
Submitted:
19 November 2024
Posted:
20 November 2024
You are already at the latest version
Abstract
Background. Given the complexity of lung cancer surgery, this study aims to provide an overview of hospitals authorised to perform lung cancer surgery in France, and assess their performance focusing on severe post-operative complications and 30-day in-hospital mortality based on the Clavien-Dindo classification (grade>2). Methods. We included all patients (N=64,304) who underwent pulmonary resection for lung cancer from the French hospital database (2019–2023). To quantify variations within regions, we used the ratio of the 90th to the 10th decile of the standardised outcome rate of the hospitals. We used a hierarchical logistic regression model to estimate the adjusted odds ratio (aOR) according to the number of annual procedures. We then used the results of this modeling to see how the standardised rate estimate might evolve after simulating a new organisation of hospitals authorised to perform this surgery. Results. A total of 18,151 patients (28%) had severe complications (Clavien-Dindo>2). Compared to hospital performing less than 100 procedures/year, the risk of severe complications was significantly reduced for hospitals performing between 101 and 250 procedures (aOR=0.83[0.77-0.89]) and more than 250 procedures/year (aOR=0.85[0.77-0.93]). A simulation of hospital reorganisation, using 100 procedures/year as the threshold value shows that this would have prevented 477 severe complications over the period. Conclusion. This study shows inequalities in performance indicators between hospitals in each French region. The influence of the volume of activity raises questions about the need to restructure the offer of care for complex surgeries such as lung cancer surgery.
Keywords:
lung cancer
; surgery
; postoperative complications
; quality assessment
1. Introduction
Lung cancer (LC) remains one of the most prevalent and deadly forms of cancer worldwide. While surgery is a key treatment option, only about 20% of lung cancer patients in France are eligible for surgery due to the advanced stage of the disease at diagnosis or poor general patient health. This reflects the challenges associated with disease progression and the patient's overall condition, limiting the potential for surgical intervention [1]. LC surgery requires specialised care, ideally provided by dedicated hospitals with expertise in thoracic oncology. The French government launched the first ‘Cancer Plan’ in 2009 [2], which radically reformed cancer care, one of the key measures being the requirement for hospitals performing cancer-related surgery to obtain specific authorisation. Under the plan, hospitals were required to perform a minimum of 30 LC related procedures/year in order to obtain authorisation. Recently, this threshold was raised, with hospitals now having to perform at least 40 procedures a year to retain their authorisation [3]. At present, 146 hospitals across France are authorised to perform thoracic cancer surgery [3]. The quality of the results obtained by the teams performing these surgeries has been relatively little studied in France, unlike in other European countries and the United States [4,5]. Given the complexity of LC surgery, it has become imperative to carry out an in-depth assessment of the current state of these surgical practices throughout France, in order to improve the quality of care and in particular the frequency of severe post-operative complications. This study aims to provide an overview of hospitals authorised to perform LC surgery, and to assess their performance on the basis of key outcomes. The specific objectives of this work are as follows. Firstly, we aim to describe the characteristics of all hospitals in France that perform LC surgery, including their public or private status, their distribution across the 13 French regions, and the characteristics of the patients they admit. Secondly, we aim to assess the surgical performance of these hospitals, focusing on the Clavien Dindo classification (grade>2) as the main outcome indicator, including severe post-operative complications and 30-day in-hospital mortality.
2. Materials and Methods
Database and Inclusion
This study utilised the French national hospital database from the Programme de Médicalisation des Systèmes d’Information (PMSI), which includes discharge abstracts for all inpatient admissions to both public and private hospitals across France. Diagnoses recorded during the hospital stay are classified according to the 10th edition of the International Classification of Diseases (ICD-10) [6,7], while medical and surgical procedures performed during hospitalisation are coded according to the French Common Classification of Medical Procedures (CCAM). We included patients from this database who underwent pulmonary resection for LC in France between 2019 and 2023. Specifically, we selected patients with a primary diagnosis of LC (ICD-10 codes C34), along with a corresponding surgical procedure for LC (CCAM codes) performed during the same hospital admission [8,9].
Patient Characteristics
For each patient, we collected data on age, gender, and surgery-related factors including the type of surgical approach (thoracotomy, video assisted thoracic surgery (VATS) or robot-assisted surgery) and the nature of the resection (limited resection, lobectomy, bilobectomy or pneumonectomy). Additionally, we considered comorbidities such as various diseases (pulmonary, cardiovascular, peripheral vascular, liver, neurological, kidney, hematologic, metabolic, infectious), but also cerebrovascular events, anemia and other therapies (preoperative chemotherapy and steroids). We also calculated a modified Charlson Comorbidity Index (CCI) to assess the overall comorbidity burden [10].
Region and Hospital Characteristics
In France, hospitals are classified into several categories, including academic (teaching) hospital, non-academic hospital, non-profit private hospital, or private hospital. For each hospital, we also determined the number of pulmonary resection performed per year.
The hospitals were located in one of the 13 regions in metropolitan France: Auvergne-Rhones-Alpes (ARA), Bourgogne-Franche-Comté (BFC), Bretagne (BRE), Centre Val-de-Loire (CVL), Corse (COR), Grand-Est (GE), Hauts-de-France (HdF), Ile-de-France (IdF), Normandie (NOR), Nouvelle Aquitaine (NA), Occitanie (OC), Pays de la Loire (PdL), and Provence-Alpes-Côte d’Azur (PACA).
Outcome (Quality Indicator)
Our main outcome was based on the Clavien-Dindo classification [11], which was transformed into a binary variable. The variable was equal to 1 if the Clavien-Dindo classification was higher than 2. This grade > 2 rating included severe post-operative complications and 30-day in-hospital mortality.
Severe post-operative complications were defined as the presence of one or more of the following postoperative conditions: pain, parietal complications, tracheostomy, reintubation, adult respiratory distress syndrome, bronchopleural fistula, empyema respiratory failure, arrhythmia, malnutrition, phlebitis, pleural effusion, pulmonary embolism, pneumonia, bleeding requiring re-operation, myocardial infarction, stroke, ischemia of the lower limbs, septicemia, and heart failure.
Thirty-day in-hospital mortality was defined as all deaths occurring during the same hospital stay as the operation or within 30 days of the operation.
Hereafter, we will refer to this outcome (Clavien-Dindo>2) as severe complication.
Statistical Analyses
The number of annual procedures for each establishment was categorised into 3 quantiles: < 100, 101 to 250 and > 250 procedures/year.
To estimate the standardised outcome rate (Clavien-Dindo>2), we used an indirect method by including the following variables in the logistic regression model: age, sex, comorbidities, Charlson score, type of pulmonary resection, surgical approach and year. To describe regional variations in the number of procedures and the standardised outcome rate, we used the median, the 1st quartile and the 3rd quartile. To quantify variations within regions, we used the ratio of the 90th to the 10th decile of the standardised outcome rate of the hospitals. We used a hierarchical logistic regression model to estimate the adjusted odds ratio (aOR) for each of the three classes of number of annual procedures and type of establishment, with their 95% confidence interval. We also included patient characteristics, type of procedure and year in the model. These models are used to estimate unexplained heterogeneity between regions, indicated by the inter-regional variance [12,13].
Finally, we used the results of this modeling to see how the standardised rate estimate might evolve after simulating a new organisation of hospitals authorised to perform this surgery. We used the estimated standardised rate using the logistic regression model explained above to obtain the number of events expected in each region if only those centers performing more than 100 procedures/year were selected. Finally, the number of avoidable severe complications or deaths was calculated as the difference between the observed number of complications and the expected number of events.
The calculations were carried out using STATA V.18 statistical software (StataCorp, College Station, Texas, USA).
Ethics, Patient and Public Involvement
Patients and the public were not involved in this study. As this was a national retrospective analysis using pseudonymised data (no personally identifiable information), patient consent was not applicable. The French national hospital database does not contain any identifying details: patient identities are pseudonymised, allowing data linkage for the same individual without knowing their identity. Ethical approval for the use of this database was granted by the French National Commission for Data Protection. (declaration of compliance with reference methodology 05 obtained on 7/08/2018 under number 2204633 v0) and this study thus adhered to the tenets of the declaration of Helsinki
3. Results
From 2019 to 2023, 64,304 patients underwent lung resection for cancer. The number of surgeries increased over time (2019: 12,367 patients, 2023: 14,227 patients, Table 1). A total of 18,151 patients (28%) had a severe complication (Clavien-Dindo>2), which was used as a quality indicator. Over the study period, we observed a decrease in severe post-operative complications, as well as in mortality (Clavien-Dindo=5), which fell from 2.3% in 2019 to 1.5% in 2023 (Table 1).
Regions and Characteristics of Hospitals
A total of 171 hospitals were performing lung resections for cancer during the study period. The median number of procedures/year in France was 53, with interquartile ranges of 16 and 101. By region and according to the size of the region, the number of hospitals ranged from 2 in Corsica to 24 in Rhône-Alpes-Auvergne (Table 2). However, the number of hospitals is not proportional to the size of the population in the region. For example, 24 hospitals performed lung resections in Rhône-Alpes-Auvergne, whereas only 19 hospitals were counted in the more populous Ile-de-France region (Table 2). The variation in the number of annual procedures performed by hospitals in the different metropolitan regions is shown in Table 2. The medians range from 20 for Corsica to 121 for Grand-Est. In most regions, 25% of hospitals carry out fewer than 20 procedures/year.
Standardised Rate of Severe Complications (Clavien-Dindo>2) in the Current Situation: Estimation and Modelling
Supplement Figure S1 shows the distribution of the median standardised complication rates for hospitals in the different regions, with some regions exceeding the national rate of 28%, such as Centre-Val-de-Loire, Corsica, Grand-Est and Ile-de-France. The 90/10 interdecile ratios for the regions are shown in Figure 1.
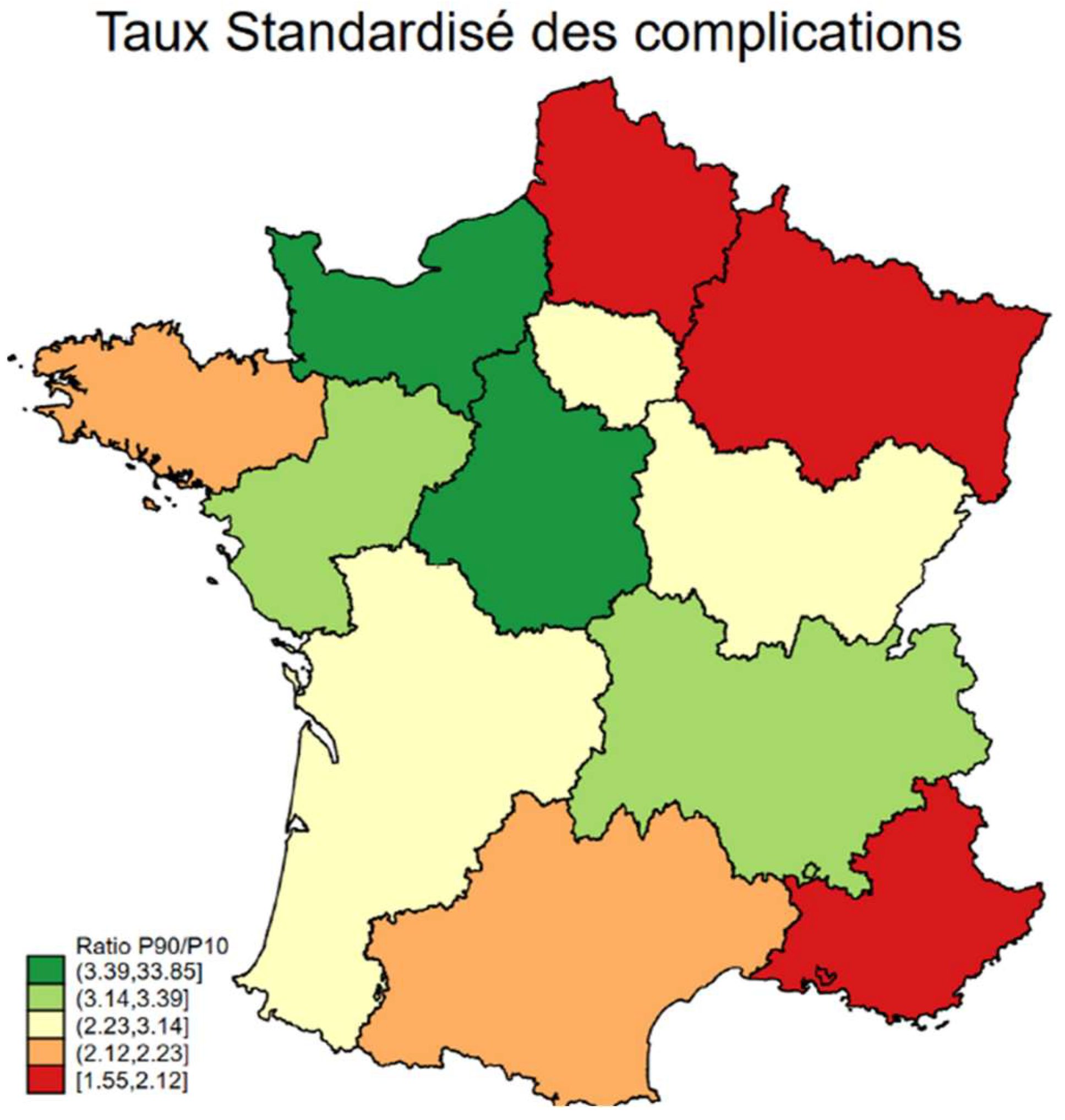
This ratio is greater than 3, meaning severe complication rates up to three times higher between hospitals, for the following regions: Normandy, Centre-Val-de-Loire, Pays de la Loire and Rhône-Alpes-Auvergne. For the other regions, the inequalities are less significant, with ratios ranging from 2 to 1.55. The classification of hospitals into 4 quantiles of standardised complication rates is shown in Table 3. In the regions of Centre Val-de-Loire, Corsica, Grand-Est, Ile-de-France, Nouvelle Aquitaine and Provence-Alpes-Cote d'Azur, most hospitals fell into the classes with a high rate of severe complications. In the other regions, the distribution was fairly balanced between the 4 classes, except for Pays de la Loire where most hospitals were in the 1st class with a low rate of severe complications.
The number of annual procedures, transformed into 3 classes, was included in the hierarchical logistic regression model used to estimate inter-regional variance (Table 4). Teams from hospitals performing more than 100 lung resections per year reduced the risk of having a severe complication or post-operative death by 20% compared with hospitals performing less than 100 procedures/year (aOR=0.83[ 0.77-0.89] for hospitals performing between 101 and 250 lung resections per year and AOR=0.85[0.77-0.93] for hospitals performing more than 250 procedures/year). Private not-for-profit and private for-profit hospitals had respective aORs of 1.35[1.19-1.52] and 1.10[1.01- 1.19] compared with non-academic hospitals (Table 4). The median OR was 1.132, showing moderate heterogeneity between regions, taking into account the same patient and hospital characteristics.
Estimate of the Standardised Rate of Severe Complications (Clavien-Dindo>2) After Simulation of a Reorganisation Of Hospitals
Following the results of our model, we simulated a reorganisation of the hospitals, taking 100 procedures/year as a threshold value to be authorised to perform LC surgery. If this were the case, only 44 hospitals would be performing lung resections for cancer. This hypothetical organisation would have made it possible to avoid 477 severe complications or deaths.
4. Discussion
This study, conducted from 2019 to 2023, included all French hospitals (171 hospitals) performing lung cancer surgery hospitals. While the differences in severe complication (Clavien-Dindo>2) rates between regions are minor, the variations between hospitals within those regions are significant with complication rates up to three times higher between hospitals. We identified that the primary factor explaining this variation is low surgical volume and that the results are much better for hospitals carrying out more than 100 procedures/year. After observing that many hospitals had a low surgical volume (in most regions, 25% of hospitals perform fewer than 20 procedures/year), we simulated a new organisation in which a threshold of 100 procedures/year would be required to be authorised to perform this surgery. This simulated organisation, with a number of authorised hospitals reduced to 44, enabled us to estimate that 477 severe post-operative complications or deaths could have been avoided over the period 2019-2023.
The limitations of our study primarily relate to the use of ICD-10 codes for patient selection and outcome assessment. Misclassification or underreporting of biases, especially regarding comorbidities, is a potential limitation of this study. Coding practices may differ between hospitals, as diagnoses can be recorded by either clinicians or information system technicians. However, the quality of coding is routinely audited in a standardized manner by medical information professionals at each hospital to ensure the accuracy of diagnoses and enhance the documentation of comorbidities.
It is also conceivable that there could be significant differences between hospitals regarding the severity of illness, which could impact the analyses of mortality and severe postoperative complications. Nevertheless, we used a multilevel analysis model to account for this variability between hospitals. In addition, over-reporting of milder forms of complications would not have a significant impact on our results since we focused on severe complications.
Another limitation concerns the tumor, node, metastasis (TNM) stage, which can influence mortality but cannot be recorded in the PMSI. However, metastatic stages were excluded from the analyses. Additionally, it is the type of lung resection that influences 30-day mortality and severe postoperative complications, independent of TNM stage [9].
Moreover, there is a lack of certain variables, including the American Society of Anesthesiologists (ASA) score, ECOG performance status, smoking history and forced expiratory volume in one second (FEV1). However, we accounted for pre-existing pulmonary disease, which usually correlates with impaired FEV1. We also utilised the modified CCI, which has been validated as a preoperative risk score. The body mass index (BMI) is not included in our database, but we included obesity in the metabolic disease variable.
The PMSI database did not provide information on the number of beds in the surgical and intensive care unit, nurses, medical practitioners and surgeries performed by residents. This database did not contain data on the organisation of the surgical team, such as tumor board meetings, adherence to guidelines and surgeon experience. However, these factors could potentially impact the quality of care. Patient quality of life is another essential indicator that cannot be measured by the PMSI.
One of the strength of our findings is the large sample size comprising 64,304 patients. Our national administrative database is an invaluable resource for evaluating the quality of care, as it collects detailed patient information from all hospitals in France, with nationwide recruitment over a five-year period. It offers a comprehensive source of epidemiological data on hospitalised patients in France [14,15]. Furthermore, the data related to pulmonary resection for LC are sufficiently reliable, allowing for precise identification of these patients, as demonstrated in previous studies [9].
The aim of this study was to assess the results of LC surgery, showing the variability in quality of care between hospitals. Our results demonstrate that there is a need to change how this type of surgery is currently offered in France. In particular, centralisation would be an appropriate means to ensure that hospitals performing LC surgery to have sufficient volumes of activity. This type of study has not been carried out in France so far [16,17,18,19].
According to a literature review previously published by our team, the standardised 30-day mortality rate for LC surgery is higher in France than in most other European countries. In light of our findings, it is worth considering whether these differences can be partly explained by the dispersion of surgical teams in France, some of which have low annual case volumes. For instance, when we compare England and France, which have similar populations, only 27 hospitals in England have been authorised to perform lung resections versus 146 in France [20].
Many countries have already recognised the need to consolidate the hospitals performing these surgeries, a process known as regionalisation. For example, Denmark, Sweden, Finland, England, Norway, Portugal, and Ireland have implemented regionalisation of surgical facilities for complex operations. Other countries, like Austria, Germany, Switzerland, the Netherlands, and Belgium, have opted to increase the minimum threshold required to obtain authorisation.
In all these countries, the current minimum threshold is higher than in France [21,22,23], and even if the authorisation threshold for cancer surgery has recently been raised from 30 to 40 procedures/year [3], this threshold remains lower.
This study appears to confirm the detrimental effect of the dispersion of LC surgery on quality of care, especially since this dispersion is not evenly distributed.
The principle of consolidating hospitals to provide high-performing surgical facilities that benefit patients is supported by numerous publications, which have shown that the volume of surgical activity correlates with the quality of care. Furthermore, it has been shown that the dispersion of hospitals creates inequalities in patient access to innovative technologies, such as robotic surgery. For instance, teams that perform few surgical procedures struggle to implement robotic surgery programs. These programs require surgeons to undergo adequate training, which is difficult to achieve effectively if the surgical activity is too low.
We believe that the consolidation of surgical facilities can only be successful if it is carried out on a regional scale, in consultation with relevant stakeholders, and taking into account the specific needs of the population, particularly their socio-demographic characteristics. The designated hospital should include high-performing surgical facilities, both in terms of operating rooms and intensive care units, with access to innovative technologies. Another crucial criterion is the competence of the medical and surgical teams, as well as multidisciplinary collaboration. Consolidation could make selected hospitals more attractive to practitioners, offering them the opportunity to train and work within competent multidisciplinary teams.
5. Conclusions
This study shows that there are differences in practice between hospitals in each French region. However, variations in the standardised complication rate between regions remain moderate. The significant influence of the volume of activity on the occurrence of severe post-operative complications and mortality raises questions about the need to restructure the offer of care for complex surgeries such as LC surgery.
While the authorisation threshold for cancer surgery was recently raised from 30 to 40 procedures/year, this work suggests that to improve the results of LC surgery, this threshold should be raised to at least 100 procedures/year, if France wants to catch up with other European countries in terms of quality of results.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1. Distribution of the median observed rate and standardised rate of severe complications (Clavien-Dindo > 2) in metropolitan regions
Author Contributions
Conceptualization, AB and CQ; methodology, AB and CQ; software, JC and AB; validation, JC, AB and CQ; formal analysis, JC and AB.; writing—original draft preparation, AB; writing—review and editing, JC, AB and CQ; supervision, AB and CQ. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the Fondation ARC pour la recherche sur le cancer (www.fondation-arc.org) which had no role in the study. We also confirm the independence of researchers from the funder and that all authors, external and internal, had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the National Committee for data protection: declaration of conformity to the methodology of reference 05 obtained on 7/08/2018 under the number 2204633 v0.
Informed Consent Statement
Patient consent was not required, and patient-identifying information was not used in the research as this national retrospective study was based on pseudonymised data. In fact, the French national administrative hospital database does not contain any patient-identifying data. The patient's identity is pseudonymised, making it possible to link data from the same patient without knowing his or her identity.
Data Availability Statement
The use of the data from the French hospital database by our department was approved by the National Committee for data protection. We are not allowed to transmit these data. PMSI data are available for researchers who meet the criteria for access to these French confidential data (this access is submitted to the approval of the National Committee for data protection) from the national agency for the management of hospitalization (ATIH - Agence technique de l'information sur l'hospitalisation).vAddress: Agence technique de l'information sur l'hospitalisation 117 boulevard Marius Vivier Merle - 69329 Lyon Cedex 03
Acknowledgments
The authors thank Suzanne Rankin for reviewing the English and Gwenaëlle Periard for her help with the layout and management of this article.
Conflicts of Interest
No competing interest.
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; et al. Cancer statistics for the year 2020: An overview. Int J Cancer 2021. [CrossRef] [PubMed]
- Ministère de l’Enseignement Supérieur et de la Recherche, Ministère de la Santé et des Sports. Plan Cancer 2009– 2013. Available online: http://www.e-cancer.fr/Plan-cancer/Les-Plans-cancer-de-2003-a-2013/Le-Plancancer-2009-2013. Date last accessed: March 2016. Date last updated: September 30, 2012.
- Institut National Du Cancer. L’organisation de l’offre de soins - Professionnels de santé [Internet]. [cité 1 oct 2024]. Disponible sur: https://www.e-cancer.fr/Professionnels-de-sante/L-organisation-de-l-offre-de-soins/.
- Kozower, B.D.; O’Brien, S.M.; Kosinski, A.S.; Magee, M.J.; Dokholyan, R.; Jacobs, J.P.; et al. The Society of Thoracic Surgeons Composite Score for Rating Program Performance for Lobectomy for Lung Cancer. Ann Thorac Surg. 2016, 101, 1379–86. [Google Scholar] [CrossRef] [PubMed]
- Ten Berge, M.G.; Beck, N.; Steup, W.H.; Verhagen, A.F.T.M.; van Brakel, T.J.; Schreurs, W.H.; et al. Textbook outcome as a composite outcome measure in non-small-cell lung cancer surgery. Eur J Cardio-Thorac Surg Off J Eur Assoc Cardio-Thorac Surg. 2021, 59, 92–99. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. http://apps.who.int/classifications/icd10/browse/2016/en Date last accessed: March 1, 2016. Date last updated: 2016.
- Iezzoni, L.I. Assessing quality using administrative data. Ann Intern Med. 1997, 127, 666–674. [Google Scholar] [CrossRef]
- Bernard, A.; Cottenet, J.; Pagès, P.B.; Quantin, C. Mortality and failure-to-rescue major complication trends after lung cancer surgery between 2005 and 2020: a nationwide population-based study. BMJ Open. 2023, 13, e075463. [Google Scholar] [CrossRef]
- Bernard, A.; Cottenet, J.; Quantin, C. Is the Validity of Logistic Regression Models Developed with a National Hospital Database Inferior to Models Developed from Clinical Databases to Analyze Surgical Lung Cancers? Cancers 2024, 16, 734. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Seely, A.J.E.; Ivanovic, J.; Threader, J.; Al-Hussaini, A.; Al-Shehab, D.; Ramsay, T.; et al. Systematic classification of morbidity and mortality after thoracic surgery. Ann Thorac Surg. 2010, 90, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W. Clinical prediction models. A practical approach to development, validating and updating. SpringerVerlag, New York 16. Funnel plots for comparing institutional. 2009.
- Normand, S.L.T.; Shahian, D.M. Statistical and Clinical Aspects of Hospital Outcomes Profiling. Stat Sci. 2007, 22, 206–226. [Google Scholar] [CrossRef]
- Piroth, L.; Cottenet, J.; Mariet, A.S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; et al. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: a nationwide, population-based retrospective cohort study. Lancet Respir Med. 2021, 9, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Viennet, M.; Tapia, S.; Cottenet, J.; Bernard, A.; Ortega-Deballon, P.; Quantin, C. Increased risk of colon cancer after acute appendicitis: a nationwide, population-based study. EClinicalMedicine 2023, 63, 102196. [Google Scholar] [CrossRef] [PubMed]
- David, E.A.; Cooke, D.T.; Chen, Y.; Perry, A.; Canter, R.J.; Cress, R. Surgery in high-volume hospitals not commission on cancer accreditation leads to increased cancer-specific survival for early-stage lung cancer. Am J Surg. 2015, 210, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Siewers, A.E.; Finlayson, E.V.A.; Stukel, T.A.; Lucas, F.L.; Batista, I.; et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002, 346, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, E.V.A.; Goodney, P.P.; Birkmeyer, J.D. Hospital volume and operative mortality in cancer surgery: a national study. Arch Surg Chic Ill 1960. 2003, 138, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Lien, Y.C.; Huang, M.T.; Lin, H.C. Association between surgeon and hospital volume and in-hospital fatalities after lung cancer resections: the experience of an Asian country. Ann Thorac Surg. 2007, 83, 1837–1843. [Google Scholar] [CrossRef] [PubMed]
- Bernard, A.; Riviere, A.; Cottenet, J.; Madeleine, L.; Quantin, C.; Pages, P.B. Comparaison de la mortalité des résections pulmonaires en France aux autres pays Européens. Rev Mal Respir. 2022, 39, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.R.; Voeten, D.M.; Gisbertz, S.S.; Ruurda, J.P.; Achiam, M.P.; Nilsson, M.; et al. Western European Variation in the Organization of Esophageal Cancer Surgical Care. Dis Esophagus Off J Int Soc Dis Esophagus. 2024, 37, doae033. [Google Scholar] [CrossRef] [PubMed]
- Sheetz, K.H.; Dimick, J.B.; Nathan, H. Centralization of High-Risk Cancer Surgery Within Existing Hospital Systems. J Clin Oncol Off J Am Soc Clin Oncol. 2019, 37, 3234–3242. [Google Scholar] [CrossRef] [PubMed]
- Vonlanthen, R.; Lodge, P.; Barkun, J.S.; Farges, O.; Rogiers, X.; Soreide, K.; et al. Toward a Consensus on Centralization in Surgery. Ann Surg. 2018, 268, 712–724. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Distribution of Clavien-Dindo classification, especially post-operative complications and 30-day mortality (Clavien-Dindo > 2).
Table 1.
Distribution of Clavien-Dindo classification, especially post-operative complications and 30-day mortality (Clavien-Dindo > 2).
| 2019 | 2020 | 2021 | 2022 | 2023 | |
| n=12,367 | n=11,792 | n=12,542 | n=13,376 | n=14,227 | |
| None | 6,528 (52.8) | 6,298 (53.4) | 6,972 (55.6) | 7,594 (56.8) | 7,969 (56.0) |
| Clavien-Dindo ≤ 2 | 1,863 (15.1) | 1,764 (15.0) | 1,911 (15.2) | 2,039 (15.2) | 2,331 (16.4) |
| Clavien-Dindo > 2 | |||||
| Clavien-Dindo IIIa | 1,308 (10.6) | 1,207 (10.2) | 1,178 (9.4) | 1,264 (9.4) | 1,375 (9.7) |
| Clavien-Dindo IIIb | 638 (5.2) | 652 (5.5) | 634 (5.1) | 668 (5.0) | 748 (5.3) |
| Clavien-Dindo IVa | 337 (2.7) | 361 (3.1) | 408 (3.3) | 440 (3.3) | 497 (3.5) |
| Clavien-Dindo IVb | 1,412 (11.4) | 1,240 (10.5) | 1,196 (9.5) | 1,151 (8.6) | 1,088 (7.6) |
| Clavien-Dindo V | 281 (2.3) | 270 (2.3) | 243 (1.9) | 220 (1.6) | 219 (1.5) |
(Percentage).
Table 2.
Description of the number of annual procedures for hospitals in each region.
| Region | Number of hospitals | Number of procedures | ||||
| p10 | p25 | Median | p75 | p90 | ||
| ARA | 24 | 10 | 10 | 50 | 87 | 106 |
| BFC | 5 | 10 | 20 | 35 | 43 | 281 |
| BRE | 13 | 10 | 35 | 70 | 97 | 128 |
| COR | 2 | 16 | 16 | 20 | 23 | 23 |
| CVL | 8 | 10 | 23 | 44 | 68 | 122 |
| GE | 13 | 10 | 56 | 121 | 139 | 218 |
| HdF | 12 | 10 | 20 | 71 | 108 | 222 |
| IdF | 19 | 10 | 11 | 54 | 135 | 327 |
| NA | 17 | 10 | 27 | 41 | 96 | 138 |
| NOR | 8 | 10 | 18 | 42 | 135 | 261 |
| OCC | 17 | 10 | 27 | 53 | 87 | 238 |
| PACA | 19 | 10 | 17 | 51 | 101 | 229 |
| PdL | 14 | 10 | 10 | 43 | 56 | 113 |
Auvergne-Rhones-Alpes (ARA), Bourgogne-Franche-Comté (BFC), Bretagne (BRE), Corse (COR), Centre Val-de-Loire (CVL), Grand-Est (GE), Hauts-de-France (HdF), Ile-de-France (IdF), Nouvelle Aquitaine (NA), Normandie (NOR), Occitanie (OC), Provence-Alpes-Côte d’Azur (PACA), Pays de la Loire (PdL).
Table 3.
Number of hospitals in each region according to their level of performance.
| Regions | Quantiles of the standardised severe complication (Clavien-Dindo > 2) rate | |||
| <23% | 23-26% | 27-35% | >35% | |
| ARA | 7 | 6 | 7 | 4 |
| 29.17 | 25.00 | 29.17 | 16.67 | |
| BFC | 1 | 2 | 2 | 0 |
| 20.00 | 40.00 | 40.00 | 0.00 | |
| BRE | 7 | 2 | 3 | 1 |
| 53.85 | 15.38 | 23.08 | 7.69 | |
| CVL | 1 | 1 | 4 | 2 |
| 12.50 | 12.50 | 50.00 | 25.00 | |
| COR | 0 | 0 | 0 | 2 |
| 0.00 | 0.00 | 0.00 | 100.00 | |
| GE | 2 | 0 | 5 | 6 |
| 15.38 | 0.00 | 38.46 | 46.15 | |
| HdF | 5 | 1 | 4 | 2 |
| 41.67 | 8.33 | 33.33 | 16.67 | |
| IdF | 5 | 3 | 2 | 9 |
| 26.32 | 15.79 | 10.53 | 47.37 | |
| NOR | 6 | 1 | 0 | 1 |
| 75.00 | 12.50 | 0.00 | 12.50 | |
| NA | 5 | 2 | 6 | 4 |
| 29.41 | 11.76 | 35.29 | 23.53 | |
| OCC | 7 | 5 | 1 | 4 |
| 41.18 | 29.41 | 5.88 | 23.53 | |
| PdL | 8 | 2 | 2 | 2 |
| 57.14 | 14.29 | 14.29 | 14.29 | |
| PACA | 3 | 5 | 5 | 6 |
| 15.79 | 26.32 | 26.32 | 31.58 | |
Auvergne-Rhones-Alpes (ARA), Bourgogne-Franche-Comté (BFC), Bretagne (BRE), Corse (COR), Centre Val-de-Loire (CVL), Grand-Est (GE), Hauts-de-France (HdF), Ile-de-France (IdF), Nouvelle Aquitaine (NA), Normandie (NOR), Occitanie (OC), Provence-Alpes-Côte d’Azur (PACA), Pays de la Loire (PdL).
Table 4.
Hierarchical logistic regression: Adjusted Odds Ratio of number of annual procedures and type of hospital on the risk of severe complication (Clavien-Dindo > 2).
Table 4.
Hierarchical logistic regression: Adjusted Odds Ratio of number of annual procedures and type of hospital on the risk of severe complication (Clavien-Dindo > 2).
| aOR | 95%CI | p-value | |
| Number of annual procedures <100 101-250 >250 |
1 0.83 0.85 |
0.77-0.89 0.77-0.93 |
0.0001 |
| Type of hospital Non-academic hospital Academic (teaching) hospital Non-profit private hospital Private hospital |
1 0.98 1.35 1.10 |
0.89-1.08 1.19-1.52 1.01- 1.19 |
0.0001 |
| Inter-regional variance | 0.034 | 0.015-0.077 |
95%CI: 95% confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



