
Submitted:
14 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Background and Objectives: Communication gaps contribute substantially to anxiety, depression, and post-traumatic stress disorder (PTSD) among relatives of critically ill patients. This study evaluated whether supplementing routine bedside meetings with a concise, co-designed informational brochure was associated with reduced psychological distress and improved satisfaction among family members in the intensive care unit (ICU). Materials and Methods: We conducted a single-centre prospective before–after observational study in a mixed medical–surgical ICU in Naples, Italy. Relatives of adult patients with an ICU length of stay >72 h completed the Hospital Anxiety and Depression Scale (HADS) and the Short Screening Scale for PTSD (SSS-PTSD) at ICU discharge. The pre-intervention phase enrolled 12 relatives (May–September 2018); following a co-design and staff training period, the post-intervention phase enrolled 23 relatives (April–October 2019). Primary outcomes were the prevalence of anxiety (HADS-A ≥8), depression (HADS-D ≥8), and probable PTSD (SSS-PTSD ≥4). Groups were compared using Fisher’s exact test and the Mann–Whitney U test. Results: Anxiety remained highly prevalent (100% pre vs. 95.7% post; p = 1.00). Depression severity decreased, with median HADS-D scores declining from 13 (IQR 10–18) to 9 (IQR 7–12) (p = 0.021), while the prevalence of HADS-D ≥8 was lower post-intervention (91.7% vs. 73.9%; p = 0.38). The prevalence of probable PTSD was numerically reduced from 58.3% to 30.4% (p = 0.116). Perceived comprehension improved (7.9 ± 1.1 vs. 8.6 ± 0.9; p = 0.037), whereas objective comprehension remained unchanged. Overall family satisfaction increased (FS-ICU-24: 66 ± 15 vs. 75 ± 12; p = 0.041). Staff depersonalization decreased from 35% to 10% (p = 0.048). Conclusions: In this real-world before–after study, integrating a low-cost, co-designed brochure into clinician–family communication was associated with reduced depressive symptom severity, a numerical reduction in PTSD prevalence, and improved satisfaction, without adverse effects on staff well-being. These findings support the use of structured written information in family-centred ICU care.
Keywords:
intensive care unit
; family-centred care
; anxiety
; depression
; post-traumatic stress disorder
; Hospital Anxiety and Depression Scale
; family satisfaction
1. Introduction
Admission to an intensive care unit (ICU) represents a profoundly stressful experience not only for patients but also for their family members. Relatives are suddenly exposed to a highly technological environment, uncertainty regarding prognosis, and complex medical terminology, often under conditions of emotional vulnerability. As a result, a substantial proportion of family members develop clinically relevant psychological symptoms, including anxiety, depression, and post-traumatic stress disorder (PTSD), a constellation increasingly recognized as post-intensive care syndrome–family (PICS-F) [1]. Previous studies and systematic reviews have consistently reported high rates of anxiety and depressive symptoms among relatives of critically ill patients during the ICU stay, with a non-negligible proportion developing persistent PTSD symptoms after discharge or death of the patient [2,3,4]. These psychological sequelae are not merely transient emotional reactions; they can impair decision-making capacity, reduce satisfaction with care, and adversely affect long-term quality of life for families and caregivers [5]. Consequently, international critical care societies now emphasize family-centred care as a core component of high-quality ICU practice [6]. Among the modifiable determinants of PICS-F, communication quality has emerged as one of the most influential factors. Inconsistent information delivery, limited opportunities for clarification, and difficulties in understanding the clinical situation have been repeatedly associated with higher psychological distress among family members [7,8]. Interventions aimed at improving clinician–family communication, such as structured family conferences or dedicated communication facilitators, have demonstrated benefits in selected settings, including reductions in depressive symptoms and improved satisfaction [9,10,11]. However, these approaches are often resource-intensive and may be difficult to implement consistently in routine clinical practice, particularly in settings with limited staffing or high patient turnover [12,13].
Written informational tools, including brochures, leaflets, and ICU diaries, have been proposed as lower-cost strategies to complement verbal communication. Such tools allow relatives to revisit information at their own pace, share content with other family members, and reduce uncertainty related to unfamiliar ICU processes [14,15,16,17]. Qualitative studies suggest that families value clear, accessible written materials, yet quantitative evidence regarding their impact on psychological outcomes remains limited and heterogeneous [18]. Moreover, few studies have evaluated co-designed materials developed with direct input from families and frontline clinicians.
The need for scalable, low-resource communication strategies became particularly evident during the COVID-19 pandemic, when visiting restrictions further strained clinician–family interactions and exacerbated psychological distress among relatives [5,16]. These circumstances highlighted the importance of interventions that can enhance understanding and emotional support without increasing staff workload or burnout.
Against this background, we conducted a single-centre prospective before–after study to evaluate whether supplementing routine bedside discussions with a concise, co-designed informational brochure was associated with reduced anxiety, depression, and PTSD symptoms among ICU relatives at the time of patient discharge. Secondary objectives included assessing perceived and objective comprehension of clinical information, family satisfaction with care, and potential effects on staff well-being. We hypothesized that the introduction of a structured written communication tool would be associated with lower psychological distress and improved satisfaction, without adverse effects on clinicians.
2. Materials and Methods
2.1. Study Design and Setting
We conducted a single-centre prospective before–after observational study in a six-bed mixed medical–surgical intensive care unit (ICU) at the University of Campania “Luigi Vanvitelli” Teaching Hospital, Naples, Italy. The ICU admits postoperative and emergency patients, excluding neurosurgical trauma. Standard visiting hours consisted of one 60-minute visit per day. No dedicated family liaison service was available during the study period.
The pre-intervention phase was conducted from May to September 2018. Following a co-design and staff training period, the post-intervention phase took place from April to October 2019. The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
2.2. Intervention: Co-Designed Informational Brochure
The intervention consisted of a concise, pictorial informational brochure designed to complement routine bedside clinician–family discussions. The brochure was developed through a multidisciplinary co-design process involving former ICU family advisors, bedside nurses, and intensivists. Key content areas included: (i) ICU layout and visitation rules; (ii) explanations of common monitoring devices and life-support equipment; (iii) simplified schematics of major organ failures and supportive therapies; (iv) typical clinical trajectories and recovery milestones; and (v) explicit acknowledgment of prognostic uncertainty. The brochure was provided in Italian, with an English version available upon request.
Before implementation, ICU clinicians participated in a 60-minute training session focused on empathetic communication, teach-back techniques, and appropriate integration of the brochure into routine bedside updates. During the post-intervention phase, the brochure was handed to relatives at the first bedside meeting and referenced during subsequent encounters.
2.3. Participants
Eligible participants were first-degree relatives (spouse, parent, or adult child) of adult ICU patients with a length of stay exceeding 72 h. Exclusion criteria were insufficient proficiency in Italian or English, documented cognitive impairment, or ongoing medico-legal disputes. During the pre-intervention period, 44 patients were admitted, of whom 28 met eligibility criteria and 12 relatives consented to participate. During the post-intervention period, 158 patients were admitted, 41 were eligible, and 23 relatives participated.
2.4. Outcome Measures
2.4.1. Psychological Distress
Anxiety and depressive symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS), which includes two subscales (HADS-A and HADS-D), each ranging from 0 to 21. Scores ≥8 indicate at least mild symptoms, and scores ≥11 indicate probable clinical caseness. Post-traumatic stress symptoms were screened using the Short Screening Scale for PTSD (SSS-PTSD), a seven-item questionnaire in which scores ≥4 indicate probable PTSD.
2.4.2. Comprehension and Family Satisfaction
Perceived comprehension of clinical information was measured using a 0–10 visual analogue scale. Objective comprehension was assessed using a structured Comprehension Assessment Interview, in which clinicians and relatives independently listed affected organs and ongoing treatments; concordance was expressed as a percentage. Family satisfaction was evaluated using the 24-item Family Satisfaction in the ICU questionnaire (FS-ICU-24), including overall and information subscale scores.
2.4.3. Staff Well-Being
Clinician well-being was assessed using the Maslach Burnout Inventory–Human Services Survey, focusing on emotional exhaustion, depersonalization, and personal accomplishment, and the Jefferson Scale of Physician Empathy.
2.5. Endpoints
Primary endpoints were the prevalence of anxiety (HADS-A ≥8), depression (HADS-D ≥8), and probable PTSD (SSS-PTSD ≥4) at ICU discharge. Secondary endpoints included median HADS scores, perceived and objective comprehension, FS-ICU-24 scores, and changes in staff burnout and empathy.
2.6. Statistical Analysis
Continuous variables are presented as mean ± standard deviation or median with interquartile range (IQR), as appropriate, and were compared using Student’s t-test or the Mann–Whitney U test. Categorical variables are reported as counts and percentages and were compared using two-sided Fisher’s exact test. Effect sizes were expressed as r for continuous outcomes and φ for categorical outcomes. All tests were two-tailed with a significance threshold of p < 0.05. No adjustment for multiple comparisons was applied due to the exploratory nature of the study. Statistical analyses were performed using R software (version 4.3).
2.7. Ethics and Consent
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were assessed according to the institutional framework in place at the time of the study; due to subsequent institutional reorganization and replacement of local Ethics Committees after 2018, archival documentation of the original ethics approval is no longer available from the currently competent Ethics Committee. The study was observational and non-interventional. Written informed consent was waived, and verbal consent to participate was obtained from all enrolled relatives.
2.8. Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request, subject to privacy and ethical restrictions.
2.9. Generative Artificial Intelligence Disclosure
Generative artificial intelligence tools were not used for data analysis, study design, or interpretation of results. The use of AI-assisted tools was limited to language editing and formatting, and therefore does not require formal disclosure according to MDPI guidelines.
3. Results
Baseline characteristics and all study outcomes are summarized in Table 1. The main psychological outcomes are visually depicted in Figure 1.
3.1. Psychological Outcomes
Anxiety symptoms, defined as a Hospital Anxiety and Depression Scale–Anxiety (HADS-A) score ≥ 8, were highly prevalent in both study phases, affecting all relatives in the pre-intervention group (12/12, 100%) and nearly all relatives in the post-intervention group (22/23, 95.7%), with no statistically significant difference between groups (p = 1.00; Table 1, Figure 1a). Median HADS-A scores showed a non-significant numerical decrease after the intervention (15 [IQR 13–17] vs. 14 [IQR 9–15]; p = 0.097; Table 1).
Depressive symptoms were less severe following the introduction of the brochure. Although the prevalence of HADS-D ≥ 8 decreased from 91.7% (11/12) in the pre-intervention phase to 73.9% (17/23) in the post-intervention phase, this difference did not reach statistical significance (p = 0.38; Table 1, Figure 1b). In contrast, median HADS-D scores were significantly lower in the post-intervention group (13 [IQR 10–18] vs. 9 [IQR 7–12]; p = 0.021; Table 1).
The prevalence of probable post-traumatic stress disorder (PTSD), defined as a Short Screening Scale for PTSD (SSS-PTSD) score ≥ 4, was numerically reduced after the intervention, declining from 58.3% (7/12) in the pre-intervention group to 30.4% (7/23) in the post-intervention group, although this difference did not reach statistical significance (p = 0.116; Table 1, Figure 1c).
3.2. Comprehension and Family Satisfaction
Perceived comprehension of clinical information improved significantly after the introduction of the brochure, increasing from a mean score of 7.9 ± 1.1 to 8.6 ± 0.9 (p = 0.037; Table 1). Objective comprehension, assessed by concordance between clinician and relative reports, remained unchanged for both affected organ systems and ongoing treatments (Table 1).
Overall family satisfaction, measured using the Family Satisfaction in the Intensive Care Unit questionnaire (FS-ICU-24), increased significantly in the post-intervention phase (66 ± 15 vs. 75 ± 12; p = 0.041; Table 1).
3.3. Staff Well-Being
Measures of staff well-being are reported in Table 1. The proportion of clinicians with high depersonalization scores decreased from 35% in the pre-intervention phase to 10% in the post-intervention phase (p = 0.048). No statistically significant differences were observed in emotional exhaustion or personal accomplishment scores. Mean scores on the Jefferson Scale of Physician Empathy remained stable across study phases.
4. Discussion
In this single-centre prospective before–after study, the introduction of a concise, co-designed informational brochure integrated into routine clinician–family communication was associated with a reduction in depressive symptom severity, a numerical decrease in the prevalence of probable post-traumatic stress disorder (PTSD), and improved family satisfaction, without adverse effects on staff well-being. Anxiety symptoms remained highly prevalent in both study phases, highlighting the complexity of psychological distress among relatives of critically ill patients.
The most robust finding of the present study was the significant reduction in depressive symptom severity, as reflected by lower median HADS-D scores after the intervention. Although the proportion of relatives meeting the HADS-D ≥ 8 threshold did not differ significantly between groups, the observed shift toward lower symptom severity suggests a clinically meaningful benefit. This pattern is consistent with prior studies indicating that structured communication interventions may be more effective in mitigating depressive burden than in eliminating distress altogether, particularly in the acute ICU setting.
The prevalence of probable PTSD was approximately halved following the introduction of the brochure, although this difference did not reach statistical significance. Given the limited sample size, this finding should be interpreted cautiously; however, the direction and magnitude of the effect are aligned with existing evidence identifying communication quality as a key modifiable determinant of post-intensive care syndrome–family (PICS-F). Written informational tools may contribute to PTSD risk reduction by decreasing uncertainty, normalizing the ICU experience, and allowing relatives to process information at their own pace.
In contrast, anxiety symptoms remained almost universal both before and after the intervention. Acute anxiety among ICU relatives is likely driven by factors beyond informational needs alone, including perceived threat to life, emotional attachment, and uncertainty regarding outcomes. These findings suggest that while written communication tools may alleviate depressive and post-traumatic stress symptoms, they are insufficient as a standalone strategy to address anxiety in this context and should be complemented by additional emotional or psychological support interventions.
An important secondary finding was the improvement in perceived comprehension of clinical information, despite unchanged objective comprehension. This dissociation suggests that the brochure primarily enhanced emotional reassurance and confidence rather than factual recall. Such an effect is clinically relevant, as perceived understanding has been shown to influence satisfaction, trust in clinicians, and engagement in shared decision-making, even when objective knowledge remains stable.
Notably, the intervention was associated with a reduction in staff depersonalization without changes in emotional exhaustion or empathy scores. This finding challenges concerns that enhanced family communication may increase clinician workload or burnout. On the contrary, clearer expectations and improved family understanding may reduce emotionally taxing interactions, supporting the sustainability of low-resource communication strategies in routine ICU practice.
The present study has several limitations. Its single-centre design and modest sample size limit generalizability and statistical power, particularly for binary outcomes such as PTSD prevalence. The non-randomized before–after design introduces potential confounding related to temporal changes in practice or case mix. Additionally, psychological outcomes were assessed at ICU discharge, precluding conclusions regarding long-term persistence of benefits.
Despite these limitations, the study has notable strengths, including its prospective design, use of validated psychological instruments, integration of both family- and staff-centred outcomes, and focus on a pragmatic, low-cost intervention developed through a co-design process. Importantly, the intervention was implemented without additional personnel or structural resources, enhancing its scalability.
Future research should include multicentre randomized or cluster-randomized studies with larger samples and longer follow-up to confirm the durability of observed effects and to identify subgroups most likely to benefit. The integration of written materials with digital tools or structured emotional support interventions may further enhance outcomes for families of critically ill patients.
In summary, supplementing routine ICU communication with a concise, co-designed informational brochure was associated with reduced depressive symptom severity, improved satisfaction, and preserved staff well-being. These findings support the incorporation of structured written information into family-centred ICU care as a feasible and scalable strategy.
5. Conclusions
In this prospective before–after study, the integration of a concise, co-designed informational brochure into routine clinician–family communication in the intensive care unit was associated with a reduction in depressive symptom severity, a numerical decrease in the prevalence of probable post-traumatic stress disorder, and improved family satisfaction, without adverse effects on staff well-being. Anxiety symptoms remained highly prevalent, indicating that written informational tools alone are insufficient to address all dimensions of psychological distress among relatives of critically ill patients.
These findings suggest that structured written information, when embedded within empathic bedside communication, may represent a feasible, low-cost, and scalable component of family-centred ICU care. Larger multicentre studies with longer follow-up are warranted to confirm the durability of these effects and to define the optimal integration of written materials with additional psychological support strategies.
Author Contributions
Conceptualization, M.F.; methodology, V.P.; formal analysis, M.F.; data curation, N.P.; visualization, F.C.; writing—original draft preparation, M.F.; writing—review and editing, M.C.P., M.B.P., and M.F.; project administration, P.S.; funding acquisition, M.C.P. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by Italy’s National Recovery and Resilience Plan (PNRR), Mission 4 “Education and Research,” Component 2 “From Research to Business,” Investment 1.3 “Creation of extended partnerships among universities, research centers, and enterprises for funding fundamental research projects,” funded by the European Union – NextGenerationEU (CUP I83C22001810007). The APC was funded by the authors. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the local Ethics Committee of the University of Campania “Luigi Vanvitelli” in 2018. Due to subsequent institutional reorganization, the original approval documentation is no longer retrievable.
Informed Consent Statement
Informed consent to participate was obtained verbally from all subjects involved in the study. Written informed consent for publication was not required, as no identifiable personal data are included in this manuscript.
Data Availability Statement
Data Availability Statement: The data supporting the findings of this study are not publicly available due to privacy and ethical restrictions. Anonymized data may be made available from the corresponding author upon reasonable request, subject to institutional and ethical approval.
Acknowledgments
The authors would like to thank the nursing staff of the Intensive Care Unit of the University of Campania “Luigi Vanvitelli” Teaching Hospital for their support in facilitating family communication and data collection during the study period. During the preparation of this manuscript, the authors used generative artificial intelligence tools for language editing and formatting purposes only. The authors reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ICU | Intensive Care Unit |
| PICS-F | Post-Intensive Care Syndrome–Family |
| HADS | Hospital Anxiety and Depression Scale |
| HADS-A | Hospital Anxiety and Depression Scale—Anxiety |
| HADS-D | Hospital Anxiety and Depression Scale—Depression |
| PTSD | Post-Traumatic Stress Disorder |
| SSS-PTSD | Short Screening Scale for Post-Traumatic Stress Disorder |
| FS-ICU-24 | Family Satisfaction in the Intensive Care Unit questionnaire |
| VAS | Visual Analogue Scale |
| IQR | Interquartile Range |
| PNRR | National Recovery and Resilience Plan |
References
- Smith, A.C.; Ferguson, H.N.; Russell, R.M.; Savsani, P.; Wang, S. Post-intensive care syndrome–family. Crit. Care Clin. 2025, 41, 73–88. [Google Scholar] [CrossRef]
- Curtis, J.R.; Treece, P.D.; Nielsen, E.L.; Gold, J.; Ciechanowski, P.S.; Shannon, S.E.; et al. Randomized trial of communication facilitators to reduce family distress and intensity of end-of-life care. Am. J. Respir. Crit. Care Med. 2016, 193, 154–162. [Google Scholar] [CrossRef]
- Ito, Y.; Tsubaki, M.; Kobayashi, M.; Yagome, S.; Sakaguchi, Y. Effect size estimates of risk factors for post-intensive care syndrome–family: A systematic review and meta-analysis. Heart Lung 2023, 59, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sarigiannis, K.A.; Tringali, J.J.; Vu, J.; Eaton England, A.; Lietzau, S.; Hebert, C.; et al. Symptoms of anxiety, depression, and stress among families of critically ill patients with COVID-19: A longitudinal clinical trial. Ann. Am. Thorac. Soc. 2023, 20, 705–712. [Google Scholar] [CrossRef]
- Krewulak, K.D.; Jaworska, N.; Spence, K.L.; Mizen, S.J.; Kupsch, S.; Stelfox, H.T.; et al. Impact of restricted visitation policies during the COVID-19 pandemic on communication between critically ill patients, families, and clinicians. Ann. Am. Thorac. Soc. 2022, 19, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, M.N.; Gee, P.M.; Hopkins, R.O.; Butler, J.M.; Groat, D.; Stokes, S.C.; et al. Patient- and family-centered outcomes after intensive care unit admission. Am. J. Crit. Care 2025, 34, 12–20. [Google Scholar] [CrossRef]
- Smerat, H.; Abu Ejheisheh, M.; Ayed, A.; Aqtam, I.; Batran, A. Patient satisfaction with the quality of nursing care in critical care units and medical wards. PLoS ONE 2025, 20, e0322804. [Google Scholar] [CrossRef]
- Park, E.J.; Seong, J.; Shin, J.W.; Tate, J.A.; Choi, J. Communication interventions for families in adult intensive care units during the COVID-19 pandemic: A systematic review. Heart Lung 2024, 68, 175–190. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.Y.; Oczkowski, S.J.W.; Lewis, K.; Birriel, B.; Downar, J.; Farrier, C.E.; et al. Society of Critical Care Medicine guidelines on family-centered care for adult ICUs: 2024 update. Crit. Care Med. 2025, 53, e465–e482. [Google Scholar] [CrossRef]
- Lv, Y.; Li, P.; Li, R.; Zhang, T.; Cai, K. Impact of patient- and family-centered care interventions on intensive care unit outcomes: A meta-analysis of randomized controlled trials. Braz. J. Anesthesiol. 2025, 75, 844577. [Google Scholar] [CrossRef]
- LaGrotte, C.A.; Baldwin, C.; Hunter, K.; Damuth, E.; Loperfido, N.; Moosavi, T.; et al. Patient and family experience in the ICU: Targets for improvement. J. Patient Exp. 2025, 12, 23743735251314650. [Google Scholar] [CrossRef]
- Liyew, T.M.; Mersha, A.T.; Admassie, B.M.; Arefayne, N.R. Family satisfaction with care provided in intensive care units: A multicenter study. Patient Relat. Outcome Meas. 2024, 15, 105–119. [Google Scholar] [CrossRef]
- Mickelson, R.S.; Piras, S.E.; Brown, L.; Carlile, C.; Drumright, K.S.; Boehm, L. The use and usefulness of ICU diaries to support family members. J. Crit. Care 2021, 61, 168–176. [Google Scholar] [CrossRef]
- Keen, A.; George, A.; Stuck, B.T.; Snyder, C.; Fleck, K.; Azar, J.; et al. Nurse perceptions of a family liaison role implemented during COVID-19. Intensive Crit. Care Nurs. 2022, 70, 103185. [Google Scholar] [CrossRef]
- Davidson, J.E.; Aslakson, R.A.; Long, A.C.; Puntillo, K.A.; Kross, E.K.; Hart, J.; et al. Guidelines for family-centered care in the ICU. Crit. Care Med. 2017, 45, 103–128. [Google Scholar] [CrossRef]
- White, D.B.; Angus, D.C.; Shields, A.M.; Buddadhumaruk, P.; Pidro, C.; Paner, C.; et al. A randomized trial of a family-support intervention in intensive care units. N. Engl. J. Med. 2018, 378, 2365–2375. [Google Scholar] [CrossRef]
- Nosaka, N.; Noguchi, A.; Takeuchi, T.; Wakabayashi, K. Long-term prevalence of PTSD symptoms in family members of severe COVID-19 patients. J. Intensive Care 2024, 12, 53. [Google Scholar] [CrossRef] [PubMed]
- Reifarth, E.; Böll, B.; Köpke, S.; Altenrath, L.; Garcia Borrega, J.; Kochanek, M.; et al. Multicomponent communication intervention to support family members of the critically ill. Crit. Care Med. 2025. [Google Scholar] [CrossRef] [PubMed]
- Negro, A.; Villa, G.; Zangrillo, A.; Rosa, D.; Manara, D.F. Diaries in intensive care units: An Italian qualitative study. Nurs. Crit. Care 2022, 27, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Calderone, A.; Debay, V.; Goldfarb, M.J. Family presence on rounds in adult critical care: A scoping review. Crit. Care Explor. 2022, 4, e0787. [Google Scholar] [CrossRef]
- Bibas, L.; Peretz-Larochelle, M.; Adhikari, N.K.J.; Goldfarb, M.J.; Luk, A.; Englesakis, M.; et al. Surrogate decision-making interventions in critical illness. JAMA Netw. Open 2019, 2, e197229. [Google Scholar] [CrossRef] [PubMed]
- Crossfield, C.; Ozavci, G.; Digby, R.; Bucknall, T. Telehealth communication with ICU families: A systematic review. Aust. Crit. Care 2025, 38, 101094. [Google Scholar] [CrossRef]
- Herrmann, C. International experiences with the Hospital Anxiety and Depression Scale. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Breslau, N.; Peterson, E.L.; Kessler, R.C.; Schultz, L.R. Short screening scale for DSM-IV post-traumatic stress disorder. Am. J. Psychiatry 1999, 156, 908–911. [Google Scholar] [CrossRef]
- Costa, D.K.; Barg, F.K.; Asch, D.A.; Kahn, J.M. Facilitators of interprofessional care in ICUs. Res. Nurs. Health 2014, 37, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Haave, R.O.; Bakke, H.H.; Schröder, A. Family satisfaction in the intensive care unit. BMC Emerg. Med. 2021, 21, 20. [Google Scholar] [CrossRef]
- Dale, B.; Frivold, G. Psychometric testing of the FS-ICU-24 questionnaire. J. Multidiscip. Healthc. 2018, 11, 653–659. [Google Scholar] [CrossRef]
- Kalyan, G.; Saini, S.K.; Kumari, B.; Kumar, P. Integrating families into neonatal care. Indian J. Pediatr. 2024, 91, 351–357. [Google Scholar] [CrossRef]
- LoBiondo-Wood, G.; Haber, J. Nursing Research: Methods and Critical Appraisal for Evidence-Based Practice, 10th ed.; Elsevier: St. Louis, MO, USA, 2021. [Google Scholar]
- Shah, M.; Surenderan, K.; Pathare, G.; Rai, S.; Patel, M.; Rathod, D.; et al. Enhancing family satisfaction in the ICU through communication. Cureus 2025, 17, e82683. [Google Scholar]
- Jorge, N.; Hipólito-Reis, I.; Esteves, N.; Costa, L.; Mendonça, I.; Oliveira, T.; et al. Family satisfaction with critical care before and after COVID-19. Cureus 2023, 15, e33853. [Google Scholar] [CrossRef] [PubMed]
- de Aquino, V.W.; da Silveira, G.F.; Boniatti, M.M.; Terres, M.D.S. Communication and shared decision-making in the ICU. Indian J. Crit. Care Med. 2024, 28, 977–987. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pre- and post-intervention prevalence of anxiety, depression, and probable post-traumatic stress disorder among relatives of intensive care unit patients. Panel (a) shows anxiety prevalence defined as HADS-A ≥ 8; panel (b) shows depression prevalence defined as HADS-D ≥ 8; panel (c) shows probable post-traumatic stress disorder defined as SSS-PTSD ≥ 4. Differences between groups were assessed using Fisher’s exact test.
Figure 1.
Pre- and post-intervention prevalence of anxiety, depression, and probable post-traumatic stress disorder among relatives of intensive care unit patients. Panel (a) shows anxiety prevalence defined as HADS-A ≥ 8; panel (b) shows depression prevalence defined as HADS-D ≥ 8; panel (c) shows probable post-traumatic stress disorder defined as SSS-PTSD ≥ 4. Differences between groups were assessed using Fisher’s exact test.
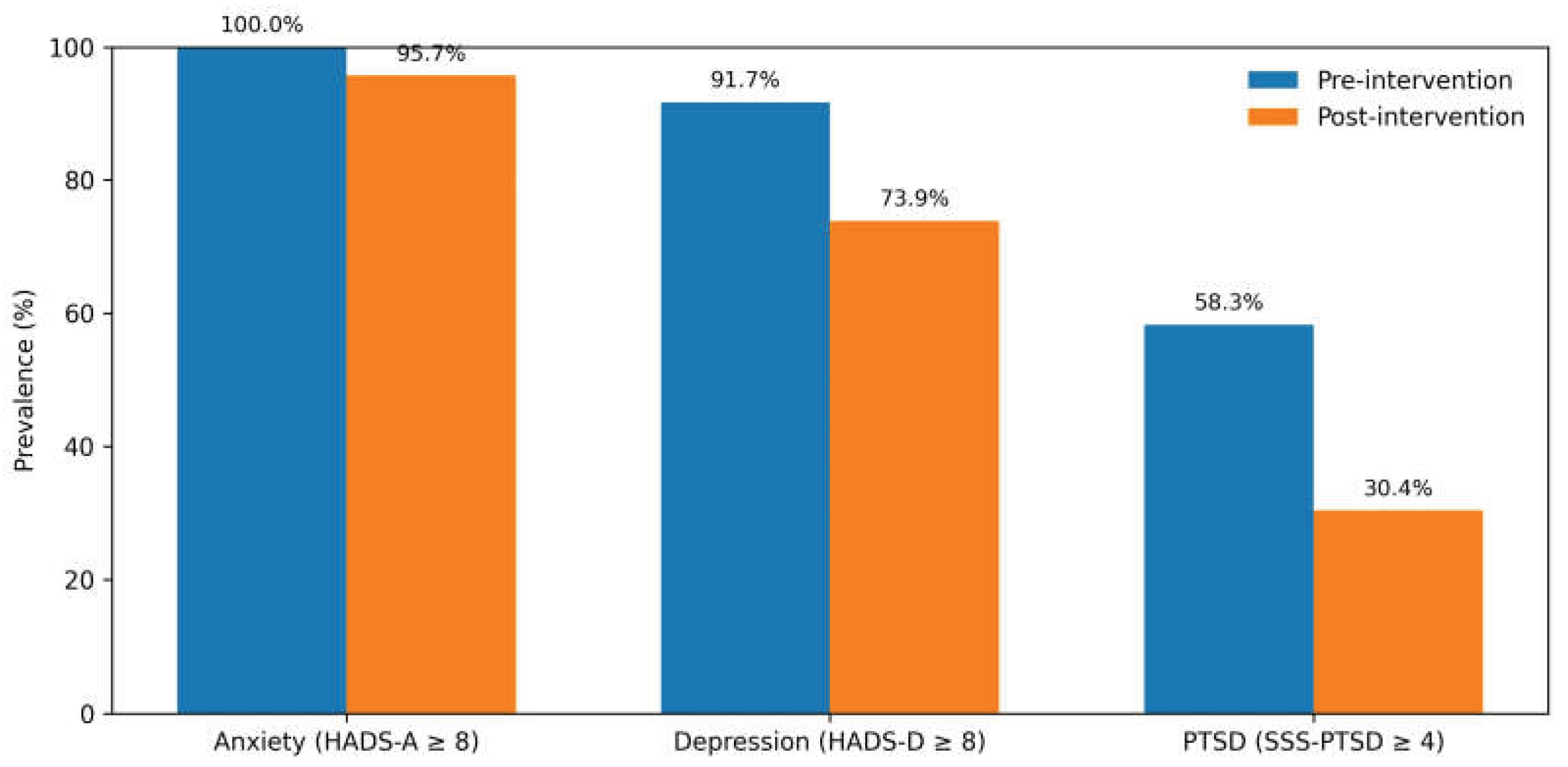

Table 1.
Psychological outcomes, comprehension, family satisfaction, and staff well-being before and after the intervention.
Table 1.
Psychological outcomes, comprehension, family satisfaction, and staff well-being before and after the intervention.
| Outcome | Pre-intervention (n = 12) | Post-intervention (n = 23) | p-value |
|---|---|---|---|
| Psychological outcomes | |||
| HADS-A1 ≥ 8, n (%) | 12 (100) | 22 (95.7) | 1.00 |
| HADS-A1 score, median (IQR2) | 15 (13–17) | 14 (9–15) | 0.097 |
| HADS-D3 ≥ 8, n (%) | 11 (91.7) | 17 (73.9) | 0.38 |
| HADS-D3 score, median (IQR2) | 13 (10–18) | 9 (7–12) | 0.021 |
| SSS-PTSD 4 ≥ 4, n (%) | 7 (58.3) | 7 (30.4) | 0.116 |
|
Comprehension and satisfaction |
|||
| Perceived comprehension (VAS 5 0–10) | 7.9 ± 1.1 | 8.6 ± 0.9 | 0.037 |
| Objective comprehension— organ failures (%) |
89.4 ± 5.1 | 89.1 ± 4.0 | 0.87 |
| Objective comprehension—treatments (%) | 77.1 ± 6.2 | 76.6 ± 5.4 | 0.79 |
| FS-ICU-246 overall score | 66 ± 15 | 75 ± 12 | 0.041 |
| Staff well-being | |||
| High depersonalization, n (%) | 35 | 10 | 0.048 |
| Emotional exhaustion score | no significant change | no significant change | 7 n.s. |
| Personal accomplishment score | no significant change | no significant change | 7 n.s. |
| Jefferson Scale of Physician Empathy | stable | stable | 7 n.s. |
1 HADS-A, Hospital Anxiety and Depression Scale—Anxiety; 2 IQR, interquartile range; 3 HADS-D, Hospital Anxiety and Depression Scale—Depression; 4 SSS-PTSD, Short Screening Scale for Post-Traumatic Stress Disorder; 5 VAS, visual analogue scale; 6 FS-ICU-24, Family Satisfaction in the Intensive Care Unit questionnaire; 7 n.s., not significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



