
Submitted:
21 January 2026
Posted:
22 January 2026
You are already at the latest version
Abstract
Background/Objectives: This study compared the hemodynamic performance of fenestrated (FEVAR), branched (BEVAR) and chimney endovascular aortic aneurysm repair (chEVAR) in patients with complex aortic aneurysms. Methods: The pre- (native) and post-endovascular repair (endograft-defined) blood lumen was reconstructed from computed tomography angiographies of nine (9) elective patients treated with FEVAR (n=3), BEVAR (n=3), and chEVAR (n=3). Computational Fluid Dynamics (CFD) simulations obtained blood flow properties. Velocity magnitude, wall shear stress (WSS), time-averaged wall shear stress (TAWSS), oscillatory shear index (OSI), relative residence time (RRT) and local normalized helicity (LNH) were computed at peak-systole and mid-diastole. The hemodynamic data were statistically analyzed to evaluate correlations between FEVAR, BEVAR and chEVAR, focusing on targeted visceral arteries. Results: Only slight differences were observed regarding RRT, OSI and TAWSS between FEVAR and BEVAR, whereas the chEVAR group demonstrated a marked deviation from both. In FEVAR, the postoperative helical flow structures appeared more compact, while in BEVAR, they were more developed and exhibited a more rotational configuration. The LNH of the visceral vessel patterns exhibited similar qualitative features across groups. Regarding TAWSS, higher values were found in BEVAR, whereas chEVAR showed the lowest. Conclusions: FEVAR, BEVAR, and chEVAR improved postoperative blood flow characteristics toward near-physiological conditions, reducing undesired flow patterns and recirculation zones. FEVAR showed more stable visceral flow, BEVAR demonstrated higher flow rates and fewer recirculation zones while chEVAR exhibited more streamlined visceral artery flow with reduced regurgitation at bridging stent entries. Despite variations, all approaches effectively preserved visceral artery perfusion.
Keywords:
FEVAR
; BEVAR
; ChEVAR
; computational fluid dynamics
; hemodynamic performance
; endograft-specific flow analysis
1. Introduction
Endovascular repair using fenestrated and branched endografts is the first line treatment for patients with juxtarenal and pararenal abdominal aortic aneurysms (AAAs) [1,2] while off-the-shelf solutions may may be used in urgent setting or when the anatomy does not permit a custom-made endograft application [3]. Endovascular treatment for complex aneurysms has emerged as a preferred approach in contemporary medical practice. The advancements in endovascular solutions, including the use of custom-made grafts that incorporate branches and fenestrations, alongside off-the-shelf devices, have greatly enhanced the feasibility and effectiveness of these interventions. Despite the high technical success, low early mortality and morbidity recorded in large retrospective cohorts of high-volume aortic centers, the durability of complex endovascular approaches is still questioned due to the higher reintervention rates [4,5,6]. Especially for complex endovascular aortic repair, target vessel adverse events are the leading cause for reintervention during the mid-term follow-up [5,6]. Previous analyses on fenestrated versus branched devices showed that fenestrations, when applicable, are superior to branches in terms of target vessel instability [7].
Recent studies show that postoperative hemodynamics in the visceral branches critically influence F / BEVAR and chEVAR success [8,9]. Abnormal flow patterns and shear-stress distributions have been linked to branch stenosis, impaired organ perfusion, and increase target vessel instability events. Given the variability in endograft and techniques, understanding the impact of configuration on target vessels blood flow remains an important unresolved issue [1,10,11,12]. Due to the lack of patient-specific hemodynamic data at the inlet and outlets of the 3D vascular models, advanced multiscale cardiovascular models, 3D–1D, can generate the required waveforms for the 3D simulations and assisted understanding of complex hemodynamic features [13].
This study aims to compare the blood-flow characteristics in target vessels after complex endovascular aortic aneurysm repair using different approaches (FEVAR, BEVAR and chEVAR) using patient-specific computational models.
2. Materials and Methods
Study design and patient selection. A retrospective analysis was conducted on blood flow features pre- and post- FEVAR, BEVAR and chEVAR, see Supplementary Figure 1, among patients that were managed for degenerative complex aortic aneurysms between 2018 and 2021 in a single-tertiary center. Computed tomography angiography (CTA) scans were used to define the pre- and post-repair blood flow lumens of patients with complex aortic aneurysms using computational fluid dynamics simulations, with special focus on the hemodynamic properties of the visceral vessels [8,13].
Patients with juxta-renal, para-renal and thoracoabdominal aortic aneurysms that were managed using FEVAR, BEVAR or chEVAR under elective setting and completed the one-month CTA (slice thickness <1mm and arterial phase) imaging follow-up were considered eligible. A revascularization and bridging of three (for chEVAR) or four target vessels was a criterion for inclusion. The decision for the treatment approach relied on patient-specific characteristics, anatomy of the aorta and target vessels and availability of devices and materials. Patients managed for aortic dissections (acute or chronic), pseudoaneurysms or had an anamnesis of previous endovascular or open aortic aneurysm repair were excluded. No surgeon-modified endografts were used during the study period.
Pseudonymized pre- and post-operative computed tomography angiographies (CTA) of 3 cases for each technique (FEVAR, BEVAR and chEVAR) were collected and analyzed. This study complied with the declaration of Helsinki. No Ethics Committee approval was required due to its retrospective nature and pseudonymized information.
Endovascular approaches. FEVAR was used for the treatment of juxta- and para-renal aortic aneurysms, if the apposition of the device on the aortic wall and especially the level of the target vessels was expected. All FEVAR cases were managed with company-manufactured custom-made devices relying on the Zenith Platform (Cook Medical, Bloomington, IN, USA) [14]. BEVAR was chosen for patients with more extensive aortic pathologies, including thoracoabdominal aneurysms, when a device apposition on the aortic wall was not expected. Patients managed with BEVAR were treated using off-the-shelf branched devices (T-Branch device, William Cook Europe, Bjaeverskov, Denmark); all relying on the Zenith platform. ChEVAR was used in urgent cases (symptomatic or ruptured juxta- or pararenal aortic aneurysms) or aneurysms with a diameter over 70mm, when a custom-made was not available due to the long-time interval for device design and manufacture. For patients managed with chEVAR, the Endurant IIs (Medtronic, Santa Rosa, CA, USA) device was used as aortic component. All aortic devices were oversized by 20%, except for chEVAR, where the aortic device was oversized by 30%, respecting that three target vessels were revascularized [15].
All target vessels were bridged using the same bridging stents (BeGraft Peripheral, Bentley, Hechingen, Germany). The bridging stent diameter and length was decided upon the technical features of the main device and the distal landing zone and anatomy of the target vessels. Details on anatomic parameters and devices are presented in Table 1.
Modeling. The 3D model of the FEVAR, chEVAR, BEVAR system, including the Celiac Artery (CA), Superior mesenteric Artery (SMA), Left Renal Artery (LRA), Right Renal Artery (RRA), was constructed using the CTA scan for each patient Supplementary Figure 1A. The reconstruction of the DICOM images into a 3D lumen model was performed using the methodology mentioned in previous studies [8,9,13].
The reconstruction of geometry under consideration started just above the CA and ended just below the iliac bifurcation, while the region of interest was the visceral aorta and specifically the CA, SMA, RRA and LRA. For the FEVAR and BEVAR cases, the segmentation was performed as a combined structure. Regarding chEVAR cases, the lumen of the covered abdominal aorta and stented visceral arteries (SMA, RRA, LRA) were segmented separately using the same software, Supplementary Figure 1. The optimal smoothing factor value (SFV) was determined to be 0.05, based on a smoothing parameter study performed on renal and mesenteric diameters using the Vascular Modeling Toolkit (VMTK) [8].
The following hemodynamic parameters: Time Average Wall Shear Stress (TAWSS), Oscillatory Shear Index (OSI), Relative residence time (RRT) and Local Normalized Helicity (LNH) were calculated. The postoperative results presented correspond to a representative patient from each group, as no significant differences between patients were observed.
Numerical simulations were performed with the software package Ansys Fluent (Ansys Inc., Canonsburg, Pennsylvania, United States). Blood was considered a Newtonian fluid with a density of ρ = 1050 kg/m-3 and a kinematic viscosity of v=3.2 × 10-6 m3 s-1. The zero-velocity condition was applied on the surface of the endograft, following the rigid wall assumption. Over two million tetrahedral elements were discretized from the fluid domain, with an additional three-layer boundary the inner element size was approximately 1 mm. The boundary conditions at the inlet and outlets were defined using the flow and pressure waveforms obtained from the multiscale model (0D-3D) developed in our previous studies [9,13]. Specifically, a flow waveform representing physiological (healthy) conditions, obtained from the literature, was applied to the input [9,13]. At the outlets, resistance-based boundary conditions (pressure waveforms) derived from the 1D mathematical model were imposed for each respective artery. The velocity profile at the outputs was almost parabolic during the systolic phase [8,13,16,17,18,19,20]. Convergence to the solution at each step was considered achieved when the computational error fell below 10-4. We used exclusively the results of the last cardiac cycle, avoiding any dynamic behavior of the first pulses [10]. Grid independence tests were performed in regions of predicted disturbed flow to determine the optimal mesh size. The simulation was considered grid-independent when the hemodynamic parameters (velocity and pressure) varied by less than 2% between successive mesh refinements [21]. In all 3D cases, a parabolic velocity waveform is imposed at the inlet, no-slip condition at the wall (i.e. on the stent-graft surface) and pressure waveforms at all outlets (Supplementary Figure 2). The latter (pressure waveforms) were derived from a 1D hemodynamic model of the entire arterial network [13,16,18,19,20,22,23,24,25]. Paraview (Kitware Inc.) software was used for the visualization of hemodynamic parameters.
Statistical analysis. Differences in hemodynamic parameters (RRT, OSI, TAWSS) among the three endograft groups were assessed in the target vessels (SMA, LRA, RRA) using one-way ANOVA, with p < 0.05 considered statistically significant.
3. Results
Wall Shear Stress (WSS). Postoperatively, during the peak systole, WSS values showed the maximum value of 3Pa for all designs (Figure 1). Higher WSS values across the whole structure and especially in the visceral arteries were observed for BEVAR cases, followed by intermediate values for FEVAR and the lowest values for chEVAR as shown in Table 2.
Local Normalized Helicity (LNH). The helical structures in all three endograft groups are distributed evenly throughout the device (Figure 2). In FEVAR cases (Figure 2A), the helical patterns appear more compact and smoother compared to those observed in BEVAR (Figure 2C). Postoperatively, the helical structures in BEVAR were more pronounced and exhibited a clearer rotational configuration (|LNH| < 0.3). According to the literature, a threshold value of 0.3 is typically considered indicative of rotational flow structures [26,27,28]. In contrast, in FEVAR cases (Figure 2A), the local normalized helicity (LNH) shows less rotational behavior compared to chEVAR (Figure 2B). Additionally, in the visceral arteries of all groups, a relatively uniform distribution of helical structures was observed postoperatively.
Time Averaged Wall Shear Stress (TAWSS). The results were evaluated assuming a maximum TAWSS value of 3Pa. As shown in Table 2, BEVAR exhibited the highest TAWSS values, compared to the other two techniques. BEVAR and FEVAR demonstrated relatively high TAWSS, with only minor deviations between them, whereas chEVAR cases showed significantly lower TAWSS (Figure 3). In BEVAR cases, increased TAWSS was distributed across nearly the entire surface of the structure, while in FEVAR cases, moderate TAWSS values were observed primarily in the region below the renal arteries and above the iliac bifurcation (Figure 3A).
Oscillatory Shear Index (OSI) and Relative Residence Time (RRT). There were areas of low OSI values, in the main aortic endograft for all groups. More regions of low value of localized OSI, mainly occurred in the FEVAR and BEVAR cases. OSI showed intense oscillations in individual locations of the visceral arteries in the chEVAR group. In postoperative BEVAR cases, the OSI showing increased values among the mesenteric and renal arteries Supplementary Figure 3C. In BEVAR target vessels, low levels of OSI in proximal end and moderate values in the distal end were recorded, in contrary to chEVARs, where high value localized OSI prevails [Supplementary Figures 3C and B]. In all cases, the RRT values were mainly driven by the OSI patterns following the opposite behavior (Supplementary Figures 3 and 4).
Flow comparison in FEVAR, chEVAR and BEVAR. The flow at peak systole in FEVAR, chEVAR and BEVAR groups is depicted in Figure 4. The maximum flow velocity in the visceral arteries was recorded in BEVAR ~2.5 m/s versus ~2.2 m/s in chEVAR and ~1.7m/s in FEVAR cases (Table 2). No statistically significant differences in visceral vessel flow were observed between FEVAR and chEVAR. The endograft segment between the CA and renal arteries showed increased flow in BEVAR, while the flow was smoother in the main body of the other two techniques (Figure 4) than in chEVAR [Supplementary Figure 5B], during the systolic phase.
Mean visceral hemodynamics. No statistically significant differences were found in RRT and OSI of the target vessels among the techniques. Comparing the mean values of hemodynamic parameters (RRT, OSI and TAWSS), only slight differences were observed between FEVAR and BEVAR. In contrast, chEVAR showed deviation from the other two groups Figure 5.
Statistically significant differences (p < 0.05) were observed for TAWSS, for the SMA (p = 0.0162) and RRA (p = 0.0255) in the post-operative setting. Regurgitant flow in the visceral arteries was computed and compared across FEVAR, chEVAR, and BEVAR cases. chEVAR exhibited the highest mean value, FEVAR intermediate, and BEVAR the lowest, Table 3 [8,17].
4. Discussion
FEVAR / BEVAR expanded their targeted patient population and currently represents the recommended approach in patients with adequate anatomy and complex aortic aneurysms while chimney technique received a lot of criticism regarding the risk for failure of the proximal landing zone and higher endoleak rates and represents mainly a bailout approach [29,30,31]. FEVAR and chEVAR endovascular aortic repair have been applied in anatomically suitable complex aortic aneurysms. Regardless of the technique, endovascular management seems to provide a higher benefit in terms of mortality and morbidity perioperatively while the need for reintervention still represents a major issue, with most of them though being minor and endovascularly performed, without impact on survival [29,30,31]. Except for the main device, target-vessels’ fate plays a significant role in FBEVAR and chEVAR clinical success, with endoleaks, occlusions and instability affecting the durability of the procedure and being related mainly to branches [32]. In this study a multiscale computational approach composed of simple holistic mathematical models combined with advanced 3D CFD simulations could provide clinicians with important information about patients’ hemodynamics. Further clinicians can evaluate the applications of the 3 methods, follow the appropriate treatment strategy for each patient in the treatment of complex aneurysms and predict any postoperative complications. In this analysis evaluating the hemodynamic performance of fenestrated, branched devices and chimney approaches, it was shown that all techniques lead to a reconstruction of the aortic and visceral vessel geometry and hemodynamic results close to normal levels [8,10,11,12,13]. Higher-pressure values during the systolic phase were obtained proximally in the main device regarding target-EVAR cases followed by chEVAR while the lowest values were recorded in FEVAR cases. Overall, FEVAR and BEVAR seem to provide similar smoother flow with less regurgitation than the chimney technique.
FEVAR and chEVAR are usually applied in anatomically similar complex abdominal aortic aneurysms, but their application may lead to distinct local hemodynamic changes. An overall improvement in hemodynamics was detected after repair with either technique, with improved hemodynamics towards normal values and reduced recirculation zones in the main graft and target vessels. Preoperatively, a disturbed pro-thrombotic WSS profile was recorded in several zones of the sac in both FEVAR and chEVAR cases. The LNH results showed a better organization of the helical structures at post-operative setting, decreasing thrombus formation, with either modality. Similarly, TAWSS increased and OSI decreased post-operatively, signaling non-disturbed blood flow. The RRT was locally reduced. The flow in target vessels tended to be more streamlined in chEVAR, compared to evident recirculation regions at renal and superior mesenteric artery fenestrations (p = 0.06); a finding probably related to the configuration of the bridging stent, with chimney grafts running vertically while the fenestration bridging stents run transversely. However, FEVAR showed less intense flow regurgitation in bridging stents.
Regarding the comparative findings on BEVAR and FEVAR, the hemodynamic characteristics after the repair were clearly improved regardless of the approach. The WSS profiles of BEVARs show slightly higher values, compared to FEVARs. LNH in both cases improved by suppressing the disturbed blood flow but providing a more balanced distribution in FEVARs cases. The distribution of TAWSS in BEVAR was prominently increased in the entire structure, which leads to low values of OSI and RRT. The flow in target vessels seems to be more streamlined in FEVAR but presents an instant increase, compared to BEVAR where the flow develops gradually, with BEVAR showing slightly less recirculation zones in the branches, in contrast to FEVAR where the flow is more stable. These findings justify the fact that in FEVAR, we have less occlusion and more stable technical outcomes in target vessels as also reported in the literature [33,34].
Limitations. The elastic properties of the graft material were not considered, and the surface of the lumen was modeled as rigid. Blood could be modeled as non-Newtonian fluid, separating red blood cells from plasma, which were considered in the current study as a single continuum medium. The geometric and structural parameters employed in the 1D arterial model were based on bibliographic data. A future arterial model could be constructed with a geometry and elasticity database derived from patient-based measurements, and the model predictions would be compared with non-invasive measurements. The selection of the patients utilized in the present study was made after anatomical control, so that our sample is morphologically comparable. In the comparative results of FEVAR, chEVAR and BEVAR, the different preoperative anatomical characteristics should be considered. To validate the hemodynamic predictions, we could impose patient-specific boundary conditions on each individual patient. An extended study on a larger cohort of patients could shed light on the hemodynamics of patients undergoing complex endovascular repair. In addition, patient-specific boundary conditions could be imposed on each individual patient for obtaining more accurate hemodynamic predictions.
5. Conclusions
In this study, a multiscale modeling framework was employed, coupling low-order computational models with three-dimensional CFD simulations to investigate postoperative aortic hemodynamics. Key flow-related quantities, including velocity, local normalized helicity (LNH), wall shear stress (WSS), and time-averaged wall shear stress (TAWSS), were analyzed in patient-specific aortic geometries following implantation of advanced endovascular devices, namely BEVAR, chEVAR, and FEVAR.
All three endovascular designes led to an overall improvement in postoperative blood flow characteristics toward near-physiological conditions, with a reduction in adverse flow patterns and recirculation zones. FEVAR demonstrated more stable visceral artery perfusion, BEVAR exhibited higher flow rates with fewer recirculation regions, while chEVAR showed more streamlined visceral artery flow accompanied by reduced regurgitation at the bridging stent entries. Despite these differences, all configurations effectively preserved visceral artery perfusion.
Overall, all EVAR designs produced comparable hemodynamic outcomes across most parameters and consistently improved flow conditions relative to the pathological state. FEVAR was associated with lower velocity magnitudes and more uniform, smoother helicity distributions compared to BEVAR and chEVAR. In contrast, the multiscale model predicted higher visceral artery flow values in the BEVAR configuration relative to FEVAR. The use of three-dimensional, patient-specific aortic models enhances the clinical relevance of the present findings and supports their potential application in personalized treatment planning. These results may further contribute to the future technological refinement of branch endografts tailored for use in F/BEVAR and chEVAR procedures.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, S.M, S.K, A.R, L.F., P.N., G.K., A.G., M.X. and M.M.; methodology, S.M, S.K, A.R, L.F., P.N., G.K., A.G., M.X. and M.M.; software, S.M, S.K, A.R, L.F., and M.X.; validation, S.M, S.K, A.R, L.F., P.N., M.X. and M.M.; formal analysis, S.M, S.K, A.R, L.F., P.N., G.K., A.G., M.X. and M.M.; investigation, S.M, S.K, A.R, L.F., P.N., G.K., A.G., M.X. and M.M.; resources, A.G., M.X. and M.M.; data curation, S.M, S.K, A.R, L.F., P.N., G.K., A.G., M.X. and M.M.; writing—original draft preparation, S.M, S.K, A.R, L.F., P.N., G.K., A.G., M.X. and M.M.; writing—review and editing, S.M, S.K, A.R, L.F., P.N., G.K., A.G., M.X. and M.M.; visualization, S.M, S.K, A.R and L.F.; supervision, P.N., G.K., A.G., M.X. and M.M.; project administration, A.G., M.X. and M.M.; funding acquisition, G.K., A.G., M.X. and M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially carried out within the framework of the Action “Flagship actions in interdisciplinary scientific fields with a special focus on the productive fabric”, which is implemented through the National Recovery and Resilience Plan Greece 2.0, funded by the European Union—NextGenerationEU (Project ID: TAEDR-0535983).”.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FEVAR | Fenestrated endovascular repair |
| BEVAR | Branched endovascular repair |
| chEVAR | Chimney endovascular repair |
| CFD | Computational fluid dynamics |
| WSS | Wall shear stress |
| AAA | Abdominal aortic aneurysm |
| RRA | Right renal artery |
| LRA | Left renal artery |
| SMA | Superior mesenteric Artery |
| CA | Celiac artery |
| RRT | Relative residence time |
| OSI | Oscillatory Shear Index |
| TAWSS | Time-averaged wall shear stress |
| LNH | Local normalized helicity |
References
- Tran K, Deslarzes-Dubuis C, DeGlise S, Kaladji A, Yang W, Marsden AL, et al. Patient-specific computational flow simulation reveals significant differences in paravisceral aortic hemodynamics between fenestrated and branched endovascular aneurysm repair. JVS-Vascular Science 2024;5. [CrossRef]
- Greenberg R, Eagleton M, Mastracci T. Branched endografts for thoracoabdominal aneurysms. The Journal of Thoracic and Cardiovascular Surgery 2010; 140:S171–8. [CrossRef]
- Wanhainen A, Van Herzeele I, Bastos Goncalves F, Bellmunt Montoya S, Berard X, Boyle JR, D'Oria M, Prendes CF, Karkos CD, Kazimierczak A, Koelemay MJW, Kölbel T, Mani K, Melissano G, Powell JT, Trimarchi S, Tsilimparis N; ESVS Guidelines Committee; Antoniou GA, Björck M, Coscas R, Dias NV, Kolh P, Lepidi S, Mees BME, Resch TA, Ricco JB, Tulamo R, Twine CP; Document Reviewers; Branzan D, Cheng SWK, Dalman RL, Dick F, Golledge J, Haulon S, van Herwaarden JA, Ilic NS, Jawien A, Mastracci TM, Oderich GS, Verzini F, Yeung KK. Editor's Choice -- European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. Eur J Vasc Endovasc Surg. 2024 Feb;67(2):192-331.
- Finnesgard EJ, Jones DW, Beck AW, Eagleton MJ, Farber MA, Gasper WJ, Lee WA, Oderich GS, Schneider DB, Sweet MP, Timaran CH, Schanzer A; United States Aortic Research Consortium. Trends and outcomes over time with fenestrated and branched endovascular aortic repair in the United States Aortic Research Consortium. J Vasc Surg. 2025 Jun;81(6):1235-1243. [CrossRef]
- Fargion AT, Esposito D, Speziali S, Pulli R, Gallitto E, Faggioli G, Gargiulo M, Bertoglio L, Melissano G, Chiesa R, Simonte G, Isernia G, Lenti M, Pratesi C; Italian Multicentre Fenestrated and Branched (IMF&B) Study Group. Fate of target visceral vessels in fenestrated and branched complex endovascular aortic repair. J Vasc Surg. 2023 Sep;78(3):584-592.e2.
- Dossabhoy SS, Simons JP, Diamond KR, Flahive JM, Aiello FA, Arous EJ, Messina LM, Schanzer A. Reinterventions after fenestrated or branched endovascular aortic aneurysm repair. J Vasc Surg. 2018 Sep;68(3):669-681. [CrossRef]
- Gorgatti F, Nana P, Panuccio G, Rohlffs F, Torrealba JI, Kölbel T. Post-dissection Thoraco-abdominal Aortic Aneurysm Managed by Fenestrated or Branched Endovascular Aortic Repair. Eur J Vasc Endovasc Surg. 2024 Sep;68(3):325-334. [CrossRef]
- Malatos S, Fazzini L, Raptis A, Nana P, Kouvelos G, Tasso P, et al. Evaluation of Hemodynamic Properties After Chimney and Fenestrated Endovascular Aneurysm Repair. Annals of Vascular Surgery 2024; 104:237–47. [CrossRef]
- Katsoudas S, Malatos S, Raptis A, Matsagkas M, Giannoukas A, Xenos M. Blood Flow Simulation in Bifurcating Arteries: A Multiscale Approach After Fenestrated and Branched Endovascular Aneurysm Repair. Mathematics. 2025; 13(9):1362. [CrossRef]
- Raptis A, Xenos M, Georgakarakos E, Kouvelos G, Giannoukas A, Labropoulos N, et al. Comparison of physiological and post-endovascular aneurysm repair infrarenal blood flow. Comput Methods Biomech Biomed Engin 2017; 20:242–9. [CrossRef]
- Suess T, Anderson J, Danielson L, Pohlson K, Remund T, Blears E, et al. Examination of near-wall hemodynamic parameters in the renal bridging stent of various stent graft configurations for repairing visceral branched aortic aneurysms. Journal of Vascular Surgery 2016; 64:788–96. [CrossRef]
- Tran K, Deslarzes-Dubuis C, DeGlise S, Kaladji A, Yang W, Marsden AL, et al. Patient-specific computational flow simulation reveals significant differences in paravisceral aortic hemodynamics between fenestrated and branched endovascular aneurysm repair. JVS-Vascular Science 2024;5. [CrossRef] [PubMed]
- Malatos S, Raptis A, Xenos MA, Kouvelos G, Katsargyris A, Giannoukas A, et al. A multiscale model for hemodynamic properties’ prediction after fenestrated endovascular aneurysm repair. A pilot study 2019;1.
- Chait J, Tenorio ER, Mendes BC, Barbosa Lima GB, Marcondes GB, Wong J, Macedo TA, De Martino RR, Oderich GS. Impact of gap distance between fenestration and aortic wall on target artery instability following fenestrated-branched endovascular aortic repair. J Vasc Surg. 2022 Jul;76(1):79-87.e4. [CrossRef]
- Fazzini S, Martinelli O, Torsello G, Austermann M, Pipitone MD, Torsello GF, Irace L, Donas KP. The PROTAGORAS 2.0 Study to Identify Sizing and Planning Predictors for Optimal Outcomes in Abdominal Chimney Endovascular Procedures. Eur J Vasc Endovasc Surg. 2021 Apr;61(4):591-602. [CrossRef]
- Olufsen MS, Peskin CS, Kim WY, Pedersen EM, Nadim A, Larsen J. Numerical simulation and experimental validation of blood flow in arteries with structured-tree outflow conditions. Ann Biomed Eng 2000; 28:1281–99. [CrossRef]
- Reymond P, Merenda F, Perren F, Rüfenacht D, Stergiopulos N. Validation of a one-dimensional model of the systemic arterial tree. American Journal of Physiology-Heart and Circulatory Physiology 2009; 297:H208–22. [CrossRef]
- Malatos S. Advances in Low-Dimensional Mathematical Modeling of the Human Cardiovascular System n.d.
- Morbiducci U, Ponzini R, Gallo D, Bignardi C, Rizzo G. Inflow boundary conditions for image-based computational hemodynamics: impact of idealized versus measured velocity profiles in the human aorta. J Biomech 2013; 46:102–9. [CrossRef]
- van de Vosse F, Stergiopulos N. Pulse Wave Propagation in the Arterial Tree. Annu Rev Fluid Mech 2011; 43:467–99. [CrossRef]
- Raptis A, Xenos M, Georgakarakos E, Kouvelos G, Giannoukas A, Matsagkas M. Hemodynamic Profile of Two Aortic Endografts Accounting for Their Postimplantation Position. Journal of Medical Devices 2017;11. [CrossRef]
- Reymond P, Bohraus Y, Perren F, Lazeyras F, Stergiopulos N. Validation of a patient-specific one-dimensional model of the systemic arterial tree. Am J Physiol Heart Circ Physiol 2011;301:H1173-1182. [CrossRef]
- Alastruey J, Parker K, Peiro J, Sherwin S. Lumped parameter outflow models for 1-D blood flow simulations: Effect on pulse waves and parameter estimation. Communications in Computational Physics 2008; 4:317–36.
- Sherwin SJ, Franke V, Peiró J, Parker K. One-dimensional modelling of a vascular network in space-time variables. Journal of Engineering Mathematics 2003; 47:217–50. [CrossRef]
- Xiao N, Humphrey JD, Figueroa CA. Multi-scale computational model of three-dimensional hemodynamics within a deformable full-body arterial network. Journal of Computational Physics 2013; 244:22–40. [CrossRef]
- Tasso P, Raptis A, Matsagkas M, Rizzini ML, Gallo D, Xenos M, et al. Abdominal Aortic Aneurysm Endovascular Repair: Profiling Postimplantation Morphometry and Hemodynamics With Image-Based Computational Fluid Dynamics. J Biomech Eng 2018; 140:111003. [CrossRef]
- Pan W, Kulisa P, Bou-Saïd B, Hajem ME, Simoëns S, Sigovan M. A proposal of risk indicators for pathological development from hemodynamic simulation: application to aortic dissection. Journal of Cardiology and Cardiovascular Medicine 2023; 8:029–38. [CrossRef]
- Gallo D, Bijari PB, Morbiducci U, Qiao Y, Xie YJ, Etesami M, et al. Segment-specific associations between local haemodynamic and imaging markers of early atherosclerosis at the carotid artery: an in vivo human study. J R Soc Interface 2018; 15:20180352. [CrossRef]
- Raulli SJ, Gomes VC, Parodi FE, Vasan P, Sun D, Marston WA, Pascarella L, McGinigle KL, Wood JC, Farber MA. Five-year outcomes of fenestrated and branched endovascular repair of complex aortic aneurysms based on aneurysm extent. J Vasc Surg. 2024 Aug;80(2):302-310. [CrossRef]
- Dossabhoy SS, Sorondo SM, Tran K, Stern JR, Dalman RL, Lee JT. Reintervention does not affect long-term survival after fenestrated endovascular aneurysm repair. J Vasc Surg. 2022 Nov;76(5):1180-1188.e8. [CrossRef]
- Bannazadeh M, Beckerman WE, Korayem AH, McKinsey JF. Two-year evaluation of fenestrated and parallel branch endografts for the treatment of juxtarenal, suprarenal, and thoracoabdominal aneurysms at a single institution. J Vasc Surg. 2020 Jan;71(1):15-22. [CrossRef]
- Tenorio ER, Schanzer A, Timaran CH, Schneider DB, Mendes BC, Eagleton MJ, Farber MA, Parodi FE, Gasper WJ, Beck AW, Sweet MP, Huang Y, Oderich GS; U.S. Fenestrated and Branched Aortic Research Consortium. Mid-term Renal and Mesenteric Artery Outcomes During Fenestrated and Branched Endovascular Aortic Repair for Complex Abdominal and Thoracoabdominal Aortic Aneurysms in the United States Aortic Research Consortium. Ann Surg. 2023 Oct 1;278(4): e893-e902. [CrossRef]
- T Pini R, Faggioli G, Gallitto E, Mascoli C, Fenelli C, Ancetti S, Vacirca A, Gargiulo M. The different effect of branches and fenestrations on early and long-term visceral vessel patency in complex aortic endovascular repair. J Vasc Surg. 2020 Apr;71(4):1128-1134. [CrossRef]
- T Martin-Gonzalez T, Mastracci T, Carrell T, Constantinou J, Dias N, Katsargyris A, Modarai B, Resch T, Verhoeven E, Haulon S. Mid-term Outcomes of Renal Branches Versus Renal Fenestrations for Thoraco-abdominal Aneurysm Repair. Eur J Vasc Endovasc Surg. 2016 Aug;52(2):141-8. [CrossRef]
Figure 1.
WSS in (A) FEVAR, (B) ChEVAR and (C) BEVAR cases, for systolic peak and diastole.
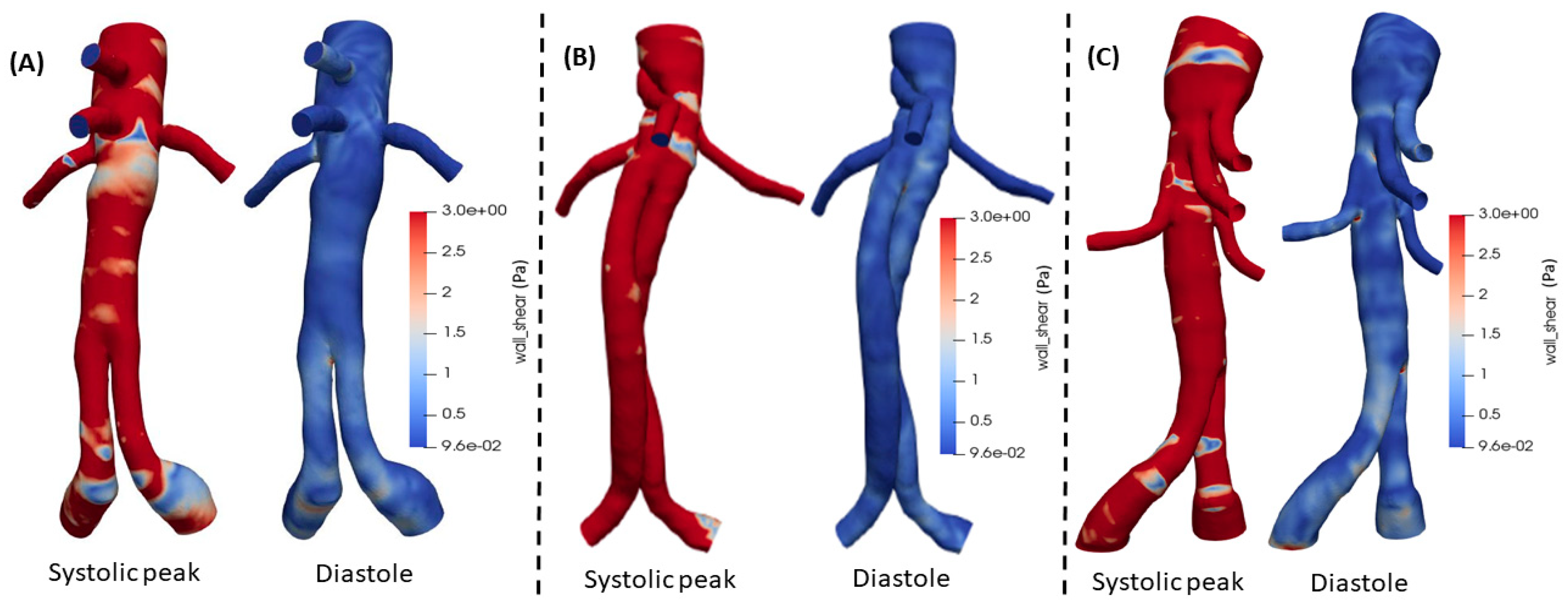
Figure 2.
LNH in (A) FEVAR, (B) ChEVAR and (C) BEVAR cases in different cardiac phases.
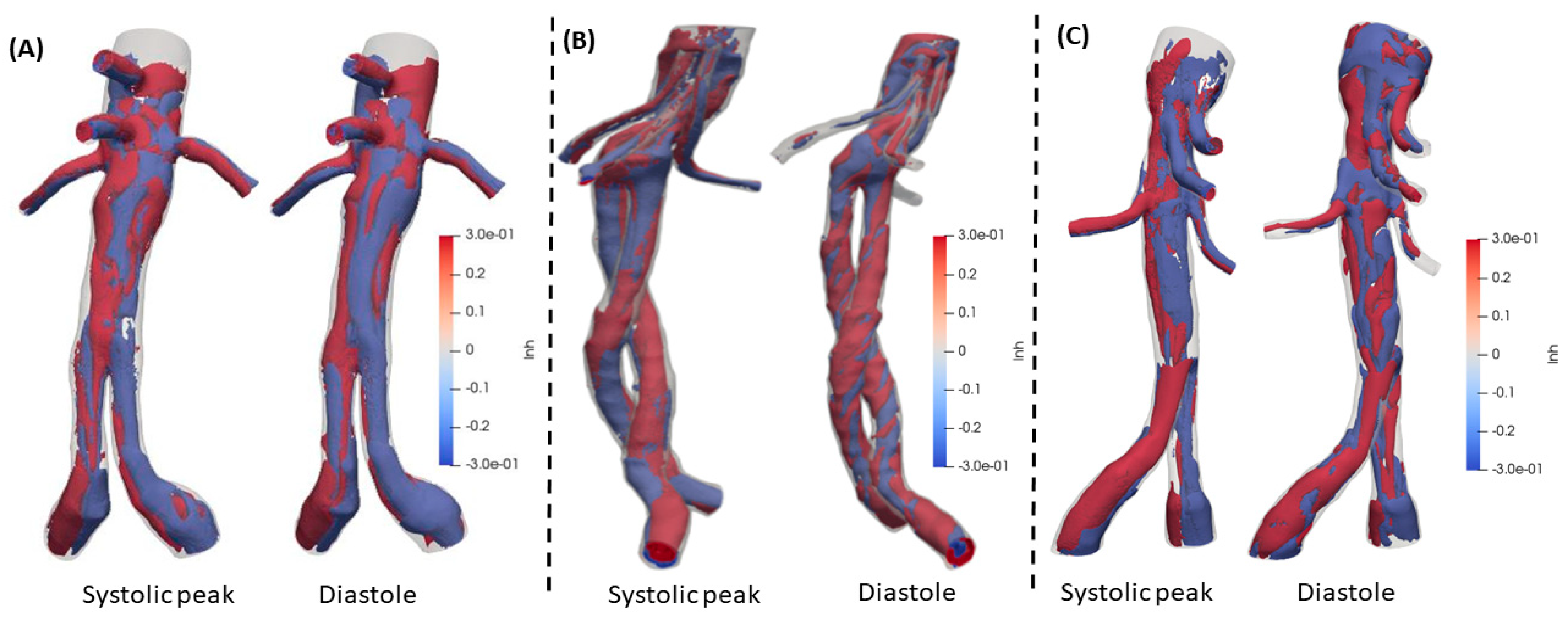
Figure 3.
Time averaged Wall Shear Stress (TAWSS) in (A) FEVAR, (B) chEVAR and (C) BEVAR cases.
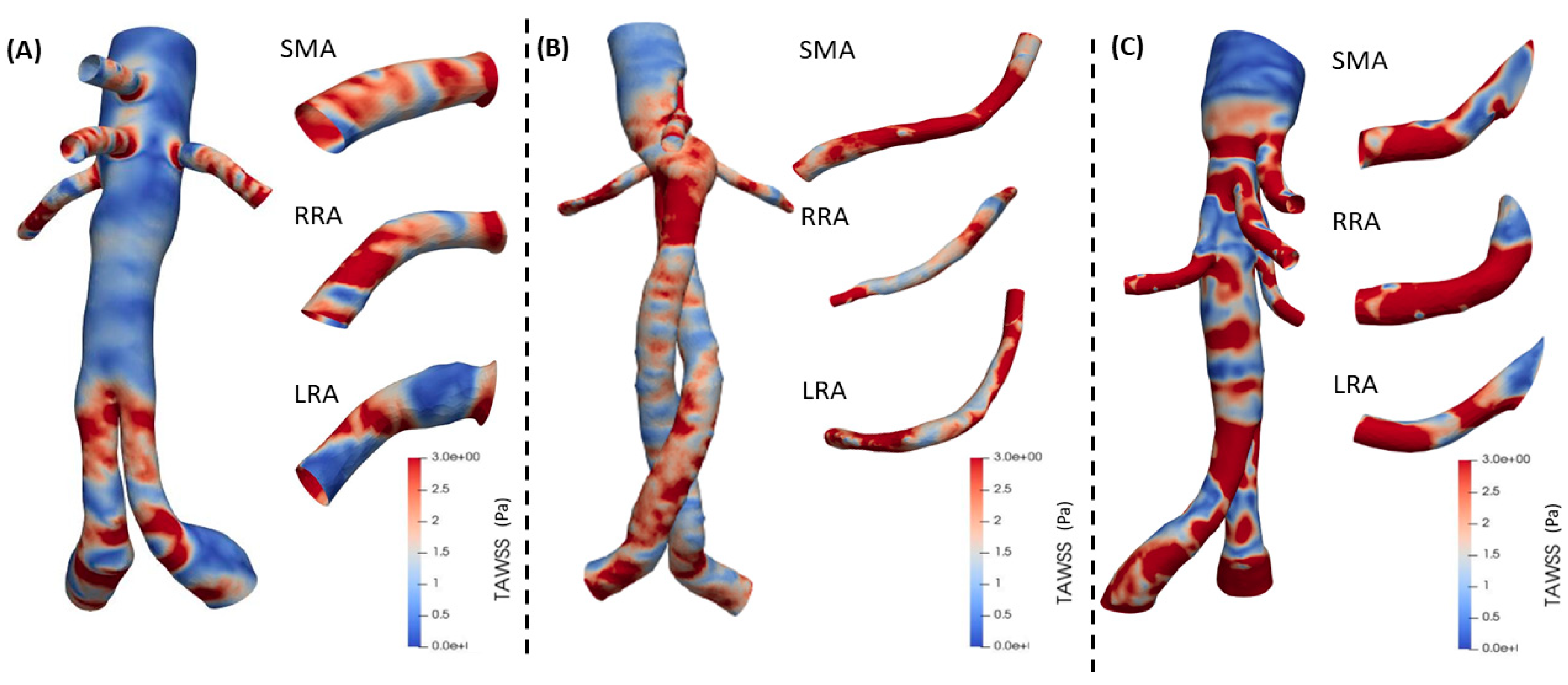
Figure 4.
Flow comparison (velocity magnitude) of the secondary arteries at systolic peak, mesenteric (SMA) and renal arteries (LRA, RRA), between (A) FEVAR, (B) chEVAR and (C) BEVAR cases.
Figure 4.
Flow comparison (velocity magnitude) of the secondary arteries at systolic peak, mesenteric (SMA) and renal arteries (LRA, RRA), between (A) FEVAR, (B) chEVAR and (C) BEVAR cases.
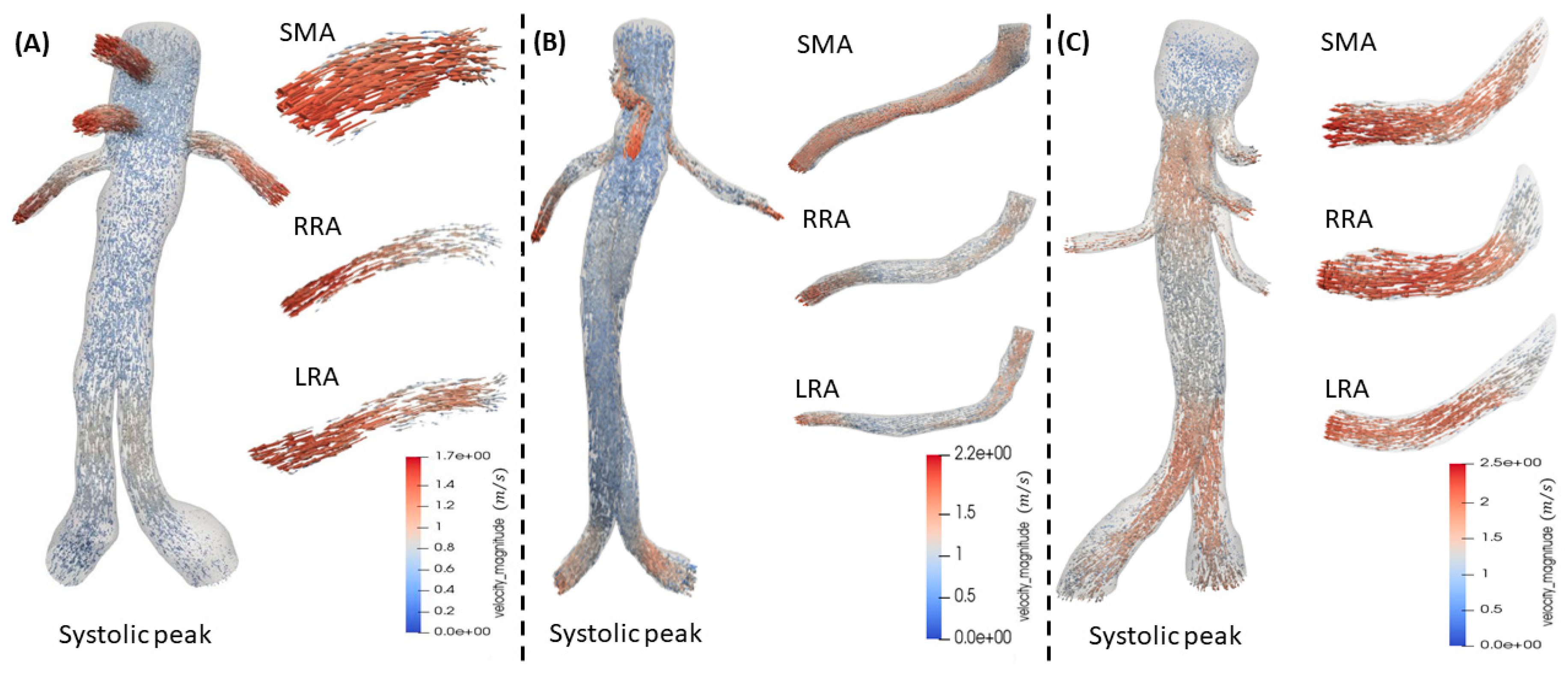
Figure 5.
Mean values for the hemodynamic parameters (RRT, OSI and TAWSS) between FEVAR, chEVAR and BEVAR endograft groups.
Figure 5.
Mean values for the hemodynamic parameters (RRT, OSI and TAWSS) between FEVAR, chEVAR and BEVAR endograft groups.


Table 1.
Main body and bridging stent details of each patient.
| Cases | Main body | Max aortic diameter at proximal landing zone | Max visceral aortic diameter | Infrarenal aortic angulation | Neck calcification/ thrombus in >25% of the circumference of landing zone | Bridging stent | Diameter of TVs at landing zone | Angles of TVs* |
| FEVAR | ||||||||
| 1 | COOK FENESTRATED GRAFT: 36x22x162mm | 30.2mm | 33.0mm | 20.0° | No | RRA: BeGraft 6x28mm - LRA: BeGraft 6x28mm - SMA: BeGraft 8x37mm - CA: BeGraft 9x37mm | RRA: 6.1mm LRA: 6.1mm SMA: 7.5mm |
RRA: 25° LRA: 3° SMA: 27° |
| 2 | COOK FENESTRATED GRAFT: 30x22x114mm | 26.0mm | 29.6mm | 8.0° | No | RRA: BeGraft 6x28mm - LRA: BeGraft 6x28mm - SMA: BeGraft 8x37mm | RRA: 6.0mm LRA: 5.7mm SMA: 7.6mm |
RRA: 23° LRA: 18° SMA: 10° |
| 3 | COOK FENESTRATED GRAFT: 38x35x162mm | 31.5mm | 30.7mm | 17.0° | No | RRA: BeGraft 6x28mm - LRA: Begraft 6x28mm - SMA: Begraft 8x37mm - CA: Begraft 9x37mm | RRA: 5.7mm LRA: 6.0mm SMA: 7.7mm |
RRA: 27° LRA: 17° SMA: 23° |
| ChEVAR | ||||||||
| 1 | ENDURANT IIs GRAFT: 36x14x103mm | 27.6mm | 32.0mm | 15.8° | No | RRA: BeGraft 6x58mm - LRA: BeGraft 6x58mm - SMA: BeGraft 8x57mm | RRA: 5.3mm LRA: 6.0mm SMA: 7.9mm |
RRA: 32° LRA: 12° SMA: 31° |
| 2 | ENDURANT IIs GRAFT: 36x14x103mm | 27.1mm | 27.6mm | 31.0° | No | RRA: Begraft 6x58mm - LRA: BeGraft 6x58mm - SMA: BeGraft 8x57mm | RRA: 5.1mm LRA: 5.6mm SMA: 7.9mm |
RRA: 37° LRA: 8° SMA: 26° |
| 3 | ENDURANT IIs GRAFT: 36x14x103mm | 27.0mm | 29.0mm | 28.0° | No | RRA: BeGraft 6x58mm - LRA: BeGraft 6x58mm - SMA: BeGraft 8x57mm | RRA: 5.5mm LRA: 5.9mm SMA: 7.7mm |
RRA: 24° LRA: 28° SMA: 43° |
| BEVAR | ||||||||
| 1 | COOK T-BRANCH DEVICE: 34x19x202mm | 30.5mm | 36.8mm | 15° | No | RRA: BeGraft 6x57mm – LRA: BeGraft 6x57 – CA: BeGraft 8*57 – SMA: BeGraft 8x57 | RRA: 5.6MM LRA:5.2MM CA: 8.1MM SMA: 7.8MM |
RRA:21° LRA:20° SMA: 17° |
| 2 | COOK THORACIC 49x36x217mm+ COOK T-BRANCH DEVICE: 34x19x202mm | 26mm | 32.4mm | 14° | No | RRA: BeGraft 7x57mm – LRA: BeGraft 7x57 – CA: BeGraft 9x59mm – SMA: BeGraft 8x57mm | RRA: 6.7mm LRA:7mm CA: 8.6mm SMA: 8.1mm |
RRA:6° LRA:16° SMA: 6° |
| 3 | COOK T-BRANCH DEVICE: 34x19x202mm | 31mm | 33mm | 15° | No | RRA: BeGraft 6x57mm – LRA: BeGraft 7x57 – CA: BeGraft 8x59mm – SMA: BeGraft 9x57mm | RRA: 6.5mm LRA:7.1mm CA: 8mm SMA: 8.6mm |
RRA:10° LRA:14° SMA: 101° |
Table 2.
Mean values for the hemodynamic parameters, between FEVAR, chEVAR and BEVAR cohorts.
| FEVAR | ChEVAR | BEVAR | FEVAR | ChEVAR | BEVAR | FEVAR | ChEVAR | BEVAR | |
| RRT-Mean (1/Pa) | SMA | SMA | SMA | RRA | RRA | RRA | LRA | LRA | LRA |
| P1 | 1,0069 | 0,5225 | 0,5350 | 1,0478 | 1,0941 | 0,5196 | 1,4802 | 0,9316 | 0,8077 |
| P2 | 0,6430 | 1,7459 | 0,9139 | 0,6088 | 2,0717 | 0,7050 | 0,5181 | 0,8775 | 0,6557 |
| P3 | 0,5212 | 0,8302 | 0,6503 | 0,8630 | 1,0577 | 0,4820 | 0,7628 | 0,9322 | 0,9160 |
| Average | 0,7237 | 1,0328 | 0,6997 | 0,8399 | 1,4078 | 0,5689 | 0,9204 | 0,9138 | 0,7931 |
| OSI-Mean (Dimensionless) | SMA | SMA | SMA | RRA | RRA | RRA | LRA | LRA | LRA |
| P1 | 0,0070 | 0,0084 | 0,0062 | 0,0061 | 0,0175 | 0,0067 | 0,0107 | 0,0073 | 0,0091 |
| P2 | 0,0038 | 0,0118 | 0,0095 | 0,0052 | 0,0129 | 0,0064 | 0,0050 | 0,0210 | 0,0045 |
| P3 | 0,0040 | 0,0073 | 0,0075 | 0,0033 | 0,0053 | 0,0098 | 0,0038 | 0,0057 | 0,0111 |
| Average | 0,0049 | 0,0092 | 0,0077 | 0,0048 | 0,0119 | 0,0076 | 0,0065 | 0,0114 | 0,0083 |
| TAWSS-Mean (Pa) | SMA | SMA | SMA | RRA | RRA | RRA | LRA | LRA | LRA |
| P1 | 2,0107 | 1,6635 | 3,3955 | 1,8828 | 0,9943 | 4,5400 | 1,7417 | 1,4609 | 2,8088 |
| P2 | 2,4245 | 1,1021 | 2,5005 | 2,7818 | 1,3462 | 3,0023 | 2,8822 | 2,1734 | 2,1953 |
| P3 | 2,6638 | 1,9726 | 3,0866 | 2,2412 | 2,7191 | 4,3557 | 2,4512 | 2,1275 | 2,1453 |
| Average | 2,3663 | 1,5794 | 2,9942 | 2,3019 | 1,6865 | 3,9660 | 2,3584 | 1,9206 | 2,3831 |
| Mean Flow Rate of the cardiac cycle (l / s) | SMA | SMA | SMA | RRA | RRA | RRA | LRA | LRA | LRA |
| P1 | 1,20E-05 | 7,05E-06 | 1,25E-05 | 7,77E-06 | 3,22E-06 | 8,78E-06 | 7,99E-06 | 4,79E-06 | 8,78E-06 |
| P2 | 4,53E-06 | 4,39E-06 | 8,67E-06 | 5,77E-06 | 1,59E-06 | 6,88E-06 | 4,78E-06 | 4,14E-06 | 4,14E-06 |
| P3 | 8,29E-06 | 3,92E-06 | 1,13E-05 | 5,04E-06 | 1,62E-06 | 6,65E-06 | 5,90E-06 | 2,51E-06 | 5,90E-06 |
| Average | 8,28E-06 | 5,12E-06 | 1,08E-05 | 6,20E-06 | 2,15E-06 | 7,44E-06 | 6,22E-06 | 3,81E-06 | 6,27E-06 |
| Pressure-MAP (Mean Arterial Pressure) (Pa) | SMA | SMA | SMA | RRA | RRA | RRA | LRA | LRA | LRA |
| P1 | 12448,0 | 12595,4 | 13042,2 | 12423,6 | 12607,7 | 12881,4 | 12436,0 | 12523,1 | 12937,9 |
| P2 | 12449,0 | 12528,7 | 12794,0 | 12425,3 | 12515,9 | 12691,8 | 12436,3 | 12573,5 | 12652,1 |
| P3 | 12447,6 | 12447,3 | 12903,6 | 12423,6 | 12423,3 | 12889,4 | 12436,0 | 12437,0 | 12986,0 |
| Average | 12448,2 | 12523,8 | 12913,2 | 12424,2 | 12515,6 | 12820,9 | 12436,1 | 12511,2 | 12858,7 |
| WSS-Mean at peak systole (Pa) | SMA | SMA | SMA | RRA | RRA | RRA | LRA | LRA | LRA |
| P1 | 15,75 | 11,40 | 23,92 | 12,61 | 7,96 | 31,86 | 13,09 | 9,94 | 26,29 |
| P2 | 21,32 | 14,95 | 22,98 | 20,66 | 12,23 | 21,89 | 22,79 | 15,52 | 19,16 |
| P3 | 20,58 | 27,57 | 26,27 | 18,05 | 19,52 | 33,24 | 19,60 | 18,70 | 26,67 |
| Average | 19,22 | 17,98 | 24,39 | 17,11 | 13,24 | 28,99 | 18,50 | 14,72 | 24,04 |
Table 3.
Percentage of flow reversal in visceral arteries of FEVAR, chEVAR and BEVAR cases.
| FEVAR cases | ||||
| Target vessel | Patient 1 (%) | Patient 2 (%) | Patient 3 (%) | Mean Value |
| SMA | 11.1834 | 24.7713 | 14.3677 | 16.7741 |
| LRA | 5.4558 | 19.0680 | 6.2420 | 10.2552 |
| RRA | 1.6034 | 10.3179 | 6.0401 | 5.9871 |
| ChEVAR cases | ||||
| Target vessel | Patient 1 (%) | Patient 2 (%) | Patient 3 (%) | Mean Value |
| SMA | 14.3160 | 29.9458 | 20.5075 | 21.5897 |
| LRA | 11.9259 | 21.2901 | 29.2485 | 20.8215 |
| RRA | 10.0024 | 36.8587 | 26.1691 | 24.3434 |
| BEVAR cases | ||||
| Target vessel | Patient 1 (%) | Patient 2 (%) | Patient 3 (%) | Mean Value |
| SMA | 3.6570 | 13.2076 | 12.8335 | 9.8994 |
| LRA | 2.2868 | 23.7582 | 60.3961 | 28.0514 |
| RRA | 2.2868 | 2.4989 | 10.3019 | 5.0292 |
Footnotes: SMA: superior mesenteric artery; LRA: left renal artery; RRA: right renal artery.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



