Submitted:
19 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Introduction: Segmentectomy for non–small cell lung cancer (NSCLC) is increasingly performed for small-sized lesions. However, prognostic factors associated with poor out-comes after this lung-sparing oncologic surgery remain unclear. Methods: We conducted a single-center retrospective study including 100 patients who underwent segmentectomy in real-life practice. Results: Univariate analyses identified compromise segmentectomy (HR 3.52; p = 0.005), complex segmentectomy (HR 2.56; p = 0.02), resection of a lesion with SUVmax > 6 (HR 2.86; p = 0.017), and thoracotomy approach (HR 2.62; p = 0.02) as risk factors for mortality. Regarding recurrence, thoracotomy (HR 2,77; p= 0,04) was a poor prognostic factor. Conclusion: We have identified risk factors for mortality and recurrence after segmentectomy and highlighted the need for improved assessment of the manage-ment of patients candidates for compromise segmentectomies.
Keywords:
lung cancer
; oncologic resection
; segmentectomy
; sublobar resection
; post-operative recurrence
; pos-operative survival
1. Introduction
In localized-stage non–small cell lung cancer (NSCLC), the standard treatment is curative-intent surgery consisting of an anatomical resection of the pulmonary parenchyma with thorough lymph node dissection. Historically, tumor resection was performed as a lobectomy; however, technical advances and accumulating scientific evidence have recently allowed thoracic surgeons to limit the extent of resection to one or more segmentectomies in eligible patients. This increasingly widespread practice has recently been incorporated into the latest international guidelines [1]. These recommendations apply to peripheral nodules smaller than 2 cm, with cN0 status on PET and CT imaging, as well as to pure ground-glass lesions.
Considering these changes in clinical practice, it is necessary to clarify the risk factors for recurrence and mortality following sublobar oncologic surgery in real life.
2. Material and Methods
2.1. Study Design and Population
We conducted a single-center retrospective study at the CHRU of Tours (France) including all consecutive patients who underwent segmentectomy (single or multiple) for NSCLC between January 1, 2019, and December 31, 2022. Patient records and data were prospectively entered into the French national EPITHOR database and subsequently reviewed retrospectively. Patients with incomplete resection R1 or R2 were excluded.
All included patients underwent 18F-FDG PET–CT and thin-slice chest CT to determine the cTNM stage, lesion location, and consolidation-to-tumor ratio (C/T ratio, defined as the ratio of the solid component of the lesion to its maximum diameter) [2]. Eligibility criteria for intentional segmentectomy were the presence of a lesion smaller than 2 cm, cN0 status on PET and CT imaging, and pure ground-glass lesions up to 3 cm. A compromise segmentectomy was sometimes performed in patients with lesions larger than 2 cm who could not tolerate lobectomy (bifocal tumors, impaired FEV1 and/or DLCO and/or VO₂max, or significant comorbidities), or in patients with lesions spanning more than one lobe. Patients with neuroendocrine tumors of the carcinoid type were excluded.
2.2. Surgical Procedure
Segmentectomies were performed via thoracotomy, Video-assisted thoracoscopy (VATS) or video-assisted mini-thoracotomy. Vidéo-assisted mini-thoracotomy is defined by an incision of approximately 7 cm, without rib spreading, using both direct vision and video-assisted thoracoscopic guidance. Fissures and intersegmental planes were divided using staplers after verification of resection margins. Systematic lymph node dissection (radical or lobe-specific) was performed in all cases. When intraoperative lymph node involvement was suspected, frozen-section analysis was requested, and lobectomy was performed if N+ disease was confirmed. A simple segmentectomy was defined as involving a single intersegmental plane, such as apicodorsal (S1–S2), right anterior (S3R), lingular (S4–S5), culmen (S1–S2–S3L), superior segment (S6), or basal pyramid (S7–S8–S9–S10) segmentectomies. A complex segmentectomy was defined as involving two or more intersegmental planes, such as segmentectomies within the basal pyramid, apical (S1), dorsal (S2), or left anterior (S3L) segments [3].
2.3. Postoperative Follow-Up
All patients in this series were seen in the thoracic surgery outpatient clinic one month after hospital discharge. They subsequently underwent CT-based follow-up and clinical evaluation by their pulmonologist every six months for two years, then annually for five years. Patient outcomes were assessed in 2025 either through medical correspondence or direct telephone interviews with the patients. Recurrence was classified into three categories: local (recurrence at the bronchial stump or within the operated lobe); regional (ipsilateral recurrence in another lobe, hilar or mediastinal lymph node recurrence, or recurrence within the ipsilateral pleural cavity); and distant (contralateral recurrence or recurrence outside the thorax).
2.4. Statistical Analysis
The primary endpoint was disease-free survival (DFS), with overall survival (OS) as the secondary endpoint. Analyses were performed using R software and initially consisted of univariate Cox regression analyses of clinical and intraoperative variables. Additional analyses were conducted according to resection margin status (R0 vs. Run), segmentectomy complexity (simple vs. complex), C/T ratio (cutoff 0.5) [4], segmentectomy intent (intentional vs. compromise), and SUVmax (cutoff 6) [5]. Uncertain resection (Run) is defined by the IASLC as an insufficient lymh node dissection, positivity of the highest mediastinal lymph node, presence of carcinoma in situ at bronchus margin or positive pleural cytology [6]. Variables found to be statistically significant in univariate analyses were subsequently included in a multivariate Cox regression model. Kaplan–Meier survival curves were also generated for surgical approach, segmentectomy intent, resection complexity, and SUVmax.
3. Results
We included 100 patients whose clinical characteristics are reported in Table 1. Most patients presented adenocarcinomas (84%), Stage 0-I (78%). Surgery was mainly performed by video-assisted mini-thoracotomy (70%), compromise segmentectomy represented 19% of cases, R0 was obtained for 60% of patients. The mean follow-up duration was 43.7 months. Eighteen patients experienced recurrence, and 22 patients died, among whom 8 deaths were cancer-related. Among the recurrences, there were 6 local recurrences, 3 locoregional recurrences, 5 metastatic recurrences, and 3 new primary cancers. The mean time to recurrence was 20 months, while the mean time to death was 27.2 months.
The results of overall survival and disease-free survival in univariate Cox regression analysis are presented in Table 2:
The results of overall survival and disease-free survival in multivariate analysis are presented in Table 3:
4. Discussion
In our study, performing a compromise segmentectomy appeared to be a strong predictor of mortality in both univariate analysis [HR 3.52; 95% CI (1.45–8.53); p = 0.005] and multivariate analysis [HR 3.47; 95% CI (1.16–10.41); p = 0.026], with no significant effect on disease-free survival in the univariate Cox model [HR 1.73; 95% CI (0.58–5.19); p = 0.32], although this effect was observed in the Kaplan–Meier curves (p = 0.026). In detail, among the 19 patients who underwent a compromise segmentectomy, 8 died, whereas only 4 experienced disease recurrence. These findings highlight excess mortality primarily related to patients’ intrinsic frailty rather than to resections that could be initially considered oncologically inadequate. Moreover, the follow-up duration for this subgroup was 43.6 months, comparable to that of the overall cohort, suggesting good oncologic disease control.
Thoracotomy also appeared to be a poor prognostic factor for both DFS and OS [HR 2.77; 95% CI (1.01–7.59); p = 0.04 and HR 2.62; 95% CI (1.12–6.14); p = 0.02, respectively, in the univariate model]. This excess mortality has already been well documented [7] and may be explained by both the higher morbidity associated with open surgery and the treatment of more advanced disease stages that are not amenable to minimally invasive approaches.
An SUVmax > 6 also appeared to be a predictor of mortality in univariate analysis [HR 2.86; 95% CI (1.20–6.81); p = 0.017], but this effect was not significant in the multivariate model [HR 2.20; 95% CI (0.86–5.60); p = 0.098]. No effect of this variable was observed on disease-free survival [HR 0.81; 95% CI (0.22–2.95); p = 0.75]. As a reminder, SUVmax is a relative marker of metabolic activity compared with the metabolic activity of the rest of the body. A high SUVmax may therefore reflect either highly active and potentially aggressive disease or moderately aggressive disease occurring in a patient with low baseline metabolism due to frailty. Kocaman et al. [7] demonstrated that a high SUVmax was a factor for recurrence and mortality and suggested the superiority of lobectomy over segmentectomy in patients operated on for stage I lung cancer. This parameter should probably be considered when deciding to perform a segmentectomy, alongside tumor size.
We also observed increased mortality in univariate models among patients who underwent complex segmentectomy [HR 2.56; 95% CI (1.10–5.93); p = 0.02]. This effect, which could partly be explained by reduced resection margins [8], has not been demonstrated in previous series [3,9]. Furthermore, the absence of an effect on recurrence and in the multivariate model again suggests that these were lung-sparing procedures performed in more fragile patients.
In our study, the consolidation-to-tumor ratio (C/T ratio) did not impact OS or DFS, although it has previously been described as a prognostic factor of malignancy and aggressiveness [4,10]. Other recurrence risk factors described in the literature but not explored in our study include resection margins smaller than the tumor size [11], visceral pleural invasion, and spread through air spaces (STAS) [12], the impact of which remains debated in the setting of segmentectomy.
The central finding of this study is the demonstration of impaired overall prognosis in patients undergoing compromise segmentectomies. While segmentectomy is now recognized as a safe procedure [13,14] and is increasingly integrated into clinical practice [15], its indications remain limited. In the context of an increasingly elderly and comorbid patient population, or in patients with multiple lesions to treat, choosing a compromise segmentectomy outside standard indications may be part of a lung-sparing strategy which, although modest [16], could prove crucial in cases of multisite, sequential, and/or iterative surgery at recurrence. To further explore the relevance of such compromises, a randomized trial comparing lobectomy, segmentectomy, and possibly stereotactic radiotherapy in a cohort of polymorbid patients with borderline respiratory function and/or multisite lesions could likely provide valuable guidance to thoracic oncology teams.
Our study has limitations, primarily related to its retrospective and single-center design, although the longitudinal follow-up allowed excellent data completeness with no patients lost to follow-up. The relatively small number of included patients is also a limiting factor, increasing the risk of insufficient statistical power, which may explain the lack of significance of some well-established factors such as TNM stage or R0/Run status. Nevertheless, to our knowledge, this study is the only one to date that reflects real-world practice in a single center within an unselected patient population including compromise segmentectomies.
5. Conclusions
Our study demonstrated a significant impairment in prognosis for patients undergoing compromise segmentectomies, as well as a real impact of lesion SUVmax, thoracotomy, and the complexity of the resection on mid-term mortality. Further studies will be needed to determine the optimal management strategy for these patients who fall at the margins of standard indications.
Author Contributions
Conceptualization, D.C., and A.L.; methodology, X.C., A.G. and A.E.; validation, X.C., A.G. and A.L.; formal analysis A.G., X.C. and A.L.; investigation, X.C., B.L., A.E. and A.L.; resources, X.C. and A.L.; writing—original draft preparation, X.C. and A.L.; writing—review and editing, X.C., A.G., D.C., D.S. and A.L.; supervision, A.L.; project administration, A.L.; funding acquisition, D.C., B.L., D.S. and A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The publication charges were supported by Association Thorax à Tours.
Data Availability Statement
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| NSCLC | Non–small cell lung cancer |
| DFS | Disease-free survival |
| OS | Overall survival |
| HR | Hazard ratio |
| 95% CI | 95% confidence interval |
| VATS | Video-assisted thoracoscopic surgery |
| CTR | Consolidation-to-tumor ratio |
| NRS | Numeric rating scale |
| DLCO | Diffusing capacity for carbon monoxide |
| FEV1 | Forced expiratory volume in one second |
| BMI | Body mass index |
| Run | Uncertain resection |
References
- Zer, A.; Ahn, M.-J.; Barlesi, F.; Bubendorf, L.; Ruysscher, D.D.; Garrido, P.; Gautschi, O.; Hendriks, L.E.; Jänne, P.A.; Kerr, K.M.; et al. Early and Locally Advanced Non-Small-Cell Lung Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up☆. Annals of Oncology 2025, 0. [Google Scholar] [CrossRef] [PubMed]
- Asamura, H.; Hishida, T.; Suzuki, K.; Koike, T.; Nakamura, K.; Kusumoto, M.; Nagai, K.; Tada, H.; Mitsudomi, T.; Tsuboi, M.; et al. Radiographically Determined Noninvasive Adenocarcinoma of the Lung: Survival Outcomes of Japan Clinical Oncology Group 0201. The Journal of Thoracic and Cardiovascular Surgery 2013, 146, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Handa, Y.; Tsutani, Y.; Mimae, T.; Tasaki, T.; Miyata, Y.; Okada, M. Surgical Outcomes of Complex Versus Simple Segmentectomy for Stage I Non-Small Cell Lung Cancer. The Annals of Thoracic Surgery 2019, 107, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Song, W.; Wang, D.; Chang, J.; Wang, Y.; Tian, J.; Zhou, S.; Dong, Y.; Zhou, J.; Li, J.; et al. Prognostic Value of Consolidation-to-Tumor Ratio on Computed Tomography in NSCLC: A Meta-Analysis. World J Surg Oncol 2023, 21, 190. [Google Scholar] [CrossRef] [PubMed]
- Kocaman, G.; Ibrahımov, F.; Kahya, Y.; Araz, M.; Elhan, A.H.; Enön, S. Suvmax of the Lesion Should Be Considered in the Treatment Plan for Stage I Non-Small Cell Lung Cancer. Ann Nucl Med 2025, 39, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Cansouline, X.; Elmraki, A.; Lipan, B.; Sizaret, D.; Sordet, M.; Tallet, A.; Vandier, C.; Carmier, D.; Ammi, M.; Legras, A.; et al. Uncertain Resection in Lung Cancer: A Comprehensive Review of the International Association for the Study of Lung Cancer Classification. Cancers 2025, 17. [Google Scholar] [CrossRef] [PubMed]
- Ye, B.; Wang, M. Video-Assisted Thoracoscopic Surgery versus Thoracotomy for Non-Small Cell Lung Cancer: A Meta-Analysis. Comb Chem High Throughput Screen 2019, 22, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.H. Is Complex Segmentectomy Safe? Eur J Cardiothorac Surg 2022, 61, 108–109. [Google Scholar] [CrossRef] [PubMed]
- Teng, H.; Huang, H.-K.; Ko, K.-H.; Huang, T.-W. Long-Term Prognosis of Complex versus Simple Segmentectomy for Stage I Non-Small Cell Lung Cancer. J Formos Med Assoc 2025, S0929-6646((25)00566-2). [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Bai, G.; Ji, Y.; Peng, Y.; Zang, R.; Gao, S. Consolidation Tumor Ratio Combined With Pathological Features Could Predict Status of Lymph Nodes of Early-Stage Lung Adenocarcinoma. Front Oncol 2021, 11, 749643. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Watanabe, S.-I.; Wakabayashi, M.; Yotsukura, M.; Mimae, T.; Hattori, A.; Miyoshi, T.; Isaka, M.; Endo, M.; Yoshioka, H.; et al. Risk Factors for Locoregional Relapse After Segmentectomy: Supplementary Analysis of the JCOG0802/WJOG4607L Trial. J Thorac Oncol 2025, 20, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.-Y.; Shen, C.; Wang, X.; Wang, F.-Q.; Wang, Y. Could Less Be Enough: Sublobar Resection vs Lobectomy for Clinical Stage IA Non-Small Cell Lung Cancer Patients with Visceral Pleural Invasion or Spread through Air Spaces. Int J Surg 2025, 111, 2675–2685. [Google Scholar] [CrossRef] [PubMed]
- Altorki, N.; Wang, X.; Kozono, D.; Watt, C.; Landrenau, R.; Wigle, D.; Port, J.; Jones, D.R.; Conti, M.; Ashrafi, A.S.; et al. Lobar or Sublobar Resection for Peripheral Stage IA Non–Small-Cell Lung Cancer. New England Journal of Medicine 2023, 388, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Saji, H.; Okada, M.; Tsuboi, M.; Nakajima, R.; Suzuki, K.; Aokage, K.; Aoki, T.; Okami, J.; Yoshino, I.; Ito, H.; et al. Segmentectomy versus Lobectomy in Small-Sized Peripheral Non-Small-Cell Lung Cancer (JCOG0802/WJOG4607L): A Multicentre, Open-Label, Phase 3, Randomised, Controlled, Non-Inferiority Trial. The Lancet 2022, 399, 1607–1617. [Google Scholar] [CrossRef] [PubMed]
- Cardillo, G.; Petersen, R.H.; Ricciardi, S.; Patel, A.; Lodhia, J.V.; Gooseman, M.R.; Brunelli, A.; Dunning, J.; Fang, W.; Gossot, D.; et al. European Guidelines for the Surgical Management of Pure Ground-Glass Opacities and Part-Solid Nodules: Task Force of the European Association of Cardio-Thoracic Surgery and the European Society of Thoracic Surgeons. Eur J Cardiothorac Surg 2023, 64, ezad222. [Google Scholar] [CrossRef] [PubMed]
- Charloux, A.; Quoix, E. Lung Segmentectomy: Does It Offer a Real Functional Benefit over Lobectomy? Eur Respir Rev 2017, 26, 170079. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan–Meier survival curves for overall survival. A: Overall survival curves for the SUVmax < 6 and > 6 groups. B: Overall survival curves for the intentional and compromise segmentectomy groups. C: Overall survival curves for the VATS and thoracotomy groups. D: Overall survival curves for the simple and complex segmentectomy groups.
Figure 1.
Kaplan–Meier survival curves for overall survival. A: Overall survival curves for the SUVmax < 6 and > 6 groups. B: Overall survival curves for the intentional and compromise segmentectomy groups. C: Overall survival curves for the VATS and thoracotomy groups. D: Overall survival curves for the simple and complex segmentectomy groups.
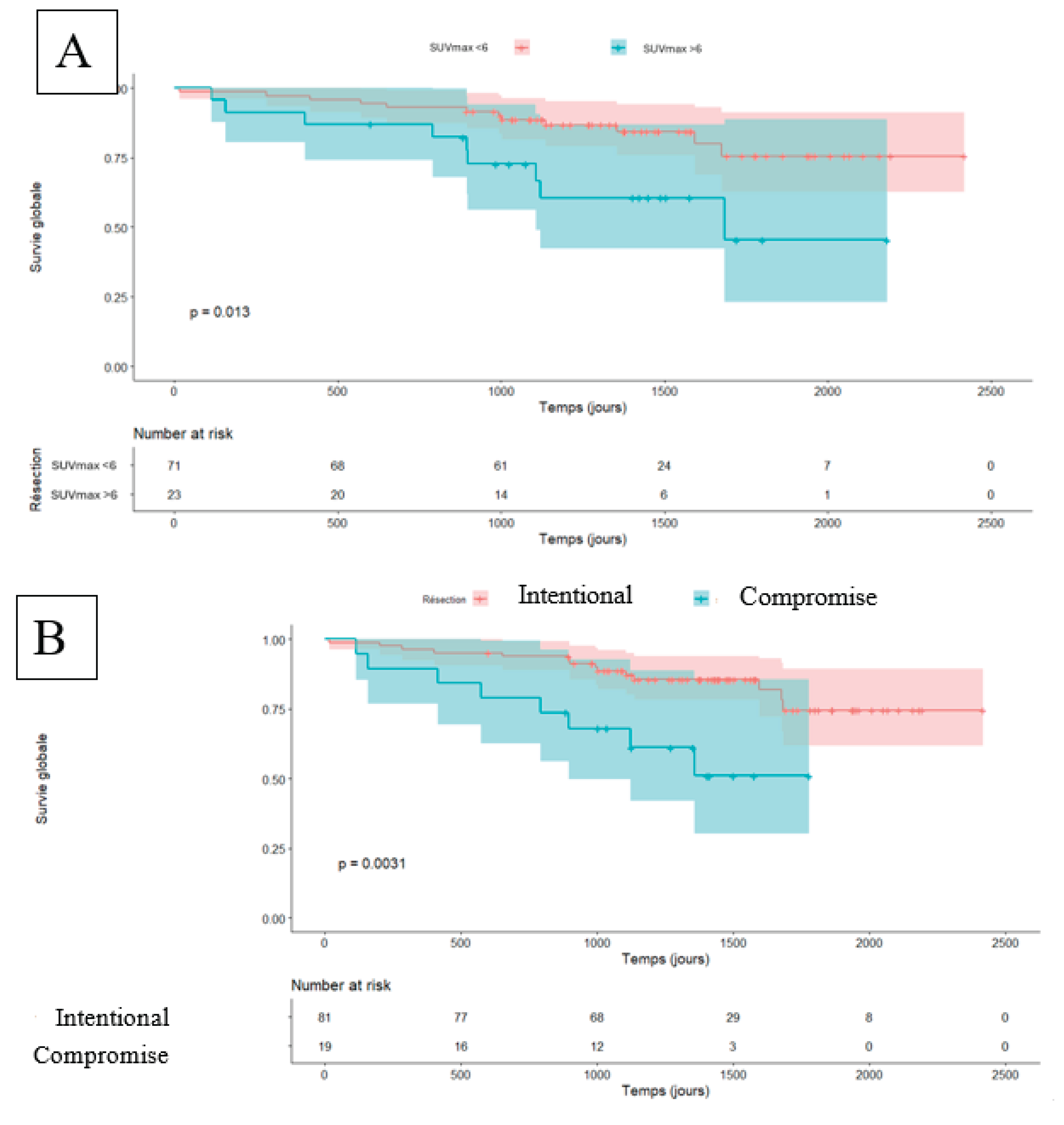
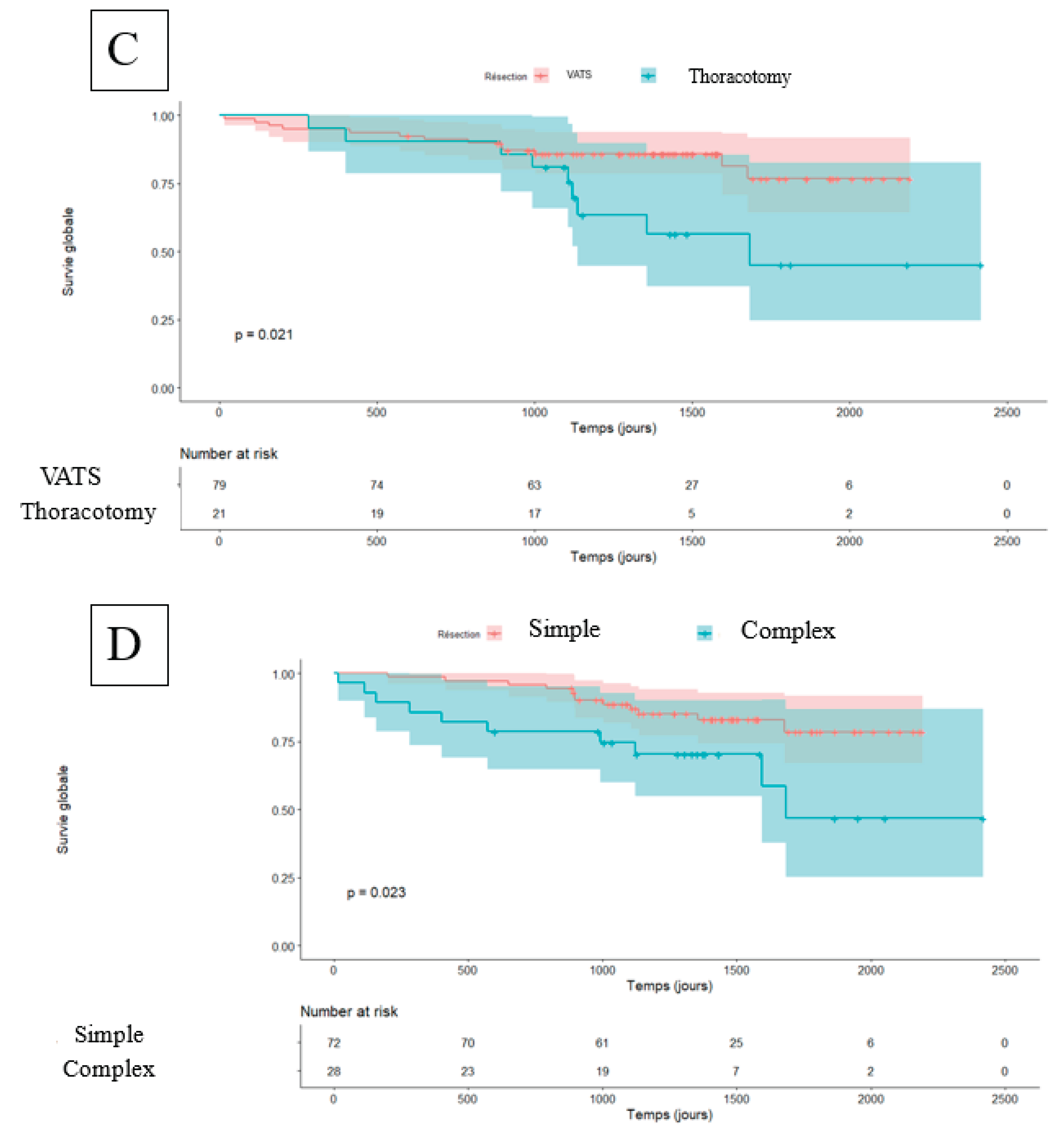
Figure 2.
Kaplan–Meier survival curves for Disease Free Survival. A: Disease Free Survival curves for the SUVmax < 6 and > 6 groups. B: Disease Free Survival curves for the intentional and compromise segmentectomy groups. C: Disease Free Survival curves for the VATS and thoracotomy groups. D: Disease Free Survival curves for the simple and complex segmentectomy groups.
Figure 2.
Kaplan–Meier survival curves for Disease Free Survival. A: Disease Free Survival curves for the SUVmax < 6 and > 6 groups. B: Disease Free Survival curves for the intentional and compromise segmentectomy groups. C: Disease Free Survival curves for the VATS and thoracotomy groups. D: Disease Free Survival curves for the simple and complex segmentectomy groups.
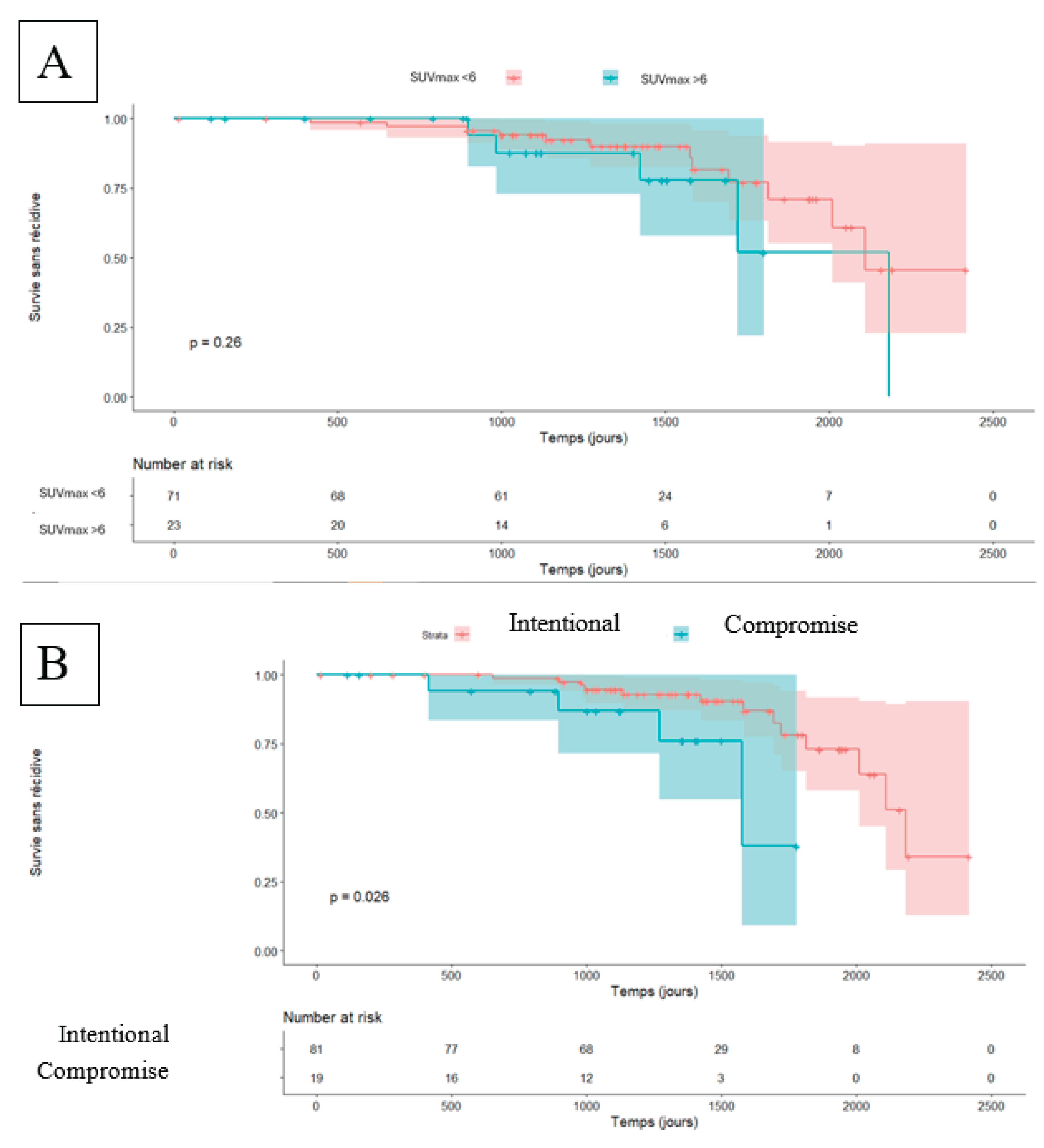
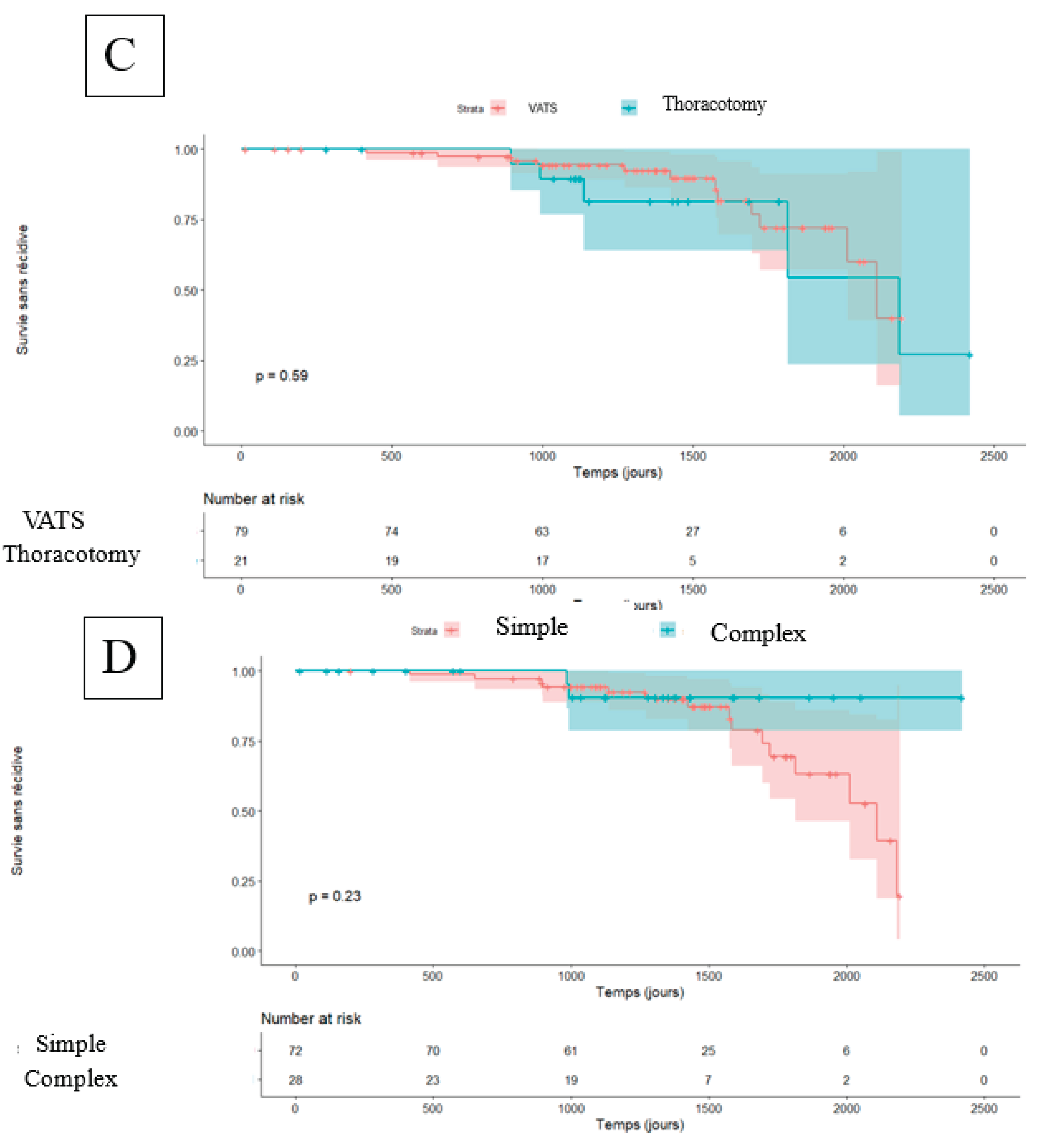

Table 1.
Clinical characteristics of the cohort.
| Variable | Value, n or average (%) |
|---|---|
| Clinical characteristics | |
| Sex M, (M/F) | 60 (60/40) |
| Age (IQR) | 70 (61-74) |
| BMI (IQR) | 26,62 (23,2-29,1) |
| OMS 0-1/2-3 | 96/4 (96%/4%) |
| Respiratory function | |
| Dyspnea 0-1/2-4 | 98/2 (98%/2%) |
| Smoker | 75 (75%) |
| Pack-year (IQR) | 37 (20-50) |
| Pre-opérative FEV1 - % théoric (IQR) | 83 (71-100) |
| Predicted post-operative FEV1 - % théoric (IQR) | 73 (64-85) |
| Pre-operative Tiffeneau ratio (IQR) | 74 (60-80) |
| Pre-operative DLCO (IQR) | 70 (58-88) |
| SUVmax (IQR) | 3,2 (2,1-5,8) |
| CTR (IQR) | 0,85 (0,5-1) |
| cTNM | |
| T1 | 84 (84%) |
| T2 | 5 (5%) |
| T3-T4 | 11 (11%) |
| N0/N1-2 | 95/5 (95%/5%) |
| Surgical procedure | |
| Video-assisted mini-thoracotomy | 70 (70%) |
| Thoracotomy | 22 (22%) |
| VATS | 9 (9%) |
| Compromise segmentectomy | 19 (19%) |
| Operative time (IQR) | 184 (150-204) |
| Hospital length stay (IQR) | 3 (2-6) |
| Numeric Rating Scale for pain (IQR) | 5 (3-6) |
| Anatomopathology | |
| Adenocarcinoma | 84 (84%) |
| Squamous cell carcinoma | 16 (16%) |
| pTNM | |
| T1 | 77 (77%) |
| T2 | 9 (9%) |
| T3-T4 | 14 (14%) |
| N0/N1-2 | 90/10 (90%/10%) |
| R0/Run | 60/40 (60%/40%) |
| Stage 0-I | 78 (78%) |
| Stage II | 12 (12%) |
| Stage III | 10 (10%) |
| Recurrence | 17 (17%) |
| Death | 22 (22%) |
IQR : Interquartile range ; CTR : consolidation tumor-ratio.
Table 2.
Univariate results for disease-free survival and overall survival.
| Disease Free Survival (DFS) | Overall Survival (OS) | |||||
|---|---|---|---|---|---|---|
| Characteristic | HR | 95% CI | p-value | HR | 95% CI | p-value |
| Sex (M) | 3,28 | [0.94–11.46] | 0,06 | 4,75 | 1.40–16.08 | 0,012 |
| Age | 1,01 | [0.95–1.08] | 0,77 | 1,05 | 0.99–1.11 | 0,089 |
| BMI | 1,03 | [0.93–1.15] | 0,54 | 0,91 | 0.83–1.01 | 0,068 |
| OMS | 1,22 | [0.64–2.35] | 0,54 | 1,35 | 0.77–2.38 | 0,29 |
| préop FEV1 | 1,01 | [0.99–1.03] | 0,24 | 0,99 | 0.97–1.01 | 0,32 |
| préop DLCO | 1,02 | [1–1.05] | 0,06 | 0,99 | 0.97–1.01 | 0,27 |
| cTNM Stage | 2,46 | [0.92–6.55] | 0,07 | 2,25 | 0.91–5.53 | 0,077 |
| Diabetes | 1,77 | [0.57–5.51] | 0,32 | 0,61 | 0.14–2.60 | 0,50 |
| Coronary disease | 1,84 | [0.41–8.23] | 0,42 | 0,70 | 0.09–5.19 | 0,72 |
| Thoracotomy | 2,77 | [1.01–7.59] | 0,04 | 2,62 | 1.12–6.14 | 0,02 |
| ASA | 1,05 | [0.45–2.44] | 0,91 | 1,32 | 0.65–2.69 | 0,44 |
| Operative time | 1 | [0.99–1.01] | 0,99 | 1,00 | 0.99–1.01 | 0,99 |
| Number of segments removed | 0,57 | [0.16–2.01] | 0,38 | 1,25 | 0.51–3.06 | 0,63 |
| Complex segmentectomy | 0,68 | [0.22–2.16] | 0,51 | 2,56 | 1.10–5.93 | 0,02 |
| Run | 0,65 | [0.23–1.85] | 0,42 | 1,75 | [0.76–4.05] | 0,19 |
| pTNM Stage | 1,01 | [0.34–2.94] | 0,99 | 3,55 | [1.53–8.23] | 0,003 |
| Hospital length stay | 0,99 | [0.9–1.1] | 0,90 | 1,00 | [0.93–1.06] | 0,89 |
| SUVmax | 0,81 | [0.22–2.95] | 0,75 | 2,86 | [1.20–6.81] | 0,017 |
| Compromise Segmentecomy | 1,73 | [0.58–5.19] | 0,32 | 3,52 | [1.45–8.53] | 0,005 |
| CTR | 0,83 | [0.31–2.2] | 0,70 | 1,15 | [0.50–2.65] | 0,74 |
| NRS max | 1,07 | [0.85–1.34] | 0,56 | 0,93 | [0.76–1.14] | 0,47 |
HR: Hazard Ratio; 95%CI: 95% Confidence interval; CTR: consolidation tumor-ratio; NRS: Numerical Rating Scale (for pain).
Table 3.
Multivariate results for disease-free survival and overall survival.
| Disease Free Survival (DFS) | Overall Survival (OS) | |||||
|---|---|---|---|---|---|---|
| Characteristic | HR | 95% CI | p-value | HR | 95% CI | p-value |
| Sex (M) | 5.36 | 1.07 – 26.91 | 0.042 | 2.95 | [0.83-10.47] | 0.094 |
| pTNM Stage | 0.89 | 0.21 – 3.69 | 0.871 | 1.06 | [0.33-3.38] | 0.91 |
| Compromise Segmentecomy | 0.66 | 0.10 – 4.28 | 0.668 | 3.47 | [1.16-10.41] | 0.026 |
| SUVmax | 0.47 | 0.10 – 2.32 | 0.356 | 2.2 | [0.86-5.60] | 0.098 |
| Thoracotomy | 5.40 | 1.51 – 19.24 | 0.009 | 1.7 | [0.65-4.46] | 0.28 |
| Complex segmentectomy | 0.61 | 0.14 – 2.76 | 0.524 | 2.03 | [0.78-5.28] | 0.15 |
HR: Hazard Ratio; 95%CI: 95% Confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



