
Submitted:
21 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Background Pellagra, a disease caused by niacin (vitamin B3) deficiency, is characterized by the "3 Ds": dermatitis, diarrhea, and dementia. While rare in industrialized nations, it persists in at-risk populations, particularly those with alcohol use disorder, malabsorption, or post-bariatric surgery. Case presentation This case presents a 64-year-old woman with chronic alcohol dependence and a history of sleeve gastrectomy, who developed advanced pellagra. Her clinical symptoms included a diffuse pruritic rash, diarrhea, cognitive decline, and severe leg pain. Clinical exams was notable for a symmetric hyperpigmented rash on both forearms, the neck and the upper back. Laboratory tests confirmed a significantly low serum niacin level (< 20). Initial diagnoses, such as toxic shock syndrome or Stevens-Johnson syndrome, were ruled out after a skin biopsy showed nonspecific spongiotic dermatitis. After starting oral niacin supplementation, gastrointestinal and dermatologic symptoms improved, though her cognitive impairment persisted. The patient’s condition was complicated by sepsis, acute kidney injury, and multi-organ failure, leading to eventual brain death. Discussion This case highlights the challenges of diagnosing pellagra in a modern clinical setting, especially when compounded by other medical conditions. Despite early treatment, delayed recognition and aggressive systemic complications contributed to a fatal outcome. It underscores the importance of considering secondary pellagra in patients with risk factors and the need for early diagnosis and niacin replacement to prevent severe outcomes.
Keywords:
thiamin deficiency
; pruritic rash
; cognitive impairment
; malabsorption
Introduction
Pellagra is a disease caused by a deficiency of niacin, also known as vitamin B3. It is a form of malnutrition, specifically characterized by a lack of essential micronutrients.[1] Niacin plays a crucial role in cell functioning throughout the body.[2] A deficiency can lead to symptoms affecting various parts of the body, including the skin, mouth, bowels, and brain. If left untreated, pellagra can cause lasting damage to the nervous system and even death.[3] Pellagra is rare in the United States, affecting less than 1% of the population and typically arising from secondary causes, such as alcohol use.[1]
Primary pellagra caused by inadequate dietary intake remains a significant issue in impoverished and food-limited populations. In contrast, niacin deficiency in industrialized countries is more likely to occur from secondary causes — from health conditions or substances that prevent the body’s ability to absorb or utilize niacin.[4]
Classic pellagra is characterized by a combination of symptoms that healthcare providers describe as the “3 Ds”: diarrhea, dermatitis, and dementia. Some also include a fourth “D” for death. Death can occur if pellagra is left untreated for several years.[1]
We present a case of pellagra in a 64-year-old patient with a history of chronic alcohol dependence and prior sleeve gastrectomy. The patient exhibited the classic triad of dermatitis, diarrhea, and cognitive impairment, and laboratory evaluation revealed a markedly reduced serum vitamin B3 (niacin) level.
Case Presentation
We present a 64-year-old woman with a medical history of hypertension, diabetes mellitus, gout, chronic back and knee pain, chronic alcohol dependence (approximately one bottle daily), and prior sleeve gastrectomy. She presented to the emergency department with progressively worsening severe bilateral leg pain and swelling, dysphagia with decreased oral intake, and a one-week history of diarrhea. She additionally reported a three-week history of sore throat and a one-month history of a pruritic rash involving the scalp, torso, chest, and extremities.
On arrival, she was hypotensive, tachycardic, and febrile to 103 °F. Skin examination was notable for diffuse extensive skin excoriations with bilateral lower extremities skin ulcer together with symmetric hyperpigmented rash on both forearms, the neck and the upper back (Figure 1). Mucus membrane exam was notable for red tongue with cracked lips. Initial laboratory evaluation demonstrated leukocytosis (25,000/µL) with neutrophilia (89%), hyperkalemia (6.4 mmol/L), hyponatremia (127 mmol/L), creatinine 6.2 mg/dL, BUN 79 mg/dL, lactic acid 4.2 mmol/L, and a markedly elevated TSH (30,000). CT imaging of the lower extremities showed diffuse bilateral soft tissue edema consistent with cellulitis.
The patient was admitted to the medical intensive care unit (ICU) for septic shock secondary to lower limb cellulitis and open skin ulcers. Blood cultures grew MRSA in two sets and Staphylococcus epidermidis. The patient was maintained on IV fluids and IV antibiotics and became stable enough to be transferred to the medical floor after resolution of septic shock and implementing adequate leg wounds care. However, her mentation remained fluctuating from a baseline of AAOx1.
Based on the patient’s presentation, initial dermatologic evaluation raised concern for toxic shock syndrome, potentially due to Staphylococcus aureus vs atypical or abortive form of Stevens–Johnson syndrome. However, a punch biopsy revealed only nonspecific spongiotic dermatitis, prompting reconsideration of the differential (Figure 2). When integrated with the patient’s chronic alcohol use, prior sleeve gastrectomy, and the triad of dermatitis, diarrhea, and cognitive impairment, these findings ultimately raised strong suspicion for secondary pellagra.
Further labs revealed severe vitamin B3 deficiency (<20) with normal B6, B12 and folic acid levels.. Oral niacin 500 mg daily was initiated, leading to resolution of the diarrhea and a gradual improvement of dermatitis over subsequent days; however, cognitive status continued to fluctuate with episodes of agitation and delusions.
Neurology consultation and MRI revealed a new 4-mm right occipital infarct and chronic vascular dementia. Endocrinology was consulted for worsening hypothyroidism (TSH 47→30 mlU/L), prompting an increase in levothyroxine to 100 mcg daily.
Wound care and podiatry were consulted for a worsening right foot wound with purulent drainage; wound cultures grew Pseudomonas, and the patient underwent debridement and grafting of the right foot and ankle. The hospital course was complicated by recurrent hypotension (BP 75/53 mm Hg), hypothermia (93 °F), and tachycardia, with extensive painful intergluteal and buttock wounds. Medical ICU re-evaluation was requested for worsening sepsis, hypernatremia, and acute kidney injury (AKI), and she was transferred back to the medical ICU where pressors were initiated. Over a few days, the patient became increasingly irritable with worsening mentation. She received haloperidol and quetiapine for agitation. Given poor oral intake and persistent electrolyte derangements, nasogastric tube feeding was attempted but refused. The patient subsequently developed loose stools and abdominal discomfort. Tool studies were unremarkable. Abdominal X-ray revealed incidental pneumoperitoneum; CT confirmed pneumoperitoneum without extravasation. Surgery was consulted, and conservative management was pursued.
The patient was downgraded to the medical floor and remained hemodynamically stable but persistently mental declinement. Over a few days, she developed hospital-acquired pneumonia with lactic acidosis, and worsening mentation, hypothermia, hypotension, and hypernatremia, accompanied by hallucinations. She was transferred to the medical ICU for septic shock and started on broad-spectrum antibiotics and vasopressors. Persistent diarrhea prompted repeat vitamin testing, CT was unremarkable. Potent broad spectrum ABs were started.
The patient stabilized and returned to the medicine floors on continuing the Abs regimen. She initially improved but developed worsening anemia with a significant hemorrhage from the debrided right foot wound requiring repeated dressing changes before hemostasis was achieved. Later on, recurrent hypotension with MAP <65, prompted fluid resuscitation and increased midodrine dosing.
In the setting of persistent hypernatremia and worsening AKI, the patient became hypotensive (BP 75/40) with lactic acidosis (5.8) and leukocytosis (26,030/µL), necessitating Medical ICU readmission for management of acute encephalopathy, septic shock, and AKI. Vasopressor requirements increased significantly (2→14). She received another blood transfusion for anemia. Throughout her MICU course she remained agitated and confused. Niacin levels remained low despite supplementation. Worsening AKI required initiation of hemodialysis. As her condition progressed to multiorgan failure, the family elected to transition her to comfort care, and she was transferred to the medical floor. The patient was found unresponsive with fixed, dilated pupils and brain death was pronounced.
Discussion
This case highlights an advanced and fatal presentation of pellagra in a patient with profound risk factors, including chronic alcohol use disorder, sleeve gastrectomy, and multiorgan dysfunction. Although pellagra is considered rare in industrialized nations, occurring in less than 1% of the U.S. population, modern cases continue to emerge among individuals with nutritional compromise, malabsorption, or substance use disorders.[5] This patient exhibited the classic triad of dermatitis, diarrhea, and dementia, representing what is often described as a “textbook presentation” of pellagra.[1] However, her course was complicated by delayed recognition, sepsis, renal failure, and refractory metabolic derangements.
Niacin Microbiology
(Niacin, primarily in the forms of nicotinic acid and nicotinamide, functions biologically as nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP), which play essential roles in cellular redox reactions.[6] Dietary niacin is absorbed after conversion to nicotinamide and nicotinic acid and is subsequently reconverted to NAD and NADP within tissues, with rapid uptake by the liver, kidneys, and erythrocytes; additionally, hepatic conversion of tryptophan contributes significantly to overall niacin availability.[7]
Vitamin B3 deficiency reduces NAD+ and NADP+ availability, impairing redox reactions, mitochondrial ATP production, and DNA repair. [5] Highly metabolically active tissues are most affected. In our patient, this deficiency likely caused photosensitive dermatitis through impaired keratinocyte DNA repair and oxidative stress, gastrointestinal mucosal atrophy leading to malabsorption and diarrhea, and neuropsychiatric symptoms—including confusion, fluctuating sensorium, and hallucinations—due to disrupted neuronal metabolism and neurotransmitter homeostasis.
Etiology of Niacin deficiency
In resource-rich settings, secondary pellagra most often results from impaired absorption or metabolism of niacin and tryptophan.[3] Chronic alcohol use decreases intestinal niacin absorption, increases urinary losses, and limits tryptophan-to-niacin conversion. [8] Bariatric surgery, particularly sleeve gastrectomy, further predisposes patients to micronutrient deficiencies, with pellagra reported months to years postoperatively despite supplementation.[9] These factors likely acted synergistically to precipitate severe vitamin B3 deficiency in this patient.
Beyond malabsorption and nutritional deprivation, several metabolic and genetic conditions can precipitate niacin deficiency and pellagra.Carcinoid syndrome diverts tryptophan to serotonin, reducing endogenous niacin synthesis despite adequate intake,[1] while Hartnup disease impairs intestinal and renal tryptophan absorption and causes pellagra-like features.[10] However, most contemporary reports attribute pellagra to alcohol use disorder, poor intake, or malabsorption, with limited evaluation for these rarer etiologies.[11]Consistent with the recommended evaluations, the team pursued a broad workup to exclude alternative causes of her symptoms, including thyroid dysfunction, infectious etiologies, structural neurologic disease, and autoimmune pathology. MRI confirmed a small occipital infarct and chronic vascular changes, but these findings were not sufficient to explain the severity of her neuropsychiatric decline. Thus, the absence of alternative causes and the presence of significant nutritional risk factors support an acquired rather than metabolic deficiency, while underscoring the need to consider these diagnoses in atypical or refractory cases.
Diagnostic Challenges
The cutaneous findings in our patient were consistent with previously reported cases of pellagra. Symmetric, hyperpigmented, photosensitive rashes involving sun-exposed areas—particularly the neck, forearms, and upper torso—have been repeatedly described as hallmark features of pellagra. [1] Case series involving post-bariatric surgery patients similarly report photodistributed dermatitis as a presenting feature of pellagra, often months to years after surgery, even in patients receiving supplementation. [9] These findings support our interpretation that the patient’s skin manifestations were consistent with reported post-gastrectomy pellagra cases.
In contrast, early diagnostic consideration in our case focused on toxic shock syndrome and Stevens–Johnson syndrome. This diagnostic uncertainty is supported by prior reports noting that pellagra skin biopsies are often nonspecific and may demonstrate only spongiotic or eczematous changes. [12] Thus, the nonspecific biopsy findings in our patient do not contradict the diagnosis and are consistent with existing literature.
Prior case reports highlight the diagnostic challenges and neurologic sequelae of pellagra in modern clinical settings. A Cureus case report described progressive neuropsychiatric decline due to niacin deficiency, underscoring how nonspecific cognitive symptoms can delay diagnosis.[13] Similarly, Zhang et al. reported alcoholic pellagra presenting with dementia and polyneuropathy, emphasizing advanced central and peripheral nervous system involvement in the context of chronic malnutrition.[11] In a similar vein, our patient exhibited a markedly more severe and fulminant course, complicated by sepsis, acute renal failure, and metabolic instability in the setting of prior bariatric surgery and delayed niacin repletion. While all cases shared overlapping neurologic manifestations and risk factors for nutritional deficiency, the rapid multisystem deterioration and fatal outcome in our patient highlight the consequences of delayed recognition and treatment
Sequence of Symptom Development and Resolution
Based on current literature, our patient’s course mirrored the classic temporal pattern of pellagra, with early gastrointestinal symptoms (diarrhea and anorexia), followed by dermatologic involvement and subsequent neuropsychiatric decline, as described in prior reviews.[1,5] After niacin initiation, recovery occurred in the expected order, with rapid improvement in gastrointestinal symptoms, followed by gradual resolution of dermatitis, while neurologic deficits showed minimal recovery. This pattern is consistent with prior reports demonstrating prompt response of gastrointestinal and cutaneous manifestations to niacin replacement, whereas neurologic symptoms often persist or recover incompletely, particularly in advanced disease[14,15]
Therapeutic Considerations: Oral vs IV Niacin
Niacin therapy is highly effective, with expected improvement in diarrhea and dermatitis within days and cognitive recovery within the first week.[1] Our patient received oral niacin 500 mg daily, consistent with guideline-supported regimens and exhibited the expected improvement in diarrhea and dermatitis within days.[5] However, given the persistent neuropsychiatry symptoms, intravenous niacin or higher-dose divided oral regimens may have improved systemic absorption and clinical response as early aggressive replacement has been associated with improved neurologic outcomes in severe cases.[14,16]
This case underscores the importance of recognizing pellagra as a potentially reversible yet frequently overlooked diagnosis. Reversible dementias remain underrecognized in hospitalized patients, particularly when acute illnesses such as sepsis or renal failure dominate clinical attention. Contemporary reports from regions with shifting nutritional patterns and from addiction-medicine settings reinforce that pellagra remains clinically relevant.[9] Clinicians should maintain vigilance for pellagra in patients presenting with unexplained dermatologic, gastrointestinal, and neuropsychiatric symptoms, especially in those with alcohol use disorder or prior bariatric surgery.
Conclusion
This case contributes to the growing modern literature describing severe and atypical presentations of secondary pellagra. It emphasizes the need for early recognition, comprehensive evaluation, and aggressive vitamin replacement, particularly in patients with combined risk factors such as chronic alcohol use and bariatric surgery. Although dermatologic and gastrointestinal symptoms improved with niacin therapy, the rapid multisystem deterioration and fatal outcome in our patient highlight the consequences of delayed recognition and treatment. As global and domestic patterns of malnutrition evolve, heightened awareness of pellagra remains essential across internal medicine, dermatology, gastroenterology, and neurology.
Author Contributions
Study design: A.E., N.A., and A.D. Resources and Data Curation: A.E., H.P., P.P. Manuscript Drafting: A.E., H.P., S.B., K.M., F.M. Post drafting review and polishing: A.E., A.D., N.A.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was waived because the patient died before the case was considered for publication. The next of kin was contacted on multiple occasions but did not respond.
Data Availability Statement
Data would be available upon request from the authors.
Acknowledgments
The authors would like to thank the Department of Dermatology and all consulting services for their contributions to patient care and for providing supportive materials, including clinical photographs. This work would not have been possible without their valuable contributions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hegyi, J.; Schwartz, R.A.; Hegyi, V. Pellagra: dermatitis, dementia, and diarrhea. Int. J. Dermatol. 2004, 43, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Rout, P. Vitamin B3. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, 2025. Updated February 29, 2024; Available online: https://www.ncbi.nlm.nih.gov/books/NBK526107/ (accessed on 15 December 2025).
- National Institutes of Health Office of Dietary Supplements. Niacin fact sheet for health professionals. National Institutes of Health. 2023. Available online: https://ods.od.nih.gov/factsheets/Niacin-HealthProfessional/ (accessed on 15 December 2025).
- World Health Organization. Micronutrient deficiencies. World Health Organization. 2023. Available online: https://www.who.int/health-topics/micronutrients (accessed on 14 December 2025).
- Redzic, Z.; Gupta, V. Pellagra. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, 2025; Available online: https://www.ncbi.nlm.nih.gov/books/NBK470550/ (accessed on 15 December 2025).
- Horwitt, M.K.; Harper, A.E.; Henderson, L.M. Niacin-tryptophan relationships for evaluating niacin equivalents. Am. J. Clin. Nutr. 1981, 34, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Jacobson, E.L.; Jacobson, M.K. Position of cyclization in cyclic ADP-ribose. Biochem Biophys Res Commun. 1993, 194, 1143–1147. [Google Scholar] [CrossRef] [PubMed]
- Badawy, A.A.B. Pellagra and alcoholism: a biochemical perspective. Alcohol. Alcohol. 2014, 49, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Matapandeu, G.; Dunn, R.; Pagels, P.; et al. Pellagra outbreak following bariatric surgery: a case series. Nutrients 2017, 9, 1025. [Google Scholar] [CrossRef]
- The Metabolic and Molecular Bases of Inherited Disease chapter on Hartnup disorder, 8th ed.; Scriver, CR, Beaudet, AL, Sly, WS, Valle, D, Eds.; McGraw-Hill: New York, NY, 2001. [Google Scholar]
- Zhang, Q.; Man, X.; Wang, W.; et al. A case of alcoholic pellagra presenting with dementia and polyneuropathy. Neurol. Sci. 2022, 43, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, D.; Patel, M.; Shah, K.; et al. Pellagra: a review of diagnostic challenges. Cureus 2021, 13, e16233. [Google Scholar] [CrossRef]
- Navari, Y.; Bagheri, A.; Foreback, J. A rare case of pellagra in a chronic alcoholic. Cureus 2023, 15, e47909. [Google Scholar] [CrossRef] [PubMed]
- Castiello, R.J.; Lynch, P.J. Pellagra—reversibility of neurologic sequelae. Arch. Dermatol 1972, 105, 569–572. [Google Scholar]
- Sharma, A.; Sharma, A.; Sharma, D.D. Dementia associated with Pellagra: A rare case report. Indian. J. Psychiatry 2024, 66, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Lotharius, K.C.; Ferguson, G.S.; Camargo, S.; Luck, G.; Perumareddi, P. Pellagra in complex clinical settings: a case involving bariatric surgery, Whipple procedure, and alcohol use disorder. Cureus 2025, 17, e90935. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Hypererythemic scaly V shaped symmetric lesions covering the upper and mid back representing the classic rash in sun-exposed areas of patients with Niacin deficiency.
Figure 1.
Hypererythemic scaly V shaped symmetric lesions covering the upper and mid back representing the classic rash in sun-exposed areas of patients with Niacin deficiency.

Figure 2.
a, b Skin biopsy showing spongiotic dermatitis with perivascular lymphocytic infiltration with eosinophils.
Figure 2.
a, b Skin biopsy showing spongiotic dermatitis with perivascular lymphocytic infiltration with eosinophils.
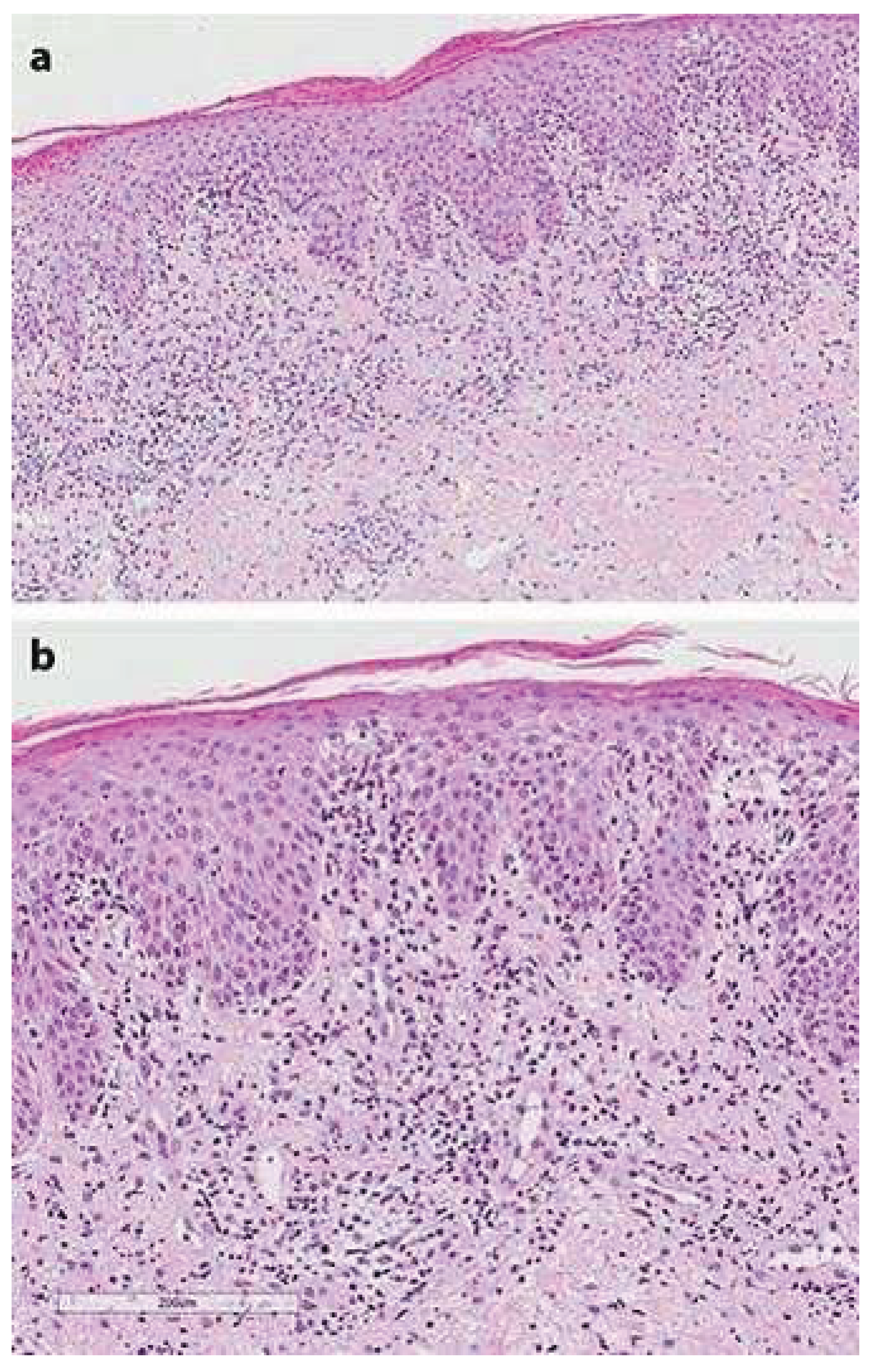

Table 1.
Laboratory Findings recorded during hospitalization Reference Ranges.
| Laboratory Test | Patient Value(s) | Reference Range | Interpretation |
| White Blood Cell Count (WBC) | 25,000/µL; later 26,030/µL | 4,000–11,000/µL | Marked leukocytosis |
| Neutrophils (%) | 89% | 40–70% | Neutrophilia |
| Sodium (Na+) | 127 mmol/L; later hypernatremia (155) | 135–145 mmol/L | Initial hyponatremia → later hypernatremia |
| Potassium (K+) | 6.4 mmol/L | 3.5–5.0 mmol/L | Hyperkalemia |
| Blood Urea Nitrogen (BUN) | 79 mg/dL | 7–20 mg/dL | Elevated |
| Creatinine | 6.2 mg/dL | 0.6–1.3 mg/dL | Severe acute kidney injury |
| Lactic Acid | 4.2 mmol/L; later 5.8 mmol/L | 0.5–2.2 mmol/L | Lactic acidosis |
| Thyroid-Stimulating Hormone (TSH) | 30 → 47 → 30 mIU/L | 0.4–4.5 mIU/L | Severe hypothyroidism |
| Vitamin B3 (Niacin) | <20 (units not specified) | 50–80 (laboratory dependent) | Severe deficiency |
| Vitamin B6 | 25 | 5–50 µg/L | Normal |
| Vitamin B12 | 500 | 200–900 pg/mL | Normal |
| Folic Acid | 20 | >3 ng/mL | Normal |
| Blood Cultures | MRSA; Staphylococcus epidermidis | No growth | Positive for bacteremia |
| Wound Cultures | Pseudomonas aeruginosa | No growth | Positive |
| Stool Studies | Unremarkable | Negative | Normal |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



