
Submitted:
22 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Introduction: Sequencing therapy in CD is currently intensively discussed due to the development of novel drugs and lack of standardized criteria for drug positioning in first and further treatment lines. The aim of this study was to compare the efficacy of a second line advanced therapy in Romanian patients with CD who have failed an anti-TNF agent. Methods: We performed a multicenter retrospective study that included adult patients with CD who had secondary loss of response after an initial response with an an-ti-TNF drug. The main outcome was clinical remission at 12 weeks of second-line treatment (CDAI < 150). Secondary outcomes included clinical response (decrease of CDAI ≥ 25%), persistence of therapy at 1 year and rates of adverse events. Results: From 2008 to 2024, 216 patients were either switched to another anti-TNF or swapped to another therapeutic class due to failure of a first anti-TNF drug. Secondary lines of treatment in-cluded infliximab (IFX), adalimumab (ADA), vedolizumab (VDZ), ustekinumab (UST). The highest rate of clinical remission (81%) was obtained with the sequence ADA-IFX in 26/32(81%) patients and ADA-UST in 62/82(76%) patients, followed by IFX-UST in 22/33(67%) and IFX-ADA 34/51(67%). Persistence on therapy at 1 year was better for the sequence ADA-UST(73%) and IFX-UST(67%) and ADA-IFX(63%) compared to IFX-ADA(59%) and IFX-VDZ(44%)(p< 0.001). Conclusions: In patients with CD who have failed a first anti-TNF, the highest rate of clinical re-mission at 12 weeks was obtained with second line IFX and UST whilst vedolizumab showed lower efficacy. UST demonstrated the most favorable long-term treatment persistence at 1 year.
Keywords:
Crohn’s disease
; treatment sequencing
; biologic therapy
; second-line therapy
; real-world data
; infliximab
; adalimumab
; ustekinumab
; vedolizumab
1. Introduction
Crohn’s disease (CD) is an inflammatory bowel disease that causes relapsing inflammation in the gastrointestinal tract that can lead to irreversible bowel damage and increase in disability. The physiopathology of the disease is explained by an abnormal immune response to a complex interplay of factors, including genetic susceptibility, environmental triggers, and an alterations in the gut microbiota [1,2]. Incidence of CD is increasing worldwide and all age groups can be affected, from children to elderly [3]. At the moment, there is no treatment that can permanently cure the disease, which leads to high clinical, social, economic and psychological burden [4]. Since 1990, starting with the approval in Europe of infliximab as the first biologic agent for the treatment of CD and followed by adalimumab and golimumab, the use of anti-TNF has significantly improved CD outcomes [5,6,7,8,9]. Despite initial efficacy, a significant proportion of patients experience secondary loss of response to anti-TNF drugs or develop adverse reactions or intolerance, necessitating change of therapy [10]. In the last 10 years, significant advances have been made in the field of CD with the development of new molecules that target different immunological pathways with promising results in achieving disease control [11]. Alongside the expanding therapeutic landscape and improved insight into the natural history of CD, there has been a paradigm shift toward tighter disease control. As a result, treatment goals have progressed beyond clinical remission, aiming for deeper endpoints, including endoscopic healing and even transmural remission [12,13]. Emerging data demonstrates a decreased efficacy of advanced therapy when used in bio-experienced patients when compared with bio-naïve patients, highliting that the choice of second-line therapy could be a key determinant of long-term disease control [14,15].
For patients with CD following anti-TNF failure, there is still insufficient evidence to determine the optimal choice of second-line therapy [11]. This topic remains an area of active research. One of the maincontroversies is whether patients who experience secondary loss of response to an anti-TNF agent should be switched to a different agent within the same class or should transition to a drug with different mechanism of action [16]. Currently there are no definitive position statements or guideline-endorsed algorithms for the selection of a second-line therapy after anti-TNF failure. The existing literature data comes from network analysis, metanalysis and retrospective observational studies based on real-world clinical cohorts [17,18,19]. More extensive real-world data and larger cohort studies are needed to better inform second-line therapeutic strategies.
Our study aimed to assess the comparative efficacy of second-line biologic therapies in a multicenter cohort of Romanian patients with CD who experienced secondary loss of response to a first anti-TNF agents.
2. Material and Methods
2.1. Participants and Eligibility
We conducted a retrospective study, which enrolled all patients diagnosed with and treated for Crohn's disease between January 2008 - December 2024, registered in the Romanian inflammatory bowel disease database (IBD Prospect), from six Gastroenterology departments across Romania: academic centers from Bucharest, Iasi and Cluj. The enrolled patients met the inclusion criteria as outlined below. 547 patients with Crohn’s disease on biologic therapy were screened for the study. 295 (55%) were excluded because they remained on first-line biologic. Of the 252 people who required a switch to 2nd line treatment, 36 patients had Ustekinumab as their first line of treatment, so they were also excluded from the study.
The study included patients diagnosed with CD based on standard diagnostic criteria as determined by the physicians who had been receiving anti-TNF agents – IFX (infliximab) or ADA (adalimumab) – for at least 3 months, had an initial response to therapy as defined by a decrease of Crohn’s disease Activity Index (CDAI) with at least 25%, had secondary loss of response defined by clinically active disease (CDAI >150) and had received at least 12 weeks of therapy with a second-line biologic agent. The choice of second-line therapy after anti-TNF failure was made at the discretion of the treating physician based on clinical judgment and local practice.
IBD phenotype, history of surgical interventions, treatment initiation and discontinuation dates, diagnostic delay (defined as the time from first symptoms to diagnosis), the interval from diagnosis to initiation of first biologic therapy and levels of fecal calprotectin, hemoglobin, and C- reactive protein at the time of biologic switch and periodically during disease monitoring were all systematically recorded.
All patients provided written informed consent.
The study was approved by the Ethics Committee of the Fundeni Clinical Institute.
2.2. Statistical Analysis
The main outcome was clinical remission at 12 weeks of second-line treatment defined by CDAI < 150. Secondary outcomes included clinical response at 12 weeks on therapy defined by decrease of CDAI ≥ 25%, persistence of therapy at 1 year and rates of reported adverse events. Patients who failed to achieve either remission or response were classified as primary non-responders. The data analysis was conducted employing the statistical software SPSS (version 20.0, IBM Corporation, Armonk, NY, USA). The assessment of data normality was executed through the Kolmogorov-Smirnov test. Quantitative variables exhibiting a parametric distribution were presented as mean and standard deviation, while those with a non-parametric distribution were summarized as median with the range between minimum and maximum values. For comparative analysis, the independent sample t-test was utilized for normally distributed data, while the Mann-Whitney U test was employed for non-normally distributed data. Categorical variables were expressed as percentages and subjected to comparison using Fisher's exact test. A two-sided hypothesis testing approach was applied, and a p-value less than 0.05 was deemed indicative of statistical significance.
3. Results
3.1. Biologic Therapy Utilization and Baseline Cohort Characteristics
Following data screening and application of the eligibility criteria, a total of 216 patients who had failed first-line anti-TNF therapy were included in the final analysis. The follow-up duration had a median of 48 months ( minimum 24 months and maximum 180 months). Baseline characteristics of the overall cohort are summarized in Table 1.
Second-line therapies were represented by a second anti-TNF (IFX or ADA), UST (ustekinumab) and VDZ (vedolizumab). The most common second-line treatment sequence was ADA followed by UST in 82 (32.5%) of patients. This was followed in frequency by the IFX to ADA sequence in 51 (20.2%) patients, IFX to UST in 33 (13.2%) patients, ADA to IFX in 32 (12.7%) patients and IFX to VDZ in 18 (7.1%) patients. The highest CDAI scores at 2nd line therapy initiation were observed in the group of patients who failed IFX as first line and were treated with VDZ in second line. The highest levels of fecal calprotectin were observed in IFX failure group and received as second-line therapy UST, ADA or VDZ. Perianal disease was observed most frequently among patients who experienced first-line failure with IFX and were subsequently treated with ADA as second-line therapy, comprising 18 (35.4 % ) patients. The stricturing phenotype was predominantly found among patients who failed ADA and were most frequently switched to UST 34 (41.5%) and IFX 24 (75%) patients respectively. Patients’ characteristics across different second-line biologic treatment strategies are shown in Table 2.
3.2. Efficacy of Second-Line Therapy After Anti-TNF Failure
Overall, patients reported a complete clinical response rate of 70.7% at 12 weeks, a partial response rate of 11.8%, while the non-response rate was 16.8%.
Figure 1 shows the comparative results obtained with second-line biological therapy when patients were treated in the first-line with Adalimumab.
The highest clinical remission rate at 12 weeks was observed in ADA- IFX group with 81% of patients achieving remission ( n=26 out of 32) (p<0.001 for the comparison with the group treated with IFX in the first line and ADA in second line. This was followed by the ADA-UST group, where 76 % of patients achieved clinical remission ( n=62 out of 82).
Clinical response rates at 12 weeks when Infliximab was used in the first line are represented in Figure 2. IFX- UST and IFX-ADA groups both with 67 % remission rate ( n=22/33 and 34/51), respectively (p<0.001 for comparison with people who received first-line treatment with ADA).
The highest partial clinical response rate at 12 weeks was observed in the IFX- UST group (21%, 7/33), followed by ADA-IFX (19%, 6/32), IFX-ADA (18%, 9/51), and ADA- UST (17%, 14/82), p<0.001.
Primary non -response to second-line therapy was observed in the IFX-UST group (21%, 7/33), followed by ADA-UST (17%,14/82), IFX-ADA (18%, 9/51), and IFX-VDZ (17% 3/18),p<0.001. No cases of primary non-response were recorded in the ADA-IFX group.
In Figure 3 we represented persistence on treatment over a year with 2nd line biological therapy (on different therapeutic sequence).
The highest persistence rate at 1 year was observed in the ADA-UST group where 73% of patients (n=60/82) remained on therapy. This was followed by IFX-UST, with a persistence rate of 67% (n=22/33), and ADA-IFX with 62.5 % (n=20/32). In the IFX-ADA group, 59% of patients (n=30/51) maintained treatment at 1 year while the lowest persistence was recorded in the IFX-VEDO sequence where only 44 % of patients ( n=8/18) continued therapy. These differences were statistically significant ( p<0.001). 43 patients out of 216 (20%) discontinued 2nd-line biological treatment, most due to loss of response (38, that is 17.5%), and only a minority (5) due to adverse events. 4 adverse events were recorded in the group ADA→ IFX, one severe allergic reaction and 3 severe bacterial infections. In the IFX-ADA group, a severe bacterial infection (pulmonary tuberculosis) was the reason for discontinuation of 2nd-line biological treatment.
4. Discussion
Anti TNF agents were the first biologic therapies introduced for the treatment of moderate-to-severe CD and despite the emergence of multiple other monoclonal antibodies and therapeutic molecules, they continued to be widely used as first-line biologic therapy in CD [11,20,21]. Real-life data from Romania shows that Infliximab and Adalimumab have similar efficacy and safety profile in the treatment of Crohn's disease [22,23].
However, long-term data have consistently shown high rates of loss of response after an initial favorable response (secondary loss of response) in more than 50% of patients over exposure to anti-TNF agents [24,25,26,27]. Our study screened 547 persons in total, but 55% were excluded, because they persisted on Infliximab or Adalimumab, a proportion similar to data in the literature; we assessed the comparative efficacy of second-line biologic treatments in a multicenter cohort of 216 Romanian patients with CD who experienced secondary loss of response to an initial anti- TNF therapy and we evaluated the 1-year persistence to second-line treatment as a measure of long-term therapeutic efficacy. Patients in this cohort were treated with both the original molecules and biosimilars, given that existing studies demonstrate that they have comparable efficacy and safety [28,29]. When comparing clinical outcomes across second-line biologic sequences we found that ADA-IFX sequence demonstrated the highest rate of clinical remission (81%) at 12 weeks. Guideline recommendations suggest that in the case of primary non-response to a first anti-TNF agents, switching to a biologic with a different mechanism of action is advised. Conversely, in cases of secondary loss of response, transitioning to a second anti-TNF agent within the same class may be considered [21]. However real-world evidence and randomized clinical trial data are conflicting. Kapizioni C. et al demonstrated that VDZ and UST both offer similar superior efficacy as second line therapy in CD following anti-TNF failure rather than a second anti-TNF [16]. Also results from Attauabi M. et al. network metanalysis (NMA) concluded that in bio-exposed CD patients upadacitinib and risankizumab ranked highest in inducing clinical response (including adalimumab exposed patients), however infliximab was not investigated in these group [19]. In a NMA, Singh S. et al. suggests ADA (after secondary loss of response to IFX) or Risankizumab as preferred second line therapy in CD [30]. Most of these studies did not differentiate between secondary loss of response due to immunogenicity, where switching to another anti-TNF might still be effective and loss of response occurring despite adequate drug levels that would suggest a loss of response due to the ineffective mechanism of action. Furthermore anti TNF therapeutic drug monitoring was not performed in most studies at the point of treatment failure. Consistent with limitations observed in previous research, our study did not include therapeutic drug monitoring at the time of secondary loss of response. Furthermore in both ulcerative colitis and CD, IFX and ADA efficacy does not appear to be equivalent even at therapeutic drug levels. In perianal fistulizing CD, guideline recommendations suggests anti-TNF therapy, IFX being preferred over ADA [11]. While comparative data in CD remain limited, stronger evidence exists in UC where IFX has demonstrated superior efficacy over ADA [31]. Our study showed that the highest rate of clinical remission in induction was achieved in patients with CD treated with IFX as second line therapy after adalimumab failure. This finding contributes additional evidence in positioning anti TNF agents efficacy in CD and suggests that IFX may be an effective option for patients who fail first line ADA therapy. Significantly higher rates of clinical remission at 12 weeks were also observed in the sequence ADA-UST in 76% (63/82) of patients. Our findings are consistent with the previously published data that position UST as a high potency molecule in second-line after anti-TNF therapy [16,32,33]. The lowest rates of clinical remission were observed in the IFX-VDZ group in 44% (8/18). Along with the existing literature data our findings suggest that VDZ may be a better option as a first-line therapy in CD [34,35,36]. However, it is important to take into consideration the small sample size included in our study and that the majority of patients 55.6% (10/18) had perianal CD. Considering CD phenotype, the highest proportion of perianal fistulizing CD was seen in the IFX-ADA group 35% (18/52 ) patients, in which the primary endpoint of clinical remission after induction was achieved at a significant rate of 67%. The highest proportion of stricturing CD was seen in ADA-IFX group followed by ADA-UST group: 75% (24/32) patients and 41.5%(34/82) patients, respectively; both groups achieved clinical remission at 12 weeks with significant rates of 81% and 76 %. The data supports the benefit of these sequences of biologics after anti-TNF failure in this subgroup of patients.
The highest persistence rate at 1 year was observed in the ADA-UST group, where 73% of patients (n=60/82) remained on therapy, followed by IFX-UST with a persistence rate of 67% (n=22/33). The results are consistent with the favorable long-term persistence profile of UST reported in the literature [37,38].
ADA-IFX group has also shown significant high rates of treatment persistence at 1 year: 62.5% (20/32 patients). This significantly better persistence on biological treatment when ADA was prescribed in the first line is also described in a recently published study by Louis E. et al, who used a semi-Markov sequential model in order to identify the optimal position of ADA and VDZ in the treatment sequence in Crohn’s disease [34].
Our study has several limitations. Firstly, the relatively small study cohort that may limit the generalizability of our findings. Secondly, the retrospective design is inherently associated with potential selection bias, missing data, and unmeasured confounders. The most important limitation is that there are statistically significant differences between the patients included in the 5 therapeutic sequences (IFX→UST, IFX→ADA, ADA→IFX, ADA→UST, IFX→VDZ) in terms of age at onset, disease location, evolutionary pattern, proportion of smokers, proportion of people with perianal fistulas and those who required surgical interventions for resection of the small intestine or colon.
Third, therapeutic drug monitoring values at baseline were not available, preventing assessment of TNF drug levels sat the time of secondary loss of response. Finally, information regarding whether patients received optimized dosing during second-line therapy was not systematically recorded. While acknowledging these limitations, it is important to highlight the study’s main strengths. We performed a multicenter analysis that provides real-world evidence in a field where data on second-line biologic sequencing in CD remain limited. Moreover, we included long-term assessment of treatment persistence at 1 year, adding clinically relevant information to guide therapeutic decision making.
5. Conclusions
In this multicenter real-world cohort of Romanian patients with CD experiencing secondary loss of response to a first anti-TNF, second-line IFX and UST achieved the highest clinical remission rates at 12 weeks while VDZ showed lower effectiveness. UST demonstrated the most favorable long-term treatment persistence at 1 year. These findings provide additional evidence to guide second-line biologic sequencing in CD.
Author Contributions
Corina Meianu drafted the manuscript. Carmen Monica Preda designed and carried out the study. Anca Trifan, Alina Tantau, Ana Maria Singeap, Cristian Tieranu, Horia Minea, Ana Maria Buzuleac, Lucian Negreanu, Remus Popescu, Andreea Bota, Tudor Stroie, Cosmin Alexandru Ciora carried out the study. Mircea Diculescu contributed by critical revision of the manuscript. All authors read and approved the final manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
Corina Meianu, Carmen Monica Preda, Anca Trifan, Alina Tantau, Ana Maria Singeap, Cristian Tieranu, Lucian Negreanu, Tudor Stroie, Mircea Diculescu received honoraria and educational grants from Abbvie, Ewopharma, Sandoz, Johnson&Johnson, Takeda, CellTrion.
References
- Torres, J; Mehandru, S; Colombel, JF; Peyrin-Biroulet, L. Crohn's disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Alatab, S; Sepanlou, SG; Ikuta, K; et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet Gastroenterology & Hepatology 2020, 5, 17–30. [Google Scholar] [CrossRef]
- Hracs, L; Windsor, J.W; Gorospe, J; et al. Global evolution of inflammatory bowel disease across epidemiologic stages. Nature 2025, 642, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Keyashian, K; Dehghan, M; Sceats, L; Kin, C; Limketkai, BN; Park, KT. Comparative Incidence of Inflammatory Bowel Disease in Different Age Groups in the United States. Inflamm Bowel Dis. 2019, 25, 1983–1989. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/remicade. [CrossRef] [PubMed]
- Hanauer, SB; Feagan, BG; Lichtenstein, GR; et al. Maintenance infliximab for Crohn's disease: the ACCENT I randomised trial. Lancet 2002, 359, 1541–1549. [Google Scholar] [CrossRef]
- Colombel, J; Sandborn, WJ; Rutgeerts, P; et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn's disease: the CHARM trial. Gastroenterology 2007, 132, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Olivera, P; Thiriet, L; Luc, A; Baumann, C; Danese, S; Peyrin-Biroulet, L. Treatment Persistence for Infliximab Versus Adalimumab in Crohn's Disease: A 14-Year Single-Center Experience. Inflamm Bowel Dis. 2017, 23, 976–985. [Google Scholar] [CrossRef]
- Sands, BE; Anderson, FH; Bernstein, CN; et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl Journal Med 2004, 350, 876–85. [Google Scholar] [CrossRef]
- Blesl, A; Binder, L; Högenauer, C; et al. Limited long-term treatment persistence of first anti-TNF therapy in 538 patients with inflammatory bowel diseases: a 20-year real-world study. Aliment Pharmacol Ther. 2021, 54, 667–677. [Google Scholar] [CrossRef]
- Gordon, H; Minozzi, S; Kopylov, U; et al. ECCO Guidelines on Therapeutics in Crohn's Disease: Medical Treatment. J Crohns Colitis 2024, 18, 1531–1555. [Google Scholar] [CrossRef]
- Turner, D; Ricciuto, A; Lewis, A; et al. International Organization for the Study of IBD. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- Le Berre, C; Ricciuto, A; Peyrin-Biroulet, L; Turner, D. Evolving Short- and Long-Term Goals of Management of Inflammatory Bowel Diseases: Getting It Right, Making It Last. Gastroenterology 2022, 162, 1424–1438. [Google Scholar] [CrossRef]
- Bressler, B. Is there an optimal sequence of biologic therapies for inflammatory bowel disease? Therap Adv Gastroenterol. 2023, 16, 17562848231159452. [Google Scholar] [CrossRef] [PubMed]
- Pudipeddi, A; Ko, Y; Paramsothy, S; Leong, RW. Vedolizumab has longer persistence than infliximab as a first-line biological agent but not as a second-line biological agent in moderate-to-severe ulcerative colitis: real-world registry data from the Persistence Australian National IBD Cohort (PANIC) study. Therap Adv Gastroenterol. 2022, 15, 17562848221080793. [Google Scholar] [CrossRef] [PubMed]
- Kapizioni, C; Desoki, R; Lam, D.; Parkes, M; Raine, T.; UK IBD BioResource Investigators. Biologic Therapy for Inflammatory Bowel Disease: Real-World Comparative Effectiveness and Impact of Drug Sequencing in 13 222 Patients within the UK IBD BioResource. J Crohns Colitis 2024, 18, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Barberio, B; Gracie, DJ; Black, CJ. Efficacy of biological therapies and small molecules in induction and maintenance of remission in luminal Crohn’s disease: systematic review and network meta-analysis. Gut 2023, 72, 264–274. [Google Scholar] [CrossRef]
- Kappelman, MD; Adimadhyam, S; Hou, L; et al. Real-World Evidence Comparing Vedolizumab and Ustekinumab in Antitumor Necrosis Factor-Experienced Patients With Crohn's Disease. Am J Gastroenterol. 2023, 118, 674–684. [Google Scholar] [CrossRef]
- Attauabi, M; Steenholdt, C; Poulsen, A; et al. Network meta-analysis: Comparative onset of early effect of biologics and small molecules in moderately to severely active luminal Crohn's disease. Aliment Pharmacol Ther. 2024, 60, 124–143. [Google Scholar] [CrossRef]
- Feuerstein, JD; Ho, EY; Shmidt, E; American Gastroenterological Association Institute Clinical Guidelines Committee. AGA Clinical Practice Guidelines on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn's Disease. Gastroenterology 2021, 160, 2496–2508. [Google Scholar] [CrossRef]
- Lamb, CA; Kennedy, NA; Raine, T; Gaya, DR; Iqbal, TH; Taylor, SA; Smith, M; Brookes, M; Hansen, R; Hawthorne, AB; IBD guidelines eDelphi consensus group. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef]
- Preda, CM; Fulger, LE; Negreanu, L; Manuc, M; Sandra, I; Diculescu, MM. Adalimumab versus infliximab in treating post-operative recurrence of Crohn's disease: a national cohort study. Rev Esp Enferm Dig. 2016, 108, 642–647. [Google Scholar] [CrossRef]
- Preda, C; Fulger, LE; Gheorghe, L; et al. Infliximab and Adalimumab in Crohn’s disease: real- life data from a national cohort study. Current Health Sciences Journal 2016, 42, 115–124. [Google Scholar]
- Papamichael, K; Cheifetz, AS. Use of anti-TNF drug levels to optimise patient management. Frontline Gastroenterol. 2016, 7, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K; Cheifetz, AS; Melmed, GY. Appropriate Therapeutic Drug Monitoring of Biologic Agents for Patients With Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol. 2019, 17, 1655–1668.e3. [Google Scholar] [CrossRef]
- Solitano, V; Facciorusso, A; McGovern, DPB; et al. HLA-DQA1∗05 Genotype and Immunogenicity to Tumor Necrosis Factor-α Antagonists: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2023, 21, 3019–3029.e5. [Google Scholar] [CrossRef] [PubMed]
- Mateescu, RB; Gheorghe, C; Trifan, AV; et al. Safety, Efficacy and Persistence of Advanced Therapies in Inflammatory Bowel Disease: Results from ORIGINS. A Retrospective Observational Study. J Gastrointestin Liver Dis. 2023, 32, 444–451. [Google Scholar] [CrossRef]
- Tursi, A; Mocci, G; Cuomo, A; et al. Replacement of Adalimumab Originator to Adalimumab Biosimilar for a Non-Medical Reason in Patients with Inflammatory Bowel Disease: A Real-life Comparison of Adalimumab Biosimilars Currently Available in Italy. J Gastrointestin Liver Dis. 2022, 31, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Gros, B; Plevris, N; Constantine-Cooke, N; et al. Multiple infliximab biosimilar switches appear to be safe and effective in a real-world inflammatory bowel disease cohort. United European Gastroenterol J. 2023, 11, 179–188. [Google Scholar] [CrossRef]
- Singh, S; Murad, MH; Fumery, M; et al. Comparative efficacy and safety of biologic therapies for moderate-to-severe Crohn's disease: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2021, 6, 1002–1014. [Google Scholar] [CrossRef]
- Singh, S; Loftus, EV, Jr.; Limketkai, BN. AGA Clinical Guidelines Committee. AGA Living Clinical Practice Guideline on Pharmacological Management of Moderate-to-Severe Ulcerative Colitis. Gastroenterology 2024, 167, 1307–1343. [Google Scholar] [CrossRef]
- Feagan, BG; Sandborn, WJ; Gasink; UNITI–IM-UNITI Study Group. Ustekinumab as Induction and Maintenance Therapy for Crohn's Disease. N Engl J Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef]
- Sharip, MT; Nishad, N; Pillay, L; et al. Ustekinumab or Vedolizumab after Failure of Anti-TNF Agents in Crohn's Disease: A Review of Comparative Effectiveness Studies. J Clin Med. 2024, 13, 2187. [Google Scholar] [CrossRef]
- Louis, E; Litkiewicz, M; Agboton, C; Armuzzi, A. Therapeutic sequencing in inflammatory bowel disease: Determining the optimal position of vedolizumab for long-term Crohn's disease control using real-world evidence. United European Gastroenterol J. 2024, 12, 574–584. [Google Scholar] [CrossRef]
- Sandborn, WJ; Feagan, BG; Rutgeerts, P; et al. GEMINI 2 Study Group. Vedolizumab as induction and maintenance therapy for Crohn's disease. N Engl J Med. 2013, 369, 711–21. [Google Scholar] [CrossRef] [PubMed]
- Alric, H; Amiot, A; Kirchgesner, J; Tréton, X; et al. Vedolizumab Clinical Decision Support Tool Predicts Efficacy of Vedolizumab But Not Ustekinumab in Refractory Crohn's Disease. Inflamm Bowel Dis. 2022, 28, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Abreu, MT; Rowbotham, DS; Danese, S. Efficacy and Safety of Maintenance Ustekinumab for Ulcerative Colitis Through 3 Years: UNIFI Long-term Extension. J Crohns Colitis 2022, 16, 1222–1234. [Google Scholar] [CrossRef] [PubMed]
- Afif, W; Arasaradnam, RP; Abreu, MT. Efficacy and Safety of Ustekinumab for Ulcerative Colitis Through 4 Years: Final Results of the UNIFI Long-Term Maintenance Study. Am J Gastroenterol. 2024, 119, 910–921. [Google Scholar] [CrossRef]
Figure 1.
Rate of response in patients treated with ADA as 1ST line sequence.
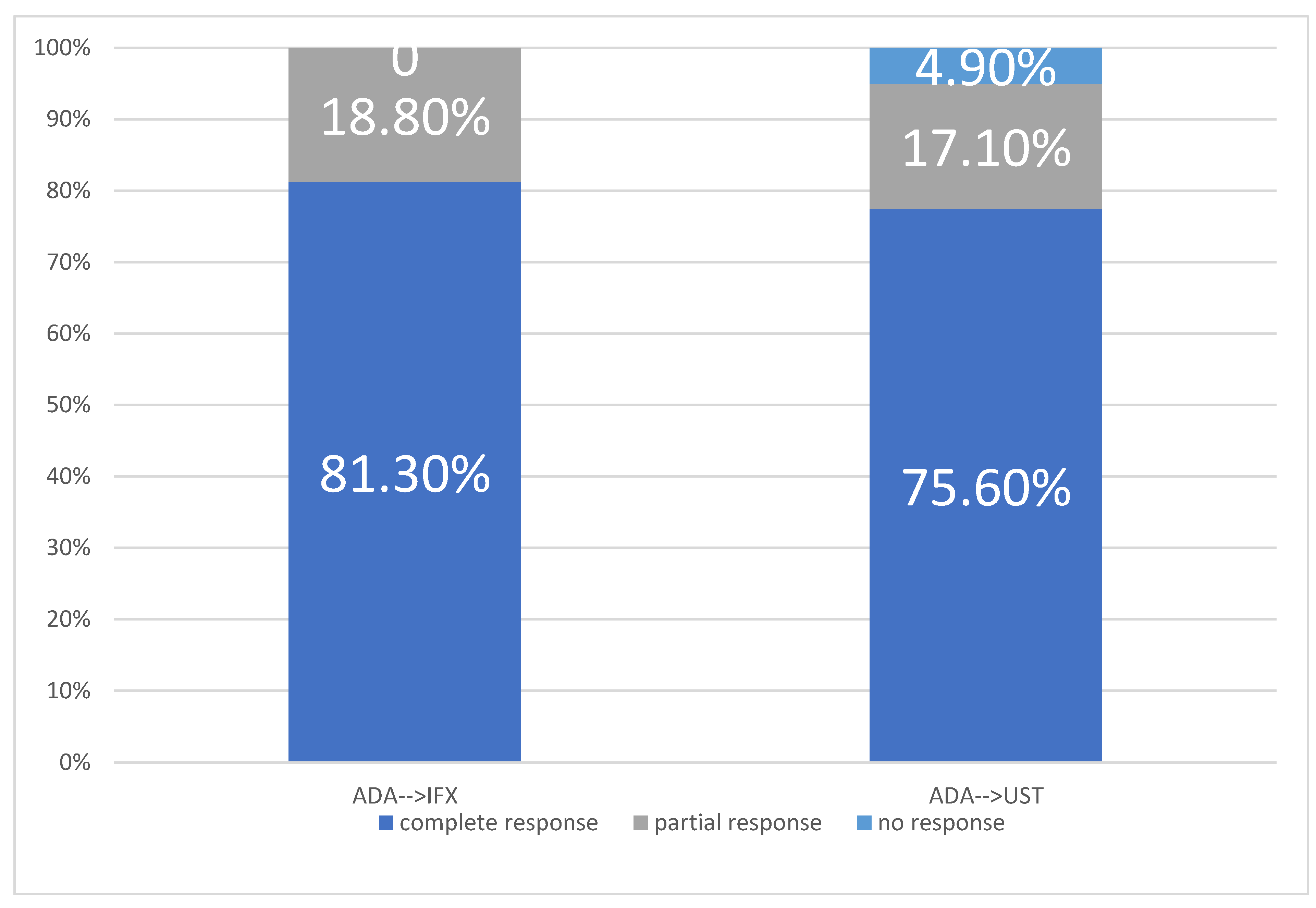
Figure 2.
Rate of response in IFX as 1ST line sequence.
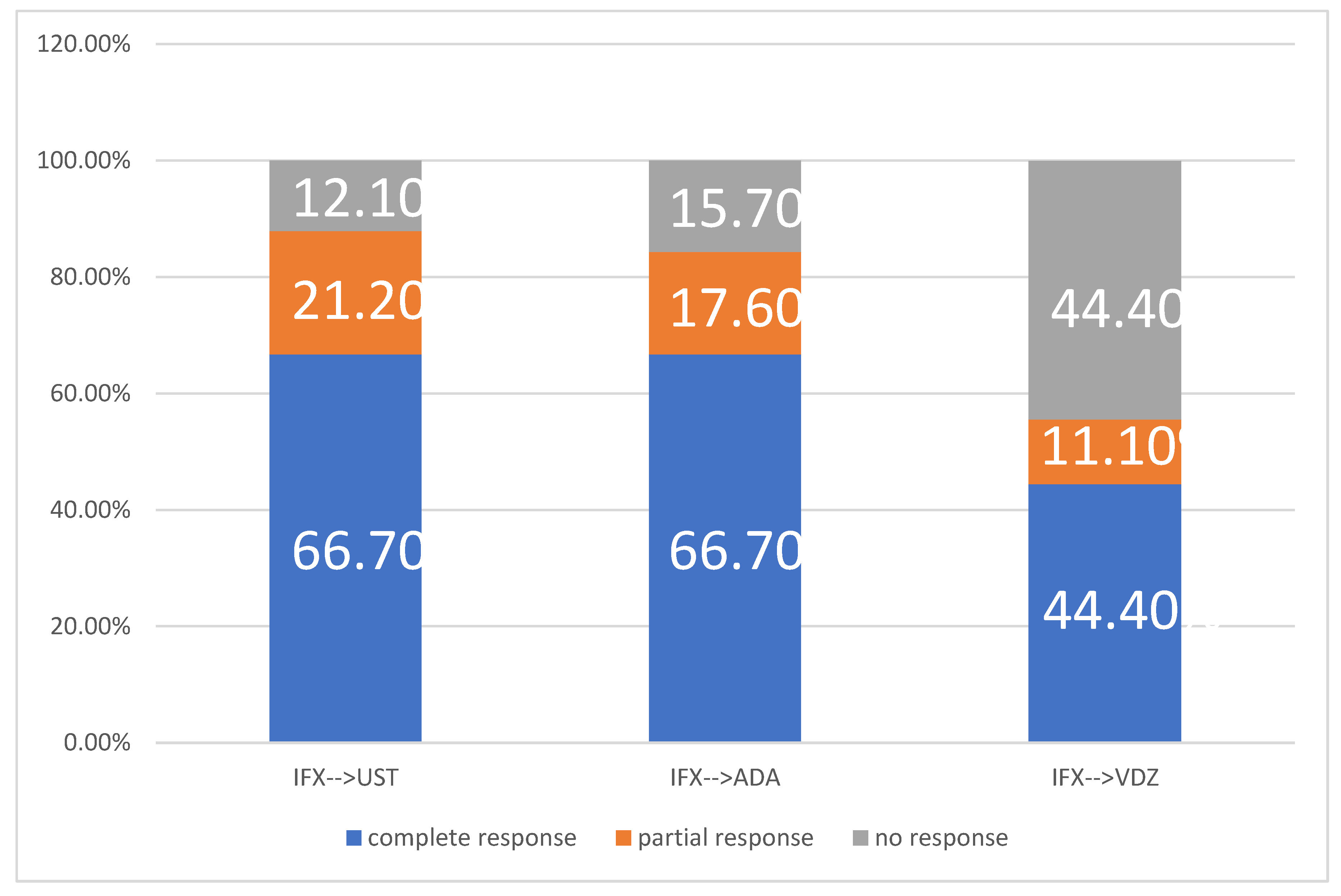
Figure 3.
Persistence on treatment over one year with 2nd line biological therapy (on different therapeutic sequence).
Figure 3.
Persistence on treatment over one year with 2nd line biological therapy (on different therapeutic sequence).
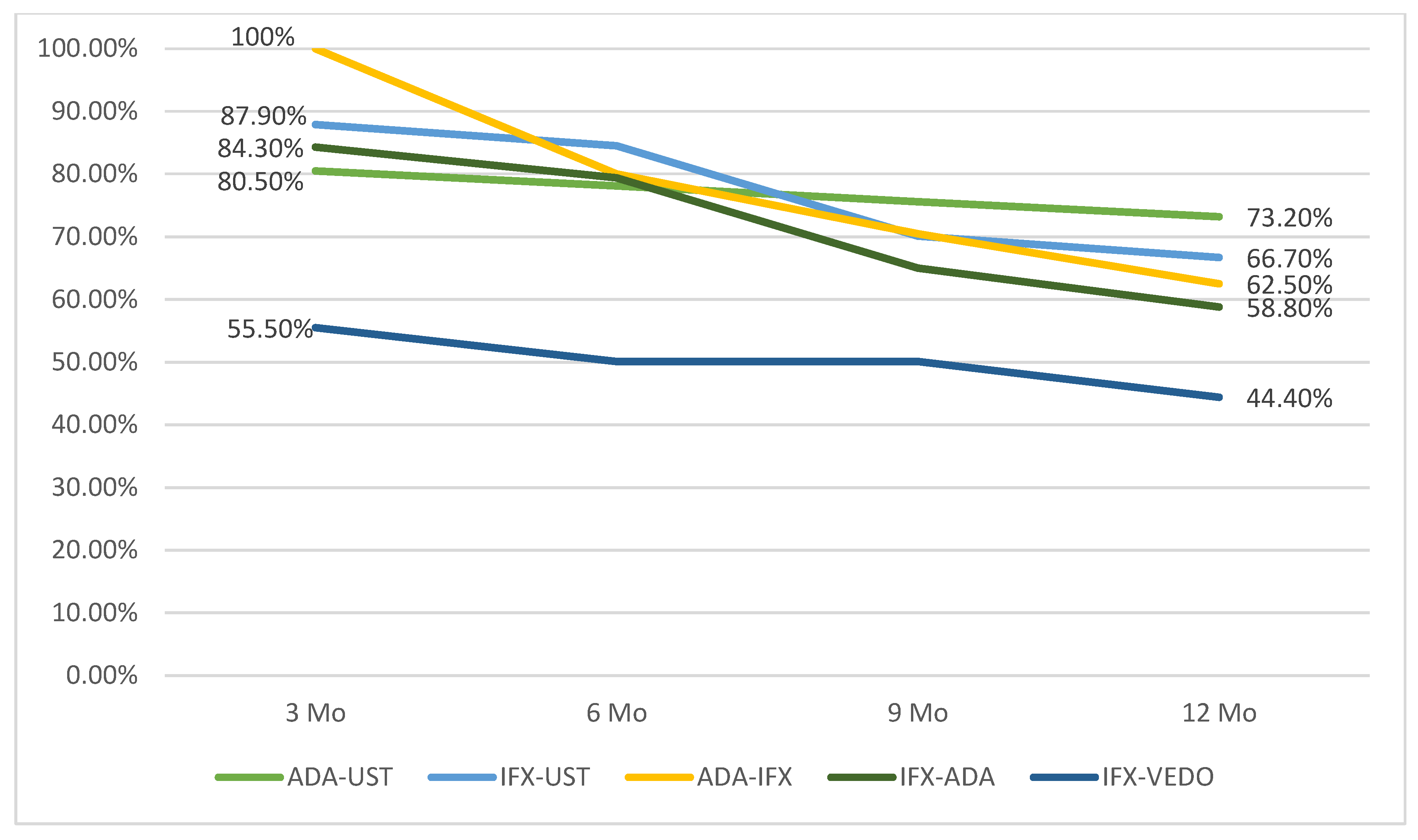

Table 1.
Baseline characteristics of the overall cohort.
| Number of Patients | 216 (100%) |
| Sex | Males - 129 (59.7%) Females –87 (40.3%) |
| Age (medina,minim, maxim ) | 33 (11- 69) |
| Smokers | Active Smokers – 86 (39.7%) Ex-smokers – 17 (7.9%) Non-smokers – 113 (52.4%) |
| BMI (median,minim,maxim) | 23.38 (10.34, 40.40) |
| Location- ileal | 63 (29) |
| Location- ileo-colonic | 63 (29) |
| Location-colonic | 90 (42.10) |
| Non-stricturing, non fistulizing | 114 (53%) |
| Stricturing | 66 (30.4) |
| Perianal disease | 35 (16.4%) |
| Surgical Intervention | 81 (31.9%) |
| CDAI (median, minim-maxim) | 245 ( 150, 557) |
| Calprotectin (median, minim,maxim) | 650 ( 3.30, 7762) |
| Hb at initiation (median, minim, maxim) | 12.7 (5.4, 17) |
| CRP at initiation (median, minim, maxim) | 11.2 (0.15, 270) |
| Latency from symptoms to diagnosis (months) (median, minim, maxim) |
7 (1-288) |
| Interval diagnosis-biologic initiation (months) (median, minim, maxim) |
8 (1-444) |
BMI:Body Mass Index, CDAI:Crohn’s Disease Activity Index, Hb:hemoglobin, CRP:C-reactive protein.
Table 2.
Patient characteristics by type of second-line biologic therapy.
| IFX→ UST |
IFX→ ADA |
ADA→ IFX |
ADA→ UST |
IFX→ VDZ |
p-value | |
| Patient No (%) | 33 (13.1%) | 51 (20.2%) | 32 (12.7%) | 82 (32.5%) | 18 (7.1%) | |
| Age (median, minim, maxim | 25 (17-42) | 28 ( 11-35) | 29 (28-39) | 34 (18-69) | 37 (27- 50) | <0.001 |
| Smoker No ( %) |
4 (12%) | 28 (55%) | 10 (31%) | 38 (46%) | 12( 67%) | <0.001 |
| BMI (median, minim, maxim | 23 (18-28.4) | 21 (19-30) | 24 (22-26) | 21 (18-40.4) | 24 (21-27) | 0.005 |
| L1: ileal L2: colonic L3: ileo-colonic |
L1: 5 (15.2%) L2 : 8 (24.2%) L3: 20 (60.6%) |
L1: 15 (29.4%) L2: 22 (43.1%) L3: 14 (27.5%) |
L1: 18 (56.2%) L2: 2 (6.2%) L3: 12 (37.6%) |
L1 : 26 (31.7%) L2 :20 (24.4%) L3 : 36 (43.9%) |
L1 – 0 (0%) L2 – 10 (55.6%) L3 – 8 (44.4%) |
<0.001 |
| Non- stricturing non penetrating: No (%) | 19 (57.6%) | 23 (45.1%) | 6 (18.8%) | 40 (48.8%) | 14 (77.8%) | <0.001 |
| Stricturing: No (%) | 12 (36.3%) | 20 (39.2%) | 24 (75%) | 34 (41.5%) | 2 (11.1%) | <0.001 |
| Perianal | 6 (18.2%) | 18 (35.3%) | 12 (37.5%) | 10 (12.2%) | 10 (55.6%) | <0.001 |
| Surgery | 18 (54.5%) | 24 (47.1%) | 20 (62.5%) | 34 (41.5%) | 2 (11.1%) | <0.001 |
| CDAI (median, minim, maxim) | 260 (150- 557) | 224 ( 156- 390) | 216.5 (150-370) | 260 (150- 520) | 350 (162-432) | <0.001 |
| Calprotectin (median, minim, maxim) |
1000 ( 236- 2950) | 1115.96 (3.3- 2500) |
567 (345-1100) | 968 (123- 3241) | 1050 (111-2325) | <0.001 |
| Hgb at initiation (median, minim, maxim) |
11.8 (8.60- 16.10) | 13.1 (10-15.6) | 12 (10-15.8) | 12.9 (6.4-16.6) | 11.4 ( 9- 13.2) | 0.010 |
| CRP at initiation (median, minim, maxim) |
8 (2-37) | 12 (1.11 -116) | 22.9 (7 - 200) | 11.1 (0.15- 120) | 45 (12-101) | <0.001 |
| Latency from symptoms to diagnosis (months) (median, minim, maxim) |
8 (1- 15) | 6 (1-120) | 12 (4-240) | 5 (1- 72) | 8 (2- 36) | <0.001 |
| Interval from diagnosis to biologic initation (months) (median, minim, maxim) |
8 (1- 276) | 10 (1-444) | 11 (1- 144) | 8.5 (1- 108) | 84(3- 120) | 0.016 |
ADA : adalimumab, IFX: infliximab, UST: ustekinumab, VDZ: vedolizumab, BMI:Body Mass Index, CDAI:Crohn’s Disease Activity Index, Hb:hemoglobin, CRP:C-reactive protein.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



