
Submitted:
22 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Background: Atrial fibrillation (AF) is a prevalent arrhythmia closely associated with cardiometabolic disorders and systemic inflammation. Epicardial adipose tissue (EAT), located in direct contact with the atrial myocardium, has emerged as a biologically active tissue involved in atrial remodeling through inflammatory, fibrotic, and electrophysiological mechanisms. The objective of this review is to summarize current translational and clinical evidence on the role of EAT in AF pathophysiology and to discuss its implications for diagnostic assessment, interventional management, and cardiometabolic therapeutic strategies. Methods: A narrative review of experimental, translational, and clinical studies was conducted using major biomedical databases. The literature was evaluated with a focus on mechanisms linking EAT to atrial remodeling, noninvasive imaging techniques for EAT characterization, echocardiographic and electroanatomical markers of atrial disease, outcomes of catheter ablation strategies, and pharmacological interventions targeting metabolic and inflammatory pathways. Results:The available evidence indicates that increased EAT volume and altered inflammatory activity are associated with atrial fibrosis, conduction abnormalities, and impaired atrial function, contributing to AF initiation and persistence. Multimodality imaging, including cardiac computed tomography and cardiac magnetic resonance, enables quantitative and qualitative assessment of EAT and supports clinical phenotyping. Clinical studies report an association between higher EAT burden and increased AF recurrence after pulmonary vein isolation, particularly in patients with persistent AF. Emerging cardiometabolic therapies, such as glucagon-like peptide-1 receptor agonists and dual GIP/GLP-1 agonists, have been shown to reduce EAT volume and inflammatory markers, although direct evidence linking these interventions to improved AF outcomes remains limited. Conclusions: EAT represents a relevant pathophysiological interface between metabolic disease and AF with potential clinical implications. Incorporating EAT assessment into routine evaluation may enhance risk stratification and support personalized AF management. Further prospective studies are required to define its role as a therapeutic target in clinical practice.
Keywords:
epicardial adipose tissue
; atrial fibrillation
; echocardiography
; catheter ablation
; glp-1 receptor agonists
; gip/glp-1 dual agonists
1. Introduction
Epicardial adipose tissue (EAT) is a specialized visceral fat depot located between the myocardium and the visceral layer of the pericardium [1]. It is uniquely positioned in close proximity to the cardiac muscle and shares its microcirculation, which facilitates direct paracrine and vasocrine interactions with the underlying myocardium [2]. Under physiological conditions, EAT performs several beneficial functions, including mechanical protection of coronary arteries, thermoregulation, and secretion of anti-inflammatory adipokines [3]. However, in pathologic states such as obesity, insulin resistance, and systemic inflammation, EAT undergoes phenotypic changes characterized by hypertrophy, inflammatory cell infiltration, and a shift toward a pro-inflammatory and profibrotic secretome [4].
Mounting evidence implicates EAT in the development and progression of atrial fibrillation (AF) [5]. Through the release of cytokines (e.g., interleukin-6, TNF-α), chemokines, and extracellular matrix-modulating enzymes, EAT promotes structural remodeling of the atrial myocardium, including fibrosis and adipocyte infiltration [6]. These changes disrupt the normal atrial architecture and contribute to conduction heterogeneity, delayed atrial conduction, and increased susceptibility to arrhythmogenesis [7]. In this context, EAT functions not merely as a passive bystander but as an active contributor to the arrhythmic substrate.
Echocardiographic and advanced imaging studies have demonstrated that increased EAT volume correlates with impaired atrial function, reduced atrial strain, and prolonged atrial conduction time—all predictors of AF onset and recurrence [8]. Moreover, EAT burden appears to negatively influence the efficacy of rhythm control strategies such as catheter ablation [9].
Given the growing prevalence of obesity and AF, understanding the mechanistic role of EAT is essential for identifying novel therapeutic targets. This review aims to explore the pathophysiological mechanisms linking EAT to AF, the diagnostic and prognostic value of imaging-derived EAT metrics, and emerging therapeutic strategies—including catheter ablation approaches and novel metabolic agents such as GLP-1 and GIP receptor agonists—that may modulate EAT and improve AF outcomes [10].
2. Distribution, Physiological Role, and Contribution to Atrial Fibrosis of Epicardial Adipose Tissue
EAT is predominantly distributed along the atrioventricular and interventricular grooves, surrounding the coronary arteries, and enveloping both atria—particularly the posterior left atrial wall and the left atrial appendage [11]. This fat depot is unique in that it lies directly over the myocardium, with no separating fascia, and shares a common embryologic origin with visceral fat (Figure 1). Under normal conditions, EAT exerts cardioprotective functions, including mechanical cushioning of coronary vessels, fatty acid storage and supply to the myocardium, thermoregulation, and secretion of anti-inflammatory adipokines such as adiponectin [12].
However, in pathological states such as obesity, type 2 diabetes, and metabolic syndrome, EAT undergoes expansion and phenotypic transformation [13]. The resulting tissue exhibits increased infiltration of inflammatory cells (e.g., macrophages, T lymphocytes) and shifts its secretory profile toward pro-inflammatory cytokines (e.g., IL-6, TNF-α), profibrotic mediators (e.g., TGF-β), and matrix metalloproteinases [14]. These molecules diffuse locally to the adjacent atrial myocardium, where they promote oxidative stress, myocyte apoptosis, and fibroblast activation [15]. This paracrine signaling fosters interstitial fibrosis, alters atrial conduction velocity, and increases electrical heterogeneity, all of which contribute to the substrate for atrial fibrillation [16]. Notably, fibrotic remodeling tends to be most pronounced in regions with high EAT density, such as the posterior left atrial wall, which may explain the increased arrhythmogenicity of these areas and their relevance in ablation strategies [17].
3. Cardiac CT and MRI in the Assessment of Epicardial Adipose Tissue
Cardiac imaging modalities such as computed tomography (CT – Figure 2) and magnetic resonance imaging (MRI) provide detailed, reproducible quantification of EAT and play an increasingly important role in risk stratification and procedural planning in AF [18]. Non-contrast ECG-gated cardiac CT is considered the gold standard for EAT volume assessment due to its high spatial resolution and ability to distinguish fat based on its characteristic attenuation (typically –190 to –30 Hounsfield units) [19]. CT allows for precise quantification of EAT volume and distribution, particularly around the left atrium and pulmonary veins, where fat accumulation is most relevant to arrhythmogenesis [20]. In addition, periatrial EAT thickness measured on CT has been correlated with low-voltage zones and fibrotic remodeling seen on electroanatomical mapping [21].
Cardiac magnetic resonance imaging (CMR) offers complementary advantages, including superior tissue characterization without ionizing radiation [22]. While CMR-based fat quantification is less commonly used in clinical practice, advanced techniques such as Dixon sequences or fat–water separation imaging enable reliable estimation of EAT volume and characterization of adjacent myocardial tissue [23]. Importantly, CMR also permits late gadolinium enhancement (LGE) imaging to detect atrial fibrosis, which can be spatially correlated with epicardial fat distribution—highlighting the mechanistic link between EAT and atrial remodeling [24]. Moreover, combining EAT volume measurements with fibrosis burden on CMR may improve the prediction of AF recurrence after catheter ablation.
Both CT and CMR thus provide valuable anatomic and functional data that enhance the understanding of EAT’s role in AF and support a phenotype-driven approach to patient management.
4. Echocardiographic Assessment of Atrial Function in Patients with Increased Epicardial Adipose Tissue
In patients with abundant EAT, echocardiographic evaluation reveals distinct alterations in atrial mechanics that reflect early structural and electrical remodeling [25]. Speckle-tracking echocardiography (STE) has emerged as a sensitive modality for assessing atrial function through myocardial deformation parameters, particularly atrial strain (Figure 3). Left atrial strain is typically evaluated during three phases: reservoir (LASr), conduit (LAScd), and contraction (LASct). In individuals with increased EAT, a consistent reduction in LASr and LAScd is observed, indicating impaired atrial compliance and passive emptying due to atrial stiffness and interstitial fibrosis [26]. The contractile strain (LASct) may also be reduced, particularly in advanced remodeling, reflecting impaired booster pump function.
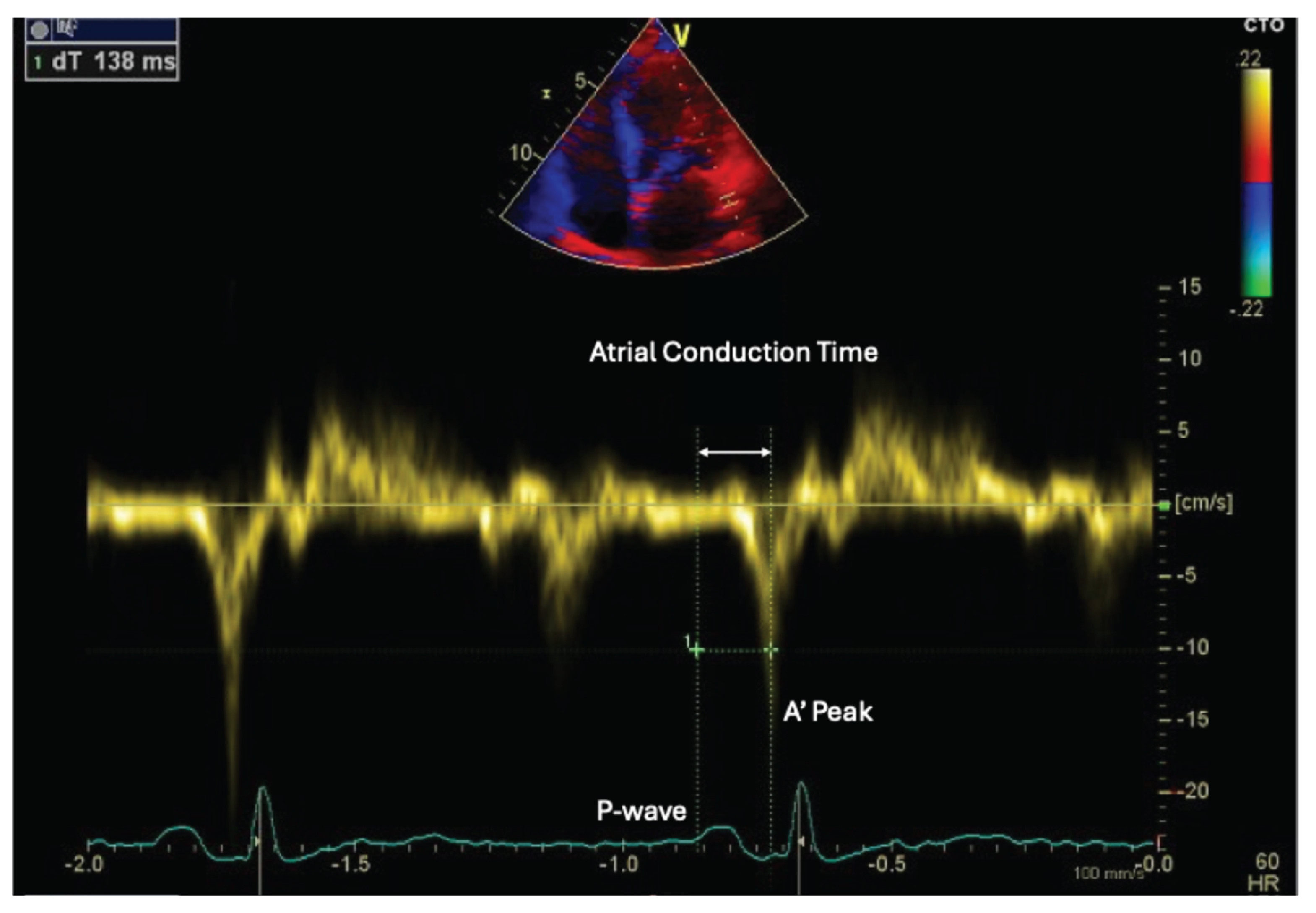
In addition to strain parameters, atrial electromechanical delay—typically assessed by tissue Doppler imaging (TDI) as the time interval from the onset of the P wave on ECG to the peak A’ velocity at the lateral mitral annulus (PA-TDI)—is often prolonged in patients with high EAT volume (Figure 4) [27]. This reflects slowed atrial conduction and is associated with heterogeneous and anisotropic propagation of electrical impulses due to fibrosis and fatty infiltration [28].
Furthermore, indices of atrial dyssynchrony, such as intra-atrial and inter-atrial electromechanical delay (measured as time differences in PA-TDI between septal and lateral or left and right atrial sites), are frequently abnormal in this population. Atrial mechanical dyssynchrony is thought to result from regional variability in fibrotic remodeling and inflammatory infiltration, particularly in regions where EAT is most abundant, such as the posterior and inferior left atrial walls.
Collectively, these echocardiographic findings support the concept that EAT is not merely an inert fat depot but an active driver of atrial dysfunction. The alterations in strain, conduction time, and mechanical synchrony observed in EAT-rich patients provide valuable insights into early atrial cardiomyopathy and may help refine risk stratification and timing of intervention in atrial fibrillation management [29].
5. Electroanatomical Mapping of the Left Atrium
In patients with paroxysmal atrial fibrillation (PAF) and increased EAT, electroanatomical mapping (EAM) of the left atrium frequently reveals early yet distinct structural and electrical alterations that suggest an arrhythmogenic substrate beyond pulmonary vein (PV) triggers [30]. High-resolution voltage mapping performed during sinus rhythm typically shows areas of low-voltage (<0.5 mV) or fractionated electrograms in the posterior, inferior, and lateral walls of the LA—regions commonly adjacent to epicardial fat depots. While PAF is classically associated with preserved global atrial voltage, in patients with increased EAT, a patchy low-voltage substrate may be evident even in the absence of persistent AF or overt structural heart disease [31].
These low-voltage zones (LVZs) are thought to reflect localized fibrosis, adipocyte infiltration, and interstitial inflammation driven by paracrine effects of EAT [32]. Fractionated or prolonged electrograms in these areas are indicative of conduction slowing and heterogeneity, promoting reentrant circuit formation. Studies have demonstrated a spatial correlation between high EAT thickness on imaging (e.g., CT or MRI) and low-voltage areas on mapping, supporting the hypothesis that EAT contributes directly to arrhythmogenic remodeling [33].
Activation mapping may further reveal areas of delayed or fragmented conduction, often in the posterior wall, where epicardial fat accumulation is most pronounced [34]. The presence of such conduction abnormalities despite a paroxysmal AF phenotype suggests an early stage of atrial cardiomyopathy, sometimes referred to as “fibro-fatty atrial myopathy.” In this context, tailored ablation strategies beyond pulmonary vein isolation (PVI)—such as posterior wall isolation or ablation of low-voltage areas—may be beneficial, although data are still evolving [35].
Importantly, the identification of EAT-related atrial remodeling during EAM may inform procedural planning and prognosis, as patients with more extensive EAT and associated electrical abnormalities may have a higher risk of AF recurrence post-ablation, even in the paroxysmal stage.
6. Posterior Wall Electroanatomical Ablation vs Cryoballoon PVI
In patients with PAF and high EAT burden, the posterior wall of the left atrium emerges as a key arrhythmogenic substrate [36]. This region, heavily influenced by adjacent EAT, demonstrates early structural remodeling, including fibro-fatty infiltration, localized inflammation, and conduction delay [37]. While pulmonary vein isolation (PVI) remains the foundation of catheter ablation, emerging evidence suggests that PVI alone—especially when performed using cryoballoon technology—may be insufficient in this specific phenotype, as it fails to address non-pulmonary vein triggers and diseased atrial myocardium located within the posterior wall [38].
Point-by-point radiofrequency (RF) ablation enables detailed electroanatomical mapping and precise lesion delivery, allowing not only for PVI but also for posterior wall isolation (PWI) through linear ablation (e.g., roof and inferior lines) and substrate modification targeting low-voltage and fractionated regions [39]. In contrast, cryoballoon PVI, although effective in standard PAF, offers limited substrate adaptability and does not routinely achieve posterior wall isolation [40].
Clinical data support the superiority of posterior wall modification in selected patients. In the POBI-AF trial, adjunctive posterior wall isolation in addition to PVI resulted in significantly lower arrhythmia recurrence compared to PVI alone, particularly in patients with evidence of posterior wall low-voltage areas [41]. Similarly, observational studies have demonstrated that EAT volume correlates with the extent of posterior low-voltage substrate, and that patients with greater EAT burden benefit most from tailored ablation strategies that include the posterior wall [42]. In contrast, the CAPLA trial, which compared PVI alone to PVI plus posterior wall isolation in unselected patients, did not find a significant difference—highlighting the need for phenotypic stratification, such as EAT quantification, when selecting patients who may benefit from substrate-guided approaches [43].
Therefore, in patients with paroxysmal AF and high posterior EAT burden—whether identified by cardiac imaging (e.g., CT or MRI) or inferred from electroanatomical voltage mapping—electroanatomical ablation of the posterior wall via RF may provide superior rhythm outcomes compared to cryoballoon PVI alone. This supports a personalized, substrate-directed approach to ablation in metabolically remodeled atria.
7. Therapeutic Implications of GLP-1 Receptor Agonists and Dual GIP/GLP-1 Agonists
The recognition of EAT as an active contributor to atrial remodeling and arrhythmogenesis has prompted interest in pharmacological strategies targeting adipose tissue reduction to mitigate AF risk [44]. Among these, glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and dual glucose-dependent insulinotropic polypeptide/glucagon-like peptide-1 receptor agonists (GIP/GLP-1 RAs) have emerged as promising agents that extend beyond glycemic control to influence adipose tissue metabolism, inflammation, and fibrosis [45].
GLP-1 RAs, such as liraglutide and semaglutide, have demonstrated efficacy in reducing visceral and epicardial fat volumes, likely through mechanisms including appetite suppression, weight loss, increased energy expenditure, and improved insulin sensitivity [46]. These agents may exert anti-inflammatory and anti-fibrotic effects within the myocardium and surrounding adipose depots, potentially stabilizing the arrhythmogenic substrate [47].
Dual GIP/GLP-1 RAs, such as tirzepatide, have shown superior efficacy in weight reduction and visceral fat loss compared to GLP-1 RAs alone [48]. While GIP has traditionally been associated with anabolic effects on adipose tissue, recent studies suggest that GIP can exert lipolytic effects under certain conditions. Specifically, GIP receptor activation has been linked to increased lipolysis in human subcutaneous adipose tissue, as evidenced by elevated glycerol release, indicating enhanced breakdown of triglycerides [49]. Furthermore, GIP receptor expression is higher in visceral adipose tissue compared to subcutaneous fat, suggesting a more pronounced effect of GIP on visceral fat depots [50].
The combined activation of GLP-1 and GIP receptors may therefore synergistically promote the reduction of EAT and visceral fat, potentially ameliorating the pro-arrhythmic substrate associated with AF. Although direct evidence linking these pharmacotherapies to reduced AF incidence is still emerging, the observed reductions in EAT volume and improvements in metabolic profiles support their potential role as adjunctive therapies in AF management, particularly in obese or metabolically compromised individuals.
8. Conclusions
EAT is now recognized as an active pathophysiological contributor to AF, particularly in individuals with obesity and metabolic dysfunction. Through local paracrine effects, EAT promotes atrial fibrosis, electrical conduction abnormalities, and atrial mechanical dysfunction—creating a vulnerable substrate for AF initiation and maintenance. Echocardiographic assessment of atrial strain, conduction time, and dyssynchrony, alongside electroanatomical mapping, can reveal early signs of atrial remodeling in patients with significant EAT burden.
The presence of EAT has important implications for the choice and effectiveness of ablation strategies. While pulmonary vein isolation remains the procedural foundation, adjunctive posterior wall ablation using radiofrequency energy appears superior to cryoballoon-based approaches in patients with posterior atrial remodeling linked to epicardial fat infiltration.
Pharmacologic strategies targeting EAT are emerging as valuable adjuncts in rhythm control. GLP-1 receptor agonists and dual GIP/GLP-1 receptor agonists have demonstrated the ability to reduce visceral and epicardial fat, improve inflammatory and metabolic profiles, and may indirectly reduce AF susceptibility. Notably, GIP agonism—historically considered anabolic—may exhibit lipolytic effects in visceral depots, further enhancing the therapeutic value of dual agonist therapy.
Integrating EAT assessment into the clinical management of AF can enable more personalized and mechanism-based interventions, combining imaging, electrophysiology, and metabolic modulation to improve outcomes in this increasingly prevalent patient population. Future clinical trials should validate the benefits of integrating EAT assessment and targeted interventions into comprehensive AF management strategies, particularly among obese and metabolically compromised populations.
Funding
This research received no external funding.
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| EAM EAT GLP-1 GIP LAA LGE PA-TDI PVI PWI VAT |
Electroanatomical mapping Epicardial adipose tissue Glucagon-like peptide-1 Glucose-dependent insulinotropic polypeptide Left atrial appendage Late gadolinium enhancement P-wave to A’-wave tissue Doppler imaging interval Pulmonary vein isolation Posterior wall isolation Visceral adipose tissue |
References
- Raggi, P; Stillman, AE. Clinical Role of Epicardial Adipose Tissue. Can J Cardiol 2025, 41(9), 1753–1763. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G. Epicardial adipose tissue in contemporary cardiology. Nat Rev Cardiol 2022, 19(9), 593–606. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Şengül, C; Özveren, O. Epicardial adipose tissue: a review of physiology, pathophysiology, and clinical applications. Anadolu Kardiyol Derg 2013, 13(3), 261–5. [Google Scholar] [CrossRef] [PubMed]
- Bodenstab, ML; Varghese, RT; Iacobellis, G. Cardio-Lipotoxicity of Epicardial Adipose Tissue. Biomolecules 2024, 14(11), 1465. [Google Scholar] [CrossRef] [PubMed Central]
- Cacciapuoti, F; Caso, I; Crispo, S; Verde, N; Capone, V; Gottilla, R; Materazzi, C; Volpicelli, M; Ziviello, F; Mauro, C; et al. Linking Epicardial Adipose Tissue to Atrial Remodeling: Clinical Implications of Strain Imaging. Hearts 2025, 6(1), 3. [Google Scholar] [CrossRef]
- Packer, M. Epicardial Adipose Tissue May Mediate Deleterious Effects of Obesity and Inflammation on the Myocardium. J Am Coll Cardiol. 2018, 71(20), 2360–2372. [Google Scholar] [CrossRef] [PubMed]
- Conte, M; Petraglia, L; Cabaro, S; Valerio, V; Poggio, P; Pilato, E; Attena, E; Russo, V; Ferro, A; Formisano, P; Leosco, D; Parisi, V. Epicardial Adipose Tissue and Cardiac Arrhythmias: Focus on Atrial Fibrillation. Front Cardiovasc Med. 2022, 9, 932262. [Google Scholar] [CrossRef] [PubMed Central]
- Ma, M; Zheng, X; Wu, X; Xie, Q. Epicardial adipose tissue thickness on transthoracic echocardiography predicts 2-year incident atrial fibrillation in elderly hypertensive patients. Front Cardiovasc Med 2025, 12, 1650423. [Google Scholar] [CrossRef] [PubMed Central]
- Nakahara, S; Hori, Y; Kobayashi, S; Sakai, Y; Taguchi, I; Takayanagi, K; Nagashima, K; Sonoda, K; Kogawa, R; Sasaki, N; Watanabe, I; Okumura, Y. Epicardial adipose tissue-based defragmentation approach to persistent atrial fibrillation: its impact on complex fractionated electrograms and ablation outcome. Heart Rhythm 2014, 11(8), 1343–51. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G. Epicardial Fat Inflammation and GLP-1/GIP Receptor Analogs: Are we Shifting our Perspective? Curr Cardiol Rep. 2025, 27(1), 161. [Google Scholar] [CrossRef] [PubMed]
- Hasebe, H; Yoshida, K; Nogami, A; Ieda, M. Difference in epicardial adipose tissue distribution between paroxysmal atrial fibrillation and coronary artery disease. Heart Vessels 2020, 35(8), 1070–1078. [Google Scholar] [CrossRef] [PubMed]
- Neeland, IJ; Zhu, F; Graca, G; Lymperopoulos, A; Iacobellis, G; Farzaneh, A; Bos, D; Ghanbari, M; Goldberger, JJ; Kavousi, M; Greenland, P. Metabolomics Profiling of Epicardial Adipose Tissue: MESA and the Rotterdam Study. J Am Heart Assoc. 2025, 14(13), e039750. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cacciapuoti, F; Liguori, C; Nasti, R; Capone, V; Cacciapuoti, F. Unlocking the Mysteries of Epicardial Adipose Tissue: Implications of Cardiometabolic Syndrome. Research in Cardiovascular Medicine 2024, 13(2), 23–28. [Google Scholar] [CrossRef]
- Vyas, V; Sandhar, B; Keane, JM; Wood, EG; Blythe, H; Jones, A; Shahaj, E; Fanti, S; Williams, J; Metic, N; Efremova, M; Ng, HL; Nageswaran, G; Byrne, S; Feldhahn, N; Marelli-Berg, F; Chain, B; Tinker, A; Finlay, MC; Longhi, MP. Tissue-resident memory T cells in epicardial adipose tissue comprise transcriptionally distinct subsets that are modulated in atrial fibrillation. Nat Cardiovasc Res. 2024, 3(9), 1067–1082. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Carena, MC; Badi, I; Polkinghorne, M; Akoumianakis, I; Psarros, C; Wahome, E; Kotanidis, CP; Akawi, N; Antonopoulos, AS; Chauhan, J; Sayeed, R; Krasopoulos, G; Srivastava, V; Farid, S; Walcot, N; Douglas, G; Channon, KM; Casadei, B; Antoniades, C. Role of Human Epicardial Adipose Tissue-Derived miR-92a-3p in Myocardial Redox State. J Am Coll Cardiol. 2023, 82(4), 317–332. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sha, R; Baines, O; Hayes, A; Tompkins, K; Kalla, M; Holmes, AP; O'Shea, C; Pavlovic, D. Impact of Obesity on Atrial Fibrillation Pathogenesis and Treatment Options. J Am Heart Assoc. 2024, 13(1), e032277. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nakatani, Y; Sakamoto, T; Yamaguchi, Y; Tsujino, Y; Kinugawa, K. Epicardial adipose tissue affects the efficacy of left atrial posterior wall isolation for persistent atrial fibrillation. J Arrhythm. 2020, 36(4), 652–659. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huber, AT; Fankhauser, S; Wittmer, S; Chollet, L; Lam, A; Maurhofer, J; Madaffari, A; Seiler, J; Servatius, H; Haeberlin, A; Noti, F; Brugger, N; von Tengg-Kobligk, H; Gräni, C; Roten, L; Tanner, H; Reichlin, T. Epicardial adipose tissue dispersion at CT and recurrent atrial fibrillation after pulmonary vein isolation. Eur Radiol 2024, 34(8), 4928–4938. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trimarchi, G; Carerj, ML; Zito, C; Bella, GD; Taverna, G; Cusmà Piccione, M; Crea, P; Lo Giudice, S; Buonpane, A; Bonanni, M; Restelli, D; Paradossi, U; Monteleone, A; Micari, A; Carerj, S. Epicardial Adipose Tissue: A Multimodal Imaging Diagnostic Perspective. Medicina (Kaunas) 2025, 61(6), 961. [Google Scholar] [CrossRef] [PubMed Central]
- West, HW; Siddique, M; Williams, MC; Volpe, L; Desai, R; Lyasheva, M; Thomas, S; Dangas, K; Kotanidis, CP; Tomlins, P; Mahon, C; Kardos, A; Adlam, D; Graby, J; Rodrigues, JCL; Shirodaria, C; Deanfield, J; Mehta, NN; Neubauer, S; Channon, KM; Desai, MY; Nicol, ED; Newby, DE; Antoniades, C; ORFAN Investigators. Deep-Learning for Epicardial Adipose Tissue Assessment With Computed Tomography: Implications for Cardiovascular Risk Prediction. JACC Cardiovasc Imaging 2023, 16(6), 800–816. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Umar, A; Hocking, J; Massin, SZ; Suszko, A; Wintersperger, BJ; Chauhan, VS. Association of Cardiac CT-Derived Epicardial Adipose Tissue With Atrial Fibrillation in Patients Without Left Atrial Fibrosis as Defined by Endocardial Voltage Mapping. J Cardiovasc Electrophysiol. 2025, 36(2), 489–500. [Google Scholar] [CrossRef] [PubMed]
- Duca, F; Mascherbauer, K; Donà, C; Koschutnik, M; Binder, C; Nitsche, C; Halavina, K; Beitzke, D; Loewe, C; Bartko, P; Waldmann, E; Mascherbauer, J; Hengstenberg, C; Kammerlander, A. Association of epicardial adipose tissue on magnetic resonance imaging with cardiovascular outcomes: Quality over quantity? Obesity (Silver Spring). 2024, 32(9), 1670–1679. [Google Scholar] [CrossRef] [PubMed]
- Firouznia, M; Ylipää, E; Henningsson, M; Carlhäll, CJ. Poincare guided geometric UNet for left atrial epicardial adipose tissue segmentation in Dixon MRI images. Sci Rep. 2025, 15(1), 25549. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Skoda, I; Henningsson, M; Stenberg, S; Sundin, J; Carlhäll, CJ. Simultaneous Assessment of Left Atrial Fibrosis and Epicardial Adipose Tissue Using 3D Late Gadolinium Enhanced Dixon MRI. J Magn Reson Imaging 2022, 56(5), 1393–1403. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eroğlu, S. How do we measure epicardial adipose tissue thickness by transthoracic echocardiography? Anatol J Cardiol 2015, 15(5), 416–9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nabati, M; Moradgholi, F; Moosazadeh, M; Parsaee, H. The correlation between epicardial fat thickness and longitudinal left atrial reservoir strain in patients with type 2 diabetes mellitus and controls. Ultrasound J 2023, 15(1), 37. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Müller, P; Weijs, B; Bemelmans, NMAA; Mügge, A; Eckardt, L; Crijns, HJGM; Bax, JJ; Linz, D; den Uijl, DW. Echocardiography-derived total atrial conduction time (PA-TDI duration): risk stratification and guidance in atrial fibrillation management. Clin Res Cardiol. 2021, 110(11), 1734–1742. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Karsum, EH; Andersen, DM; Modin, D; Biering-Sørensen, SR; Mogelvang, R; Jensen, G; Schnohr, P; Gislason, G; Biering-Sørensen, T. The prognostic value of left atrial dyssynchrony measured by speckle tracking echocardiography in the general population. Int J Cardiovasc Imaging 2021, 37(5), 1679–1688. [Google Scholar] [CrossRef] [PubMed]
- Cacciapuoti, F; Caso, I; Gottilla, R; Minicucci, F; Volpicelli, M; Caso, P. Left Atrial Mechanics and Remodeling in Paroxysmal Atrial Fibrillation: Introducing the EASE Score for Pre-Ablation Risk Prediction. Med Sci (Basel) 2025, 13(3), 131. [Google Scholar] [CrossRef] [PubMed Central]
- Zghaib, T; Ipek, EG; Zahid, S; Balouch, MA; Misra, S; Ashikaga, H; Berger, RD; Marine, JE; Spragg, DD; Zimmerman, SL; Zipunnikov, V; Trayanova, N; Calkins, H; Nazarian, S. Association of left atrial epicardial adipose tissue with electrogram bipolar voltage and fractionation: Electrophysiologic substrates for atrial fibrillation. Heart Rhythm 2016, 13(12), 2333–2339. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shao, Y; Chen, L; Chen, W; Sang, C; Xu, C; Zhang, C. Left atrial epicardial adipose tissue is associated with low voltage zones in the left atrium in patients with non-valvular atrial fibrillation. Front Cardiovasc Med. 2022, 9, 924646. [Google Scholar] [CrossRef] [PubMed Central]
- Tonko, JB; Silberbauer, J; Lambiase, PD. Peak frequency analysis for epicardial contact mapping: How (in)frequent is epicardial adipose tissue? Heart Rhythm 2024, 21(10), 1898–1899. [Google Scholar] [CrossRef] [PubMed]
- Firouznia, M; Molnar, D; Edin, C; Hjelmgren, O; Östgren, CJ; Lundberg, P; Henningsson, M; Bergström, G; Carlhäll, CJ. Head-to-Head Comparison between MRI and CT in the Evaluation of Volume and Quality of Epicardial Adipose Tissue. Radiol Cardiothorac Imaging 2025, 7(4), e240531. [Google Scholar] [CrossRef] [PubMed]
- Qiu, B; Li, F; Sang, C; Shen, J; Shao, Y; Chen, W; Hu, X; Li, C; Hu, C; Zhang, C; Wang, Z; Chen, M. Combination of Epicardial Adipose Tissue and Left Atrial Low-Voltage Areas Predicting Atrial Fibrillation Recurrence after Radiofrequency Ablation. Cardiology 2025, 150(1), 48–55. [Google Scholar] [CrossRef] [PubMed]
- Cacciapuoti, F; Gottilla, R; Caso, I; Crispo, S; Pirozzi, C; Minicucci, F; Volpicelli, M. One size does not fit all: Echocardiography as a decision-making tool in atrial fibrillation management – A case series. J Cardiovasc Echography 2025, 35, 403–9. [Google Scholar]
- Sperling, JS; Delurgio, DL; Svinarich, JT. Posterior left atrial epicardial adipose tissue: scope of the problem and impact of new technology. Curr Opin Cardiol 2022, 37(1), 54–61. [Google Scholar] [CrossRef] [PubMed]
- van Rosendael, AR; Dimitriu-Leen, AC; van Rosendael, PJ; Leung, M; Smit, JM; Saraste, A; Knuuti, J; van der Geest, RJ; van der Arend, BW; van Zwet, EW; Scholte, AJ; Delgado, V; Bax, JJ. Association Between Posterior Left Atrial Adipose Tissue Mass and Atrial Fibrillation. Circ Arrhythm Electrophysiol 2017, 10(2), e004614. [Google Scholar] [CrossRef] [PubMed]
- Momot, K; Pruc, M; Rodkiewicz, D; Koźluk, E; Krauz, K; Piątkowska, A; Zalewska, Z; Buksińska-Lisik, M; Szarpak, L; Mamcarz, A. Predictive Value of Epicardial Adipose Tissue Parameters Measured by Cardiac Computed Tomography for Recurrence of Atrial Fibrillation After Pulmonary Vein Isolation. J Clin Med. 2025, 14(19), 6963. [Google Scholar] [CrossRef] [PubMed Central]
- Liang, JJ; Elafros, MA; Muser, D; Pathak, RK; Santangeli, P; Supple, GE; Schaller, RD; Frankel, DS; Dixit, S. Comparison of Left Atrial Bipolar Voltage and Scar Using Multielectrode Fast Automated Mapping versus Point-by-Point Contact Electroanatomic Mapping in Patients With Atrial Fibrillation Undergoing Repeat Ablation. J Cardiovasc Electrophysiol. 2017, 28(3), 280–288. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, M; Jabeen, S; Danial, A; Chaychi, MTM; Zaheer, MK; Mumtaz, A; Mumtaz, T; Herweg, B. Adjunct posterior wall isolation reduces the recurrence of atrial fibrillation in patients undergoing cryoballoon ablation: A systematic review and meta-analysis. J Cardiovasc Electrophysiol. 2023, 34(10), 2043–2052. [Google Scholar] [CrossRef] [PubMed]
- Lee JM, Shim J, Park J, Yu HT, Kim TH, Park JK, Uhm JS, Kim JB, Joung B, Lee MH, Kim YH, Pak HN; POBI-AF Investigators. The Electrical Isolation of the Left Atrial Posterior Wall in Catheter Ablation of Persistent Atrial Fibrillation. JACC Clin Electrophysiol Erratum in: JACC Clin Electrophysiol. 2023 Jan;9(1):145. doi: 10.1016/j.jacep.2022.12.001. PMID: 31753429. 2019, 5(11), 1253–1261. [Google Scholar] [CrossRef]
- Anagnostopoulos, I; Kousta, M; Kossyvakis, C; Paraskevaidis, NT; Vrachatis, D; Deftereos, S; Giannopoulos, G. Epicardial Adipose Tissue and Atrial Fibrillation Recurrence following Catheter Ablation: A Systematic Review and Meta-Analysis. J Clin Med. 2023, 12(19), 6369. [Google Scholar] [CrossRef] [PubMed Central]
- Kistler, PM; Chieng, D; Sugumar, H; Ling, LH; Segan, L; Azzopardi, S; Al-Kaisey, A; Parameswaran, R; Anderson, RD; Hawson, J; Prabhu, S; Voskoboinik, A; Wong, G; Morton, JB; Pathik, B; McLellan, AJ; Lee, G; Wong, M; Finch, S; Pathak, RK; Raja, DC; Sterns, L; Ginks, M; Reid, CM; Sanders, P; Kalman, JM. Effect of Catheter Ablation Using Pulmonary Vein Isolation With vs Without Posterior Left Atrial Wall Isolation on Atrial Arrhythmia Recurrence in Patients With Persistent Atrial Fibrillation: The CAPLA Randomized Clinical Trial. JAMA 2023, 329(2), 127–135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ding, Y; Lin, F; Liu, Z; Zhou, X; Liang, X. Targeting Epicardial/Pericardial Adipose Tissue in Cardiovascular Diseases: A Novel Therapeutic Strategy. Rev Cardiovasc Med. 2025, 26(3), 26128. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wiszniewski, K; Grudniewska, A; Szabłowska-Gadomska, I; Pilichowska-Paszkiet, E; Zaborska, B; Zgliczyński, W; Dudek, P; Bik, W; Sota, M; Mrozikiewicz-Rakowska, B. Epicardial Adipose Tissue-A Novel Therapeutic Target in Obesity Cardiomyopathy. Int J Mol Sci 2025, 26(16), 7963. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Myasoedova, VA; Parisi, V; Moschetta, D; Valerio, V; Conte, M; Massaiu, I; Bozzi, M; Celeste, F; Leosco, D; Iaccarino, G; Genovese, S; Poggio, P. Efficacy of cardiometabolic drugs in reduction of epicardial adipose tissue: a systematic review and meta-analysis. Cardiovasc Diabetol 2023, 22(1), 23. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yaribeygi, H; Maleki, M; Nasimi, F; Jamialahmadi, T; Stanford, FC; Sahebkar, A. Benefits of GLP-1 Mimetics on Epicardial Adiposity. Curr Med Chem. 2023, 30(37), 4256–4265. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aronne, LJ; Horn, DB; le Roux, CW; Ho, W; Falcon, BL; Gomez Valderas, E; Das, S; Lee, CJ; Glass, LC; Senyucel, C; Dunn, JP. SURMOUNT-5 Trial Investigators. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity. N Engl J Med. 2025, 393(1), 26–36. [Google Scholar] [CrossRef] [PubMed]
- Brachs, S; Soll, D; Beer, F; Huckauf, N; Konkar, A; Spranger, J; Rütten, H; Mai, K. Hormonal regulation of human adipose tissue lipolysis: impact of adipose GIP system in overweight and obesity. Eur J Endocrinol 2025, 192(2), 91–99. [Google Scholar] [CrossRef] [PubMed]
- Rosenkilde, MM; George, JT; Véniant, MM; Holst, JJ. GIP Receptor Antagonists in the Pharmacotherapy of Obesity: Physiologic, Genetic, and Clinical Rationale. Diabetes 2025, 74(8), 1334–1338. [Google Scholar] [CrossRef]
Figure 1.
Transthoracic echocardiography showing epicardial adipose tissue. Parasternal short-axis view shows an echolucent layer consistent with epicardial adipose tissue (arrow).
Figure 1.
Transthoracic echocardiography showing epicardial adipose tissue. Parasternal short-axis view shows an echolucent layer consistent with epicardial adipose tissue (arrow).
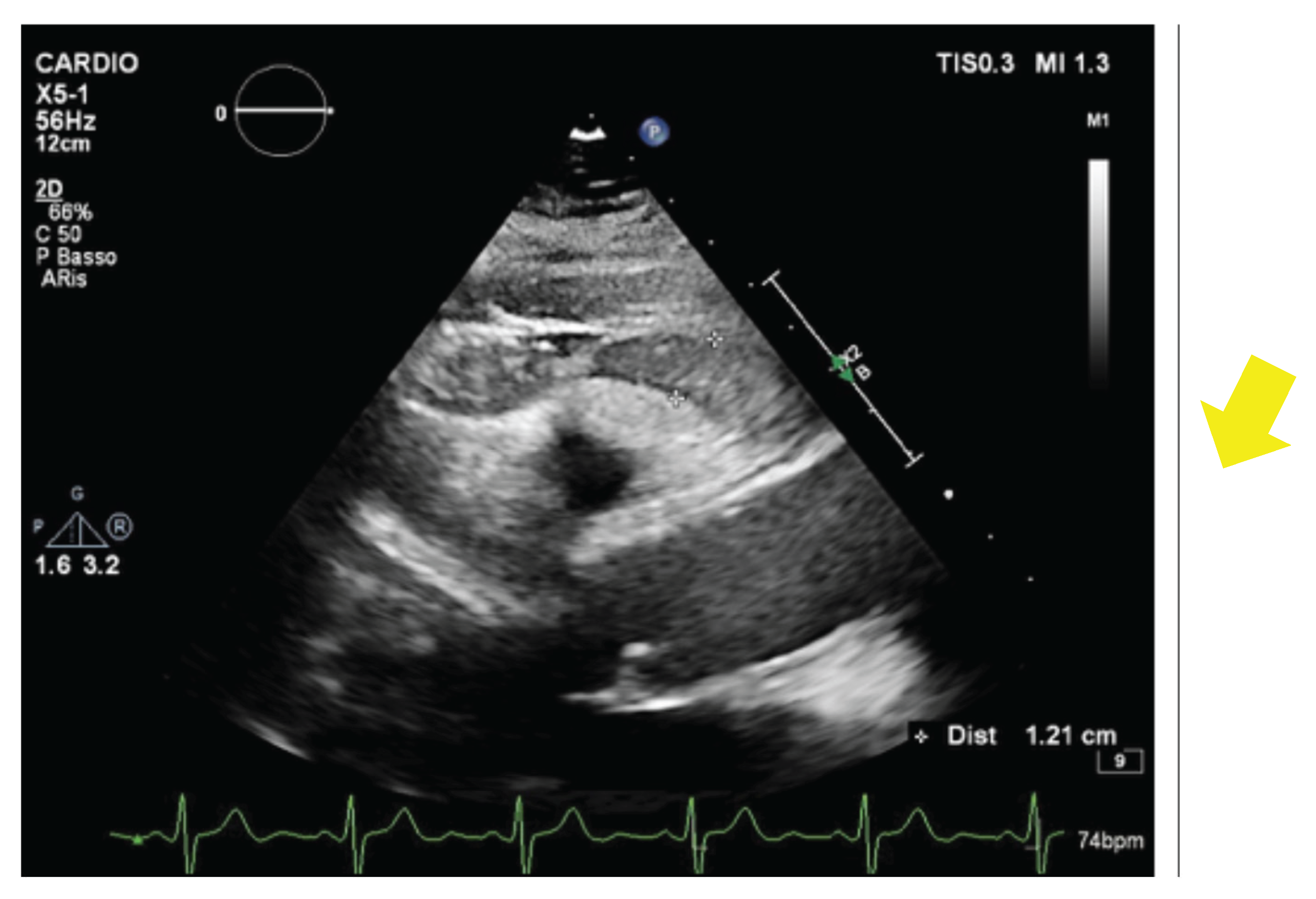
Figure 2.
Cardiac computed tomography illustrating periatrial epicardial adipose tissue (arrow).
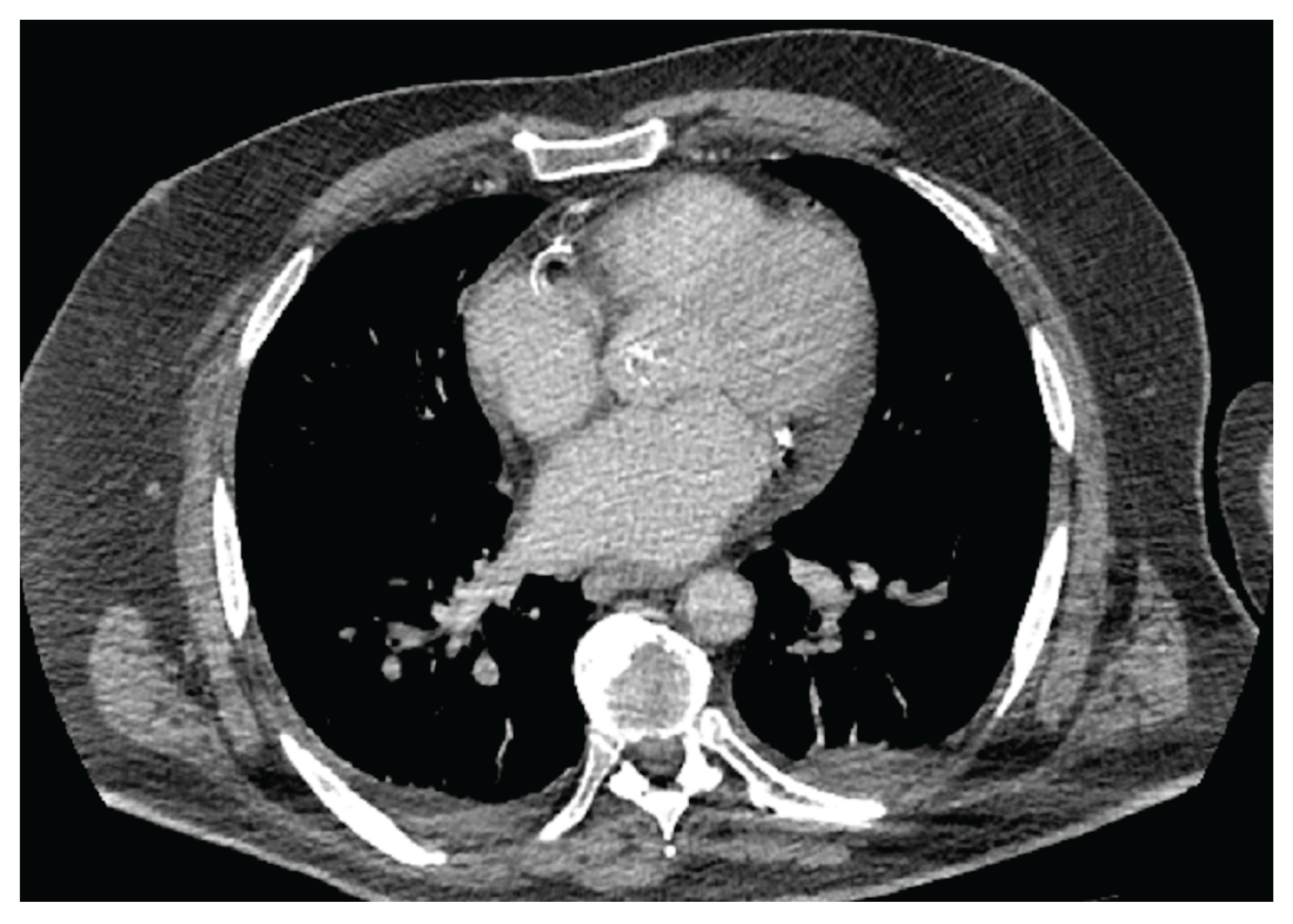
Figure 3.
Speckle-tracking echocardiography illustrating left atrial functional impairment in the presence of increased epicardial adipose tissue. Reduced left atrial reservoir strain and segmental dyssynchrony reflect early atrial mechanical remodeling associated with epicardial fat accumulation.
Figure 3.
Speckle-tracking echocardiography illustrating left atrial functional impairment in the presence of increased epicardial adipose tissue. Reduced left atrial reservoir strain and segmental dyssynchrony reflect early atrial mechanical remodeling associated with epicardial fat accumulation.
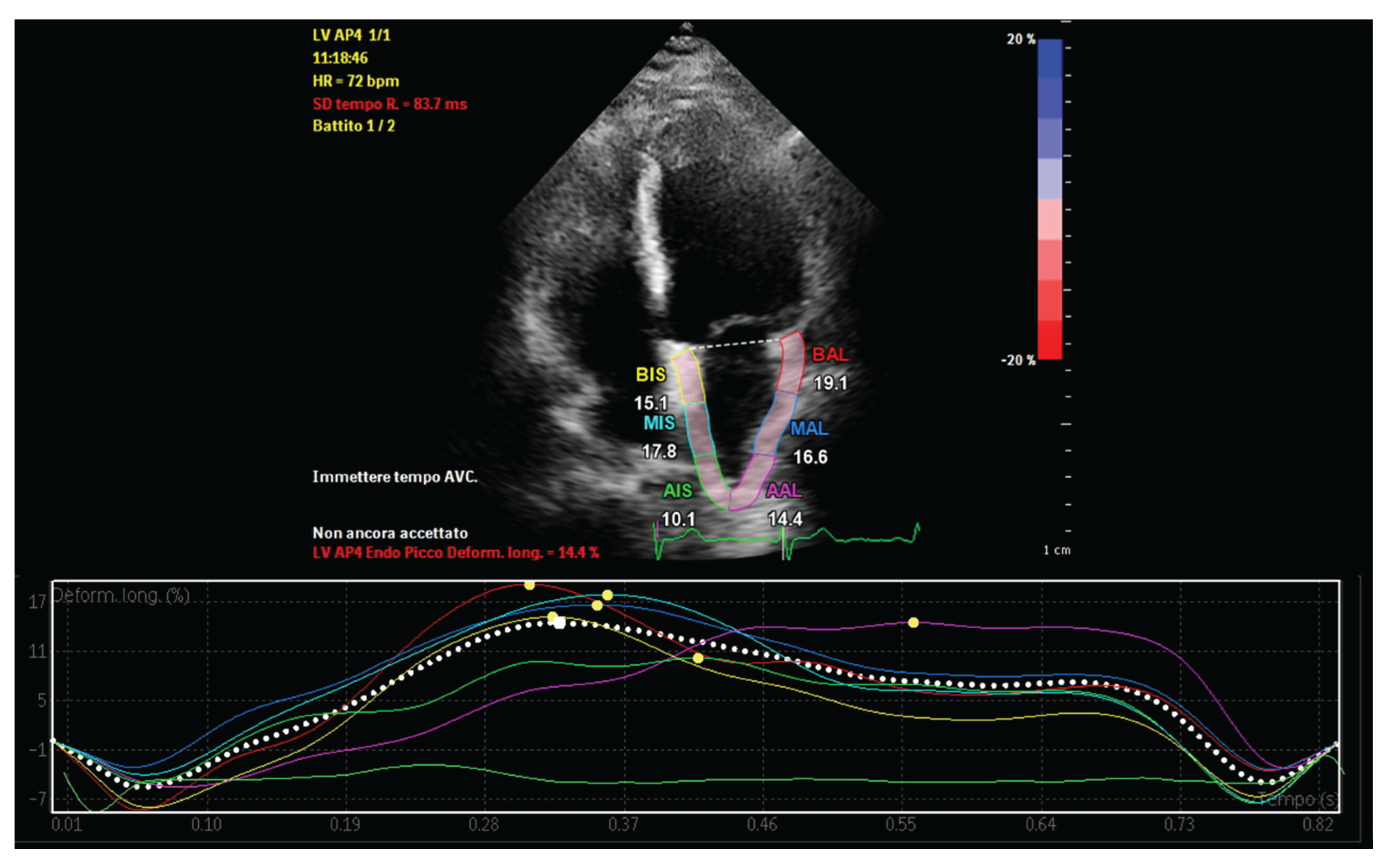
Figure 4.
Tissue Doppler imaging assessment of atrial conduction time in a patient with increased epicardial adipose tissue. Atrial conduction time (PA-TDI) is measured from the onset of the P wave on the electrocardiogram to the peak A′ velocity at the lateral mitral annulus, reflecting delayed atrial electrical activation associated with atrial remodeling.
Figure 4.
Tissue Doppler imaging assessment of atrial conduction time in a patient with increased epicardial adipose tissue. Atrial conduction time (PA-TDI) is measured from the onset of the P wave on the electrocardiogram to the peak A′ velocity at the lateral mitral annulus, reflecting delayed atrial electrical activation associated with atrial remodeling.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



