
- Rabey, JM; Dobronevsky, E; Aichenbaum, S; Gonen, O; Marton, RG; Khaigrekht, M. Repetitive transcranial magnetic stimulation combined with cognitive training is a safe and effective modality for the treatment of Alzheimer's disease: a randomized, double-blind study. J Neural Transm (Vienna) 2013, 120, 813–9. [Google Scholar] [CrossRef]
- Moussavi, Z; Uehara, M; Rutherford, G; Lithgow, B; Millikin, C; Wang, X; Saha, C; Mansouri, B; Omelan, C; Fellows, L; Fitzgerald, PB; Koski, L. Repetitive transcranial magnetic stimulation as a treatment for Alzheimer's disease: A randomized placebo-controlled double-blind clinical trial. Neurotherapeutics 2024, 21, e00331. [Google Scholar] [CrossRef]
- Dong, X; Yan, L; Huang, L; Guan, X; Dong, C; Tao, H; Wang, T; Qin, X; Wan, Q. Repetitive transcranial magnetic stimulation for the treatment of Alzheimer's disease: A systematic review and meta-analysis of randomized controlled trials. PLoS One. 2018, 13, e0205704. [Google Scholar] [CrossRef]
- Velioglu, HA; Dudukcu, EZ; Hanoglu, L; Guntekin, B; Akturk, T; Yulug, B. rTMS reduces delta and increases theta oscillations in Alzheimer's disease: A visual-evoked and event-related potentials study. CNS Neurosci Ther. 2024, 30(1), e14564. [Google Scholar] [CrossRef]
- Stultz, DJ; Osburn, S; Burns, T; Pawlowska-Wajswol, S; Walton, R. Transcranial Magnetic Stimulation (TMS) Safety with Respect to Seizures: A Literature Review. Neuropsychiatr Dis Treat. 2020, 16, 2989–3000. [Google Scholar] [CrossRef]
- Chen, HF; Sheng, XN; Yang, ZY; Shao, PF; Xu, HH; Qin, RM; Zhao, H; Bai, F. Multi-networks connectivity at baseline predicts the clinical efficacy of left angular gyrus-navigated rTMS in the spectrum of Alzheimer's disease: A sham-controlled study. CNS Neurosci Ther. 2023, 29(8), 2267–2280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Molecular and cellular mechanisms of TMS. From ref. [31] CC by 4.0.
Figure 1.
Molecular and cellular mechanisms of TMS. From ref. [31] CC by 4.0.
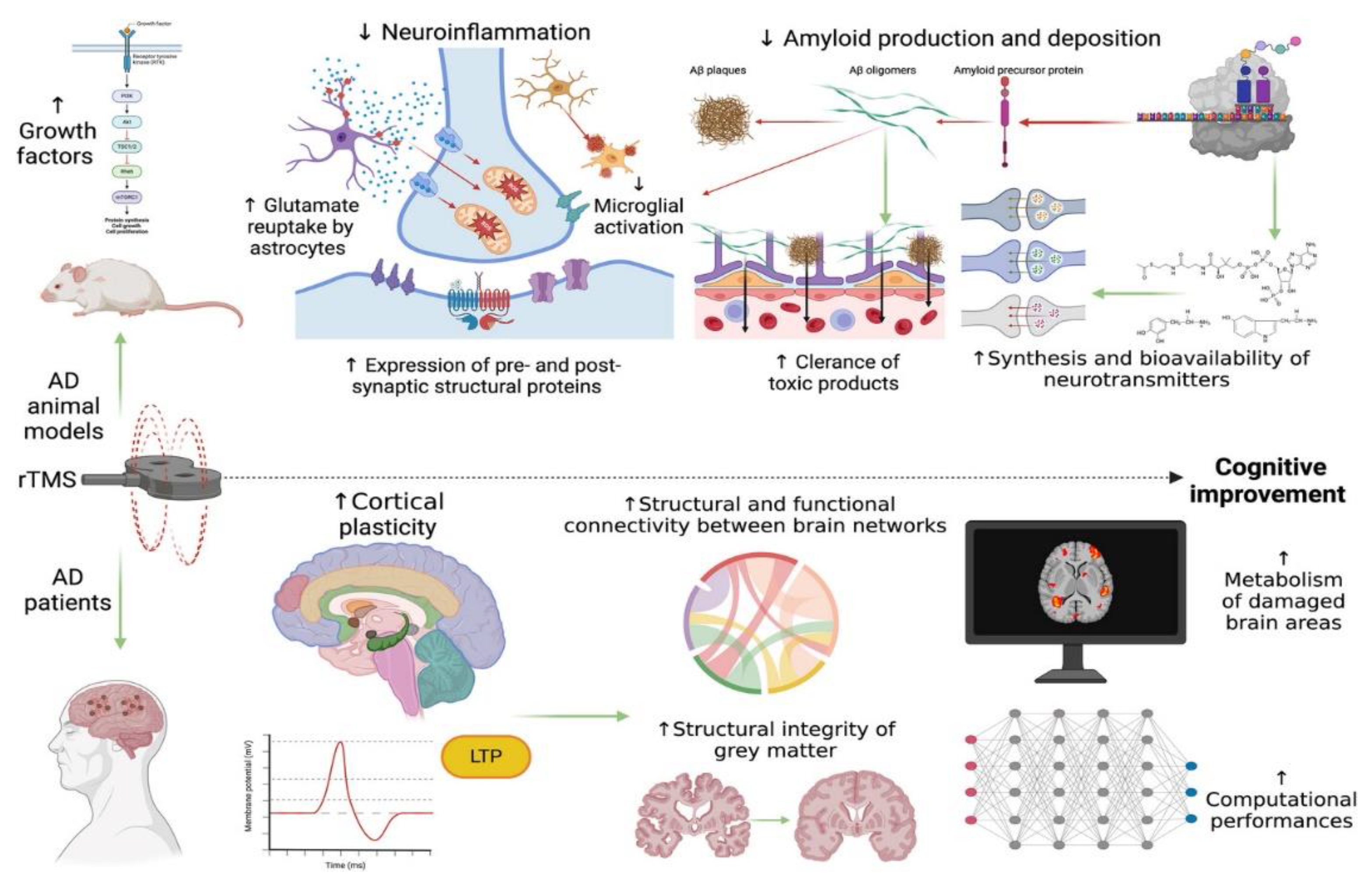

Table 1.
Summary of randomized control trials on the role of TMS efficacy in AD treatment.
| Study (Year) | Sample Size | Target Region | Frequency (Hz) | Sessions | Main Cognitive Outcomes | Notes / Biomarkers |
| Koch et al., 2025 | 60 | Precuneus | 10 | 52 weeks, weekly | Slowed decline in CDR-SB, ADAS-Cog; improvements in MMSE & ADCS-ADL | Functional MRI: increased precuneus-hippocampus connectivity |
| Jung et al., 2024 | 40 | Hippocampal network (personalized) | 20 | 8 weeks, 20 sessions | ADAS-Cog improvement; enhanced memory & attention | fMRI connectivity changes correlated with cognitive gains |
| Nguyen, et al 2017 | 10 | 6 brain areas | 10 | 25 sessions 5 weeks | MMSE & ADAS-Cog improvement | Combined with cognitive training (NeuroAD protocol) |
| Rabey et al., 2013 [69] | 45 | DLPFC + parietal | 20 | 6 weeks, 30 sessions | Memory & language improvements; functional gains | Open-label study; reported long-term retention up to 3 months |
| Moussavi et al., 2024 [70] | 156 | Bilateral DLPFC | 20 | 4 weeks, 20 sessions | ADAS-Cog improvement, | Similar results with Sham Coil |
| Liu et al., 2024 | 38 | DLPFC | 10 | 20 sessions / 4 weeks | Improvement in MMSE & ADAS-Cog | Peripheral BDNF elevation observed; no serious adverse events |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



