
Submitted:
22 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Dental anxiety is a common experience and can be considered a public health issue. This qualitative evidence synthesis used a thematic synthesis approach, to identify and synthesise findings of qualitative studies exploring adults’ lived experiences of dental anxiety.Systematic searches of Embase, Medline, Scopus, PsycINFO, Web of Science, ProQuest, CINAHL and the Cochrane Library identified eleven qualitative studies (total N = 308; age range 18–75 years; 62% female) exploring adults’ dental anxiety experiences Data were extracted and critically appraised using the Critical Appraisal Skills Programme (CASP, 2018) checklist for qualitative research, then synthesised with confidence in synthesised findings assessed using GRADE‑CERQual criteria.Eleven qualitative studies (308 adult participants) yielded 18 review findings, which were organised into nine descriptive themes and synthesised into four analytical themes. The constructed themes captured dental anxiety as a convergence of past and present experiences, shaped by the patient-clinician relationships and systemic factors in dental care. The role of shame contributed to avoidance behaviours, and the use of personal coping strategies was linked to regaining a sense of control which was perceived to be minimal whilst in the dental chair. Findings highlight the benefits of qualitative research methods for understanding the complexity of dental anxiety.
Keywords:
dental anxiety
; qualitative evidence synthesis
; patient concerns about dental treatment
; oral health psychology
1. Introduction
‘Dental anxiety’ was coined as a term describing “an excessive dread of anything being done to the teeth” (Coriat, 1946). It can also be considered as “the fear of going to see a dentist and obtaining dental treatment” (Muneer et al., 2022). Dental anxiety is a relatively common experience, with the 2021 Adult Oral Health Survey (Office for Health Improvement & Disparities, 2023) revealing that 42% of United Kingdom adults surveyed reported a dental anxiety at a moderate level and 12% at a severity level which could be considered ‘phobic’
1.1. Implications of Dental Anxiety
Across anxiety disorders, people avoid feared stimuli or situations (Dobson & Dobson, 2018). Although avoidance provides temporarily relief, it can be considered maladaptive, as it prevents exposure to the situation or stimuli and prevents learning or evidence that contradicts the fear (Ginsburg & Walkup, 2004).
Patients with dental anxiety often only attend for dental treatment in emergency situations requiring invasive or complex treatment, which reinforces fear (Appukuttan, 2016). The avoidance of dental treatment associated with high levels of dental anxiety leads to poorer oral health outcomes (Armfield et al., 2009; Armfield, 2013), increased likelihood of tooth decay and toothache (Unell et al., 1999; Silvera et al., 2021). As such, avoidance of dental treatment is a public health issue (Wide & Hakeberg, 2021).
1.2. Why Are People Dentally Anxious?
There are various reasons why patients are anxious about dental treatment. Within the existing literature in this area, patients have often been asked about their experiences using quantitative methods such as surveys. Earlier quantitative studies placed emphasis on the role of pain and discomfort (Vassend, 1993) with the focus later shifting to the dentist’s manner during treatment (Maggirias & Locker, 2002). Patients often present with needle phobia or blood-injury concerns (Armfield & Milgrom, 2011). Armfield’s cognitive-vulnerability model (Armfield, 2006) emphasises the role of individual cognitive appraisals such as perceptions of danger, unpredictability, and lack of control and disgust in shaping and maintaining dental anxiety, sometimes even in the absence of difficult previous dental experiences. Negative predictions about their dental treatment may be founded on a range of factors, such as negative experiences at the dentist (Beaton et al., 2014) learnt fear from others, or media connotations (Appukuttan, 2016).
1.3. Review Question
Qualitative research aims to uncover detailed accounts and experiences. This review aimed to identify existing qualitative literature in the area of concerns about dental treatment in adults with dental anxiety, and to synthesise the findings to allow for detailed understanding of dental anxiety from the perspective of the patient. The research question was therefore, ‘what are the concerns about dental treatment in adults with dental anxiety?’. A qualitative evidence synthesis was conducted using data from existing primary studies exploring experiences of dental anxiety, including those which were purely qualitative and mixed-method studies with a qualitative component.
2. Method
Prior to undertaking the review, a protocol was developed and pre-registered on PROSPERO (Centre for Reviews & Dissemination, 2025). A pilot review was completed in February 2024 to refine and strengthen an initial search strategy, and to extract and critically appraise findings from two primary studies.
Searches were completed on 8th February 2025 across databases OVID (including MEDLINE 1966-present, PsycINFO 1987-present and Embase 1947-present), CINAHL 1981-present via EBSCOhost, Scopus 1970-present, Web of Science 1900-present, Cochrane Library 1995-present and ProQuest Dissertations and Theses 1997-present. Reference lists of full-text articles and general background reading on the topic were screened for additional studies. The aim was to identify all primary studies of relevance to the research question.
2.1. Search Strategy
A structured search strategy was adopted with the aim of capturing qualitative studies on adult experiences of dental anxiety and filtering out studies not relevant to the population or topic. To guide the development of the strategy, the SPIDER tool (Cooke et al., 2012) was used (Sample, Phenomenon of Interest, Design, Evaluation and Research Type). Boolean operators (AND, OR, and NOT) were used to combine the strategy components effectively. Broadly, the review includes qualitative studies that explore experiences of adults with dental anxiety. Further details of the search strategy are provided in appendix D.
2.2. Study Selection
Inclusion criteria were studies that included a qualitative element and explored adults’ experiences of dental anxiety, dental fear or concerns about dental treatment.
Using the inclusion and exclusion criteria, all three reviewers blindly screened all sources by title and abstract. The primary reviewer screened all articles at full text, with reviewer two screening 66.67% of articles and reviewer three screening 33.33% of articles. Disagreements were resolved through discussion until consensus was reached.
2.3. Critical Appraisal
The Critical Appraisal Skills Programme (CASP, 2018) checklist for qualitative research was selected to assess rigour of the included studies. CASP ratings were completed independently by all three reviewers for the first three studies and, following discussion by the primary reviewer for all studies (Appendix A). Additional quality appraisal details were also gathered at this stage according to GRADE-CERQual criteria (Lewin et al., 2018), supporting the later process of determining confidence in the review findings (Appendix B).
2.4. Synthesis of Results
ENTREQ [Enhancing Transparency in Reporting the Synthesis of Qualitative Research] (Tong et al., 2012) guidelines (Appendix C) were used to improve transparency in reporting findings of synthesised qualitative research. It was decided that a thematic synthesis approach (Thomas & Harden, 2008) would be taken as it is a widely recognised approach for qualitative evidence synthesis, recommended by the Cochrane Qualitative and Implementation Methods Group (Noyes et al., 2018).
Steps were followed according to Thomas and Harden’s (2008) process of thematic synthesis. A coding spreadsheet was created on Microsoft Excel. All primary quotes from participants were transferred to the coding spreadsheet as well as any relevant text from abstracts and results sections of the studies, in order to also include researchers’ understandings (Thomas & Harden, 2008). All data relevant to people’s experiences of dental treatment and dental anxiety were free-form coded, adopting a line-by-line approach with no themes in mind. All coding was completed by the primary reviewer, generating 386 codes.
Descriptive themes were generated by grouping together similar concepts within the codes. This involved careful examination of the data for patterns and relationships and clustering them in ways that captured core ideas and commonalities across the data and refining them to form descriptions about peoples’ experiences. The descriptive themes were then able to be interpreted to generate analytical themes, which involved consideration of relationships between themes and reflection on underlying meanings and contextual factors (Thomas & Harden, 2008). All three reviewers met to discuss the development of descriptive and analytical themes. This introduced differing perspectives and highlighted assumptions behind analytical decisions.
2.5. Confidence in Review Findings
In order to assess confidence that may be placed in the review findings, the GRADE CERQual approach was applied (Lewin et al., 2018). This process was completed independently by the primary reviewer and the confidence rating system was discussed beforehand amongst the three reviewers. Confidence was assessed in a systematic and transparent way through consideration of four areas, including relevance of the studies to the review question, adequacy of data, coherence and methodological limitations.
3. Findings
3.1. Screening of Eligible Studies
Figure 1 depicts the search and selection process for this review in a PRISMA flowchart (Moher et al., 2009). The web-based software tool, Rayyan (Ouzzani et al., 2016) was used to manage the article screening process.
All fifteen papers were assessed at full-text level by the primary reviewer. Each paper was also independently reviewed by one of two additional reviewers. Disagreements were discussed based on inclusion and exclusion criteria, and consensus was reached.
3.2. Study and Participant Characteristics
Table 1 summarises descriptive information about the primary studies. A total of 293 participants were included across the 11 studies, comprising 50 men (17.1%) and 243 women (82.9%). The studies were conducted in Sweden (4 studies, 36.4%), the United Kingdom (3 studies, 27.3%), Denmark (1 study, 9.1%), the United States (1 study, 9.1%), and one study was conducted jointly in the United Kingdom and Taiwan (9.1%). Age of participants was reported in all studies and ranged from 18 to 82 years. Only one study reported on ethnicity (Calladine et al., 2022), in which 92.57% of respondents were White British. Additional details are available in Appendix D.
3.3. Quality Appraisal
Methodological strengths and weaknesses were identified across all studies using CASP (2018) checklist appraisal ratings. These ratings (Appendix A) and additional quality information captured (Appendix B) were central to the assessment of confidence in the review findings using GRADE CERQual (Lewin et al., 2018).
3.4. Reviewer Reflexivity
Researchers shape review findings due to personal and professional factors influencing the analysis (Holloway & Galvin, 2022). The primary reviewer was a trainee clinical psychologist. This allowed for a rich interpretation of the data in terms of the complexities of peoples’ experiences and an understanding of how anxiety manifests. However, as with all qualitative research, biases and assumptions mean that there was a risk of over-identification with participants’ experiences. In order to ensure the review findings appropriately reflect the data, the primary reviewer engaged with reflexivity by keeping a journal on thought processes and decision-making, and questioning assumptions throughout the process. Regular meetings with reviewer two (a clinical psychologist) and reviewer three (a dentist) supported further reflexivity.
The primary reviewer approached the data without personal experience of invasive dental treatment or dental anxiety and very limited clinical experience in dentistry. Although this allowed for open interpretation of participants’ experiences through taking a “not knowing” stance of curiosity, it was important to ensure that any interpretations were shaped by the data as opposed to assumptions as an outsider to the experience. Collaborating with two reviewers with extensive clinical experience in the field of dentistry allowed for insight into aspects of dental treatment discussed by participants in the primary studies.
4. Thematic Synthesis
4.1. Confidence in Synthesis Findings
Table 2 outlines the eighteen key findings of this qualitative evidence synthesis, including studies contributing to each finding, illustrative quotes, and GRADE CERQual assessments of confidence for each finding (Lewin et al., 2018). Thirteen of the review findings were rated as ‘moderate confidence’ and five were rated as ‘low confidence’, predominantly due to the limited number of studies contributing alongside methodological concerns in the contributing studies.
4.2. 2Analytical Themes and Review Findings
Descriptive and analytical themes are displayed in Figure 2. The 386 codes generated were then mapped onto a total of nine descriptive themes and four analytical themes. The analytical themes were: ‘dental anxiety: a convergence of past and present experiences’, ‘interpersonal and systemic factors shape the experiences of dental treatment for anxious patients’; ‘dental anxiety fuels a pattern of avoidance and shame, impacting everyday life’ and ‘navigating dental anxiety involves perseverance, a sense of control, and practical coping strategies’. Figure 2 shows relationships between the themes, including interconnectedness across the descriptive themes.
4.3. Dental Anxiety: A Convergence of Past and Present Experiences
This analytical theme was constructed to capture the interplay between past trauma and current dental experiences. This theme demonstrates the ways in which prior violations of trust or bodily autonomy may be reactivated during dental procedures, reinforcing anxiety through feelings of powerlessness and unpredictability. The three descriptive themes comprising this analytical theme frame dental anxiety as a complex experience, shaped by the interaction between previous trauma and dental treatment in the present.
Loss of Control, Powerless and Uncertainty Amplify Dental Anxiety. Participants described feeling helpless and powerless during dental procedures due to a loss of control. This feeling, alongside sudden actions of the dentist sometimes triggered distress and panic, especially in people who had previous experience of their boundaries being violated (e.g., in Wolf et al., 2020). Closely linked to this was participants’ struggles with the uncertainty of what was to come, with many participants catastrophising and imaging worst-case scenarios. For some participants, dental anxiety took a significant emotional toll, with people describing feeling an overwhelming range of emotions, including irritability and dread, or regression to a childlike state of fear.
Physical and Sensory Experiences Intensify Distress for Dentally Anxious People. Participants described experiences of physiological symptoms and exhaustion in relation to dental visits, with some describing difficulty breathing, almost fainting or feeling unable to move. Sensory triggers such as sounds and smells were captured as issues impacting on dental anxiety across three studies. Some noted that the clinical environment was a marker of reassurance, whilst others felt it exacerbated their anxiety levels. Also increasing anxiety were physical sensations within the mouth or face, as well as needle phobia and fear of choking during procedures, The impact of sensory and bodily cues was understood to intensify distress about accepting dental treatment.
Past Experiences Shape Fear, Trust and Avoidance. Participants described the impact of painful and distressing memories of dental work, with people describing lack of pain relief and forceful extractions, sometimes in childhood. Trauma, whether dental or otherwise, often led to long-term fear and difficulty trusting dental, leading to trauma responses in the dental chair and impacting on avoidance behaviours.
4.4. Interpersonal and Systemic Factors Shape the Experience for Anxious Patients
This analytical theme captures the ways in which both direct interactions with dental staff and broader organisation factors in dental care influence the experiences of dentally anxious patients. At an interpersonal level, power dynamics and communication practices in the treatment room may either alleviate or exacerbate anxiety. Systemically, factors such as appointment scheduling pressures, rushed clinics, and an anxiety-provoking waiting environment compound distress. Relational and structural forces within two descriptive themes also interact with feelings of loss of control and powerlessness as discussed in the previous analytical theme.
Dental Staff Have the Power to Ease or Exacerbate Dental Anxiety. The ways in which clinicians respond to dental anxiety was considered important, with some describing feeling safer when staff recognised and acknowledged their distress. Participants appreciated when clinicians were attuned to their anxiety, providing reassurance and building trust. Instances were described where this was not the case, with power imbalances exacerbating anxiety and communication was inadequate. Participants expressed a need for transparency, clear instructions and feeling able to speak up when distressed. There was a sense that effective communication helps reduce anxiety, especially through preparation, explanation, and continuous updates during the procedure.
Wider Factors in Dentistry Impact the Anxious Patient Beyond the Patient-Dentist Relationship. Beyond the role of clinicians, organisational pressures in dental care were seen to have some impact on participants’ anxiety in three studies. Some described rushed procedures as well as frustration when delays exacerbated their dread about an appointment. The clinical environment such as having to anxiously wait in the waiting room caused discomfort for some, and beyond the dental clinic, there was some discussion about media portrayals of dentistry inciting fear.
4.5. Dental Anxiety Fuels a Pattern of Avoidance and Shame, Impacting Everyday Life
This analytical theme was constructed to capture the self-reinforcing cycle in which dental anxiety leads to a range of avoidance behaviours such as skipping appointments or undertaking extreme oral hygiene rituals in order to try and stave off distress. These strategies were seen to lead to worsening dental health and a sense of shame about being dentally anxious and struggling with dental health. Shame was observed to be rooted in self-criticism and fear of judgement, increasing avoidance and leading to social isolation for some participants. Moments of reprieve were described when participants encountered empathic clinicians or supportive peers. Figure 2 shows the bidirectional link between shame and avoidance at the centre of this analytical theme, and how the two descriptive themes perpetuate each other unless both are addressed.
Avoidance Due to Dental Anxiety Manifests in Various Ways. This descriptive theme demonstrates the various ways in which avoidance due to dental anxiety occurs, including behaviourally in terms of not attending dental appointments, or adopting extreme self-hygiene regimes to prevent treatment or administering self-treatment. Cognitive avoidance occurred through some participants avoiding thoughts about dental care as a means to prevent distress. Social avoidance was described in terms of withdrawal from social interactions to hide dental problems or dental anxiety. This illustrates how pervasive and adaptive avoidance behaviours can be in perpetuating a cycle of worsening anxiety and poor oral health outcomes.
People Are Ashamed of Their Dental Anxiety and Dental Health. Shame was discussed by participants in terms of being dentally anxious and experiencing poor dental health outcomes. Many spoke about their own self-criticism as well as fear of being judged by others due to their anxiety. Some participants described feeling ashamed and embarrassed for neglecting their teeth, impacting on their social lives, which links back to review finding 13 in terms of avoiding others seeing their teeth as a result. Participants who found safe spaces to talk openly about their dental anxiety such as support groups or understanding clinicians reported relief.
4.6. Navigating Dental Anxiety Involves Perseverance, a Sense of Control, and Practical Coping Strategies
Finally, this analytical theme captures the ways in which participants actively work to accept dental treatment by combining personal perseverance with strategies that restore a sense of control. This was constructed to show that despite intense discomfort, some choose to endure treatment for the promise of better oral health, reframing their relationship with the dentist and setting small, achievable goals along the way. Meanwhile, for some, practical coping tools provide concrete ways to manage anxiety in the moment. This illustrates that navigating dental treatment with high levels of dental anxiety is not a passive experience but may be an intentional process in which patients rebuild a sense of agency and resilience to engage with treatment.
Enduring Discomfort and Shifting Perspectives Contribute to Greater Acceptance of Treatment. Despite their fear, some participants managed to endure dental treatment for the promise of improved oral health. People acknowledged the importance and benefits of dental treatment, showing some motivation to engage in it despite their discomfort, but this was only captured across three studies. Some participants described a shift in their outlook, for instance reclaiming a sense of agency, trying to view the dentist in a more ‘human’ way and setting small goals for themselves. Others had accessed interventions which supported this (e.g., this was a key focus in Hultvall et al., 2010) but shared that they believe some level of anxiety will always remain about dental treatment.
Practical Coping Strategies are Helpful in Managing Dental Anxiety. Some participants found using distraction, relaxation techniques, and breathing exercises helpful coping strategies whilst in the dental chair. Participants also discussed the utility of written explanations and step-by-step guidance to help them to feel prepared and reduce uncertainty, to in turn reduce their concerns and improve coping. Some people mentioned options for numbing or sedation being helpful. Overall, there were a variety of strategies that were considered to be helpful, dependent on the individual.
5. Discussion
This review aimed to identify and synthesise findings of existing qualitative research on the concerns adults with dental anxiety have about dental treatment. The four analytical themes, nine descriptive themes and eighteen review findings highlighted the impact of past and present experiences, which were shaped by the patient-clinician relationship, as well as systemic factors in dental care. Shame about dental anxiety and dental health was pervasive, and tolerating treatment was seen to be possible for some with a sense of control, personal coping strategies and motivation to accept treatment.
The themes constructed in this review may specifically be considered within a cognitive-behavioural lens, linking back to Armfield’s cognitive vulnerability model (Armfield, 2006). Catastrophising is a type of cognitive distortion which exacerbates feelings of anxiety and worry (Beck et al., 1979). Within the descriptive theme, loss of control, powerless and uncertainty amplify dental anxiety’, participants discussed their tendency to catastrophise, anticipating worst case outcomes of dental treatment (e.g., about the dentist finding a new problem requiring invasive treatment or treatment going wrong and being very painful). Participants also described feeling helpless and uneasy about potential surprises in the dental chair, describing patterns of ‘what if?’ thinking suggesting intolerance of uncertainty, in which there may be an overestimation of the probability and severity of a negative outcome (Dugas et al., 2004). Indeed, this fear of the unknown has been found to be a major contributor to dental anxiety (McNeil & Randall, 2014).
Catastrophising and intolerance of uncertainty both relate to the avoidance behaviours discussed within the descriptive theme, ‘dental anxiety fuels a pattern of avoidance and shame, impacting everyday life’, whereby avoiding dental treatment becomes a short-term way of escaping the possibility of worst-case scenarios and the lack of control. This links to existing knowledge that avoidance of dental treatment maintains fear (Berggren, 1984; Ginsburg & Walkup, 2004; Armfield et al., 2013) and leads to poorer oral health, increasing the likelihood of more invasive treatment being required (Armfield et al., 2007; Armfield et al., 2013), which is often the patient’s worst-case scenario. The shame associated with poorer oral health, as discussed in the theme, ‘dental anxiety fuels a pattern of avoidance and shame, impacting everyday life’ can also be considered to compound this avoidance and reducing help-seeking (Newton et al., 2012).
Avoidance also connects with coping and behaviour change, as discussed in the descriptive theme, ‘enduring discomfort and shifting perspectives contribute to greater acceptance of treatment’. This is in line with the existing understanding that patients trapped in shame and avoidance cycle are less likely to attempt small exposure steps to be able to try out new coping strategies like those discussed by participants, whereas attending an appointment can begin to unravel this due to exposure (Foa et al., 2017). Within the theme ‘the sensory and physiological experiences of dental care’, participants gave accounts of breath-holding, near-fainting episodes and difficult sensory experiences, highlighting the embodied nature of dental anxiety. These bodily sensations were not only symptoms but also triggers, which fits within the cognitive-behavioural fear cycle, where physiological sensations (e.g., rapid heartbeat, dizziness) are interpreted catastrophically (e.g., “I’m going to faint” or “I’m not safe”), increasing emotional distress and reinforcing avoidance behaviors (Clark & Beck, 2010; Foa et al., 2007).
Previous negative experiences of dental treatment, or wider trauma (such as torture in Hoyvik et al., 2024, and sexual abuse in Wolf., 2020) meant that for some participants, sensory cues such as smells or sounds were able to trigger distressing memories and bodily responses, as discussed in the sub-theme, ‘past experiences shape fear and distrust’. This fits with the concept of reactivation of implicit memories (van de Kolk, 2014), which increases perception of threat in the dental chair. It is evident that dental treatment has the power to re-traumatise (Kvale et al., 2004), and this is relevant beyond dental trauma, which has been observed in patients who have experienced sexual abuse, due to some areas of dental treatment mimicking aspects of traumatic experiences (Willumsen, 2004).
5.1. Clinical Implications
The findings of this review indicate that there is scope for clinicians to reduce the power imbalance and in turn reduce distress, as seen in the theme ‘interpersonal and systemic factors shape the experience for anxious patients’. Participants expressed a need for clinician empathy, transparency and clear communication to increase empowerment and reduce vulnerability, in line with key principles of trauma-informed care (Harris & Fallot, 2001). The sub-theme, ‘dental staff have the power to ease or exacerbate dental anxiety’ emphasises the role of clinicians recognising and responding to anxiety being helpful for participants, consistent with previous literature demonstrating that effective communication and patient-centred care can help patients to feel understood and not judged (Caltabiano et al., 2018; Armfield et al., 2013). Through reducing judgment and acknowledging patient fears, clinicians may lessen the shame associated with dental anxiety and poor oral health, addressing a key element of the analytical theme ‘dental anxiety fuels a pattern of avoidance and shame, impacting everyday life’.
Participants across studies discussed lack of control, as well as using personal coping strategies. These are perhaps important intervention points, due to the possibility of instilling a sense of safety as per trauma-informed care guidance (Harris & Fallot, 2001) to be able to disrupt the fear-avoidance cycle. Interventions that support this and improve the sense of control for patients may include exposure, relaxation techniques, and collaborative treatment planning, to empower patients and reduce perceived helplessness (Moore, 2022).
5.2. Strengths and Limitations of the Primary Studies
Most of the primary studies included basic demographic details such as age and gender, but offered limited or no information on participants’ ethnicity, socioeconomic background, or other indicators of diversity. In some studies, recruitment methods were also insufficiently described, which may affect the representativeness and dependability of the findings. The lack of detailed demographic reporting reduces the ability to understand the lived experiences of dental anxiety across different social or cultural contexts. This is important because cultural norms around oral health, such as attitudes toward preventive care, may be linked to early negative experiences of dental care and dental anxiety (Geers et al., 2024). Experiences of racial discrimination in healthcare are also associated with increased anxiety amongst marginalised groups (Yu et al., 2025). More consistent reporting of demographic details, including ethnicity, could have provided greater insight into these experiences across different groups.
There was a mixture of recruitment strategies across the primary studies. Snowball and purposive sampling, whist useful for reaching participants, may have led to limited diversity and reduced generalisability. Some studies, particularly those using convenience sampling from specific clinics or social media, had larger samples but were often less diverse, limiting broader applicability. Positively, all primary studies had well-defined research aims, providing clear direction for their explorations. Only one study did not use a dental anxiety measure to assess the level of dental anxiety within the population, meaning that almost all studies were able to specify the severity of the dental anxiety within their respective samples.
Across the primary studies, there was a lack of acknowledgement of reflexivity and researcher influence, which is important in qualitative research (Tong et al., 2012). Although some of the studies used reflective logs to reduce bias, details on how this was done were often unclear. Several studies also lacked sufficient explanation of their recruitment strategies, which may affect the generalisability of the findings.
5.3. Strengths and Limitations of this Review
Thomas and Harden’s (2008) method of thematic synthesis relies on inductive coding and interpretative theme development, both of which are subjective processes. Due to resource constraints, all coding and initial theme development was completed independently by a trainee clinical psychologist with no clinical experience in dentistry. Although Thomas and Harden (2008) do not explicitly advise that a second rater is required for coding, it is beneficial to have a second-rater code a sample of data to reduce the risk of personal bias in theme development and selective interpretation of the data (Flemming & Noyes, 2021). Although this was mitigated through discussion and theme refinement with a clinical psychologist supervisor and dentist collaborator both with extensive experience in dentistry, lack of collaborative coding may have reduced rigour and dependability of the findings. In order to increase rigour, a reflexive journal was maintained throughout the synthesis process to document decisions, emerging interpretations, and personal reflections and enhanced consistency in coding (Nowell et al., 2017). The involvement of a second and third rater in the screening and quality appraisal process enhanced transparency and reflexivity, as differing perspectives prompted discussion and critical reflection, leading to a deeper and more nuanced understanding of the data (Tong et al., 2012; Noyes et al., 2018).
Although some grey literature was identified through reference lists in prior reading, a more thorough search of grey literature may have yielded additional relevant sources. As a result, the limited inclusion of grey literature and exclusion of non-English studies may have introduced selection bias and excluded perspectives from underrepresented or non-Western populations. Reliance on published studies increases the risk of publication bias. Efforts were also made to access a relevant thesis, though this was unsuccessful.
5.4. Directions for Future Research
This review included eleven studies with a qualitative element exploring experiences of dental anxiety. Given the prevalence of dental anxiety, this is a small number of studies, supporting a need for more qualitative research in this area. Positively, five of these studies were published within the last five years, with three published much more recently within the last year, suggesting a growing focus on qualitative research in this area.
Further research could qualitatively explore systemic barriers and how they interact with dental anxiety and avoidance of treatment, perhaps in terms of socioeconomic disadvantages or cultural challenges. Research with asylum seekers and refugees has identified barriers to dental care such as language barriers (Paisi et al., 2020) and there are differences in treatment-seeking and patient preferences in patients with dental anxiety across different cultures (Berggren et al., 2000). Understanding these lived experiences could support the development of more inclusive person-centred interventions to support patients with dental anxiety from a broader range of backgrounds than those in this review.
Future research could also explore experiences and effectiveness of coping strategies and for patients with dental anxiety through a qualitative lens. Participants across the primary studies in this review discussed some of their personal coping strategies such as distraction, relaxation and breathing. Written explanations were also valued as a means of reducing uncertainty. Qualitative methods could uncover patient perceptions of the effectiveness of such coping strategies in the long term in reducing anxiety and avoidance of dental treatment.
6. Conclusions
This qualitative evidence synthesis offers rich insights into the lived experiences of dental anxiety across eleven primary studies. Insights from participants included the impact of previous negative experiences, the patient-clinician relationship and wider systemic factors. Participants across the primary studies also highlighted the role of shame and avoidance in perpetuating their anxiety. However, some also described how regaining a sense of control and using personal coping strategies helped them manage their anxiety. These findings suggest that empowering patients with greater control and practical coping strategies could reduce the impact of dental anxiety.
References
- Appukuttan, D. P. Strategies to manage patients with dental anxiety and dental phobia: Literature review. Clinical, Cosmetic and Investigational Dentistry 8 2016, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Armfield, J. M. Cognitive vulnerability: A model of the etiology of fear. Clinical Psychology Review 2006, 26(6), 746–768. [Google Scholar] [CrossRef]
- Armfield, J. M. Towards a better understanding of dental anxiety and fear: Cognitions vs. experiences. European Journal of Oral Sciences 2013, 118(4), 259–264. [Google Scholar] [CrossRef]
- Armfield, J. M.; Milgrom, P.; Armfield, J. A clinician guide to patients afraid of dental injections and numbness. SAAD Dig 2011, 27(7), 33–39. [Google Scholar]
- Armfield, J. M.; Stewart, J. F.; Spencer, A. J. The vicious cycle of dental fear: Exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health 7 2007, 1. [Google Scholar] [CrossRef]
- Armfield, J. M.; Stewart, J. F.; Spencer, A. J. The nature and extent of dental fear and phobia in Australia. Australian Dental Journal 2009, 53(4), 394–401. [Google Scholar] [CrossRef]
- Beaton, L.; Freeman, R.; Humphris, G. M. Why are people afraid of the dentist? Observations and explanations. Medical Principles and Practice 2014, 23(4), 295–301. [Google Scholar] [CrossRef] [PubMed]
- Beck, A. T.; Rush, A. J.; Shaw, B. F.; Emery, G. Cognitive therapy of depression; Guilford Press, 1979. [Google Scholar]
- Berggren, U.; Meynert, G. Dental fear and avoidance: Causes, symptoms, and consequences. Journal of the American Dental Association 1984, 109(2), 247–251. [Google Scholar] [CrossRef]
- Berggren, U.; Pierce, C. J.; Eli, I. Characteristics of adult dentally fearful individuals: A cross-cultural study. European Journal of Oral Sciences 2000, 108(4), 268–274. [Google Scholar] [CrossRef] [PubMed]
- Calladine, H.; Currie, C. C.; Penlington, C. A survey of patients’ concerns about visiting the dentist and how dentists can help. Journal of Oral Rehabilitation 2022, 49(4), 414–421. [Google Scholar] [CrossRef]
- Caltabiano, M. L.; Croker, F.; Page, L.; Sklavos, A.; Spiteri, J.; Hanrahan, L.; Choi, R. Dental anxiety in patients attending a student dental clinic. BMC Oral Health 18 2018, 1–8. [Google Scholar] [CrossRef]
- Centre for Reviews & Dissemination. PROSPERO pre-registration protocol (CRD42025XXXX); University of York, Centre for Reviews & Dissemination, 2025. [Google Scholar]
- Clark, D. A.; Beck, A. T. Cognitive therapy of anxiety disorders: Science and practice; Guilford Press, 2010. [Google Scholar]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qualitative Health Research 2012, 22(10), 1435–1443. [Google Scholar] [CrossRef]
- Coriat, J. Dental anxiety: A survey of its nature and prevalence. Journal of the Tennessee Dental Association 26 1946, 3–8. [Google Scholar]
- Critical Appraisal Skills Programme [CASP]. CASP qualitative checklist. 2018. Available online: https://casp-uk.net/casp-tools-checklists/.
- Dobson, K.; Dobson, D. Evidence-based practice of cognitive–behavioural therapy, 3rd ed.; Guilford Press, 2018. [Google Scholar]
- Dugas, M. J.; Schwartz, A.; Francis, K. Brief report: Intolerance of uncertainty, worry, and depression. Cognitive Therapy and Research 28 2004, 835–842. [Google Scholar] [CrossRef]
- Foa, E. B.; Keane, T. M.; Friedman, M. J.; Cohen, J. A. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress Studies, 2nd ed.; Guilford Press, 2017. [Google Scholar]
- Geers, A. L.; Seligman, L. D.; Pituch, K. A.; Clemens, K. S.; Francis, S.; Kramer, L.; Vang, M. Cultural normative beliefs in the US as a determinant of negative dental experiences and dental anxiety: A preliminary investigation. Current Psychology 2024, 1–13. [Google Scholar] [CrossRef]
- Ginsburg, G. S.; Walkup, J. T. Specific phobia. In Phobic and anxiety disorders in children and adolescents: A clinician’s guide to effective psychosocial and pharmacological interventions; 2004; pp. 175–197. [Google Scholar]
- Harris, M.; Fallot, R. D. (Eds.) Using trauma theory to design service systems: New directions for mental health services (Issue 89); Jossey-Bass, 2001. [Google Scholar]
- Holloway, I.; Galvin, K. Qualitative research in nursing and healthcare; John Wiley & Sons, 2023. [Google Scholar]
- Hoyvik, J.; Kvestad, E.; Raadal, M. Torture victims’ perspective on dental treatment: Every sign you make, every move you take. Journal of Oral Rehabilitation 2024, 51(3), 321–331. [Google Scholar] [CrossRef] [PubMed]
- Hultvall, M.; Lundgren, J.; Gabre, P. Factors of importance to maintaining regular dental care after a behavioural intervention for adults with dental fear: A qualitative study. Acta Odontologica Scandinavica 2010, 68(6), 335–343. [Google Scholar] [CrossRef]
- Kvale, G.; Berggren, U.; Milgrom, P. Dental fear in adults: A meta-analysis of behavioral interventions. Community Dentistry and Oral Epidemiology 2004, 32(4), 250–263. [Google Scholar] [CrossRef]
- Lewin, S.; Booth, A.; Glenton, C.; et al. Applying GRADE-CERQual to qualitative evidence: Introduction to the series. In Implementation Science 13; 2018; p. Article 2. [Google Scholar] [CrossRef]
- Maggirias, J.; Locker, D. Psychological factors and perceptions of pain associated with dental treatment. Community Dentistry and Oral Epidemiology 2002, 30(2), 151–159. [Google Scholar] [CrossRef]
- McNeil, D. W.; Randall, C. L. McNeil, D. W., Randall, C. L., Eds.; Dental fear and anxiety: Etiology, characteristics, and consequences. In Dental fear and anxiety: Progress in research and understanding; Springer, 2014; pp. 25–46. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine 2009, 6(7), e1000097. [Google Scholar] [CrossRef]
- Moore, R. Trusting the dentist—expecting a leap of faith vs. a well-defined strategy for anxious patients. Dentistry Journal 2022, 10(4), 66. [Google Scholar] [CrossRef]
- Muneer, M. U.; Ismail, F.; Munir, N.; Shakoor, A.; Das, G.; Ahmed, A. R.; Ahmed, M. A. Dental anxiety and influencing factors in adults. Healthcare 2022, 10(12), 2352. [Google Scholar] [CrossRef]
- Newton, T.; Asimakopoulou, K.; Daly, B.; Scambler, S.; Scott, S. The management of dental anxiety: Time for a sense of proportion? British Dental Journal 2012, 213(6), 271–274. [Google Scholar] [CrossRef]
- NHS England. NHS clinical guide for the management of patients with dental anxiety; NHS England, 2023; Available online: https://www.england.nhs.uk/long-read/clinical-guide-for-dental-anxiety-management/.
- Nowell, L. S.; Norris, J. M.; White, D. E.; Moules, N. J. Thematic analysis: Striving to meet the trustworthiness criteria. International Journal of Qualitative Methods 2017, 16(1), 1609406917733847. [Google Scholar] [CrossRef]
- Noyes, J.; Booth, A.; Cargo, M.; et al. Chapter 21: Qualitative evidence. In Cochrane Handbook for Systematic Reviews of Interventions (Version 6.3); Cochrane Collaboration, 2018. [Google Scholar]
- Office for Health Improvement; Disparities. Adult Oral Health Survey 2021: England, Wales and Northern Ireland. UK Government. 2023. Available online: https://www.gov.uk/government/statistics/adult-oral-health-survey-2021/adult-oral-health-survey-2021-report-summary.
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Systematic Reviews 5 2016, 210. [Google Scholar] [CrossRef]
- Paisi, M.; Gibson, B.; Puthussery, S.; Humphris, G. M.; Newton, J. T. Barriers to dental care among asylum seekers in the UK: A qualitative study. Community Dentistry and Oral Epidemiology 2020, 48(6), 519–528. [Google Scholar] [CrossRef]
- Silvera, D. H.; McCarthy, D. M.; McNeil, D. W. The impact of dental anxiety on oral health outcomes: A systematic review. Journal of Dental Research 2021, 100(6), 547–555. [Google Scholar]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Medical Research Methodology 8 2008, 45. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Medical Research Methodology 12 2012, 181. [Google Scholar] [CrossRef]
- Unell, L.; Söderfeldt, B.; Halling, A.; Birkhed, D. Explanatory models for clinically determined and symptom-reported caries indicators in an adult population. Acta Odontologica Scandinavica 1999, 57(3), 132–138. [Google Scholar] [CrossRef]
- Vassend, O. Anxiety, pain and discomfort associated with dental treatment. Behaviour Research and Therapy 1993, 31(7), 659–666. [Google Scholar] [CrossRef]
- Wide, U.; Hakeberg, M. Treatment of dental anxiety and phobia—Diagnostic criteria and conceptual model of behavioural treatment. Dentistry Journal 2021, 9(12), 153. [Google Scholar] [CrossRef]
- Willumsen, T. The impact of childhood sexual abuse on dental fear. Community Dentistry and Oral Epidemiology 2004, 32(1), 73–79. [Google Scholar] [CrossRef]
- Wolf, M.; Sundberg, H.; Ericsson, M. Dental care—An emotional and physical challenge for the sexually abused. European Journal of Oral Sciences 2020, 128(5), 384–391. [Google Scholar] [CrossRef]
- Yu, H.; Bauermeister, J. A.; Oyiborhoro, U.; Villarruel, A. M.; Bonett, S. The relationship between racial discrimination in healthcare, loneliness, and mental health among Black Philadelphia residents. International Journal for Equity in Health 2025, 24(1), 109. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart depicting the search and selection process.
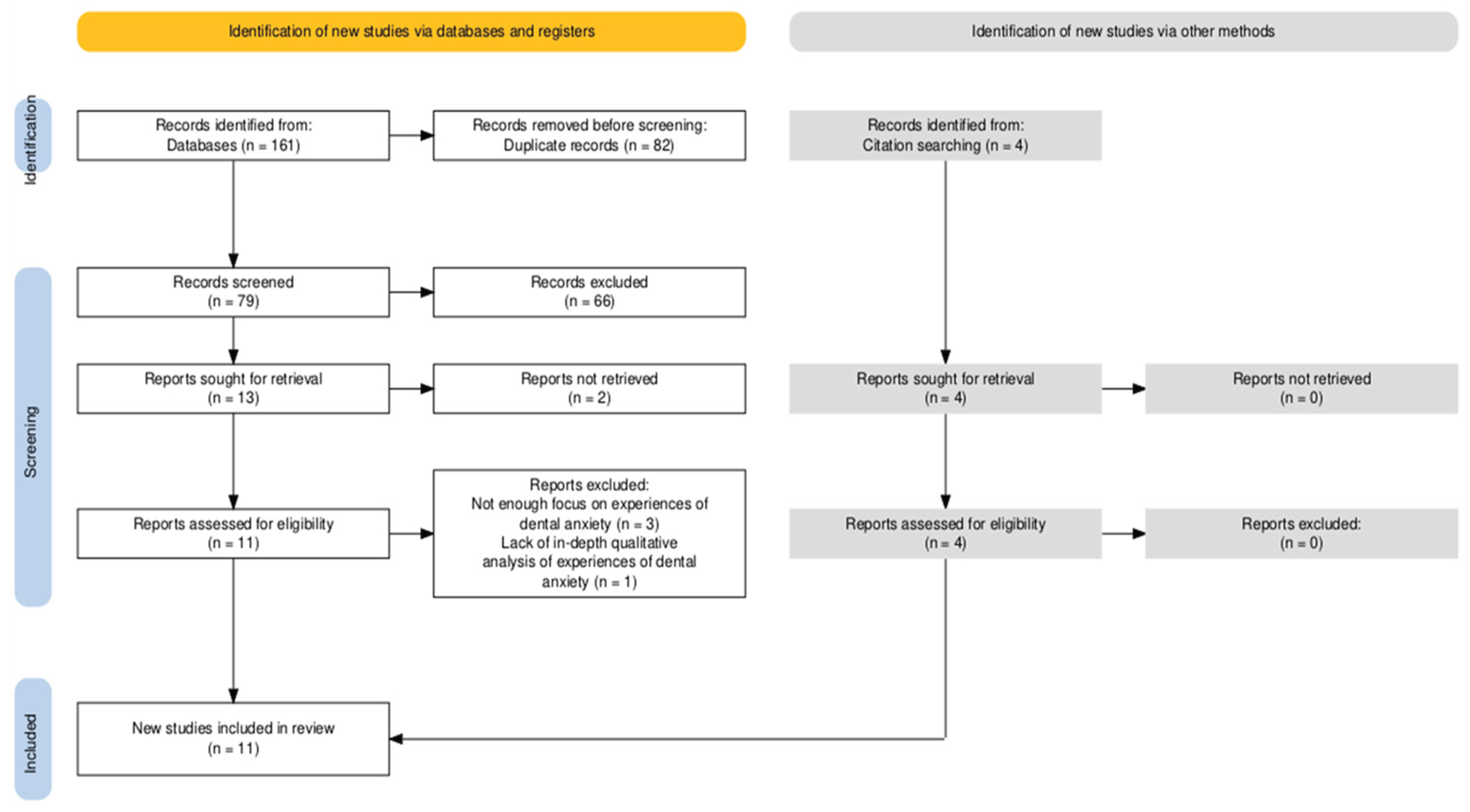
Figure 2.
Thematic map illustrating descriptive and analytical themes and the relationships between them. Numbering represents each individual review finding under each descriptive theme as listed in Table 2.
Figure 2.
Thematic map illustrating descriptive and analytical themes and the relationships between them. Numbering represents each individual review finding under each descriptive theme as listed in Table 2.
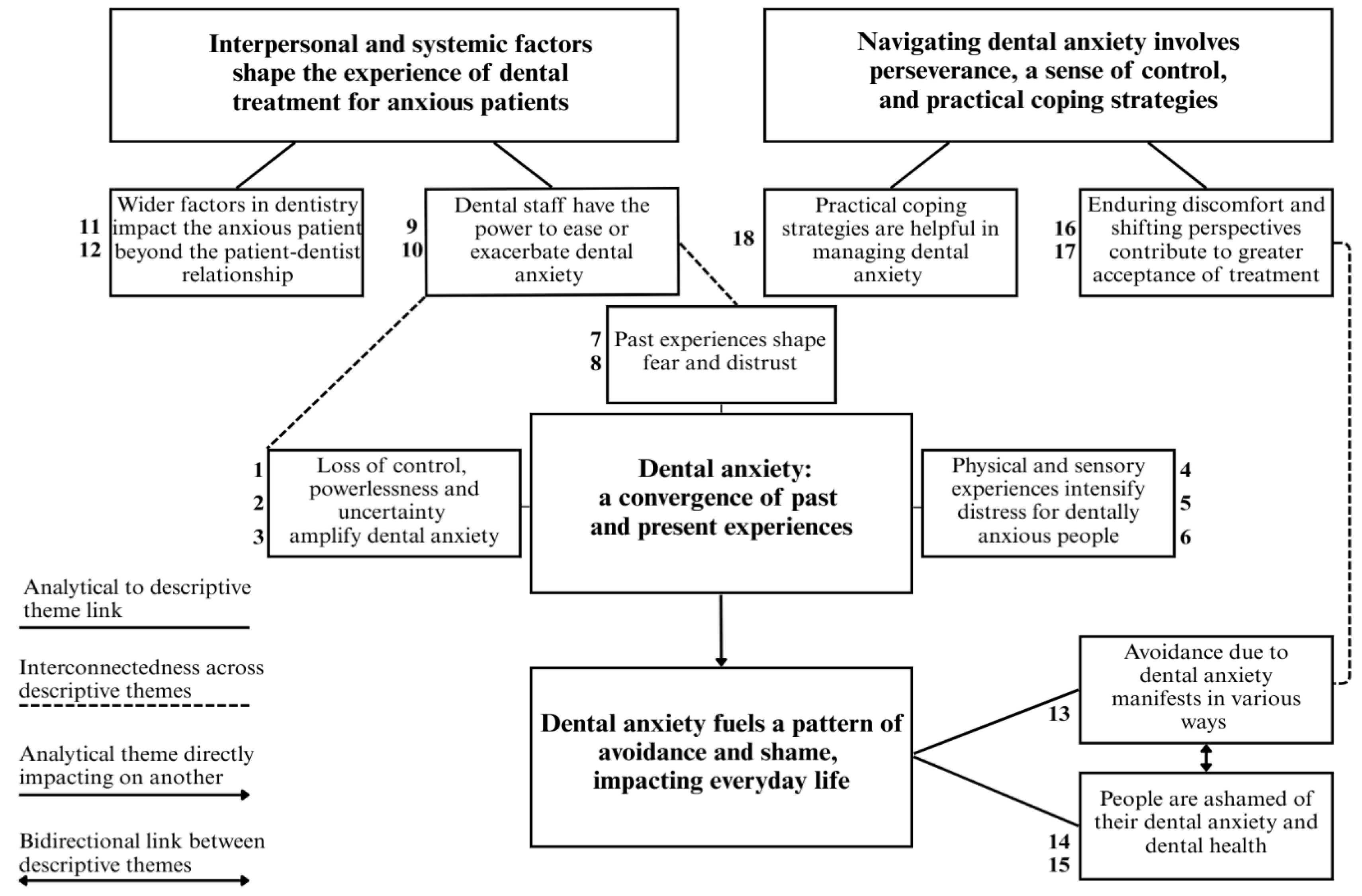

Table 1.
Summary of extracted data from primary studies included in qualitative evidence synthesis.
| Study Information | Participant Sample | Methods |
|---|---|---|
| Authors ‘Title’ |
Country Setting Number of participants Age |
Sampling strategy Qualitative data collection method Data analysis method |
| 1. Hoglund et al. (2024) ‘Dental professional recognition of dental anxiety from a patient perspective: a grounded theory study’ |
Sweden Various dental clinics N = 10 (5 men, 5 women) Range 37-68 years |
Purposive and convenience sampling Semi-structured interviews Grounded Theory |
| 2. Valastro et al. (2024) ‘Dentally anxious patients’ perceptions of oral health care’ |
United States Dental clinic N = 22 (6 men, 16 women) Range 18-71 years |
Purposive and snowball sampling Semi-structured interviews ‘Classic analysis’ |
| 3. Schneider et al. (2018) ‘Mental imagery in dentistry: Phenomenology and role in dental anxiety’ |
United Kingdom University N = 18 interviewed (2 men, 16 women) Range 18-47 years |
Convenience and purposive sampling Semi-structured interviews Thematic analysis |
| 4. Hultvall et al. (2010) ‘Factors of importance to maintaining regular dental care after a behavioural intervention for adults with dental fear: a qualitative study’ |
Sweden Specialist dental units N = 12 (4 men, 8 women) Range 25-64 years |
Convenience sampling Semi-structured interviews Thematic analysis |
| 5. Abrahamsson et al. (2002) ‘Dental phobic patients’ view of dental anxiety and experiences in dental care: A qualitative study’ |
Sweden Specialist dental fear clinic N = 18 (6 men, 12 women) Mean 39.4 years |
Strategic sampling Semi-structured interviews Grounded Theory |
| 6. Hoyvik et al. (2024) ‘Torture victims’ perspective on dental treatment: “Every sign you make, every move you take”’ |
Norway Specialist dental fear clinic N = 15 (5 men, 10 women) Range 30-65 years |
Snowball sampling Semi-structured interviews Thematic analysis |
| 7. Wolf et al. (2020) ‘Dental care—an emotional and physical challenge for the sexually abused’ |
Sweden Trauma treatment centres N = 13 (2 men, 11 women) Range 19-56 years |
Purposive sampling Semi-structured interviews Content analysis |
| 8. Calladine et al. (2022) ‘A survey of patients’ concerns about visiting the dentist and how dentists can help’ |
United Kingdom University and online N = 136 surveyed (22 men, 130 women) Range 18-82 years |
Convenience sampling Survey with open-ended questions Thematic analysis |
| 9. Moore et al. (2004) ‘The contribution of embarrassment to phobic dental anxiety: a qualitative research study’ |
Denmark Dental phobia research centre N = 30 (16 men, 14 women) Range 20-65 years |
Convenience sampling inferred Semi-structured interviews Thematic analysis |
| 10. Cohen et al. (2000) ‘The impact of dental anxiety on daily living’ |
United Kingdom Dental sedation clinic N = 20 (6 men, 14 women) Range 23-60 years |
Convenience sampling Semi-structured interviews Type of qualitative analysis not named |
| 11. Wang et al. (2017) ‘A qualitative study of patients’ views of techniques to reduce dental anxiety’ |
UK and Taiwan University N = 14 (3 men, 11 women) Range 18-49 years |
Purposive and snowball sampling Semi-structured interviews and focus groups Thematic analysis |
Table 2.
Summary of qualitative findings.
| Summary of review finding | Studies contributing to finding | Participant quotes from primary studies | CERQual confidence rating | Explanation of confidence rating |
|---|---|---|---|---|
| 1. People felt powerless, trapped, or unable to stop dental treatment. The feeling of loss of control increased anxiety. Some felt overwhelmed by sudden actions from the dentist or the inability to mentally prepare for treatment. Some linked fear to past experiences of boundaries being violated | 2, 4, 5, 7, 8, 9, 10 |
“You’re out of control, and you’re in a chair, you’re virtually, you know, laid back horizontal, lights and things and things in your mouth and, you know, you’re totally helpless” Cohen, et al. (2000) “I am afraid of how the dentist will do what he has to do and that I can’t stop him” Moore, et al. (2004) “Just that they are standing over one…or are sitting over one…” Wolf et al. (2020) |
Moderate confidence | 7 studies contribute. 6 moderate methodological concerns, 1 minor concerns. Coherence and adequacy are very good. Relevance issues largely very minor, with 1 moderate concern, 1 minor and 5 very minor concerns |
| 2. Uncertainty about treatment and fear of the unknown contributed to anxiety. People imagined worst-case scenarios and thoughts about pain or treatment going wrong | 1, 2, 3, 4, 5, 6, 7, 8, 10, 11 |
“The surprise is the worst anxious bit. Like the waiting when you’re not kind of sure… that’s stressful and they just get to work in your mouth” Wang, et al. (2017) “[I often think] about the things they could do to me, or I’ll be thinking about what could be wrong with my teeth and that’s painful.’ Schneider, et al. (2018) |
Moderate confidence | 10 studies contribute. 4 minor and 6 moderate methodological concerns. All report no or very minor coherence issues. Adequacy very good except for 1 with minor concerns. For relevance, 7 very minor, 2 minor, and 1 moderate concerns |
|
3. People described feeling emotionally overwhelmed and sometimes regressing to a childlike state of fear. Some experienced irritability, withdrawal, or a sense of dread |
4, 5, 10 |
“I’m very, very aware that I’ve got the, an appointment coming up, um, yeah, and I start getting nervous about it … I’m very aware that I can be, um, very snappy with other people, so I try, and kind of step back and keep myself to myself in work” Cohen, et al. (2000) “You start acting like a child again, you feel like a five-year-old and like the dentist is a giant” Hultvall, et al. (2010) |
Low confidence | Only 3 studies contribute. All exhibit moderate methodological concerns. All no or very minor coherence and adequacy issues. For relevance, 2 very minor and 1 moderate concerns. |
| 4. People experienced physiological symptoms and exhaustion related to dental visits. Some described feeling unable to move in the chair, forgetting to breathe, or almost blacking out. Anticipation of pain contributed to distress | 1, 2, 3, 4, 5, 7, 10 |
“When you’re afraid, you forget to breathe.” Hultvall, et al. (2010) “Everything just becomes impossible for me…I can’t handle it. I almost blackout…it goes through my whole self…” Abrahamsson, et al. (2002) |
Moderate confidence | 7 studies contribute. 2 minor methodological concerns, 5 moderate methodological concerns and all no or very minor coherence issues. Adequacy very good. For relevance, 5 very minor, 1 minor, and 1 moderate concerns |
| 5. People talked about the dental environment including sounds, smells, and sensations of dental tools. Some people talked about finding the clean atmosphere reassuring, but others described discomfort relating to this. Some experienced fear at the sight of dental equipment or images of procedures | 3, 6, 11 |
“He picked the needle up…. [from] the small box you know…It is scary as well because I imagine like, oh my God, that kind of thing will go into my teeth” Wang, et al. (2017) “And then this really obvious dentist smell, when you’re there. It’s just like (pretending being thrown back), it really hits you” Schneider et al. (2018) “It is clinical. It’s nice because… you know it’s clean” Schneider, et al. (2018) |
Low confidence | Only 3 studies contribute. 2 moderate and 1 minor methodological concerns. All have no or very minor coherence and adequacy issues. For relevance, 2 very minor and 1 minor concerns |
| 6. Anxiety was linked to physical sensations and discomfort with unwanted physical contact. Needle phobia and fear of choking or suffocation added to distress levels | 3, 5, 6, 7, 8, 10, 11 |
“I am very careful not to let people touch my face. And you know, dentists do just that” Wolf et al. (2020) “I think I’ll suffocate or drown in the water when I can’t breathe…” Abrahamsson, et al. (2002) |
Moderate confidence | 7 studies contribute. 1 very minor, 1 minor and 5 moderate methodological concerns, All no or very minor coherence issues. Adequacy very good except for 1 minor concerns. For relevance, 5 very minor, 1 minor, and 1 moderate concerns |
| 7. People described painful and distressing dental procedures, including inadequate anaesthesia, forceful extractions, and mistreatment by dentists. These experiences were often perceived as aggressive, frightening, or violating, leading to negative memories | 2, 3, 4, 5, 6, 7, 8, 9 |
“And I’ll just never forget at the end he says, ‘Wow! If I knew they had roots like that, I would have sent him to an oral surgeon” Valastro, et al. (2024) “I remember that I screamed like a wild animal that I didn’t want them to do it. So, they just closed the door into the clinic, then in come a couple more assistants and I was held down” Moore, et al. (2004) |
Moderate confidence | 8 studies contribute, 1 minor methodological concerns, 6 moderate methodological concerns, 1 minor concerns. All no or very minor coherence issues and adequacy is very good except for 1 minor concerns. For relevance, 6 very minor, 1 minor, and 1 moderate concerns |
| 8. Trauma led to long-term fear, anxiety, and trust issues. Some individuals reported post-traumatic stress reactions. Feelings of helplessness were common among those with a history of trauma | 2, 5, 6, 7, 8, 11 |
“It’s more as if the body…my body is reminded (prolonged exhalation) of it. It is more that than the thoughts themselves, but it is in fact…that is to say…it is the same disagreeable feeling or…so…as with …abuse” Wolf, et al. (2020) “Had a lot of painful experiences as a child with a mocking and rough dentist. So much so that the taste of mint brought me out in a sweat and panic” Calladine, et al. (2022) |
Moderate confidence | 6 studies contribute. 6 moderate methodological concerns. All no or very minor coherence issues. Adequacy very good except for 1 minor concerns and for relevance, 5 very minor, and 1 moderate concerns |
| 9. People talked about the importance of dental professionals recognising and understanding anxiety and providing reassurance | 1, 2, 4, 5, 6, 7, 8, 11 |
“I appreciate the fact that the dental care staff know I’m afraid, so I don’t have to talk to them about it” Hultvall, et al. (2010) “If the dentist asks if you’re nervous at the beginning it means that you start the appointment with everyone knowing where they stand” Calladine, et al. (2022) |
Moderate confidence | 8 studies contribute. 2 minor methodological concerns, 5 moderate concerns, and 1 minor concerns. All report no or very minor coherence issues. Adequacy very good except for 1 with minor concerns and for relevance, 6 very minor, 1 minor, and 1 moderate concerns |
| 10. People discussed power imbalances. People appreciated transparency, clear instructions, and the ability to speak up when distressed. People wanted straightforward communication and a collaborative relationship with the dentist | 1, 2, 4, 5, 6, 7, 8, 9, 11 |
“When you have difficult information to digest, but if the information is done by somebody who cares and then maybe he uses a lower tone and making the pace slower. Like he speaks slowly then gentle, then all the information… it will reduce your anxiety and then you can feel like, yes, I want to do this treatment” Wang, et al. (2017) “I’ve learned what demands I can make on my part” Hultvall, et al. (2010) |
Moderate confidence | 9 studies contribute. 1 minor methodological concerns, 7 moderate methodological concerns, and 1 minor concerns. All no or very minor coherence issues. Adequacy very good except for 1 study with minor concerns and for relevance, 7 very minor, 1 minor, and 1 moderate concerns |
| 11. People voiced concerns about the speed and efficiency of treatment, the discomfort or pain caused by rushed procedures due to service pressures, and the frustration with delays in treatment. It is difficult to strike a balance between efficiency and quality of care | 1, 6, 8 |
“They just administer, there is not the same ... feeling that there is time to talk, they just work” Hoglund, et al. (2024) “Yes, sometimes it’s painful. He does it fast! When he does it fast, sometimes I’m in a lot of pain. He must work more slowly! But I don’t know why he…Every time I go there and sit…he shows up late…And then, in 15 minutes he is done!” Hoyvik, et al. (2024) |
Low confidence | 3 studies contribute. 1 minor methodological concerns, 2 moderate methodological concerns. All no or very minor coherence issues. Adequacy very good and for relevance, 2 very minor and 1 minor concerns |
| 12. Wider aspects of dental treatment, out of the control of the patient or the dentist included the waiting room environment, scheduling conflicts, and the wider influence of media on dental fears | 2, 4, 6, 10 |
“It’s really uncomfortable sitting like that for so long!” Calladine, et al. (2022) “…. saw “Marathon Man” a little while back. I’ve not seen it and then, er there was, er, some horrible Nazi dentist in it, and I had to switch the film off. I just couldn’t watch it.” Cohen, et al. (2004) |
Low confidence |
4 studies contribute. 4 moderate concerns, All no or very minor coherence issues and adequacy very good. For relevance, 3 very minor and 1 moderate concerns |
| 13. People described anxiety-driven behaviours, with some avoiding dental visits, treatments, or thoughts of dental care to reduce their distress. Some tried to manage their dental anxiety through strict oral hygiene routines to prevent dental issues, or self-treatment | 1, 2, 3, 4, 5, 9, 10 |
“I had roots in my mouth, so I used my own tools to remove the things that hurt; I took painkillers constantly” Hultvall, et al. (2010) “I avoid any food that might be sticky” Valastro, et al. (2024) “I don’t think about it if I can help it” Schneider, et al. (2018) |
Moderate confidence | 7 studies contribute. 1 minor methodological concerns, 5 with moderate concerns, and 1 minor concerns. All no or very minor coherence issues and adequacy very good except for 1 with minor concerns. For relevance, 5 very minor, 1 minor, and 1 moderate concerns. |
| 14. People described shame and embarrassment about their dental anxiety, including fear of judgment from others. Some noticed a positive shift from being able to openly talk about their dental anxiety | 1, 4, 5, 8, 9, 10, 11 |
“I hate it (not being able to control my fear). It’s bad for my self-esteem… I think what kind of a damned old woman am I really? It’s childish to think like that but…why can’t I cope with this?” Abramsson, et al. (2002) “I can tell you that it really is a load off my mind to be able to talk about going to the dentist” Moore, et al. (2004) |
Moderate confidence | 7 studies contribute. 1 minor methodological concerns, 5 moderate and 1 very minor. All no or very minor coherence issues and adequacy very good except 1 minor concerns. For relevance, 5 very minor, 1 minor, and 1 moderate concerns |
| 15. People described the impact of shame, embarrassment, self-criticism, and regret about their dental and oral health and the fact they have neglected their teeth or avoided treatment. Some talked about the impact dental health has had on life | 5, 7, 8, 9, 10 |
“You feel judged because the state of your teeth is entirely your responsibility/fault. You can’t blame it on anyone else” Calladine, et al. (2022) “I have actually walked out of a dinner once because I actually felt so embarrassed, and the woman I was with had beautiful white teeth. Straight. I was embarrassed, and I walked out…” Cohen, et al. (2000) |
Moderate confidence | 5 studies contribute. 1 minor methodological concerns, 4 moderate methodological concerns and all no or very minor coherence issues. Adequacy very good except for 1 with minor concerns. For relevance, 4 very minor and 1 minor concerns |
| 16. People acknowledged the importance of treatment, showing motivation to engage in it despite discomfort. Some shared that they push through discomfort, feeling rewarded afterward with improved oral health | 2, 3, 4, 7 |
“I have shiny teeth at the end of it. So, everything is clean and nice. I really, really like the sensation of having really like squeaky clean teeth” Schneider et al. (2018) “It’s just something I force myself to do and get over. I just force myself to get through it” Valastro, et al. (2024) |
Low confidence | 4 studies contribute. 1 minor methodological concerns, 3 moderate concerns. No or very minor coherence issues and adequacy very good except for 1 with minor concerns. For relevance, 3 very minor and 1 minor concerns |
| 17. Some people talked about their perspective shifting and trying to overcome dental anxiety, sometimes through interventions. Some describe gaining a sense of control, recognising their ability to manage anxiety | 1, 2, 4, 5, 7, 9 |
“It was very important that you got to know the dentist, it wasn’t just a dentist but there was a person behind... you have ... have humanized the dentist ...from being a tool for horror and fear to becoming another human who treats you” Hoglund, et al. (2024) “I learned more about myself, about my own fear and what I could do about it” Hultvall, et al. (2010) |
Moderate confidence | 6 studies contribute. 1 minor methodological concerns, 5 moderate methodological concerns and all report or very minor coherence issues. Adequacy very good except for 1 with minor concerns. For relevance, 5 very minor and 1 minor concerns |
| 18. People found distraction relaxation and breathing exercises to be helpful coping strategies. People would like control over being able to stop treatment and written explanations to help them to feel prepared. Some mentioned sedation as a coping strategy | 1, 2, 3, 4, 8, 9, 11 |
“Yes, breathing is important, as the dental care staff have reminded me. . . and that was exactly what happened in the beginning” Hultvall, et al. (2010) “I’m a bit of a slow reader. I prefer to go through things on my own… I think it would be best if they told me something (websites) and I could go look it up myself as well” Wang, et al. (2017) |
Moderate confidence | 7 studies contribute. 1 minor methodological concerns, 5 with moderate concerns, and 1 with minor concerns. No or very minor coherence issues and adequacy very good except for 1 with minor concerns. For relevance, 5 very minor, 1 minor, and 1 moderate concerns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



