Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Introduction: Parkinson's disease (PD) contributes to increasing disability. Among the environmental, lifestyle, dietary, comorbid, and pharmacological factors that have been studied as potentially modifiable protective or risk factors for PD, physical activity (PA) appears to play a significant role in its prevention. Objectives: To present the latest and comprehensive pooled analyses and evidence and to examine their impact on primary and secondary prevention in patients with PD. Methods: A narrative literature review was conducted, searching articles in several databases, including PubMed, the Cochrane Library, Embase, and Web of Science, from 1992 to December 2025. This review focused on leisure-time and lifestyle-related physical activity (PA) and less on structured exercise in PD, which has been previously described in numerous reports. The definition of lifestyle-related physical activity (LAP) developed by Dunn et al. was used, which defines LAP as a daily accumulation of at least 30 minutes of self-selected activity, encompassing all recreational, occupational, or household activities of at least moderate to vigorous intensity, as well as unplanned (less frequently planned) activities that are part of daily life. Results: The most valuable reports on primary and secondary prevention in PD were identified; the latter was less well represented in the literature. Conclusions: Moderate- and vigorous-intensity physical activity plays a protective role in both reducing the risk of PD and slowing the progression of disability in people with PD, particularly in men. Further research is needed to identify specific types of physical activity that will be particularly recommended for patients with Parkinson's disease.
Keywords:
leisure time physical activity
; lifestyle physical activity
; physical activity
; Parkinson's disease
; PD
; prevention
1. Introduction
Parkinson's disease (PD) is a neurodegenerative disorder exhibiting both motor and non-motor symptoms, which afflicts over eight million people globally, and leads to increasing disability.[1] In the last two decades, one can observe the largest increase in age-standardized incidence rates for PD - according to Huang et al. (2023) in 1990-2019 estimated annual percentage change (EAPC) in PD was 0.61.[2] PD resulted in 5.8 million disability-adjusted life years (DALYs), an increase of 81% since 2000, and caused 329,000 deaths, an increase of over 100% since 2000.[3] Aging and sex are, along with genetics, environment, lifestyle, and immune state, significant factors in the progression of PD. Taking all of the above into account, we should do everything we can to lower the risk of developing PD and delay its progression. One of the cheapest and safest ways of primary and secondary prevention of this condition seems to include daily physical activity.
One can observe in recent years the WHO`s growing interest in the association between physical activity (PA) and health, which resulted in the creation of a Global Action Plan on Physical Activity 2018-2030 (GAPPA) to promote active lifestyles.[4] Also, several scientific articles in the same vein have been published, including the British Journal of Sports Medicine special issue on PA. In 2020, Bull et al. presented recommendations on behalf of the WHO experts, advising all adults to engage in 150-300 minutes of moderate-intensity exercise or 75-150 minutes of vigorous-intensity exercise per week, or an equivalent combination thereof. The recommendations also stressed that regular muscle-strengthening exercise and reducing sedentary behavior offered health benefits to people of all ages, regardless of circumstances, but without explaining precisely how sedentary behavior should be understood.[5]
There are many discrepancies between the definitions of PA, leisure-time PA (LTPA), and lifestyle PA (LPA), although they often overlap. Physical activity (PA) is a broad category - any movement requiring energy (Caspersen et al., 1985)[6], while leisure-time PA (LTPA) is a specific area of PA performed for pleasure/recreation (sport, walking). Lifestyle physical activity (LPA) is a strategy that integrates PA (such as walking/stair climbing) into daily activities to avoid formal exercise, as opposed to scheduled training. The key difference is the scope: PA (all movement), LTPA (leisure-time), and LPA (routine integration). PA refers to any bodily movement produced by skeletal muscles that requires energy expenditure; it includes movement during work, transportation, household chores, and leisure. LTPA refers to PA performed during leisure time, outside of work, outside of household chores, such as playing sports, hiking, dancing, or a dedicated gym session. LPA introduces more movement into daily activities (e.g., walking/cycling for transportation, climbing stairs) as an alternative to structured, often incidental (unplanned) exercise.
The definition of lifestyle PA was created in 1998 by Dunn et al. It states: “Lifestyle physical activity is the daily accumulation of at least 30 minutes of self-selected activities, which includes all leisure, occupational, or household activities that are at least moderate to vigorous in their intensity and could be planned or unplanned activities that are part of everyday life.”[7]
The following two sections discuss the importance of physical activity (PA) in primary prevention of PD and as secondary prevention, i.e., in delaying disability. As for definitions of prevention: primary prevention is action that tries to stop problems from happening, while secondary prevention is action that focuses on early detection of a problem to support early intervention and treatment. This narrative review of literature has been focused on daily and recreational PA.
2. The Importance of Physical Activity in Primary Prevention of PD
In 2009, Hirsch and Farley highlighted that for many years, physical exercise was not widely endorsed as a rehabilitation approach for individuals with idiopathic Parkinson`s disease (PD). Exercise was previously believed to neither improve PD symptoms nor benefit the condition, and in some cases, it was thought to potentially worsen the underlying pathology, leading to its avoidance. However, new scientific and translational research now indicates that non-pharmacological interventions such as physical activity or physiotherapy may have a significantly greater impact on key aspects of PD than previously assumed. Studies conducted with healthy rodents suggest that regular exercise promotes changes in central nervous system plasticity, including enhanced synaptogenesis, increased glucose utilization, angiogenesis, and neurogenesis. While these findings are preliminary and require validation in larger, prospective studies with humans, the authors posited that one of the most pressing challenges for the field lies in effectively translating this emerging knowledge about exercise-based PD treatments into practical applications within community healthcare settings.
3. Material and Methods
This narrative review was conducted to identify all relevant English-language randomized controlled trials (RCTs) available in PubMed, the Cochrane Library, Embase, and Web of Science between 1992 and November 30, 2025. The focus was on physical activity (PA), particularly leisure-time physical activity (LTPA) and lifestyle physical activity (LPA). For this purpose, medical subject headings (MeSH) and full-text searches were employed, involving terms related to physical activity, leisure-time physical activity, lifestyle physical activity, PA risk factors, and prevention.
The exclusion criteria included the following: (1) studies involving participants facing issues unrelated to PA in Parkinson's disease (PD); (2) studies with incomplete datasets or those lacking statistical analysis; (3) studies without control groups or that only included single protocols, abstracts, or conference poster presentations; and (4) studies derived from non-randomized controlled trials. While structured exercises and physical therapy were considered secondary areas of interest, the primary focus was PA's role in PD prevention.
In total, 621 articles were initially identified through the search process. Out of these, 33 met the criteria for inclusion in the meta-analysis. Additionally, nine longitudinal studies and review articles addressing PA's role in the primary prevention of PD were identified during this research.
4. Primary Prevention of PD
The first important report on the significance of PA in the primary prevention of PD comes from 1992. Sasco et al. presented the results of a case-control study conducted from 1916 to 1978 in a cohort of 50,002 men by Harvard and Pennsylvania Universities. The relationship between PA and the risk of PD was assessed in 137 men who developed PD during this time and in 548 people from the control group. The authors found that being a member of a university sports team or performing regular exercise was related to a lower risk of developing PD; however, this relationship was not statistically significant. Practicing sports involving intense physical exercise was statistically strongly associated with a decreased risk of disease, and statistically insignificant for moderate exercise.[10]
Chen et al. discovered in 2005 that higher PA was associated with a lower risk of PD in men. During nearly 20 years of prospective follow-up of 48,574 men and 77,254 women, 252 (men) and 135 (women) instances of PD were identified. Strenuous exercise at an early age was conversely associated with the risk of PD in men. Compared to men who exercised regularly for only 2 months per year, men who exercised vigorously for 10 months had a 60% lower risk of developing PD (RR 0.4; p=0.005).[11]
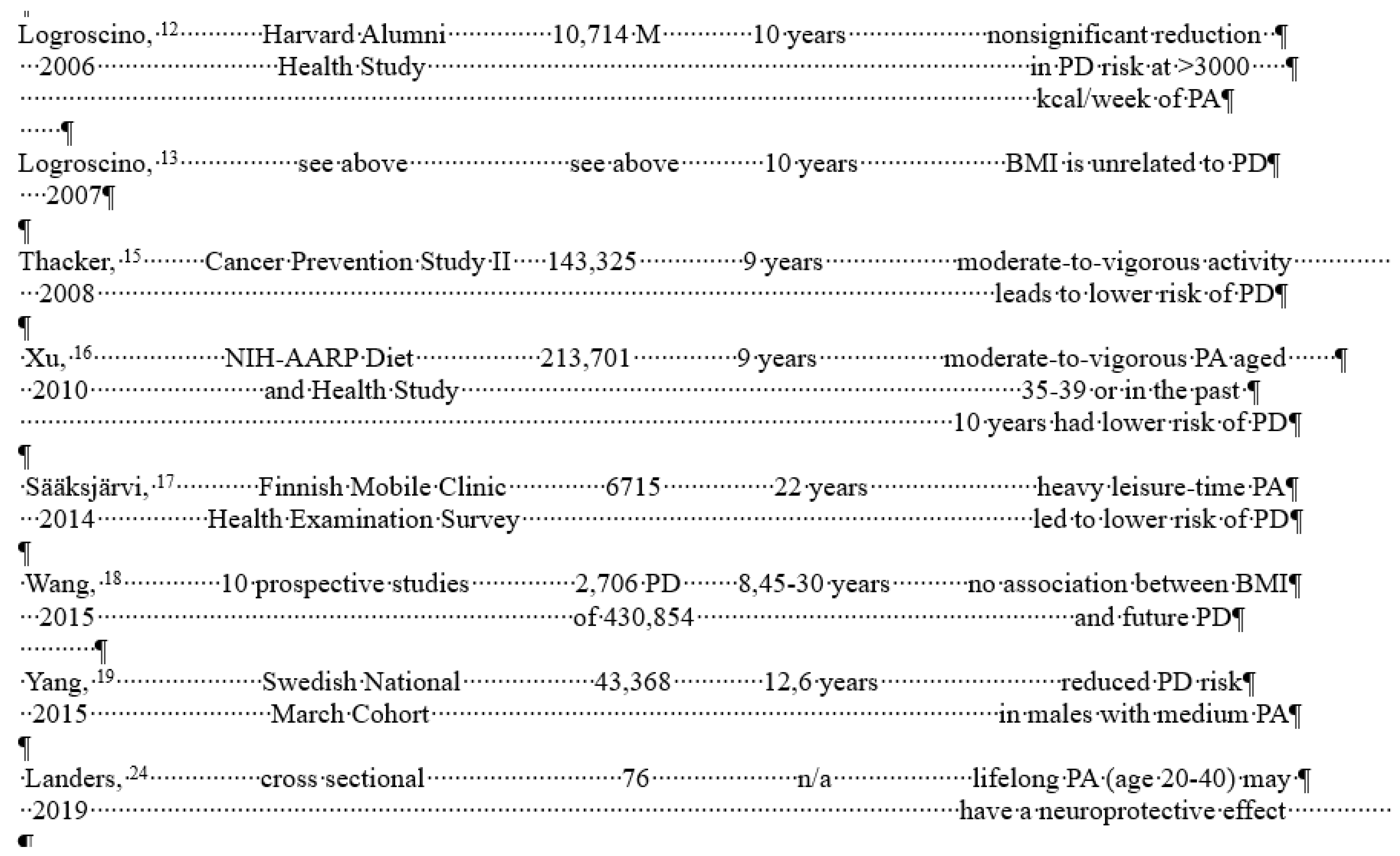
In 2006, Logroscino et al. reported on the relationship between PA and PD in 10,714 men with a mean age of 67.6 years who participated in the Harvard Alumni Health Study and were diagnosed with PD until 1988. Questions were asked about the daily number of blocks of walking (1 block = 235 kJ/week = 56 kcal), climbing stairs (118 kJ/week), and participation in sports and recreational activities in the past week. Energy expenditure was then estimated, and subjects were divided into four groups: <1000, 1000/1999, 2000-2999, or ⩾ 3000 kcal/week. PD cases occurring after 1988 (n = 101) were verified by a follow-up health questionnaire in 1993 and death certificates retrieved through 1997. The relative risks (RR) for PD associated with energy expenditure were: for <1000 =1, for 1000/1099 =1.15 (95% confidence interval (95% CI) 0.71 to 1.88), for 2000- 2999 =0.92 (0.50 to 1.71), and for ⩾ 3000 kcal/week of physical activity - 0.63 (0.36 to 1.12); p for trend = 0.12. In multivariate analysis for walking <5, 5-10, 10-20, and > 20 km/week, the RR (95% CI) was 1, 0.67 (0.37 to 1.23), 0.81, respectively (0.50 to 1.31) and 0.72 (0.39 to 1.34); p for trend = 0.26. Authors ` conclusions: these data did not clearly support the hypothesis that PAF reduces the risk of PD. However, the number of PD patients in this study was not large, the statistical power was limited, and further large studies are needed to provide additional data.[12]
The same team of researchers reported in 2007 the results of studies conducted on the same material to test the hypothesis that body mass index is associated with the risk of PD. The average body mass index (BMI) of the respondents was 24.7 (SD 3.0) kg/m2; 42% of them were overweight. Among 106 new cases of PD, body mass index at baseline was not associated with disease risk. Patients who lost at least 0.5 units of body mass index per decade between baseline and 1988 had an increased risk of PD compared with men with a stable body mass index (multivariate relative risk = 2.60, 95% confidence interval: 1, 10, 6,10).[13]
In 2007, Kwakkel et al. prepared a critical review of the literature on impact of physical therapy for PD. A systematic review of the literature identified 23 randomized controlled trials (n=1063, treatment group sizes ranging from three to 77 participants) addressing specific key areas of physical therapy (PT), including transfer, posture, balance, reaching and grasping, gait, and physical fitness. All studies were of moderate methodological quality. Patients with PD reported benefits from task-specific training for improving postural control and balance (nine studies), gait and gait-related activities (three studies), and physical fitness (five studies).[14]
Research findings from various studies have explored the relationship between physical activity (PA), body mass index (BMI), and the risk of Parkinson`s disease (PD), offering insights into potential protective or predictive factors. Thacker et al. (2008) analyzed data from 143,325 participants in the Cancer Prevention Study II Nutrition Cohort between 1992 and 2001 (mean baseline age: 63). The study found that individuals engaging in higher levels of recreational physical activity had a reduced risk of PD compared to those with no activity. The relative risk (RR) for the highest category of recreational activity (men >= 23 MET-h/week, women >= 18.5 MET-h/week) was 0.8 (95% CI: 0.6, 1.2; P trend = 0.07). Notably, moderate to vigorous activity showed a stronger association with lower PD risk than light activity, with an RR of 0.6 (95% CI: 0.4, 1.0; P trend = 0.02). These findings were consistent across genders and remained unchanged after excluding cases with symptom onset in the first four years of follow-up. The study suggests moderate to vigorous activity may contribute to reduced PD risk, or alternatively, declining activity at baseline could signal preclinical PD.[15]
Xu et al. (2010) conducted a prospective investigation using data from the NIH-AARP Diet and Health Study cohort, encompassing 213,701 participants. Higher engagement in mild to vigorous physical activity between ages 35–39 or within the last decade - reported in 1996-1997 - was linked to a lower PD incidence post-2000, with dose-response relationships evident. Regular participation in mild to vigorous PA during both time periods correlated with a roughly 40% lower risk compared to no activity in either period.[16]
In the Swedish National March cohort, Yang et al. studied data from 43,368 participants over a mean follow-up of 12.6 years to evaluate PA`s potential neuroprotective effects on dopaminergic systems and its relation to PD risk. Their analysis identified an inverse relationship between total PA and PD incidence among men, with risk ratios ranging from 0.50 to 0.55 across various categories such as household activities, commuting, and cumulative recreational activity. However, no significant associations were observed between leisure-time PA or occupational activity and PD for either gender. The researchers stated that average PA levels might contribute to a reduced PD risk.[17]
Sääksjärvi et al. (2014) examined lifestyle factors, including BMI and leisure-time physical activity (LTPA), in relation to PD occurrence through data from the Finnish Mobile Clinic Health Examination Survey cohort of 6715 individuals aged 50–79 years followed up for 22 years. A lower PD risk was associated with higher LTPA levels compared to inactivity (RR 0.27; 95% CI: 0.08–0.90). Interestingly, contrary to trends observed in other conditions, smokers showed a lower risk of PD than never smokers (RR 0.23; 95% CI: 0.08–0.67), while moderate alcohol consumption (<5 g/day) increased PD risk compared to nondrinkers. Although BMI initially showed no association with PD risk, an increased risk was detected at higher BMI levels after excluding the first 15 years of data (P trend = 0.02). These results suggest lifestyle factors may predict PD susceptibility but call for additional research.[18]
Wang et al.`s meta-analysis published in 2005 reviewed data from 10 prospective studies on BMI and PD risk. A 5 kg/m² increase in BMI did not display any notable association with PD risk, yielding a pooled RR of 1.00 (95% CI: 0.89–1.12). Subgroup analyses found a slight positive association when alcohol consumption was factored into studies (RR = 1.13; 95% CI = 0.99–1.29) and a faint inverse association when excluding alcohol consumption (RR = 0.90; 95% CI = 0.78–1.04). Overweight and obesity categories showed no significant link to PD risk in separate analyses. The authors concluded that higher BMI does not meaningfully influence PD risk but acknowledged confounding factors might obscure a potential relationship.[19]
A review by LaHue et al. (2016) underscored the association of physical inactivity with various chronic diseases, including type 2 diabetes and obesity, which are potential contributing factors to PD. They highlighted evidence linking insulin resistance, diabetes, dyslipidemia, and dietary patterns with PD development while emphasizing gender differences in biological responses to PA.[20]
Ascherio and Schwarzschild (2016) reviewed several longitudinal investigations exploring environmental and behavioral factors that influence PD risk. They identified reduced risk correlations with behaviors such as smoking, caffeine ingestion, elevated serum urate levels, regular PA, and ibuprofen use, among others.[21]
In a comprehensive narrative review of studies conducted between 2005 and 2017, Bhalsing et al. evaluated the impact of exercise and PA on PD symptoms, drawing from randomized controlled trials, cohort studies, longitudinal investigations, meta-analyses, and review articles. They emphasized the substantial gaps in knowledge regarding the most effective exercise interventions for mitigating PD symptoms, the underlying mechanisms of exercise-induced changes, and optimal methods for monitoring therapeutic outcomes. Nonetheless, they concluded that existing evidence strongly supports PA as a cost-effective and low-risk strategy to address both motor and non-motor symptoms in PD patients, recommending it universally for individuals living with the disease.[22]
Fang et al. (2018) conducted a systematic review investigating the role of PA in reducing PD risk. Their synthesis encompassed eight studies involving 2,192 patients over an average follow-up of 12 years (range: 6.1–22 years). A significant reduction in PD risk was observed among participants engaging in high levels of total PA (relative risk [RR] 0.79; 95% CI 0.68–0.91) and moderate-to-vigorous PA (RR 0.71; 95% CI 0.58–0.87), with stronger associations identified in men compared to women. Conversely, low levels of PA did not yield a discernible risk reduction (RR 0.86; 95% CI 0.60–1.23).[23]
Landers et al. (2019) examined the relationship between lifelong PA and PD severity in a cohort of 76 individuals with PD aged 70 ± 7.5 years. The study utilized several assessment tools, including the Unified Parkinson's Disease Rating Scale part III (MDS-UPDRS III)[25], the modified Lifetime Physical Activity Questionnaire (LPAQ)[26], the Activities-Specific Balance Confidence Scale (ABC)[27], and the Mini Balance Evaluation Systems Test (Mini-BESTest).[28] Additionally, buccal swabs were collected to measure levels of the val66met genotype of brain-derived neurotrophic factor (BDNF), a biomarker known to be lower in PD patients and correlated with disease severity.[24]
Belvisi et al. revised all environmental, lifestyle, nutritional, coexisting, and pharmacological factors that have been studied as possible modifiable protective or risk factors for PD in longitudinal studies. Only a couple of factors have epidemiological evidence and biological credibility to be recognized as protective factors for PD; among these are PA and activity at work.[29]
Table presents the results of studies on the role of PA in PD.
|
First Author/ Year |
Study |
No/gender |
Duration of observation | Outcomes | |
| Sasco, [10] 1992 Chen, 2005 [11] |
Harvard Colledge Univers. Pensylvania prospective |
50,002 M 48,574 M 77,254 F |
1916-1978 1930-1976 12-14 years |
lower but nonsignificant risk of PD for sports teams participants higher PA reduced risk of PD in M |
5. The Role of Physical Activity in Secondary Prevention of Disability in PD
The role of physical activity (PA) in the secondary prevention of Parkinson's disease (PD) has received considerably less attention in scholarly research compared to its role in primary prevention. Poewe and Wenniger have highlighted the persistent lack of robust data on the natural progression of PD, largely attributed to the paucity of standardized longitudinal studies. Several risk factors have been associated with the rapid progression of PD, including advanced age at onset, coexisting major depression, dementia, and an akinetic-rigid type of symptom presentation.[30]
In a systematic review conducted by Marras and colleagues, literature from English and French sources indexed in the Medline database between 1966 and 2002 was analyzed to investigate PD prognosis. The authors identified and evaluated 13 studies that met stringent quality criteria, encompassing cohort sizes ranging from 31 to 356 patients. The findings suggested that baseline motor deficits and cognitive impairment were strong predictors of future disability. Additionally, the absence of tremor in the early stages of PD, as well as advanced age at disease onset, were identified as indicators of an increased risk of disability.[31]
It is well-established that levels of PA among individuals with PD are significantly lower than those observed in the general population, though this assertion is supported by limited empirical evidence. For instance, findings from the Longitudinal Aging Study Amsterdam indicated that patients with PD engaged in 29% less physical activity compared to controls (95% CI: 10–44%). This dataset was corroborated by the ParkinsonNet trial, which analyzed daily PA using the LASA Physical Activity Questionnaire (LAPAQ) for 699 PD patients and 1,959 control participants. Although the study demonstrated a pronounced reduction in PA among patients with severe disease manifestations, it was noted that not all patients with advanced PD were entirely sedentary.[32]
Earlier investigations such as those conducted by Fertl et al. in 1993 also provide critical insights into PA patterns among patients with PD. The study examined 32 PD patients (mean age: 65.6 ± 8.1 years) and compared their activity levels with 31 healthy controls (mean age: 61.7 ± 5.8 years). Until symptom onset at an average age of 58.5 years, PA levels of PD patients were comparable to those of the control group. However, a marked decline in PA was observed as the disease progressed. Preferred activities included swimming, hiking, and gymnastics, while learning new sports appeared to pose significant challenges for individuals with PD.[33]
Further reinforcing these observations, Crizzle and Newhouse (2006) conducted an extensive critical analysis of rehabilitation interventions and PA in PD based on data sourced from prominent medical databases. Their review included seven studies that met their inclusion criteria, involving between 6 and 438 participants, with intervention periods ranging from four weeks to over four years (4.1 years). They concluded that regular physical activity and exercise tangibly contribute to reduced mortality rates while enhancing strength, balance, mobility, and functional independence in activities of daily living among individuals with PD.[34]
Nordic Walking (NW) seems to be a very attractive, cheap, universal, and safe form of PA. De Santis scanned PubMed, PsycINFO, Medline and SCOPUS up to November 2018 and found 13 relevant studies: five randomised controlled trials (RCTs), and eight observational studies. All studies showed benefits or no effects of NW in 318 patients in the early stages of low-to-moderate PD. NW was well accepted and reasonably safe. Symptom severity, walking speed, and gait pattern consistently improved after 4-24 weeks of NW relative to baseline or any control condition during the ON phases of pharmacotherapy. The benefits of NW were less consistent in the OFF phases and during follow-up in the absence of regular training. As the quality of the study was low to moderate, future single-blind RCTs need to examine the clinical significance of NW results and the training parameters needed to optimize the advantages of NW in PD.[35] Salse-Batán et al. published a systematic review and meta-analysis on the impact of NW in subjects with PD in 2022. Twelve studies were included in the review. Not a single reported statistically significant benefit of NW was clinically relevant, with the exception of walking ability. NW practice did not lead to clinically significant alterations in global motor impairment, functional mobility, and fitness in patients with PD. The authors concluded that the therapy appeared to improve walking ability and quality of life, although additional research on the latter outcome is needed.[36]
Tsukita et al. (2022) conducted a comprehensive investigation into the long-term impact of regular physical activity (PA) in individuals with early-stage Parkinson's disease (PD), utilizing data obtained from the Parkinson's Progression Markers Initiative study. This retrospective observational cohort study employed multivariate linear mixed-effects models to evaluate the interaction between regular PA and moderate-to-vigorous exercise levels, as assessed by the Physical Activity Scale for the Elderly, on the progression of clinical symptoms in PD. The analysis accounted for several covariates, including age, gender, levodopa equivalent dosage, and disease duration. The cohort included 237 patients diagnosed with early PD within the past three ± two years (median age 63.0 [range: 56.0–70.0] years; 69.2% male), and participants were followed for a duration of five [4.0–6.0] years. The findings revealed that baseline levels of regular PA and moderate-to-vigorous exercise did not significantly influence the subsequent clinical trajectory of PD. Nevertheless, mean levels of overall regular physical activity during the observational period were significantly correlated with a slower decline in postural and gait stability, as well as with better maintenance of activities of daily living. The authors highlighted in their discussion that various types of PA exerted distinct effects on clinical outcomes.[37]
Henemann et al. (2023) presented the findings of a systematic review evaluating physical therapy interventions for the management of pain in individuals with PD. The review encompassed nine clinical trials involving a total of 242 participants with PD across Hoehn and Yahr stages 1 to 4. These trials investigated a variety of physical therapy modalities, including hydrotherapy, physical therapy exercises, gait training with body weight support, electroacupuncture, and massage therapy. Across all studies, positive effects of physical therapy interventions on pain management in PD patients were documented. However, it was specifically noted that only land-based and aquatic physical therapy approaches resulted in significant improvements in pain levels. The authors emphasized the necessity for further research to ascertain the duration and sustainability of these therapeutic effects.[38]
6. Discussion
A sedentary lifestyle is broadly defined as the antithesis of physical activity. Pate et al. (2008) describe it as encompassing behaviors that do not significantly elevate energy expenditure beyond resting levels, such as sleeping, sitting, driving, lying down, watching television, or engaging in computer use. These activities are associated with an energy expenditure of 1.0–1.5 metabolic equivalent units (MET).[39] Importantly, a sedentary lifestyle should not be conflated with physical inactivity; even individuals meeting recommended levels of physical activity may experience negative health outcomes if they sit for extended periods—typically exceeding 7 to 10 hours daily.
The terms physical activity (PA), exercise, and physical fitness are frequently used interchangeably but hold distinct definitions. The World Health Organization (WHO) continues to adopt the definition of PA proposed by Caspersen et al. in 1985, which refers to any bodily movement produced by skeletal muscles resulting in energy expenditure. Exercise is considered a subset of PA and is characterized by its planned, structured, and repetitive nature, intended either to maintain or enhance physical fitness. Physical fitness itself is defined as a collection of attributes related to health or skill performance, measurable through standardized tests.[6] A physically active lifestyle can manifest in various contexts, such as the workplace or home, and can serve diverse purposes such as athletic performance or general physical conditioning. Strath et al. (2013), in a guide prepared for the American Heart Association (AHA), identified four dimensions essential for assessing PA: type or method, frequency (e.g., daily, several times weekly), duration (e.g., 15 minutes to 90 minutes), and intensity (low, moderate, or high).[40]
In a scientific statement by the AHA, Fletcher et al. classified physical exercise based on intensity using two key metrics: maximum heart rate and MET values. Moderate-intensity exercise corresponds to 50–69% of maximum heart rate and a MET range of 3.0–5.9, while vigorous-intensity exercise involves 70–89% of maximum heart rate with MET values above 6. For comparison, everyday activities such as eating correspond to METs of 1.0–1.5, whereas taking a shower yields 3.0–3.5 METs.[41]
Recent research publications have illuminated the benefits of physical activity and its implications for individuals with Parkinson's disease (PD). A systematic review and network meta-analysis conducted by German researchers for the Cochrane Database System evaluated the impact of various exercise interventions on motor symptom severity and quality of life (QoL) in PD patients. The findings demonstrated significant benefits across most exercise types included in the study; however, limited evidence differentiated between these specific interventions. These results underscore the overarching importance of engaging in exercise to enhance motor symptoms and quality of life, while suggesting that particular motor symptoms may be more effectively managed through targeted PD-specific exercise programs.[42]
Li et al. expanded on this topic by examining self-directed physical activity (SDPA) interventions through a systematic review and meta-analysis of 15 eligible reports involving individuals with early- and mid-stage PD. Their analysis indicated that SDPA improved motor function and mobility across several metrics, including the Timed Up and Go (TUG) test, six-minute walk (6MW) test, stride length, gait velocity, Unified Parkinson Disease Rating Scale Part III (UPDRS-III), and Berg Balance Scale (BBS). However, no significant improvements were observed in freezing of gait (FOG) or QoL measures assessed using the PDQ-39 scale, despite engaging in SDPA. These findings emphasize the nuanced impacts of self-directed physical activity on both motor symptoms and broader health outcomes in individuals with PD.[43]
In considering the role of exercise as medicine in PD, Langeskov-Christensen et al. concluded that identifying interventions that prevent, slow down, stop, or alleviate the disease is crucial. Exercise seems to be safe and a foundation in PD rehabilitation, but it may have even more essential benefits that could change clinical practice. In the case of PD, the existing body of knowledge supports exercise as (1) a protective lifestyle factor to prevent disease (i.e., primary prevention), (2) a potential disease-modifying therapy (i.e., secondary prevention), and (3) an effective symptomatic treatment (i.e., tertiary prevention). Based on present evidence, a paradigm shift is suggested, whereby exercise should be individually prescribed as a treatment for people with PD at an early stage of the disease, in addition to traditional medical treatment.[44]
Meyers and colleagues investigated the relationship between physical fitness levels, physical activity (PA) patterns, and all-cause mortality. Among 6,213 men undergoing exercise testing between 1987 and 2000, 842 participants had their PA patterns evaluated during adulthood. The study assessed the predictive power of exercise capacity and activity behaviors, alongside clinical data and exercise test results, in determining all-cause mortality over an average follow-up period of 5.5 ± 2 years. Findings revealed that exercise capacity was a more significant predictor of mortality than activity patterns. After adjusting for clinical characteristics, risk factors, exercise test outcomes, and activity behaviors in the multivariate analysis, only exercise capacity and energy expenditure from recreational activities during adulthood emerged as significant predictors of mortality. These variables showed stronger predictive value than traditional risk factors, including smoking, hypertension, obesity, and diabetes. Mortality rates, adjusted for age, declined with higher quartiles of exercise capacity and PA levels. Specifically, a weekly increase of 1,000 kcal in activity was found to have a similar impact on mortality reduction as an elevation in physical fitness by one metabolic equivalent, with both associated with a 20% decrease in mortality risk. The authors concluded that exercise capacity assessed through testing and weekly PA energy expenditure are superior predictors of all-cause mortality compared to established clinical measures and exercise testing data.[45]
In addition, a UK-based 2024 survey explored healthcare professionals' perspectives on encouraging exercise and PA among individuals newly diagnosed with Parkinson`s disease (PD). The survey included 29 physicians, 17 nurses, and 106 physiotherapists. Among these respondents, all nurses, 99% of physiotherapists, and 72% of physicians reported consistently promoting exercise and PA during clinic appointments. Key topics identified for promoting PA in PD patients included its impact on symptoms, the evidence supporting specific activities like Tai Chi, dancing, and Nordic walking, barriers to engagement, and referral to support groups. However, these discussions primarily occurred during physiotherapy sessions. Referrals to physiotherapy were most commonly made following incidents such as falls or mobility challenges rather than at the point of diagnosis. A notable barrier cited by many healthcare professionals—52% of physicians and 41% of nurses - was a lack of confidence in recommending exercise to individuals with PD.[46]
7. Conclusions
Evidence suggests that physical activity (PA) plays a crucial role in the effectiveness of primary and secondary prevention of Parkinson`s disease (PD), particularly when performed at moderate to high intensity levels. However, the scholarly literature reveals a notable scarcity of studies focusing on leisure-time PA and lifestyle PA. In alignment with World Health Organization (WHO) guidelines, individuals are advised to engage in 150–300 minutes of PA per week, preferably distributed over three to four days, or ideally on a daily basis. For individuals with PD, it is essential that these activities be scheduled during the "ON" phase of medication efficacy and planned in collaboration with a personal coach or healthcare professional.
When designing PA regimens for individuals with PD, careful consideration must be given to any contraindications and specific precautions. The selection of PA types should be guided by the patient’s personal preferences, physical capabilities, as well as their socioeconomic circumstances and access to local resources. Numerous scholars advocate for personalized, daily PA as a fundamental strategy in the secondary prevention of PD. The findings presented in this review support a rearticulation of Langeskov-Christensen et al.'s assertion: PA functions as a form of "medicine" for managing PD.
Looking to the future, advancements in this field depend on rigorously developed research methodologies to expand our understanding of PA's role in PD prevention and management. Future investigations should prioritize identifying specific modes of PA particularly beneficial for individuals with PD, with a strong emphasis on leisure-time and lifestyle-oriented PA interventions.
References
- Collaborators GN. Global, regional, and national burden of neurological disorders, 1990 -2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y; Li, YA; Pan, HY; Han, LY. Global, regional, and national burden of neurological disorders in 204 countries and territories worldwide. J Glob Health 2023, 13, 04160–70. [Google Scholar] [CrossRef] [PubMed]
- WHO Parkinson disease 9 August 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/parkinsondisease.
- Global action plan on physical activity 2018–2030: more active people for a healthier world. World Health Organization, Geneva 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf.
- Bull, FC; Al-Ansari, SS; Biddle, S; Borodulin, K; Buman, MP; Cardon, G; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54(24), 1451–1462. [Google Scholar] [CrossRef]
- Caspersen, CJ; Powell, KE; Christenson, GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed] [PubMed Central]
- Dunn, AL; Andersen, RE; Jakicic, JM. Lifestyle physical activity interventions. History, short- and long-term effects, and recommendations. Am J Prev Med. 1998, 15(4), 398–412. [Google Scholar] [CrossRef]
- Hillman, CH; Erickson, KI; Kramer, AF. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat Rev Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Hirsch, MA; Farley, BG. Exercise and neuroplasticity in persons living with Parkinson's disease. Eur J Phys Rehabil Med. 2009, 45, 215–229. [Google Scholar] [PubMed]
- Sasco, AJ; Paffenbarger, RS, Jr.; Gendre, I; Wing, AL. The role of physical exercise in the occurrence of Parkinson’s disease. Arch. Neurol. 1992, 49, 360–365. [Google Scholar] [CrossRef]
- Chen, H; Zhang, SM; Schwarzschild, MA; Hernán, MA; Ascherio, A. Physical activity and the risk of Parkinson disease. Neurology 2005, 64, 664–669. [Google Scholar] [CrossRef]
- Logroscino, G; Sesso, HD; Paffenbarger, RS, Jr.; Lee, I-M. Physical activity and risk of Parkinson’s disease: a prospective cohort study. J Neurol. Neurosurg. Psychiatry 2006, 77, 1318–1322. [Google Scholar] [CrossRef]
- Logroscino, G; Sesso, HD; Paffenbarger, RS, Jr.; Lee, I-M. Body Mass Index and Risk of Parkinson's Disease: A Prospective Cohort Study. Am. J. Epidemiol. 2007, 166, 1186–1190. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G; de Goede, CJ; van Wegen, EE. Impact of physical therapy for Parkinson`s disease: A critical review of the literature. Parkinsonism Relat Disord 2007, 13 Suppl 3, S478–487. [Google Scholar] [CrossRef]
- Thacker, EL; Chen, H; Patel, AV; McCullough, ML; Calle, EE; Thun, MJ; et al. Recreational physical activity and risk of Parkinson's disease. Mov Disord. 2008, 23, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q; Park, Y; Huang, X; Hollenbeck, A; Blair, A; Schatzkin, A; Chen, H. Physical activities and future risk of Parkinson`s disease. Neurology 2010, 75, 341–348. [Google Scholar] [CrossRef]
- Sääksjärvi, K; Knekt, P; Männistö, S; Lyytinen, J; Jääskeläinen, T; Kanerva, N; Heliövaara, M. Reduced risk of Parkinson's disease associated with lower body mass index and heavy leisure-time physical activity. Eur J Epidemiol. 2014, 29(4), 285–292. [Google Scholar] [CrossRef]
- Wang, YL; Wang, YT; Li, JF; Zhang, YZ; Yin, HL; Han, B. Body Mass Index and Risk of Parkinson's Disease: A Dose-Response Meta-Analysis of Prospective Studies. PLoS One 2015, 10(6), e0131778. [Google Scholar] [CrossRef]
- Yang, F; Lagerros, YT; Bellocco, R; Adami, HO; Fang, F; Pedersen, NL; Wirdefeldt, K. Physical activity and risk of Parkinson`s disease in the Swedish National march cohort. Brain 2015, 138, 269–275. [Google Scholar] [CrossRef]
- LaHue, SC; Comella, CL; Tanner, CM. The best medicine? The influence of physical activity and inactivity on Parkinson's disease. Mov Disord. 2016, 31(10), 1444–1454. [Google Scholar] [CrossRef]
- Ascherio, A; Schwarzschild, MA. The epidemiology of Parkinson's disease: risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [CrossRef]
- Bhalsing, KS; Abbas, MM; Tan, LCS. Role of Physical Activity in Parkinson's Disease. Ann Indian Acad Neurol. 2018, 21, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Fang, X; Han, D; Cheng, Q; Zhang, P; Zhao, C; Min, J; Wang, F. Association of Levels of Physical Activity With Risk of Parkinson Disease: A Systematic Review and Meta-analysis. JAMA Netw. 2018, 1, e182421-31. [Google Scholar] [CrossRef]
- Landers, MR; Johnson, KN; Johnson, S; Ormsby, T; Salgo, DC; Zornet, JB. Pre-diagnosis physical activity habits are associated with age of diagnosis in Parkinson's disease. Clin Park Relat Disord. 2019, 1, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Fahn S, Elton R. Members of the UPDRS Development Committee. In: Fahn S, Marsden CD, Calne DB, Goldstein M, eds. Recent Developments in Parkinson's Disease, Vol 2. Macmillan Health Care Information. Florham Park, NJ (1987);163:293-304.
- Postuma, RB; Berg, D; Stern, M; Poewe, W; Olanow, CW; Oertel, W; et al. MDS clinical diagnostic criteria for Parkinson's disease. Movement Dis. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Powell, LE; Myers, AM. The Activities-specific Balance Confidence (ABC) scale. J Gerontol A Biol Sci Med Sci. 1995, 50A, M28–34. [Google Scholar] [CrossRef]
- Franchignoni, F; Horak, F; Godi, M; Nardone, A; Giordano, A. Using psychometric techniques to improve the Balance Evaluation Systems Test: the mini-BESTest. J Rehabil Med. 2010, 42, 323–331. [Google Scholar] [CrossRef]
- Belvisi, D; Pellicciari, R; Fabbrini, G; Tinazzi, M; Berardelli, A; Defazio, G. Modifiable risk and protective factors in disease development, progression and clinical subtypes of Parkinson's disease: What do prospective studies suggest? Neurobiol Dis. 2020, 134, 104671. [Google Scholar] [CrossRef]
- Poewe, WH; Wenning, GK. The natural history of Parkinson's disease. Ann Neurol. 1998, 44((3) Suppl 1, S1–9. [Google Scholar] [CrossRef] [PubMed]
- Marras, C; Rochon, P; Lang, AE. Predicting motor decline and disability in Parkinson disease: a systematic review. Arch. Neurol. 2002, 59, 1724–1728. [Google Scholar] [CrossRef] [PubMed]
- Van Nimwegen, M; Speelman, AD; Hofman-van Rossum, EJ; Overeem, S; Deeg, DJ; Borm, GF; et al. Physical inactivity in Parkinson's disease. J Neurol. 2011, 258, 2214–2221. [Google Scholar] [CrossRef] [PubMed]
- Fertl, E; Doppelbauer, A; Auff, E. Physical activity and sports in patients suffering from Parkinson`s disease in comparison with healthy seniors. J Neural Transm. 1993, 5, 157–161. [Google Scholar] [CrossRef]
- Crizzle, AM; Newhouse, IJ. Is physical exercise beneficial for persons with Parkinson`s Disease? Clin J Sport Med. 2006, 16, 422–425. [Google Scholar] [CrossRef]
- De Santis, KK; Kaplan, I. The motor and the non-motor outcomes of Nordic Walking in Parkinson's disease: A systematic review. J Bodyw Mov Ther. 2020, 24(2), 4–10. [Google Scholar] [CrossRef] [PubMed]
- Salse-Batán, J; Sanchez-Lastra, MA; Suarez-Iglesias, D; Varela, S; Ayán, C. Effects of Nordic walking in people with Parkinson's disease: A systematic review and meta-analysis. Health Soc Care Community 2022, 30(5), e1505-1520. [Google Scholar] [CrossRef]
- Tsukita, K; Sakamaki-Tsukita, H; Takahashi, R. Long-term Effect of Regular Physical Activity and Exercise Habits in Patients With Early Parkinson Disease. Neurology 2022, 98(8), e859–e871. [Google Scholar] [CrossRef]
- Henemann, TT; Truchem, L; Siega, J; Paladini, LH; Israel, VL. Physical therapy interventions to manage pain in Parkinson`s disease: A systematic review. Human Movement 2023, 24(3), 31–43. [Google Scholar] [CrossRef]
- Pate, RR; O’neill, JR; Lobelo, F. The evolving definition of „sedentary”. Exerc Sport Sci Rev. 2008, 36, 173–178. [Google Scholar] [CrossRef]
- Strath SJ, Kaminsky LA, Ainsworth BE, Ekelund U, Freedson PS, Gary RA, et al.; American Heart Association Physical Activity Committee of the Council on Lifestyle and Cardiometabolic Health and Cardiovascular, Exercise, Cardiac Rehabilitation and Prevention Committee of the Council on Clinical Cardiology, and Council. Guide to the assessment of physical activity: Clinical and research applications: a scientific statement from the American Heart Association. Circulation 2013;128:2259-2279. [CrossRef]
- Fletcher, GF; Ades, PA; Kligfield, P; Arena, R; Balady, GJ; Bittner, VA. American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology, Council on Nutrition, Physical Activity and Metabolism, Council on Cardiovascular and Stroke Nursing, and Council on Epidemiology and Prevention. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Ernst, M; Folkerts, AK; Gollan, R; Lieker, E; Caro-Valenzuela, J; Adams, A; et al. Physical exercise for people with Parkinson's disease: a systematic review and network meta-analysis. Cochrane Database Syst Rev. 2023, 1(1), CD013856. [Google Scholar] [CrossRef]
- Li, H; Cao, C; Li, Y. Self-directed physical activity interventions for motor symptoms and quality of life in early and mid-stage Parkinson's disease: A systematic review and meta- analysis. Arch Gerontol Geriatr. 2024, 116, 105159–73. [Google Scholar] [CrossRef] [PubMed]
- Langeskov-Christensen, M; Franzén, E; Grøndahl Hvid, L; Dalgas, U. Exercise as medicine in Parkinson's disease. J Neurol Neurosurg Psychiatry 2024, jnnp-2023-332974. [Google Scholar] [CrossRef]
- Myers, J; Kaykha, A; George, S; Abella, J; Zaheer, N; Lear, S; Yamazaki, T; Froelicher, V. Fitness versus physical activity patterns in predicting mortality in men. Am J Med. 2004, 15;117(12), 912–918. [Google Scholar] [CrossRef]
- Agley, L; Hartley, P; Lafortune, L. Exercise and physical activity promotion for people newly diagnosed with Parkinson's disease: a UK survey exploring current practice and the views of healthcare professionals. Physiotherapy 2024, 122, 17–26. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



