
Submitted:
21 January 2026
Posted:
21 January 2026
You are already at the latest version
Abstract
Background: Chronic pain following thoracotomy remains a common and clinically significant complication that adversely affects functional recovery and quality of life. Despite advances in perioperative analgesic techniques, chronic post-thoracotomy pain continues to be under-recognized and insufficiently managed in routine clinical practice. This study aimed to determine the incidence of chronic pain after thoracotomy and to evaluate its impact on daily activities and postoperative pain management behaviors. Methods: This retrospective observational study was conducted after institutional ethics committee approval (approval no. 2023/61). Patients aged ≥15 years who underwent thoracotomy between 15 June 2022 and 15 June 2023 and were at least three months postoperative were included. Patients who underwent video-assisted thoracoscopic surgery were excluded. Demographic, surgical, anesthetic, and postoperative analgesia data were obtained from medical records. Patients were contacted by telephone to assess pain intensity using a Numeric Rating Scale (NRS), functional impact on daily activities, and analgesic medication use. The primary outcome was the incidence of chronic post-thoracotomy pain, defined as pain persisting beyond three months and reported at the time of the interview. Results: A total of 56 patients were included in the analysis. Chronic pain was reported by 55.4% of patients. Pain that interfered with daily activities and required medication use was reported by 51.5% of patients. Thirty-three patients (57.9%) reported an NRS score >3 during movement. Among patients with chronic pain, 64.7% reported self-medication without physician consultation, whereas only 11.8% sought medical advice for pain management. Conclusions: Chronic pain remains highly prevalent after thoracotomy and substantially interferes with daily functioning. A considerable proportion of patients self-manage their pain without medical supervision, underscoring the need for structured postoperative follow-up, early identification of high-risk patients, and individualized multimodal analgesic strategies to reduce the burden of chronic post-thoracotomy pain.
Keywords:
thoracotomy
; chronic post-thoracotomy pain
; postoperative pain
; pain management
; self-medication
; quality of life
; regional anesthesia
1. Introduction
Thoracotomy remains a fundamental surgical approach for accessing the thoracic cavity and is widely used in thoracic surgery. Among the various techniques, the posterolateral thoracotomy is the most commonly performed and is also recognized as the most painful, owing to extensive muscle division and retraction involving the latissimus dorsi, serratus anterior, rhomboids, and trapezius muscles [1]. Despite advances in surgical techniques and perioperative analgesia, postoperative pain following thoracotomy continues to represent a major clinical challenge. According to the International Association for the Study of Pain, chronic pain is defined as pain persisting for longer than three months [2]. Patients undergoing thoracotomy exhibit the highest rates of chronic postoperative pain among all surgical procedures, with reported prevalence rates ranging widely from 25% to 91% [3,4,5].
The development of chronic post-thoracotomy pain is multifactorial and has been associated with a broad range of demographic, treatment-related, psychosocial, genetic, and epigenetic factors [6]. In addition, geographical and cultural differences may influence pain perception and reporting, contributing to variability in prevalence across populations. Although numerous perioperative strategies have been proposed to prevent post-thoracotomy pain—including regional anesthesia techniques, multimodal analgesia, and enhanced recovery protocols—efforts to reduce chronic pain following thoracotomy have yielded inconsistent results [7]. Importantly, chronic postoperative pain substantially restricts daily activities and has a profound negative impact on functional recovery and quality of life [8].
In routine clinical practice, regional anesthesia techniques are frequently recommended to mitigate acute postoperative pain and potentially reduce the risk of chronic pain development in patients undergoing thoracotomy. However, the real-world incidence of chronic post-thoracotomy pain, its impact on daily functioning, and patients’ pain management behaviors—particularly self-medication and patterns of physician consultation—remain insufficiently characterized. Therefore, the present retrospective observational study aimed to determine the incidence of chronic pain after thoracotomy, to evaluate its impact on daily activities, and to assess postoperative pain management strategies, including the frequency of physician consultation among patients with chronic pain.
2. Materials and Methods
Study Design and Ethics Approval
This retrospective observational study was conducted after obtaining approval from the institutional ethics committee (approval no. 2023/61). The study was performed in accordance with the principles of the Declaration of Helsinki. Verbal informed consent was obtained from all participants prior to the telephone interview.
Patient Selection
The hospital database was reviewed to identify patients aged ≥15 years who had undergone thoracotomy between 15 June 2022 and 15 June 2023. Patients were included if at least three months had elapsed since surgery at the time of assessment. Exclusion criteria were age <15 years, incomplete medical records, and surgery performed using a video-assisted thoracoscopic approach.
Anesthesia and Perioperative Management
Standard institutional anesthesia protocols were applied to all patients. General anesthesia was induced with propofol and maintained using a balanced technique consisting of O2/air/sevoflurane and remifentanil infusion. Neuromuscular blockade was achieved with rocuronium at a dose of 0.5 mg/kg.
Intraoperative analgesia was provided by remifentanil infusion. In patients who had received preoperative epidural analgesia, intraoperative epidural administration was not routinely continued because of the risk of hypotension.
Before extubation, all patients received 1 g of intravenous paracetamol and 100 mg of tramadol.
Epidural analgesia, when used, was placed preoperatively. Fascial plane blocks (erector spinae plane block or serratus anterior plane block) were performed at the end of surgery according to institutional practice.
Postoperative Pain Management
For postoperative analgesia, patients who did not receive a regional block were treated with tramadol infusion (maximum daily dose not exceeding 400 mg) and intravenous paracetamol at 6-hour intervals.
In patients who underwent a fascial plane block at the end of surgery, intravenous paracetamol was administered at 6-hour intervals, and a tramadol bolus of 1 mg/kg was administered if the Numeric Rating Scale (NRS) score exceeded 4.
Surgical Procedure and Postoperative Care
All patients underwent standard posterolateral thoracotomy, with or without rib resection. Chest tubes were removed when there was no air leak and pleural drainage was <100 mL over a 24-hour period.
Data Collection
Demographic data, comorbidities, previous surgical history (e.g., upper abdominal or breast surgery), medications, intraoperative anesthesia techniques, postoperative pain management strategies, and perioperative complications were obtained from electronic medical records.
Telephone Follow-Up and Outcome Assessment
Patients were contacted chronologically by telephone to obtain additional information regarding postoperative pain and its impact on daily activities.
During the structured telephone interview, the following standardized questions were asked:
1.Did you experience any pain around the surgical incision or surrounding area three months after surgery?
2. Did you have pain before surgery? If yes, was the pain three months after surgery similar to your preoperative pain?
3. Was there any other identifiable cause for the pain?
4. Did you take any measures to relieve pain, such as rest, reducing daily activities, self-medication, or seeking medical assistance?
5. On a scale from 0 (no pain) to 10 (unbearable pain) (Numeric Rating Scale, NRS), how would you rate your pain? Did the intensity change with coughing or movement?
Chronic post-thoracotomy pain was defined as pain around the surgical incision persisting for more than three months after surgery and reported at the time of the telephone interview.
The primary outcome was the incidence of chronic post-thoracotomy pain as assessed during follow-up, whereas secondary outcomes included pain intensity, functional impact on daily activities, and postoperative pain management behaviors.
Statistical Analysis
Descriptive statistics were used to summarize the data. Continuous variables were expressed as means ± standard deviations or medians (minimum–maximum), as appropriate. Categorical variables were presented as frequencies and percentages. All statistical analyses were performed using SPSS version 27.0 software (IBM Corp., Armonk, NY, USA).
3. Results
During the one-year study period, 70 patients who underwent thoracotomy were assessed for eligibility. Four patients were excluded because of age <15 years or incomplete medical records. Consequently, 66 patients were eligible for follow-up. Of these, 10 patients could not be reached by telephone. Therefore, 56 patients (17 females and 39 males) were successfully contacted and included in the final analysis (Figure 1).
The demographic and preoperative characteristics of the patients are summarized in Table 1.
Surgical indications, previous surgeries potentially affecting chronic pain (e.g., upper abdominal or breast surgery), the duration of surgery, and thoracotomy-related variables are presented in Table 2.
Postoperative pain management techniques, analgesic medications used, and responses to the chronic pain survey are shown in Table 3.
Chronic pain persisting for more than three months after surgery was reported by 55.4% of patients. Pain that interfered with daily activities and required medication use was reported by 51.5% of patients. Thirty-three of the 56 patients (57.9%) reported a Numeric Rating Scale (NRS) score >3 during movement. Among patients with chronic pain, 64.7% reported using analgesic medication independently without physician consultation, whereas only 11.8% sought medical advice for pain management.
4. Discussion
The primary objective of this study was to determine the frequency of chronic pain in patients undergoing thoracotomy and to evaluate its impact on daily activities and pain management behaviors. The prevalence of chronic post-thoracotomy pain has been reported to vary widely across studies, reflecting differences in surgical techniques, analgesic strategies, patient populations, and methodological approaches [9,10]. In the present study, chronic pain persisting for more than three months after surgery was observed in 55.4% of patients. This finding is consistent with previous reports and underscores that chronic pain remains a common and clinically relevant complication following thoracotomy.
More than half of the patients in our cohort (51.5%) reported that their pain interfered with daily activities and necessitated medication use, a result in line with earlier research. Bayman et al. reported that pain affected the daily lives of more than 50% of patients suffering from chronic postoperative pain following thoracic surgery [11]. Similarly, chronic pain lasting from six months to three years has been observed in approximately 36% of patients undergoing thoracic surgery, highlighting the long-term functional burden associated with this condition [11]. Together, these findings emphasize that chronic post-thoracotomy pain not only persists over time but also has substantial implications for patients’ quality of life and functional capacity.
An important observation in the present study is that 64.7% of patients reported self-medication for pain relief, whereas only 11.8% sought medical consultation. This low rate of physician consultation may be influenced by multiple factors, including pain severity, socio-cultural characteristics, health literacy, and accessibility of healthcare services. In Türkiye, analgesics such as paracetamol and non-steroidal anti-inflammatory drugs (e.g., ibuprofen) are readily available without prescription, which may contribute to high rates of self-medication. Globally, the prevalence of self-medication and over-the-counter analgesic use is substantial, and inappropriate or unsupervised use should not be underestimated [12]. These findings highlight an important gap in postoperative care and underscore the need for structured follow-up and patient education regarding appropriate pain management strategies after thoracic surgery.
Chronic post-thoracotomy pain is widely recognized as a multifactorial condition [13]. Studies examining the influence of surgical techniques on chronic pain development have yielded inconsistent results. Jiwnani et al. demonstrated that a modified nerve-sparing thoracotomy did not reduce chronic pain compared with standard posterolateral thoracotomy at six months postoperatively [14]. Michel-Cherqui et al. reported that although acute pain was less frequent after a minimally invasive axillary approach, the risk of chronic pain was comparable to that of the posterolateral approach [15]. Likewise, Bayman et al. found similar frequencies and severities of pain at six months following thoracotomy and thoracoscopy [16]. Although nerve injury has traditionally been regarded as a primary contributor to chronic post-thoracotomy pain, these findings suggest that nerve-sparing surgical techniques alone do not fully prevent its occurrence and that additional perioperative factors play a substantial role.
The choice of anesthetic and analgesic techniques also appears to be a critical determinant in the development of chronic postsurgical pain. While general anesthesia reduces awareness of surgical trauma, halogenated anesthetics have been shown to stimulate peripheral nociceptive receptors, potentially exacerbating postoperative inflammation and peripheral sensitization [17]. Both inhalational anesthetics and propofol exert analgesic effects by modulating central sensitization pathways; however, inhalational agents alone appear insufficient to reduce the prevalence of chronic pain [18]. Propofol additionally interacts with glycine and γ-aminobutyric acid type A receptors and possesses antioxidative properties that may contribute to its analgesic profile [18]. Moreover, high doses of intraoperative remifentanil have been associated with chronic postsurgical pain one year after video-assisted thoracoscopic surgery, suggesting that excessive opioid exposure should be avoided when possible [19].
Preemptive analgesia may mitigate central sensitization by blocking the transmission of nociceptive impulses. Preoperative epidural analgesia has been shown to reduce the occurrence and severity of persistent pain syndromes after thoracotomy [20]. Beyond pharmacological interventions, psychological factors such as anxiety, depression, stress responses, and poor sleep quality have been identified as independent predictors of persistent postsurgical pain [21]. Cognitive behavioral therapy for high-risk patients and perioperative patient education regarding expected postoperative discomfort may help reduce fear-avoidance behaviors and improve functional recovery [22].
Genetic predisposition may further modulate the risk of chronic pain in susceptible individuals. Polymorphisms involving catechol-O-methyltransferase (COMT), voltage-gated sodium and calcium channels, and μ-opioid receptors have been implicated as potential genetic contributors to chronic pain [23]. A validated presurgical risk model incorporating six easily measurable factors—type of surgical procedure, younger age, physical and mental health status, preoperative pain at the surgical site, and preoperative pain at another location—has been shown to effectively identify patients at risk of chronic postsurgical pain [24]. Such models could facilitate early, targeted interventions and personalized perioperative pain management strategies.
Future studies should incorporate validated pain and functional interference instruments, such as the Brief Pain Inventory or neuropathic pain questionnaires (e.g., DN4 or PainDETECT), to better characterize pain phenotypes and functional outcomes.
From a clinical perspective, our findings emphasize the need for structured postoperative follow-up, early identification of high-risk patients, and individualized multimodal analgesic strategies to reduce the long-term burden of chronic post-thoracotomy pain.
This study has several limitations. First, its retrospective design precluded the formation of comparison groups and limited causal inference regarding the effects of different surgical or analgesic techniques. Second, intraoperative remifentanil doses varied among patients and could not be standardized. Third, the sample size was relatively small and restricted to a one-year period. Fourth, neuropathic pain was not specifically assessed, and information regarding patients’ socio-cultural characteristics and preoperative anxiety levels was unavailable. Additionally, postoperative follow-up durations varied among patients at the time of pain assessment. Pain outcomes were based on telephone interviews and self-reported data, which are subject to recall bias and reporting inaccuracies. The lack of in-person clinical examination further limits the objective assessment of pain characteristics. Additionally, non-response of 10 eligible patients may have introduced selection bias, as patients with more severe or milder symptoms may have been more or less likely to participate in the telephone follow-up.
5. Conclusions
In conclusion, chronic pain remains a frequent and clinically significant complication following thoracotomy, substantially impairing daily functioning and quality of life. In this study, more than half of the patients experienced persistent pain beyond three months after surgery, and a considerable proportion relied on self-medication without medical supervision. These findings underscore the need for structured postoperative follow-up, early identification of high-risk patients, and individualized multimodal analgesic strategies to reduce the long-term burden of chronic post-thoracotomy pain.
Given the multifactorial nature of post-thoracotomy pain syndrome, preventive efforts should begin in the preoperative period and incorporate individualized risk assessment, appropriate regional anesthesia techniques, and perioperative psychological support. Despite existing interventions aimed at alleviating chronic pain, its prevalence remains unacceptably high. Future prospective studies and personalized pain management approaches are warranted to reduce the burden of chronic post-thoracotomy pain and to improve long-term patient-centered outcomes.
Author Contributions
Conceptualization, F.Y., D.Ç., E.D., and İ.U.; Data curation, İ.U., E.D., and D.Ç.; Formal analysis, E.D. and D.Ç.; Investigation, F.Y. and İ.U.; Project administration, F.Y. and E.D.; Writing—original draft, F.Y.; Writing—review and editing, D.Ç. and E.D.
Funding
The authors declared that this study has received no financial support.
Institutional Review Board Statement
This retrospective observational study was conducted after obtaining approval from the institutional ethics committee (approval no. 2023/61). The study was performed in ac-cordance with the principles of the Declaration of Helsinki.
Informed Consent Statement
Verbal informed consent was obtained from all participants prior to the telephone interview.
Data Availability Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Acknowledgments
“This work was presented as an oral presentation entitled ‘Investigation of the Frequency of Chronic Pain Development After Thoracotomy’ at the 41st Annual Congress of the European Society of Regional Anaesthesia and Pain Therapy (ESRA), held from 4 to 7 September 2024 in Prague, Czech Republic.”
Conflicts of Interest
The authors have no conflict of interest to declare.
Abbreviations
The following abbreviations are used in this manuscript:
ASA: American Society of Anesthesiologists
BMI: body mass index
SD: standard deviation
ESP: erector spinae plane block
SAPB: serratus anterior plane block
PVB: paravertebral block
NSAID: non-steroidal anti-inflammatory drug
HT: hypertension
COPD: chronic obstructive pulmonary disease
CAD: coronary artery disease
DM: diabetes mellitus
References
- Raveglia, F.; Scarci, M.; Cioffi, U.; Baisi, A. Ultimate management of post-thoracotomy morbidities: A set of surgical techniques and peri-operative precautions. J. Thorac. Dis. 2019, 11, S370–S375. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Rief, W.; Barke, A.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Guastella, V.; Mick, G.; Soriano, C.; et al. A prospective study of neuropathic pain induced by thoracotomy: Incidence, clinical description, and diagnosis. Pain 2011, 152, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Arends, S.; Böhmer, A.B.; Poels, M.; et al. Post-thoracotomy pain syndrome: Seldom severe, often neuropathic, treated unspecific, and insufficient. Pain Rep. 2020, 5, e810. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, R.; Hou, B.; et al. Incidence and risk factors for chronic postsurgical pain following video-assisted thoracoscopic surgery: A retrospective study. BMC Surg. 2022, 22, 76. [Google Scholar] [CrossRef]
- Van Helmond, N.; Olesen, S.S.; Wilder-Smith, O.H.; Drewes, A.M.; Steegers, M.A.; Vissers, K.C. Predicting persistent pain after surgery: Can predicting the weather serve as an example? Anesth. Analg. 2018, 127, 1264–1267. [Google Scholar] [CrossRef]
- Bayman, E.O.; Brennan, T.J. Incidence and severity of chronic pain at 3 and 6 months after thoracotomy: Meta-analysis. J. Pain 2014, 15, 887–897. [Google Scholar] [CrossRef]
- Kar, P.; Sudheshna, K.D.; Padmaja, D.; Pathy, A.; Gopinath, R. Chronic pain following thoracotomy for lung surgeries: Its risk factors, prevalence, and impact on quality of life—A retrospective study. Indian J. Anaesth. 2019, 63, 368–374. [Google Scholar] [CrossRef]
- Israfilov, N.; Yıldırım Güçlü, Ç.; Karadağ Erkoç, S.; Özgencil, G.E. Retrospective analysis of factors affecting chronic postoperative pain after thoracotomy: Single-center experience. Turk. J. Anaesthesiol. Reanim. 2023, 51, 235–242. [Google Scholar] [CrossRef]
- Wang, H.; Li, S.; Liang, N.; Liu, W.; Liu, H.; Liu, H. Postoperative pain experiences in Chinese adult patients after thoracotomy and video-assisted thoracic surgery. J. Clin. Nurs. 2017, 26, 2744–2754. [Google Scholar] [CrossRef]
- Bayman, E.O.; Lennertz, R.; Brennan, T.J. Pain-related limitations in daily activities following thoracic surgery in a United States population. Pain Physician 2017, 20, E367–E378. [Google Scholar] [CrossRef] [PubMed]
- Perrot, S.; Cittée, J.; Louis, P.; et al. Self-medication in pain management: The state of the art of pharmacists’ role for optimal over-the-counter analgesic use. Eur. J. Pain 2019, 23, 1747–1762. [Google Scholar] [CrossRef]
- Arends, S.; Böhmer, A.B.; Poels, M.; et al. Post-thoracotomy pain syndrome: Seldom severe, often neuropathic, treated unspecific, and insufficient. Pain Rep. 2020, 5, e810. [Google Scholar] [CrossRef] [PubMed]
- Jiwnani, S.; Ranganathan, P.; Patil, V.; Agarwal, V.; Karimundackal, G.; Pramesh, C.S. Pain after posterolateral versus nerve-sparing thoracotomy: A randomized trial. J. Thorac. Cardiovasc. Surg. 2019, 157, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Michel-Cherqui, M.; Fessler, J.; Dorges, P.; et al. Chronic pain after posterolateral and axillary approaches to lung surgery: A monocentric observational study. J. Anesth. 2023, 37, 687–702. [Google Scholar] [CrossRef]
- Bayman, E.O.; Parekh, K.R.; Keech, J.; Selte, A.; Brennan, T.J. A prospective study of chronic pain after thoracic surgery. Anesthesiology 2017, 126, 938–951. [Google Scholar] [CrossRef]
- Matta, J.A.; Cornett, P.M.; Miyares, R.L.; Abe, K.; Sahibzada, N.; Ahern, G.P. General anesthetics activate a nociceptive ion channel to enhance pain and inflammation. Proc. Natl. Acad. Sci. USA 2008, 105, 8784–8789. [Google Scholar] [CrossRef]
- Yoon, S.H.; Choi, S.; Yoon, S.; Na, K.J.; Bahk, J.; Lee, H.J. Impact of general anesthesia type on chronic postsurgical pain following video-assisted thoracoscopic surgery for lung cancer: A retrospective propensity-matched cohort study. Korean J. Pain 2024, 37, 354–366. [Google Scholar] [CrossRef]
- Wang, X.; Ida, M.; Uyama, K.; Naito, Y.; Kawaguchi, M. Impact of different doses of remifentanil on chronic postsurgical pain after video-assisted thoracic surgery: A propensity score analysis. Medicine (Baltimore) 2023, 102, e34442. [Google Scholar] [CrossRef]
- Park, S.K.; Yoon, S.; Kim, B.R.; Choe, S.H.; Bahk, J.H.; Seo, J.H. Pre-emptive epidural analgesia for acute and chronic post-thoracotomy pain in adults: A systematic review and meta-analysis. Reg. Anesth. Pain Med. 2020, 45, 1006–1016. [Google Scholar] [CrossRef]
- Chen, D.; Yang, H.; Yang, L.; et al. Preoperative psychological symptoms and chronic postsurgical pain: Analysis of the prospective China Surgery and Anaesthesia Cohort study. Br. J. Anaesth. 2024, 132, 359–371. [Google Scholar] [CrossRef]
- Güven Köse, S.; Köse, H.C.; Çelikel, F.; et al. Chronic pain: An update of clinical practices and advances in chronic pain management. Eurasian J. Med. 2022, 54, 57–61. [Google Scholar] [CrossRef]
- Zorina-Lichtenwalter, K.; Bango, C.I.; Van Oudenhove, L.; et al. Genetic risk shared across 24 chronic pain conditions: Identification and characterization with genomic structural equation modeling. Pain 2023, 164, 2239–2252. [Google Scholar] [CrossRef]
- Montes, A.; Roca, G.; Cantillo, J.; Sabaté, S.; GENDOLCAT Study Group. Presurgical risk model for chronic postsurgical pain based on six clinical predictors: A prospective external validation. Pain 2020, 161, 2611–2618. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of study selection
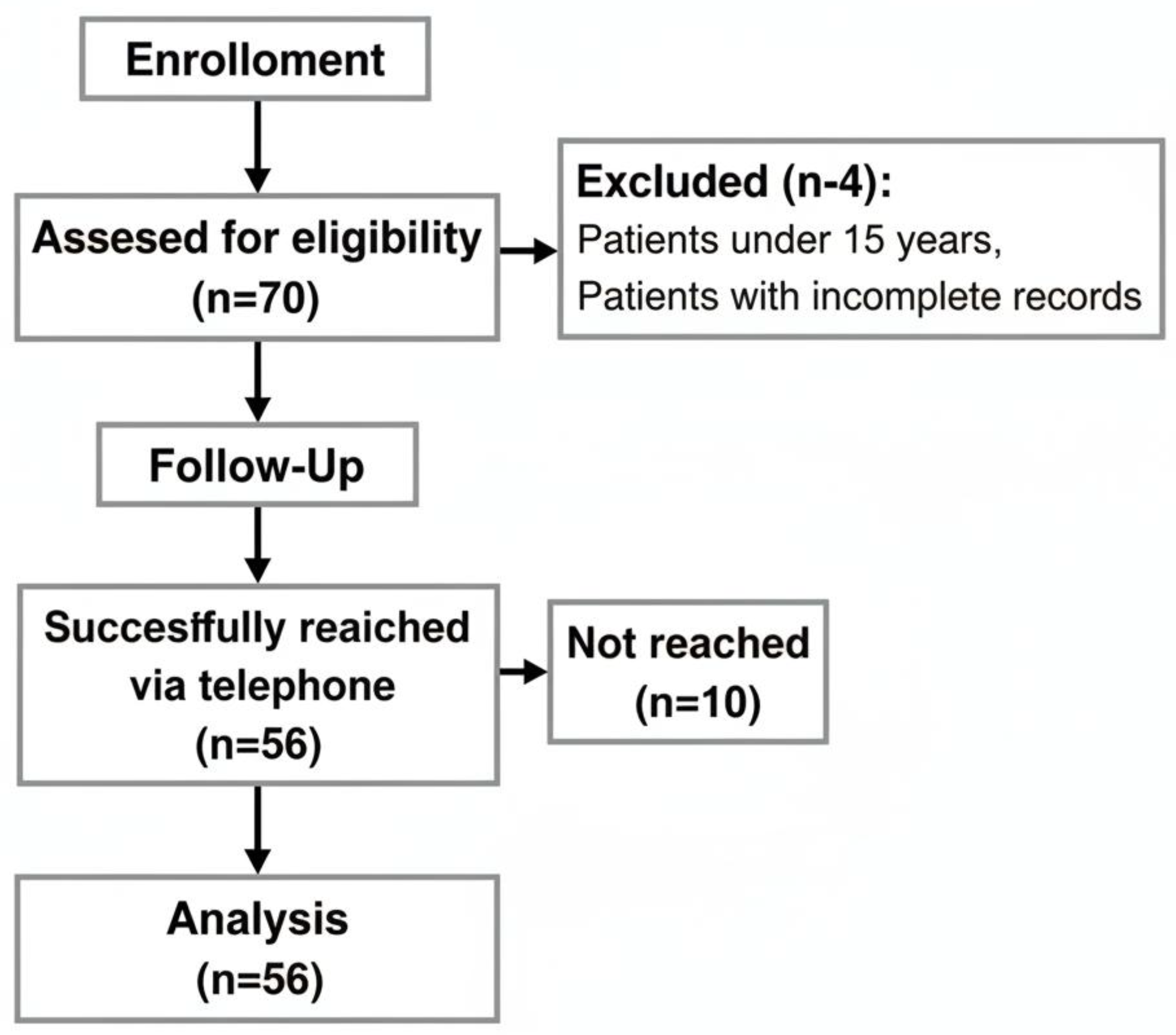

Table 1.
Demographic and preoperative characteristics of the study population (n = 56)
| Variable | Min–Max | Median | Mean ± SD / n (%) |
| Age (years) | 15.0–78.0 | 57.0 | 57.2 ± 14.2 |
| Gender | |||
| Female | — | — | 17 (30.4%) |
| Male | — | — | 39 (69.6%) |
| Body mass index (kg/m2) | 15.1–40.4 | 24.8 | 25.1 ± 5.1 |
| ASA physical status | |||
| I | — | — | 6 (10.7%) |
| II | — | — | 27 (48.2%) |
| III | — | — | 23 (41.1%) |
| Any comorbidity | |||
| No | — | — | 19 (33.9%) |
| Yes | — | — | 37 (66.1%) |
| Specific comorbidities* | |||
| Hypertension | — | — | 21 (37.5%) |
| COPD | — | — | 16 (28.6%) |
| CAD | — | — | 15 (26.8%) |
| Oncological disease | — | — | 14 (25.0%) |
| Diabetes mellitus | — | — | 12 (21.4%) |
| Rheumatological disease | — | — | 5 (8.9%) |
| Thyroid disease | — | — | 4 (7.1%) |
| Renal disease | — | — | 2 (3.6%) |
| Cerebrovascular disease | — | — | 1 (1.8%) |
| Regular medication use | |||
| No | — | — | 45 (80.4%) |
| Yes | — | — | 11 (19.6%) |
| Types of medications† | |||
| Antidepressants | — | — | 6 (54.5%) |
| Steroids | — | — | 6 (54.5%) |
| NSAIDs | — | — | 2 (18.2%) |
| Paracetamol | — | — | 1 (9.1%) |
| Opioids | — | — | 1 (9.1%) |
Data are presented as mean ± standard deviation or n (%). *Patients could have more than one comorbidity. †Percentages are calculated based on the number of patients with regular medication use (n = 11). Abbreviations: SD, standard deviation; BMI, body mass index; ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; NSAID, non-steroidal anti-inflammatory drug.
Table 2.
Surgical characteristics of the study population (n = 56).
| Variable | Min–Max | Median | Mean ± SD / n (%) |
| Previous surgical history | |||
| No | — | — | 45 (80.4%) |
| Yes | — | — | 11 (19.6%) |
| Type of previous surgery† | |||
| Upper abdominal surgery | — | — | 7 (63.6%) |
| Previous thoracotomy | — | — | 5 (45.5%) |
| Breast surgery | — | — | 1 (9.1%) |
| Indications for thoracotomy | |||
| Lobectomy | — | — | 33 (58.9%) |
| Decortication | — | — | 5 (8.9%) |
| Pleural biopsy | — | — | 4 (7.1%) |
| Wedge resection | — | — | 4 (7.1%) |
| Cyst excision | — | — | 2 (3.6%) |
| Cystectomy | — | — | 2 (3.6%) |
| Nodule excision | — | — | 2 (3.6%) |
| Pneumonectomy | — | — | 2 (3.6%) |
| Biopsy | — | — | 1 (1.8%) |
| Chest wall resection | — | — | 1 (1.8%) |
| Hydatid cyst surgery | — | — | 1 (1.8%) |
| Rib resection | — | — | 1 (1.8%) |
| Segmentectomy | — | — | 1 (1.8%) |
| Liquid drainage | — | — | 1 (1.8%) |
| Thoracic side | |||
| Right | — | — | 35 (62.5%) |
| Left | — | — | 20 (35.7%) |
| Bilateral | — | — | 1 (1.8%) |
| Duration of surgery (min) | 150.0–420.0 | 270.0 | 249.8 ± 81.6 |
Data are presented as mean ± standard deviation or n (%). †Percentages are calculated based on the number of patients with a history of previous surgery (n = 11). Abbreviations: SD, standard deviation.
Table 3.
Characteristics of chronic post-thoracotomy pain (n = 56).
| Variable | Min–Max | Median | Mean ± SD / n (%) |
| Postoperative month at assessment | 7.0–19.0 | 14.0 | 13.5 ± 3.4 |
| Postoperative regional block | |||
| No block | — | — | 31 (55.4%) |
| Epidural | — | — | 7 (12.5%) |
| ESP block | — | — | 11 (19.6%) |
| SAPB | — | — | 1 (1.8%) |
| PVB | — | — | 4 (7.1%) |
| Intercostal block | — | — | 2 (3.6%) |
| Postoperative analgesic medications* | |||
| NSAIDs | — | — | 47 (83.9%) |
| Tramadol infusion | — | — | 37 (66.1%) |
| Paracetamol | — | — | 47 (83.9%) |
| Paracetamol + NSAID | — | — | 1 (1.8%) |
| Chronic pain at ≥3 months | |||
| No | — | — | 25 (44.6%) |
| Yes | — | — | 31 (55.4%) |
| Preoperative pain comparison† | |||
| No preoperative pain | — | — | 43 (76.8%) |
| Yes (similar pain postoperatively) | — | — | 1 (1.8%) |
| Yes (less pain postoperatively) | — | — | 2 (3.6%) |
| Yes (more pain postoperatively) | — | — | 7 (12.5%) |
| Other identifiable cause of pain | |||
| No | — | — | 48 (85.7%) |
| Yes | — | — | 5 (8.9%) |
| Pain management behaviors | |||
| No measures taken | — | — | 22 (39.3%) |
| Any measure taken | — | — | 34 (60.7%) |
| Self-medication‡ | — | — | 22 (64.7%) |
| Doctor’s prescription‡ | — | — | 4 (11.8%) |
Data are presented as mean ± standard deviation or n (%). *Patients could have received more than one postoperative analgesic medication. †Percentages are calculated based on the number of patients reporting any preoperative pain (n = 10). ‡Percentages are calculated based on the number of patients who took any measures to relieve pain (n = 34). Abbreviations: SD, standard deviation; ESP, erector spinae plane block; SAPB, serratus anterior plane block; PVB, paravertebral block; NSAID, non-steroidal anti-inflammatory drug.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



