
Submitted:
24 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Brucellosis is a common zoonotic infection in India, caused by a facultative intracellular, Gram-negative coccobacillus and frequently presents with nonspecific symptoms. This study aimed to assess serum cytokine levels (IL-6, IL-10, IFN-γ, and IL-2) by ELISA and to correlate them with inflammatory markers (ESR, and CRP)in patients with suspected brucellosis presenting with rheumatoid arthritis–like manifestations and polyarthralgia. This study included 111 patients, comprising 72 brucellosis-positive arthritis patients and 39 brucellosis- negative arthritis patients as controls. In this study, we investigated the variation in levels of four cytokines (IL-2, IL-6, IL-10 and IFN-γ) among brucellosis-positive and brucellosis-negative arthritis patients and their relationship with clinical parameters. The mean serum levels of IL-2 and IL-10 were markedly higher in brucellosis-positive arthritis patients. As brucellosis is an important cause of inflammatory arthritis, characterized by elevated serum levels of IL-10 and IL-2 and increased inflammatory markers, including ESR and CRP, along with relatively lower levels of IFN-γ and IL-6, which are linked to the inflammatory rheumatoid arthritis. The observed associations with raw dairy consumption, contact with unvaccinated livestock, and direct animal exposure highlight the need for early diagnosis, effective livestock immunization programs, and strengthened One Health–based public health interventions to reduce disease burden
Keywords:
Brucellosis
; arthritis
; ELISA
; cytokines
; ESR
; CRP
1. Introduction
Brucella is an intracellular-bacteria that causes brucellosis, a zoonotic infection common worldwide. It is a facultative, Gram-negative intracellular pathogen that can evade the host's immune system, leading to chronic infections in both humans and animals. In humans, brucellosis can present with a variety of symptoms, including fever and musculoskeletal issues such as arthritis [1]. Due to the non-specific symptoms of brucellosis, which can overlap with rheumatologic complications, accurate diagnosis is essential; for this, haematological parameters and inflammatory markers play a crucial role [2].
To understand the host immune responses and to differentiate infectious from non-infectious inflammatory diseases, the study of cytokines has emerged as a promising approach. Although both IFN-γ and IL-6 have been thoroughly studied in autoimmune arthritis, their function in Brucella-associated arthritis is still unidentified. Pro-inflammatory cytokines such as IL-6, IL-2, and IFN-γ play key roles in acute infection, while anti-inflammatory cytokines such as IL-10 show immunological regulation during chronic infection. In the case of brucellosis, IL-2 is essential for the growth of T cell populations, especially Th1 cells, which are necessary for efficient immune responses against intracellular infections [3]. Interleukin-10 (IL-10), a cytokine that reduces inflammation and controls immune responses to limit excessive tissue damage. IL-10 has been demonstrated to reduce the bactericidal activity of macrophages and prevent the synthesis of pro-inflammatory cytokines in brucellosis, which promotes the persistence of bacteria [4]. IL-6 has been shown to facilitate the development of CD8+ T cells and increase the bactericidal activity of macrophages, thereby aiding in the removal of Brucella abortus in the context of brucellosis, while Th1 cells release the cytokine interferon-gamma (IFN-γ), which stimulates macrophages to eliminate intracellular infections. IFN-γ is essential for regulating Brucella infection in brucellosis because it increases macrophage bactericidal activity and encourages naive T cells to differentiate into Th1 effector cells [5]. In this study, we aimed to investigate the levels of various cytokines (IL-6, IL-10, IFN-γ, and IL-2) in brucellosis patients suffering with arthritis, and to identify the perfect biomarker to enquire about the severity of the illness.
2. Materials and Methods
2.1. Patients
This study is a cross-sectional investigation conducted at JNMCH, AMU, Aligarh, from April 2023 to October 2025. A total of 111 patients presenting with arthritis and polyarthralgia were included in this study after obtaining appropriate informed consent.
2.2. Sample Collection
This study included 111 patients, comprising 72 brucellosis-positive arthritis patients and 39 brucellosis- negative arthritis patients. 5 ml of blood was taken from each individual, and the serum was extracted. Additionally, a pre-designed questionnaire was used to gather demographic data and risk factors associated with the disease.
2.3. Laboratory Diagnosis
SAT (Serum Agglutination Test): SAT was performed to detect anti-Brucella antibodies by serially diluting serum samples and adding Brucella antigen. The SAT antigen was purchased from Tulip Diagnostics, Goa. For the test, the serum samples were diluted from one tube to another with 0.25% phenol saline, from 1:5 to 1:320. Each sample was then incubated for 24 hours at 37°C with one drop of Brucel antigen. After 24 hours, agglutination was observed. The highest dilution showing agglutination was recorded as the 1:160 titre, considered positive [6].
RBPT (Rose Bengal Plate Test): RBPT, a rapid slide agglutination test, was done using antigen received from IVRI, Izatnagar, Bareilly. Equal volumes (30 μL) of serum and antigen were mixed for 4 minutes, and visible agglutination indicated a positive result [7].
ELISA (Enzyme-linked Immunosorbent Assay): ELISA was designed as an indirect method of examining the patient’s immune system to find antibodies that confirm prior and present exposure to the disease. To perform ELISA for IgG & IgM antibodies, we used coated microplates, reagents, positive and negative controls, a calibrator, and, most importantly, patient sera, then processed according to the manufacturer’s instructions (ELISA IgG CALBIOTECH & ELISA IgM CALBIOTECH) After performing the test, we had to quantify specific antibodies generated in response to human brucellosis at an optical density of 450 and 655 nm, and then the result was interpreted accordingly. We have successfully identified antibodies in the patient’s serum after performing assay.
RT-PCR: In our study, we employed real-time PCR to amplify a 731-base-pair segment of the omp31 gene from Brucella. We performed RT-PCR tests in a total volume of 20 µl. Primers and fluorescently labelled probes were used, and reaction was carried out in a BIO-RAD device. Positive control was obtained from ICAR, Mathura. After completion of RT-PCR cycles, a graph was seen.
Conventional PCR: In our study, primers targeting the IS711 gene of B. abortus were used for conventional PCR. A total of 12.5 µl volume Master mix was prepared in a Master Mix tube, then reaction was conducted in a thermal cycler. Afterwards a 1.5% agarose gel stained with ethidium bromide was employed for gel electrophoresis to determine positive PCR results.
Blood Culture: We have taken 5 ml blood samples from OPD/IPD patients with suspected symptoms of brucellosis and injected them into FA Plus bottles for incubation. Blood cultures were performed using the BacT/ALERT system (bioMérieux, Inc.) according to the manufacturer’s instructions.
Cytokine analysis: The concentration levels of various cytokines (IL-6, IL-10, IL-2, and IFN-γ) were determined using the commercially available ELISA kits (Diaclone, France). The tests were performed according to the manufacturer's instructions. Briefly, 100 µL of standards, controls, and patient samples were added to pre-coated wells along with 50 µL of biotinylated antibody and incubated for 1 hours at room temperature. After washing three times, 100 µL of streptavidin-HRP was added and incubated for 30 min at room temperature. Following another wash, 100 µL of TMB substrate was added and incubated for 12–15 min in the dark. The reaction was stopped by adding 100 µL stop solution. The optical density was measured at 450 nm as well as dual (450 nm & 655nm). The concentration of each cytokine was calculated by comparing the O.D. of each sample with the standards provided in the kit. A standard curve was constructed with the Human cytokine concentration on the y-axis and absorbance on the x-axis. Cytokine levels were calculated from the same.
2.4. Statistical Analysis
Chi-square tests, multiple logistic regression and independent t-tests were used to compare epidemiological variables, clinical symptoms, haematological, biochemical parameters and cytokine profiles.
3. Results
Subsections
Out of 111 patients presenting with joint pain and polyarthralgia, 72 (64.9%) were serologically positive for brucellosis. As shown in Figure 1, among the brucellosis-positive arthritis patients, 37 (51.3%) were positive for ELISA IgG, 24 (33.3%) for ELISA IgM, 27 (37.5%) for Rose Bengal Plate Test (RBPT), 23 (31.9%) for Standard Agglutination Test (SAT), 12 (16.6%) for RT-PCR, 7 (9.7%) for conventional PCR, and 2 (2.7%) for culture, respectively. In addition, 39 brucellosis-negative arthritis patients were also included as controls.
Patients were categorized into acute and chronic brucellosis based on disease duration. The main demographic and clinical characteristics of the 72 Brucella-positive cases are summarized in Table 1. The majority of patients were female, with a male-to-female ratio of 7:17. The age of the patients ranged from 15 to 80 years, with the highest prevalence (44.4%) observed in the 20–40-year age group. The most common risk factor among Brucella-positive arthritis patients was a history of close contact with animals (69.5%), and most patients belonged to rural areas. Arthralgia was the most frequent symptom, reported in 100% of cases, followed by body ache (70.8%), joint pain (69.4%), muscle pain (50%), fever (40.2%), and fatigue (26.3%).
Comparison of cytokine levels & other biochemical parameters between Brucella-positive arthritis patients and controls: As demonstrated in Table 2, the brucellosis-positive patients group had considerably higher mean levels of IL-10 (1.0±0.5) and IL-2 (4.5±6.6) than the control group, and the mean levels of IL-6 (2.4±8.9) and IFN-γ (1.8±3.3) were higher in the control group than in the Brucellosis-positive arthritis individuals. Brucella-positive arthritis patients showed slightly elevated ESR (21.8±11.4) and CRP (4.5±6.7), suggesting a moderate but consistent inflammatory response, although there were no significant haematological differences between the groups, as indicated by comparable haemoglobin (Hb) and ALP levels. There were no statistically significant changes in any of the variables (p > 0.05); however, ESR had the lowest p-value (.093), but still not significant.
As shown in Table 3, a series of chi-square tests were performed to examine associations between Brucella seropositivity, various risk factors and clinical symptoms. Sex distribution value (χ² = 1.308, p = .253), demonstrating that Brucella exposure risk is not limited to a particular gender. None of the associations reached conventional statistical significance (all p > .05). The largest χ² value observed was for vaccination status (χ²(3) = 6.94, p = .074), which approached but did not reach statistical significance. Other variables with non-significant χ² included cow contact (χ²(1) = 2.35, p = .126) which is consistent with known B. abortus transmission patterns, but other livestock exposures indicated no significant relationships, socio-economic status (χ²(1) = 2.48, p = .115), and shared water source (χ²(3) = 5.72, p = .126). Symptoms such as fever, malaise, joint pain, and weakness were similarly distributed, showing diagnostic overlap between the healthy group and Brucella-positive arthritis patients.
As shown in Table 4, a binary logistic regression was performed to examine whether IL-6, IL-10, IL-2, and IFN-γ predict seropositivity for Brucella. The full model did not significantly predict sero status, χ²(4) = 3.53, p = .473, and none of the cytokine predictors were statistically significant (all p > .05). The initial classification suggested poor specificity (0%) despite perfect sensitivity (100%), with overall accuracy 51.9%. These results indicate no evidence in the present sample that the tested cytokines are associated with Brucella seropositivity; however, the analysis is limited by sample size and model performance.
4. Discussion
Human brucellosis is still a neglected but significant zoonotic disease. Recent data indicate that there are about 2.1 million new cases in humans each year, with substantial regional variation in incidence [8]. Regional, livestock reservoir, monitoring intensity, and diagnostic approach each possess a significant impact on prevalence estimates. Close human-animal contact, the consumption of unpasteurized dairy products, and inadequate implementation of animal surveillance are among the causes of the highest burdens reported in endemic areas, especially in the Middle East, South Asia, the Mediterranean basin, and sub-Saharan Africa [9,10].
Brucellosis can cause major complications, if not diagnosed properly, as it affects several organ systems, including the central nervous system, cardiovascular system, gastrointestinal system, genitourinary system, hepatic system, and musculoskeletal system [11]. Peripheral arthritis, sacroiliitis, spondylitis, and osteomyelitis are examples of musculoskeletal disorders that can result in severe issues, in which osteoarticular involvement is the most frequent primary complication [12]. To determine the relationship between Brucella and arthritis, diagnosis confirmation is essential, as the disease presents with nonspecific clinical symptoms that often resemble those of other rheumatologic conditions [13]. According to a study by Turan et al. (2011), osteoarticular complications occurred in most of the brucellosis-positive patients, with a high percentage of 47%[14]. In another study by Ebrahimpour et al. (2017), demonstrated that 10.8% of the brucellosis-positive patients with focal problems had polyarthritis [15]. Another study by Colmenero et al. (1996) shows that bacterial localisation in the synovial and osseous tissues causes brucella arthritis and spondylitis, leading to persistent inflammation and joint deterioration, as they demonstrated that 66% of the patients suffered with Osteoarticular complications [16]. Ariza et al. (1993) also emphasized the high prevalence of musculoskeletal symptoms in brucellosis [17]. The present study found that a significant proportion (45.5%) of brucellosis-positive patients presented with arthralgia and arthritis.
In our study, we found that females showed a higher positivity rate (70.8%) among the Brucella-positive arthritis patients than males. This data showed similarity with previous research conducted by Gotuzzo et al. (1987)[18]. According to our study, most Brucella-positive arthritis patients had a history of close contact with animals (69.5%), and they mainly came from rural areas (54.2%), highlighting the occupational and environmental exposure linked to brucellosis. These findings are similar to those of Kumari et al. (2023)[19], who reported higher brucellosis prevalence among rural populations with a history of animal contact. A major risk factor identified in our study was the presence of unvaccinated animals (79.1%), which play an important role in the transmission of the disease, as also demonstrated by Gwida et al. (2010)[20] and Corbel (2006)[21]. In our study, consumption of raw dairy products was reported by 56.9% of Brucella-positive arthritis patients, supporting findings by Faddane et al. (2022)[22] demonstrated that unpasteurised milk is a key route of transmission of brucellosis. Additionally, exposures such as keeping animals near sleeping areas (37.5%), contact with cows (29.1%), and sharing water sources with animals (20.8%) were common, similar to studies reported by Zhang et al. (2019)[23] and Mantur & Amarnath (2008)[24], emphasising the importance of close human–animal contact in brucellosis transmission. We found a strong directional trend that indicated a connection with cow contact (p =.126). This pattern aligns with the known epidemiology of B. abortus, which is mainly associated with cattle, although this association is not statistically significant. Environmental factors, such as animals near sleeping areas and shared water sources, showed positive trends linked to disease transmission (Gwida et al., 2010)[20].
Inflammatory markers show a clinically significant trend towards elevated values in Brucella-positive patients, especially ESR and CRP [25]. In our study, Brucella-positive arthritis patients had higher levels of inflammatory markers such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), which indicate active systemic inflammation. This data showed similarity with previous research conducted by S Almohrij et al. (2025)[26], in which they demonstrated that elevated ESR and CRP in Brucella-positive arthritis patients served as more useful indicators of infection. According to another study, by Bosilkovski et al. (2004)[27], both acute and chronic brucellosis are frequently associated with elevated CRP and ESR, which are especially linked to osteoarticular involvement. These indicators show persistent inflammatory activity. However, another study by Colmenero et al. (1996)[16], demonstrated that ESR and CRP elevation are associated with tissue involvement and the severity of the disease, particularly in patients with sacroiliitis, spondylitis, and arthritis.
In our study, cytokine analysis showed higher IL-10 and IL-2 levels in Brucella-positive arthritis patients, suggesting that Brucella infection influences immune-modulating and T-cell-related responses. Conversely, IL-6 and IFN-γ levels were somewhat lower, indicating a reduced Th1 and pro-inflammatory response. Overall, the immunopathology of Brucella infection aligns with these data.
According to our analysis, brucellosis-positive arthritis patients had elevated levels of IL-10 and IL-2. IL-10, a crucial anti-inflammatory cytokine, can reduce pro-inflammatory cytokine production and suppress macrophage activation, and helps Brucella to survive inside the host cells. Similar to our findings, research conducted by Saadati et al. (2019)[1], demonstrated that a higher level of IL-10 cytokine played an important role in the brucellosis-positive arthritis patients. Another elevated cytokine in brucellosis-positive arthritis patients was IL-2, which increased T-cell activation, T-cell proliferation and immunological modulation. Our study is showing similarity with the research conducted by Tang et al. (2021)[28], in which they demonstrated that a higher level of IL-2 cytokine is mostly present in patients with acute brucellosis.
On the other hand, opposite cytokine effects were observed, in which we detected a lower levels of IFN-γ and IL-6 cytokines in the Brucella-positive arthritis patients. Our findings are corroborated by the study of Murphy et al. (2001)[29], which demonstrated that reduced IFN-γ production may be partly due to elevated IL-10, as IL-10 can affect the production of IFN-γ through altering the antigen-presenting capacity of macrophages. Another study by GhaznaviRad et al. (2017)[30] showed that decreased IFN-γ responses were presented in individuals with chronic brucellosis, suggesting that insufficient Th1 responses may play a role in joint localisation and infection persistence. Chronic and relapsing brucellosis has also been associated with decreased IFN-γ production. Another cytokine with a lower level was IL-6. While IL-6 is frequently increased in acute infections, it also contributes to the elimination of bacteria and the control of inflammatory reactions. Our Brucella-positive arthritis patients with lower IL-6 levels might be the result of IL-10 mediated reduction of macrophage activity, which favours persistent infection over efficient inflammatory clearance. Our study is supported by the previous research in which Brucella-negative inflammatory arthritis, especially rheumatoid arthritis, increased levels of IL-6 and IFN-γ are frequently observed, indicating ongoing joint inflammation [31]. On the other hand, our patients with Brucella-positive arthritis had higher levels of IL-2 and IL-10 and lower levels of IFN-γ and IL-6. Overall, the data reveal that inflammatory and cytokine responses were largely comparable amongst groups, demonstrating a variable host response pattern and explaining the complexity of brucellosis-related immunological alterations.
5. Conclusions
This study identifies brucellosis as an important cause of inflammatory arthritis. Brucella-positive arthritis patients exhibited elevated levels of IL-10 and IL-2, along with increased ESR and CRP, reflecting ongoing inflammatory activity. In contrast, relatively lower levels of pro-inflammatory cytokines IFN-γ and IL-6 may indicate chronic immune adaptation in affected individuals. These results demonstrate that Brucella-positive arthritis has a different cytokine profile than Brucella-negative inflammatory arthritis, demonstrating the biological significance and importance of our study. Key risk factors included close contact with animals, exposure to unvaccinated livestock, and consumption of raw dairy products. Collectively, these findings underscore the importance of animal vaccination programs, early diagnosis, and strengthened public health control measures, particularly within a One Health framework, to reduce the burden of brucellosis-associated arthritis.
Funding
This study is part of a project funded by the Indian Council of Medical Research, New Delhi. (Project ID: ZON/65/2022/ECD-II).
Institutional Review Board Statement
The study was approved by the Institutional Ethics Committee, Faculty of Medicine, AMU, Aligarh (IEC JNMC/270 Dated 01/03/21).
Acknowledgments
We appreciate the Indian Council of Medical Research supporting this research. We also thank our institution's Viral Research and Diagnostic Laboratory, Department of Microbiology, for providing study infrastructure. We acknowledge Dr. Syed Ghazanfar Ali, Mr. Sivan, Ms. Shibli Javed, and Mr. Sanaullah for their assistance with various technical aspects of the study.
Conflicts of Interest
The authors declare that they have no known competing interest.
References
- Saadati, N; Khodashahi, M; Naghibzadeh, B; Khodashahi, R. Relation between cytokines and Brucella arthritis, spondylitis, and sacroiliitis. Rheum Res. 2019, 4, 57–61. [Google Scholar] [CrossRef]
- Spernovasilis, N; Karantanas, A; Markaki, I; Konsoula, A; Ntontis, Z; Koutserimpas, C; et al. Brucella spondylitis: current knowledge and recent advances. J Clin Med. 2024, 13, 595. [Google Scholar] [CrossRef]
- Franzoni, G; Signorelli, F; Donniacuo, A; Schiavo, L; Napoletano, M; De Matteis, G; et al. Exploring potential cytokine profiles as diagnostic biomarkers for brucellosis in Mediterranean buffaloes. Front Vet Sci. 2025, 12, 1583858. [Google Scholar] [CrossRef]
- Zafari, P; Zarifian, A; Alizadeh-Navaei, R; Taghadosi, M; Rafiei, A. Association between polymorphisms of cytokine genes and brucellosis: a comprehensive systematic review and meta-analysis. Cytokine 2020, 127, 154949. [Google Scholar] [CrossRef]
- Skyberg, JA; Thornburg, T; Kochetkova, I; Layton, W; Callis, G; Rollins, MF; et al. IFN-γ-deficient mice develop IL-1-dependent cutaneous and musculoskeletal inflammation during experimental brucellosis. J Leukoc Biol. 2012, 92, 375–87. [Google Scholar] [CrossRef]
- Copur, B; Pasa, O. The role of the serum tube agglutination test in the monitoring of human brucellosis: evaluation of post-treatment SAT titers. Rev Assoc Med Bras (1992) 2022, 68, 1234–9. [Google Scholar] [CrossRef]
- Patil, DP; Ajantha, GS; Shubhada, C; Jain, PA; Kalabhavi, A; Shetty, PC; et al. Trend of human brucellosis over a decade at tertiary care centre in North Karnataka. Indian J Med Microbiol. 2016, 34, 427–32. [Google Scholar] [PubMed]
- Laine, CG; Johnson, VE; Scott, HM; Arenas-Gamboa, AM. Global estimate of human brucellosis incidence. Emerg Infect Dis. 2023, 29, 1789–97. [Google Scholar] [CrossRef] [PubMed]
- Sherasiya, R. Global prevalence of human brucellosis: a systematic review and meta-analysis. Res Sq 2024. [Google Scholar] [CrossRef]
- Suresh, KP; Patil, SS; Nayak, A; Dhanze, H; Rajamani, S; Shivamallu, C; et al. Prevalence of brucellosis in livestock of African and Asian continents: a systematic review and meta-analysis. Front Vet Sci. 2022, 9, 923657. [Google Scholar] [CrossRef] [PubMed]
- Solís García del Pozo, J; Solera, J. Systematic review and meta-analysis of randomized clinical trials in the treatment of human brucellosis. PLoS One 2012, 7, e32090. [Google Scholar] [CrossRef] [PubMed]
- Buzgan, T; Karahocagil, MK; Irmak, H; Baran, AI; Karsen, H; Evirgen, O; et al. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Int J Infect Dis. 2010, 14, e469–78. [Google Scholar] [CrossRef]
- Pappas, G; Akritidis, N; Bosilkovski, M; Tsianos, E. Brucellosis. N Engl J Med. 2005, 352, 2325–36. [Google Scholar] [CrossRef]
- Turan, H; Serefhanoglu, K; Karadeli, E; Togan, T; Arslan, H. Osteoarticular involvement among 202 brucellosis cases identified in Central Anatolia region of Turkey. Intern Med. 2011, 50, 421–28. [Google Scholar] [CrossRef]
- Ebrahimpour, S; Bayani, M; Moulana, Z; Hasanjani Roushan, MR. Skeletal complications of brucellosis: a study of 464 cases in Babol, Iran. Caspian J Intern Med. 2017, 8, 44–8. [Google Scholar]
- Colmenero, JD; Reguera, JM; Martos, F; Sánchez-de-Mora, D; Delgado, M; Causse, M; et al. Complications associated with Brucella melitensis infection: a study of 530 cases. Medicine (Baltimore) 1996, 75, 195. [Google Scholar] [CrossRef]
- Ariza, J; Pujol, M; Valverde, J; Nolla, JM; Rufí, G; Viladrich, PF; et al. Brucellar sacroiliitis: findings in 63 episodes and current relevance. Clin Infect Dis. 1993, 16, 761–5. [Google Scholar] [CrossRef]
- Gotuzzo, E; Seas, C; Guerra, JG; Carrillo, C; Bocanegra, TS; Calvo, A; et al. Brucellar arthritis: a study of 39 Peruvian families. Ann Rheum Dis. 1987, 46, 506–9. [Google Scholar] [CrossRef] [PubMed]
- Kumari, R; Kalyan, RK; Jahan, A; Jain, A; Kumar, P; Gupta, KK; et al. Human brucellosis: an observational study from a tertiary care centre in North India. Cureus 2023, 15, e42980. [Google Scholar] [CrossRef]
- Gwida, M; Al Dahouk, S; Melzer, F; Rösler, U; Neubauer, H; Tomaso, H. Brucellosis – regionally emerging zoonotic disease? Croat Med J. 2010, 51, 289–95. [Google Scholar] [CrossRef]
- Corbel, MJ. Brucellosis in humans and animals; World Health Organization: Geneva, 2006. [Google Scholar]
- Faddane, K; Moumni, H; Cherkaoui, I; Lakranbi, M; Hamdi, S; Ezzikouri, S; et al. Seroprevalence of human brucellosis in Morocco and associated risk factors. Vet World 2022, 15, 2224–33. [Google Scholar] [CrossRef]
- Zhang, N; Zhou, H; Huang, DS; Guan, P. Brucellosis awareness and knowledge in communities worldwide: a systematic review and meta-analysis of 79 observational studies. PLoS Negl Trop Dis. 2019, 13, e0007366. [Google Scholar] [CrossRef]
- Mantur, BG; Amarnath, SK. Brucellosis in India – a review. J Biosci. 2008, 33, 539–47. [Google Scholar] [CrossRef] [PubMed]
- Xu, N; Dong, X; Yao, Y; Guan, Y; Chen, F; Zheng, F; et al. Improved early detection of focal brucellosis complications with anti-Brucella IgG. J Clin Microbiol. 2020, 58, e00903-20. [Google Scholar] [CrossRef]
- Almohrij, S; Bahabri, I; Alghamdi, RM; Bosaeed, M. Brucella septic arthritis: a case series and review of the literature. J Infect Public Health 2025, 18, 102993. [Google Scholar] [CrossRef]
- Bosilkovski, M; Krteva, L; Caparoska, S; Dimzova, M. Osteoarticular involvement in brucellosis: study of 196 cases in the Republic of Macedonia. Croat Med J. 2004, 45, 727–33. [Google Scholar]
- Tang, Y; Ma, C; Sun, H; Yang, S; Yu, F; Li, X; et al. Serum levels of seven general cytokines in acute brucellosis before and after treatment. Infect Drug Resist. 2021, 14, 5501–10. [Google Scholar] [CrossRef]
- Murphy, EA; Sathiyaseelan, J; Parent, MA; Zou, B; Baldwin, CL. Interferon-gamma is crucial for surviving a Brucella abortus infection in both resistant C57BL/6 and susceptible BALB/c mice. Immunology 2001, 103, 511–18. [Google Scholar] [CrossRef] [PubMed]
- Ghaznavi Rad, E; Khosravi, K; Zarinfar, N; Mosayebi, G. Reduced IFN-γ production in chronic brucellosis patients. Iran J Immunol. 2017, 14, 215–22. [Google Scholar]
- Lama, M; Sarkar, R; Ghosh, B. Serum Cytokine Profiles in Patients with Rheumatoid Arthritis Before and After Treatment with Methotrexate. Journal of Interferon & Cytokine Research 2023, 43, 344–50. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Positive cases by different diagnostic methods in Brucellosis-positive arthritis patients (n=72).
Figure 1.
Positive cases by different diagnostic methods in Brucellosis-positive arthritis patients (n=72).
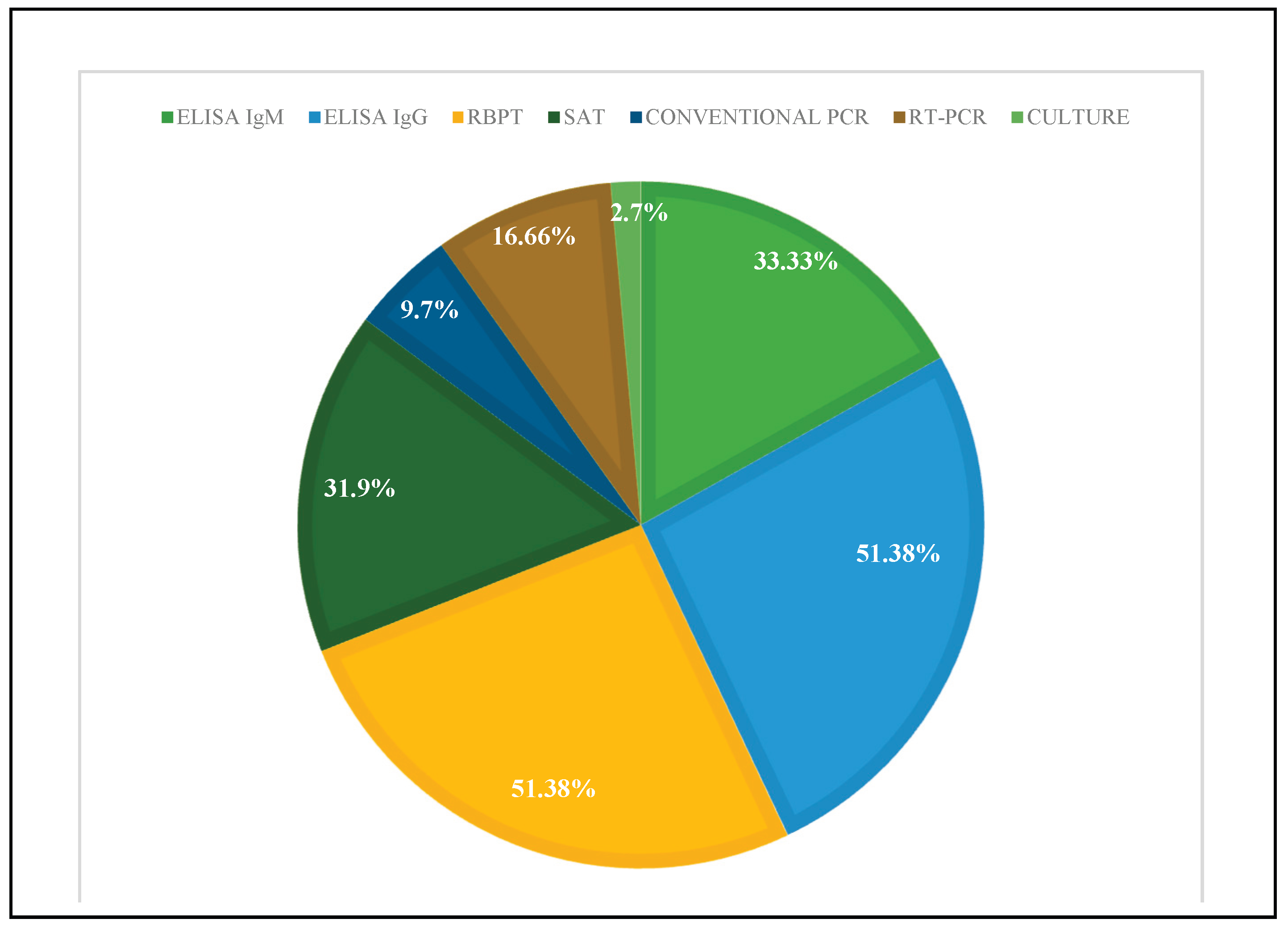

Table 1.
Demographic and clinical features of Brucellosis-positive Arthritis patients (n=72).
|
Clinical indicators Sex Male Female |
Brucella-positive arthritis patients (n=72) 21 (29.1%) 51 (70.8%) |
|
Age (Years) <20 20-40 40-60 60-80 |
4 (5.5%) 32 (44.4%) 30 (41.6%) 6 (8.3%) |
|
Locality Rural Urban |
39 (54.2%) 33 (45.8%) |
|
Animal contact Yes No |
50 (69.5%) 22 (30.5%) |
|
Symptoms Fever Malaise Sweating Anorexia Muscle pain Yellow skin Arthralgia Joint pain Epididymalocharditis Endocardititis Headache Fatigue Weakness Body ache Breathlessness Testicular swelling Confusion |
29 (40.2%) 6 (8.3%) 14 (19.4%) 9 (12.5%) 36 (50%) 7 (9.7%) 72 (100%) 50 (69.4%) 5 (6.9%) 2 (2.7%) 18 (25%) 19 (26.3%) 24 (33.3%) 51 (70.8%) 6 (8.3%) 3 (4.1%) 4 (5.5%) |
Table 2.
Comparison of cytokines levels & other biochemical parameters between Brucella-positive arthritis patients and controls (n=111).
Table 2.
Comparison of cytokines levels & other biochemical parameters between Brucella-positive arthritis patients and controls (n=111).
| Variable | Brucella− (n) | Mean (SD) | Brucella+ (n) | Mean (SD) | P value |
|---|---|---|---|---|---|
| Hemoglobin (g/dL) | 39 | 10.33 (2.27) | 71 | 10.49 (2.03) | .697 |
| TLC (/mm³) | 39 | 4,133 (4,445) | 71 | 4,724 (11,697) | .763 |
| ESR (mm/hr) | 38 | 18.21 (9.18) | 71 | 21.86 (11.46) | .093 |
| ALP (IU/L) | 37 | 102.6 (54.9) | 68 | 104.9 (40.9) | .813 |
| CRP (mg/dL) | 38 | 3.84 (5.38) | 71 | 4.57 (6.71) | .561 |
| RA factor (IU/mL) | 37 | 13.55 (51.01) | 70 | 13.07 (38.82) | .957 |
| IL-6 (pg/mL) | 39 | 2.45 (8.99) | 72 | 1.47 (2.54) | .386 |
| IL-10 (pg/mL) | 39 | 0.96 (0.47) | 70 | 1.02 (0.55) | .582 |
| IL-2 (pg/mL) | 39 | 3.14 (4.42) | 72 | 4.52 (6.66) | .250 |
| IFN-γ (pg/mL) | 38 | 1.83 (3.30) | 72 | 1.57 (2.74) | .652 |
Table 3.
Association between Brucella seropositivity, various risk factors and clinical symptoms (n=72).
Table 3.
Association between Brucella seropositivity, various risk factors and clinical symptoms (n=72).
| Variable (row) | χ² (Pearson) | df | p (2-tailed) |
|---|---|---|---|
| Sex | 1.308 | 1 | .253 |
| Cow (contact) | 2.347 | 1 | .126 |
| Buffalo (contact) | 0.910 | 1 | .340 |
| Goats (contact) | 0.234 | 1 | .629 |
| Duration (exposure) | 1.898 | 1 | .168 |
| Native place | 0.460 | 1 | .498 |
| Socio-economy | 2.483 | 1 | .115 |
| Smoker | 2.862 | 3 | .413 |
| Drinker | 2.629 | 2 | .269 |
| Recent travel | 2.695 | 3 | .441 |
| Raw meat consumption | 3.199 | 3 | .362 |
| Raw dairy consumption | 3.422 | 3 | .331 |
| Fever (symptom) | 3.173 | 3 | .366 |
| Malaise | 3.318 | 3 | .345 |
| Joint/back pain | 2.501 | 3 | .475 |
| Weakness in limbs | 3.985 | 3 | .263 |
| Bodyache | 3.824 | 3 | .281 |
| Rashes | 3.051 | 3 | .384 |
| Neck stiffness | 2.957 | 3 | .398 |
| Vaccinated | 6.943 | 3 | .074 |
| Animals near sleeping area | 5.365 | 3 | .147 |
| Share water source | 5.720 | 3 | .126 |
Table 4.
Logistic Regression analysis to identify the cytokine levels, and seropositivity in Brucella-positive arthritis patients (n=72).
Table 4.
Logistic Regression analysis to identify the cytokine levels, and seropositivity in Brucella-positive arthritis patients (n=72).
| Predictor | B (β) | SE | Wald | df | p | Exp(B) | Score | Score p |
|---|---|---|---|---|---|---|---|---|
| Constant | 0.074 | 0.193 | 0.148 | 1 | .700 | 1.08 | — | — |
| Cytokine IL-6 | — | — | — | — | — | — | 0.962 | .327 |
| Cytokine IL-10 | — | — | — | — | — | — | 0.031 | .861 |
| Cytokine IL-2 | — | — | — | — | — | — | 0.682 | .409 |
| Cytokine IFN-γ | — | — | — | — | — | — | 2.071 | .150 |
| Model (Omnibus) | χ² = 3.529 | df = 4 | — | — | p = .473 | — | — | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



