
Submitted:
22 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Introduction: Healthcare workers experience high rates of job-related stress and burnout, contributing to a substantial burden of mental and emotional health conditions. Exposure to natural environments is associated with improved mental health outcomes. However, for healthcare workers, the effects of nature in the workplace have been underexplored. This analysis reports the health effects of gaining a window view of nature among a sample of healthcare workers.Methods: In November 2023, a rehabilitation hospital moved its primary location from a midsize [redacted for anonymous review] city to a nearby area surrounded by woodlands. Employees completed surveys on work environment, job satisfaction and burnout, and health-related outcomes prior to the move, four weeks after the move, and one year after the move.Results: In difference-in-differences models controlling for gender, age, and change in job category, participants who gained a window view of a natural environment had greater odds of experiencing improvements in their reported satisfaction of their window view (OR=8.05, p=0.02). However, no statistically-significant improvements were reported for outcomes relating to job satisfaction, stress, burnout, or mental health associated with the change in window view. Conclusions: Although participants gaining window views of nature reported increases in window view satisfaction, we found no changes to job-related or health-related outcomes either at the first followup or one year after the move associated with gaining a window view of nature. Greater doses of nature in workplace environments, or different kinds of strategies, may be necessary to promote mental health among healthcare workers.
Keywords:
nature
; window view
; healthcare
; stress
; workplace
Introduction
Research shows that healthcare workers have disproportionately high rates of job-related stress and burnout, with some statistics suggesting rates double the level of the general population. [1] The burden of burnout in this population increased in recent years as a result of the COVID-19 pandemic, particularly for physicians and nurses. [2] The result of prolonged workplace stressors, employees experiencing burnout report exhaustion and cynicism toward their work. [3] Burnout is also significantly associated with other mental and emotional health outcomes, including anxiety and depression. [4]
Beneficial associations between exposure to natural environments and greenspace and positive health outcomes, including mental wellbeing, [5] have been well established in literature. Although the conceptualization of greenspace in these studies is frequently concerned with the environment surrounding participants’ homes, other sources of exposure have been shown to be effective at improving health outcomes. In a foundational study, Ulrich et al. found that surgery patients who were assigned to rooms with window views of nature recovered more quickly than did patients who did not have such views. [6] Since then, the concept of bringing natural environments and views of natural environments into healthcare settings have become increasingly prominent. For example, many hospitals have implemented healing gardens designed as semi-private emotional retreats to enable patients to relax, refocus, and deal with stressors. [7]
Window views of nature have also been explored in workplace settings as a strategy to deal with job stress. Workplace exposure to nature and window views of nature have been associated with increased job satisfaction [8], and reduced stress [9] and greater reported wellbeing. [10] One study of office workers found that views of sky, trees, flowers, and park-like environments were associated with higher satisfaction with window views, and that higher satisfaction with window views was subsequently associated with better work ability and job satisfaction. [11] However, despite these promising findings, the effect of window views of nature for work-related and mental health outcomes for healthcare workers have been underexplored.
In summer 2023, the [redacted for anonymous review] relocated its main facility in [redacted for anonymous review] from [redacted for anonymous review] to a new facility in [redacted for anonymous review], a nearby less densely-developed suburban area surrounded by woodlands. Practitioners based in the [redacted for anonymous review] location moved their primary work locations to the new [redacted for anonymous review] facility, which had plans for outdoor therapy gardens, green spaces, and trails on the grounds. [12] This move was expected to increase the exposure of many of these employees to natural environments during the workday, especially through increasing window views of nature.
To test the effect of this increased exposure to window views of nature, we conducted a series of surveys of [redacted for anonymous review] healthcare workers, with a baseline several weeks before the planned move, a first follow-up survey several weeks after the move, and a second follow-up a year later. Surveys asked participants about aspects of the work environment, including their window views, as well as job satisfaction, stress, and mental and emotional health outcomes. This study reports the results of our investigation of the effects of gaining a window view of nature on these outcomes among our participants.
Methods
The move of employees from the city hospital to the suburban hospital provided the opportunity to conduct a natural experiment. Based on survey data from employees before and after the move, we considered participants exposed if they gained a window view of nature following the move. Employees who did not gain a window view of nature served as controls. We used difference-in-differences models to assess changes to employee’s perceptions of their window views, job stress and job satisfaction, and health-related variables.
Survey
We conducted a series of electronic surveys among hospital employees, using an instrument that assessed job-related outcomes and perceived health outcomes. Items relating to job satisfaction and job stress were job satisfaction, work ability, workplace supportiveness, and resilience. The survey assessed job satisfaction with the multiple-choice question “How would you rate your overall job satisfaction? Very satisfied, satisfied, neither satisfied nor dissatisfied, dissatisfied, or very dissatisfied.” For analysis, we binarized this question as “Very satisfied or satisfied” versus all other responses. We assessed work ability with the single question “How do you rate your current work ability compared to when it was best?” which is operationalized as a continuous 0-10 value with 0 indicating “completely unable to work” and 10 indicating “work ability at its best.” We used the work supportiveness subscale of the Mini Z Worklife and Burnout Reduction Instrument, operationalized as continuous. [13] We assessed perceived resilience using the Brief Resilience Scale, [14] which we operationalized as continuous.
Health outcomes of interest were general perceived health, anxiety, depression, stress, physical activity, and sleepiness. We assessed perceived general health with the multiple choice question “Would you say your general health is… excellent, very good, good, fair, or poor?” We then binarized these responses as “Excellent or very good” versus “good, fair, or poor” for analysis. We used the Hospital Anxiety and Depression Scale [15] to assess anxiety and depression symptoms, which were each operationalized as continuous. We used the Perceived Stress Scale [16] for stress, operationalized as continuous. We operationalized physical activity as the number of days in the past week that participants reported exercising 30 minutes or more. We assessed sleepiness using the Epworth Sleepiness Scale [17].
Window Views
To assess participant window views in their primary workspace, window view content was assessed with the item “What dominates the view of the outdoor environment from your work station?” This survey question was adapted from Lottrup et al. (2015) [11] and included nine multiple choice responses: buildings/signs, cars/traffic, sky, trees, mowed lawn, flowers, park-like environment, wild self-seeded natural environment, or no view of the outdoor environment. Participants could also provide a free response if none of the multiple choice options were sufficient.
We categorized the responses of window views as “no window view,” “built environment view,” or “nature view.” Some participants reported a mix of built-environmental and natural features through their window, and these were categorized based on what seemed like the most predominant feature. For example, a response of “Parking lot, trees” was categorized as a built-environmental view, while a response of “we have traffic, bushes, trees, and sky” was categorized as a nature view. Participants who reported that they had no consistent workspace, such as participants who worked in patients’ homes, were coded as no response for this variable rather than a window view category.
Our main exposure variable for this analysis is the gain of a window view of nature, a longitudinal construction based on two waves of data of the window view question. Participants who responded to the window view question in both the baseline and first follow-up surveys were assigned a value for this exposure. Participants who did not report a window view of nature in the baseline survey, but did report a window view of nature in the first follow up, were considered “exposed.” Participants who did not report gaining a window view of nature served as the control group.
Recruitment
Hospital administrators sent out emails inviting employees to complete each of the surveys. Emails were sent to a listserv of all employees who were active at the time of each survey, including practitioners, administrators, clerical and service staff; the total number ranged between 1000 and 1500 employees.
Emails included a link and QR code to the online survey. Potential participants were notified that the survey was voluntary and their participation would not affect their employment. Participants of any of the surveys were enrolled in a drawing for twenty $50 gift cards distributed after the final survey. Because hospital administrators were involved in distributing the gift cards, administrators would be aware of the participation of the twenty winning participants. However, neither individual-level nor otherwise identifiable survey data were provided to the hospital, and the full list of email addresses of participants were kept confidentially by the research team.
The baseline survey was administered prior to the hospital move in July 2023, the first follow-up during October-November 2023, and the second follow-up during October-November 2024. The study protocol was approved by the Lehigh University Institutional Review Board (2063381-3).
Statistical Analysis
To determine the effect of gaining a window view of nature on job satisfaction and health outcomes, we employed a difference-in-differences analysis. Each outcome of interest was assessed in separate mixed-effect models with random intercepts for participant. Linear regression models were used for continuous outcome variables and logistic regression models were used for binary outcome variables. All models included a two-way interaction term between exposure status (gaining a window view between baseline and follow-up, or not) and survey wave, which served as the difference-in-differences parameter. Both uncontrolled models and models controlling for age, gender, and change in job category were computed.
Because relatively few participants completed all three surveys, the main models were restricted to the baseline and first follow-up waves. Participants were included in models if they had sufficient survey completion in the baseline and first follow-up waves to have complete data for all variables in each respective model. However, because this time period reflects only a few weeks after the move to the suburban location, it may not provide enough follow-up time for changes in outcomes to manifest. Therefore, a sensitivity analysis was performed restricted to the baseline and second follow-up waves, allowing a full year of follow-up time after the move. Participants were included in these models if they had sufficient survey completion in the baseline and second follow-up waves to have complete data for all variables in each respective model. All analyses were conducted in R version 4.4.3, and models were fitted in the lme4 package.
Results
Survey Respondents
A total of 330 participants partially completed the baseline survey, with 285 completing the survey fully. 128 participants fully completed both the baseline survey and the first follow-up. However, only 43 participants fully completed all three waves of surveys. Therefore, to preserve as much data as possible, all models focus on the baseline and first follow-up surveys.
The most common job category reported at baseline was therapist (n=269), followed by clerical jobs (n=88), registered nurses, (n=86), and management positions (n=85). Twenty participants reported changing job categories between baseline and the first follow-up. Additionally, at the first follow-up survey, 55 participants reported changing facilities after the baseline survey, of whom 35 reported that they moved to the new suburban facility.
Table 1 provides information on the demographic composition of the survey respondents at baseline, stratified by whether or not respondents gained a view of nature between baseline and the first follow-up, the primary exposure of this analysis. No demographic characteristic is statistically significantly different between exposure categories.
Window Views
In each survey wave, participants reported whether or not they had a window view in their work area, and if they did, what was visible through their window. Figure 1 presents the distributions of window views reported in each survey wave, including rates of missing data for this question. Between the baseline and first follow-up survey, the proportion of participants reporting a view of nature increased relative to participants reporting a built-environment view.
We constructed our main exposure variable, the gain of a nature view, for those participants who responded to the window view question in both the baseline survey and the first follow-up survey (n=146). Of these participants, 16 participants gained a window view of nature (intervened) and 130 did not (control). Participants who reported changing their work location between baseline and the first follow-up were more likely to gain a window view of nature (n=8, 20.5%) than participants who did not move between the two waves (n=8, 6.3%).
Table 2 shows the distribution of all outcome variables at the baseline survey, stratified by exposure category. No outcomes at baseline were statistically different between participants who did and did not gain a nature view, showing balance. Because only those participants who responded both to the baseline and first follow-up survey have a constructed “gained nature view” variable, the combined distribution of intervened and control participants does not necessarily match the overall distribution of all participants at baseline.
Modeling Results
In both controlled and uncontrolled models, participants who gained a window view of nature between baseline and followup were more likely to report an increase in their satisfaction with the window view (Table 3). Controlling for age, gender, and job change, participants who gained a nature view had 8.05 times the odds of increasing their satisfaction with the window view between baseline and followup than were participants who did not gain a window view. However, the relationship between gaining a nature view and changes in satisfaction with natural lighting was not significant. Both of these models assessing changes to perceptions of window view and lighting were by necessity restricted to those participants who reported some window view in both the baseline and first followup surveys, as participants without window views skipped survey questions relating to those window views.
Table 4 shows the results of models assessing the relationships between gaining a window view of nature and job-related variables. In uncontrolled models, there is a significant association between gaining a nature view and experiencing an increase in perceived workplace supportiveness (b=1.60, p=0.034), but this relationship is not maintained after controlling for age, gender, and job change, and no other job-related outcomes are significant. Similarly, Table 5 presents uncontrolled and controlled models for health-related outcomes, none of which have a significant relationship with gaining a window view of nature.
Although controlled difference-in-differences models demonstrate that participants who gained a window view of nature were more likely to report increases in their satisfaction with their window view, this increase in window view satisfaction does not translate to consistent improvements in job satisfaction or in mental or physical health outcomes between the baseline survey and first follow-up survey. A sensitivity analysis focusing on the contrast between the baseline and second follow-up survey to provide a longer follow-up window did not have sufficient positivity for stable results, but consistently with the main analysis did not find improvements in job satisfaction or health outcomes associated with gaining a window view of nature.
Discussion
Taking advantage of a natural experiment occurring when participants moved their primary work location to an area with greater exposure to nature, this study employed a longitudinal difference-in-differences approach to examine the effect of gaining a window view of nature on the job satisfaction and health of a sample of healthcare workers at a rehabilitation hospital. Consistent with prior research, participants who gained a window view of nature experienced increases in their satisfaction with their window view relative to participants who did not gain a window view of nature. However, effects on job satisfaction, stress, and health outcomes were not statistically significant. Although the main models used data from only a few weeks following the move, these results were consistent with models using one-year followup times.
Several important limitations to this study should be taken into account. First, although several hundred participants initially completed the baseline survey, retention at follow-up was inconsistent, and only eight participants reported gaining a window view of nature across survey waves. This low number of intervened participants limits the statistical power of our study as well as our ability to conduct more nuanced stratified analyses. Second, participants were not randomized to intervention categories. While we demonstrated statistical balance between exposed and control participants on all measured variables, unmeasured confounding is a risk in any nonrandomized design, and could threaten the validity of the results we report. Finally, our primary measure of exposure is based only on participant perception and self-report. This could compromise our ability consistently to categorize exposure status between participants, particularly when participants reported complex window views that mixed natural and built-environmental components, or if participants are inconsistent in defining their “primary work area.”
Our analysis is part of a growing body of research that goes beyond cross-sectional associations to assess the impact of interventions that increase participants’ exposure to natural environments. This work aims both to better elucidate causal relationships between greenspace and health as well as to determine what kind of interventions are effective at promoting wellbeing. While cross-sectional research frequently identifies positive associations between greenspace exposure and both physical and mental health, results from these intervention studies are less consistent. As interest in the concept of health promotion through greenspace increases, this work is increasingly important to determine the composition and magnitude of successful interventions. For example, while window views of nature have been demonstrated to be a successful intervention in patient populations, our study suggests that different intervention types (or higher “dosages” of nature) may be necessary to improve job satisfaction, reduce stress, and improve the mental health of healthcare workers. However, we also note that our results from a natural experiment of a facility move may not be generalizable to other kinds of interventions adding greenspace to workplaces, such as landscaping changes, garden construction, or building renovation.
Interventions other than workplace nature exposure may be beneficial for the mental health of healthcare workers. Studies suggest that burnout in this population can be attributed to too-high workloads, [2] including large amounts of bureaucratic tasks, [1] as well as aspects of organizational climate. [18] Hiring additional staff to manage growing workloads, streamlining work processes, promoting the autonomy of healthcare workers, and improving relationships with leadership have been demonstrated to reduce burnout rates. [19] In addition, other aspects of workplace physical environments, such as overall aesthetic appeal, privacy, safety, and layout changes that improve convenience and flow have been shown to improve job satisfaction among healthcare workers. [20]
Given the high rates of job-related stress and burnout experienced by healthcare workers, finding and implementing effective workplace interventions to improve employee mental health is essential. Given prior studies showing employee preferences for natural environments in the workplace, such as healing gardens, researchers should continue to explore the role of greenspace in healthcare settings both to improve patient outcomes as well as employee wellbeing.
Acknowledgments
We would like to thank Dr. Stephanie A. Kolakowsky-Hayner for assisting with the design and implementation of this research. No specific funding was obtained for this project. .
Conflicts of Interest
The authors declare no conflicts of interest regarding this manuscript.
References
- Reith, TP. Burnout in United States Healthcare Professionals: A Narrative Review. Cureus. Published online. 4 December 2018. [CrossRef]
- Ghahramani, S; Lankarani, KB; Yousefi, M; Heydari, K; Shahabi, S; Azmand, S. A Systematic Review and Meta-Analysis of Burnout Among Healthcare Workers During COVID-19. Front Psychiatry 2021, 12, 758849. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C; Schaufeli, WB; Leiter, MP. Job Burnout. Annu Rev Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Koutsimani, P; Montgomery, A; Georganta, K. The Relationship Between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Front Psychol. 2019, 10, 284. [Google Scholar] [CrossRef] [PubMed]
- Houlden, V; Weich, S; Porto de Albuquerque, J; Jarvis, S; Rees, K. The relationship between greenspace and the mental wellbeing of adults: A systematic review. PLoS ONE 2018, 13, e0203000. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, RS. View Through a Window May Influence Recovery from Surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Nieberler-Walker, K; Desha, C; Bosman, C; Roiko, A; Caldera, S. Therapeutic Hospital Gardens: Literature Review and Working Definition. HERD Health Environ Res Des J. 2023, 16, 260–295. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R; Bardwell, LV; Ford, HA; Kaplan, S. The corporate back-40: Employee benefits of wildlife enhancement efforts on corporate land. Hum Dimens Wildl. 1996, 1, 1–13. [Google Scholar] [CrossRef]
- Shin, Won-sop; Shin, WS. The influence of forest view through a window on job satisfaction and job stress. Scand J For Res. 2007, 22, 248–253. [Google Scholar] [CrossRef]
- Gilchrist, K; Brown, C; Montarzino, A. Workplace settings and wellbeing: Greenspace use and views contribute to employee wellbeing at peri-urban business sites. Landsc Urban Plan. 2015, 138, 32–40. [Google Scholar] [CrossRef]
- Lottrup, Lene; Lottrup, L; Stigsdotter, Ulrika K.; et al. The Workplace Window View: A Determinant of Office Workers’ Work Ability and Job Satisfaction. Landsc Res. 2015, 40, 57–75. [Google Scholar] [CrossRef]
- redacted for anonymous review.
- Linzer, M; McLoughlin, C; Poplau, S; et al. The Mini Z Worklife and Burnout Reduction Instrument: Psychometrics and Clinical Implications. J Gen Intern Med. 2022, 37, 2876–2878. [Google Scholar] [CrossRef] [PubMed]
- Smith, BW; Dalen, J; Wiggins, K; Tooley, E; Christopher, P; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int J Behav Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, AS; Snaith, RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S; Kamarck, T; Mermelstein, R. A Global Measure of Perceived Stress. J Health Soc Behav. 1983, 24, 385. [Google Scholar] [CrossRef] [PubMed]
- Johns, MW. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Bronkhorst, B; Tummers, L; Steijn, B; Vijverberg, D. Organizational climate and employee mental health outcomes: A systematic review of studies in health care organizations. Health Care Manage Rev. 2015, 40, 254–271. [Google Scholar] [CrossRef] [PubMed]
- Rehder, K; Adair, KC; Sexton, JB. The Science of Health Care Worker Burnout: Assessing and Improving Health Care Worker Well-Being. Arch Pathol Lab Med. 2021, 145, 1095–1109. [Google Scholar] [CrossRef] [PubMed]
- Jin, HY; Gold, C; Cho, J; Marzban, F; Lim, L. The Role of Healthcare Facility Design on the Mental Health of Healthcare Professionals: A Literature Review. HERD Health Environ Res Des J. 2023, 16, 270–286. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Window views in each wave.
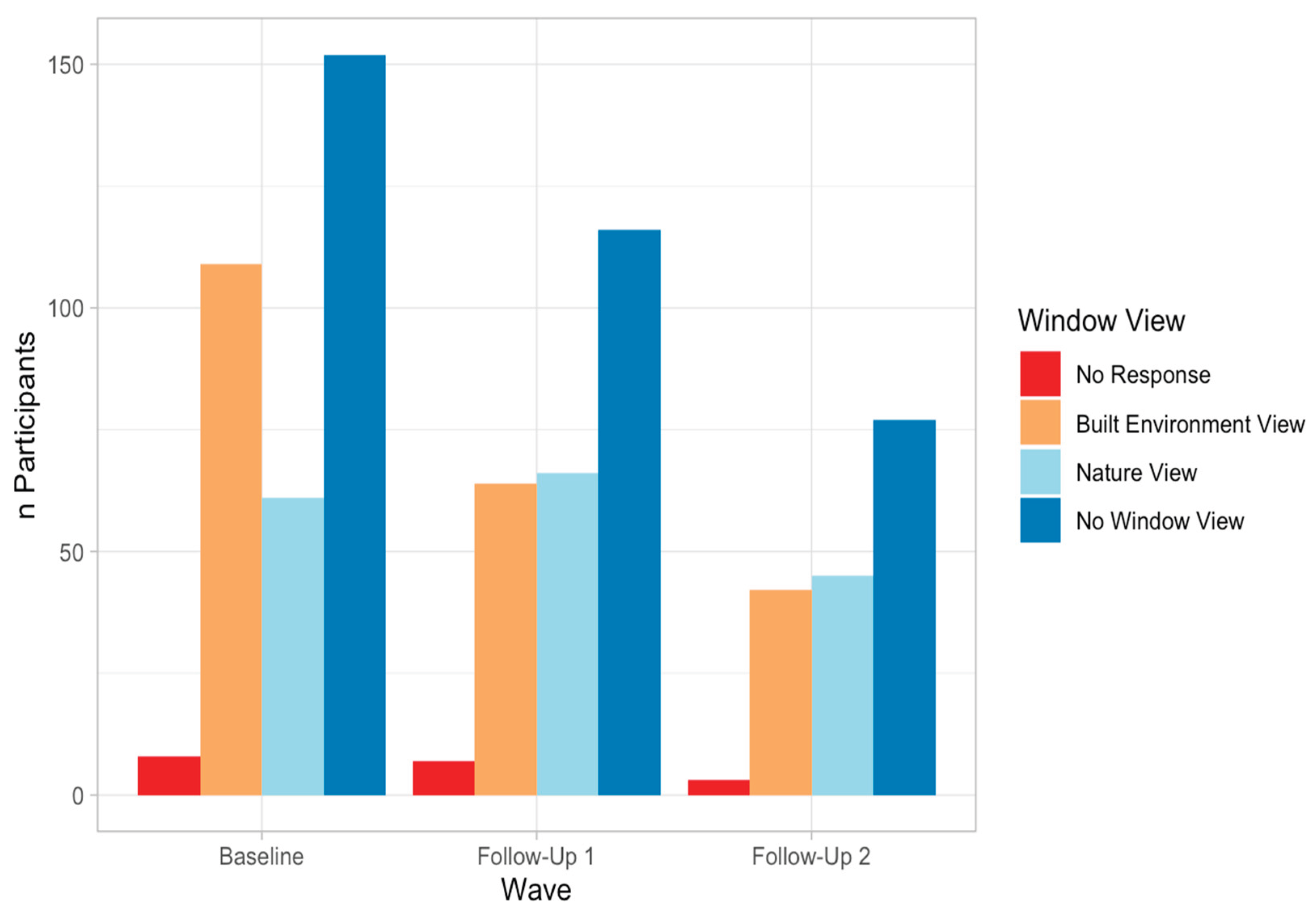

Table 1.
Participant Characteristics.
| Overall | Gained Nature View | Did Not Gain Nature View | P-value | ||
| Gender | Male | 45 (13.64%) | 3 (18.75%) | 19 (14.62%) | 0.863 |
| Female | 274 (83.03%) | 13 (81.25%) | 109 (83.85%) | ||
| Age | 44.55 (12.46) | 40.94 (12.32) | 44.6 (12.35) | 0.279 | |
| Race | White | 282 (85.45%) | 14 (87.5%) | 119 (91.54%) | 0.063 |
| Black | 8 (2.42%) | 0 (0%) | 3 (2.31%) | ||
| Asian | 10 (3.03%) | 0 (0%) | 2 (1.54%) | ||
| Other/Prefer Not to Answer | 23 (6.97%) | 2 (12.5%) | 5 (3.85%) | ||
| Ethnicity | Hispanic/Latino | 18 (5.45%) | 1 (6.25%) | 4 (3.08%) | 0.722 |
| Not Hispanic/Latino | 289 (87.58%) | 14 (87.5%) | 120 (92.31%) | ||
| Prefer not to answer | 15 (4.55%) | 1 (6.25%) | 5 (3.85%) |
Table 2.
Balance between intervened and control participants.
| Overall | Gained Nature View | Did Not Gain Nature View | P-value | |
|---|---|---|---|---|
| Natural Light Presence (Present) | 55.45% | 62.5% | 60.77% | >0.999 |
| Satisfaction with Window View (Very satisfied or satisfied) | 29.39% | 25% | 35.38% | 0.449 |
| Satisfaction with Window Lighting (Very satisfied or satisfied) | 73.64% | 93.75% | 72.31% | 0.120 |
| Job Satisfaction (Very satisfied or satisfied) | 80% | 93.75% | 83.08% | 0.493 |
| Work Ability | 7.9 (1.67) | 8.4 (0.97) | 7.9 (1.62) | 0.168 |
| Workplace Supportiveness | 18.2 (3.49) | 17.7 (2.81) | 18 (3.31) | 0.714 |
| Resilience | 3.7 (0.66) | 3.3 (0.73) | 3.7 (0.65) | 0.060 |
| General Health (Excellent or very good) | 49.7% | 43.75% | 54.62% | 0.492 |
| Anxiety | 6.7 (3.6) | 7.2 (3.19) | 7 (3.57) | 0.782 |
| Depression | 3.3 (2.59) | 3.2 (2.21) | 3.5 (2.72) | 0.674 |
| Stress | 15.6 (5.92) | 16.6 (5.81) | 15.5 (5.73) | 0.486 |
| Days of Physical Activity | 3.1 (2.06) | 2.4 (1.21) | 3.1 (2.16) | 0.064 |
| Sleepiness | 8.7 (2.06) | 8.3 (1.21) | 8.6 (2.16) | 0.883 |
Table 3.
Modeling results for window view satisfaction.
| Uncontrolled Models | Controlled Models | ||||
| Form | Parameter | P-value | Parameter | P-value | |
| Satisfaction with Window View | Binary | 6.54 | 0.01 | 8.05 | 0.02 |
| Satisfaction with Window Lighting | Binary | -0.4 | 0.78 | -0.49 | 0.73 |
Table 4.
Modeling results for job-related outcomes.
| Uncontrolled Models | Controlled Models | ||||
| Form | Parameter | P-value | Parameter | P-value | |
| Job Satisfaction | Binary | 363.2 | 0.62 | 158.7 | >0.99 |
| Work Ability | Continuous | 0.06 | 0.91 | 0.12 | 0.82 |
| Workplace Supportiveness | Continuous | 1.6 | 0.03 | 1.18 | 0.14 |
| Resilience | Continuous | 0.24 | 0.09 | 0.28 | 0.05 |
Table 5.
Modeling results for health outcomes.
| Uncontrolled Models | Controlled Models | ||||
| Form | Parameter | P-value | Parameter | P-value | |
| General Health | Binary | -0.55 | 0.83 | -1.14 | 0.67 |
| Anxiety | Continuous | -0.52 | 0.44 | -0.53 | 0.46 |
| Depression | Continuous | 0.28 | 0.60 | -0.14 | 0.81 |
| Stress | Continuous | -1.72 | 0.17 | -2.16 | 0.11 |
| Physical Activity | Continuous | 0.28 | 0.49 | 0.1 | 0.81 |
| Sleepiness | Continuous | 0.68 | 0.49 | 0.55 | 0.61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



