
Submitted:
24 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Epithelial ovarian cancer is predominantly characterized by peritoneal dissemination, providing a strong biological rationale for intraperitoneal (IP) chemotherapy. Although IP cisplatin-based regimens have demonstrated substantial survival benefits in pivotal randomized trials, toxicity and catheter-related complications limit their widespread adoption. IP carboplatin has emerged as a pragmatic alternative with improved tolerability while preserving its pharmacokinetic advantages. This review summarizes the biological and pharmacological rationale for IP carboplatin and critically examines the clinical evidence, with a particular emphasis on the Intraperitoneal Carboplatin for Ovarian Cancer (iPocc) trial and its divergence from Gynecologic Oncology Group (GOG)-252. We further discuss the potential applicability of IP carboplatin beyond the traditional setting of minimal residual disease, including patients undergoing neoadjuvant chemotherapy and interval debulking surgery, as well as its possible use in the contemporary era of maintenance therapy. Collectively, the accumulated evidence supports renewed consideration of IP carboplatin as a versatile component in modern ovarian cancer management.
Keywords:
ovarian cancer
; intraperitoneal chemotherapy
; carboplatin
; dose-dense TC therapy
1. Introduction
Epithelial ovarian cancer is predominantly a peritoneal disease, a biological characteristic that has long supported the rationale for intraperitoneal (IP) chemotherapy. The peritoneal–plasma barrier enables markedly higher local drug exposure within the peritoneal cavity while simultaneously limiting systemic absorption. Pharmacokinetic studies have demonstrated that the IP administration of platinum agents achieves peritoneal concentrations approximately 10–20 times higher than those attained via intravenous (IV) delivery, thereby ensuring sustained tumor exposure [1].
This pharmacokinetic advantage has translated into meaningful clinical benefits, as evidenced by a series of pivotal Gynecologic Oncology Group (GOG) trials. In particular, GOG-114 and GOG-172 demonstrated a considerable overall survival (OS) advantage with IP cisplatin-based chemotherapy in patients with optimally debulked advanced ovarian cancer [2,3]. Despite substantial treatment-related toxicity and lower completion rates, GOG-172 reported a median OS improvement exceeding 15 months compared to standard IV therapy (49.7 versus 65.6 months). Importantly, long-term follow-up analyses have confirmed that this survival benefit persists beyond 10 years, particularly in patients who completed the planned IP treatment cycles [4].
Nevertheless, the clinical implementation of IP chemotherapy is hindered by toxicity, catheter-related complications, and limited tolerability, which are largely attributable to the use of IP cisplatin [5,6]. These challenges have prompted the exploration of carboplatin as an alternative IP platinum agent. Carboplatin offers a more favorable toxicity profile while maintaining antitumor efficacy, and its pharmacokinetic properties, including high IP drug concentrations, support its suitability for IP administration. Consequently, IP carboplatin has emerged as a pragmatic evolution of regional chemotherapy, aiming to preserve the pharmacokinetic and survival advantages of IP delivery while improving feasibility and treatment adherence. In this review, we summarize the historical development and biological rationale of IP chemotherapy and critically examines the role of IP carboplatin in the modern management of ovarian cancer.
2. Pharmacokinetic Characteristics of Platinum Agents: IP Therapy as a Systemic Delivery Route (Table 1)
The pharmacokinetic behavior of IP-administered anticancer agents depends largely on their molecular weight and hydrophilicity [7]. Platinum compounds, such as cisplatin and carboplatin, are low-molecular-weight water-soluble agents that are rapidly absorbed from the peritoneal cavity into the systemic circulation through capillary and lymphatic pathways. Thus, although IP administration achieves markedly high regional drug concentrations, the systemic platinum exposure closely mirrors that achieved by IV delivery.
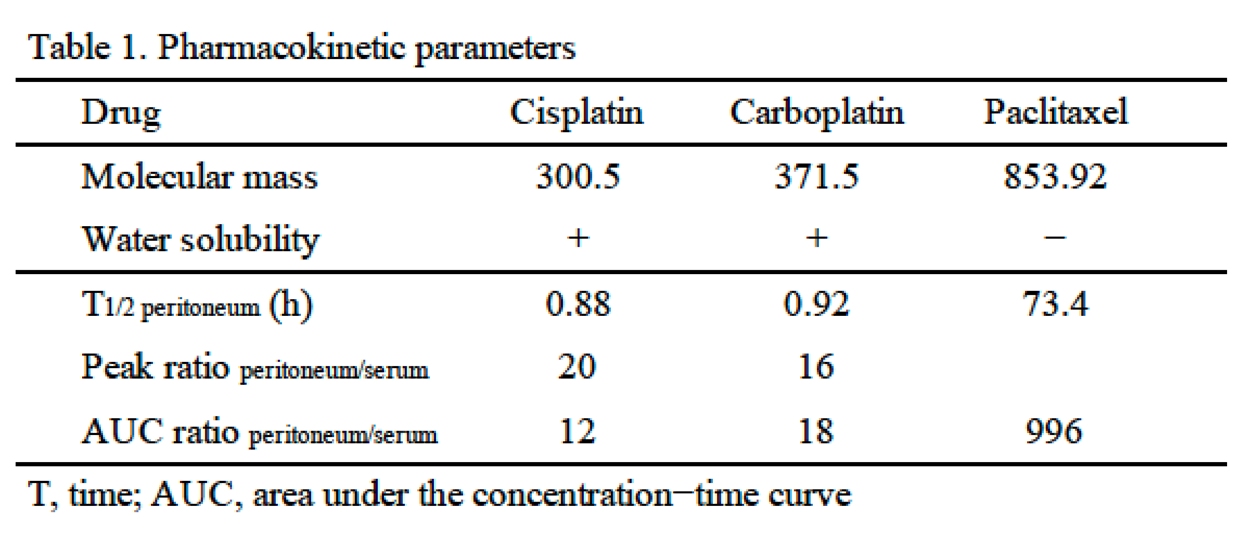
Pharmacokinetic analyses have demonstrated that, following IP carboplatin administration, the 24-h area under the concentration–time curve (AUC) for serum platinum is nearly identical to that achieved with IV administration [8]. In contrast, peritoneal AUC remains approximately 15–20-fold higher with the IP route. This dual pharmacokinetic profile indicates that IP platinum therapy provides intensified regional exposure while maintaining systemic drug efficacy comparable to that of conventional IV administration.
Conversely, paclitaxel exhibits distinct pharmacokinetic properties. As a high molecular weight hydrophobic compound, paclitaxel is retained within the peritoneal cavity for prolonged periods, resulting in an exceptionally high peritoneal-to-plasma AUC ratio, often exceeding 1,000. Although this property supports sustained local exposure, systemic absorption is limited and delayed. Furthermore, prolonged local retention of paclitaxel has been associated with increased peritoneal irritation and catheter-related complications, as documented in landmark trials such as GOG-172 [3].
Notably, the depth of direct drug penetration from the peritoneal surface into the tumor tissue is limited to a few millimeters (typically 1–3 mm) [9,10]. Therefore, the clinical efficacy of IP chemotherapy cannot be solely attributed to its direct diffusion into the peritoneal implants. For platinum-based agents, rapid systemic absorption facilitates secondary tumor exposure via the underlying vasculature (tumor-feeding blood vessels). This enables IP administration to function as a systemic treatment while simultaneously delivering high local concentrations to the serosal surface. This mechanistic synergy explains why IP platinum therapy remains effective even in patients with larger residual tumors, a finding supported by both historical GOG trials and more recent studies on IP carboplatin.
Overall, for rapidly absorbed agents such as platinum compounds, the IP route should be redefined not merely as a local treatment but also as a sophisticated systemic delivery strategy that enhances regional intensity without compromising systemic availability.
3. IP Carboplatin for Ovarian Cancer with Large Residual Tumor Burden
The pharmacokinetic properties of platinum-based agents provide a biological rationale for the potential efficacy of IP platinum therapy even in the presence of relatively large residual tumor burdens. Although the depth of peritoneal drug penetration is limited, systemic absorption of platinum following IP administration contributes substantially to overall drug exposure. Accordingly, IP delivery of platinum agents should not be regarded as a purely regional treatment but rather as a hybrid modality that combines intensified peritoneal exposure with effective systemic chemotherapy.
Clinical evidence supports this conceptual framework. Long-term follow-up analyses of the GOG-114 and GOG-172 trials demonstrated that the survival benefit of IP therapy was not restricted to patients with minimal residual disease [4]. Importantly, improved outcomes were observed among patients who completed a greater number of IP cycles, suggesting that treatment completion and cumulative systemic platinum exposure, rather than residual tumor size alone, may be key determinants of benefit. Although these findings should be interpreted with caution owing to the potential selection bias, they suggest that the efficacy of IP platinum therapy extends beyond purely microscopic diseases. Moreover, several retrospective and phase II studies evaluating IP carboplatin in combination with IV paclitaxel have demonstrated clinical activity in patients with suboptimal residual disease following primary cytoreductive surgery [11,12]. Collectively, these data support the feasibility of IP carboplatin in clinical settings traditionally considered less suitable for IP therapy.
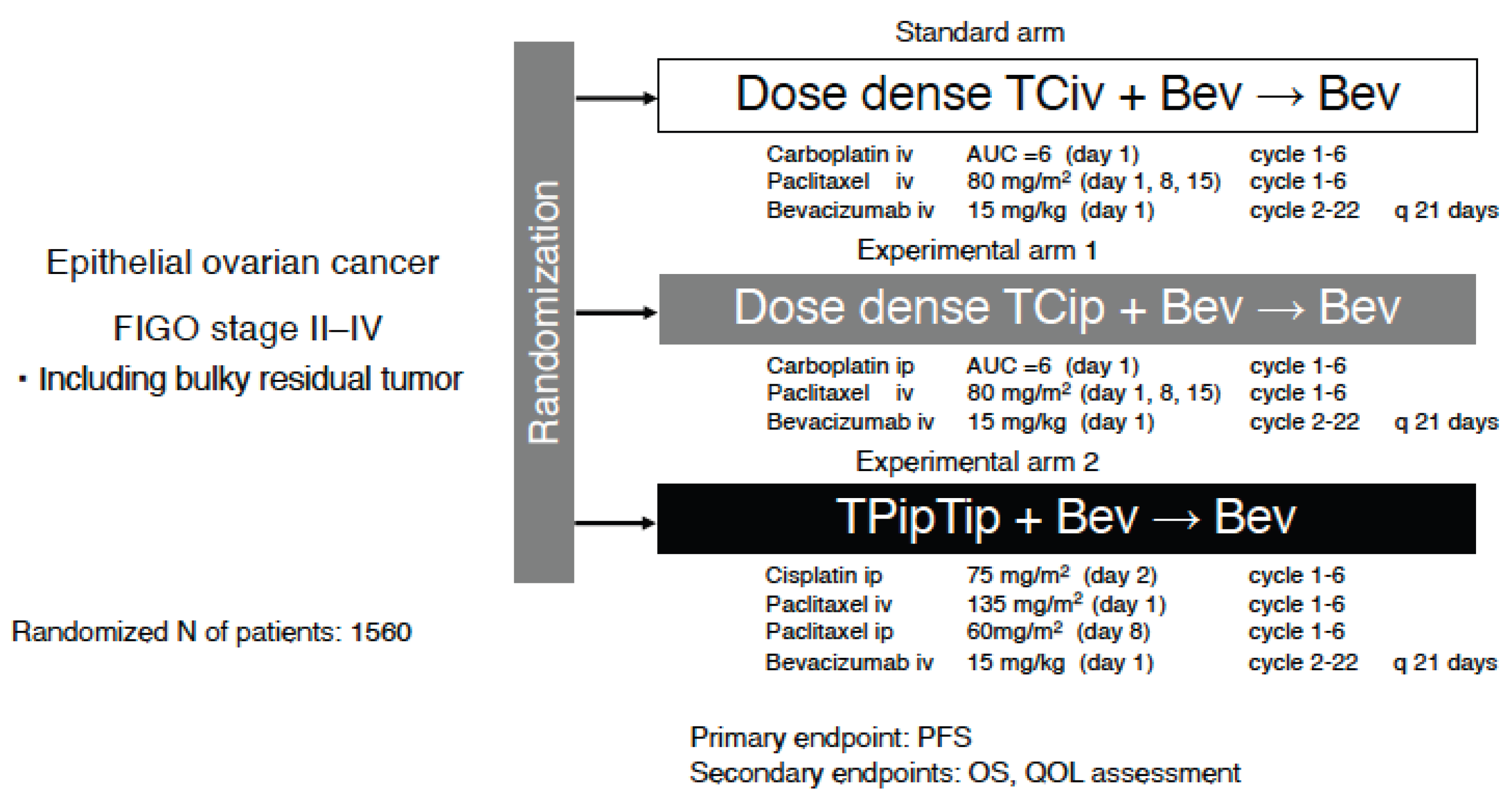
More recently, the Intraperitoneal Carboplatin for Ovarian Cancer (iPocc) trial provided prospective randomized evidence that IP administration of carboplatin was superior to IV administration in patients with epithelial ovarian cancer, including those with larger residual tumors (Figure 1) [13]. Notably, this benefit was achieved with an acceptable safety profile, with port-related complications identified as the main additional toxicities. Therefore, the iPocc trial expanded the clinical applicability of IP chemotherapy by demonstrating that IP carboplatin can retain therapeutic efficacy across a broader spectrum of tumors than previously assumed.
Collectively, these pharmacokinetic and clinical data support IP carboplatin as a rational treatment option for selected patients with ovarian cancer, including those with relatively large residual tumor volumes. Rather than being strictly limited to patients with minimal residual disease, IP carboplatin may offer intensified peritoneal drug exposure without compromising systemic efficacy, provided that treatment delivery and completion can be adequately maintained. However, patients who complete a greater number of IP cycles likely represent a biologically and clinically favorable subset, introducing an inherent selection bias that limits causal interpretation.
4. Why Did GOG-252 Fail to Confirm Benefit While iPocc Was Positive? Differences in Populations and Trial Context (Table 2)
Although both GOG-252 and iPocc evaluated IP carboplatin delivery within a modern paclitaxel–carboplatin backbone, their trial designs and clinical contexts were fundamentally distinct, likely contributing to their divergent outcomes (Figure 2) [13,14].
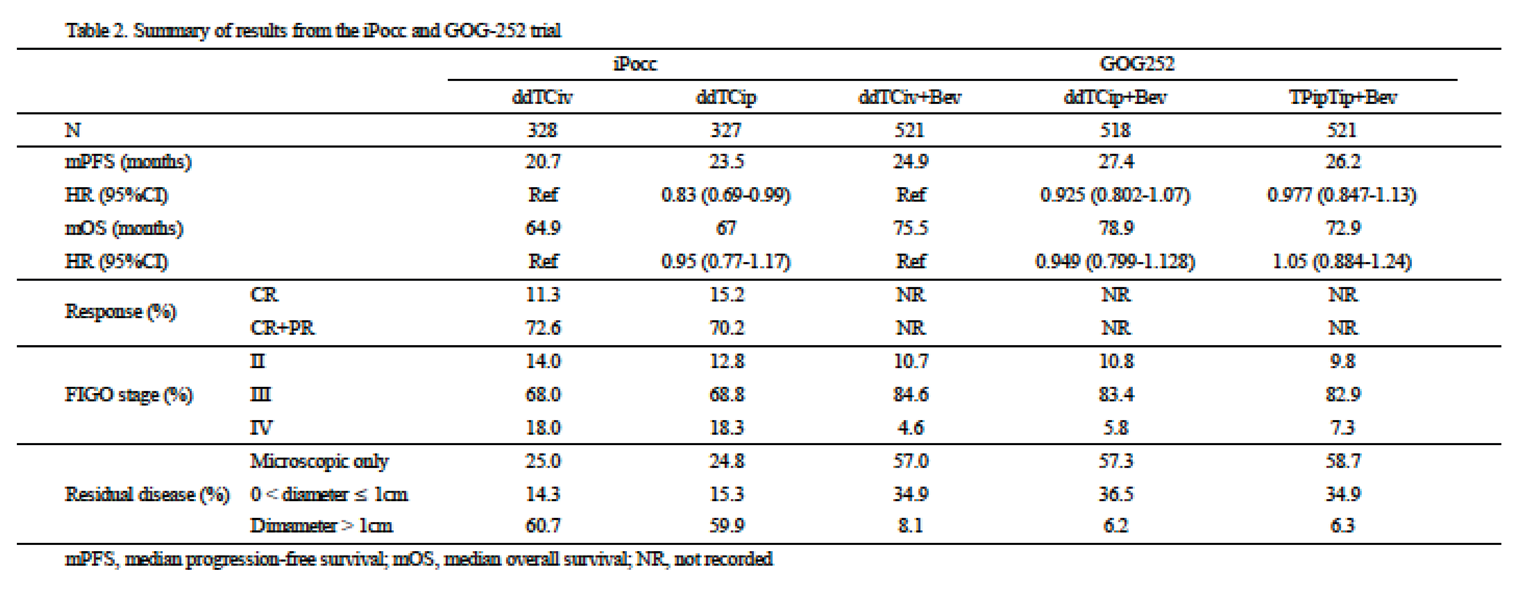
First, the use of bevacizumab differed substantially between the two trials. In GOG-252, bevacizumab was administered concomitantly and as a maintenance therapy across all treatment arms. In this context, neither IP regimen (dose-dense TCip [ddTCip] or tri-weekly TCip) improved progression-free survival (PFS) or OS compared with the IV control arm (median PFS: 24.9 vs. 27.4 vs. 26.2 months; hazard ratio [HR] 0.925 and 0.977, respectively). In contrast, iPocc was designed to isolate the specific effect of the IP route by excluding bevacizumab and ensuring that all variables, except the administration route, remained identical (dose-dense TCiv [ddTCiv] vs. ddTCip). This approach effectively minimizes confounding factors that may mask regional advantages of IP delivery.
Furthermore, there were notable differences in patient populations and surgical pathways. The iPocc trial enrolled patients with FIGO stage II–IV epithelial ovarian cancer and specifically addressed whether IP carboplatin could improve outcomes even in patients with suboptimal cytoreduction after primary debulking surgery (PDS). Patients undergoing interval debulking surgery (IDS) after neoadjuvant chemotherapy (NAC) were also included. This broader inclusion eligibility aligns with the evolving paradigm that, for rapidly absorbed platinum agents, IP administration functions as a hybrid strategy of regional intensification and systemic therapy and may benefit a wider range of patients than previously assumed.
Third, potential interaction between antiangiogenic therapy and IP chemotherapy warrants further investigation. Subgroup analyses of the GOG-252 trial suggested that bevacizumab may attenuate the relative benefit of IP carboplatin. While the precise mechanism remains unclear, a plausible biological explanation is that bevacizumab may optimize peritoneal control by altering vascular permeability and drug distribution, thereby reducing the incremental advantage of IP carboplatin over IV counterpart and making a positive treatment signal more difficult to detect.
Finally, survival data from iPocc support the long-term efficacy of this approach. In iPocc, IP carboplatin significantly improved PFS compared with IV administration (median PFS 20.7 vs. 23.5 months; HR 0.83; P = 0.041). Notably, the PFS curves exhibited sustained separation during long-term follow-up, suggesting that a subset of patients derived a durable benefit from IP delivery. Collectively, these discrepancies in design and context indicate that the “negative” results of GOG-252 do not refute the efficacy of IP carboplatin; rather, they may reflect a trial architecture in which universal bevacizumab use may have inadvertently diluted the route-specific therapeutic effect.
5. Unresolved Questions and Limitations
Despite the pharmacological rationale for IP carboplatin, several limitations must be addressed before its widespread clinical adoption.
5.1. Selection Bias and Treatment Adherence
A significant challenge in interpreting IP therapy trials is the inherent selection bias. Long-term data from GOG-114 and GOG-172 showed that survival benefits correlated with the number of cycles completed [4]. However, patients who tolerate multiple IP cycles often possess favorable baseline characteristics, such as superior performance status and less aggressive tumor biology. While the iPocc trial suggested benefits across various residual disease strata, treatment completion may act as a surrogate for a favorable prognosis, making it difficult to isolate the true therapeutic effect of the IP route from patient-related factors [13].
5.2. Lack of Biomarker Stratification
Most IP trials, including iPocc, were designed before the routine use of molecular profiling. Consequently, there is a lack of data on how homologous recombination deficiency (HRD) or BRCA1/2 mutation status influences the efficacy of IP carboplatin. It remains unknown whether the intensified local exposure provided by the IP route offers incremental benefits over IV therapy in specific molecular subgroups, limiting our ability to personalize treatment in the modern era of precision oncology.
5.3. Interaction with Bevacizumab and PARP Inhibitors
The compatibility of IP carboplatin with current maintenance therapies is not yet established. In GOG-252, the universal administration of bevacizumab may have masked the potential benefits of IP delivery, yet the biological interaction between anti-angiogenic agents and IP drug distribution remains speculative [14]. Furthermore, the integration of IP carboplatin with PARP inhibitors is a critical evidence gap. While intensified platinum responses could theoretically enhance the efficacy of subsequent PARP inhibition, this has not been prospectively validated.
5.4. Generalizability and Surgical Expertise
The safety of IP carboplatin relies heavily on institutional infrastructure and surgical expertise in port management. Catheter-related complications remain a concern, and the impact of NAC on peritoneal anatomy and port safety is not fully characterized. These factors may limit the reproducibility of results from high-volume specialized centers in broader clinical practice.
6. Expanding the Clinical Scope: NAC/IDS, Suboptimal Cytoreduction, and the PARP-Inhibitor Era
The design of the iPocc trial and subsequent subgroup observations support a broader conceptualization of IP carboplatin, moving beyond the traditional “optimal debulking only” paradigm. Subgroup analyses suggested favorable outcomes with ddTCip across all residual tumor strata, indicating that the regimen remains a viable consideration even for patients planned for NAC followed by IDS. This expansion is clinically relevant, as real-world practice increasingly incorporates NAC/IDS strategies, particularly when complete upfront resection is not feasible.
6.1. Suboptimal Residual Disease or NAC Settings
The iPocc trial is unique in explicitly testing whether IP carboplatin improves outcomes in patients with suboptimal cytoreduction after PDS. Mechanistically, this is supported by platinum pharmacokinetics, as rapid peritoneal absorption yields systemic exposure comparable to IV delivery while maintaining markedly higher IP concentrations. This “bidirectional” tumor exposure, occurring via both the peritoneal surface and the tumor vasculature, provides a biologically plausible basis for efficacy even in the presence of larger residual tumor implants. Patients with suboptimal residual disease may therefore be good candidates for IP carboplatin therapy, including chemotherapy administered as NAC.
6.2. NAC Followed by IDS Settings
Conceptually, NAC followed by IDS may markedly reduce the tumor burden and enhance the regional efficacy of IP therapy by minimizing drug diffusion distances. Concurrently, IP platinum is rapidly absorbed into the systemic circulation, providing systemic exposure comparable to that achieved by IV administration. Consequently, if catheter/port placement is feasible and patient tolerability is maintained, IP carboplatin represents a reasonable intensification strategy following IDS. Nevertheless, it remains unclear whether surgical alterations or adhesions resulting from IDS increase the risk of catheter-related complications. Further ancillary analyses and prospective studies are needed to address these uncertainties.
6.3. Positioning Alongside Poly(ADP-ribose) Polymerase (PARP) Inhibitors
A pivotal unresolved issue is whether the clinical benefits of IP carboplatin are preserved when integrated with modern maintenance strategies, specifically PARP inhibitors. Although current evidence has yet to define the impact of this interaction, necessitating rigorous, randomized phase III trials, a compelling conceptual rationale for this combination exists. Tumors characterized by homologous recombination deficiency, including those with BRCA1/2 mutations, exhibit marked sensitivity to both platinum agents and PARP inhibition [15,16]. Consequently, intensified IP platinum exposure may augment the depth of the initial clinical response, potentially optimizing the therapeutic landscape for subsequent PARP maintenance and extending the duration of disease control.
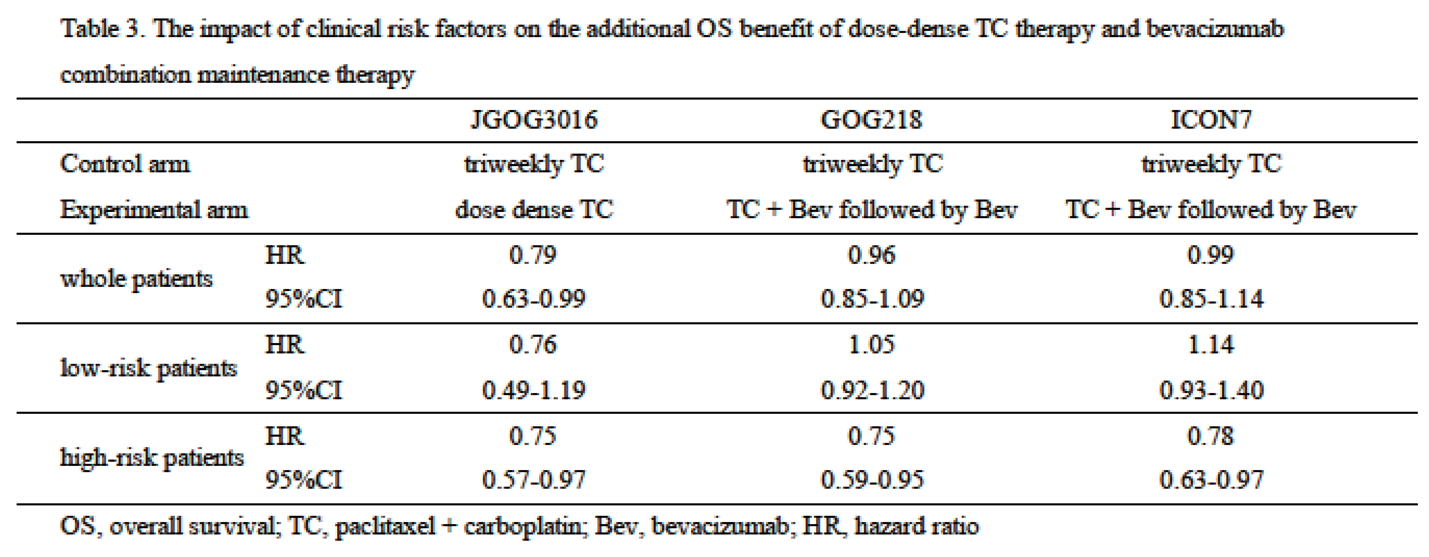
6.4. Should We Use Dose-Dense TC Therapy or Bevacizumab Combination Maintenance Therapy (Table 3)?
Across three large randomized trials comparing conventional triweekly paclitaxel plus carboplatin (TC) with either ddTC or TC combined with bevacizumab followed by bevacizumab maintenance—namely JGOG3016, GOG-218, and ICON7—distinct and clinically relevant patterns of treatment effect have been observed [17,18,19]. In JGOG3016, ddTC was associated with a significant overall survival benefit that appeared largely independent of established clinical risk factors. In contrast, in GOG-218 and ICON7, the addition of bevacizumab followed by maintenance therapy yielded the greatest benefit in patients with high-risk disease, whereas its impact was attenuated or absent in patients with lower-risk features. These findings collectively suggest that intensified paclitaxel delivery through a dose-dense schedule may exert antitumor effects with relatively limited dependence on baseline clinical risk stratification, whereas the benefit of anti-angiogenic therapy using bevacizumab is more context dependent. Within this framework, the integration of IP carboplatin into a ddTC backbone represents a biologically and clinically coherent strategy. Given that dose-dense paclitaxel appears to provide consistent benefit across a broad clinical spectrum, ddTCip may be applicable to a wide range of patients without substantial modification based on conventional clinical risk factors. This contrasts with bevacizumab-containing strategies, which may require more selective application based on disease burden and risk profile.
6.5. Practical Considerations
From a practical standpoint, successful implementation of IP carboplatin requires standardized port placement techniques, close monitoring of port-related complications, and patient education. When these elements are appropriately addressed, IP carboplatin demonstrates high treatment adherence and a safety profile comparable to that IV chemotherapy, with the added advantage of enhanced peritoneal drug exposure.
6.6. Future Directions
Given the well-established biological interplay between platinum sensitivity and HRD, the clinical efficacy of first-line chemotherapy combining ddTCip followed by PARP inhibitor maintenance therapy warrants urgent prospective investigation. Such trials should incorporate comprehensive biomarker analyses, including BRCA1/2 mutation status and broader HRD profiling, to determine whether intensified platinum exposure during induction therapy can enhance the depth of initial response and, in turn, improve the magnitude and durability of benefit from subsequent PARP inhibitor–based maintenance therapy. Although this hypothesis remains unproven, it is biologically plausible that enhanced intraperitoneal and systemic platinum exposure achieved through IP carboplatin could optimize the therapeutic context for PARP inhibition, particularly in HRD-positive tumors. Carefully designed clinical trials integrating molecular stratification will therefore be essential to define the precise role of IP carboplatin within contemporary, biomarker-driven treatment algorithms for ovarian cancer.
7. Conclusions
IP platinum therapy should not be viewed solely as a locoregional treatment for microscopic peritoneal disease. Because platinum agents are rapidly absorbed into the systemic circulation, IP administration represents a hybrid delivery strategy that combines intensified peritoneal exposure with effective systemic chemotherapy. The clinical detectability of benefit from IP platinum is highly dependent on trial context, including concomitant therapies, patient selection, and surgical pathways. Divergent outcomes among contemporary trials therefore do not necessarily negate its biological efficacy but may instead reflect dilution of route-specific effects within certain treatment frameworks. Within this context, IP carboplatin emerges as a feasible and biologically rational option that may address specific unmet needs in modern ovarian cancer management, even in the era of PARP inhibitor–based maintenance therapy. Its optimal role will depend on careful patient selection, institutional expertise, and prospective integration with molecularly informed treatment strategies.
Author Contributions
Conceptualization, S.N.; Writing—original draft, S.N.; Writing—review and editing, A.F., Y.T., M.T., R.I., Y.T., H.S., K.O., H.M., N.I., J.H., C.O., H.M., and H. M. Supervision: All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AUC | Area under the concentration–time curve |
| GOG | Gynecologic Oncology Group |
| IDS | Interval debulking surgery |
| IP | Intraperitoneal |
| IV | Intravenous |
| NAC | Neoadjuvant chemotherapy |
| OS | Overall survival |
| PARP | Poly(ADP-ribose) polymerase |
| PDS | Primary debulking surgery |
| PFS | Progression-free survival |
| QOL | Quality of life |
References
- Fujiwara, K.; Nagao, S.; Aotani, E.; Hasegawa, K. Principle and evolving role of intraperitoneal chemotherapy in ovarian cancer. Expert Opin Pharmacother 2013, 14, 1797–1806. [Google Scholar] [CrossRef] [PubMed]
- Markman, M.; Bundy, B.N.; Alberts, D.S.; Fowler, J.M.; Clark-Pearson, D.L.; Carson, L.F.; Wadler, S.; Sickel, J. Phase III trial of standard-dose intravenous cisplatin plus paclitaxel versus moderately high-dose carboplatin followed by intravenous paclitaxel and intraperitoneal cisplatin in small-volume stage III ovarian carcinoma: an intergroup study of the Gynecologic Oncology Group, Southwestern Oncology Group, and Eastern Cooperative Oncology Group. J Clin Oncol 2001, 19, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.K.; Bundy, B.; Wenzel, L.; Huang, H.Q.; Baergen, R.; Lele, S.; Copeland, L.J.; Walker, J.L.; Burger, R.A.; Gynecologic Oncology Group. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. In N Engl J Med; PMID, 2006; Volume 354, pp. 34–43. [Google Scholar] [CrossRef]
- Tewari, D.; Java, J.J.; Salani, R.; Armstrong, D.K.; Markman, M.; Herzog, T.; Monk, B.J.; Chan, J.K. Long-term survival advantage and prognostic factors associated with intraperitoneal chemotherapy treatment in advanced ovarian cancer: a gynecologic oncology group study. J Clin Oncol 2015, 33, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Armstrong, D.K.; Huang, H.Q.; Fowler, J.; Webster, K.; Burger, R.A.; Clarke-Pearson, D. Intraperitoneal catheter outcomes in a phase III trial of intravenous versus intraperitoneal chemotherapy in optimal stage III ovarian and primary peritoneal cancer: a Gynecologic Oncology Group Study. Gynecol Oncol 2006, 100, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, K.; Nagao, S.; Tan, D.; Hasegawa, K. Intraperitoneal chemotherapy is now back for ovarian cancer. Int J Clin Oncol 2025, 30, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, K.; Armstrong, D.; Morgan, M.; Markman, M. Principles and practice of intraperitoneal chemotherapy for ovarian cancer. In Int J Gynecol Cancer; PMID, 2007; Volume 17, pp. 1–20. [Google Scholar] [CrossRef]
- Miyagi, Y.; Fujiwara, K.; Kigawa, J.; Itamochi, H.; Nagao, S.; Aotani, E.; Terakawa, N.; Kohno, I. Sankai Gynecology Study Group (SGSG). Intraperitoneal carboplatin infusion may be a pharmacologically more reasonable route than intravenous administration as a systemic chemotherapy. A comparative pharmacokinetic analysis of platinum using a new mathematical model after intraperitoneal vs. intravenous infusion of carboplatin—a Sankai Gynecology Study Group (SGSG) study. Gynecol Oncol 2005, 99, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Los, G.; Mutsaers, P.H.; van der Vijgh, W.J.; Baldew, G.S.; de Graaf, P.W.; McVie, J.G. Direct diffusion of cis-diamminedichloroplatinum(II) in intraperitoneal rat tumors after intraperitoneal chemotherapy: a comparison with systemic chemotherapy. Cancer Res 1989, 49, 3380–3384. [Google Scholar] [PubMed]
- Dedrick, R.L.; Flessner, M.F. Pharmacokinetic problems in peritoneal drug administration: tissue penetration and surface exposure. J Natl Cancer Inst 1997, 89, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Nagao, S.; Fujiwara, K.; Ohishi, R.; Nakanishi, Y.; Iwasa, N.; Shimizu, M.; Goto, T.; Shimoya, K. Combination chemotherapy of intraperitoneal carboplatin and intravenous paclitaxel in suboptimally debulked epithelial ovarian cancer. Int J Gynecol Cancer 2008, 18, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, K.; Nagao, S.; Kigawa, J.; Noma, J.; Akamatsu, N.; Miyagi, Y.; Numa, F.; Okada, M.; Aotani, E. Phase II study of intraperitoneal carboplatin with intravenous paclitaxel in patients with suboptimal residual epithelial ovarian or primary peritoneal cancer: a Sankai Gynecology Cancer Study Group Study. Int J Gynecol Cancer 2009, 19, 834–837. [Google Scholar] [CrossRef] [PubMed]
- Nagao, S.; Fujiwara, K.; Yamamoto, K.; Tanabe, H.; Okamoto, A.; Takehara, K.; Saito, M.; Fujiwara, H.; Tan, D.S.P.; Yamaguchi, S.; et al. Intraperitoneal carboplatin for ovarian cancer—A Phase 2/3 trial. NEJM Evid 2023, 2, EVIDoa2200225. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Brady, M.F.; Wenzel, L.; Fleming, G.F.; Huang, H.Q.; DiSilvestro, P.A.; Fujiwara, K.; Alberts, D.S.; Zheng, W.; Tewari, K.S.; et al. Randomized trial of intravenous versus intraperitoneal chemotherapy plus bevacizumab in advanced ovarian carcinoma: an NRG oncology/Gynecologic Oncology Group study. J Clin Oncol 2019, 37, 1380–1390. [Google Scholar] [CrossRef] [PubMed]
- Lesnock, J.L.; Darcy, K.M.; Tian, C.; Deloia, J.A.; Thrall, M.M.; Zahn, C.; Armstrong, D.K.; Birrer, M.J.; Krivak, T.C. BRCA1 expression and improved survival in ovarian cancer patients treated with intraperitoneal cisplatin and paclitaxel: a Gynecologic Oncology Group Study. Br J Cancer 2013, 108, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Petousis, S.; Kahramanoglu, I.; Appenzeller-Herzog, C.; Angeles, M.A.; Margioula-Siarkou, C.; Kacperczyk-Bartnik, J.; Bilir, E.; Chatzakis, C.; Caruso, G.; Bizzarri, N.; et al. PARP inhibitor maintenance after first-line chemotherapy in advanced-stage epithelial ovarian cancer: A systematic review and meta-analysis. JAMA Netw Open 2025, 8, e2541648. [Google Scholar] [CrossRef] [PubMed]
- Katsumata, N; Yasuda, M; Isonishi, S; Takahashi, F; Michimae, H; et al. Long-term results of dose-dense paclitaxel and carboplatin versus conventional paclitaxel and carboplatin for treatment of advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer (JGOG 3016): a randomised, controlled, open-label trial. Lancet Oncol 2013, 14(10), 1020–6. [Google Scholar] [CrossRef] [PubMed]
- Oza, AM; Cook, AD; Pfisterer, J; Embleton, A; Ledermann, JA; et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial. Lancet Oncol 2015, 16(8), 928–36. [Google Scholar] [CrossRef] [PubMed]
- Burger, RA; Brady, MF; Bookman, MA; Fleming, GF; Monk, BJ; et al. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med 2011, 365(26), 2473–83. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schema of iPocc trial. AUC, area under the concentration–time curve; NAC, neoadjuvant chemotherapy; IDS, interval debulking surgery; PFS, progression-free survival; OS, overall survival; QOL, quality of life; IP, intraperitoneal; IV, intravenous.
Figure 1.
Schema of iPocc trial. AUC, area under the concentration–time curve; NAC, neoadjuvant chemotherapy; IDS, interval debulking surgery; PFS, progression-free survival; OS, overall survival; QOL, quality of life; IP, intraperitoneal; IV, intravenous.
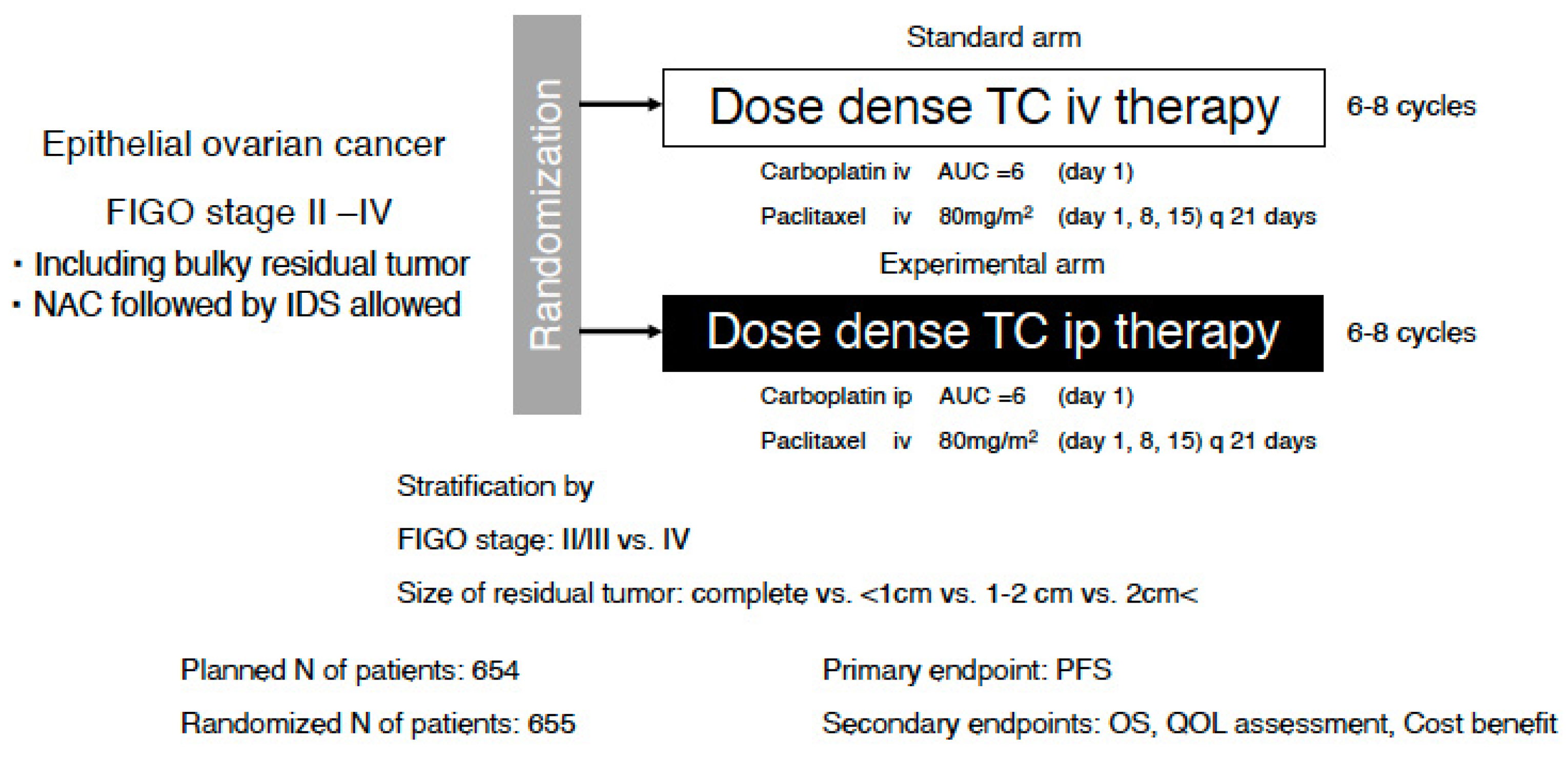
Figure 2.
Schema of GOG-252 trial. AUC, area under the concentration–time curve; PFS, progression-free survival; OS, overall survival; QOL, quality of life; IP, intraperitoneal; IV, intravenous.
Figure 2.
Schema of GOG-252 trial. AUC, area under the concentration–time curve; PFS, progression-free survival; OS, overall survival; QOL, quality of life; IP, intraperitoneal; IV, intravenous.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



