
Submitted:
21 January 2026
Posted:
22 January 2026
You are already at the latest version
Abstract
Background/Objectives: Anxiety and suicidal ideation are major mental health concerns during the perinatal period, impacting both mothers and newborns. While studies from South America address this issue, no prior systematic reviews have synthesized the findings. This review and meta-analysis aimed to explore the relationship between anxiety and suicidal ideation in perinatal women in South American countries. Methods: A systematic review and meta-analysis were registered in PROSPERO (CRD42025631849). Database searches were conducted in PubMed, Scopus, Web of Science, SciELO, and LILACS, including studies published up to December 2024, with no restrictions on year of publication. Study quality was evaluated using Joanna Briggs Institute tools. A random-effects model was used for the meta-analysis, following PRISMA guidelines. Results: Suicidal ideation was linked to 23 variables, such as age, race, depression, mother-infant bonding, violence, marital status, drug use, planned pregnancy, anxiety, low birth weight, and preterm birth. Anxiety was associated with 10 variables, including age, race, marital status, hyperglycemia, disabilities, eating habits, and mother-child relationship. The meta-analysis revealed a strong, significant association between suicidal ideation and violence, with affected women being 2.84 times more likely to report ideation. Conclusions: Violence and marital status emerged as key factors, reinforcing the need for screening and maternal mental health policies.
Keywords:
perinatal care
; pregnancy
; anxiety
; suicidal ideation
; South America
1. Introduction
Globally, suicide occupies a significant position among the leading causes of death, with a worldwide rate of 9 per 100,000 inhabitants [1]. This phenomenon is widely recognized as a serious public health problem, with devastating consequences for both individuals and societies, underscoring the need for effective prevention and psychosocial support strategies. In the period from 2000 to 2019, the Americas region saw a 17% increase in the suicide rate, in contrast to the global decrease of 36% [1].
The prevalence of this phenomenon is also significant during the perinatal period [2]. Many authors define the perinatal period depending on the cultural and social context, but a widely accepted definition worldwide is the period that refers to pregnancy and the 12 months after delivery [3]. This time interval is considered essential for monitoring the physical and mental health of women. In developed countries, suicide during the perinatal period accounts for a range of 5% to 44% of maternal deaths, with a diagnostic identification of only about 50% of affected cases [3]. In addition, there is still a paucity of specific data on the perinatal period. However, a survey carried out with 358 pregnant women revealed that 7.8% of them had suicidal ideation [4], pointing to the relevance of considering women’s mental health during pregnancy, especially in contexts with limited resources for adequate care.
Suicidal ideation is widely recognized as one of the main risk indicators for suicide, especially in the perinatal setting. The prevalence of this phenomenon varies significantly, depending on factors such as the type of study, the population analyzed, the assessment instruments used, and the specific stage of pregnancy. A meta-analysis of 71 studies estimated the prevalence at around 8% [5], while other research has indicated a range between 7% and 12% [2]. Factors such as age, education level, history of mental disorders, number of children, unplanned pregnancy, pregnancy complications, depression, domestic violence, socioeconomic difficulties, anxiety, marital status, history of abortion, sleep disorders, stress, newborn illnesses, immigrant status, and barriers to access to medical care have often been associated with suicidal ideation during this period [2,6,7]. In addition to being an important predictor of suicide, suicidal ideation in the perinatal period is linked to adverse outcomes for both mother and baby, such as increased risk of prematurity, low birth weight, congenital anomalies or respiratory distress syndrome among others. Furthermore, increases early fetal losses by up to six times, also compromising the mother-child bond and child development [6,8].
Another factor widely associated with suicide is the prevalence of anxiety in the perinatal period. Anxiety during the perinatal period is an emotional condition that can result in great physical and psychological pain, impacting both the mother and the newborn [9,10]. It is estimated, according to the World Health Organization (WHO), that between 21% and 25% of pregnant women worldwide have symptoms of anxiety. The prevalence is particularly worrying in low- and middle-income countries, where it affects approximately one in five pregnant women, compare to high-income countries where the proportion is one in 10 women [9]. However, most of them do not receive the necessary support, as less than 20% of health professionals examine mental health issues during prenatal care[10,11]. Throughout pregnancy, anxiety can cause hormonal changes, such as elevated cortisol and noradrenaline, which are linked to adverse outcomes, including low birth weight, early delivery, and problems with fetal development [12,13]. In the postpartum period, women with high levels of anxiety may face obstacles in interacting with their children, which can lead to emotional and behavioral problems in the child [14].
In the available literature, we identify reviews that explored anxiety in the perinatal period, although with some limitations that highlight the need for further investigations. Smythe et al. [15] In 2022, published a review aimed at examining the prevalence of perinatal mood disorders in both parents (mother and father). However, their anxiety-related results were based on only three studies conducted in Italy, Portugal, and Poland, restricting the generalizability of their review results. Similarly, de Araújo et al. [16] conducted an exploratory study and literature review on the subject, but with the limitation of using exclusively the Virtual Health Library (VHL) database for the period from 2010 to 2021. Although the research presented relevant data, the context of the countries included was not specified, which compromises the understanding of the geographic scope of the evidence. Moreover, a review published in 2007 analyzed the scientific production on anxiety in the perinatal population from 1998 to 2003, but considering the data from this investigation, the need for recent studies that broaden and deepen the understanding of anxiety in the perinatal period emerges [17].
Regarding suicidal ideation in the perinatal period, previous studies have limitations that justify further research. Meili Xiao et al. [5] included, in their review, databases in English and Chinese; Although they included 15 studies in the South American context, their review may have the limitation of not having identified studies published in Portuguese or Spanish. In addition, the review period was limited to August 31, 2020, which may not include enough research taking into account the post-pandemic period and its effect in mental health.
To our knowledge, we did not find systematic reviews in the literature that aimed to investigate anxiety and suicidal ideation exclusively in the context of South America, which is justified by the high prevalence of these two variables associated with this population. For all these reasons, this systematic review aims to describe the existing evidence on anxiety and suicidal ideation in women during the perinatal and postpartum period in South America.
2. Materials and Methods
2.1. Design
Systematic review with narrative synthesis and meta-analysis was conducted after prospective registration (PROSPERO ID: CRD42025631849) to determine the available knowledge on anxiety and suicidal ideation in women in the perinatal period, based on original studies, following the recommendations of the Cochrane Manual of Systematic Reviews [18] and the PRISMA declaration [19]. In terms of period, we adopted the criteria widely used worldwide, which refer to the period from the puerperium to pregnancy and to the 12 months after delivery [3].
2.2. Search Strategy
The search covered the PubMed, Scopus, Scielo, Virtual Health Library (LILACS, BDENF - Nursing, MEDLINE, CVSP - Brazil, Sec. Est. Saúde SP, Index Psicología - Revistas, IBECS, Coleciona SUS, HomeoIndex - Homeopathy, Multimedia Resources, PAHO-IRIS, PIE) and Google Scholar databases without the application of language filters or time restrictions until December 2024. In addition, a complementary search was carried out in the bibliographic references of the selected articles. Google Scholar was included as a complementary source to increase the sensitivity of the search and to identify studies from South America that may not be indexed in traditional databases. Although no time limits were imposed, older studies were retained due to the scarcity of research conducted in South America and their continued relevance to perinatal mental health in the region. The search strategies used are detailed in Chart 1.
2.3. Selection of Studies
The inclusion criteria were defined as original articles that investigated the variables of anxiety and suicidal ideation in the population of pregnant women and women in the puerperium period (pregnancy and up to 12 months after delivery), belonging to South American countries.
2.4. Data Extraction
The data were extracted from the studies and organized in a previously prepared Excel spreadsheet. The variables collected included the names of the authors, year and country of publication, study population, study design, sample size and type, measurement instrument, study variable, type of measurement, and the results obtained. These data were collected independently by two researchers; In case of divergence, a joint analysis process was carried out until a consensus was reached. The articles were imported into the EndNote© reference manager for evaluation and selection.
2.5. Assessment of the Quality of the Included Studies
The criteria proposed by Boyle were considered [20] y Viswanathan et al. [21] to assess methodological quality: selection bias, considered controlled when the sample was probabilistic; classification bias, related to the validity and reliability of the instruments used (including content validity and internal consistency assessed by Cronbach’s alpha); and confounding bias, considered under control when the confounding variables were properly considered.
A variable is considered to be controlled for confounding bias when methods that ensure comparability between the groups analyzed are used. This can be done through techniques such as stratification, pairing, or the use of propensity scores. Additionally, control can be achieved through statistical adjustments, such as stratified analyses or multivariate models.
The evaluation of the quality criteria of the studies was carried out independently by two authors, and disagreements were resolved by consensus.
2.6. Data Analysis
The data were grouped and synthesized in a descriptive way. In the first stage of the analysis, the articles were read in full to obtain a general understanding of the results. Then, in the second stage, the information was organized in tables and the independent variables associated with anxiety and suicidal ideation were listed. It was observed that the included studies presented differences in the methods of data collection and in the statistics used for analysis. The heterogeneity in the measurements and results of the studies made it impossible to use a statistical method to combine the data from all the included articles. Thus, it was possible to perform a total of 03 meta-analyses for the suicidal ideation variable. Different observational designs (cross-sectional, cohort, and longitudinal studies) were included to provide a comprehensive overview of the available evidence. However, causal inferences were not assumed, and findings were synthesized narratively when methodological heterogeneity precluded quantitative pooling.
To perform the meta-analysis, a random-effects model was adopted, as recommended by Cooper et al. [22], with the aim of generalizing the findings to a broader population of family caregivers. All subsequent analytical procedures were conducted using the Comprehensive Meta-Analysis software, version 3.
Heterogeneity between the studies was investigated using the Q test (significance level of 0.1) in order to assess the homogeneity of the effect sizes. Additionally, the I² index, proposed by Higgins, was used [23] to estimate the proportion of total variability that cannot be attributed to chance. This index ranges from 0% (absence of heterogeneity) to 100% (maximum heterogeneity), and is interpreted as follows: 25% indicates low heterogeneity, 50% indicates moderate and 75% high heterogeneity.
To identify the presence of publication bias, the recommendations of Guyatt et al. were followed. [24] using different approaches: visual inspection of the symmetry of the funnel plot, Egger et al. test. [25] and the Trim and Fill correction method [26]. The Egger test evaluates the symmetry of the funnel plot through a regression between the precision and the size of the effect, considering the null hypothesis that the slope is equal to zero (alpha = 0.1). The Trim and Fill method estimates the adjusted combined effect by simulating a scenario in which publication bias is absent.
3. Results
3.1. Description of Search Results
The search strategies in our review resulted in the identification of 1.742 studies. Of these, 365 were excluded because they were duplicates. Among the remaining 1,377 articles, 978 were eliminated because they were not related to the topic, 289 because they did not address the target population, 27 because they dealt with populations from other continents, and 58 because they were not original studies. After this initial screening, 25 articles were selected for full reading, of which 21 were included in the final sample. The others were excluded because they did not meet the previously defined criteria. A detailed flowchart of the process of selection, exclusion, and inclusion of studies, adapted from the PRISMA model, is presented in Figure 1.
3.2. General Characteristics of the Included Studies
In our review we included a total of 21 studies [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47]. The total sample of participants was 26.962 women.
The included articles were published between 2007 and 2024, with 12 articles of Brazilian origin [27,28,29,30,31,32,36,39,41,42,44,45] , 8 from Peru [33,34,35,38,40,43,46,47] and 1 from Paraguay [37].
About the types of research 13 are cross-sectional studies [27,28,29,30,31,32,33,34,36,37,38,42,47], 7 cohort [35,40,41,43,44,45,46] and 1 longitudinal prospective [39].
A total of 20 instruments were presented that differed in the data collection methodology of the studies, the most used being the Patient Health Questionnaire (PHQ-9) present in studies in Brazil and Peru [29,31,33,34,35,40,46,47], mostly used to assess suicidal ideation.
The State-Trait Anxiety Inventory was the second most common instrument used in the studies [30,39,44,45]. Next, the Beck Suicidal Ideation Scale (BSI) instruments [27,32] predominant in a Brazilian study and the Self-Report Questionnaire-20 (SRQ-20) used in Paraguay and Brazil [36,37], and the General Anxiety Disorder test (GAD-7) [42,43], being the most directed instrument for assessing the level of anxiety and with prevalence in more recent studies. Table 1 presents the main characteristics of the studies included in our review.
According to the data in Table 1, the included studies related the variable of suicidal ideation with 23 variables: age, race/color, depression, mother-baby bond, postpartum depression, violence by a general intimate partner, marital status, use of licit and illicit drugs, planned pregnancy, anxiety, violence (physical abuse), violence (sexual abuse), migraine, sleep quality, sleep quality and depression, low infant birth weight, small for gestational age (below 10th percentile), preterm birth, women currently pregnant, violence (childhood abuse), violence (intimate partner), metabolic markers (choline), metabolic markers (phenylanalin).
Regarding the anxiety variable, the studies included in our review show that this variable was related to 10 variables: age, race/color, marital status, mild hyperglycemia, attachment to parents (lack of attention), mother-child relationship, disabilities (daily activities, social participation, education, work and personal care), prematurity, and eating habits.
3.3. Description of the Quality of the Studies
Table 2 presents the results of the evaluation of the methodological quality of the 21 studies included. It was found that only 3 studies adopted probabilistic sampling (14.2%). All included articles met the criteria for controlling for classification bias and confounding
3.4. Anxiety in the Perinatal Period
Of the 21 articles included in our review, 8 studied the relationship between anxiety and different variables, and were conducted in countries such as Brazil [28,30,39,41,42,44,45] and Peru [43], developed in the period from 2007 to 2024. The sample of publications ranged from 101 to 2068 participants, with a total of 5,566 women analyzed in the studies focused on anxiety. Regarding the sample, six used the non-probabilistic [30,39,41,42,43,45] and two probabilistic [28,44]. Regarding the participants of the studies, pregnant women were addressed in five publications [28,30,39,43,44], pregnant and postpartum women in two [42,45] and postpartum women in a [41].
The Faisal-Cury study [30] showed a statistical relationship between anxiety and the variables age, race/color, and marital status in a population of 432 pregnant women. Among these, the relationship between anxiety and age identified that older women (30 to 44 years) are less likely to have anxiety than women aged 14 to 19 years (OR: 0.46; CI: 0.23; 0.92). Regarding the relationship between anxiety and race/color, no relationship was found between women who declare themselves “other” compared to those who declare themselves white (OR: 1.57; CI: 0.94; 2.62). And regarding anxiety and marital status, statistically women who reported another marital status were 2.66 times more likely to have anxiety symptoms than married women (CI: 1.37; 5.14).
A prospective longitudinal study with 101 pregnant women [39], identified that anxiety and mild hyperglycemia during pregnancy did not have a statistically significant association in the groups of hyperglycemic and normoglycemic women.
The Matos et al. [28] analyzed the relationship between bonding with parents and anxiety in a sample of 870 pregnant women. The authors noted that pregnant women who reported a lack of maternal care were 2.08 times more likely to have anxiety disorders than those who reported adequate maternal care
Other Cohort Research [43] with 2068 pregnant women showed that women who reported stress-related sleep disorders are 2.50 times more likely to have anxiety. Prematurity was not statistically associated with anxiety in the groups of women who had premature children (p= 0.55) [44].
Other research [42] with 185 pregnant and puerperal women, estimated a high adherence to the common Brazilian pattern of eating habits (β = -1.200, 95% CI -2.220 to -0.181) and to healthy patterns (β = -1.290, 95% CI -2.438 to -0.134) indicating a negative association with anxiety symptom scores throughout the study period. Regarding the factors related to the factors of functional disability of daily activities (social participation, education, work and personal care), there was no significance [42].
3.5. Suicidal Ideation in the Perinatal Period
Of the 21 studies included, 13 showed some relationship with suicidal ideation in our reference population. The research was conducted in countries such as Peru [33,34,35,38,40,46,47], followed by Brazil [27,30,31,32,36] and Paraguay [37].
The target population addressed was 11 publications with pregnant women [27,29,32,33,34,35,38,40,46,47], one with women in the postpartum period [37] and one that included pregnant and postpartum women [31], totaling a population of 21,396 women. Samples vary considerably in size, ranging from studies with only 100 participants to investigations with more than 6,500 women, with a total of 21. 396 women analyzed in studies focused on anxiety
Non-probability sampling was used in 12 [29,31,32,33,34,35,36,37,38,40,46,47] and probabilistic in one [27].
The variables investigated related to suicidal ideation are diverse. Sociodemographic factors such as age were mentioned in five articles [29,31,36,37,38] covering a total of 10,558 women, marital status in four studies, and a total of 9,789 women [27,36,37,38] and race/color in two [29,38] with an exhibition of 3,189 women. Among these five studies cited above that include a direct relationship between suicidal ideation and age, two of these [29,37] showed significance and prevalence that younger pregnant and puerperal women (15 to 19 years) have a higher risk of suicidal ideations compared to women aged 40 to 44 years.
Of the four studies that evaluated the relationship between marital status and suicidal ideation, three of these [27,36,37] showed higher probabilities of suicidal ideation in single women than in married women, ranging from 1.87 (CI: 1.42; 2.47) to 2.42 (CI: 1.33; 4.39) the odds of suicidal ideation. Regarding race/color of the three studies that bring this variable, only one [29] showed statistical significance, women who identify themselves as non-white are 1.53 times more likely to have suicidal ideations (CI: 1.26; 1.85).
Perinatal depression appeared in six studies as one of the variables most strongly associated with suicidal ideation, with a total of 6,136 women in the sample, evidencing the close relationship between psychological distress and suicidal ideation [29,31,32,33,34,46]. When depression is related to suicidal ideation in the perinatal period, a study conducted in Peru [46] From a population of 1,517 women, it identified that 51% of women with suicidal ideation were depressed. And this relationship has been confirmed in other studies [29,32,33], identifying that pregnant women with depression are 2.44 to 8.12 times more likely to have suicidal ideations. Even so, a study carried out with women in the puerperal period associates that those suffering from depression are 13.60 times more likely to have suicidal ideations [31]. In addition, the study by Freitas et al. [32] concluded that anxiety is also associated with a higher frequency of suicidal ideation (P value = 0.006).
Exposure to violence was addressed in different publications, with intimate partner violence in two [27,38], child abuse in two other studies [38,47] and sexual and physical violence in a study [32]. Fonseca-Machado’s research [27], showed that women who have suffered some type of intimate partner violence are 6.29 (CI: 2.34; 16.9) more likely to report suicidal ideation. Thus, women who suffered some type of abuse in childhood were 2.57 (CI: 2.08; 3.17) more likely to report suicidal ideation during pregnancy [38].
Factors related to lifestyle and healthy habits were also mentioned in publications, such as the use of drugs and other substances (OR= 0.58; CI: 0.15; 2,24) [27], and the absence of gestational planning [27] (OR= 0.74; CI: 0.24; 2,33), but did not obtain significance regarding the relationship with suicidal ideation.
On the other hand, low sleep quality (OR= 4.81; CI: 3.19; 7.24) was significant, and it was identified that pregnant women who have worse sleep quality are 4.81% more likely to have suicidal ideations. Still, in this same study, it states that women with poorer sleep quality and depression are 13.60 times more likely to have suicidal ideations [34].
In a study by Friedman et al. [33], the relationship of women with migraine is highlighted and states that they had more than twice the probability of suicidal ideation (OR= 2.17; CI: 1.80; 2.61). In addition, metabolic markers such as choline and phenylalanine (choline OR: 0.29; CI: 0.11; 0.81 y phenylalanine OR= 0.41; CI: 0.19; 0.91) demonstrated a greater protective association in the central nervous system and fetal development, and also affirmed the direct binding of dopamine and norepinephrine, essential mood neurotransmitters [40], demonstrate relevance in their relationships with suicidal ideation.
One study also addressed aspects of mother-infant bonding [31] and obstetric outcomes, such as preterm birth, low birth weight, and intrauterine growth restriction [35] associated with suicidal ideation. Participants with suicidal ideation were nearly four times more likely to give birth to a small-for-gestational-age baby (OR: 3.73, CI: 1.59; 8.74) [35].
Another relevant factor that shows statistical significance is that women in the puerperal period who have impairments in the construction of mother-child bonding are 6.57 times more likely to have suicidal ideations (OR: 6.57; CI: 2.37; 18,20) [31].
3.6. Results of the Meta-Analyses
Meta-analyses were conducted to examine the relationship between suicidal ideation and two sociodemographic variables: age and marital status, including only studies with adequate methodological quality. In both cases, a positive but non-significant association was observed. The results were consistent, with low heterogeneity and no indication of publication bias (Table 3 and supplementary document). On the other hand, the meta-analysis on exposure to violence showed a statistically significant positive association.
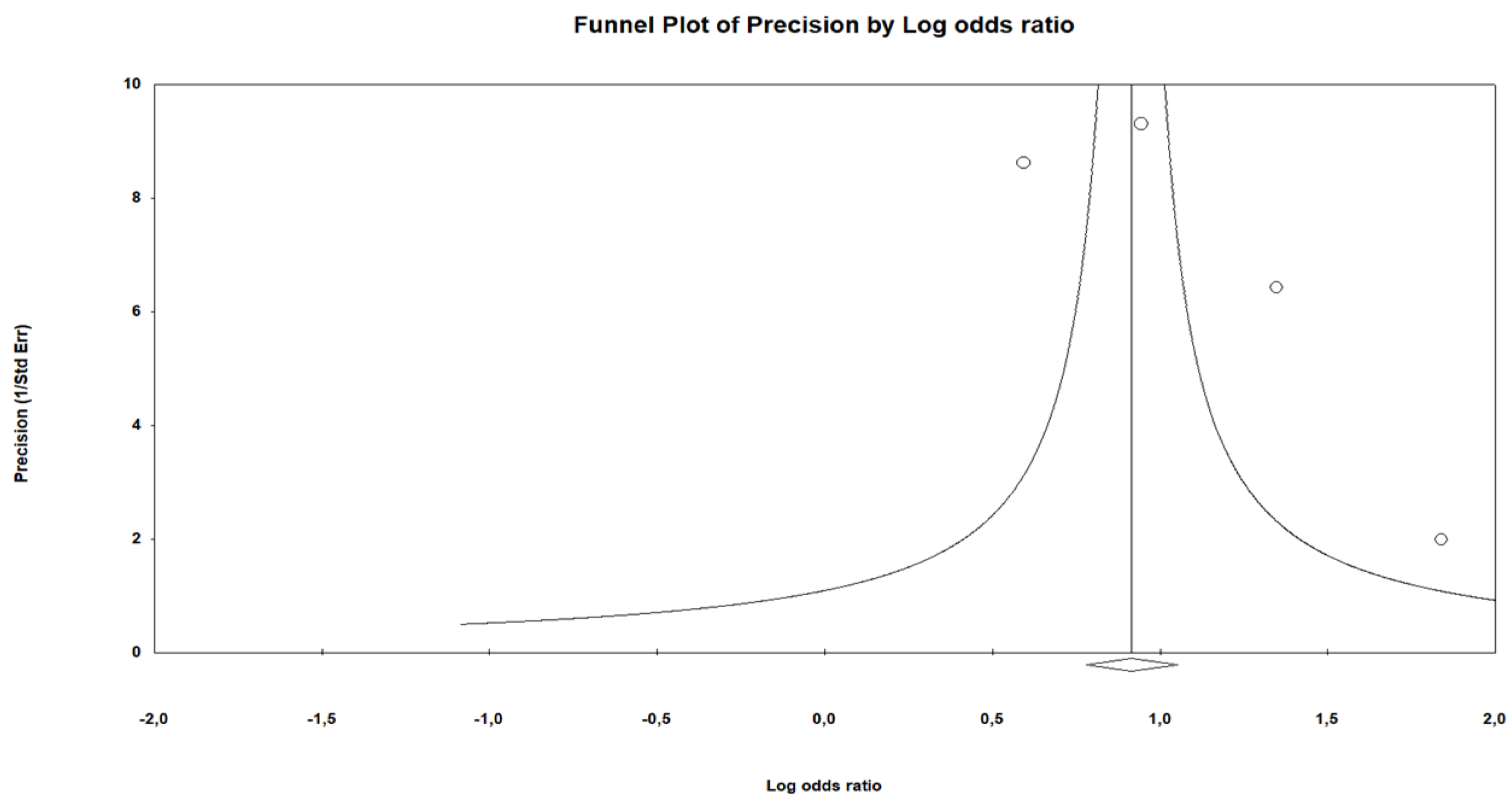
3.6.1. Results of the Meta-Analysis: Suicidal Ideation and Violence
A meta-analysis was carried out to evaluate the association between suicidal ideation and experience of violence, selecting studies with proven methodological quality. The results showed a significant positive association, with a large magnitude of effect. The average number of participants per study was 1,376 (total N = 5,504; K = 4). All studies indicated a positive association, with low heterogeneity (I² = 24.50), demonstrating data consistency. The sensitivity analysis revealed a slight variation (12.28%), which did not compromise the overall robustness. Despite the asymmetry in the funnel graph, the Egger test (p = 0.394) did not show relevant bias. Although Egger’s test did not indicate publication bias, this test is known to be underpowered when fewer than 10 studies are included and should therefore be interpreted with caution. The Trim and Fill method minimally adjusted the effect, with limited variation (12.28%), suggesting a reduced impact of possible biases in the estimate. Women who have suffered some type of violence during pregnancy or the postpartum period are 2.84 times more likely to have suicidal ideations. Given the small number of studies included in each meta-analysis, the findings should be interpreted as exploratory rather than definitive.
Figure 2.
Funnel chart Suicidal ideation and violence.
4. Discussion
Our results describe the available evidence on the variables of anxiety and suicidal ideation in perinatal and postpartum women in South America, constituting, to our knowledge, the first systematic review on this topic in the region. On the one hand, suicidal ideation was related to 23 distinct variables, including age, race/color, depression, mother-infant bonding, postpartum depression, violence (by a general intimate partner, physical and sexual abuse, and childhood abuse), marital status, use of licit and illicit drugs, planned pregnancy, anxiety, migraine, sleep quality, sleep quality, depression, low infant birth weight, small for gestational age , preterm birth, currently pregnant women, metabolic markers (choline and phenylanalin). On the other hand, anxiety was associated with 10 variables, including age, race/color, marital status, mild hyperglycemia, attachment to parents (lack of attention), mother-child relationship, disabilities impact daily activities, social participation, education, work, and personal care, prematurity, and eating habits. In addition, it was possible to perform a meta-analysis for the variable suicidal ideation and its relationship with age, violence, and marital status.
Although the international literature consistently points to factors such as depression, domestic violence, unplanned pregnancies and socioeconomic difficulties as the main predictors of suicidal ideation in the perinatal period [48,49], our findings on the perinatal and postpartum period in women in South America show a more complex picture, involving 23 variables, some of which have been less explored in previous studies, such as metabolic markers (choline and phenylalanine), migraine, or sleep quality. Our findings may indicate that, beyond the well-known psychosocial factors, biological and clinical elements could also significantly contribute to the development of suicidal ideation. Furthermore, the study emphasizes the link between suicidal ideation not only with gestational depression but also with postpartum depression and the mother-baby bond, highlighting an emotional aspect that remains underexplored in most quantitative research. [50]. The inclusion of factors such as low birth weight, preterm birth, and intrauterine growth restriction also reinforces the link between maternal distress and adverse obstetric outcomes, as has been suggested in previous studies [51], but rarely investigated in South American countries. In this sense, our study broadens the scope of variables associated with suicidal ideation in this context, pointing to the need for integrated approaches that are sensitive to the regional context
The association between anxiety and attachment to parents in childhood (lack of attention) also brings to light the influence of early adverse factors and experiences on perinatal mental health, in line with the findings of Racine et al. [52]. Unlike other studies that tend to focus on more traditional psychosocial variables, such as social support or education level, our study revealed a greater diversity of factors, including clinical and functional conditions. This may reflect the specificities of the South American context regarding the greater heterogeneity of the instruments and criteria used in the included studies. Thus, our study reinforces the problem of creating public policies aimed at the early detection and follow-up of perinatal anxiety in South American countries, incorporating a biopsychosocial and intersectoral view.
Although some previous reviews have already addressed anxiety and suicidal ideation in the perinatal period, they have limitations that justify the need for new, broader and contextualized studies. The review by Smythe et al. [15], examined the prevalence of perinatal mood disorders in both parents, but the data on anxiety were based on only three studies With regard to suicidal ideation, the review by Meili Xiao et al. [5] included studies from South America, but can be considered outdated currently. In view of these gaps, our study represents an advance in updating and expanding the scope of the search, considering multiple databases, without language restrictions, and with a specific focus on South America, providing a more comprehensive, current, and culturally contextualized view of the factors associated with anxiety and suicidal ideation in the perinatal period.
The results of the present meta-analysis reveal relevant evidence on factors associated with suicidal ideation in the perinatal period. Although the number of studies included in each analysis limits the possibility of extrapolation to other contexts, this is, to date, the first study with a specific focus on this topic in the region. The analyses showed positive associations between suicidal ideation and different sociodemographic variables, such as marital status and age, although these did not reach statistical significance. However, the association between suicidal ideation and experience of violence was statistically significant and of high magnitude, with consistent results among the included studies. Women who experienced any form of violence during pregnancy or postpartum were nearly three times more likely to develop suicidal thoughts compared to those who did not face such violence. These findings highlight the critical need to address violence as a key risk factor in safeguarding the mental health of women throughout pregnancy and the postpartum period. Despite the relevance of our results, this systematic review with meta-analyses has limitations that should be considered. First, the small number of studies included in some analyses made it difficult to generalize the findings, especially for different sociocultural contexts. In addition, there was methodological heterogeneity among the studies, both in relation to the instruments used to assess suicidal ideation and anxiety, as well as to the sample designs and inclusion criteria. The diversity in the time frames and in the definitions of the variables may have influenced the effect estimates. Another relevant limitation refers to the predominance of cross-sectional descriptive studies, which prevents the establishment of causal relationships. While the predominance of studies conducted in South American countries may initially appear to limit the generalizability of the findings to other regions, this focus constitutes a distinctive strength of our research. Given that South America remains underrepresented in international reviews on suicidal ideation and anxiety, our emphasis on this region addresses a significant gap in the literature. This geographical focus aligns precisely with the primary objective of this systematic review: to deepen the understanding of suicidal ideation and anxiety within the South American perinatal context. By providing contextually relevant evidence, our study offers valuable insights that can inform region-specific interventions and policies, thereby advancing the body of knowledge in this underserved area. Building upon the current findings, future research should aim to enhance methodological rigor within South American contexts by employing longitudinal designs and representative sampling strategies. Such approaches would facilitate a more comprehensive understanding of the complex factors associated with suicidal ideation and anxiety during the perinatal period.
From a clinical perspective, this systematic review with meta-analyses underscores the imperative to integrate routine screening for suicidal ideation, anxiety, and related risk factors such as violence into standard maternal healthcare practices. Equipping primary care providers, particularly nurses, with specialized training in sensitive assessment and intervention techniques is crucial for fostering active listening and ensuring timely referrals. Moreover, adherence to evidence-based clinical protocols, implementation of violence prevention measures, and the reinforcement of psychosocial support networks are vital strategies that can substantially mitigate adverse maternal mental health outcomes
5. Conclusions
This review examines perinatal and postpartum suicidal ideation and anxiety in South American women, identifying marital status as key associated factor. Violence emerges as a significant risk, increasing suicidal ideation nearly threefold, and emphasizes the need for screening and policy efforts in maternal mental health.
Author Contributions
Conceptualization, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; methodology, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; software, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; validation, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; formal analysis, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; investigation, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; resources, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; data curation, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; writing—original draft preparation, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; writing—review and editing, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; visualization, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; supervision, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V.; project administration, H.S.D., D.D.J.P., E.L.A., M.R., D.L.R. and S.M.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
NA.
Informed Consent Statement
NA.
Data Availability Statement
Dataset available on request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. One in 100 deaths is by suicide. Available online: https://www.who.int/es/news/item/17-06-2021-one-in-100-deaths-is-by-suicide](https://www.who.int/es/news/item/17-06-2021-one-in-100-deaths-is-by-suicide (accessed on 30 Jun 2025).
- Dudeney, E.; Coates, R.; Ayers, S.; McCabe, R. Measures of suicidality in perinatal women: A systematic review. J. Affect. Disord. 2023, 324, 210–231. [Google Scholar] [CrossRef] [PubMed]
- England, N.; Improvement, N.; England, NCCfMH. The perinatal mental health care pathways. 2018. [Google Scholar]
- Fonseca-Machado, M.d.O.; Alves, L.C.; Haas, V.J.; Monteiro, J.C.d.S.; Gomes-Sponholz, F. Sob a sombra da maternidade: gravidez, ideação suicida e violência por parceiro íntimo. Rev. Psiquiatr. do Rio Grande do Sul 2015, 37, 258–264. [Google Scholar]
- Xiao, M.; Hu, Y.; Huang, S.; Wang, G.; Zhao, J.; Lei, J. Prevalence of suicidal ideation in pregnancy and the postpartum: A systematic review and meta-analysis. J. Affect. Disord. 2022, 296, 322–336. [Google Scholar] [CrossRef]
- Bright, A.-M.; Doody, O.; Tuohy, T. Women with perinatal suicidal ideation–A scoping review of the biopsychosocial risk factors to inform health service provision and research. PLoS ONE 2022, 17(9), e0274862. [Google Scholar] [CrossRef]
- Gabriel, J.C.; Mendes, M.L.R. Ideação suicida: fatores de risco no período perinatal. Rev. Bras. Enferm. 2023, 12 (Suppl. 3), 37–43. [Google Scholar]
- Gelaye, B.; Kajeepeta, S.; Williams, M.A. Suicidal ideation in pregnancy: an epidemiologic review. Ann. Glob. Health 2016, 19, 741–751. [Google Scholar] [CrossRef]
- World Health Organization. Guide for integration of perinatal mental health in maternal and child health services; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Juarez Padilla, J.; Lara-Cinisomo, S.; Navarrete, L.; Lara, M.A. Perinatal anxiety symptoms: Rates and risk factors in Mexican women. Int. J. Environ. Res. Public Health 2021, 18(1), 82. [Google Scholar] [CrossRef]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.R.; Fawcett, J.M. The prevalence of anxiety disorders during pregnancy and the postpartum period: a multivariate Bayesian meta-analysis. J. Clin. Psychol. 2019, 80(4), 1181. [Google Scholar] [CrossRef]
- DiPietro, J.A.; Hilton, S.C.; Hawkins, M.; Costigan, K.A.; Pressman, E.K. Maternal stress and affect influence fetal neurobehavioral development. Dev. Psychobiol. 2002, 38(5), 659. [Google Scholar] [CrossRef]
- Grigoriadis, S.; Graves, L.; Peer, M.; Mamisashvili, L.; Tomlinson, G.; Vigod, S.N.; et al. Maternal anxiety during pregnancy and the association with adverse perinatal outcomes: systematic review and meta-analysis. 2018, 79(5), 813. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Prenatal anxiety effects: a review. Infant Behav. Dev. 2017, 49, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Smythe, K.L.; Petersen, I.; Schartau, P. Prevalence of perinatal depression and anxiety in both parents: a systematic review and meta-analysis. J. Neonatal Nurs. 2022, 5(6), e2218969. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, A.L.S.; Xavier, J.E.C.A.; Lima, M.I.F.; Jacó, A.P.; Araújo, M.T.C.; Santos, P.Í.O.S.; et al. Ansiedade na fase perinatal: revisão de literatura. J. Enferm. Cent. Afr. 2021, 10(15), e566101523521. [Google Scholar] [CrossRef]
- Correia, L.L.; Linhares, M.B.M. Ansiedad maternal en el período prenatal y postnatal: revisión de la literatura. Rev. Lat. Am. Enferm. 2007, 15, 677–683. [Google Scholar] [CrossRef]
- Centro Cochrane Iberoamericano. Manual Cochrane de revisiones sistemáticas de intervenciones, versión 5.1.0 [actualizada en marzo de 2011]; Centro Cochrane Iberoamericano: Barcelona, 2012. [Google Scholar]
- Page, M.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10(1), 89. [Google Scholar] [CrossRef]
- Michael, H.B. Guidelines for evaluating prevalence studies. Evid. Based Ment. Health 1998, 1(2). [Google Scholar]
- Viswanathan, M.; Berkman, N.D.; Dryden, D.M.; Hartling, L. Assessing risk of bias and confounding in observational studies of interventions or exposures: further development of the RTI item bank. 2013. [Google Scholar]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis; Russell Sage Foundation: New York, USA, 2019. [Google Scholar]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Measuring inconsistency in meta-analyses. BMJ (Clin. Res. Ed.) 2003, 327(7414), 557–560. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Santesso, N.; Helfand, M.; Vist, G.; Kunz, R.; et al. GRADE guidelines: 12. Preparing summary of findings tables—binary outcomes. 2013, 66(2), 158–172. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315(7109), 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56(2), 455–463. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Machado, M.; Alves, L.; Haas, V.; Monteiro, J.; Gomes-Sponholz, F. Under the shadow of maternity: pregnancy, suicidal ideation, and intimate partner violence. Rev. Psiquiatr. do Rio Grande do Sul 2015, 37(4-5), 258–264. [Google Scholar]
- de Matos, M.B.; Scholl, C.C.; Trettim, J.P.; Molina, M.L.; Soares, M.C.; Coelho, F.T.; et al. The perception of parental bonding in pregnant adolescents and its association with generalized anxiety disorder. 2018, 54, 51–56. [Google Scholar] [CrossRef]
- Faisal-Cury, A.; Levy, R.B.; Matijasevich, A.J.; Lara, M.C. The relationship between mother–child bonding impairment and suicidal ideation in São Paulo, Brazil. 2021, 25, 706–714. [Google Scholar] [CrossRef]
- Faisal-Cury, A.; Rossi Menezes, P. Prevalence of anxiety and depression during pregnancy in a private setting sample. Ann. Glob. Health 2007, 10, 25–32. [Google Scholar] [CrossRef]
- Faisal-Cury, A.; Tabb, K.M.; Maruyama, J.M.; Matijasevich, A. Depression moderates the association between pregnancy and suicidal ideation among pregnant and non-pregnant reproductive age women in Brazil. Front. Psychiatry 2022, 13, 1029048. [Google Scholar] [CrossRef]
- Freitas, G.V.S.d.; Botega, N.J. Gravidez na adolescência: prevalência de depressão, ansiedade e ideação suicida. Rev. Assoc. Med. Bras. 2002, 48, 245–249. [Google Scholar]
- Friedman, L.E.; Gelaye, B.; Rondon, M.B.; Sanchez, S.E.; Peterlin, B.L.; Williams, M.A.; et al. Association of migraine headaches with suicidal ideation among pregnant women in Lima, Peru. J. Headache Pain 2016, 56(4), 741–749. [Google Scholar]
- Gelaye, B.; Addae, G.; Neway, B.; Larrabure-Torrealva, G.T.; Qiu, C.; Stoner, L.; et al. Poor sleep quality, antepartum depression and suicidal ideation among pregnant women. 2017, 209, 195–200. [Google Scholar]
- Gelaye, B.; Domingue, A.; Rebelo, F.; Friedman, L.E.; Qiu, C.; Sanchez, S.E.; et al. Association of antepartum suicidal ideation during the third trimester with infant birth weight and gestational age at delivery. 2019, 24(2), 127–136. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Faisal-Cury, A.; Chan, Y.-F.; Tabb, K.; Katon, W.; Menezes, P.R. Suicidal ideation during pregnancy: prevalence and associated factors among low-income women in São Paulo, Brazil. Ann. Glob. Health 2012, 15, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Ishida, K.; Stupp, P.; Serbanescu, F.; Tullo, E. Perinatal risk for common mental disorders and suicidal ideation among women in Paraguay. Int. J. Gynaecol. Obstet. 2010, 110(3), 235–240. [Google Scholar] [CrossRef] [PubMed]
- Levey, E.J.; Rondon, M.B.; Sanchez, S.; Zhong, Q.-Y.; Williams, M.A.; Gelaye, B. Suicide risk assessment: examining transitions in suicidal behaviors among pregnant women in Perú. 2019, 22, 65–73. [Google Scholar] [CrossRef]
- Marquesim, N.A.Q.; Cavassini, A.C.M.; Morceli, G.; Magalhães, C.G.; Rudge, M.V.C.; Calderon, I.d.M.P.; et al. Depression and anxiety in pregnant women with diabetes or mild hyperglycemia. 2016, 293, 833–837. [Google Scholar] [CrossRef]
- Mitro, S.D.; Larrabure-Torrealva, G.T.; Sanchez, S.E.; Molsberry, S.A.; Williams, M.A.; Clish, C.; et al. Metabolomic markers of antepartum depression and suicidal ideation. 2019, 262, 422. [Google Scholar] [CrossRef]
- Morais, A.O.d.S.; Simões, V.M.F.; Rodrigues, L.d.S.; Batista, R.F.L.; Lamy, Z.C.; Carvalho, C.A.d.; et al. Maternal depressive symptoms and anxiety and interference in the mother/child relationship based on a prenatal cohort: an approach with structural equations modeling. 2017, 33, e00032016. [Google Scholar]
- Pabon, S.; Guida, J.P.; Lamus, M.N.; Charles, C.M.; Parpinelli, M.A.; Escobar, M.F.; et al. Impacts of childbirth on anxiety, disability, and depression: results from a Brazilian cohort. 2024, 45(9), 1034–1047. [Google Scholar] [CrossRef]
- Sanchez, S.E.; Friedman, L.E.; Rondon, M.B.; Drake, C.L.; Williams, M.A.; Gelaye, B. Association of stress-related sleep disturbance with psychiatric symptoms among pregnant women. 2020, 70, 27–32. [Google Scholar] [CrossRef]
- Soares, M.C.; de Matos, M.B.; da Cunha, G.K.; Leite, C.F.; Caruccio, H.S.; Trettim, J.P.; et al. Suicide risk and prematurity: A study with pregnant adolescents. 2021, 133, 125–133. [Google Scholar] [CrossRef]
- Vilela, A.A.F.; de J.P. Pinto, T.; Rebelo, F.; Benaim, C.; Lepsch, J.; Dias-Silva, C.H.; et al. Association of prepregnancy dietary patterns and anxiety symptoms from midpregnancy to early postpartum in a prospective cohort of Brazilian women. 2015, 115(10), 1626–1635. [Google Scholar]
- Zhong, Q.-Y.; Gelaye, B.; Rondon, M.B.; Sánchez, S.E.; Simon, G.E.; Henderson, D.C.; et al. Using the Patient Health Questionnaire (PHQ-9) and the Edinburgh Postnatal Depression Scale (EPDS) to assess suicidal ideation among pregnant women in Lima, Peru. 2015, 18, 783–792. [Google Scholar]
- Zhong, Q.-Y.; Wells, A.; Rondon, M.B.; Williams, M.A.; Barrios, Y.V.; Sanchez, S.E.; et al. Childhood abuse and suicidal ideation in a cohort of pregnant Peruvian women. 2016, 215(4), 501.e1–501.e8. [Google Scholar]
- Oates, M. Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. BMJ 2003, 67(1), 219–229. [Google Scholar] [CrossRef]
- Lancaster, C.A.; Gold, K.J.; Flynn, H.A.; Yoo, H.; Marcus, S.M.; Davis, M.M.; et al. Risk factors for depressive symptoms during pregnancy: a systematic review. Am. J. Obstet. Gynecol. 2010, 202(1), 5–14. [Google Scholar] [CrossRef]
- Howard, L.M.; Molyneaux, E.; Dennis, C.-L.; Rochat, T.; Stein, A.; Milgrom, J. Non-psychotic mental disorders in the perinatal period. Lancet 2014, 384(9956), 1775–1788. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, V.; Pearson, J.L.; Colpe, L. Prevalence of suicidality during pregnancy and the postpartum. Arch. Womens Ment. Health 2005, 8(2), 77–87. [Google Scholar]
- Racine, N.; Plamondon, A.; Madigan, S.; McDonald, S.; Tough, S.J.P. Maternal adverse childhood experiences and infant development. 2018, 141(4). [Google Scholar] [CrossRef] [PubMed]
Chart 1.
Search strategies employed.
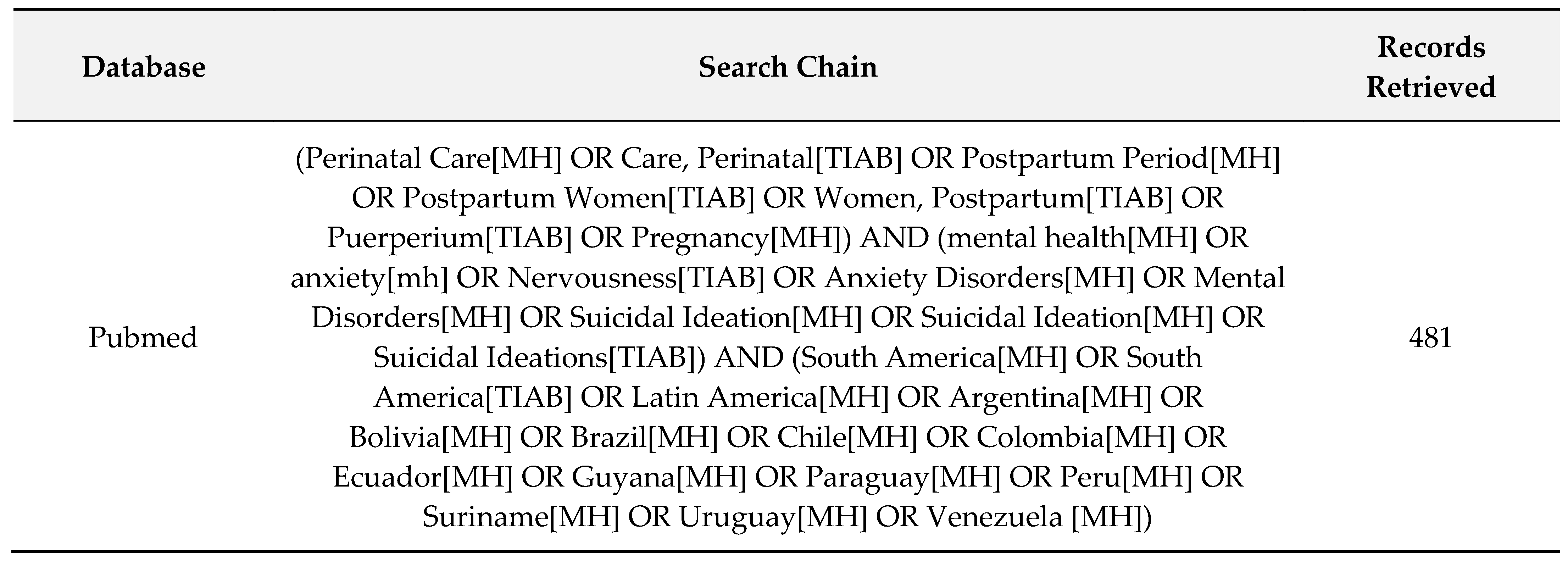
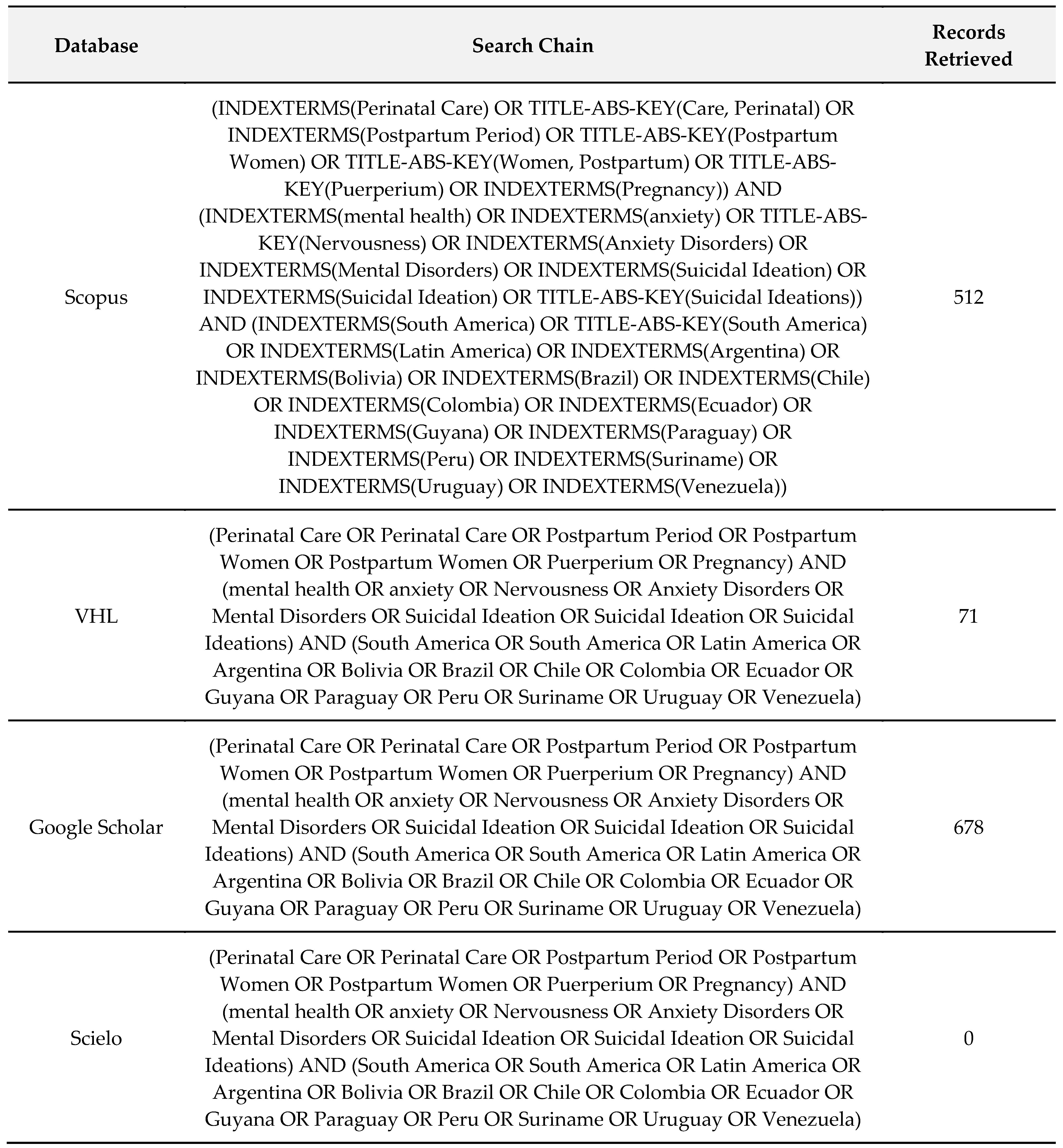
Figure 1.
PRISMA diagram.
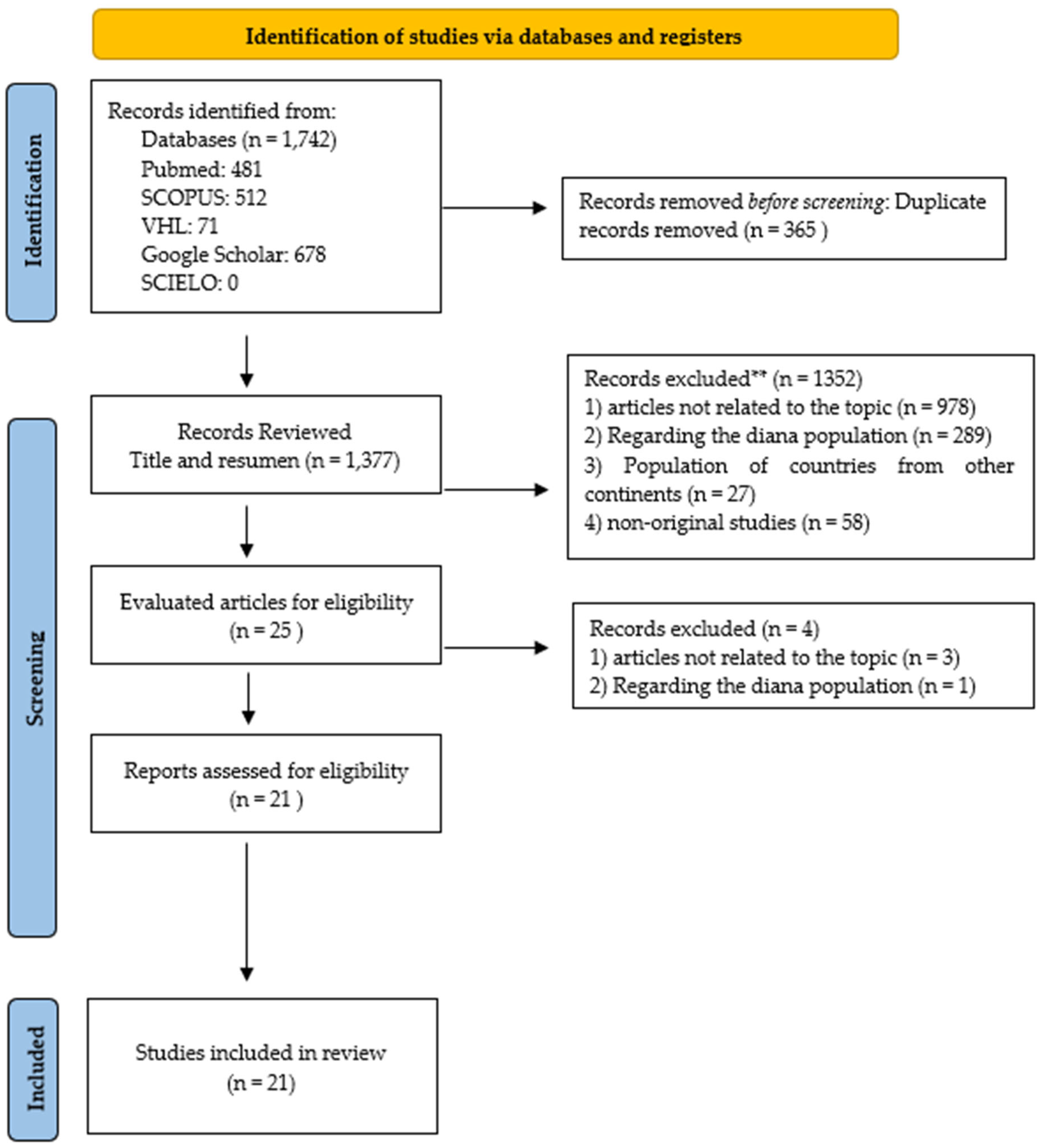

Table 1.
Description of included studies.
| Studio (Author-Year), Country | N | Drawing | Population | Type of show | Dependent variable | Independent variables | Measuring instruments |
| Faisal-Cury et al. 2007, Brazil [30] | 432 | Cross-sectional description | Pregnant |
Non-probabilistic |
Anxiety | Age, Race/color, Marital status | State-Trait Anxiety Inventory |
| Faisal-Cury et al. 2020, Brazil [29] | 769 | Cross-sectional description | Pregnant |
Non-probabilistic |
Suicidal ideation | Age, race/color, and depression | Patient Health Questionnaire (PHQ-9) |
| Faisal-Cury et al. 2021, Brazil [31] | 358 | Cross-sectional description | Women in the postpartum period |
Non-probabilistic |
Suicidal ideation | Mother-infant bonding, age, race/color, and postpartum depression | Patient Health Questionnaire (PHQ-9) |
| Fonseca-Machado et al. 2015a, Brazil [27] | 358 | Cross-sectional description | Pregnant | Probabilistic | Suicidal ideation | General intimate partner violence, marital status, legal or illegal drug use during pregnancy, and planned pregnancy | Beck Suicidal Ideation Scale (BSI) World Health Organization Multi-country Study on Women’s Health and Domestic Violence |
| Freitas et al, 2002, Brazil [32] | 120 | Cross-sectional description | Pregnant | Non-probabilistic | Suicidal ideation | Depression, anxiety, Violence (physical abuse) and violence (sexual abuse) | Hospital Anxiety and Depression Scale (HAD) Beck Suicidal Ideation Scale (BSI) |
| Friedman et al., 2016, Peru [33] | 3372 | Cross-sectional description | Pregnant | Non-probabilistic | Suicidal ideation | Migraine and depression | Patient Health Questionnaire (PHQ-9) International Classification of Headache Disorders (ICHD)-III |
| Studio (Author-Year), Country | N | Drawing | Population | Type of show | Dependent variable | Independent variables | Measuring instruments |
| Gelaye et al. 2016, Peru [34] | 1299 | Cross-sectional description | Pregnant | Non-probabilistic | Suicidal ideation | Sleep quality and Sleep quality and depression | Patient Health Questionnaire (PHQ-9) The Pittsburgh Sleep Quality Index (PSQI) |
| Gelaye et al. 2019, Peru [35] | 1108 | Cohort | Pregnant |
Non-probabilistic |
Suicidal ideation | Low infant birth weight, small for gestational age (below the 10th percentile), and preterm delivery | Patient Health Questionnaire (PHQ-9) |
| Huang et al. 2011, Brazil [36] | 831 | Cross-sectional description | Pregnant | Non-probabilistic | Suicidal ideation | Age and marital status | Self-Report Questionnaire-20 (SRQ-20) |
| Ishida et al. 2010, Paraguay [37] | 6538 | Cross-sectional description | Pregnant women and women in the puerperium | Non-probabilistic | Suicidal ideation | Currently pregnant women, age and marital status | Self-Report Questionnaire-20 (SRQ-20) |
| Levey et al. 2018, Peru [38] | 2062 | Cross-sectional description | Pregnant | Non-probabilistic | Suicidal ideation |
Age, race/color, marital status, violence (childhood abuse), and violence (intimate partner) |
The Suicide Questionnaire from the WHO CIDI |
| Marquesim et al. 2016, Brazil [39] | 101 | Prospective longitudinal |
Pregnant |
Non-probabilistic |
Anxiety | Mild hyperglycemia | State-Trait Anxiety Inventory |
| Matos et al. 2018, Brazil [28] | 870 | Cross-sectional description | Pregnant | Probabilistic | Anxiety | Bonding with parents (lack of maternal attention) and mother-child relationship | Mini International Neuropsychiatric Interview (MINI) Parental Bonding Instrument (PBI) |
| Morais et al. 2017, Brazil [41] | 1140 | Prospective cohort | Women in the postpartum period | Non-probabilistic | Anxiety | Mother-child relationship | Prenatal Self-Administered Questionnaire Postpartum Bonding Questionnaire (PBQ) |
| Studio (Author-Year), Country | N | Drawing | Population | Type of show | Dependent variable | Independent variables | Measuring instruments |
| Mitro et al. 2020, Peru [40] | 100 | Cohort | Pregnant | Non-probabilistic | Suicidal ideation | Metabolomic markers (choline) and Metabolomic markers (phenylalanine) | Patient Health Questionnaire (PHQ-9) |
| Pabon et al. 2024, Brazil [42] | 125 | Cohort | Pregnant Women in the puerperium |
Non-probabilistic | Suicidal ideation | Disability (daily activities, social participation, education, work, and personal care.) | General Anxiety Disorder test (GAD-7) WHO Disability Assessment Schedule 2.0 (WHODAS 2.0 12-item ) |
| Qiu-Yue et al. 2015, Peru [46] | 1517 | Cohort | Pregnant | Non-probabilistic | Suicidal ideation | Depression | Patient Health Questionnaire (PHQ-9) Edinburgh Postnatal Depression Scale (EPDS) |
| Sanchez et al. 2020, Peru [43] | 2068 | Cohort | Pregnant |
Non-probabilistic |
Anxiety | Stress-related sleep disorders | Generalized Anxiety Disorder Questionnaire (GAD-7) |
| Soares et al. 2021, Brazil [44] | 645 | Cohort | Pregnant |
Probabilistic |
Anxiety | Prematurity | The Beck Anxiety Inventory |
| Vilela et al. 2015, Brazil [45] | 185 | Cohort | Pregnant women and women in the puerperium | Non-probabilistic | Anxiety | Eating habits | The food frequency questionnaire (FFQ) State-Trait Anxiety Inventory (STAI) |
| Zhong et al. 2016, Peru [47] | 2964 | Cross-sectional description | Pregnant | Non-probabilistic | Suicidal ideation | Violence (child abuse) | Childhood Physical and Sexual Abuse Questionnaire Patient Health Questionnaire (PHQ-9) |
Table 2.
Evaluation of the quality of the included studies.
| Author, year and country | Selection | Classification | Confusion |
| Faisal-Cury et al. 2007, Brazil | - | + | + |
| Faisal-Cury et al. 2020, Brazil | - | + | + |
| Faisal-Cury et al. 2021, Brazil | - | + | + |
| Fonseca-Machado et al. 2015a, Brazil | + | + | + |
| Freitas et al, 2002, Brazil |
- | + | + |
| Friedman et al., 2016, Peru | - | + | + |
| Gelaye et al. 2016, Peru | - | + | + |
| Gelaye et al. 2019, Peru | - | + | + |
| Huang et al. 2011, Brazil | - | + | + |
| Ishida et al. 2010, Paraguay | - | + | + |
| Levey et al. 2018, Peru | - | + | + |
| Marquesim et al. 2016, Brazil | - | + | + |
| Matos et al. 2018, Brazil | + | + | + |
| Morais et al. 2017, Brazil | - | + | + |
| Mitro et al. 2020, Peru | - | + | + |
| Pabon et al. 2024, Brazil | - | + | + |
| Qiu-Yue et al. 2015, Peru | - | + | + |
| Sanchez et al. 2020, Peru | - | + | + |
| Soares et al. 2021, Brazil | + | + | + |
| Vilela et al. 2015, Brazil | - | + | + |
| Zhong et al. 2016, Peru |
- | + | + |
Table 3.
Meta-analysis results for suicidal ideation sub variables.
| Findings | K | N | N/K | Effect Size | 95% CI | Q | Qdf | p-value (Q) | I2 | Publication Record | |||
|
Funnel Plot |
Test de Egger (p) |
Trim and fill | |||||||||||
| Adjusted effect size | % change | ||||||||||||
| Suicidal ideation x marital status | 4 | 9.789 | 2.447 | 1,732 | 0,812; 3,697 | 20,50 | 3 | 0,000 | 20,00 | Asym | 0,633 | 1,732 | 0 |
| Suicidal ideation x Age | 5 | 10.558 | 2.111 | 0,818 | 0,461; 1,452 | 25,53 | 4 | 0,000 | 25,03 | Asym | 0,101 | 0,817 | 0 |
| Suicidal ideation x Violence | 4 | 5.504 | 1.376 | 2,848 | 1,926; 4,213 | 3,974 | 3 | 0,000 | 24,50 | Asym | 0,394 | 2,498 | 12,28 |
Abbreviations: K: number of studies; N: sample size; %: percentage of variation from the original combined effect; Asym: asymmetric.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



