
Submitted:
20 January 2026
Posted:
21 January 2026
You are already at the latest version
Abstract
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a type 2 inflammatory disease effectively treated with dupilumab, a monoclonal antibody that inhibits IL-4 and IL-13 signaling. Although efficacy of dupilumab in controlling upper airway inflammation is well established, concerns have emerged regarding its potential cardiovascular effects. Emerging evidence suggests that IL-4/IL-13 signaling plays a protective role in post-myocardial infarction remodeling by promoting anti-inflammatory macrophage polarization, angiogenesis, and controlled fibrosis, especially during the early healing phase. Pharmacological blockade of the IL-4/IL-13 signaling pathway, such as that induced by dupilumab, may theoretically impair myocardial repair mechanisms, particularly in male patients who appear more responsive to these cytokines. Although rare, dupilumab-associated hypereosinophilia and myocarditis have been reported. In patients with pre-existing ischemic heart disease or heart failure, a multidisciplinary risk–benefit evaluation should be considered. Concomitant use of cardioprotective agents such as sacubitril/valsartan or SGLT2 inhibitors may help mitigate potential cardiac risks. Future studies are needed to clarify the safety and therapeutic implications of combining dupilumab with cardiovascular therapies in patients with coexisting CRSwNP and heart disease. The aim of this review is to explore the available data on the cardiovascular impact of dupilumab and to provide possible future perspectives.
Keywords:
chronic rhinosinusitis with nasal polyps
; myocardial disease
; dupilumab
; eosinophilic myocarditis
1. Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) and eosinophilic otitis media (EOM) are clinical manifestations of type 2 (Th2-mediated) inflammation, characterized by mechanisms of type IVb hypersensitivity. This group includes diseases such as rheumatoid arthritis, atopic dermatitis, CRSwNP, and asthma (T2 endotype). Th2 cells play a central role, driven by cytokines including IL-4, IL-13, IL-5, IL-9, and IL-31. These cytokines stimulate B cells to class switch to IgE (primarily through IL-4 and IL-13) and mediate eosinophilia (mainly via IL-5), leading to inflammation and tissue damage. Eosinophils are key effector cells in this pathway, infiltrating inflamed tissues where they promote activation of cytokine and chemokine cascades and release cytotoxic granules that contribute to cell death, tissue injury, and chronic inflammation [1,2]. Their pathogenic role is particularly evident in severe eosinophilic asthma, where eosinophils sustain inflammatory signaling and contribute to mucosal remodeling [3].
CRSwNP is a complex and often refractory inflammatory disease of the upper airways that poses significant therapeutic challenges. The persistent and relapsing nature of the underlying inflammation, driven by type 2 immune responses, complicates long-term management and negatively affects quality of life. Increasing evidence has highlighted the pivotal role of Th2 cytokines, particularly IL-4 and IL-13, which perpetuate chronic eosinophilic inflammation in the sinonasal mucosa changing radically the management of this disease.
Recent advances in immunomodulatory therapies have led to the development of targeted biological agents originally indicated for severe eosinophilic asthma, including mepolizumab, reslizumab, and benralizumab, which are now also used in the management of CRSwNP and other type 2 inflammatory conditions [4].
Among these biologic therapies, dupilumab, a fully human monoclonal IgG4 antibody, specifically targets the IL-4 receptor alpha subunit (IL-4Rα), thereby inhibiting both IL-4 and IL-13 signaling. This dual blockade addresses the core inflammatory drivers of type 2 inflammation, offering a more precise and effective therapeutic option. Multiple systematic reviews and meta-analyses have shown that dupilumab significantly improves both subjective (nasal congestion, smell loss, QoL) and objective (nasal polyp score, sinus opacification) outcomes in patients with severe CRSwNP, with a favorable safety profile [5,6,7,8,9,10,11,12,13,14,15].
Although the efficacy of dupilumab in controlling upper airway inflammation is well established, the systemic effects, particularly on the cardiovascular system, remain poorly understood. The IL-4 and IL-13 pathways, though classically associated with allergic inflammation, are increasingly recognized for their complex roles in cardiovascular physiology and pathology, including vascular remodeling, fibrosis, endothelial function, and post-infarction repair.
Recent preclinical and clinical studies suggest a potential cardioprotective role for IL-4/IL-13 signaling in ischemic heart disease. Against this background, the inhibition of these cytokines by dupilumab raises important concerns regarding possible cardiovascular risks, particularly in patients with pre-existing ischemic heart disease or heart failure [16,17].
This work aims to explore the emerging evidence regarding the cardiovascular implications of dupilumab, evaluating experimental models, real-world clinical data, and mechanistic insights into IL-4/IL-13 signaling in the heart. A better understanding of these effects is essential for balancing the benefits of dupilumab in inflammatory airway disease with the need for cardiovascular safety in at-risk populations.
2. Potential Myocardial Damage Associated with Dupilumab: Hypereosinophilia and Eosinophilic Myocarditis
Currently, the mechanisms underlying potential myocardial injury associated with dupilumab therapy remain speculative and require further elucidation. One hypothesized pathway pertains to the drug’s established impact on peripheral eosinophil dynamics. Although dupilumab effectively inhibits eosinophil trafficking into tissues through blockade of IL-4 and IL-13 signaling, it does not inhibit eosinophil production or release. As a result, many patients experience a transient rise in circulating eosinophil levels during the initial phases of treatment [18].
Clinical trials and post-marketing data have reported varying rates of dupilumab-associated hypereosinophilia (defined as ≥1.5×10⁹ cells/L), depending on the indication. The highest incidence has been observed in patients with oral corticosteroid (OCS)-dependent severe asthma (35.9%), followed by moderate-to-severe asthma (14.7%), and CRSwNP (7.2%) [19,20,21]. Although most cases are asymptomatic, there have been reports of symptomatic hypereosinophilia, including rare but serious complications such as eosinophilic granulomatosis with polyangiitis (EGPA) and eosinophilic myocarditis. In the CRSwNP population specifically, symptomatic hypereosinophilia was reported in 0.7% of patients (3 out of 438), with two cases attributed to EGPA [5].
Given that eosinophilic myocarditis is a potentially life-threatening condition characterized by eosinophilic infiltration of the myocardium and subsequent myocardial injury, these findings raise concerns about a possible link between dupilumab-induced hypereosinophilia and cardiovascular adverse events. Although rare, emerging case reports suggested a temporal association between dupilumab initiation and acute myocarditis, highlighting the need for heightened clinical awareness and further mechanistic research.
A case report in the literature describes a 48-year-old man who developed suspected acute eosinophilic myocarditis temporally associated with dupilumab administration. His symptoms began one day after the first injection and progressively worsened, resulting in hospitalization on day 10. He presented with chest pain radiating to the left shoulder (worsened by leaning forward and deep breathing), fever, fatigue, myalgia, palpitations, and hypotension. Laboratory and imaging findings revealed elevated troponin levels, hypereosinophilia, electrocardiographic abnormalities, and a significantly reduced left ventricular ejection fraction (LVEF) of 30%. Based on the clinical presentation and timing, the cardiology team diagnosed hypersensitivity myocarditis, a drug-related form of eosinophilic myocarditis in which an autoimmune reaction causes myocardial inflammation. The diagnosis was made without endomyocardial biopsy or cardiac magnetic resonance imaging (CMRI), as it would not have changed the management approach. Dupilumab was permanently discontinued, and the patient was treated with intravenous methylprednisolone followed by high-dose oral prednisone (60 mg/day), which was tapered gradually. His symptoms regressed and the LVEF (50-55%) improved at 4 weeks. The strong temporal association between drug initiation and symptom onset supported the suspicion of dupilumab-induced myocarditis [22].
Additionally, in a real-world observational study by Strong et al., which monitored 69 consecutive adult patients initiating dupilumab for severe asthma, a single case of symptomatic hypereosinophilia (2.0×10⁹ cells/L) was reported at 6 months. The patient reported clinical features suggestive of eosinophilic granulomatosis with polyangiitis and cardiac involvement evident on CMRI. Although the patient had been on maintenance OCS throughout the treatment period, dupilumab was permanently discontinued following this event. Notably, eosinophil counts at baseline and at week 16 had been within normal limits (0.3×10⁹ and 0.02×10⁹ cells/L, respectively), with no available data at week 4 [23].
Two randomized controlled trials, LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52, evaluated the efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps. A total of 143 patients received dupilumab and 133 received placebo; all participants received at least one dose of the study drug. In these studies, which included routine 12-lead electrocardiographic monitoring, no cardiovascular adverse events, such as myocarditis, arrhythmias, myocardial infarction, or heart failure, were reported. The most commonly reported adverse events were nasopharyngitis, worsening nasal polyps (requiring surgery or systemic corticosteroids), headache, worsening of asthma, epistaxis, and injection-site erythema, many of which were actually more frequent in the placebo group. Over the 52-week treatment period in SINUS-52, events such as cough, bronchitis, arthralgia, accidental overdose, and injection-site reactions were slightly more frequent in patients treated with dupilumab. Notably, transient blood eosinophilia was observed, likely due to the inhibition of eosinophil tissue migration rather than increased production or release [21].
3. IL-4 and IL-13 and Impact on Myocardial Repair: Potential Myocardial Damage Associated with Dupilumab
3.1. IL-4 and IL-13: Receptors, Signaling Pathways, and Immunomodulatory Functions
Interleukins are cytokines primarily produced by leukocytes, capable of regulating both immunity and non-hematopoietic cellular processes. Besides T cells, many other cell types, including basophils, natural killer cells, type 2 innate lymphoid cells, mast cells, and eosinophils, produce IL-4 and IL-13. IL-4 and IL-13 are classically known for their role in type II T cell-mediated immunity and are well recognized as products of T-helper 2 (TH2) cells. IL-4 and IL-13 can activate B cells to promote immunoglobulin class switching toward the production of IgG1, which tags cells for phagocytic destruction, and IgE, which induces eosinophil and basophil degranulation [24]. Furthermore, IL-4 and IL-13 are well known for inducing macrophage polarization toward the M2a subtype of alternatively activated macrophages, which are generally associated with anti-inflammatory, tissue-repairing, and pro-angiogenic functions. Both IL-4 and IL-13 signal through the type II receptor composed of IL-4Rα and IL-13Rα1, activating pathways like JAK1/STAT6. The efficiency and downstream signaling depend on the ligand-receptor binding affinities and receptor availability on the cell surface. IL4/13 signaling in peripheral tissues generally stimulates cell proliferation, which can lead to beneficial effects like wound healing and tissue regeneration, but in many cases, it may also worsen disease progression by promoting pathological fibrosis [25].
3.2. Cardioprotective Roles of IL-4/IL-13 Signaling After Myocardial Infarction
Beyond their established roles in immune modulation, IL-4 and IL-13 are increasingly recognized for their involvement in tissue-specific repair processes, including in the cardiovascular system. Myocardial infarction (MI) can lead to heart failure (HF) due to the replacement of functional myocardium with fibrotic scar tissue. Inflammation following MI triggers the production of various cytokines, including IL-4 and IL-13, which are increasingly recognized as key regulators of post-injury cardiac remodeling. Notably, IL-13 expression in the heart rises significantly after MI, peaking between day 3 and day 7, aligning with the early phases of healing and suggesting a reparative role. Observational studies in humans have shown that higher IL-13 serum levels after MI correlate with improved left ventricular ejection fraction, while expression of the IL-4Rα/IL-13Rα1 receptor complex is significantly downregulated in patients with heart failure, associations that support a link between diminished IL-4/IL-13 signaling and adverse cardiac outcomes [26]. Moreover, Alvarez-Argote et al. demonstrated a central role for IL-13 signaling to macrophages in the response to post-MI injury. Using the neonatal mouse model of cardiac regeneration, they identified a pro-reparative signaling axis, IL-13/IL-4Rα, which declines markedly with age. They showed that reactivating this pathway in adult cardiac macrophages improves post-MI outcomes, suggesting that targeting IL-13 signaling in macrophages could represent a promising therapeutic strategy for ischemic heart failure in humans [27]. In this study, IL4Ra deletion in adult mice resulted in significant cardiac dilation and reduced LVEF at 28 days post-MI, compared to control mice, without affecting survival, body weight, scar size, or cardiomyocyte cross-sectional area [27].
Interestingly, some retrospective studies report elevated IL-13 levels in patients with chronic HF, correlating instead with functional decline; this apparent contradiction may reflect compensatory cytokine upregulation in response to receptor downregulation, though definitive data elucidating the underlying mechanisms are still lacking [28].
Insights from animal models offer stronger causal evidence for a cardioprotective role of IL-4/IL-13 signaling. Genetic deletion of IL-13Rα1 in uninjured mice results in systolic dysfunction, while IL-13 knockout mice display impaired post-MI recovery, marked by increased mortality, excessive fibrosis, and reduced recruitment of reparative immune cells [29,30]. Monocytes and macrophages (MUs) are the dominant immune cells involved in cardiac remodeling after MI, undergoing a biphasic response: initial proinflammatory Ly6cHI monocyte infiltration peaks between days 3 and 4, followed by a phenotypic transition to reparative MUs that facilitate angiogenesis and fibrosis. IL-4 and IL-13 drive this transition by signaling through the IL-4Rα receptor on MUs, polarizing them toward an M2a (alternatively activated) phenotype associated with anti-inflammatory and tissue-reparative functions. After MI, IL-4Rα expression increases in MUs, particularly in male mice, suggesting heightened cytokine responsiveness during healing [31,32,33,34,35,36].
Mouse models with myeloid-specific deletion of IL-4Rα demonstrate significantly impaired cardiac recovery, disorganized scarring, and thinner fibrotic tissue, underscoring the critical role of IL-4/13 in orchestrating appropriate MU function. Additional evidence shows that depletion of hepcidin in MUs enhances IL-4/13 expression and improves post-MI cardiac outcomes, but when IL-4/13 are co-deleted, these benefits are abolished. Collectively, these findings reinforce the essential role of IL-4/13 signaling in MU-driven cardiac repair. While most current data center on monocyte-derived macrophages, the role of IL-4/13 in modulating cardiac-resident MUs remains an open and promising avenue for future research [37,38,39].
3.3. Sex-Specific Effects of IL-4/IL-13 Signaling in Post-MI Cardiac Repair
In murine models, global deletion of IL-13 significantly impairs cardiac recovery after MI in male mice, leading to worsened cardiac function, increased fibrosis, and reduced survival. In contrast, female mice show less or no impairment, suggesting that IL-13 has a more protective role in males or that different repair mechanisms operate between sexes. These differences indicate that IL-4/IL-13 signaling may have sex-specific effects on the heart [29,30].
3.4. Impact of Dupilumab-Mediated IL-4/IL-13 Receptor Blockade on Cardiac Function
Recently, since IL4Ra signaling has been shown to protect against the development of heart failure after myocardial infarction in mice, Alvarez-Argote et al. investigated whether systemic IL4Ra blockade with dupilumab affects the incidence of cardiovascular diseases. They included data from 79 healthcare centers and performed a propensity score matching (PSM) analysis, resulting in 30,501 matched pairs of patients treated or not treated with dupilumab. By analyzing the occurrence of cardiovascular diseases (ischemic heart disease, heart failure, and cerebrovascular disease) from 3 months up to 1,500 days after diagnosis, they found that patients treated with dupilumab had a significantly lower cumulative risk of developing these conditions compared to untreated patients [27]. However, despite dupilumab’s protective effect in patients without chronic coronary syndrome (CCS), further analysis revealed a contrasting outcome in those with a prior diagnosis of ischemic heart disease. In this subgroup, systemic IL4Ra blockade with dupilumab was associated with an increased risk of developing heart failure. This finding aligns with experimental data from murine models, where IL4Ra signaling was shown to be crucial for cardiac function recovery following ischemic injury. These results highlight the complexity of IL-4Rα signaling in cardiovascular health and suggest that, while dupilumab may reduce cardiovascular risk in patients without CCS. The dupilumab prescription should be approached with caution in patients with pre-existing ischemic heart disease [27]. However, some limitations of the study must be considered. Firstly, only patients treated with Dupilumab for atopic dermatitis were enrolled. Despite PSM, the compared groups remained unbalanced in terms of both the incidence of cardiovascular risk factors and the severity of the underlying dermatological disease [27].
4. Personalized Cardiovascular Risk Management: Tailoring Dupilumab Use in Ischemic Heart Disease and Heart Failure
Concerns regarding the cardiologic safety of dupilumab remain partly theoretical; however, some are supported by biologically plausible mechanisms, such as its potential impact on cardiac fibrosis and post-ischemic remodeling through inhibition of IL-4 and IL-13 signaling. Considering the potential implications of IL-4/IL-13 blockade on myocardial repair, treatment with dupilumab in patients with pre-existing HF or high cardiovascular risk requires careful multidisciplinary evaluation. In particular, patients with heart failure with reduced ejection fraction (HFrEF) may represent a vulnerable population in whom inhibition of IL-4/IL-13 signaling could theoretically interfere with reparative immune mechanisms, specifically the activity of alternatively activated (M2a) macrophages, potentially accelerating ventricular dysfunction.
In the context of ischemic heart disease, the first 30 days following MI represent a critical period during which IL-4 and IL-13 play a reparative role by modulating macrophage polarization, angiogenesis, and extracellular matrix remodeling. This cardioprotective effect appears to be more pronounced in male patients, suggesting sex-specific responses to cytokine signaling. Therefore, temporary discontinuation of dupilumab during this early post-MI period could be considered in selected high-risk patients to avoid interference with endogenous repair mechanisms. However, this must be carefully balanced against the potential risks of drug suspension, particularly worsening dyspnea, which may be difficult to distinguish between nasal polyps, Ticagrelor-related dyspnea, or angina equivalents, complicating clinical management.
A potential strategy to mitigate cardiovascular risk in patients receiving dupilumab post-MI could involve co-administration of anti-inflammatory agents such as colchicine, which has demonstrated benefit in secondary prevention [40,41,42,43,44]. The COLCOT trial showed that colchicine 0.5 mg daily significantly reduced the risk of ischemic cardiovascular events in patients with recent MI, supporting its use as an adjunct to standard therapy to modulate post-infarct inflammation [45,46].
Over recent years, the advent of novel pharmacologic therapies has significantly improved the prognosis of patients with HFrEF [47,48]. Among these, sacubitril/valsartan (Entresto), a combination of a neprilysin inhibitor and an angiotensin receptor blocker, has been shown to reduce cardiovascular mortality and heart failure hospitalizations. Its dual mechanism, simultaneous inhibition of the renin-angiotensin-aldosterone system and enhancement of natriuretic peptide signaling, contributes to improved ventricular remodeling and left ventricular strain, reduced blood pressure, and decreased congestion [49,50,51,52,53,54,55,56,57]. Additionally, dapagliflozin and empagliflozin, selective sodium-glucose co-transporter-2 (SGLT2) inhibitors initially developed as antidiabetic agents, have demonstrated cardiovascular benefits independent of glycemic control [47,48,58,59,60,61,62]. The DAPA-HF trial showed that dapagliflozin significantly reduces the risk of cardiovascular death and worsening HF in patients with HFrEF, regardless of diabetes status, possibly through favorable shifts in myocardial metabolism, reduced oxidative stress, and anti-inflammatory effects [62].
Similarly, in patients with concomitant heart failure with HFrEF, integrating guideline-directed medical therapy, including sacubitril/valsartan and SGLT2 inhibitors, may not only optimize hemodynamic and metabolic status but also counterbalance the theoretical risk of impaired myocardial repair due to dupilumab. These therapeutic agents are well-established cornerstones of heart failure management, consistently demonstrating improved clinical outcomes. When combined with anti–type 2 biologics, such agents may offer additional cardioprotective benefits, particularly in carefully selected patients. Before initiating dupilumab in patients with CRSwNP and a history of cardiovascular disease, a comprehensive baseline cardiologic evaluation could be essential. In cases where ventricular dysfunction is identified, concurrent use of sacubitril/valsartan or dapagliflozin may help protect cardiac function and reduce the risk of adverse events. However, current evidence regarding the safety and efficacy of such combination therapy remains limited. Therefore, vigilant cardiac monitoring and an individualized treatment strategy are critical, especially for patients with prior myocardial infarction, documented left ventricular dysfunction, or significant systemic eosinophilia. Future research exploring the combined use of dupilumab with these cardioprotective agents could be crucial for optimizing care in patients with CRSwNP and HF or IM.
5. Conclusions and Future Directions
Dupilumab represents a significant advancement in the treatment of type 2 inflammatory diseases, such as chronic rhinosinusitis with nasal polyps. Clinical efficacy of dupilumab in reducing upper airway inflammation is well established, and the safety profile is generally favorable. However, emerging evidence suggests that IL-4 and IL-13 signaling may play a cardioprotective role during myocardial repair, particularly in the early post-infarction phase. These cytokines promote anti-inflammatory macrophage polarization, angiogenesis, and regulated fibrotic remodeling. Inhibition of this pathway through IL-4Rα blockade, as occurs with dupilumab, could theoretically interfere with these reparative mechanisms.
A tailored cardiovascular evaluation should be considered for patients with coexisting ischemic heart disease or HF before initiating dupilumab. In high-risk patients, a multidisciplinary approach, combined with cardioprotective therapies such as SGLT2 inhibitors, ARNI, or colchicine, may optimize both respiratory and cardiovascular outcomes. Further clinical studies are necessary to clarify the long-term cardiovascular safety profile of dupilumab. A deeper understanding of the systemic effects of type 2 cytokine blockade will be essential for developing personalized therapeutic strategies that ensure both efficacy and safety in complex patient populations.
Figure 1.
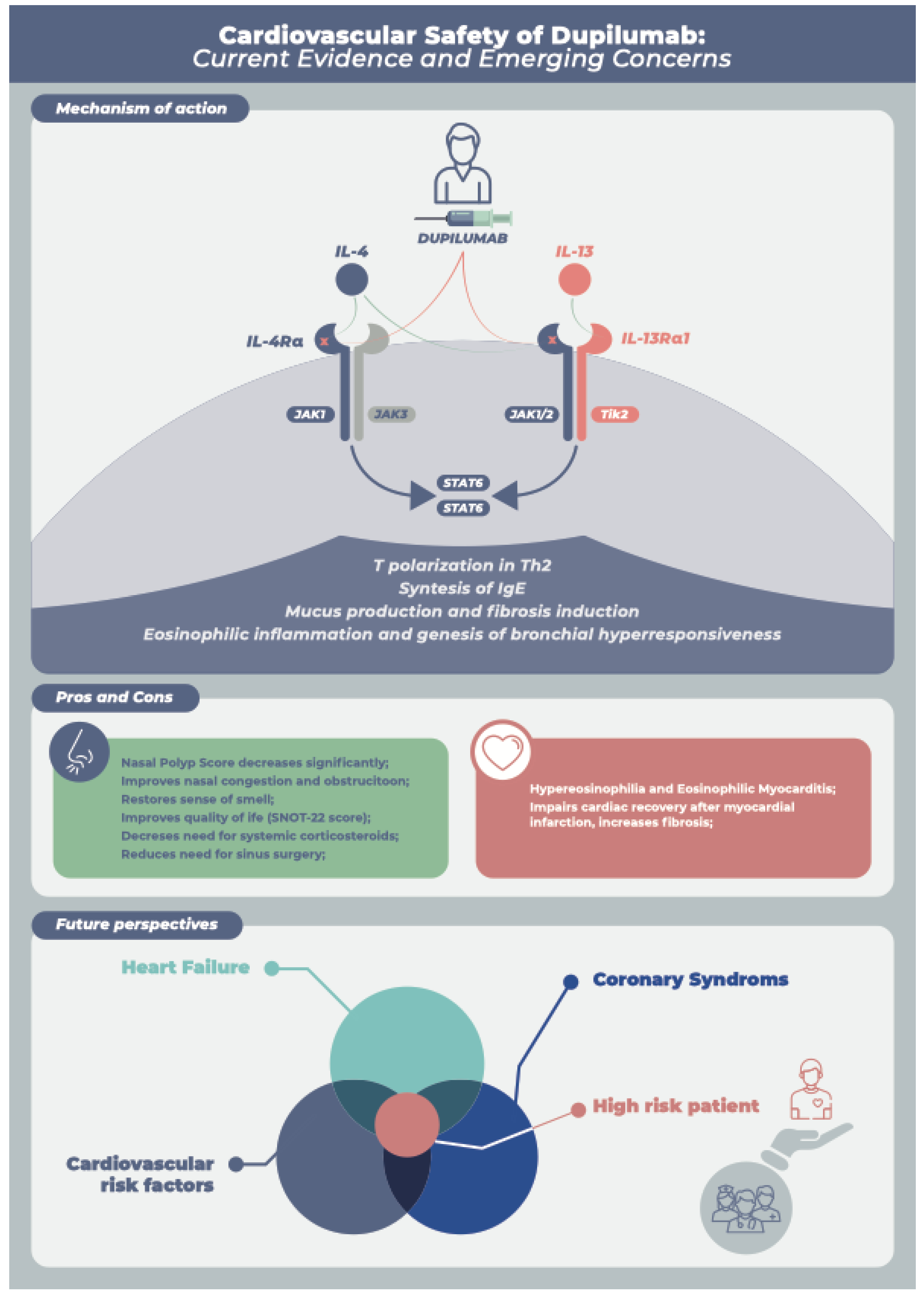
Mechanism of action and cardiovascular considerations of dupilumab therapy in patients with chronic rhinosinusitis with nasal polyps. Mechanism of Action: Dupilumab, a fully human monoclonal IgG4 antibody, binds specifically to the interleukin-4 receptor alpha subunit (IL-4Rα), thereby inhibiting both IL-4 and IL-13 signaling pathways. This dual blockade effectively reduces type 2 inflammation, leading to improvements in both subjective (nasal congestion, loss of smell, quality of life) and objective (nasal polyp score, sinus opacification) disease parameters. Pros and Cons : While dupilumab has a favorable safety profile, potential myocardial injury associated with treatment has been reported in rare cases, possibly related to hypereosinophilia or eosinophilic myocarditis, reflecting the immunomodulatory impact of IL-4/IL-13 receptor blockade on cardiac function. Personalized Cardiovascular Risk Management: Identifying patients with underlying ischemic heart disease or heart failure who may be at increased risk is crucial. A multidisciplinary approach involving both otorhinolaryngologists and cardiologists is recommended to ensure close monitoring and optimize the safety of dupilumab therapy.
Figure 1.
Mechanism of action and cardiovascular considerations of dupilumab therapy in patients with chronic rhinosinusitis with nasal polyps. Mechanism of Action: Dupilumab, a fully human monoclonal IgG4 antibody, binds specifically to the interleukin-4 receptor alpha subunit (IL-4Rα), thereby inhibiting both IL-4 and IL-13 signaling pathways. This dual blockade effectively reduces type 2 inflammation, leading to improvements in both subjective (nasal congestion, loss of smell, quality of life) and objective (nasal polyp score, sinus opacification) disease parameters. Pros and Cons : While dupilumab has a favorable safety profile, potential myocardial injury associated with treatment has been reported in rare cases, possibly related to hypereosinophilia or eosinophilic myocarditis, reflecting the immunomodulatory impact of IL-4/IL-13 receptor blockade on cardiac function. Personalized Cardiovascular Risk Management: Identifying patients with underlying ischemic heart disease or heart failure who may be at increased risk is crucial. A multidisciplinary approach involving both otorhinolaryngologists and cardiologists is recommended to ensure close monitoring and optimize the safety of dupilumab therapy.
Funding
None.
Declaration of interests
All authors declare no competing interests.
Significance Statement
Dupilumab is an effective treatment for type 2 inflammatory diseases such as CRSwNP; however, its cardiovascular safety profile remains insufficiently characterized. This review critically evaluates emerging evidence of potential interference with post-infarction myocardial repair and highlights the importance of a multidisciplinary approach in managing patients with coexisting inflammatory and cardiovascular diseases.
Abbreviations and Acronyms
| CRSwNP | Chronic rhinosinusitis with nasal polyps |
| EOM | eosinophilic otitis media |
| HF | heart failure |
| HFrEF | heart failure with reduced ejection fraction |
| LVEF | left ventricular ejection fraction |
| MI | Myocardial infarction |
| OCS | oral corticosteroid |
References
- Jutel M., Agache I., Zemelka-Wiacek M., et al. Nomenclature of allergic diseases and hypersensitivity reactions: Adapted to modern needs: An EAACI position paper. Allergy 2023;78(11):2851–74. [CrossRef]
- Correction to: Nomenclature of allergic diseases and hypersensitivity reactions: Adapted to modern needs: An EAACI position paper. Allergy 2024;79(1):269–73. [CrossRef]
- Carsuzaa F., Béquignon É., Dufour X., de Bonnecaze G., Lecron J-C., Favot L. Cytokine Signature and Involvement in Chronic Rhinosinusitis with Nasal Polyps. Int J Mol Sci 2021;23(1):417. [CrossRef]
- Bachert C., Han JK., Desrosiers M., et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. The Lancet 2019;394(10209):1638–50. [CrossRef]
- Galletti C., Giammona Indaco F., Portelli D., et al. Efficacy of Dupilumab in Patients with Chronic Rhinosinusitis with Nasal Polyps and Eosinophilic Otitis Media: A Six-Month Observational Study. Medicina (B Aires) 2025;61(8):1471. [CrossRef]
- Galletti C., Sireci F., Stilo G., et al. Mepolizumab in chronic rhinosinusitis with nasal polyps: Real life data in a multicentric Sicilian experience. Am J Otolaryngol 2025;46(1):104597. [CrossRef]
- Galletti C., Barbieri MA., Ciodaro F., et al. Effectiveness and Safety Profile of Dupilumab in Chronic Rhinosinusitis with Nasal Polyps: Real-Life Data in Tertiary Care. Pharmaceuticals 2023;16(4):630. [CrossRef]
- Galletti C., Ragusa M., Sireci F., et al. Dupilumab in chronic rhinosinusitis with nasal polyps: Real life data in a multicentric Sicilian experience. Am J Otolaryngol 2024;45(1):104106. [CrossRef]
- Bitterman D., Patel P., Wang JY., et al. Systematic review of dupilumab safety and efficacy for treatment of keloid scars. Arch Dermatol Res 2024;316(8):560. [CrossRef]
- Maurer M., Casale TB., Saini SS., et al. Dupilumab in patients with chronic spontaneous urticaria (LIBERTY-CSU CUPID): Two randomized, double-blind, placebo-controlled, phase 3 trials. Journal of Allergy and Clinical Immunology 2024;154(1):184–94. [CrossRef]
- Zhang Q., Zhong N., Dhooria S., et al. Dupilumab Efficacy and Safety in Patients With Persistent Asthma: Asia–Pacific Region. Clinical & Experimental Allergy 2025;55(8):691–700. [CrossRef]
- Silverberg JI., Bunick CG., Hong HC., et al. Efficacy and safety of upadacitinib versus dupilumab in adults and adolescents with moderate-to-severe atopic dermatitis: week 16 results of an open-label randomized efficacy assessor-blinded head-to-head phase IIIb/IV study (Level Up). British Journal of Dermatology 2024;192(1):36–45. [CrossRef]
- Reale M., Licci G., Orlando P., et al. Efficacy and safety of dupilumab in the treatment of CRSwNP in the real-life setting: a review of the literature. European Archives of Oto-Rhino-Laryngology 2024;281(10):5023–31. [CrossRef]
- Xiao Y., Yang W., Wang M. A comprehensive analysis on the safety of two biologics dupilumab and omalizumab. Front Med (Lausanne) 2024;11. [CrossRef]
- Hopkins C., Han JK., Fokkens W., et al. Dupilumab Versus Mepolizumab for Chronic Rhinosinusitis With Nasal Polyposis: An Indirect Treatment Comparison. J Allergy Clin Immunol Pract 2024;12(12):3393-3401.e15. [CrossRef]
- Chong L-Y., Piromchai P., Sharp S., et al. Biologics for chronic rhinosinusitis. Cochrane Database of Systematic Reviews 2021;2021(10). [CrossRef]
- Harb H., Chatila TA. Mechanisms of Dupilumab. Clinical & Experimental Allergy 2020;50(1):5–14. [CrossRef]
- Wenzel S., Ford L., Pearlman D., et al. Dupilumab in Persistent Asthma with Elevated Eosinophil Levels. New England Journal of Medicine 2013;368(26):2455–66. [CrossRef]
- Rabe KF., Nair P., Brusselle G., et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. New England Journal of Medicine 2018;378(26):2475–85. [CrossRef]
- Castro M., Corren J., Pavord ID., et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. New England Journal of Medicine 2018;378(26):2486–96. [CrossRef]
- Bachert C., Han JK., Desrosiers M., et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. The Lancet 2019;394(10209):1638–50. [CrossRef]
- Naidu S., Vatti R. Acute Myocarditis Following Dupilumab Initiation. Cureus 2025. [CrossRef]
- Strong A., Lin T., Sverrild A., et al. Dupilumab-associated hypereosinophilia in severe asthma. ERJ Open Res 2024;10(4):00048–2024. [CrossRef]
- Junttila IS. Tuning the Cytokine Responses: An Update on Interleukin (IL)-4 and IL-13 Receptor Complexes. Front Immunol 2018;9. [CrossRef]
- Bakhshian Nik A., Alvarez-Argote S., O’Meara CC. Interleukin 4/13 signaling in cardiac regeneration and repair. American Journal of Physiology-Heart and Circulatory Physiology 2022;323(5):H833–44. [CrossRef]
- Segiet OA. The role of interleukins in heart failure with reduced ejection fraction. The Anatolian Journal of Cardiology 2019. [CrossRef]
- Alvarez-Argote S., Paddock SJ., Flinn MA., et al. IL-13 promotes functional recovery after myocardial infarction via direct signaling to macrophages. JCI Insight 2024;9(2). [CrossRef]
- Parisi V., Cabaro S., D’Esposito V., et al. Epicardial Adipose Tissue and IL-13 Response to Myocardial Injury Drives Left Ventricular Remodeling After ST Elevation Myocardial Infarction. Front Physiol 2020;11. [CrossRef]
- Amit U., Kain D., Wagner A., et al. New Role for Interleukin-13 Receptor α1 in Myocardial Homeostasis and Heart Failure. J Am Heart Assoc 2017;6(5). [CrossRef]
- Hofmann U., Knorr S., Vogel B., et al. Interleukin-13 Deficiency Aggravates Healing and Remodeling in Male Mice After Experimental Myocardial Infarction. Circ Heart Fail 2014;7(5):822–30. [CrossRef]
- Troidl C., Möllmann H., Nef H., et al. Classically and alternatively activated macrophages contribute to tissue remodelling after myocardial infarction. J Cell Mol Med 2009;13(9b):3485–96. [CrossRef]
- Ferraro B., Leoni G., Hinkel R., et al. Pro-Angiogenic Macrophage Phenotype to Promote Myocardial Repair. J Am Coll Cardiol 2019;73(23):2990–3002. [CrossRef]
- Daseke MJ., Tenkorang-Impraim MAA., Ma Y., et al. Exogenous IL-4 shuts off pro-inflammation in neutrophils while stimulating anti-inflammation in macrophages to induce neutrophil phagocytosis following myocardial infarction. J Mol Cell Cardiol 2020;145:112–21. [CrossRef]
- DeBerge M., Yeap XY., Dehn S., et al. MerTK Cleavage on Resident Cardiac Macrophages Compromises Repair After Myocardial Ischemia Reperfusion Injury. Circ Res 2017;121(8):930–40. [CrossRef]
- Hilgendorf I., Gerhardt LMS., Tan TC., et al. Ly-6C high Monocytes Depend on Nr4a1 to Balance Both Inflammatory and Reparative Phases in the Infarcted Myocardium. Circ Res 2014;114(10):1611–22. [CrossRef]
- Nahrendorf M., Swirski FK., Aikawa E., et al. The healing myocardium sequentially mobilizes two monocyte subsets with divergent and complementary functions. J Exp Med 2007;204(12):3037–47. [CrossRef]
- Zlatanova I., Pinto C., Bonnin P., et al. Iron Regulator Hepcidin Impairs Macrophage-Dependent Cardiac Repair After Injury. Circulation 2019;139(12):1530–47. [CrossRef]
- Shintani Y., Ito T., Fields L., et al. IL-4 as a Repurposed Biological Drug for Myocardial Infarction through Augmentation of Reparative Cardiac Macrophages: Proof-of-Concept Data in Mice. Sci Rep 2017;7(1):6877. [CrossRef]
- Shiraishi M., Shintani Y., Shintani Y., et al. Alternatively activated macrophages determine repair of the infarcted adult murine heart. Journal of Clinical Investigation 2016;126(6):2151–66. [CrossRef]
- SABOURET P., ANGOULVANT D., PATHAK A., et al. How to fill the GAPS-I in secondary prevention: application of a strategy based on GLP1 analogues, antithrombotic agents, PCSK9 inhibitors, SGLT2 inhibitors and immunomodulators. Panminerva Med 2022;64(2). [CrossRef]
- Nidorf SM., Eikelboom JW., Budgeon CA., Thompson PL. Low-Dose Colchicine for Secondary Prevention of Cardiovascular Disease. J Am Coll Cardiol 2013;61(4):404–10. [CrossRef]
- Nelson K., Fuster V., Ridker PM. Low-Dose Colchicine for Secondary Prevention of Coronary Artery Disease. J Am Coll Cardiol 2023;82(7):648–60. [CrossRef]
- d’Entremont M-A., Poorthuis MHF., Fiolet ATL., et al. Colchicine for secondary prevention of vascular events: a meta-analysis of trials. Eur Heart J 2025;46(26):2564–75. [CrossRef]
- Samuel M., Berry C., Dubé M-P., et al. Long-term trials of colchicine for secondary prevention of vascular events: a meta-analysis. Eur Heart J 2025;46(26):2552–63. [CrossRef]
- Tardif J-C., Kouz S., Waters DD., et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. New England Journal of Medicine 2019;381(26):2497–505. [CrossRef]
- Bouabdallaoui N., Tardif J-C., Waters DD., et al. Time-to-treatment initiation of colchicine and cardiovascular outcomes after myocardial infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT). Eur Heart J 2020;41(42):4092–9. [CrossRef]
- McDonagh TA., Metra M., Adamo M., et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021;42(36):3599–726. [CrossRef]
- Beghini A., Sammartino AM., Papp Z., et al. 2024 update in heart failure. ESC Heart Fail 2025;12(1):8–42. [CrossRef]
- Mann DL., Givertz MM., Vader JM., et al. Effect of Treatment With Sacubitril/Valsartan in Patients With Advanced Heart Failure and Reduced Ejection Fraction. JAMA Cardiol 2022;7(1):17. [CrossRef]
- Zhou X., Zhu H., Zheng Y., Tan X., Tong X. A systematic review and meta-analysis of sacubitril-valsartan in the treatment of ventricular remodeling in patients with heart failure after acute myocardial infarction. Front Cardiovasc Med 2022;9. [CrossRef]
- de Gregorio C., Laterra G., Vaccaro V., Bitto R., Dattilo G. Time-based clinical and functional achievements in real-life HF patients on ARNI treatment. Eur J Intern Med 2020;76:115–7. [CrossRef]
- DATTILO G., BITTO R., CORREALE M., et al. Trend of perceived quality of life and functional capacity in outpatients with chronic heart failure and in treatment with sacubitril/valsartan: a real-life experience. Minerva Cardiology and Angiology 2022;70(5). [CrossRef]
- Casale M., Correale M., Laterra G., et al. Effects of Sacubitril/Valsartan in Patients with High Arrhythmic Risk and an ICD: A Longitudinal Study. Clin Drug Investig 2021;41(2):169–76. [CrossRef]
- Dattilo G., Laterra G., Licordari R., et al. The Long-Term Benefit of Sacubitril/Valsartan in Patients with HFrEF: A 5-Year Follow-Up Study in a Real World Population. J Clin Med 2023;12(19):6247. [CrossRef]
- Velazquez EJ., Morrow DA., DeVore AD., et al. Angiotensin–Neprilysin Inhibition in Acute Decompensated Heart Failure. New England Journal of Medicine 2019;380(6):539–48. [CrossRef]
- Velazquez EJ., Morrow DA., DeVore AD., et al. Angiotensin–Neprilysin Inhibition in Acute Decompensated Heart Failure. New England Journal of Medicine 2019;380(6):539–48. [CrossRef]
- McMurray JJV., Packer M., Desai AS., et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. New England Journal of Medicine 2014;371(11):993–1004. [CrossRef]
- Zinman B., Wanner C., Lachin JM., et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. New England Journal of Medicine 2015;373(22):2117–28. [CrossRef]
- Wiviott SD., Raz I., Bonaca MP., et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. New England Journal of Medicine 2019;380(4):347–57. [CrossRef]
- Verma S., Dhingra NK., Butler J., et al. Empagliflozin in the treatment of heart failure with reduced ejection fraction in addition to background therapies and therapeutic combinations (EMPEROR-Reduced): a post-hoc analysis of a randomised, double-blind trial. Lancet Diabetes Endocrinol 2022;10(1):35–45. [CrossRef]
- Anker SD., Butler J., Filippatos G., et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. New England Journal of Medicine 2021;385(16):1451–61. [CrossRef]
- McMurray JJV., Solomon SD., Inzucchi SE., et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. New England Journal of Medicine 2019;381(21):1995–2008. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



