
Submitted:
20 January 2026
Posted:
21 January 2026
You are already at the latest version
Abstract
Acne vulgaris remains a common condition, with current topical therapies often limited by suboptimal efficacy and tolerability. This study evaluated the efficacy and safety of two novel 1% hydrogen peroxide (H₂O₂) formulations, a cream-gel for facial and a sprayable lotion for truncal mild to moderate acne. 42 participants presenting facial acne and 41 with truncal acne were treated twice daily for 8 weeks. Efficacy was assessed using the Investigator’s Global Assessment (IGA), the Spanish Acne Severity Scale (EGAE), and lesion counts. After 56 days, facial acne severity improved significantly (IGA −26%, p=0.01; EGAE −31%, p=0.01), with reductions in papules (−45%, p=0.017), porphyrin count (−27%, p=0.04), sebum production (−75%, p=0.005), erythema (−35%, p=0.0001), and desquamation (−22%, p=0.02). Truncal acne severity also improved sig-nificantly (IGA −32%, p=0.001; EGAE −45%, p=0.001), with reductions in inflammatory lesions (−60%, p=0.001), porphyrin size and count (-55% and −48%, both p=0.001), ery-thema (−7%, p=0.005), and desquamation (−27%, p=0.001). Both formulations were ac-cepted by the users, with minimal local irritation and high patient satisfaction. Topical 1% H₂O₂ formulations demonstrated significant and well-tolerated efficacy in both fa-cial and truncal acne, supporting their potential as safe and patient-friendly options for managing mild to moderate acne.
Keywords:
acne vulgaris
; facial
; truncal
; topical treatment
; hydrogen peroxide
1. Introduction
Acne vulgaris is a highly prevalent, chronic inflammatory disease of the pilosebaceous unit, affecting approximately 9.38% of the global population, with the highest incidence in adolescents and young adults, among whom up to 85% are affected [1,2]. It manifests as a combination of non-inflammatory lesions (open and closed comedones) and inflammatory lesions (papules, pustules, and nodules), often leading to scarring, persistent erythema, and post-inflammatory hyperpigmentation [1,3,4]. Lesions predominantly appear on the face, neck, upper back, and chest [4]. Beyond its physical manifestations, acne imposes a substantial psychosocial burden, negatively impacting self-esteem, body image, social functioning, and overall quality of life (QoL), and is frequently associated with anxiety and depression [1,3,5,6]. Patients with both facial and truncal acne experience a greater reduction in health-related QoL compared to those with facial acne alone [7].
The pathophysiology of acne is multifactorial, involving four interrelated mechanisms: excessive sebum production, abnormal follicular keratinization, colonization by Cutibacterium acnes (C. acnes), and inflammation [4]. However, hyperseborrhea appears to play a lesser role in truncal acne, as sebum secretion on the trunk is lower than on the face [8]. Facial acne is the most prevalent manifestation, reflecting the higher density and larger size of sebaceous glands in the facial region [9]. Importantly, approximately 48–52% of patients with facial acne also present with truncal involvement. Despite its high prevalence, truncal acne remains underrecognized and undertreated in clinical practice, often overlooked by both clinicians and patients [10].
Topical therapies, including antibiotics, benzoyl peroxide, and retinoids, are the mainstay for managing mild-to-moderate acne vulgaris [4,11,12]. However, antimicrobial resistance affects over 50% of C. acnes strains, limiting the efficacy of topical antibiotics [11]. Benzoyl peroxide, although effective, is often associated with local side effects such as dryness, irritation, erythema, and pruritus [13]. These effects may result from its rapid degradation into hydrogen peroxide (H₂O₂) and benzoic acid, with the latter being primarily responsible for skin irritation and erythema [14,15] (Figure 1). Truncal acne presents additional challenges: the absence of specific evidence-based guidelines, differences in skin physiology (pH, microbiota, thickness), and the larger surface area involved [10,16,17] Practical barriers, including difficulty applying treatments to hard-to-reach areas, clothing discoloration from benzoyl peroxide, and treatment costs, further hinder adherence and outcomes [17,18]. These limitations underscore the need for safer, better tolerated options that support skin health and improve QoL [11].
In this context, H₂O₂ has emerged as a promising topical agent for improving acne symptoms while maintaining a favorable tolerability profile.14,19–24 As a reactive oxygen species (ROS), H₂O₂ contributes to oxidative damage of cellular components and can diffuse freely across membranes, exerting effects in different cellular compartments. In the skin, it plays roles in innate immune defense, apoptosis, wound repair, and modulation of vascular tone. Beyond these physiological functions, H₂O₂ exhibits antibacterial activity and acts as a debriding agent when applied topically at concentrations of 1–6%, supporting its long-standing use in wound care.24 At lower concentrations (around 1%), H₂O₂ has demonstrated efficacy in acne management comparable to benzoyl peroxide, but with a more favorable side effect profile.20–22,24 Building on this rationale, the present study aimed to evaluate the anti-acne efficacy and tolerability of two novel 1% H₂O₂ formulations: a cream-gel for facial acne and a sprayable lotion for truncal acne.
2. Materials and Methods
2.1. Study and Design
This work comprised two separate open-label, prospective clinical studies evaluating topical formulations with 1% H₂O₂ for mild to moderate acne.
The facial acne study involved 42 participants who applied a cream-gel formulation twice daily for eight consecutive weeks (56 days). The study was conducted between April and August 2022 and included four assessment visits: baseline (D0), day 14 (D14), day 28 (D28), and day 56 (D56).
The truncal acne study included 41 participants who applied a sprayable body lotion twice daily for eight consecutive weeks (56 days). This study was conducted between April 2022 and May 2023 and followed the same assessment schedule: D0, D14, D28, and D56.
Eligible participants included male and female subjects aged 12 to 33 years with oily skin and a tendency toward mild to moderate acne, either facial or truncal (back or chest). All participants had to be in good physical and mental health, available for scheduled visits to the research centers, and provide written informed consent. A washout period was required before study initiation: at least 7 days for topical anti-acne or sebum-regulating products, and at least 15 days for oral anti-acne treatments. On the first day of the study, participants were instructed not to apply any products to the experimental area.
Throughout the study, the use of topical products other than those provided, as well as sunbathing or UVA exposure on the treated areas, was not permitted. Exclusion criteria included history of allergy to cosmetic products, skin hyperreactivity, active oncological conditions, recent surgery or treatment in the study area, pregnancy or breastfeeding, participation in another clinical trial that could interfere with the protocol, and any health condition likely to compromise adherence.
The investigational product in both studies was Redoxcutane® (Laboratorio Reig Jofre S.A.), a topical formulation containing stabilized 1% H₂O₂. Stabilization maintained the pH below 4.40, preventing decomposition and precipitation of the active compound. Two presentations were evaluated: a facial cream-gel and a sprayable body lotion. Participants were instructed to apply the assigned product to the affected areas twice daily, morning and evening, after routine cleansing, and to massage until fully absorbed for a total duration of 8 weeks.
2.2. Study Procedures
2.2.1. Acne Assessment by Investigators
The list of the measurements performed in this study is shown in Table 1. The dermatologists recorded the number of inflammatory lesions for each patient and assessed acne severity using both the Investigator’s Global Assessment (IGA) scale and the Spanish Acne Severity Scale (Escala de Gravedad del Acné Española, EGAE).
2.2.2. Biometric Measurements
At each visit, biometric evaluations were conducted to monitor treatment effects. All measurements were taken on acne-affected areas. Skin pH, reflecting the integrity of the hydrolipidic film (acid mantle), was measured using the Skin-pH-Meter PH 905. C. acnes virulence was assessed via porphyrin fluorescence (Visiopor® PP 34), with treatment efficacy defined as reductions in porphyrin size, count, or intensity. Sebum production on the face or trunk was quantified using the Sebufix® F16. Two parameters were measured: the number of spots, assessed using Visioscan VC 98 combined with Sebufix® F16, and the percentage of area covered by sebum, measured solely with Sebufix® F16. Erythema was evaluated with the VisioFace® 1000D system (facial acne) and the Mexameter® MX18 (truncal acne), which detect changes in skin pigmentation, while cell renewal was assessed using the Visioscan VC 98 and Corneofix® F20, identifying dehydrated or damaged skin through the presence of thick and large corneocytes.
2.2.3. QoL Survey
At D0 and D56, volunteers completed a QoL survey, the Cardiff Acne Disability Index (CADI), to assess their perception of the impact of acne on their daily lives.
Subjective Satisfaction
A subjective survey was administered to assess volunteer satisfaction. The survey measured the percentage of participants who felt the product was effective and if it met their expectations.
2.2.4. Tolerance
Dermal tolerance and product safety were evaluated at each visit by rating changes in erythema, dryness, edema, oozing, comedogenicity, pigmentation alterations, and sensations of itching or stinging, using a three-point severity scale (mild, moderate, severe). Additionally, any adverse events reported since the previous visit were documented. The causality of these events was classified as unrelated, unlikely, possible, probable, definite, or not assessable.
2.3. Statistical Analysis
A descriptive statistical analysis of the results of the biometric parameters at different experimental time points was carried out, including mean, standard deviation, percentage of improvement compared to time 0, and graphical representations.
Multiple biometric measurements taken over time (consecutive measurements for each volunteer), and therefore correlated with each other, were accounted for by including random effects at the volunteer level, allowing the intercept to vary randomly between individuals. Linear mixed-effects models (LMM) were fitted to evaluate the efficacy of the treatment over 56 days (D0, D14, D28, and D56).
A normality analysis was performed; if the data showed a non-normal distribution, a Kruskal-Wallis test was applied. If the data followed a normal distribution, a parametric test (ANOVA) was used. A significance level of 0.05 (95% confidence interval) was established.
2.4. Ethical Considerations
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and complied with the International Conference on Harmonisation (ICH) guidelines for Good Clinical Practice (GCP), along with all applicable local regulatory requirements. Written informed consent was obtained from all participants prior to the initiation of any study-related procedures.
3. Results
3.1. Patient Characteristics
In the facial acne study, 42 patients were enrolled, with a mean age of 17.71 years and 57.14% females. One participant withdrew for reasons unrelated to the study, resulting in a final analysis of 41 subjects. In the truncal acne study, 41 patients were included, with a mean age of 19.59 years and 56.10% females, and all participants completed the study without dropouts.
3.2. Clinical Results
The IGA scale showed progressive reductions in acne severity, reaching statistical significance at day 56, with decreases of 26% in facial acne (p = 0.01) and 32% in truncal acne (p = 0.001). Additionally, a clinically meaningful improvement of ≥1 point in IGA score was observed in 63.16% of facial acne patients and 65.85% of truncal acne patients by the end of the study. The EGAE visual scale demonstrated similar improvements, with significant reductions of 31% for facial acne (p = 0.01) and 45% for truncal acne (p = 0.001) at day 56 (Figure 2).
Inflammatory lesions decreased over time in both studies. In facial acne, papules were significantly reduced by 24% at day 28 (p = 0.04) and 45% at day 56 (p = 0.017), while reductions in pustules, nodules, and cysts were observed but did not reach statistical significance (Figure 3). In truncal acne, inflammatory lesions showed a significant overall reduction of 44% at day 28 (p = 0.03) and 60% at day 56 (p = 0.001). Papules decreased significantly by 40% at day 28 (p = 0.005) and 58% at day 56 (p = 0.001), while pustules decreased by 66% at day 56 (p = 0.03). Nodules and cysts also declined, although not significantly (Figure 4).
3.3. Biometric Measurements
The different biometric measurements are shown in Figure 5 and Figure 6. The effect of treatment on C. acnes virulence was assessed by porphyrin fluorescence. In facial acne, porphyrin count showed a significant reduction of 27% at day 56 (p = 0.04), while porphyrin size and intensity decreased progressively without reaching statistical significance. In truncal acne, significant reductions were observed across all parameters. Porphyrin size decreased by 27% (p = 0.003), 30% (p = 0.002), and 55% (p = 0.001) at days 14, 28, and 56, respectively, while porphyrin count decreased by 29% (p = 0.02), 36% (p = 0.006), and 48% (p = 0.001) at the same timepoints. Porphyrin intensity showed a significant reduction of 14% at day 56 (p = 0.05).
Sebum-regulating efficacy was also analyzed. In facial acne, sebum levels, measured as the number of sebum spots, decreased progressively, with a significant 75% reduction at day 56 (p = 0.005). In truncal acne, sebum, evaluated as the percentage of area covered by sebum, decreased by 30%, 42%, and 47% at days 14, 28, and 56, respectively, although these changes were not statistically significant.
Erythema showed improvement throughout the treatment period in both facial and truncal acne. In facial acne, reductions were significant from day 14 (41%, p = 0.0001) and remained stable at day 28 (38%, p = 0.0001) and day 56 (35%, p = 0.0001). In truncal acne, significant decreases were also observed, with 6% at day 14 (p = 0.03), 17% at day 28 (p = 0.001), and 7% at day 56 (p = 0.005).
Cellular renewal, assessed through desquamation, showed early and sustained improvements. In facial acne, a significant reduction of 20% was observed two hours after application (p = 0.03), followed by significant decreases of 21% at day 28 (p = 0.02) and 22% at day 56 (p = 0.02). In truncal acne, reductions were progressive, with a non-significant 17% at two hours, followed by significant decreases of 21% (p = 0.03), 30% (p = 0.001), and 27% (p = 0.001) at days 14, 28, and 56, respectively.
After 56 days of product use, facial acne showed a 7% increase in pH, which was not statistically significant. In contrast, truncal acne exhibited a 5% decrease in pH over the same period, also not statistically significant.
3.4. QoL Survey
After 56 days of product use, participants with facial acne experienced a significant 14% reduction in negative feelings about having acne-prone skin (p = 0.03) and a 14% decrease in negative perceptions of their acne condition (p = 0.02). Non-significant reductions were observed in feelings of aggressiveness, frustration, or embarrassment (20%), as well as in the perceived impact of acne on daily life (11%) and social situations (6%). In participants with truncal acne, significant improvements were also observed, including reductions in negative emotions associated with acne such as aggressiveness, frustration, or embarrassment (21%, p = 0.02), negative perceptions of having acne-prone skin (19%, p = 0.01), and negative feelings about the overall acne condition (21%, p = 0.001).
3.5. Subjective Evaluation
In the subjective questionnaire, participants reported high levels of satisfaction with the product in both studies. In the facial acne study, 83% of patients felt that the product met their expectations, 85% noticed fewer skin imperfections, and 100% reported no unwanted symptoms or damage to clothing. In the truncal acne study, overall satisfaction reached 95%, with 85% of participants observing an improvement in the overall appearance of their skin, 90% perceiving a reduction in blemishes, 98% describing a non-greasy sensation, and 98% reporting no changes to their clothing or bed linens after product use, with no discoloration or damage observed.
3.6. Safety
Products demonstrated a high level of dermatological tolerance. In the facial acne study, four participants (9.76%) reported mild adverse events, including two cases of itching, one case of erythema, and two cases of increased lesions (papulo-pustular or papular). Of these, two events (itching and erythema with itching) were considered probably related to product use, while the remaining were considered possibly related. In the truncal acne study, 5% of participants reported undesirable effects, experiencing mild, self-limited reactions, including transient itching and slight erythema, particularly after application post-shower or on recent lesions. These reactions resolved within minutes and did not lead to treatment discontinuation. Only two mild adverse events were reported: one case of dryness and itching, and one case of isolated itching.
4. Discussion
The results of these two prospective clinical studies show that topical 1% H₂O₂ formulations are both effective and well tolerated for the treatment of mild to moderate facial and truncal acne. The cream-gel led to a significant reduction in facial acne severity after 56 days, with marked improvements in inflammatory lesions, antibacterial activity, sebum regulation, erythema, and desquamation. Likewise, the sprayable lotion significantly reduced truncal acne severity, inflammatory lesions, porphyrin-related parameters, erythema, and desquamation, while also showing a favorable trend toward sebum control. Collectively, these findings highlight the potential role of stabilized 1% H₂O₂ as a safe, well-tolerated, and effective therapeutic option for acne management across different body sites, offering a convenient alternative for both facial and truncal treatment.
These findings demonstrate that 1% stabilized H₂O₂ simultaneously targets key pathogenic mechanisms of acne, including inflammation, bacterial virulence, excess sebum, and impaired barrier function. Significant reductions in acne severity were observed in both trials, as measured by the widely used IGA and EGAE scales [25]. The anti-inflammatory effect was confirmed, notably through reductions in papules and other inflammatory lesions, consistent with previous reports [19,21,22,23,26]. Agrawal et al. found that H₂O₂ reduced inflammatory lesions by weeks 4 and 8 [19]. Kisiel et al. demonstrated a marked decrease in total acne lesions (p = 0.0003), particularly pustules (p = 0.002) [23]. Likewise, Muizzuddin et al. reported rapid improvements, with a 68% reduction in acne-related inflammation and 61% reduction in lesion size within just 4 days of treatment, and sustained efficacy over 6 weeks, with a 56% decrease in inflamed lesions [26]. Our results also indicate that 1% H₂O₂ effectively modulates porphyrins, biomarkers of C. acnes activity and inflammation. This modulation contributes to the reduction of C. acnes virulence, a key factor in acne pathogenesis in sebum-rich area [27], as previously demonstrated [28]. Erythema, associated with cytokine-mediated inflammation, capillary dilation, and epidermal thinning [29], showed significant reductions in both facial and truncal acne. Desquamation rapidly decreased within 2 hours in both trials, reflecting a fast-acting effect on skin renewal and barrier normalization that persisted throughout the study. Clinically, this early response may rapidly relieve visible flaking and surface irregularities, improving perceived efficacy and adherence. It may be explained by an early modulatory effect of stabilized H₂O₂ on keratinocyte differentiation and barrier homeostasis, likely mediated by its antimicrobial and anti-inflammatory properties. This fast-acting profile represents a key differentiating feature compared to conventional topical agents. Finally, sebum levels showed a downward trend, suggesting potential long-term regulation. This effect was more evident in facial acne and less pronounced in truncal acne due to naturally lower baseline sebum [10]. Together, these multifactorial effects explain the rapid and sustained clinical improvements observed in both facial and truncal acne.
Beyond objective clinical improvements, both studies demonstrated substantial benefits in patient-reported outcomes and tolerability, which are critical for real-world acne management. Acne and its associated lesions are known to significantly impair QoL and, in severe cases, contribute to depression or suicidal ideation [5]. Facial acne is particularly impactful due to its visibility during social interactions [9]. In facial acne, the treatment significantly reduced negative feelings about having acne-prone skin and negative perceptions of the condition itself. Similarly, in truncal acne, participants reported meaningful reductions in negative emotional responses, including frustration and embarrassment, alongside improvements in perceptions of overall acne severity. High levels of satisfaction were observed in both studies, with the majority of participants reporting a noticeable reduction in skin imperfections. Nearly all participants noted the absence of unwanted symptoms or fabric staining, an important advantage compared with conventional therapies such as benzoyl peroxide.18 These findings underscore that 1% stabilized H₂O₂ formulations not only provide robust clinical efficacy but also offer excellent tolerability and positive patient experience, factors that are essential to enhancing adherence and optimizing long-term outcomes in routine clinical practice.
Management of acne vulgaris, whether facial or truncal, is guided by disease severity. Mild cases are typically managed with topical agents, while moderate cases often require combination therapies, including systemic antibiotics [30]. Topical benzoyl peroxide is widely recommended across clinical guidelines, either as monotherapy or as an adjuvant. However, its use is frequently associated with local adverse effects such as dryness, irritation, erythema, eczema, application-site pain, and pruritus. This is thought to result from the rapid breakdown of benzoyl peroxide into H₂O₂ and benzoic acid, the latter being primarily responsible for irritation [14,15]. A recent Cochrane review reported that 11% of patients treated with benzoyl peroxide experienced adverse events [13]. In contrast, H₂O₂ formulations have demonstrated lower rates of adverse events (approximately 2%) in previous studies [19,21,22,24] making them a well-tolerated alternative. Different H₂O₂ formulations are currently available for the treatment of acne vulgaris [14,31] and our findings reinforce this profile, showing that both the facial cream-gel and the sprayable truncal lotion significantly reduce acne severity, while maintaining excellent dermatological tolerability. Furthermore, the sprayable format facilitates application to large or hard-to-reach areas, including hairy regions of the trunk, addressing practical challenges in truncal acne management [32]. These results support 1% stabilized H₂O₂ as an effective, safe, and patient-friendly alternative to benzoyl peroxide for mild to moderate acne.
5. Conclusions
This investigation demonstrates that the two novel 1% H₂O₂ topical formulations, a cream-gel for facial acne and a sprayable lotion for truncal acne, are safe, well-tolerated, and effective for mild to moderate acne. By targeting multiple pathogenic mechanisms, including inflammation, bacterial virulence, erythema, and desquamation, they provide rapid and clinically meaningful improvements in skin health and QoL. The results support the use of these formulations as promising alternatives to topical benzoyl peroxide in mild to moderate acne, with minimal associated side effects. Overall, these findings support the practical integration of the 1% H₂O₂ treatments into routine clinical practice as effective, patient-friendly alternatives or complements to existing therapies.
Author Contributions
HM, ML, LM and CN contributed equally to the conceptualization, methodology and supervision, EM and MO to formal analysis, data interpretation and investigation; HM, ML, CN, EM, LM, MO, CR and AR contributed equally to writing-review and editing, input of their expertise, and final approval of the version to be published. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by Laboratorio Reig Jofre S.A., Sant Joan Despi (Barcelona), Spain.
Institutional Review Board Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and the International Conference on Harmonization (ICH) Good Clinical Practices, and in compliance with local regulatory requirements. This study did not require approval from an ethics committee because the evaluated product is a topical cosmetic formulation containing hydrogen peroxide at a concentration permitted under the EU Cosmetics Regulation (EC) No. 1223/2009. The study procedures involved only non-invasive application consistent with normal cosmetic use, without any medical intervention or collection of biological samples. In accordance with established guidance on cosmetic product testing in the EU, studies assessing safety, tolerability, and cosmetic performance under minimal-risk conditions are not classified as clinical research and therefore do not fall under the scope of ethics committee review.
Informed Consent Statement
All subjects provided written informed consent prior to study procedures and all the images included in the article have consent for their publication.
Acknowledgments
This research was supported by Laboratorio Reig Jofre S.A. We would like to thank Dr. Goya Análisis, S.L. for conducting the statistical analysis, and Ángel Ramírez and Cèlia Torres from Alta Medical Services for their medical writing support.
Conflicts of Interest
The authors of this manuscript have the following competing interests: HM, ML, CN, CR, LM, AR are employed by Laboratorio Reig Jofre S.A. MO is employed by Dr. Goya Análisis, S.L.
References
- Heng AHS, Chew FT. Systematic review of the epidemiology of acne vulgaris. Sci Rep. 2020;10:5754. [CrossRef]
- Jin Z, Song Y, He L. A review of skin immune processes in acne. Front Immunol. 2023;14. [CrossRef]
- Dreno B, Bordet C, Seite S, Taieb C. Acne relapses: impact on quality of life and productivity. Journal of the European Academy of Dermatology and Venereology. 2019;33(5):937-943. [CrossRef]
- Vasam M, Korutla S, Bohara RA. Acne vulgaris: A review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023;36:101578. [CrossRef]
- Chilicka K, Rusztowicz M, Rogowska AM, Szyguła R, Asanova B, Nowicka D. Efficacy of Hydrogen Purification and Cosmetic Acids in the Treatment of Acne Vulgaris: A Preliminary Report. J Clin Med. 2022; 11(21):6269. [CrossRef]
- Zaenglein AL. Acne Vulgaris. Solomon CG, ed. New England Journal of Medicine. 2018;379(14):1343-1352. [CrossRef]
- Tan J, Beissert S, Cook-Bolden F, Chavda R, Harper J, Hebert A, et al. Impact of facial and truncal acne on quality of life: A multi-country population-based survey. JAAD Int. 2021;3:102–10. [CrossRef]
- Kim BR, Chun MY, Kim SA, Youn SW. Sebum Secretion of the Trunk and the Development of Truncal Acne in Women: Do Truncal Acne and Sebum Affect Each Other? Dermatology. 2015;231(1):87–93. [CrossRef]
- Szepietowska M, Dąbrowska A, Nowak B, Skinderowicz K, Wilczyński B, Krajewski P, et al. Prevalence and quality of life of facial acne: a cross-sectional study in high school students in Poland. Adv Dermatol Allergol. 2022;39(6):1035-1039. [CrossRef]
- Woo YR, Kim HS. Truncal Acne: An Overview. Journal of Clinical Medicine. 2022; 11(13):3660. [CrossRef]
- Cui H, Feng C, Guo C, Duan Z. Development of Novel Topical Anti-Acne Cream Containing Postbiotics for Mild-to-Moderate Acne. Indian J Dermatol. 2022;67(6):667-673. [CrossRef]
- Reynolds R V., Yeung H, Cheng CE, Cook-Bolden F, Desai SR, Druby KM, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):1006.e1-1006.e30. [CrossRef]
- Yang Z, Zhang Y, Lazic Mosler E, Hu J, Li H, Zhang Y, et al. Topical benzoyl peroxide for acne. Cochrane Database of Systematic Reviews. 2020; 3(3):CD011154. [CrossRef]
- Ricci F, Masini F, Fossati B, Frascione P, De Waure C, Capizzi R, et al. Combination therapy with hydrogen peroxide (4%), salicylic acid (0.5%) and D-panthenol (4%): efficacy and skyn tolerability in common acne vulgaris during sun exposure period. Eur Rev Med Pharmacol Sci. 2016;20(2):232-6.
- Egele K, Drexler H, Fartasch M, van Kampen V, Merk HF, Nowak D, et al. Benzoyl Peroxide’s Sensitisation Potential and Potency in Experimental Methods and Review of Contact Allergy and Allergic Contact Dermatitis. Contact Dermatitis. 2025;92(6):436-445. [CrossRef]
- Tan J, Alexis A, Baldwin H, Beissert S, Bettoli V, Del Rosso J, et al. Gaps and recommendations for clinical management of truncal acne from the Personalising Acne: Consensus of Experts panel. JAAD Int. 2021;5:33–40. [CrossRef]
- Ko JY, Song CH, Kim KJ, Kim NI, Kim JE, Kim HS, et al. Consensus Report on Truncal Acne: The Korean Acne and Rosacea Society Experts Panel. Ann Dermatol. 2024;36(1):35. [CrossRef]
- Poli F, Auffret N, Leccia M -T., Claudel J -P., Dréno B. Truncal acne, what do we know? Journal of the European Academy of Dermatology and Venereology. 2020;34(10):2241-2246. [CrossRef]
- Agrawal M, Saxena A, Tripathi A, Dey VK, Kushwaha S, Shrivastava P, et al. Evaluation of safety and efficacy of hydrogen peroxide stabilized cream for treatment of mild to moderate acne vulgaris in comparison with benzoyl peroxide gel-double blinded, randomized control study. IP Indian Journal of Clinical and Experimental Dermatology. 2020;6(3):217-221. [CrossRef]
- Veraldi S, Micali G, Berardesca E, Dall’Oglio F, Sinagra JL, Guanziroli E. Results of a Multicenter, Randomized, Controlled Trial of a Hydrogen Peroxide-based Kit versus a Benzoyl Peroxide-based Kit in Mild-to-moderate Acne. J Clin Aesthet Dermatol. 2016;9(10):50-54.
- Capizzi F, Landi F, Milani M, Amerio P. Skin tolerability and efficacy of combination therapy with hydrogen peroxide stabilized cream and adapalene gel in comparison with benzoyl peroxide cream and adapalene gel in common acne. A randomized, investigator-masked, controlled trial. British Journal of Dermatology. 2004;151(2):481-484. [CrossRef]
- Milani M, Bigardi A, Zavattarelli M. Efficacy and Safety of Stabilised Hydrogen Peroxide Cream (Crystacide) in Mild-to-Moderate Acne Vulgaris: A Randomised, Controlled Trial Versus Benzoyl Peroxide Gel. Curr Med Res Opin. 2003;19(2):135-8. [CrossRef]
- Kisiel K, Dębowska R, Dzilińska K, Radzikowska A, Pasikowska-Piwko M, Rogiewicz K, et al. New H2O2 dermocosmetic in acne skin care. Our Dermatology Online. 2018;9(e):e3.1-e3.6. [CrossRef]
- Murphy EC, Friedman AJ. Hydrogen peroxide and cutaneous biology: Translational applications, benefits, and risks. J Am Acad Dermatol. 2019;81(6):1379-1386. [CrossRef]
- Bae IH, Kwak JH, Na CH, Kim MS, Shin BS, Choi H. A Comprehensive Review of the Acne Grading Scale in 2023. Ann Dermatol. 2024;36(2):65-73. [CrossRef]
- Muizzuddin N, Schnittger S, Maher W, Maes DH, Mammone T. Enzymatically generated hydrogen peroxide reduces the number of acne lesions in acne vulgaris. J Cosmet Sci. 2013;64(1):1-8.
- Lee YB, Byun EJ, Kim HS. Potential Role of the Microbiome in Acne: A Comprehensive Review. J Clin Med. 2019;8(7):987. [CrossRef]
- Hernandez P, Sager B, Fa A, Liang T, Lozano C, Khazzam M. Bactericidal efficacy of hydrogen peroxide on Cutibacterium acnes. Bone Joint Res. 2019;8(1):3-10. [CrossRef]
- Amiri R, Khalili M, Mohammadi S, Iranmanesh B, Aflatoonian M. Treatment protocols and efficacy of light and laser treatments in post-acne erythema. J Cosmet Dermatol. 2022;21(2):648-656. [CrossRef]
- Kaewsanit T, Chakkavittumrong P, Waranuch N. Clinical Comparison of Topical 2.5% Benzoyl Peroxide plus 5% Niacinamide to 2.5% Benzoyl Peroxide Alone in the Treatment of Mild to Moderate Facial Acne Vulgaris. J Clin Aesthet Dermatol. 2021;14(6):35-41.
- Fabbrocini G, Panariello L. Efficacy and tolerability of a topical gel containing 3% hydrogen peroxide, 1.5% salicylic acid and 4% D-panthenol in the treatment of mild-moderate acne. G Ital Dermatol Venereol. 2016;151(3):287-291.
- Bikowski J. A review of the safety and efficacy of benzoyl peroxide (5.3%) emollient foam in the management of truncal acne vulgaris. J Clin Aesthet Dermatol. 2010;3(11):26–9.
Figure 1.
Decomposition of benzoyl peroxide into benzoic acid hydrogen peroxide.

Figure 2.
Evolution of facial (A) and truncal (B) acne severity measured by IGA or EGAE score over the course of the study, expressed as mean ± standard deviation (SD) at different time points. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD).
Figure 2.
Evolution of facial (A) and truncal (B) acne severity measured by IGA or EGAE score over the course of the study, expressed as mean ± standard deviation (SD) at different time points. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD).
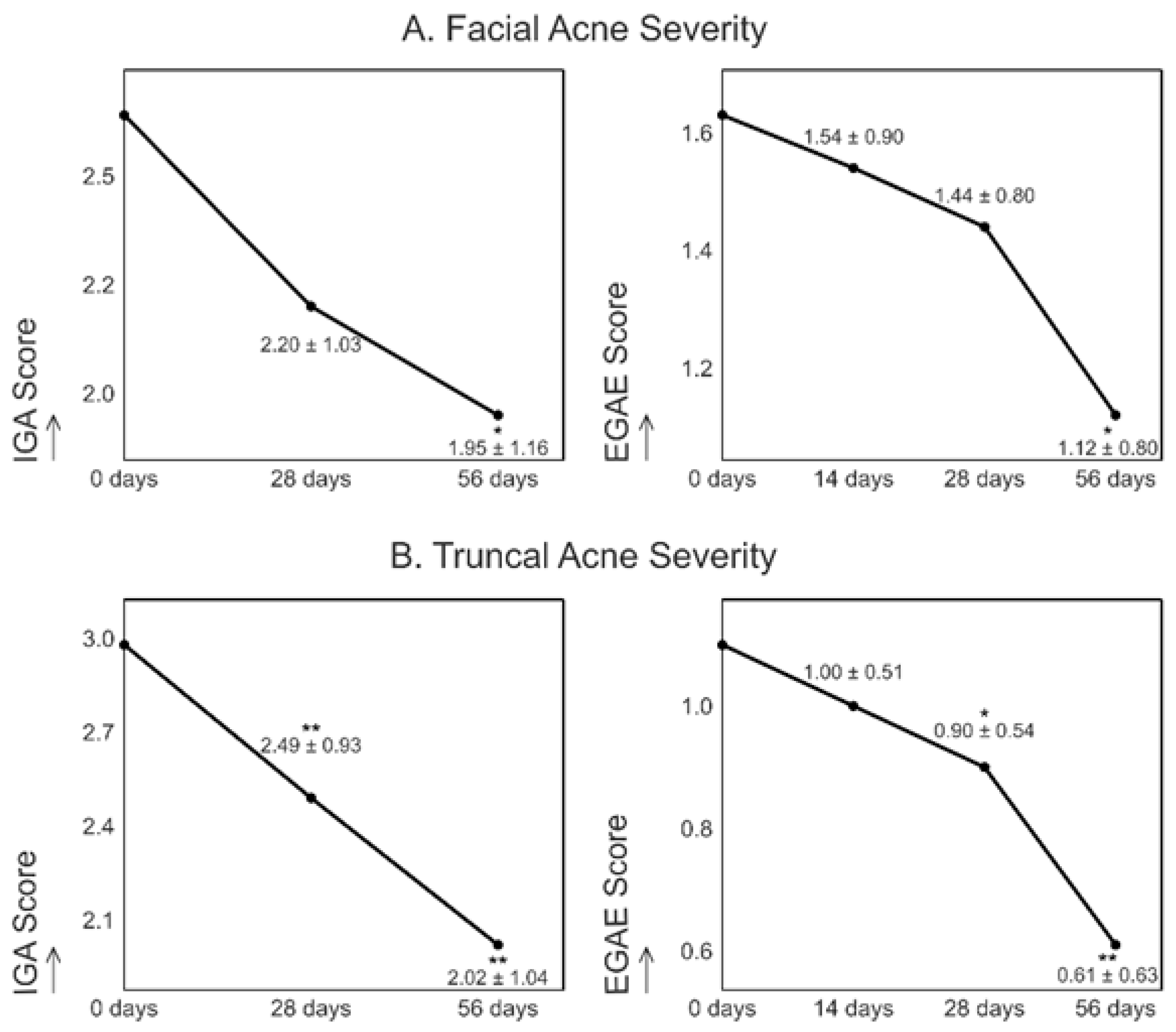
Figure 3.
Average changes in inflammatory lesions among facial acne participants: papules (A), pustules (B), nodules (C), and cysts (D), expressed as mean ± SD at different time points. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD).
Figure 3.
Average changes in inflammatory lesions among facial acne participants: papules (A), pustules (B), nodules (C), and cysts (D), expressed as mean ± SD at different time points. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD).
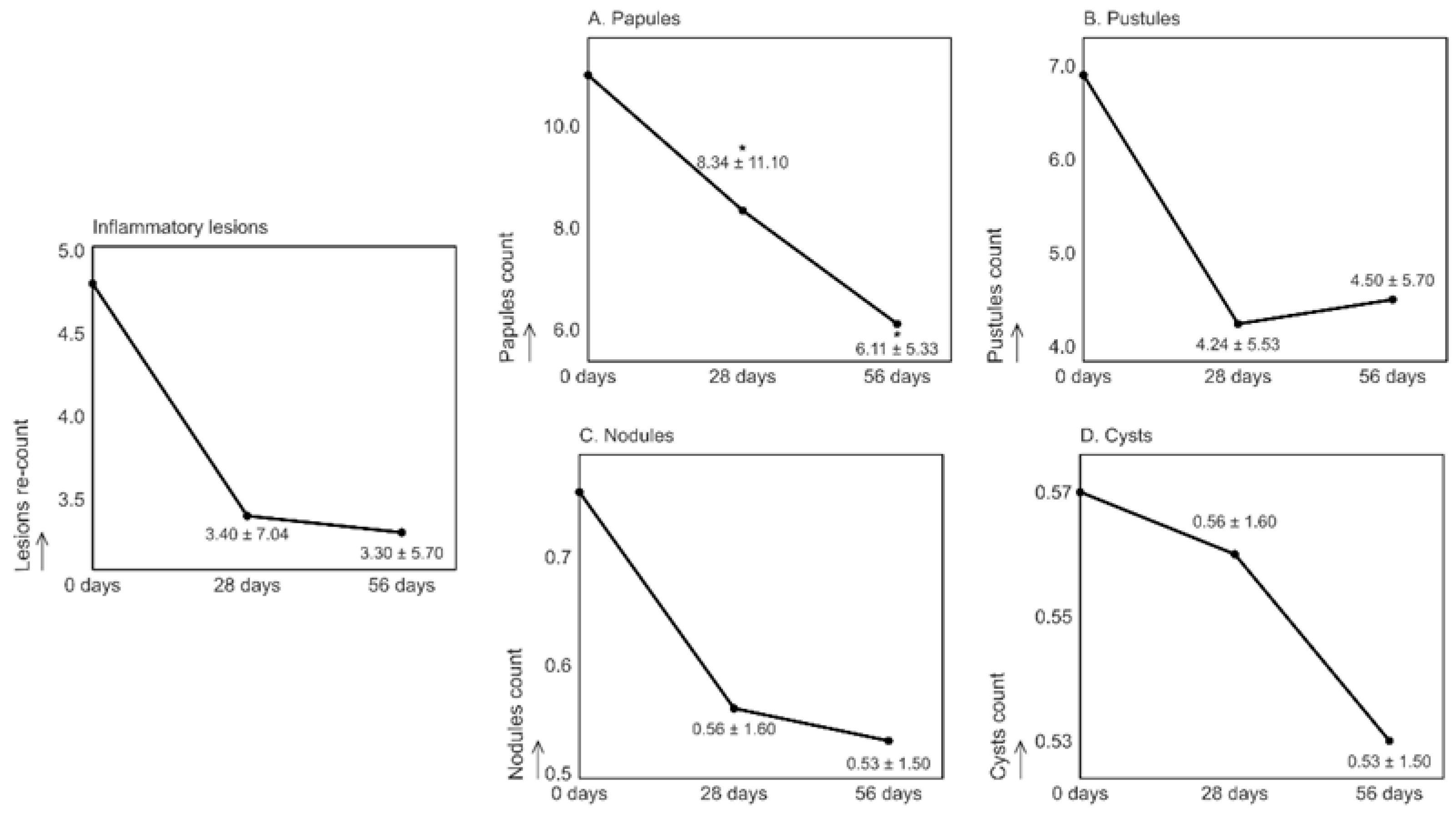
Figure 4.
Average changes in inflammatory lesions among truncal acne participants: papules (A), pustules (B), nodules (C), and cysts (D), expressed as mean ± SD at different time points. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD).
Figure 4.
Average changes in inflammatory lesions among truncal acne participants: papules (A), pustules (B), nodules (C), and cysts (D), expressed as mean ± SD at different time points. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD).
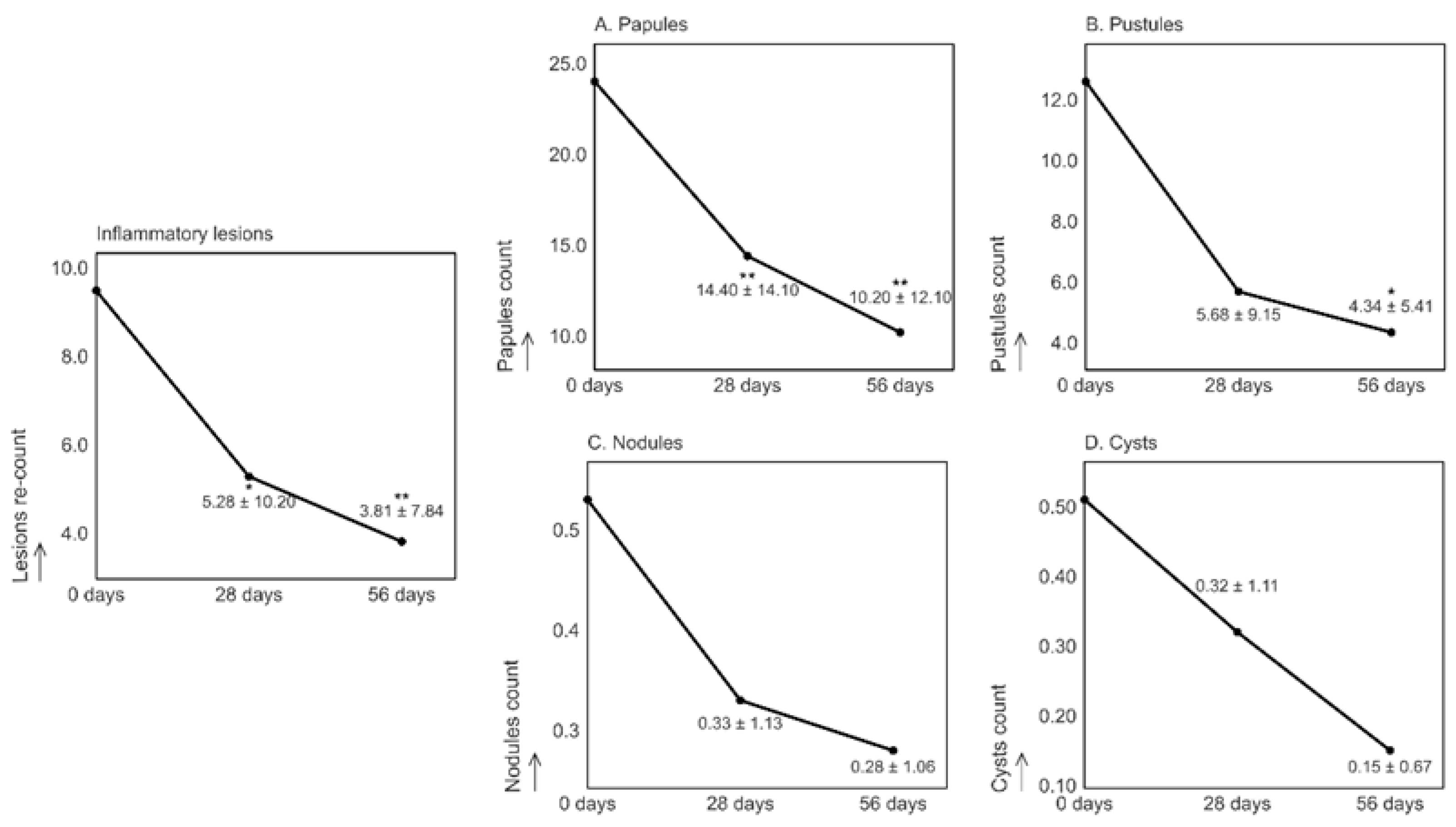
Figure 5.
Biometric measurements in facial acne: porphyrin count (A), porphyrin size (B), porphyrin intensity (C), sebum levels [sebum spots] (D), erythema (E), and skin desquamation (F). Data are presented as mean ± SD. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD). *** p <0.001 versus baseline (mean ± SD).
Figure 5.
Biometric measurements in facial acne: porphyrin count (A), porphyrin size (B), porphyrin intensity (C), sebum levels [sebum spots] (D), erythema (E), and skin desquamation (F). Data are presented as mean ± SD. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD). *** p <0.001 versus baseline (mean ± SD).
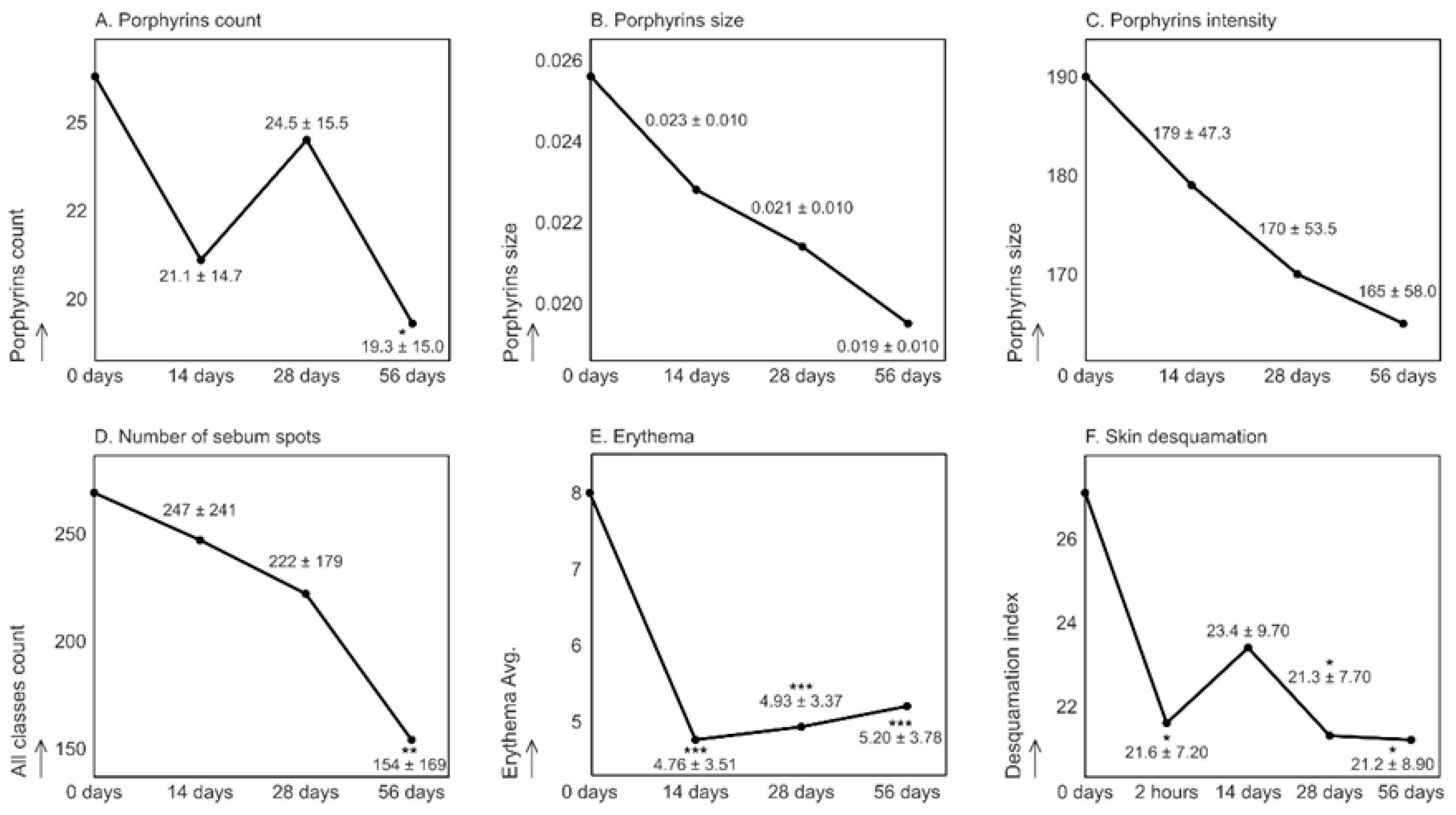
Figure 6.
Biometric measurements in truncal acne: porphyrin count (A), porphyrin size (B), porphyrin intensity (C), sebum levels [area %] (D), erythema (E), and skin desquamation (F). Data are presented as mean ± SD. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD). *** p <0.001 versus baseline (mean ± SD).
Figure 6.
Biometric measurements in truncal acne: porphyrin count (A), porphyrin size (B), porphyrin intensity (C), sebum levels [area %] (D), erythema (E), and skin desquamation (F). Data are presented as mean ± SD. *p<0.05 versus baseline (mean ± SD). **p <0.01 versus baseline (mean ± SD). *** p <0.001 versus baseline (mean ± SD).
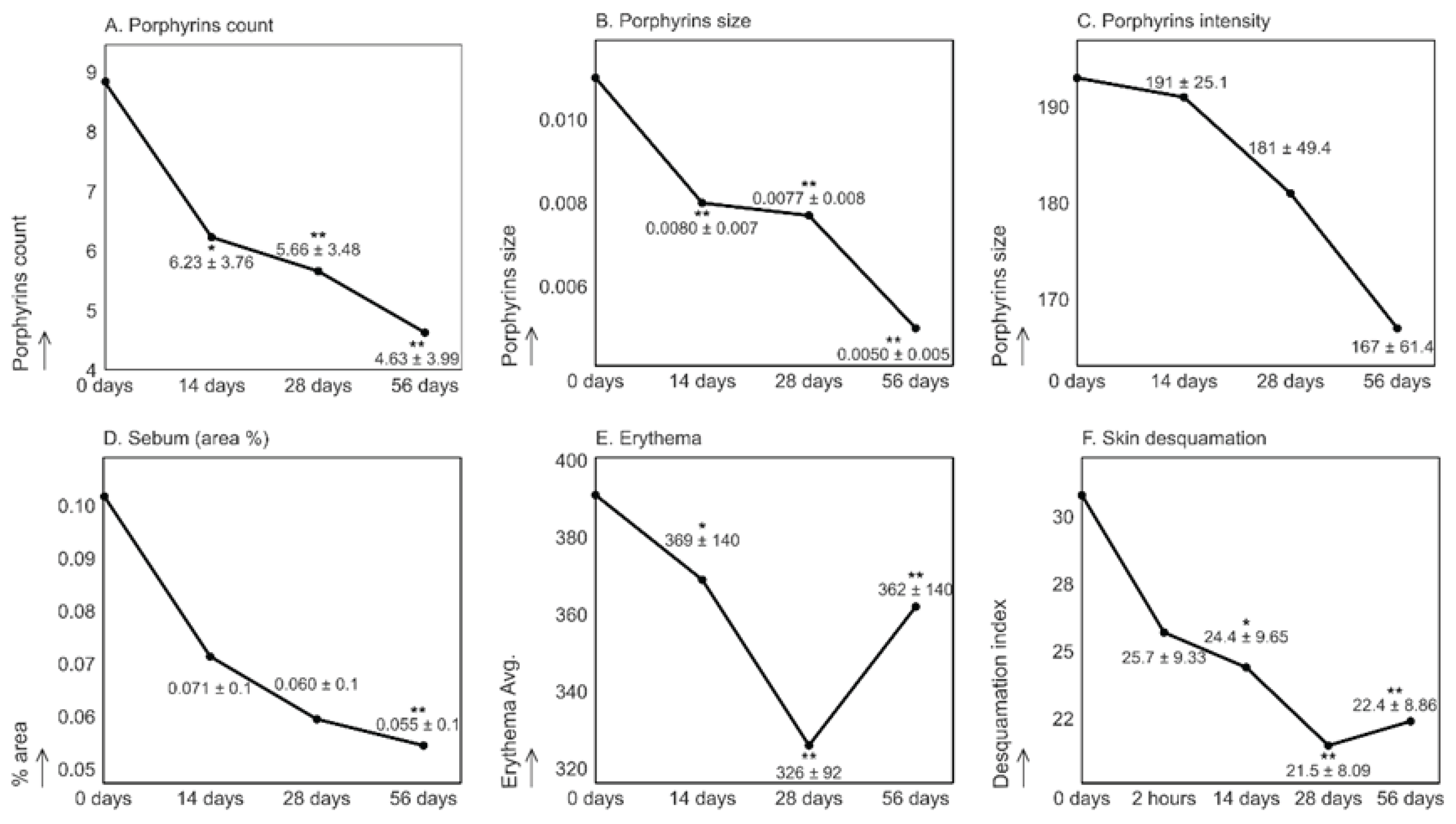

Table 1.
Summary of the measurements of the studies.
| Test | Time | Method | Zone |
|---|---|---|---|
| Skin pH regulation | D0, D14, D28 and D56 | Skin-pH-Meter PH 905 | Cheek + Back or chest |
| Anti-acne | D0, D14, D28 and D56 | Visiopor® PP 34 | Facial acne area + Back or chest |
| Sebum- regulating | D0, D14, D28 and D56 | Sebufix® F 16 Visioscan VC 98 |
Chin + Back or chest |
| Anti- erythema |
D0, D14, D28 and D56 | Visioface® 1000D Mexameter® MX18 | Acne area and control area + Back or chest |
| Cell renewal |
D0, D0+2H, D14, D28 and D56 | Corneofix® F20 plus | Cheek + Back or chest |
| Skin texture | D0, D14, D28 and D56 | Visioscan® VC 20 plus | Cheek |
| Pore analysis |
D0, D14, D28 and D56 | Visioface® 1000D | Forehead |
| Photographs | D0, D14, D28 and D56 | Canon EOS M200 Camera |
Forehead and profiles + Back or chest |
| Dermatological anti-acne efficacy | D0, D28 and D56 | Dermatological scoring, IGA scale | Whole face + Back or chest |
| D0, D14, D28 and D56 | EGAE scale | ||
| Tolerance evaluation | D56 | Dermatological evaluation | Whole face + Back or chest |
| Quality of life | D0 and D56 | CADI Survey | - |
| Subjective efficacy | D56 | Volunteer subjective survey | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



