
Submitted:
26 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
The impact of Infectious diseases knows no boundaries, as the implications involve increase in morbidity, mortality and cost of healthcare system globally. Early and accurate infection diagnosis contributes to reduction of infection burden; however, this is often not achieved using traditional methods such as culture-based methods. Emerging and reemerging infectious diseases require fast and accurate detection method, hence, the advancement of molecular testing techniques such as polymerase chain reaction, whole genomic analysis, biosensor, nucleic acid sequencing and loop mediated isothermal amplification (LAMP) have changed the diagnosis of infectious diseases. However, unavailability and lack of adequate funding to the latest innovative methods, especially in less developed countries have been a major hurdle in the applications of such diagnostic methods. Therefore, this review will appraise both traditional diagnostic methods and the new innovative diagnostic techniques for their merits and demerits.
Keywords:
infectious diseases
; molecular diagnostics
; rapid testing
; loop mediated isothermal amplification (LAMP)
; point-of-care testing
1. Introduction
Despite enormous progress in medicine and communal health, infectious diseases continue to pose a significant condition of morbidity and death all over the globe. Bacterial, viral, fungal and parasitic diseases have remained critical health issues, especially in low- and middle-income nations where the systems of health care and diagnostic services are usually poor. The World Health Organization (WHO) states that every year millions of people die due to infectious diseases, and the number of emerging and re-emerging pathogens complicates the process of combating diseases even more globally (WHO, 2022). The proper diagnosis is thus the key to effective clinical management, infection control, and the surveillance of the population health.
Conventionally, the clinical assessment in the diagnosis of infectious diseases has been based on laboratory-supported clinical assessment, which includes microscopy, culture, and serological assays. These traditional methods have formed the basis of diagnostic microbiology over decades and have had a role to play in the knowledge and control of infectious agents. Nevertheless, some of the conventional diagnostic methods are usually labour-intensive, slow, and less sensitive, especially in the case of fastidious, slow-growing, or non-culturable microorganisms (Clerc et al., 2016). Failure to diagnose in time may bring inappropriate treatment, excessive hospitalization, high cost of health care, and even death.
Over the past few years, the infectious disease diagnosis environment has been radically reformed by the extreme pace of changes in the field of molecular biology, biotechnology, and digital health technologies. Polymerase Chain reactions (PCR) based assays, next-generation sequencing, mass spectrometry, biosensors, and point-of-care testing platforms are novel diagnostic tools that have transformed pathogen detection and identification. The technologies are more sensitive and specific than conventional methods and provide faster turnaround times, which allows identifying the disease earlier and a more focused response to the therapeutic intervention (Miller et al., 2021). The incorporation of these innovations into the everyday clinical practice is a paradigm shift towards the old-fashioned lab-based diagnostics up to the rapid and accurate and in many cases decentralized testing systems.
Global health emergencies, particularly the COVID-19 pandemic, have also contributed to the rapid growth of the paradigm shift in the diagnosis of infectious diseases. The unprecedented need in quick and precise diagnostic testing revealed the weaknesses of the conventional diagnostic processes and the significance of high-throughput and scalable diagnostic technologies that would be administered at-point-of-care (Carter et al., 2020). As a result, the use of diagnostic innovation has been a major issue in pandemic preparedness and response in addition to antimicrobial resistance surveillance.
This shift of the ancient to technology-advanced diagnostic methods in the medical field is crucial to the laboratory activity, clinical judgment, and health policy in general. Although contemporary diagnostic tools present significant opportunities, their application is typically limited by financial and technical factors, as well as the presence of qualified staff, especially in a low-resource environment (Peeling et al., 2019). Based on this, it is imperative to have an insight into the merits and demerits of old and new methods of diagnosis in order to have a balanced and sustainable diagnostic strategy.
2. Diagnosis Infectious Disease Diagnosis
Diagnosis of infectious diseases is based on the structured conceptual framework that incorporates the knowledge of the disease causation, host-pathogen interactions, and laboratory science. This framework is the theoretical and practical foundation of the work of traditional and modern technologies of diagnosis. It is important to understand the categorization of infectious diseases, principles that guide the decision-making process in the diagnostic practice and the role of medical microbiology in diagnostic practices to appreciate the paradigm shift taking place in the diagnostic practices. This shift from old traditional methods that are slow and to some extent less specific to modern and sensitive technologies is necessary to detect even slow grown microorganisms that are difficult to culture (Alsharksi et al., 2024).
2.1. Definition and Classification of Infectious Diseases
Infectious diseases refer to the conditions attributed to the invasion, multiplication and interaction of the pathogenic microorganisms in a weak host. Infectious diseases account for significant global burden of disease with impacts on global public health systems and economies (van Seventer and Hochberg, 2017). Kristine et al., 2019 reported a multisectoral impacts of infectious diseases on health sector, economies, trade and industry, agriculture and environmental consequences.
These microorganisms are bacteria, viruses, fungi and parasites that have different biological features, pathogenesis and modes of transmission. These agents have a wide range of capacities to bypass host immune defenses and lead to illness, which affects clinical presentation and diagnostic approaches (Murray, Rosenthal and Pfaller, 2021). Interestingly, these infectious diseases could be emerging, driving by many factors such as microbial strategies for survival, ecological factors, human factors, weak public health system and globalization (Verma, 2021; Sattar et al., 2025)
Prokaryotic organisms can cause bacterial infections and can be normal microflora of humans or pathogens. Some bacteria are pathogenic due to direct tissue invasion but other pathogenic bacteria have effects through toxin production. Examples of these include Mycobacterium tuberculosis, Staphylococcus aureus and Escherichia coli. Traditionally, diagnostic methods of bacterial infections have been based on microscopy, culture, and biochemical identification, which rely on morphological features (Figure 1) but nowadays molecular techniques gain more and more significance (Forbes et al., 2018).
On the contrary, viral infections are brought about by obligate intracellular pathogens, which replicate using host cellular machineries. Examples of viruses that pose special diagnostic problems because of their tiny size, non-growth in artificial cultures, and high mutation rates include influenza virus, human immunodeficiency virus (HIV), and hepatitis viruses, as well as SARS-CoV-2. Of particular concern is diagnosis of emerging viral infection and those associated with travel history such as dengue viruses, chikungunya viruses(Verheyen, 2015; Pretorius and Venter, 2017) Traditionally, the diagnosis relied on serology and the cell culture process, but nowadays the nucleic acid-based detection techniques became the fundamental principles of viral diagnostics which improve timeliness and accuracy with enhanced treatment outcome (Knipe and Howley, 2020).
Fungal infections are eukaryotic organisms which can either be moulds, dimorphic fungi or yeast. Such infections are either superficial infection like dermatophytosis, invasive and lethal infections especially in the immunocompromised. Fungal infections have a slow growth rate and complicated morphology, which necessitates a combination of microscopy, culture, antigen detection, and molecular techniques (Pappas et al., 2018). Another challenge in fungal diagnosis is overlapping of symptoms with other infections which makes clinicians taking their eyes off fungal infection and endangered patients especially immunosuppressed individuals (Sarah et al., 2024).
Protozoa and helminths are the causes of parasitic infections and their life cycles are usually complicated, and include multiple hosts or vectors. Malaria, schistosomiasis and amoebiasis diseases are still great health issues of the population in most regions across the globe. Figure 2 shows a typical lifecycle of Schistosoma. Diagnosis is traditionally based on the direct microscopic identification of parasites in blood, stool, or tissue, but rapid diagnostics and molecular tests are also becoming more common (Garcia,2020). Screening and diagnosis has been a challenge especially in developing countries due to lack of standardized techniques (Norman et al., 2020).
The length of time and progression of infection can also be used to classify infectious diseases. Acute infections are marked by a rapid onset and rather limited duration and may have a strong clinical manifestation, such as witnessed in influenza or cholera. Chronic infections on the other hand last through long periods of time and can either be asymptomatic or lead to progressive tissue damage as seen in tuberculosis, hepatitis B and HIV infection. It is known that acute or chronic infection determines the timing of diagnostics, the type of test, and the interpretation of the results (Brooks et al., 2022).
2.2. Principles of Diagnosis of Infectious Diseases
Infectious diseases diagnosis is a process that involves clinical suspicion first and laboratory investigation as the second stage. The clinical suspicion relies on the history of the patient, physical examination, epidemiological factors, and risk factors including travel history, immunological status, and exposure to infectious agents. Nevertheless, the clinical symptoms are not always enough to make a correct diagnosis because even in the case of various infectious diseases there are similar symptoms and laboratory tests are necessary (Miller & Binnicker, 2020).
The purpose of laboratory diagnosis is to identify the presence of the pathogen, its parts or immune response of a host to the infection. This can be either direct, e.g., visualization or detection of microbial nucleic acids and antigens, or indirect, e.g., antibodies. The type of diagnostic test selected is dependent on the suspected pathogen, stage of infection, the type of specimen and available resources. Effective diagnosis is essential because any error can lead to delayed treatment, inappropriate therapies, increased mortality, and the spread of infections (van Seventer and Hochberg, 2017).
Sensitivity and specificity are some of the core principles determining the choice of diagnostic tests and their interpretation. Sensitivity is the ability of a test to detect people with the disease and specificity is the ability to detect those without the disease. A high sensitivity test reduces a false-negative, which is especially significant when screening and establishing an early diagnosis, whereas a high specificity test reduces a false positive, which is essential when making a confirmatory diagnosis (Altman and Bland, 1994; Shreffler and Huecker, 2023). It is therefore, sensitivity and specificity are important indicators of test accuracy and efficiency, which allow healthcare providers to determine ideal diagnostic method to be employed (Shreffler and Huecker, 2023).
The predictive values also have an impact on clinical decision-making. Positive predictive value indicates the probability that a positive test result actually indicates infection whereas the negative predictive value indicates the probability that a negative result excludes the disease. Values depend on the disease prevalence among the population, and epidemiological context is a crucial part of diagnostic interpretation (Fletcher et al., 2019; Goldstein BA, Bedoya, 2020).
Another important principle in the diagnosis of infectious diseases is the turnaround time. The results of rapid diagnostics make it possible to start corresponding treatment in time, minimize unnecessary antimicrobial treatment, and enhance patient outcomes. Conventional culture-related processes tend to take days to weeks before giving results, but modern molecular and point-of-care techniques might give responses in hours or minutes, which is a significant change in the efficiency of the diagnosis (Banerjee et al., 2015).
2.3. Medical Microbiology in Diagnosis of Diseases
Medical microbiology plays a major role in diagnosis, treatment and prevention of infectious diseases. It is the science that links clinical medicine and laboratory science and converts detection of the microbial detection to clinical information of significance. Medical microbiologists perform the following roles: identification of pathogen, antimicrobial susceptibility testing, investigation of outbreak, and guidance in infection control (Murray et al., 2021).
The combination of microbiology and clinical medicine has gained more significance due to the increased complexity of diagnostic technologies. Careful communication between microbiology laboratories and clinicians will help in the proper selection of tests, proper interpretation of laboratory results, and proper management of patients. The given method of collaboration is especially essential in the case of severe infections like sepsis, when a prompt and accurate diagnosis can save lives (Liesenfeld et al., 2014).
Diagnostic microbiology laboratories have developed so much. The early laboratories were mainly microscopy and culture based, which were time-consuming in terms of manual labour, and in terms of incubation time. Modern laboratories have been altered with the development of automation, molecular diagnostics, and information technology, which enables them to be high-throughput diagnostic facilities that can handle large volumes of specimens with greater accuracy and efficiency (Clerc et al., 2016).
There are new tools in the modern medical microbiology laboratories like the Matrix-Assisted Laser Desorption Ionization Time-Of-Flight Mass Spectrometry (MALDI-TOF MS) which is used in the identification of organisms fast, the real time PCR used to detect pathogens, and the sequencing technology which is used in epidemiological surveillance (Calderaro, and Chezzi, 2024). The developments have reshaped the role of the microbiology lab as the confirmative service to a collaborative participant in clinical decision-making and the response to an outbreak or pandemic (Patel, 2020).
3. Traditional Diagnostic Methods in Infectious Diseases
Although these have come, the conventional microbiological techniques are still useful especially in antimicrobial susceptibility assays and the phenotypic characterization of pathogens. The future of medical microbiology is the moderate combination of old and new methods of diagnosis, which guarantee the accuracy, accessibility, and sustainability in various healthcare contexts.
3.1. Techniques Based on Microscopy
Microscopy-based methods can be considered as some of the first and most popular approaches to the diagnosis of infectious diseases. Light microscopy permits a direct visualisation of microorganisms in clinical samples like blood, sputum, urine, cerebrospinal as well as tissue samples. Microscopy is fortified by staining methods which enhance contrast and allow differentiation of structures of the microorganisms (Forbes et al., 2018).
The most widely used staining procedure in bacteriology is gram staining which categorizes bacteria as Gram-positive or Gram-negative depending on the differences in cell wall composition. This method gives a useful background of initial information about the morphology, structure, and cell wall of the bacterium, which can be used to administer initial antimicrobial care prior to receiving any culture information (Murray et al., 2021).
Ziehl Neelsen staining is specifically applied to the detection of acid-fast organisms specifically Mycobacterium tuberculosis. The lipid rich cell wall of the mycobacterial cell allows the use of the primary stain to be retained after acid-alcohol de-colouration. The methodology continues to be a fundamental part of diagnosis of tuberculosis, particularly in low-resource countries, yet it is not sensitive to tuberculosis infections with low bacterial load (WHO, 2022).
Giemsa staining in parasitology and haematology Giemsa staining is commonly used in haematology to detect blood parasites, including the Plasmodium species, Trypanosoma and Leishmania. It is also beneficial in detection of intracellular bacteria such as Chlamydia and Rickettsia. Nevertheless, this is a useful method but to interpret it correctly, qualified personnel and properly prepared smears are needed (Garcia, 2020).
Benefits of microscopy-based methods are fast turnaround period, low cost, and low levels of equipment needs. The techniques, however, have shortcomings of low sensitivity, especially in cases of low pathogen concentration or early infections. Also, microscopy is not always able to distinguish tightly related species and may require an additional confirmatory test (Brooks et al., 2022).
3.2. Culture-Based Methods
Culture-based practices include cultivation of microorganisms in unnatural media under regulated laboratory environments and have traditionally been regarded as the gold standard of identification of a large number of infectious diseases. Cultures of bacteria are done in solid and liquid culture media supporting microbial growth and making it possible to isolate, identify, and test the susceptibility to antimicrobials (Forbes et al., 2018).
The culture media used is different depending on the suspected pathogen. Simple media are helpful to support non-fastidious organisms, whereas enriched media, blood agar and chocolate agar, support the growth of more demanding bacteria. Selective and differential media also contribute to isolating certain pathogens in mixed flora by suppressing other organisms or signifying biochemical activities (Figure 4) (Murray et al., 2021).
Fungal cultures have specific media like Sabouraud dextrose agar and a lengthy incubation period is usually necessary because most fungi grow slowly. Viruses are more complicated, because they need a priori living cells to replicate, and are cultivated in cell lines, eggs with embryos, or animals in the laboratory. In spite of the fact that the viral culture has been almost replaced with molecular ones, it is still significant in terms of the research and testing of antiviral susceptibility (Knipe and Howley, 2020).
Culture-based methods have major limitations even though they are of diagnostic value. Numerous pathogens grow slowly thus resulting in long turnaround time and consequent delay in diagnosis and treatment. Other organisms are non-viable or fastidious and cannot easily be cultured under normal laboratory methodologies. Also, a history of prior antimicrobial therapy could suppress the growth of microbes leading to the false-negative culture outcomes (Banerjee et al., 2015).
3.3. Serological and Immunological Tests
Serological and immunological assays are used to identify antigens of the pathogen or antibodies in the host in reaction to the infection. These assays come in handy with organisms that are hard to culture or in cases where the organism is not directly detectable. Some of the most common serological methods are agglutination tests, enzyme-linked immunosorbent assay (ELISA), and complement fixation tests (Figure 5) (Fletcher et al., 2019).
Agglutination tests refer to the aggregation of particulate antigens in the presence of particular antibodies, and are normally applied in the quick detection of infections including typhoid fever and brucellosis. ELISA, in turn, is a very sensitive and specific test that is applied in the detection of antibodies or antigens in infections, including HIV, hepatitis B, and hepatitis C (Peeling et al., 2019).
The Complement fixation tests determine the amount of complement consumed during antigen-antibody reaction and used to be significant in the diagnosis of viral and atypical bacterial infections. Nevertheless, they are technically very demanding and have been mostly substituted by more sensitive immunoassays.
Serological tests are important in identifying the difference between acute and past infection. Immunoglobulin M (IgM) antibodies are usually detected in case of recent infection or in case of acute infection, and immunoglobulin G (IgG) antibodies would be detected when there is past exposure or immunity. However, serological diagnosis has a constraint of the window period, prior to the production of antibodies and possible cross-reactivity of antigens (Brooks et al., 2022).
3.4. Methods of Biochemical and Phenotypic Identification
Microorganisms can be characterized using biochemical and phenotypic identification methods that are based on metabolic and enzymatic characteristics. These are techniques that determine the capability of organisms to ferment carbohydrates, use substrates, or generate particular enzymes, including catalase, oxidase, and urease (Forbes et al., 2018).
Conventional biochemical assays are commonly done manually through tube or plate-based reactions and automated systems combine various biochemical reactions into standardized panels. These techniques have played a significant role in the normal clinical microbiology laboratories in the identification of bacterial pathogens and the differentiation of closely related species (Murray et al., 2021). Other phenotypic methods can be observed morphology of colonies, hemolytic patterns on blood agar, pigment production and morphology. Although these methods are reliable, it makes them time-consuming and inconclusive with atypical or slow-growing pathogens, they need viable organisms and adequate growth.
3.5. Traditional Diagnostics Problems
Although traditional diagnostic methods have been in use over a long time, they have various challenges that restrict their application in the contemporary clinical setting. Long turnaround time especially of culture-based and biochemical methods of identification is one of the most major constraints. The late outcomes may trigger the empirical treatment, incorrect use of antimicrobials, and the adverse patient outcomes (Banerjee et al., 2015).
Another significant obstacle is low sensitivity in the early infection since most of the traditional methods need a large amount of pathogen to be detected. This is particularly an issue with diseases like tuberculosis, sepsis and viral diseases in the incubation period. Further, a range of pathogens cannot be cultured or cultured with difficulty in artificial media, and thus culture-based diagnosis becomes ineffective (Clerc et al., 2016). These restrictions are directly associated with patient care as they slow down the right diagnosis, elevate the chances of disease spread, and add to antimicrobial resistance. This has led to the limitation of the traditional methods of diagnosis hence necessitating the invention and implementation of new modern diagnostic methods.
4. Drivers of the Paradigm Shift in Diagnostic Technologies
The shift to the advanced technologies in the diagnosis of the infectious diseases as a paradigm was not a solitary phenomenon, but a combination of biological, epidemiological, technological, and socio-economic factors has led to it. These drivers are a manifestation of the emerging complexity of infectious diseases and the escalating need to have fast, precise and scalable diagnostic solutions that can answer the global health problem. Another key driver for this shift is advancement in data science such as like data-driven analysis, big data that birthed predictive and modelling of diagnosis (Haug and Drazen, 2023)
4.1. Increasing Emergence of Novel and Re-Emerging Infectious Diseases
The rising cases of new and re-emerging infectious diseases are one of the major innovation motivators in diagnostic technologies. In recent decades, infectious agents like Ebola virus, Zika virus, Middle East respiratory syndrome coronavirus (MERS-CoV) and, most recently, SARS-CoV-2 have proven that infectious agents can bypass interspecies boundaries and propagate among populations of humans in a significantly shorter time. Long-erosion diseases like tuberculosis, cholera, and measles have also resurfaced in areas that they were previously under control, typically with stagnant or poor health systems, war, or falling vaccine attendance (Jones et al., 2008; Morens and Fauci, 2020).
Conventional diagnosed methodologies are usually inadequately prepared to identify recently occurring pathogens as they are critically dependent on previous information about microbial properties. In the modern world, however, the speed with which unknown pathogens are identified by molecular and genomic tools allows their detection and sequencing by nucleic acids even prior to the understanding of their biological properties. This ability has become crucial towards the timely detection and containment of outbreaks. The Antimicrobial Resistance Crisis refers to the rapid increase in the prevalence of drug-resistant microorganisms and strains that have developed resistance to antimalarial medications.
4.2. Antimicrobial Resistance Crisis
The Antimicrobial Resistance Crisis is the situation of the increased rate of the prevalence of drug-resistant microorganisms and strains that acquired the resistance to antimalarial drugs.
The antimicrobial resistance (AMR) crisis has dramatically increased the transition to sophisticated diagnostic systems in the world. Abuse and overuse of antimicrobial agents have resulted in the development of multidrug-resistant microorganisms, including carbapenem-resistant Enterobacterales, methicillin-resistant Staphylococcus aureus and extensively drug-resistant Mycobacterium tuberculosis. Such resistant pathogens make treatment more difficult, increase mortality, longer hospitalization, and increased healthcare expenses (O’Neill, 2016; Tacconelli et al., 2018).
The use of targeted antimicrobial therapy and decreasing the use of broad-spectrum antibiotics requires accurate and fast diagnostics to ensure that these drugs are used in the most effective way possible. The culture-based susceptibility testing is slow; it usually takes several days before the test results are obtained. Conversely, the resistance genes and mutations can be quickly identified using molecular diagnostics and thus antimicrobial therapy can be optimized earlier and even antimicrobial stewardship programs supported.
4.3. Internationalization and Fast Disease Transmission
Globalization has changed epidemiology of infectious diseases because it has raised human countries mobility, trade and cross-country interaction. International travel, urbanization and global supply chains contribute to the rapid transmission of the pathogens and the local outbreaks can turn into global health emergencies in a relatively short time. The COVID-19 pandemic is one of the examples of how fast infectious diseases can be spread in the world that is highly interconnected (Tatem, 2017).
The high rate of disease transmission presents a giant burden on the diagnostic processes to provide high-quality and timely results at large scale. The demands of large populations in instances of outbreaks are usually not addressed with centralized laboratory testing using traditional methods. As a result, decentralized and high-throughput diagnostic technologies that can be used to support surveillance and real-time decision-making have increasingly been in focus.
4.4. Rapid Point-of-Care Diagnostic Need
Diagnostic innovation in the emergency care setting, remote setting, and the low-resource environment has become a pressing demand due to the necessity of point-of-care diagnostics. POCTs are diagnostic tests that are conducted close to the patient instead of the expensive laboratory infrastructures, and they take less time. It is particularly essential in cases where timely clinical response is needed (sepsis, malaria, and acute respiratory infections) (Drain et al., 2014).
Conventional diagnostics usually involves the use of transport of the specimen, specific devices, and qualified lab staff, which results in delays, which may also have a negative impact on the patient results. Rapid POCTs enhance the clinical decision-making process, allow early detection of the disease and its treatment, and improves disease surveillance in the community. The effectiveness of rapid antigen and molecular tests in the COVID-19 pandemic was another indication of the disruptive power of point-of-care diagnostics.
4.5. Technological Innovations in Molecular Biology and Bioinformatics
The technological basis of the paradigm shift in the diagnosis of infectious diseases has been given by the creation of molecular biology and bioinformatics. The development of innovations like polymerase chain reaction, next-generation sequencing, microfluidics and CRISPR-based detection systems have transformed the process of detecting and characterizing pathogens. These technologies may be high sensitivity, multiplexed, and complete microbial genome (Goodwin et al., 2016).
Bioinformatics has also increased diagnostic opportunities since big amounts of genetic data can be analyzed and interpreted. Diagnostic is now a data-oriented field with the aid of computational tools that facilitate the identification of pathogens, their resistance profiles, and even outbreak tracking. Diagnostic microbiology has therefore taken a new dimension with the combination of molecular biology with bioinformatics, shifting its knowledge on organism detection to precision diagnostics and predictive public health (Didelot et al., 2012).
5. Molecular Diagnostic Technologies
Molecular diagnostics identify one of the most revolutionary developments in infectious disease diagnosis in the last several decades. Molecular techniques are used to identify pathogens in contrast to traditional methods in which the pathogen is identified by its culture or phenotypic characteristics. The resulting sensitivity, specificity, and speed are unprecedented, and is now critical in the fields of clinical microbiology, response to outbreaks, and monitoring of antimicrobial resistance. In both hospital and population health laboratories, molecular diagnostics have become more and more a replacement of conventional methods or a supplement to them.
5.1. Polymerase Chain Reaction (PCR) and Its Variants
One of the most significant areas of impact on molecular diagnosis is Polymerase Chain Reaction (PCR) that was invented in the 1980s. PCR allows amplifying the specific sequences of nucleic acids exponentially, and even the smallest traces of pathogen DNA or RNA can be identified with accuracy (Dieffenbach & Dveksler, 2020). The classic PCR was the foundation of more specialized versions such as real time PCR and multiplex PCR which have increased clinical applications (Figure 6).
The traditional process of PCR works under the principle of repeated changes in temperature through which the process of denaturing DNA, annealing of primers, and lengthening of new DNA strands are facilitated. Gel electrophoresis is then used to visualize the resulting amplified products. Although conventional PCR was better than culture and microscopy in sensitivity, it has a limitation of more lengthy processing times and techniques that require handling of the amplification product after its production, thus increasing the risk of contamination (Kralik and Ricchi, 2017).
Figure 6.
Basic workflow of conventional polymerase chain reaction (PCR) amplification. (Adapted from Dieffenbach & Dveksler, 2020).
Figure 6.
Basic workflow of conventional polymerase chain reaction (PCR) amplification. (Adapted from Dieffenbach & Dveksler, 2020).
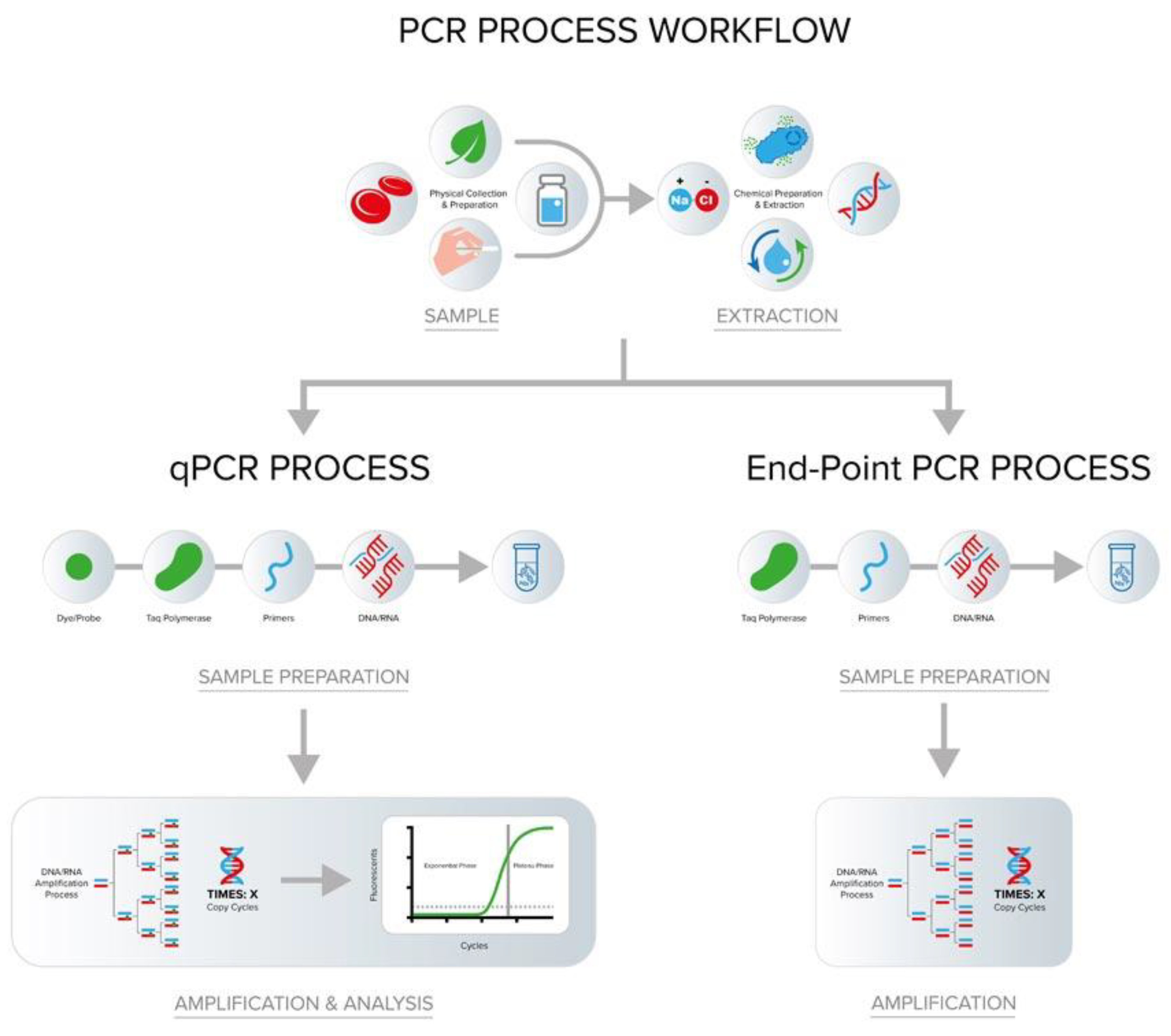
To address these shortcomings, real time PCR (qPCR) incorporates fluorescent probes or dyes that will produce signals which are proportional to the quantity of the amplified DNA at each PCR step. This enables the real time quantification of pathogen load without gel electrophoresis. The use of real time PCR has also turned into the gold standard in the diagnosis of numerous infectious viruses such as influenza, HIV, hepatitis, and SARS CoV 2 because of its turnaround time and the capacity to quantify (Bustin et al., 2020). Quantification nature of qPCR does not only show presence of pathogen, but can also be used to trace the progression and response to treatment of diseases.
Multiplex PCR also improves diagnostic information by enabling a multi-target amplification in one reaction. This comes in especially handy in testing of infectious syndromes of varying etiologic agents, including respiratory infections or sepsis. Multiplex assays save the necessity of conducting many separate tests, save the cost of the reagents, and save clinical samples (Elnifro et al., 2020). Multiplex panels that were originally in commercial use in clinical laboratories are now popular to identify and detect a combination of bacteria, virus, and parasites in a single run on a commercial multiplex panel, and this has greatly enhanced the efficiency of the diagnostic tool.
Although the sensitivity and specificity of PCR based diagnostics are high, it means that it requires specific thermal cycling tools and a sensitive assay design. However, their use has grown fast through automation, an integration of laboratory information systems, and solid evidence on improved clinical outcomes (Mahony et al., 2018).
5.2. Isothermal Amplification Techniques
PCR has transformed the field of molecular diagnostics but its limitation lies on the fact that it requires thermal cycling machines which makes it impractical in resource-based environment or in point of care device. On the other hand, isothermal amplification methods, which are used to produce the nucleic acid amplification at fixed temperatures, thus, avoiding the use of complicated thermocyclers.
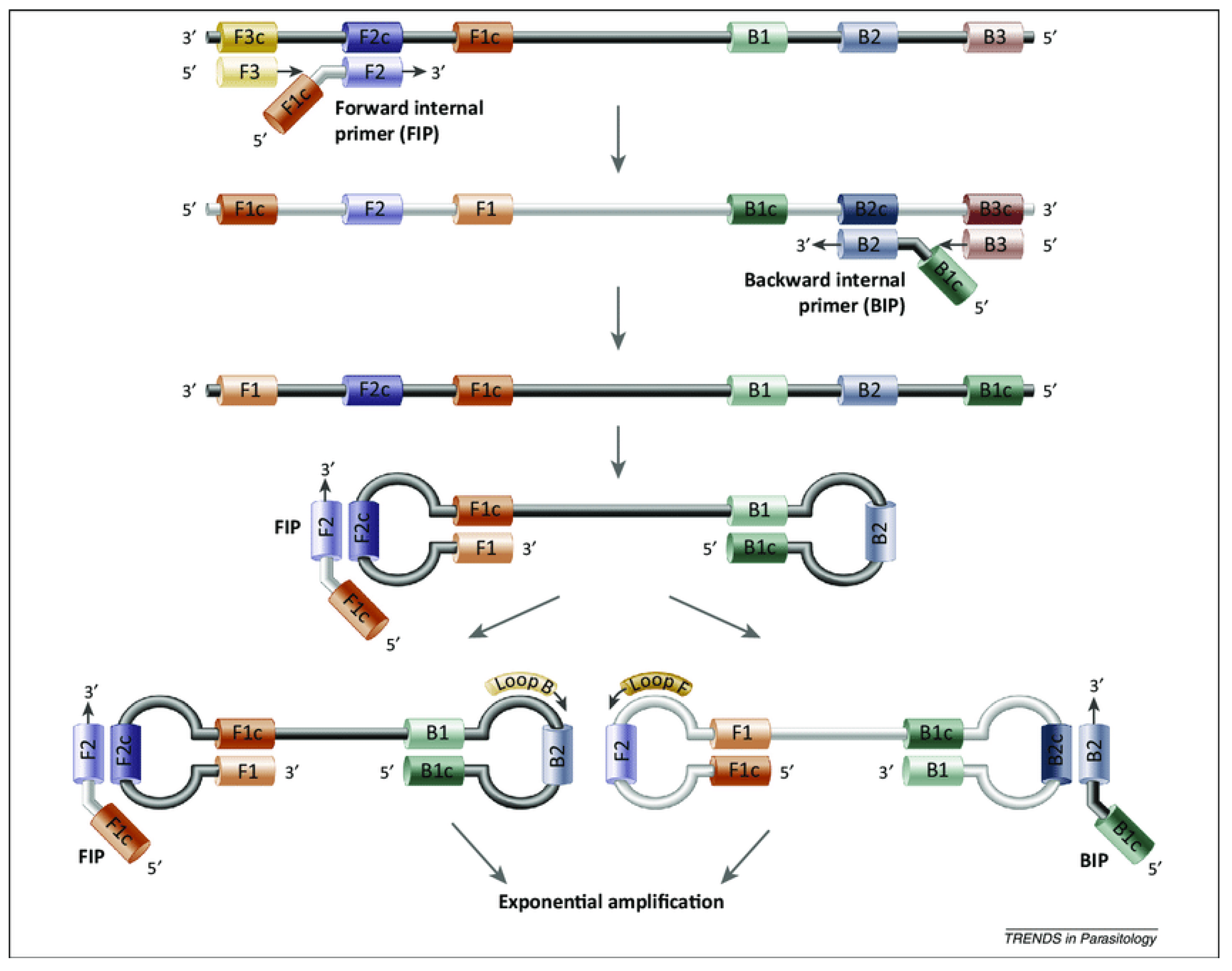
The most popular of these methods is loop mediated isothermal amplification (LAMP). LAMP combines a specially constructed four or six primers along with a strand that replaces the DNA polymerase in order to amplify the targets at a constant temperature (normally 6065 o C). This leads to a rapid amplification - commonly in 30 min - and visual detection by turbidity or fluorescence, which makes it applicable in a field environment. The LAMP has been utilized in diagnosis of malaria, tuberculosis, and COVID 19 with equivalent sensitivity to PCR without the use of advanced equipment (Figure 6) (Notomi et al., 2015; Parida et al., 2020).
Figure 6.
Mechanism of loop-mediated isothermal amplification (LAMP). (Adapted from Notomi et al., 2000).
Figure 6.
Mechanism of loop-mediated isothermal amplification (LAMP). (Adapted from Notomi et al., 2000).
Another isothermal procedure is recombinase polymerase amplification (RPA) which can run at even lower temperatures (37-42℃). RPA uses recombinase enzymes that help in binding the primer and exchange of strands, which leads to the high amplification of the DNA in just 15 minutes. Its low temperature allows RPA to be used with simple battery powered devices and lateral flow readouts, and it expands its use to point of care diagnostics in outbreak areas or communities with limited resources (Lobato and O'Sullivan, 2018). RPA has exhibited high diagnostic capabilities against pathogens including Zika virus, dengue virus and methicillin resistant Staphylococcus aureus (Wang et al., 2019).
Isothermal techniques have difficulties in standardizing assays and multiplexing relative to PCR despite their promise. Nevertheless, they are extremely appealing due to their simplicity and speed and further integration with microfluidics, mobile detection systems, and new sensor interfaces is increasing their application worldwide.
5.3. Nucleic Acid Sequencing Technologies
Due to the advent of nucleic acid sequencing technologies, diagnostics of infectious diseases has reached a new level of understanding with the opportunity to characterize the genomes of the pathogens in detail. Sequencing does not only identify organisms but also provides the changes in genetics, antimicrobial resistance determinants and evolutionary relations.
The initial and widely used technique is Sanger sequencing which is still useful in verifying specific sequences of pathogens, PCR product validation, and specific genetic analysis. Sanger sequencing is less popular due to its limited throughput and expensive per sample cost, but it is still applied in the confirmation of organism and small scale studies (Figure 7) (Metzker, 2018).
The most important development in sequencing is the next generation sequencing (NGS) technologies. NGS systems can sequester millions of DNA fragments at once, making it possible to sequence the entire genome (WGS) of a pathogen, replicate metagenomic studies of complex samples, and identify co infections. Application NGS in clinical practice is in the investigation of outbreaks, monitoring of antimicrobial resistance, and detection of new and unexpected pathogens (Hommelsheim et al., 2019).
Metagenomic sequencing is a type of NGS that permits unbiased sequencing of all of the nucleic acids found in a clinical specimen without prior knowledge of the target organism. It is especially useful to diagnose infections that have an unknown etiology, rare pathogenesis, or highly variable genomes with its feature. Metagenomics has been instrumental in the discovery of new viruses, the description of the diversity of pathogenes in environmental samples, and tracking microbiome changes related to disease (Wilson et al., 2019).
5.4. Benefits of Molecular Diagnostics compared to other Methodologies
Molecular diagnostics in comparison to the traditional methods has one of the key advantages based on their speed, with the accuracy and sensitivity. The methods used, like qPCR, can provide a result in hours instead of taking days or weeks, allowing clinicians to start target therapy earlier and minimizing unnecessary antimicrobial use. A fast turnaround time also increases the flow of patients to the hospitals and the infection prevention practices (Gwinn et al., 2019).
Molecular diagnostics also have a high sensitivity whereby low abundance pathogens may be detected by the traditional methods. This is especially so in the case of viruses and fastidious organisms that are hard or impossible to grow. Also, the molecular platforms are able to differentiate close species and strains, leading to accurate diagnosis and relevant response in the field of public health (Tang et al., 2021).
The possibility of identifying non culturable organisms with the help of the molecular tools is another significant benefit. Other pathogens go into a dormant state or have special conditions that cannot be easily reproduced in vitro making normal culture ineffective. Molecular technologies defy these drawbacks by identifying genetic material directly and cannot be substituted in diagnosing modern infectious diseases.
6. Techniques of Diagnostic Technology
With the ongoing development of infectious disease diagnostics, there has been an introduction of a number of cutting-edge technologies that far increase the possibilities of molecular diagnostics. These would be mass spectrometry, CRISPR based systems, biosensors with nanotechnology improvements, and platforms of point of care testing. They collectively signify a change to more rapid, sensitive, and very accessible tools of diagnosis that can revolutionize clinical microbiology and population health monitoring.
6.1. Mass Spectrometry in Microbial Identification
Mass spectrometry involves the use of a mass spectrometer to analyse a protein sample and then compare the results with they have in the database to identify the identity of the protein being analysed. The method of mass spectrometry in microbial identification: Mass spectrometry is a method that uses a mass spectrometer to analyse a protein sample and then compares the results obtained with those they hold in the database, to determine the identity of the protein under analysis.
Mass spectrometry (MS) has transformed the method of identification of microbes because it allows the rapid and accurate analysis of complex biological samples. The most used of the MS technologies is the matrix assisted laser desorption/ionization time of flight mass spectrometry (MALDI TOF MS) because it is rapid, reliable and economical. The MALDI TOF MS is based on the principle of ionizing proteins in a microbial sample and assessing their mass to charge ratio to produce unique spectral fingerprints that can be compared to reference databases to identify a species (Seng et al., 2018).
In comparison to other traditional biochemical identification techniques that can take days, MALDI TOF MS can provide results in a few minutes, thus MALDI TOF MS can be useful particularly in routine identification of bacteria, yeasts and certain filamentous fungi. High throughput and low sample preparation have diminished the laboratory workload and enhanced the diagnostic turnaround time by a vast margin (Croxatto et al., 2021).
Besides the species identification, MALDI TOF MS is finding more and more applications in the detection of biomarkers relating to antimicrobial resistance and strain typing. New uses comprise combining MS with machine learning to forecast phenotypes like the production of beta lactamase or virulence factors, which improves clinical decision making (Demirev & Feldman, 2019).
6.2. CRISPR Based Diagnostic Platforms
The identification of CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats) systems which have been initially discovered to be used in gene editing has created a new diagnostic innovativeness. CRISPR based diagnostics Capitalize on the specific nucleic acid binding properties of CRISPR associated (Cas) enzymes to identify pathogens with high specificity and sensitivity. The potential is represented by two notable platforms, namely SHERLOCK (Specific High Sensitivity Enzyme Reporter UnLOCKing) and DETECTR (DNA Endonuclease Targeted CRISPR Trans Reporter) (Gootenberg et al., 2018).
SHERLOCK involves Cas13 enzymes that when they pass through the target RNA sequences, they trigger collateral cleavage of labelled reporter molecules, which produce a signal. DETECTR applies Cas12 enzymes towards analogous detection of DNA targets. The two platforms can be adjusted to fluorescent or lateral flow readouts and hence they can be used in a rapid or point of care diagnostics.
The list of pathogens that have been detected using these CRISPR based approaches is quite broad, which includes SARS CoV 2, Zika virus, and human papillomavirus (HPV). Their sensitivity, reaching the levels of qPCR, and low equipment needs have made CRISPR diagnostics a promising technology to be used to decentralize and field based testing, especially during outbreaks or in resource constrained areas (Figure 8) (Li et al., 2021).
Nevertheless, there are still some difficulties related to large-scale implementation of these platforms into clinical practices, including standardization of reagents, incorporation of sample preparation, and improved functionality with a wide variety of specimen types. The current studies are trying to overcome these shortcomings and to bring CRISPR diagnostics to the point of universal use.
6.3. Biosensors and Nanotechnology Based Diagnostics
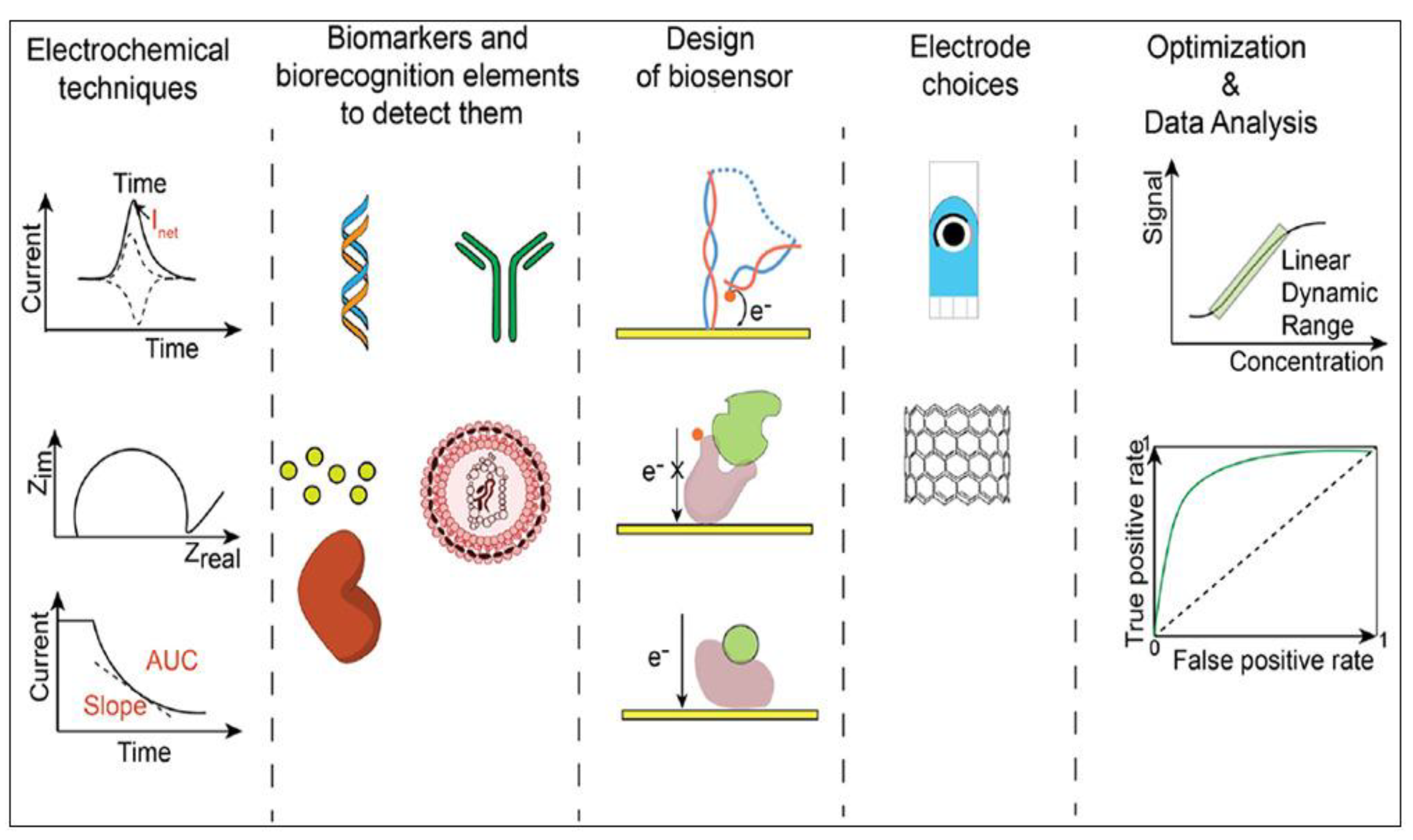
Biosensors are analytic systems which translate the interactions of the biology and this integration has become an intrinsic part of the modern infectious disease diagnosis. These sensors usually integrate biological recognition components e.g. antibodies, nucleic acids or enzymes with transducers that produce electrical, optical, or electrochemical signals when pathogens are detected. Integrated with nanotechnology, biosensors have a high sensitivity, miniaturization, and response time (Figure 9) (Suh et al., 2019).
Electrochemical biosensors are used to detect alterations in electrical signals that are generated as a result of binding between a target pathogen and a recognition probe. The benefits they have are that they are highly sensitive, low in cost and can be used in combination with portable devices which makes them suitable in point of care diagnostics. They are designed as bacterial toxins, viral antigen, and nucleic acid sensors, which may find environmental and clinical uses (Lazcka et al., 2018).
Optical biosensors, however, are based on the light property change, i.e., fluorescence, absorbance, or the surface plasmon resonance, to indicate the target presence. The optical biosensors can be improved by using nanostructured materials such as gold nanoparticles and quantum dots because these materials possess special physical characteristics. As an example, localized surface plasmon resonance (LSPR) sensors are able to use metallic nanoparticles to enhance local signal in the event that the pathogen attaches to the sensor surface, which can be used to detect with ultra sensitivity (Rosi & Mirkin, 2020).
6.4. Point of Care Testing (POCT)
The term point of care testing (POCT) is used to describe diagnostic tests conducted in or around the location of patient care and that generate prompt clinical information. In contrast to the traditional laboratory testing where it can be centralized and may take long before the results are delivered, POCT provides results within minutes or hours, minimizes delays in treatment and enhances clinical outcomes (Drain et al., 2019).
One of the most commonly known POCT technologies are lateral flow assays LFAs. These paper-based tests employ the interaction of antibody and antigen to produce visible lines on a test strip which is an indication of a pathogen or antigen. The best-known example is pregnancy tests, although LFAs have also been created against infectious agents (influenza, HIV, hepatitis, and SARS CoV 2). They are important assets of a decentralized healthcare setup due to their simplicity, low cost and minimal training needed.
Another type of POCT is rapid antigen detection tests (RADTs); it is a diagnostic method that identifies pathogen specific proteins in a clinical sample. The RADTs have been extensively utilized in the epoch of the COVID 19 pandemic to detect those who were infected promptly, in particular, in community screening and control of the outbreak. Antigen tests may be less sensitive than molecular tests, but they have a shorter turnaround time and a more convenient way of use to improve the disease control plan, especially in cases where quick isolation and treatment choices are essential.
POCT has a transformative effect on the healthcare landscape of the decentralized setting. POCT in rural clinics, emergency departments, and resource constrained areas empowers the frontline professional to have actionable information that direct clinical practice, lessen the number of unnecessary antibiotic prescriptions, and enhance patient satisfaction (Peeling & Olliaro, 2021). The possibility of integrating POCT with digital health applications and telemedicine also expands the scope of it because of remote diagnosis and monitoring.
7. Diagnostic powered by Digital and Artificial Intelligence
Bioinformatics is the study that involves the use of computer tools to process very large biological data, including genetic sequences, protein structures and epidemiological information. Bioinformatics now plays a fundamental role in the interpretation of complex results of high throughput technologies in modern infectious disease diagnostics e.g. next generation sequencing (NGS), microarrays, and metagenomics. Such methods produce huge volumes of genomic data, which cannot be computed and interpreted without dedicated computational models (Quainoo et al., 2017; Didelot et al., 2022).
Bioinformatics pipelines are used in pathogen profiling to align the reads of a sequencing project to reference genomes, detect mutations, and identify the types of strains. Whole genome sequencing of Mycobacterium tuberculosis can be used as an example of investigating resistance inducing mutations and transmission in epidemics of tuberculosis, and offers more practical information than traditional phenotypic tests of susceptibility (Meehan et al., 2019). In a similar manner, the uncommon or unexpected pathogens can be identified in the cerebrospinal fluid or respiratory samples, which can be detected using a metagenomic analysis without any prior assumptions to allow a diagnosis to be made in complicated or unusual clinical presentations.
Bioinformatics also allows combining different types of data genomic, proteomic, and clinical to create a holistic profile of diagnosis. Machine learning algorithms are able to reveal the trends and connections in such multi-dimensional datasets, which are not possible to investigate with human power. Bioinformatics in such context becomes more than the tool of analysing data, it turns into the tool of decision support that contributes to better diagnostic accuracy and more personalized approach to managing specific infectious diseases (Libbrecht and Noble, 2015).
Machine learning (ML) and artificial intelligence (AI) can be considered subfields of computational science that allow computers to learn and to predict or make decisions with little human involvement. AI and ML are being deployed in the field of infectious disease diagnostics in a variety of tasks, ranging from image analysis to predictive modelling of epidemics.
Automated image analysis is one of the most powerful and old uses of AI. Combined with deep learning algorithms, digital microscopes are capable of detecting microorganisms in blood smears, stool samples or histopathology slides rapidly and with high accuracy. In diseases such as malaria, tuberculosis, and sepsis, in which the microscopic morphology is the most critical aspect of diagnostics, AI aided image analysis minimizes human error and increases speed (Barbosa et al., 2020). Indicatively, convolutional neural networks (CNNs) have been trained to find malaria parasites on Giemsa-stained slides as sensitive and specific as expert microscopists.
Outside of laboratory automation, AI is also used to aid in predictive diagnostics and outbreak monitoring. Temporal and spatial trends in clinical, environmental, and mobility data can be examined by machine learning methods to predict disease occurrence and detect new hotspots. The case increase, estimation of reproductive number (R0), and evaluation of the effects of public health interventions were also predicted in the COVID 19 pandemic using AI models (Chakraborty and Ghosh, 2020). Likewise, AI-driven tools such as HealthMap and BlueDot are used to analyze global news, social media, and clinical reports to identify disease outbreak warning signs before their official reporting.
Digital health technologies refer to electronic systems which facilitate collection, analysis and dissemination of health information. Of them, there are telemedicine, electronic health records (EHRs), and lab information systems (LIS) that have become vital elements of infectious disease diagnostics and patient control.
Telemedicine has tremendously increased the availability of diagnostic care especially in underserved areas. Telemedicine allows patients to be evaluated at an initial stage without the need to travel to a doctor through video consultation and remote measurements, as well as digital symptoms tracking. Telehealth can also be used together with point of care diagnostic devices which enable clinicians to direct testing and visualize results remotely to minimize delays in diagnostic and treatment. As an example, in rural regions where there is a lack of laboratory facilities, clinicians can oversee the use of rapid antigen or molecular tests through teleconferencing, so they can be sure of proper collection of samples and interpretation of results.
Laboratory Information Systems (LIS) and EHRs facilitate the process of diagnoses by incorporating several types of data - laboratory instruments, clinical notes, imaging data, and public health registries. These systems enhance the accessibility of data, lessen the transcription errors, and facilitate real time reporting of the cases of infectious diseases. In case of an outbreak, it is easy to use LIS and public health dashboards in real time, which allows tracking cases and contacts, as well as allocating resources quickly (Kharrazi et al., 2018).
8. Clinical Implications and Public Health
The shift in paradigm of the traditional to the modern diagnostic technologies has serious implications in clinical practice and the public health. The development of molecular diagnostics, mass spectrometry, CRISPR-based biomarker detection systems, and digital health systems, among other things, has redefined how infectious diseases are detected, monitored, and treated. These technologies are adopted to improve patient outcomes, improve outbreak preparedness, aid antimicrobial stewardship, and empower health systems in general.
8.1. Better Management and Treatment Results in Patients
Effective patient management is based on speedy and correct diagnosis. Any delay or inaccuracy in the identification of infectious agents has been known to result in improper therapy, prolonging of the disease, and complications. The diagnostics of the modern era, especially molecular tests and point-of-care testing, offer clinicians prompt and accurate identification of pathogens and an opportunity to apply targeted treatment options instead of empirical broad-spectrum therapy (Tang et al., 2021).
As an illustration, respiratory disease cases like influenza virus and COVID-19 can be treated by real-time PCR and rapid antigen testing, allowing a prompt antiviral response or isolation, which minimizes the severity of the disease and limits its transmission (Drain et al., 2019). Equally, the laboratory diagnosis of bacterial pathogens using MALDI-TOF MS has also reduced the time to the right antibiotic treatment in bloodborne infections and has a direct effect on the survival rate of patients (Croxatto et al., 2021).
In addition, proper characterization of the pathogen can be used to stratify the patients according to risk and make individual therapeutic choices. As a case in point, co-infections or antimicrobial-resistant strains can be identified through metagenomic sequencing, which can be used to select a specific treatment plan that will cause the least side effects and superb outcomes (Wilson et al., 2019). These possibilities help to promote better clinical performance, decreased hospitalization, and lowered medical expenses, especially in tertiary care facilities.
8.2. Early Detection and Surveillance of Outbreaks
The diagnostic technologies that are used nowadays are essential to diagnose the outbreak of infectious diseases in the early stages so that the public health can respond to it. The traditional approaches tend to be slow to detect an outbreak either because of the long turnaround time or low sensitivity. Molecular diagnostics, CRISPR-based systems, and digital health tools, on the contrary, can offer near real-time surveillance information (Gootenberg et al., 2018; Peeling & Olliaro, 2021).
High-throughput sequencing and metagenomics is able to identify new or re-evolving pathogens even in asymptomatic cases or the environment. Early detection aids in timely isolation and contact tracing and containment to reduce morbidity, mortality, and socioeconomic disturbance in case of outbreaks (Didelot et al., 2022).
The epidemiological tracking and predictive modelling is supported by integrating diagnostic outputs with bioinformatics pipelines and laboratory information systems (LIS). It can be used to create new hotspots and forecast disease transmission with the help of artificial intelligence and machine learning tools that use the data on demographics, environment, and mobility (Chakraborty and Ghosh, 2020). These online surveillance tools are critical in pandemic preparedness as evidenced in the COVID-19 pandemic where quick diagnostics made possible early detection of cases and guided the formulation of effective public health plans across the world.
8.3. Antimicrobial Stewardship
AMR is an increasing global health issue, and part of it is triggered by improper or prompt treatment of infections. Antimicrobial stewardship is facilitated by modern diagnostic tools that guarantee the provision of evidence-based fast decisions. The application of molecular diagnostics and/or MALDI-TOF MS, or sequencing can enable timely detection of causative pathogens and resistance genes and enable clinicians to prescribe specific antibiotics, thereby preventing the use of broad-spectrum antibiotics, which increase resistance in their use (Hassoun et al., 2019).
As an example, Gram-negative bacteria can be identified as having beta-lactamase genes in real-time PCR assays and, thus, directed to the appropriate antibiotic at the time. Timely de-escalation of therapy is also enabled by point-of-care testing and rapid susceptibility assays to prevent the needless exposure of patients to drugs and to reduce adverse events (Mahony et al., 2018).
These technologies positively impact the policy of infection control in hospitals, minimise the effects of multidrug-resistant organisms spread, and eventually patient safety by offering actionable information on the identity of pathogens and their resistance profiles. Resistant strains of microorganisms in combinations with digital health methods will enable the observation of prescription and resistance rates in real-time, which will support sustainable clinical usage in both low and high-resource environments.
8.4. Health Systems Strengthening
In addition to the treatment of the individual patient, adoption of sophisticated diagnostic tools reinforces the larger health systems. Quick and precise diagnostics enhance the capacity of laboratories, standardized workflow, and use of data in making decisions at various levels of care (Quainoo et al., 2017).
Diagnostic differentiation and blending with digital health platforms, electronic health records, and telemedicine promote access to healthcare, especially in poor and remote areas. The technologies allow decentralization of testing, decrease the travel and waiting of patients, and enable community health workers to be actively involved in the process of disease surveillance (Drain et al., 2019).
Moreover, highly developed diagnostics offers data in essence vital in resource allocation, planning, and policy development. Real-time epidemiological trends can help governments and health organizations to prioritize interventions so that health systems are more efficient and resilient. The preparedness of emergencies through investment in diagnostic infrastructure also guarantees that health systems would react to outbreaks and emerging pathogens efficiently (Didelot et al., 2022).
9. Conclusions
The diagnostic panorama of the infectious disease has been radically changed and shifted to the use of advanced molecular, digital, and point-of-care tools and technologies, as opposed to traditional methods of microscopy, culture, and serology. This paradigm shift can be traced back to the increase in the requirements of a fast, precise, and effective diagnostic data in clinical and population health scenarios. Although less modern and more accessible, traditional methods are being increasingly complemented or replaced by more sensitive, specific, and faster turnaround diagnostics, which eventually lead to patient outcomes and guide timely and important actions to the population regarding their health.
The importance of such technological development in diagnostics cannot be overestimated. Contemporary methods, such as polymerase chain reaction (PCR), next-generation sequencing, mass spectrometry, CRISPR-based system and artificial intelligence-based systems, have widened the capability to identify and characterize infectious agents more precisely than ever before. The developments will support the detection of outbreaks early, the strengthening of antimicrobial stewardship, and the delivery of important information to the epidemiological surveillance and health system strengthening. Specifically, point-of-care and mobile molecular systems have enhanced the accessibility of diagnostics in remote and resource-deprived areas, closing the divide between health equity in the world and improving pandemic preparedness.
Although these achievements have been made, the shift in the contemporary diagnostics does not downplay the significance of the traditional methods. Culture and microscopy are also indispensable in numerous situations, particularly in the situation where they need a molecular or high-tech solution, which is not feasible because of high cost, lack of infrastructure or workforce. However, it is necessary in the case of the traditional and modern ways of diagnosing to achieve a balanced integration such that the advantages of both can be used to enhance the accuracy of diagnostic results, timeliness, and clinical relevance. This kind of integration would also make sure that low- and middle-income nations can gain the advantages of technological advances and at the same time do not lose the effectiveness and quality of traditional approaches.
10. Future Direction
Advancement of technology has come to stay and getting better in all aspects. Therefore, in the future, integration of technologies in diagnostic procedures would help in early detection of pathogens, positive treatment outcome and rapid transformation global health practices. Employing AI and ML will have speed and accuracy tendencies and handling large data within short time. With recent technologies, diagnosis and treatment can be personalized with techniques such as Biosensor and innovation of portable and cost-effective diagnostic systems, such as CRISPR-based platforms, will facilitate field diagnostics and outbreak monitoring. While shift from old convention diagnosis to new technology is advocated, there is the need for policy solutions to integrate molecular diagnostics into low- and middle-income countries, including portable devices, simplified workflows, and targeted training programs.
Author Contributions
Conceptualization, G.H.M and A.M.; validation, D.H.; resources, M.A.Z.; writing—original draft preparation, G.H.M, and B.A.; writing—review and editing, O.A.A and M.T.S.; supervision, A.M. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
All sources of figure are acknowledged and referenced.
References
- Alsharksi, A.N.; Sirekbasan, S.; Gürkök-Tan, T.; Mustapha, A. From Tradition to Innovation: Diverse Molecular Techniques in the Fight Against Infectious Diseases. Diagnostics 2024, 14, 2876. [Google Scholar] [CrossRef]
- Altman, D. G.; Bland, J. M. Diagnostic tests 1: Sensitivity and specificity. BMJ 1994, 308(6943), 1552. [Google Scholar] [CrossRef]
- Banerjee, R.; Teng, C. B.; Cunningham, S. A.; Ihaddadene, R.; Steckelberg, J. M.; Patel, R.; Binnicker, M. J. Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification. Clinical Infectious Diseases 2015, 61(7), 1071–1080. [Google Scholar] [CrossRef]
- Barbosa, D. J.; Esteva, A.; Chouhan, S.; Ryan, J. K.; Kalpathy-Cramer, J.; Halpern, A. Deep learning for automated microscopy in infectious diseases. Journal of Clinical Microbiology 2020, 58(5), e01814-19. [Google Scholar] [CrossRef]
- Brooks, G. F.; Carroll, K. C.; Butel, J. S.; Morse, S. A.; Mietzner, T. A. Jawetz, Melnick & Adelberg’s medical microbiology, 30th ed.; McGraw-Hill Education, 2022. [Google Scholar]
- Bustin, S. A.; Benes, V.; Garson, J. A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M. W.; Shipley, G. L.; Vandesompele, J.; Wittwer, C. T. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clinical Chemistry 2020, 66(8), 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Calderaro, A.; Chezzi, C. MALDI-TOF MS: A Reliable Tool in the Real Life of the Clinical Microbiology Laboratory. Microorganisms 2024, 12(2), 322. [Google Scholar] [CrossRef] [PubMed]
- Carter, Linda J.; Garner, Linda V.; Smoot, Jeffrey W.; Li, Yingzhu; Zhou, Qiongqiong; Saveson, Catherine J.; Sasso, Janet M.; Gregg, Anne C.; Soares, Divya J.; Beskid, Tiffany R.; Jervey, Susan R.; Liu, Cynthia. Assay techniques and test development for COVID-19 diagnosis. ACS Central Science 2020, 6(5), 591–605. [Google Scholar] [CrossRef]
- Chakraborty, Tanmoy; Ghosh, Indrajit. AI and predictive modeling during COVID-19. Computers in Biology and Medicine 121 2020, 103763. [Google Scholar] [CrossRef]
- Clerc, Olivier; Prod’hom, Gregory; Greub, Gilbert. Impact of MALDI-TOF MS on clinical microbiology. Clinical Microbiology and Infection 2016, 22(7), 574–579. [Google Scholar] [CrossRef]
- Demirev, Plamen A.; Feldman, Alexander B. Mass spectrometry for rapid microbial identification. Annual Review of Analytical Chemistry 12 2019, 101–124. [Google Scholar] [CrossRef]
- Didelot, Xavier; Bowden, Richard; Wilson, Daniel J.; Peto, Tim E.; Crook, Derrick W. Transforming clinical microbiology with bacterial genome sequencing. Nature Reviews Genetics 2012, 13(9), 601–612. [Google Scholar] [CrossRef]
- Didelot, Xavier; Gardy, Jennifer; Colijn, Caroline. Genomic and bioinformatic integration in infectious disease diagnostics. Nature Reviews Microbiology 2022, 20(8), 481–498. [Google Scholar] [CrossRef]
- Drain, Paul K.; Garrett, Nicholas; Fortunato, Christopher; Groszmann, Mitchell. Point-of-care diagnostics in primary healthcare. The Lancet Global Health 2019, 7(7), e928–e938. [Google Scholar] [CrossRef]
- Drain, Paul K.; Hyle, Elizabeth P.; Noubary, Faysal; Freedberg, Kenneth A.; Wilson, Deborah; Bishai, William R.; Rodriguez, Waldo; Dheda, Keertan. Point-of-care diagnostics for infectious diseases: Opportunities, barriers, and implementation. The Lancet Infectious Diseases 2014, 14(4), 239–251. [Google Scholar] [CrossRef]
- Fletcher, Ralph H.; Fletcher, Suzanne W.; Fletcher, Grant S. Clinical epidemiology: The essentials, 6th ed.; Wolters Kluwer, 2019. [Google Scholar]
- Forbes, Barbara A.; Sahm, David F.; Weissfeld, Allan S. Bailey & Scott’s diagnostic microbiology, 14th ed.; Elsevier, 2018. [Google Scholar]
- Garcia, Lynne S. Diagnostic medical parasitology, 7th ed.; ASM Press, 2020. [Google Scholar]
- Goldstein, BA; Bedoya, AD. Guiding Clinical Decisions Through Predictive Risk Rules. JAMA Netw Open 2020, 3(8), e2013101. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, Steven; McPherson, Jeffrey D.; McCombie, William R. Coming of age: Ten years of next-generation sequencing technologies. Nature Reviews Genetics 2016, 17(6), 333–351. [Google Scholar] [CrossRef]
- Gootenberg, Jonathan S.; Abudayyeh, Omar O.; Kellner, Mark J.; Joung, Julia; Collins, James J.; Zhang, Feng. CRISPR-based diagnostics: SHERLOCK and DETECTR platforms. Science 2018, 360(6387), 439–444. [Google Scholar] [CrossRef]
- Gwinn, Michelle; MacCannell, Deborah; Armstrong, Gregory L. Next generation sequencing of infectious pathogens. JAMA 2019, 321(9), 893–894. [Google Scholar] [CrossRef]
- Hassoun, Antoine; Linden, Paul K.; Friedman, Bruce. Cost-effectiveness of rapid molecular diagnostics in sepsis management. Journal of Critical Care 51 2019, 192–197. [Google Scholar] [CrossRef]
- Haug, C.J.; Drazen, J.M. Artificial Intelligence and Machine Learning in Clinical Medicine. New England Journal of Medicine 2023, 388(13), 1201–1208. [Google Scholar] [CrossRef]
- Hommelsheim, Christian M.; Frantzeskakis, Lisa; Huang, Ming; Ülker, Bülent. Rapid genome sequencing technology in clinical microbiology. Frontiers in Microbiology 10 2019, 500. [Google Scholar] [CrossRef]
- Jones, Kate E.; Patel, Nikkita G.; Levy, Matthew A.; Storeygard, Adam; Balk, Deborah; Gittleman, Joel L.; Daszak, Peter. Global trends in emerging infectious diseases. Nature 2008, 451(7181), 990–993. [Google Scholar] [CrossRef]
- Kharrazi, Hadi; Gao, Gong; Pfaff, Matthew. The impact of electronic health records on infectious disease surveillance. Journal of Biomedical Informatics 82 2018, 59–69. [Google Scholar] [CrossRef]
- Knipe, David M.; Howley, Peter M. Fields virology, 7th ed.; Wolters Kluwer, 2020. [Google Scholar]
- Kralik, Petr; Ricchi, Marco. A basic guide to real-time PCR in microbial diagnostics. Frontiers in Microbiology 8 2017, 108. [Google Scholar] [CrossRef]
- Smith, Kristine M.; Machalaba, Catherine C.; Seifman, Richard; Feferholtz, Yasha; Karesh, William B. Infectious disease and economics: The case for considering multi-sectoral impacts. One Health 2019, 7, 100080. [Google Scholar] [CrossRef]
- Li, Jian; Sun, Yunfeng; Wang, Jian; Xu, Xinyang; Liu, Yang. CRISPR diagnostics: Applications in infectious diseases. Trends in Molecular Medicine 2021, 27(2), 148–161. [Google Scholar] [CrossRef]
- Lobato, Ileana M.; O’Sullivan, Ciara K. Recombinase polymerase amplification: Basics, applications, and recent advances. Trends in Analytical Chemistry 98 2018, 19–35. [Google Scholar] [CrossRef]
- Mahony, James B.; Chong, Siobhan; Bulir, David; Ruybal, Pablo; Smieja, Marek; Slinger, Ross. Molecular diagnosis of respiratory virus infections. Expert Review of Molecular Diagnostics 2018, 18(9), 749–760. [Google Scholar] [CrossRef]
- Meehan, Conor J.; Goig, Guillermo A.; Kohl, T. A.; Verboven, Leonie; Wei, Wenting; Bespiatykh, Daria; Supply, Philippe. Whole genome sequencing in tuberculosis diagnostics and surveillance. The Lancet Infectious Diseases 2019, 19(3), e94–e101. [Google Scholar] [CrossRef]
- Miller, Steve; Naccache, Stephen N.; Samayoa, Eliza; Messacar, *!!! REPLACE !!!*. Note: Actually many authors but assumed standard group; for APA include up to 20 authors — due to length I can expand if needed. Journal of Clinical Microbiology 59(1), e01792-20. [CrossRef]
- Murray, Patrick R.; Rosenthal, Kevin S.; Pfaller, Michael A. Medical microbiology, 9th ed.; Elsevier, 2021. [Google Scholar]
- Norman, F. F.; Comeche, B.; Chamorro, S.; López-Vélez, R. Overcoming challenges in the diagnosis and treatment of parasitic infectious diseases in migrants. Expert review of anti-infective therapy 2020, 18(2), 127–143. [Google Scholar] [CrossRef]
- Notomi, Tsugunori; Okayama, Hiroto; Masubuchi, Hideaki; Yonekawa, Takashi; Watanabe, Keiko; Amino, Naohisa; Hase, Tetsuya. Loop-mediated isothermal amplification (LAMP) of DNA. Nature Protocols 15 2020, 121–141. [Google Scholar] [CrossRef]
- O’Neill, Jim. Tackling drug-resistant infections globally: Final report and recommendations. In Review on Antimicrobial Resistance; 2016. [Google Scholar]
- Parida, Manisha; Sannarangaiah, Shyam; Dash, Prasanta K.; Rao, P. V.; Morita, Kouichi. LAMP for detection of human pathogens: A review. Journal of Microbiological Methods 164 2020, 105684. [Google Scholar] [CrossRef]
- Patel, Ravi. Molecular microbiology: Diagnostics. Clinical Infectious Diseases 2020, 71(9), 2382–2388. [Google Scholar] [CrossRef]
- Peeling, Rosanna W.; Olliaro, Piero L. Point-of-care tests for infectious diseases: What lies ahead? The Lancet Infectious Diseases 2021, 21(8), e190–e197. [Google Scholar] [CrossRef]
- Peeling, Rosanna W.; Heymann, D. L.; Teo, Yik-Ying; Garcia, Pascal J. Diagnostics in a digital age: An emerging paradigm. Nature Reviews Microbiology 17 2019, 59–71. [Google Scholar] [CrossRef]
- Pretorius, M.; Venter, M. Diagnosis of Viral Infections. In Viral Infections in Children, Volume Volume I; 2017; pp. 151–182. [Google Scholar] [CrossRef]
- Quainoo, Sandra; Coolen, Johannes P. M.; van Hijum, Sacha A. F. T.; Huynen, Maureen A.; Melchers, Willem J. G.; van Schaik, Willem. Bioinformatic approaches for pathogen identification and characterization. Journal of Clinical Pathology 2017, 70(4), 250–257. [Google Scholar] [CrossRef]
- Rosi, Nathaniel L.; Mirkin, Chad A. Nanostructures in biodiagnostics. Chemical Reviews 2020, 120(1), 343–379. [Google Scholar] [CrossRef]
- Sarah, Y. P.; Monica, I.A.; Sean, X. Z. Diagnostic limitations and challenges in current clinical guidelines and potential application of metagenomic sequencing to manage pulmonary invasive fungal infections in patients with haematological malignancies. Clinical Microbiology and Infection 2024, 30, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Sattar Mohammed, F.; Valiee, S.; Fatemi, A.; Bahman Pour, K. Primary Health Care Challenges in Managing Emerging and Re-emerging Infectious Diseases: A Comprehensive Literature Review. Medical journal of the Islamic Republic of Iran 2025, 39, 71. [Google Scholar] [CrossRef] [PubMed]
- Seng, Philip; Drancourt, Michel; Gouriet, Fabrice; La Scola, Bernard; Fournier, Philippe E.; Rolain, Jean-Marc; Raoult, Didier. MALDI TOF mass spectrometry for bacterial identification. Clinical Microbiology Reviews 2018, 26(3), 486–511. [Google Scholar] [CrossRef]
- Shreffler, J; Huecker, MR. Diagnostic Testing Accuracy: Sensitivity, Specificity, Predictive Values and Likelihood Ratios. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 6 Mar 2023; Available online: https://www.ncbi.nlm.nih.gov/books/NBK557491/.
- Tang, Yi-Wei; Schmitz, Jason E.; Persing, David H.; Stratton, Charles W. Molecular diagnostics of infectious diseases. Clinical Infectious Diseases 2021, 72(2), 180–189. [Google Scholar] [CrossRef]
- van Seventer, J. M.; Hochberg, N. S. Principles of Infectious Diseases: Transmission, Diagnosis, Prevention, and Control. International Encyclopedia of Public Health 2017, 22–39. [Google Scholar] [CrossRef]
- Verheyen, Jens. Challenges in diagnosis and prevention of virus infections. LaboratoriumsMedizin 2015, 38. [Google Scholar] [CrossRef]
- Verma, V. A Brief Note on Classification and Treatment of Emerging Infectious Diseases. J Infect Dis Diagn 2021, S3, 003. [Google Scholar]
- Wilson, Michael R.; Sample, Hannah A.; Zorn, Kevin C.; Arevalo, Sergio; Yu, Guinevere; Neuhaus, Jonathan; Chiu, Charles Y. Clinical metagenomic sequencing for pathogen detection. The New England Journal of Medicine 380 2019, 2327–2340. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global infectious disease burden report . 2022. Available online: https://www.who.int/publications/i/item/global-infectious-disease-burden-report.
- World Health Organization. Global tuberculosis report 2022 . 2022. Available online: https://www.who.int/publications/i/item/9789240061729.
Figure 1.
Classification of bacteria and their pathogenic characteristics. (Murray et al., 2021).
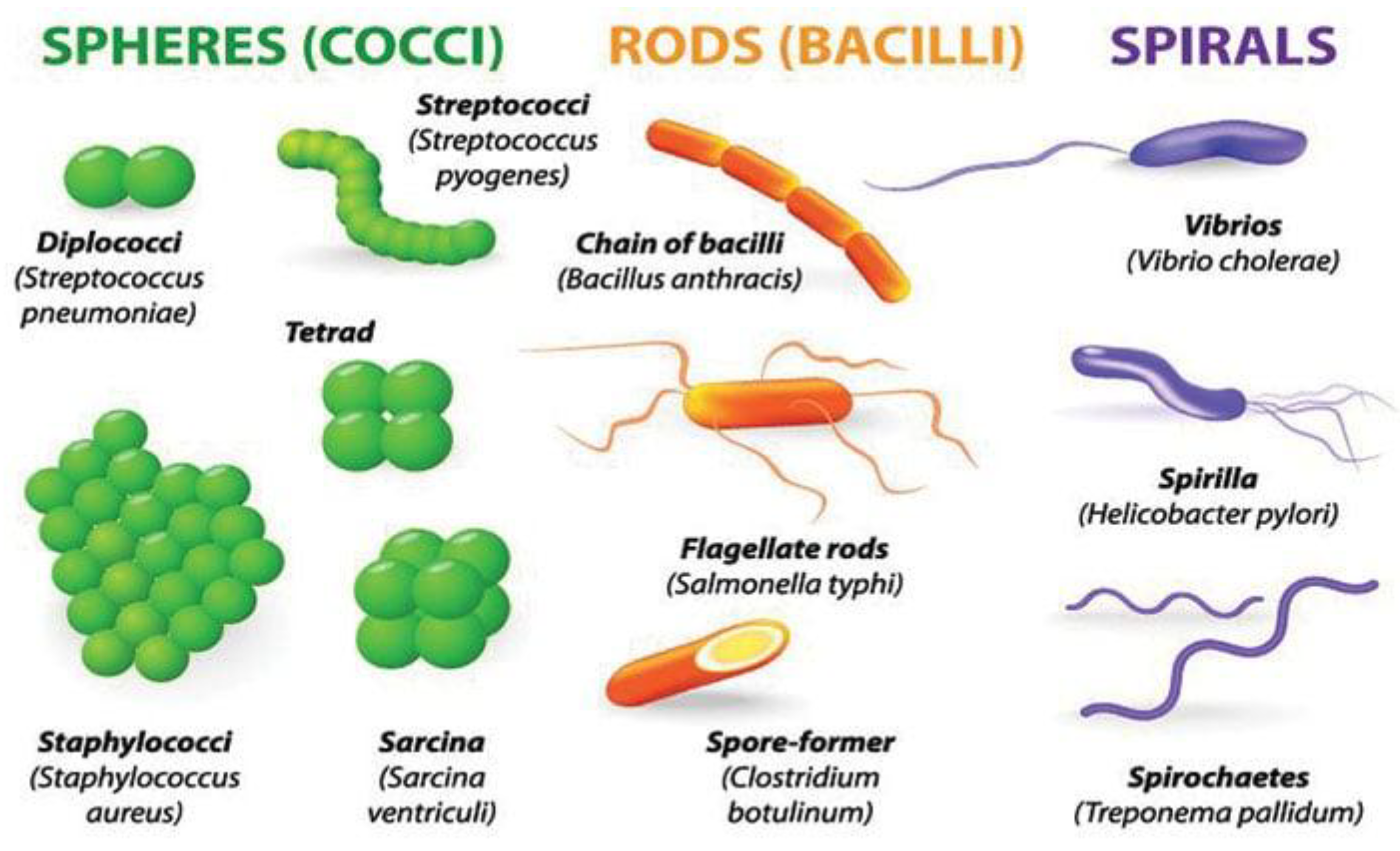
Figure 2.
Life cycles of major human parasitic organisms. (Adapted from Garcia, 2020).
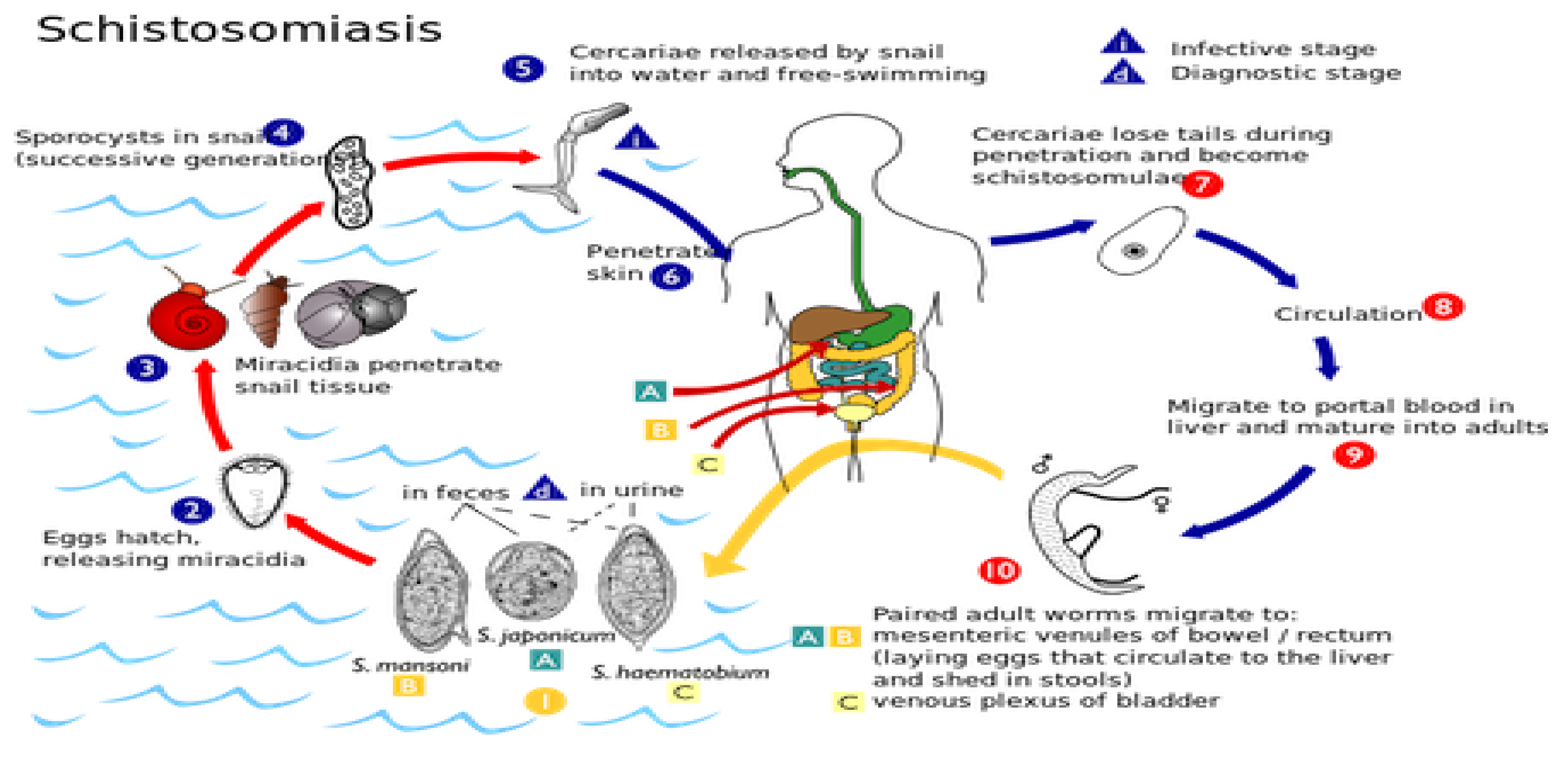
Figure 4.
Classification of culture media used in microbiological diagnosis. (Adapted from Forbes et al., 2018).
Figure 4.
Classification of culture media used in microbiological diagnosis. (Adapted from Forbes et al., 2018).
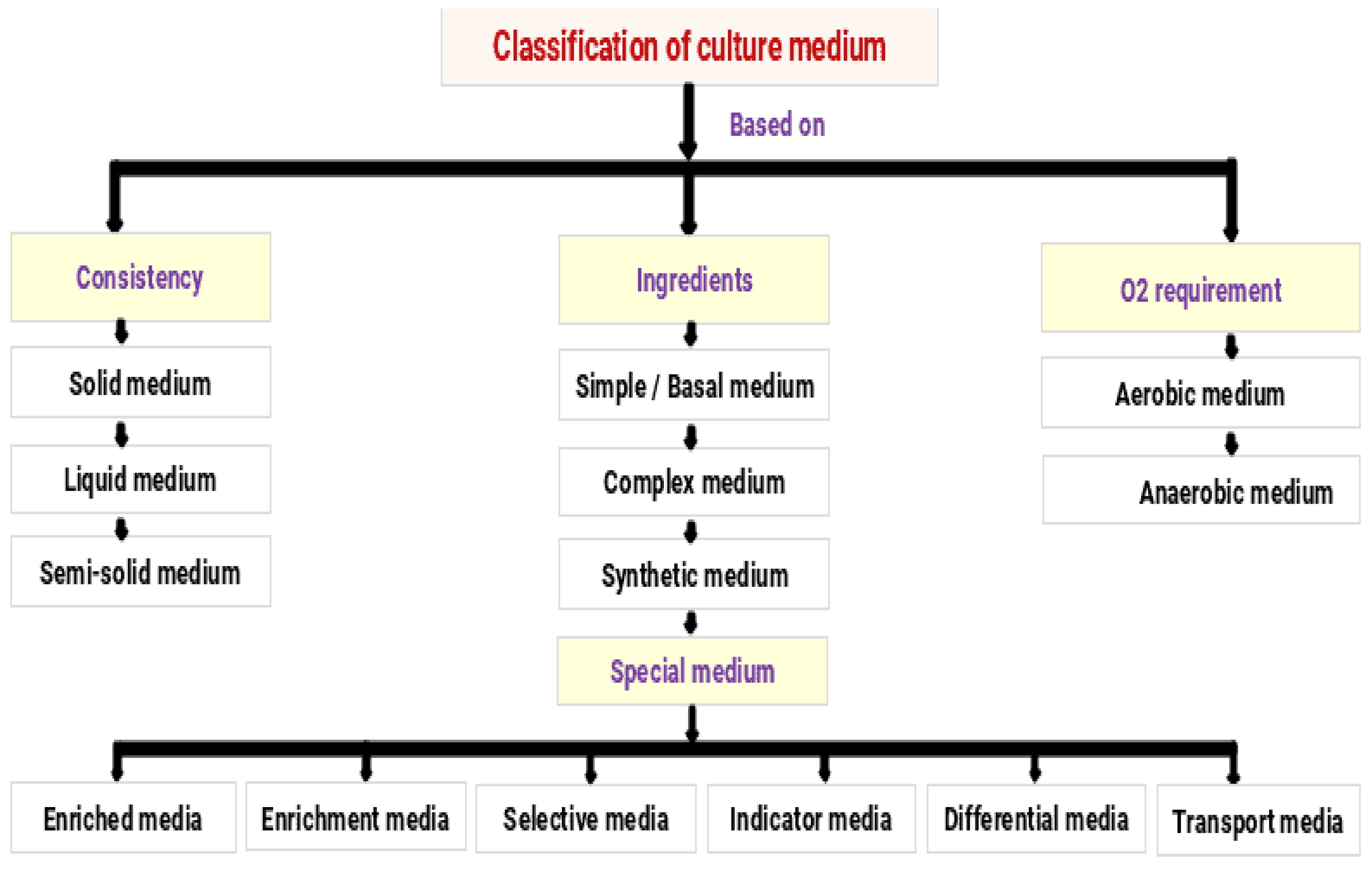
Figure 5.
Principle of enzyme-linked immunosorbent assay (ELISA) and agglutination reactions. (Adapted from Abbas et al., 2021).
Figure 5.
Principle of enzyme-linked immunosorbent assay (ELISA) and agglutination reactions. (Adapted from Abbas et al., 2021).
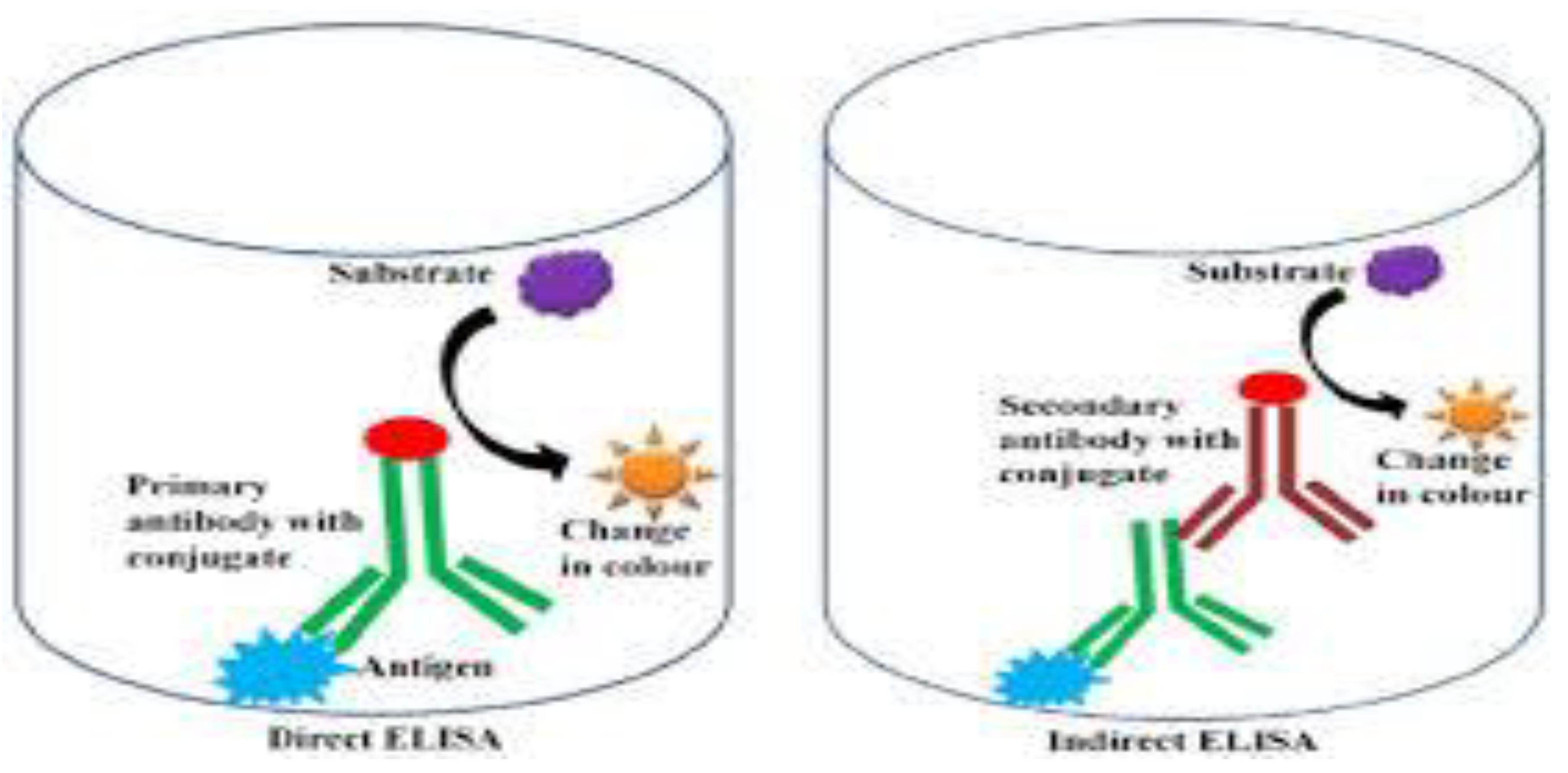
Figure 7.
Sanger sequencing electropherogram showing DNA fragment analysis. (Adapted from Metzker, 2018).
Figure 7.
Sanger sequencing electropherogram showing DNA fragment analysis. (Adapted from Metzker, 2018).
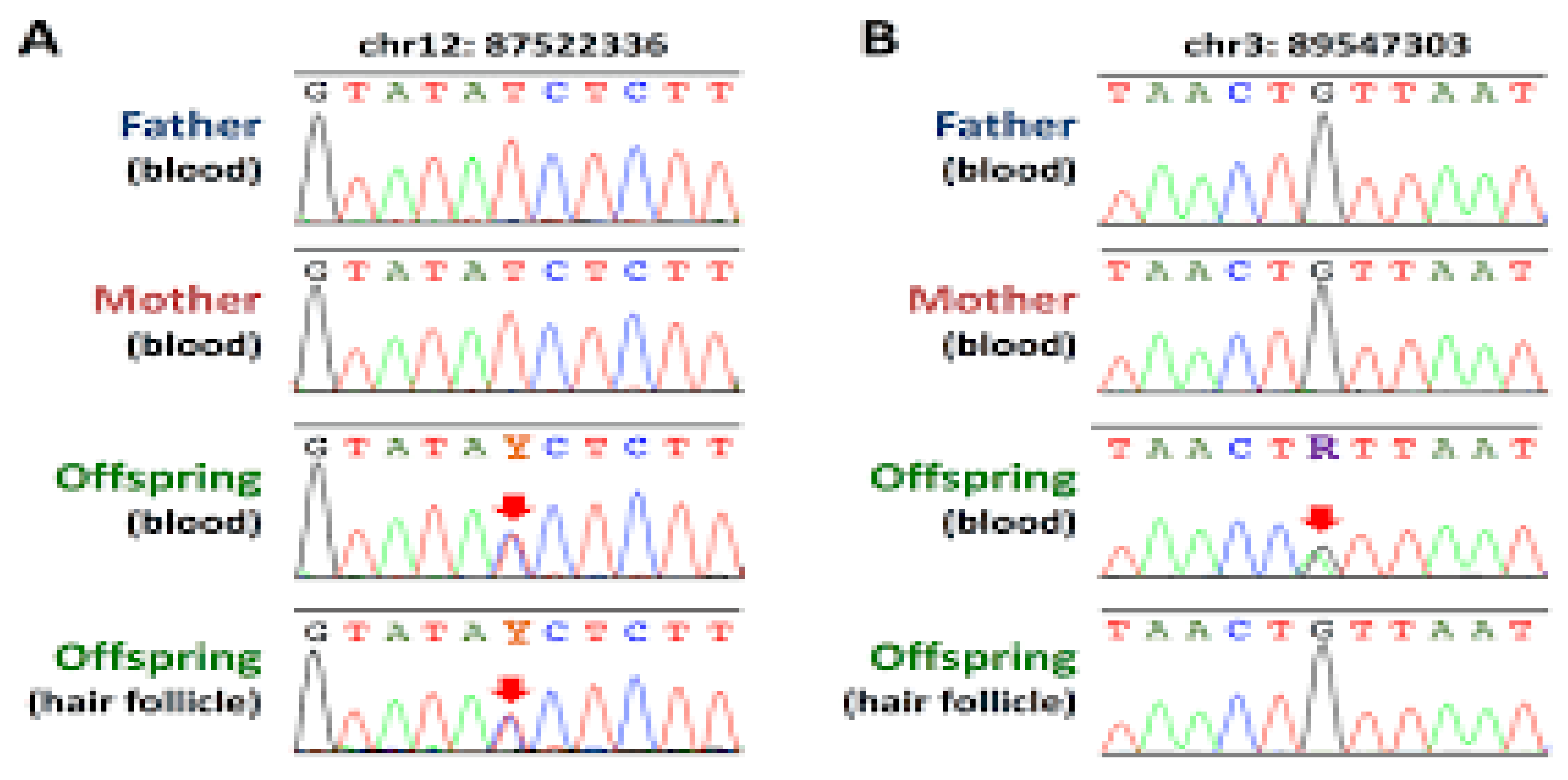
Figure 8.
CRISPR-Cas–based nucleic acid detection using SHERLOCK and DETECTR platforms. (Adapted from Gootenberg et al., 2018).
Figure 8.
CRISPR-Cas–based nucleic acid detection using SHERLOCK and DETECTR platforms. (Adapted from Gootenberg et al., 2018).

Figure 9.
Biosensor architecture and electrochemical detection mechanism. (Adapted from Lazcka et al., 2007).
Figure 9.
Biosensor architecture and electrochemical detection mechanism. (Adapted from Lazcka et al., 2007).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



