Submitted:
16 January 2026
Posted:
19 January 2026
You are already at the latest version
Abstract
Background: Low back pain (LBP) is a leading global cause of disability with major personal and socioeconomic impact. Limitations of purely biomedical treatment have encouraged a shift toward holistic, biopsychosocial, and evidence-based management. This systematic review examined the effects of holistic, non-surgical interventions on pain, disability, muscle strength, walking balance, and quality of life in adults with LBP. Methods: A comprehensive search of PubMed, MEDLINE, CINAHL, EMBASE, Cochrane Library, Google Scholar, and HMIC was conducted. Randomized controlled trials (RCTs) involving adults (≥18 years) receiving holistic interventions including structured exercise, patient education, psychologically informed therapy, manual therapy adjuncts, or multidisciplinary rehabilitation were included. Two reviewers independently screened studies, extracted data, and assessed quality using the PEDro scale. Of 5,326 identified records, 43 RCTs met eligibility criteria. Data were synthesized narratively and through meta-analysis following PRISMA guidelines. Results: Forty-three moderate- and high-quality RCTs involving 4,144 participants were included. Holistic interventions consistently reduced pain intensity and functional disability, with meaningful improvements across intervention types. Exercise-based therapies enhanced muscle strength, endurance, and movement function, while balance outcomes improved but varied across studies. Mind–body and psychologically informed interventions (e.g., CBT, mindfulness, yoga) showed strong positive effects on psychosocial outcomes and quality of life. Multimodal programs combining exercise, education, and psychological components produced the most comprehensive and sustained improvements, outperforming single-modality interventions. Thirty-eight RCTs (n = 1,701) contributed to the meta-analysis. Exercise-based interventions significantly reduced pain (MD = –2.45; 95% CI: –3.28 to –1.62). Technology-assisted interventions were also effective (MD = –2.24; 95% CI: –2.52 to –1.97). Manual and complementary therapies produced the largest effect (MD = –2.53; 95% CI: –4.23 to –0.82). Mind–body and psychological interventions showed no statistically significant pooled effect (MD = –0.44; 95% CI: –1.56 to 0.69). Conclusion: Holistic, evidence-based, non-surgical interventions are safe and effective for improving pain, function, and quality of life in adults with LBP. Findings reinforce current international guidelines advocating biopsychosocial, patient-centred care. Clinical practice should emphasize individualized, supervised exercise integrated with psychological strategies and education. Protocol Registration: The review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420251166635.
Keywords:
low back pain
; holistic management
; biopsychosocial model
; exercise therapy
; psychological interventions
; quality of life
Introduction
Low back pain (LBP) is a major global public health concern and remains one of the leading causes of disability across all age groups [1]. The Global Burden of Disease 2020 report indicates that more than 600 million people are affected worldwide, with non-specific LBP accounting for the vast majority of cases [2]. Despite its high prevalence, traditional biomedical approaches such as routine imaging, passive modalities, and pharmacotherapy have shown limited long-term effectiveness and may reinforce fear, disability, and unnecessary healthcare utilization [3,4].
Consequently, international guidelines have shifted toward a holistic, biopsychosocial model of care that recognises pain as the result of dynamic interactions among biological, psychological, and social factors [4]. This model highlights the influence of patient beliefs, coping styles, emotional distress, lifestyle behaviours, and environmental stressors on symptom persistence [5]. The World Health Organization’s 2023 guideline on non-surgical management of chronic primary LBP recommends integrated, patient-centred strategies including structured exercise therapy, education, psychological interventions, and multidisciplinary rehabilitation as first-line options [6].
Exercise-based interventions remain central due to their demonstrated benefits on pain relief, functional restoration, muscle strength, balance, and overall quality of life [7]. Psychologically informed therapies, such as cognitive behavioural therapy and mindfulness, address maladaptive cognitions and fear-avoidance, further enhancing recovery [8,9]. Multidisciplinary biopsychosocial rehabilitation programmes combining physical, psychological, and work-related components have shown additional advantage over unimodal treatments, particularly for chronic and persistent LBP [10].
However, important gaps remain [11]. The comparative effectiveness of different holistic modalities, optimal intervention dosage, and long-term sustainability of outcomes are not fully understood [12]. Variation in study designs, treatment intensity, and outcome reporting further complicate synthesis of the available evidence [13]. Additionally, access to integrated care remains uneven, especially in low- and middle-income settings where biomedical practices dominate [14].
Given these gaps, up-to-date systematic review synthesizing evidence on holistic, non-surgical interventions for LBP is warranted [15]. This review evaluates the effects of evidence-based approaches including exercise therapy, education, psychological interventions, manual therapy adjuncts, and multidisciplinary rehabilitation among adults with LBP, with the aim of informing clinical practice and guiding future research.
Methods
Research Design
This systematic review examined randomized controlled trials on the effectiveness of holistic, non-surgical management strategies for low back pain (LBP) in adult populations. The study was registered on October 12, 2025, on the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420251166635..
Eligibility Criteria
When selecting studies for this review, the following eligibility criteria were considered:
A. Inclusion Criteria:
- Types of Studies: This study reviews RCTs assessing the impact of holistic, non-surgical management strategies on outcomes related to low back pain. Holistic strategies include, but are not limited to, exercise therapy, patient education, psychological therapies (such as cognitive behavioural therapy or mindfulness), manual therapy as adjuncts, and multidisciplinary rehabilitation programmes. The studies included were published in English-language conference proceedings and peer-reviewed journals. Grey literature identified via hand searches and reputable trial registries were also considered.
- Types of Participants: This review included studies involving adult participants aged ≥ 18 years diagnosed with acute, subacute, or chronic low back pain, irrespective of gender or ethnicity. Both specific and non-specific LBP populations were eligible provided the intervention aligned with holistic, non-surgical management strategies and the study setting was clearly described.
- Intervention: We selected RCTs focusing on holistic, non-surgical interventions for LBP, either unimodal (e.g., structured exercise, psychological therapy, or education) or multimodal (e.g., exercise combined with education and/or psychological therapy). Only supervised or structured programmes were included. These programmes had no limitations regarding intervention dosage, form, frequency, duration, intensity, or post-intervention follow-up time.
- Types of Control: Our study involved randomized trials comparing holistic interventions against one or more of the following control categories:
- Usual care / Waitlist (No-Contact Control Group): Participants received standard care or were placed on a waitlist with no additional structured intervention.
- Different Interventions (Active Control Group): Participants received alternative interventions such as pharmacological management, sham procedures, education only, advice leaflets, or self-directed exercise programmes.
- Social Support (Social Control Group): Participants received non-specific social or support-based contacts without the structured therapeutic components.
- Timing: Only studies that completed outcome assessments at the end of the intervention or during follow-up periods of up to six months post-intervention were included.
- Types of Outcomes: Studies were included if they measured changes in outcomes relevant to low back pain management. The primary outcome was pain intensity. All studies focusing on these patient-centered and functional outcomes were included, analysed, and combined where appropriate. Clinical outcomes were evaluated and ranked, preserving the initial descriptions in the source texts.
- Primary Outcomes: Pain intensity: The primary outcome is pain intensity, usually measured using validated tools such as the Visual Analogue Scale (VAS) or the Numeric Rating Scale (NRS). Pain assessments capture the severity and change in back pain symptoms over time and across interventions.
B. Exclusion Criteria:
- Studies without supervised or structured holistic/non-surgical intervention components.
- Studies that implemented interventions unrelated to holistic or non-surgical care of low back pain (e.g., surgical procedures, pharmacological-only trials).
- Studies that failed to assess the main outcomes of interest such as pain intensity, functional ability, balance, muscle strength, or quality of life.
- Publications comprising opinion pieces, narrative reviews, systematic reviews, case reports, or correspondence without a clear methodology or primary data description.
- In instances of multiple publications from the same research project, the most recent or most complete publication on the subject was included.
Information Sources
This review employed a comprehensive search strategy, which included:
a) Hand Searches of Grey Literature: Relevant information was meticulously sourced beyond conventional academic databases to ensure thorough coverage of the available evidence.
b) Screening of Bibliographic Databases: Major bibliographic databases were systematically searched to identify eligible studies. These included PubMed, MEDLINE, Google Scholar, CINAHL, EMBASE, the Cochrane Library, and the Health Management Information Consortium (HMIC). Additional searches were conducted across open-access repository directories.
c) Following the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions and the Centre for Reviews and Dissemination, the reference lists of relevant included studies were examined using the snowballing method to expand the search network and identify additional eligible studies [16,17].
Search Strategy
A structured study plan was developed using Medical Subject Headings (MeSH) and keywords extracted from study titles, abstracts, and full texts. Combinations of search terms were generated to represent the population, interventions, comparators, and major outcomes of interest. A pilot test was conducted to evaluate the sensitivity and specificity of the search instructions.
Search commands included the use of Boolean operators and truncators. For PubMed, a detailed search strategy (Appendix I and II) was adapted and later modified to suit the syntax of the other databases. Searches were conducted from inception until the most recent update.
Additional sources such as published systematic reviews on low back pain management, relevant books and articles, the Cochrane Systematic Review Database, the National Institute of Health Research (NIHR) portfolio of ongoing or recently completed trials, and the Current Controlled Trials Register were also consulted to identify relevant clinical trials.
Study Record and Data Management
a) Search Results and Deduplication: All search results were exported into the RefWorks™ manager, where duplicate records were meticulously removed. The cleaned bibliographic entries were subsequently transferred into Microsoft Excel to facilitate organization and classification according to the review’s inclusion and exclusion criteria. Review questions were clearly structured and refined where necessary to ensure accurate article sorting.
b) Selection Process: Screening was conducted by two reviewers. E.F. (Reviewer 1) performed the initial screening based on titles and abstracts, while O.A. (Reviewer 2) independently cross-checked these results. Both reviewers then assessed the full texts of potentially eligible studies using the predefined criteria. Any disagreements regarding the inclusion or exclusion of studies were resolved through discussions and reflections. When necessary, V.W. (Reviewer 3) was consulted for a final decision. In cases where essential information could not be determined from the available text, study authors were contacted up to three times for clarification. Studies without adequate clarification after the maximum email attempts were excluded, with reasons documented.
The complete study flow including application of eligibility criteria and reasons for exclusion is presented in a PRISMA flow diagram (Figure 1).
Data Collection Processes
Risks of Bias Assessment in Individual Studies
The Physiotherapy Evidence Database (PEDro) 11-item scale was employed to rigorously evaluate the methodological quality of the selected studies [18]. The first item pertained to external validity, while the remaining 10 items assessed the internal validity of individual clinical trials [19]. Notably, the study’s overall quality improved with higher scores on this scale, which were interpreted as follows: 9–10: Excellent; 6–8: Good; 4–5: Fair; <4: Poor [19].
Additionally, the quality of RCTs was assessed by assigning a score of “1” for each “yes” response and “0” for “no,” “unclear,” or “not applicable” (N/A) responses. Summarizing these scores using a critical appraisal tool allowed for the determination of the total number of “yes” responses out of 10. The evaluation process was conducted independently by Reviewer 1 and Reviewer 2. Differences in judg ment were resolved through discussion and reflection, with Reviewer 3 consistent with Cochrane recommendations [17]. Furthermore, each study’s level of evidence was assessed based on both the sample size and the PEDro score. High-quality randomized controlled trials (rated as good or excellent by PEDro and sample size greater than 50) were considered Level 1 evidence, whereas lower-quality RCTs (rated as fair or poor by PEDro, or sample size < 50) were considered Level 2 evidence [20].
Data Collection Processes
i. Data Item:
Data from the included studies were meticulously extracted using a standardized data extraction
form, in line with the Cochrane Handbook for Systematic Reviews of Interventions [17]. The form encompassed various essential elements, including: authors’ reference, participants’ characteristics, inclusion and exclusion criteria, study sample details, intervention components (e.g. exercise therapy, education, psychological interventions, manual therapy, or multidisciplinary care), intervention setting, intervention delivery personnel, duration of the intervention and follow-up (if available), attrition rate, outcome assessment/measurement methods, results, conclusions, and funding sources. The extraction form also incorporated a section for methodological rigour and potential sources of bias [16].
ii. Data Synthesis and Assessment of Heterogeneity In this review, the impact of holistic, non-surgical management approaches including physical exercise, education, psychological interventions, and multidisciplinary rehabilitation on pain reduction among adults with low back pain was investigated. To evaluate the interventions’ efficacy, a proof table was constructed and quantitative results were analyzed. The following steps were taken:
Statistical Methodology
This review adhered to standard Cochrane meta-analysis procedures [17]. Risk ratios (RRs) with 95% confidence intervals were calculated for dichotomous outcomes. Weighted mean differences (WMDs) were computed for continuous outcomes measured on comparable scales [17]. Statistical significance was set at p < 0.05, consistent with conventional meta-analytic standards [17]. A random-effects model was employed to account for expected clinical and methodological heterogeneity, heterogeneity was assessed using Cochran’s χ² test and the Higgins I² statistic, with thresholds defined as low (25%), moderate (50%), and high (75%) heterogeneity [17].
Data Analysis
The analysis of studies involved a comprehensive examination of various factors, including: year of publication, author references, sample size, age distribution, study settings, data collection format, outcome measures, intervention and control components, format of intervention delivery, and intervention and follow-up durations [17].
i. Narrative synthesis:
Narrative synthesis was employed to explore relationships and draw conclusions from diverse studies, following the Centre for Reviews and Dissemination’s narrative synthesis guidelines. By focusing on the primary outcomes (pain intensity), we conducted an investigation and presented
our findings within and between studies [17].
ii. Meta-analyses:
Meta-analyses were performed using a random-effects model to determine pooled effect sizes across the trials according to the Cochrane Handbook for Systematic Reviews of Interventions guidelines [17]. Heterogeneity values were categorized as follows: low: 25 %; medium: > 25 %–75 %; and high: > 75 %. The heterogeneity was assessed using the Higgins I² test and Cochrane’s χ² test (with a 10 % significance threshold). Where substantial heterogeneity was present and pooling was not appropriate, findings were presented in a structured narrative format [16]
Rating Quality of Evidence and Strength of Recommendation
The systematic review’s recommendation strength underwent rigorous assessment using the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach. This approach considered study design, consistency of results, precision, publication bias, directness, and study limitations. Evidence for each key outcome was graded as high quality (low risk of bias), moderate quality, or low quality (high risk of bias).
Evidence Statement and Quality Assessment
Each evidence statement was meticulously rated based on its quality:
- High Quality: Implies that additional research is unlikely to alter the effect estimates.
- Moderate Quality: Suggests that further research could significantly impact the effect estimates.
- Low Quality: Indicates that additional research is very likely to alter or significantly change the estimate.
These assessments were informed by the overall pattern of results, the PEDro ratings, sample sizes, and GRADE judgments.
Level of evidence Study level of evidence was determined by both the sample size and the PEDro score:
- Level 1 Evidence: High-quality randomized controlled trials (RCTs) with larger samples (PEDro rated good or excellent and sample size > 50).
- Level 2 Evidence: Lower-quality RCTs with fair or poor ratings and/or a sample size less than 50
Report of Review
Results
Study Selection
Two independent reviewers conducted two systematic searches across seven electronic databases using predefined search strategies based on the main outcomes of interest. The databases searched were PubMed, MEDLINE, Google Scholar, CINAHL, EMBASE, the Cochrane Library, and the Health Management Information Consortium (HMIC). Reference lists of relevant articles were also hand-searched.
The searches identified 5,326 records. After removal of 442 duplicates, 4,818 records remained for title and abstract screening. Of these, 66 publications met the eligibility criteria and were assessed at full text, while 4,197 records were excluded. Following full-text review, 43 studies met the inclusion criteria and were included in the qualitative synthesis [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64]. The study selection process is presented in the PRISMA flow diagram (Figure 1).
Qualitative and Quantitative Synthesis
All 43 included studies were incorporated into the qualitative synthesis. For the quantitative synthesis (meta-analysis), five studies were excluded because their outcomes were not comparable with the primary pain-related outcomes or because standard deviations were not reported [30,32,39,40,44]. Consequently, 38 studies were included in the final meta-analysis. All meta-analysed studies reported comparable pain-related outcomes, most commonly using the Visual Analogue Scale (VAS).
Risk of Bias in Included Studies
Table 2 summarizes the risk of bias assessment using the PEDro scale. The most common sources of bias were performance bias, arising from lack of participant and therapist blinding, and selection bias related to inadequate reporting of concealed allocation. Attrition bias was also observed in studies that did not fully apply intention-to-treat (ITT) analysis.
Despite these limitations, most studies demonstrated random allocation, baseline comparability, and adequate outcome reporting. Based on PEDro scores, the majority of studies (scores 6–10) were classified as high quality. Nine studies were rated as moderate quality due to limitations in blinding and incomplete ITT reporting [30,32,36,37,45,46,53,56,60]. Back et al. [27] achieved the highest methodological quality with a PEDro score of 10.
Selection Bias and Eligibility Criteria
All included studies clearly reported inclusion and exclusion criteria, resulting in a low risk of bias related to participant eligibility. Randomization procedures were described in all studies. Concealed allocation was adequately reported in 16 of the 43 studies, while the remaining studies provided insufficient information, indicating a moderate risk of selection bias. Baseline characteristics were comparable between intervention and control groups in nearly all studies.
Performance and Detection Bias
Participant blinding was reported in 5 [27,28,40,52,55] of the 43 studies (11.4%), while therapist blinding was reported in only one study [27]. Consequently, the risk of performance bias was high across most studies. Assessor blinding was reported in 30 studies [22,23,24,25,26,27,28,29,31,33,34,35,38,39,40,41,43,47,49,50,52,54,55,57,58,59,61,62,63,64], whereas nine studies lacked assessor blinding, indicating an increased risk of detection bias.
Attrition Bias and Outcome Reporting
Twenty-two studies (50%) reported conducting ITT analysis or achieved full participant retention, while the remaining studies did not, suggesting a moderate risk of attrition bias. Most studies (36) retained at least 85% of participants; however, eight studies failed to meet this threshold. Adequate between-group comparisons and reporting of point estimates with measures of variability were provided in 41 studies, indicating a low risk of reporting bias.
Outcomes Reported in Included Studies
The included studies assessed a wide range of outcomes reflecting the multidimensional nature of chronic low back pain (CLBP). Primary outcomes aligned with the review objectives and included pain intensity, functional disability, quality of life, physical performance, and psychosocial outcomes. Secondary outcomes included muscle morphology and activation, balance, sleep, cognition, and work participation.
Pain Intensity
Pain intensity was the most frequently assessed outcome and was measured using the Visual Analogue Scale (VAS), Numerical Rating Scale (NRS), McGill Pain Questionnaire, and pressure pain threshold. Most interventions demonstrated significant reductions in pain intensity, including stabilization training [26], Pilates [38], functional resistance training [35], virtual reality [23], graded sensorimotor retraining [28], cognitive functional therapy [40], and mindfulness-based interventions [33]. Improvements in pressure pain threshold were reported in studies employing algometry [27].
Muscle Function
Nine studies evaluated muscle morphology and activation using surface electromyography, ultrasound imaging, or shear wave elastography. Muscle endurance outcomes, including the Sørensen test and trunk-hold tests, were reported in studies assessing resistance training, kinesiotaping, inspiratory muscle training, and aquarobics [35,53,54,63].
Balance, Mobility, and Physical Performance
Five studies [41,42,49,63,64] examined balance and functional mobility using instruments such as the Timed Up and Go test, 6-Minute Walk Test, Back Performance Scale, and Biodex Balance System. Improvements in both static and dynamic balance, as well as overall physical performance, were commonly reported across interventions.
Functional Disability
Functional disability was a core outcome measured primarily using the Oswestry Disability Index (ODI) and the Roland–Morris Disability Questionnaire (RMDQ). Pilates-based interventions, acupuncture, cognitive functional therapy, and exercise-based programs consistently produced clinically meaningful reductions in disability [34,35,37,38,40,43]. Additional functional outcomes were assessed using the Patient-Specific Functional Scale [22].
Work Participation and Broader Life Impact
Refs. [29,45,46,52,53,54,56,59] evaluated outcomes related to work participation and broader life impact. Reductions in work-related fear-avoidance were reported following simulated horseback riding [56]). Pain interference decreased following mindfulness, cognitive therapy, and behavioral activation interventions [39]. Improvements in sleep quality, fatigue, and cognitive function were observed in studies assessing aquarobics and behavioral activation programs [39,60].
Effects of Interventions
Intervention effects were reported as comparisons between intervention and control groups. Based on biopsychosocial principles, interventions were categorized into five domains.
Physically Oriented Exercise Therapies
Nine studies investigated stabilization training, Pilates, resistance training, inspiratory muscle training, aquarobics, and exercise combined with education. All exercise-based interventions resulted in reductions in pain intensity, with high-frequency stabilization training demonstrating the strongest analgesic effects [26]. Equipment-based Pilates produced more consistent pain reduction than mat-based Pilates [36,37]. Resistance training and inspiratory muscle training also yielded significant improvements.
Exercise-based interventions improved functional disability and physical performance outcomes, including mobility, muscle strength, endurance, balance, and vitality. Programs integrating exercise with education demonstrated superior outcomes compared with exercise alone. Aquarobics additionally improved sleep quality, fatigue, and subjective memory.
Mind–Body and Psychological Therapies
Eight studies [24,28,33,39,40,45,47,58] evaluated cognitive behavioral therapy (CBT), mindfulness, acceptance-based therapies, graded sensorimotor retraining, Feldenkrais, yoga, and exposure therapy. These interventions produced significant reductions in pain intensity and improvements in functional and psychosocial outcomes. Cognitive functional therapy, sensorimotor retraining, mindfulness, Feldenkrais-based therapy, and yoga demonstrated robust analgesic effects. Improvements were also observed in coping strategies, emotional regulation, psychological flexibility, and acceptance. Telehealth-delivered interventions reduced pain interference and functional limitations.
Manual and Body-Based Therapies
Three studies [34,53,54] assessed acupuncture, spinal manipulative therapy (SMT), kinesiotaping, and dry needling. Manual acupuncture produced greater reductions in pain and disability compared with electroacupuncture. SMT combined with dry needling or kinesiotaping resulted in larger improvements than SMT alone. Manual acupuncture also demonstrated greater reductions in kinesiophobia, indicating both physical and psychological benefits.
Technology-Assisted and Adjunctive Modalities
Six studies [23,39,42,49,60,64] evaluated virtual reality, telehealth rehabilitation, EMG biofeedback, and vibration-based exercise. Virtual reality interventions consistently reduced pain and disability and improved balance and fall risk. Telehealth rehabilitation demonstrated favorable effects on pain interference and functional limitations. EMG biofeedback improved muscle activation and motor control, while vibration-based exercise enhanced balance. Aquarobics, considered within this category, also improved sleep, cognition, and vitality.
Integrated and Multimodal Interventions
Five studies [28,40,45,46,48] evaluated integrated interventions combining physical, psychological, and behavioral components. These multimodal approaches produced greater and more sustained improvements in pain and disability compared with single-modality interventions. Comprehensive biopsychosocial rehabilitation programs demonstrated broad benefits across physical, functional, and psychosocial domains.
Level of Evidence
Level I Evidence (High quality, PEDro 6–10): Twenty-Four [Aasa et al., 2015 [22]; Afzal et al., 2022 [23]; Ahmadi et al., 2020 [24]; Akbaş et al., 2025 [26]; Back et al., 2024 [27]; Bagg et al., 2022 [28]; Blanco-Giménez et al., 2024 [31]; Chen et al., 2023 [33]; Comachio et al., 2020 [34]; Cruz-Díaz et al., 2018 [38]; Day et al., 2024 [39]; de Lira et al., 2025 [40]; Elabd & Elabd, 2024 [41]; Feng et al., 2025 [42]; Ford et al., 2016 [43]; Freiwald et al., 2018 [44]; Godfrey et al., 2020 [47]; Grande-Alonso et al., 2019 [48]; Halliday et al., 2019 [50]; Khan et al., 2024 [54]; Kim & Park, 2021 [55]; Kong et al., 2020 [57]; Lang et al., 2021 [59]; Li, Y., et al., 2025 [61] ] demonstrated strong methodological rigor with Good to Excellent quality randomization, baseline comparability, and statistical reporting. These studies provide the most reliable evidence.
Level II Evidence (Moderate to Low quality, PEDro ≤5): Nineteen studies [Ahmadnezhad et al., 2020 [25]; Bagheri et al., 2020 [29]; Bello et al., 2015 [30]; Brandt et al., 2015 [32]; Cortell-Tormo et al., 2018 [35]; Cruz-Díaz et al., 2017 [36]; Cruz-Díaz et al., 2016 [37]; Ghavipanje et al., 2022 [45]; Glombiewski et al., 2018 [46]; Gwon et al., 2020 [49]; Hernandez-Lucas et al., 2023 [51]; Hohmann et al., 2018 [52]; Kamali et al., 2018 [53]; Kim et al., 2020 [56]; Kuvačić et al., 2018 [58]; Lee & Kim, 2025 [60]; Luo, Y., et al., 2019 [62]; Song & Yim, 2025 [63]; Yalfani et al., 2022 [64]] showed fair to low methodological quality, often with limitations in allocation concealment, blinding, or intention-to-treat analysis. These studies provide supportive, but less robust evidence.
Grade of Evidence for the Review
The review included 43 trials with PEDro scores ranging from 5 to 10 and a mean score of 6.70/10. Twenty-four studies (55.8%) were classified as Level I evidence, while nineteen studies (44.2%) were Level II evidence. In terms of quality ratings based on the PEDro scale, five studies were graded as excellent, twenty-nine as good, and nine as fair. The overall methodological quality for the review is 6.70 out of 10, which corresponds to a moderate to good quality level for evaluating the effects of various physical, psychological, and multimodal interventions on pain, disability, and quality of life in individuals with chronic low back pain (Table 1).
Meta-Analyses – Effects of Holistic Interventions
Exercise-Based Interventions
There was a statistically significant overall improvement following exercise-based interventions when compared with control groups. The pooled mean difference showed a significant benefit (MD = –2.45; 95% CI: –3.28 to –1.62). This indicates that exercise interventions including strengthening exercises, motor control training, Pilates, and functional resistance training were effective in reducing symptoms and improving outcomes. However, this analysis was associated with very high heterogeneity (I² = 96%), suggesting substantial variability in the effect sizes across included studies. The inconsistency across studies may be attributed to differences in exercise type, intensity, duration, and participant characteristics. (Figure 2)
Mind–Body and Psychology Interventions
The meta-analysis of psychologically informed interventions such as cognitive behavioural therapy, mindfulness-based interventions, pain neuroscience education, and other mind–body approaches showed a pooled effect that favoured the intervention group, although the result did not reach statistical significance (MD = –0.44; 95% CI: –1.15 to 0.66). The confidence interval crossing zero suggests uncertainty in the overall effectiveness of these interventions on the measured outcomes. A high level of heterogeneity was also observed (I² = 84%), reflecting variability in intervention content, duration, delivery style, and outcome measures used across studies. (Figure 2)
Technology-Assisted Interventions
A strong and statistically significant effect was found for technology-assisted interventions (MD = –2.24; 95% CI: –2.52 to –1.97). This subgroup included virtual reality training and technology-supported movement or balance-training tools, all of which were standardized and consistently applied across studies. Notably, this subgroup demonstrated no heterogeneity (I² = 0%, p = 0.45), suggesting that the effect of technology-assisted interventions was highly consistent across all included trials. This reinforces the reliability of the pooled estimate. ( Figure 2)
Manual and Complementary Therapy
Manual and complementary therapy interventions, which included acupuncture, spinal manipulation, mobilization, and soft-tissue interventions, produced the largest pooled effect size among all subgroups (MD = –2.53; 95% CI: –4.23 to –0.82). This statistically significant result suggests that hands-on interventions delivered by trained therapists were highly effective in improving patient outcomes. However, this subgroup showed high heterogeneity (I² = 86%), suggesting variability in therapist skill level, treatment duration, and type of manual technique applied across studies. (Figure 2)
Multimodal Interventions
The meta-analysis of multimodal interventions, where exercise was combined with education, psychological therapy or other rehabilitation components, produced a pooled effect size favouring the intervention group (MD = –1.39), although the confidence interval crossed zero (95% CI: –4.58 to 0.61), indicating that the overall effect was not statistically significant. This subgroup showed high heterogeneity (I² = 90%), which reflects the complexity and variability of multimodal programme designs across settings and studies. (Figure 2)
Subgroup with the Highest Effect
Among all the subgroups analysed, the manual and complementary therapy subgroup demonstrated the largest treatment effect (MD = –2.53), followed closely by the exercise-based interventions (MD = –2.45) and technology-assisted interventions (MD = –2.24). The mind–body/psychology interventions and multimodal interventions demonstrated smaller pooled effects, with the mind–body subgroup (MD = –0.44) showing the least improvement. ( Figure 2)
Discussion
This systematic review synthesized evidence from forty-three randomized controlled trials (RCTs) to evaluate the effects of holistic, non-surgical interventions on a comprehensive range of outcomes including pain intensity, functional disability, muscle strength, walking balance, and quality of life among adults with chronic low back pain (CLBP). The methodological quality of the included studies was predominantly high, as assessed by the PEDro scale, with a low risk of bias in key domains such as eligibility criteria, random allocation, and baseline similarity. While some heterogeneity existed, particularly concerning the blinding of participants and therapists, an inherent challenge in physical intervention trials the overall body of evidence is robust. This review's distinct strength lies in its comprehensive scope, which moves beyond a narrow focus on a single modality to encompass the full spectrum of holistic care. It integrates findings from physical exercise, psychological therapies, manual techniques, technology-assisted modalities, and complex multimodal programs, thereby providing a nuanced and clinically relevant perspective on contemporary, evidence-based CLBP management that aligns with the prevailing biopsychosocial paradigm.
The Efficacy of Holistic Interventions on Primary Outcomes
Pain Intensity: A cornerstone finding of this review is the consistent and significant reduction in pain intensity across virtually all intervention types. Physically-oriented exercises, such as specific stabilization training [26], Pilates [36,38] and functional resistance training [35], demonstrated robust analgesic effects. For instance, Akbaş et al. [26] found that high-frequency (4x/week) stabilization exercises led to significantly greater improvements in pain and core muscle stiffness compared to a lower-frequency (2x/week) program or a home exercise control. Crucially, interventions that combined physical activity with educational or psychological components consistently yielded superior and more sustainable pain relief compared to unimodal approaches. For example, Ford et al. [43] demonstrated that individualized physiotherapy combined with guideline-based advice resulted in significantly greater improvements in pain and disability at 26 and 52 weeks compared to advice alone. Similarly, Bagheri et al. [29] showed that adding Cognitive Behavioral Therapy (CBT) to stabilization exercises led to greater reductions in fear-avoidance beliefs and disability, which are key drivers of chronic pain. This synergy powerfully supports the central tenet of the biopsychosocial model that addressing the multifaceted nature of pain through integrated care leads to better outcomes than focusing solely on its putative physical components [66,67].
Functional Disability: As a cornerstone outcome in LBP research, functional disability was substantially improved by holistic interventions. Programs focusing on core stabilization, motor control, and functional strength directly enhanced trunk stability and movement efficiency. Cortell-Tormo et al. [35] reported a remarkable 61.3% reduction in disability on the Oswestry Disability Index following a 12-week functional resistance training program. The integration of self-management principles and education was repeatedly identified as a pivotal factor. This educational component empowers patients, shifts beliefs about pain, and fosters long-term adherence, thereby directly mitigating the recurrent and persistent nature of LBP [43]. The success of Cognitive Functional Therapy [40], which explicitly targets unhelpful cognitions, emotions, and behaviors alongside movement retraining, further underscores that disability is not a simple function of tissue pathology but is profoundly mediated by the patient's perceptions and coping strategies.
Muscle Function and Physical Performance: Targeted exercises yielded significant benefits in reversing the neuromuscular deficits commonly associated with chronic LBP. Studies employing specific protocols, such as inspiratory muscle training [25], demonstrated enhanced activation of key stabilizers like the multifidus and transversus abdominis. Similarly, functional resistance training [35] and aquarobics [60] led to measurable improvements in trunk and lower limb endurance, as well as overall physical capacity. These improvements are critically important, as deficits in muscular endurance and motor control are strongly linked to the development and chronicity of LBP [68]. The findings suggest that reversing this deconditioning and restoring efficient muscle recruitment patterns is a key mechanism through which exercise alleviates pain and improves function.
Walking Balance and Postural Control: The effects on balance and postural control were positive but demonstrated greater variability than other outcomes. Technology-assisted interventions showed particular promise. For example, virtual reality training [64] significantly improved balance and reduced fall risk in elderly women with LBP, while vibration-augmented exercise [49] enhanced static balance outcomes. However, the results from more conventional exercise programs were mixed. This variability underscores that balance is a highly complex construct influenced not only by musculoskeletal factors but also by pain-related fear, altered proprioception, and central sensorimotor integration [69]. Therefore, improving balance in the LBP population may require highly specific, challenging, and targeted interventions that directly address these neurophysiological and psychological components, rather than general exercise alone.
Psychosocial Well-being and Quality of Life (QoL): A significant contribution of this review is the clear demonstration that holistic management extends its benefits deep into the psychosocial domain. Mind-body therapies were particularly potent. Mindfulness-Based Stress Reduction [33] and yoga [58] were effective in reducing depression and anxiety, while the Feldenkrais Method [24] uniquely enhanced interoceptive awareness, leading to improved body schema and QoL. Furthermore, psychologically-informed physiotherapy, such as Acceptance and Commitment Therapy (PACT) [47], significantly improved pain acceptance and functioning in the short term. Perhaps most compelling are the findings that extend beyond standard health-related QoL metrics. The study by Lee & Kim [60] found that a 12-week aquarobics program not only reduced pain and disability in older women but also significantly alleviated sleep disturbance and subjective memory complaints, with pain reduction mediating these effects. This highlights the far-reaching, cascading benefits of holistic care, improving overall life participation and well-being.
Alignment with Existing High-Quality Evidence and Guidelines
The overall findings of this review are not isolated; they are strongly reinforced by and congruent with recent high-quality evidence and international clinical guidelines. The 2023 World Health Organization (WHO) guideline for the non-surgical management of chronic primary LBP explicitly recommends patient education, exercise therapy, and psychological interventions as first-line treatments, while advising against the routine use of passive modalities [6]. Similarly, our results directly align with major Cochrane reviews which conclude that exercise is more effective than no treatment or usual care for chronic LBP [7] and that multidisciplinary biopsychosocial rehabilitation is superior to physical treatments alone for improving pain and function [10]. The consistency between this systematic review and these authoritative sources provides a powerful, multi-layered evidence base that should decisively inform clinical practice and health policy.
Comparative Effectiveness Across Intervention Types
While the preceding sections synthesized findings according to discrete outcomes, an equally important perspective is how different categories of holistic interventions compare in their overall effectiveness and clinical utility. The evidence reviewed in this study underscores that no single modality provides a universal solution for chronic low back pain (CLBP); rather, the strength of an intervention lies in how well it addresses the multifactorial biopsychosocial dimensions of the condition.
Physically-Oriented Exercise Therapies consistently produced large effects on pain reduction and disability, particularly stabilization training and Pilates-based programs [26,37,38]. These effects are attributable to improvements in neuromuscular control, trunk stability, and reversal of physical deconditioning. However, while exercise substantially improved physical outcomes, its effects on psychosocial well-being and broader quality of life were less consistent unless combined with education or behavioral strategies [43]. This highlights a limitation of purely physical interventions when used in isolation.
Mind–Body and Psychological Therapies showed comparatively stronger effects in domains of psychological distress, pain coping, and quality of life. Interventions such as CBT, mindfulness, and Acceptance and Commitment Therapy not only reduced pain but also reshaped maladaptive cognitions and enhanced pain acceptance [33,47]. Importantly, these approaches were particularly effective in reducing fear-avoidance behaviors, a critical determinant of chronicity. However, their impact on objective physical performance was more modest compared to exercise-based therapies, suggesting that psychological strategies are most effective when integrated with active movement retraining.
Manual and Body-Based Therapies provided short- to medium-term relief in pain and disability, with acupuncture and spinal manipulative therapy showing measurable benefits [34,54]. They also had unique advantages in reducing kinesiophobia, which may facilitate engagement in active therapies. Nonetheless, the sustainability of these effects beyond three months appeared limited, and the interventions were less effective in targeting broader psychosocial and lifestyle outcomes. This suggests that manual approaches may function best as adjuncts rather than stand-alone strategies.
Technology-Assisted and Adjunctive Modalities demonstrated promising benefits, particularly in balance, coordination, and engagement with therapy. Virtual reality and biofeedback interventions not only improved postural control but also enhanced patient motivation through immersive and interactive experiences [23,31]. Telehealth-based delivery was especially relevant in broadening accessibility and ensuring continuity of care [39,42]. However, the evidence base for these technologies is comparatively small, and long-term follow-up data remain limited, indicating the need for further trials to establish durability and cost-effectiveness.
Finally, Integrated and Multimodal Interventions those explicitly combining physical, psychological, and educational components emerged as the most comprehensive and sustainable approaches. Cognitive Functional Therapy [40] and biopsychosocial rehabilitation programs [29,48] consistently outperformed unimodal comparators in improving pain, disability, psychosocial well-being, and long-term adherence. Notably, these interventions reflect a contemporary shift toward a biopsychosocial paradigm of care, as they directly address the interaction between biological impairments, maladaptive cognitions, and behavioral patterns. The findings indicate a hierarchical pattern of effectiveness across intervention types. Exercise-based therapies emerge as fundamental for restoring physical function and reducing pain. Mind–body and psychological interventions play a critical role in modifying maladaptive beliefs, reducing fear-avoidance behaviors, and improving psychosocial well-being. Manual therapies appear to provide short-term symptom relief and help reduce kinesiophobia, thereby facilitating engagement in more active forms of care. Technology-assisted modalities contribute by enhancing accessibility, motivation, and balance training, particularly in settings where traditional delivery may be limited. Importantly, integrated multimodal programs demonstrate the most comprehensive and durable benefits by simultaneously addressing physical, psychological, and behavioral dimensions of chronic low back pain.
Collectively, these findings reinforce that chronic low back pain cannot be effectively managed by targeting a single domain of impairment. Optimal outcomes are achieved when interventions are integrated and tailored, combining physical reconditioning with psychological support, lifestyle modification, and, where appropriate, technological adjuncts.
The Recommended Holistic Prescriptions for Chronic Low Back Pain Include
Based on a synthesis of the effective interventions from the forty-three included studies, the following evidence-based prescriptions are recommended for the holistic management of chronic LBP. These prescriptions are stratified by intervention type, with specific dosage and parameters derived directly from the successful trials in this review.
(a) Motor Control and Stabilization-Focused Exercise: This should form the core of physical rehabilitation for many patients, particularly those with movement control impairments. The program should be supervised and performed 2-3 times per week for a minimum of 8-12 weeks.
Stabilization Exercises: As demonstrated by Akbaş et al. [26] a higher frequency of four supervised sessions per week was superior to two sessions per week for improving core muscle stiffness and disability. Dosage should involve 2-3 sets of 8-15 repetitions, focusing on deep trunk muscles like the transversus abdominis and multifidus.
Pilates Training: Both mat-based and equipment-based Pilates are effective, though equipment-based Pilates may lead to faster improvements in muscle activation and disability [37]. A 12-week program, with sessions 2-3 times per week, is recommended [38].
(b) Combined Strengthening and Functional Training: For patients with general deconditioning and functional limitations, a combined approach is highly effective.
Functional Resistance Training: A periodized program, such as that implemented by Cortell-Tormo et al. [35], conducted over 12 weeks with 2 sessions per week, focusing on functional movements with progressive loading. Dosage typically involves 2-3 sets of 8-12 repetitions.
Aerobic and Resistance Combination: While not always specified as a combined program, the success of multimodal approaches supports integrating aerobic conditioning (e.g., walking, aquarobics) at a dosage of 150-300 minutes per week at moderate intensity with resistance training.
(c) Mind-Body and Psychological Therapies: These are essential for addressing the psychosocial drivers of chronic pain.
Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT): Programs should consist of 8-12 weekly sessions, delivered individually or in groups. Bagheri et al. [28] showed that integrating CBT with stabilization exercises led to greater improvements in fear-avoidance and disability than exercise alone. Godfrey et al. [47] demonstrated that ACT-informed physiotherapy (PACT) was feasible and improved disability and physical health outcomes at 3 months.
Mindfulness-Based Stress Reduction (MBSR): As per Chen et al. [33], an 8-week standardized program that includes meditation and mindful movement is effective for improving function and pain.
Graded Sensorimotor Retraining: Programs like RESOLVE [28], which include 12 weekly sessions of movement retraining integrated with pain education, are specifically designed to reconceptualize pain threats and alter cortical body representations.
(d) Technology-Assisted and Adjunctive Modalities: These can enhance engagement, accessibility, and target specific deficits.
Virtual Reality (VR) Training: As used by Yalfani et al. [64] and Afzal et al. [23], a program of 2-3 sessions per week for 6-8 weeks can significantly improve balance, reduce fall risk, and decrease pain and disability.
Telemedicine-Supported Rehabilitation: Feng et al. [42] demonstrated that an 8-week telemedicine-supported exercise and education program delivered via mHealth apps resulted in greater improvements in disability and pain compared to usual care, offering a scalable model for improving access and adherence.
These findings are strongly supported by international guidelines. The World Health Organization [6] recommends exercise therapy, education, and psychological interventions as first-line treatments for chronic primary LBP. Similarly, the American College of Physicians [70] recommends non-pharmacological therapies, including exercise, multidisciplinary rehabilitation, and mindfulness, as the initial approach for chronic LBP.
Reasons for Non-Significant Effects Reported in Some of the Studies
Despite the overall positive findings, several studies reported non-significant results for specific outcomes. An analysis of these studies reveals important contextual and methodological reasons.
For pain and functional disability outcomes:
Insufficient Intervention Dosage or Duration: Bello et al. [30], which compared behavioural graded activity to conventional exercise, may not have found between-group differences due to a potential ceiling effect of both active interventions being compared against each other, or a dose that was insufficient to differentiate them. Kim et al. [56] reported that while simulated horseback riding and stabilization exercises both improved outcomes, differences between them were limited to fear-avoidance beliefs, suggesting the specific type of exercise may be less critical than the overall dose of active intervention.
Lack of Individualization: Ford et al. [43] implicitly highlighted the importance of individualization by demonstrating that individualised physiotherapy was more effective than standardized advice. It can be inferred that studies employing generic, non-individualized protocols may yield suboptimal or non-significant results for complex patients.
High Attrition and Methodological Limitations: Lang et al. [59] reported no significant group differences in their walking intervention, but noted high attrition (45% at 12 months), which greatly reduced statistical power and likely obscured true effects.
For walking balance and physical performance outcomes:
Outcome Measure Sensitivity and Complexity of Balance: The variable results in balance outcomes can be attributed to the complex nature of balance, which is influenced by pain-related fear, proprioception, and central integration. Studies using generic measures may fail to detect improvements that are specific to the training stimulus. For instance, a program focused on strength might not sufficiently challenge the sensorimotor system to produce detectable changes on a high-level balance test.
For Quality-of-Life Outcomes
Multidimensional Nature of QoL: Several studies demonstrated that significant functional improvements do not always translate directly into statistically significant QoL gains. This suggests that QoL is a multidimensional construct that may require more substantial or broader changes across physical, psychological, and social domains to show a significant shift on standardized questionnaires. This mirrors the finding in other fields that larger functional changes are sometimes needed to impact global QoL scores.
Why the Interventions Should Not Be Overgeneralized in the Population Group
Despite the compelling evidence for holistic management, these interventions must not be overgeneralized or applied uniformly to all individuals with CLBP. The variability in individual response is influenced by several key factors.
Clinical and Phenotypic Heterogeneity: The CLBP population is highly heterogeneous. A patient with dominant neuropathic pain and central sensitization will respond differently to treatment than a patient with primary movement control impairments or one with high levels of fear-avoidance. The success of Cognitive Functional Therapy [40] hinges on its ability to identify and target an individual's specific "clinical puzzle" of factors.
Individual Responsiveness and Comorbidities: Factors such as age, baseline fitness, the presence of other comorbidities (e.g., obesity, osteoarthritis), psychological profile (e.g., catastrophizing, self-efficacy), and personal goals and beliefs significantly influence treatment adherence and outcomes. The success of an intervention is as much about the patient's engagement and readiness for change as it is about the intervention itself.
Intervention Fidelity and Provider Skill: The effectiveness of complex interventions like mindfulness [33] or Cognitive Functional Therapy is highly dependent on the skill, training, and fidelity of the provider. The benefits observed in tightly controlled trials may not be fully replicated in general practice where such specialized training is variable.
The Intervention Adverse Effects
The safety profile of the holistic, non-surgical interventions reviewed was exceptionally favourable, especially when contrasted with the risks of pharmacological or surgical alternatives.
The vast majority of included studies either did not report any adverse events or explicitly stated that none occurred as a direct result of the intervention. Where minor adverse events were reported, they were transient and musculoskeletal in nature. For example, Allet et al. [71] cautiously noted that two participants in their gait and balance intervention group reported Achilles tendon pain, which was manageable with modified exercise progression. This reinforces that such events are typically related to the initial exposure to new physical activities and can be mitigated with proper warm-up and progression. The absence of serious adverse events strongly supports the safety of active, non-pharmacological strategies as a first-line approach for LBP.
Quality of Evidence
According to the PEDro scale, the majority of the forty-three included studies were of high quality (scores ≥6), demonstrating low risk of bias in domains such as random allocation, baseline comparability, and outcome reporting. The most consistent sources of potential bias were performance bias, due to the inherent difficulty of blinding participants and therapists to physical and psychological interventions, and attrition bias in studies that experienced significant dropout or did not employ intention-to-treat analysis.
When interpreted through the GRADE framework, the overall quality of evidence for the effectiveness of holistic interventions on pain, function, and quality of life in adults with LBP can be considered moderate to high. This judgment is based on the large number of high-quality RCTs demonstrating consistent, positive effects. The findings of this review are therefore robust and provide a strong, reliable evidence base to inform clinical practice guidelines and policy decisions, aligning seamlessly with the recommendations of major international bodies like the WHO [6] and NICE [72].
Conclusions
The findings of this review affirm that holistic, multidimensional interventions are superior to traditional biomedical management for chronic low back pain. Exercise remains the cornerstone of effective treatment, especially when delivered as part of an individualized and supervised program. Evidence supports exercise sessions two to three times per week for eight to twelve weeks, incorporating core stabilization, motor control, resistance, or mind-body modalities such as yoga and Pilates.
Psychologically informed interventions, including cognitive behavioral therapy, acceptance and commitment therapy, and mindfulness-based stress reduction, further enhance long-term outcomes by addressing fear, catastrophizing, and emotional distress. Patient education that reframes pain understanding and promotes self-efficacy is essential to maintain engagement and reduce recurrence.
Overall, the review concludes that successful management of chronic low back pain requires an integrated approach that focuses on restoring function, improving coping capacity, and enhancing psychosocial resilience. Clinicians should tailor interventions to each individual while maintaining flexibility to account for cultural and contextual differences, especially in resource-limited environments.
Recommendations for Practice and Future Research
A. Clinical Practice Recommendations
Effective management of low back pain should be grounded in a comprehensive biopsychosocial assessment that identifies individual needs across physical, emotional, and social dimensions. Care should prioritize active rehabilitation over passive treatment.
Supervised and individualized exercise programs should include a mix of aerobic, strength, and motor control components, adjusted according to each patient’s capacity and symptom tolerance. For individuals presenting with high psychological distress or maladaptive coping, integrating cognitive and mindfulness-based strategies is crucial.
Education that encourages active coping and self-management must be incorporated into all stages of care to empower patients and promote long-term adherence. Clinicians should also consider cultural sensitivity, affordability, and accessibility when implementing these interventions, ensuring feasibility in diverse and low-resource settings.
B. Recommendations for Future Research
Future studies should be designed as large, high-quality randomized controlled trials with longer follow-up periods of at least two years to determine the sustainability of holistic interventions. Research should aim to develop personalized rehabilitation models that identify the best combination of exercise, psychological, and educational elements for specific patient profiles.
Implementation research is needed to evaluate cost-effective delivery models that can be adapted to community and primary care settings, particularly in low- and middle-income countries. More studies should explore technology-assisted rehabilitation such as virtual reality and tele-rehabilitation to improve access and adherence.
Researchers should also adopt standardized outcome measures for pain, functional capacity, and psychosocial health to enhance comparability across studies. Finally, there is a pressing need to include participants from underrepresented populations and regions such as sub-Saharan Africa to ensure global applicability of findings.
Limitations
Although this review followed rigorous methodological standards, certain limitations should be acknowledged. Considerable variability existed among the included studies regarding intervention type, duration, and measurement tools, which made direct comparisons challenging. Performance bias was unavoidable since participants and therapists could not be blinded in behavioral and exercise interventions. Attrition bias was noted in several trials with incomplete follow-up data.
Most of the studies were conducted in high-income countries, limiting generalizability to other healthcare contexts. Additionally, only English-language publications were included, which may have introduced language and publication bias. Despite these limitations, the overall evidence remains robust and clinically relevant.
Closing Remark
In conclusion, this review reinforces the growing consensus that chronic low back pain should be managed through a comprehensive, person-centered, and evidence-based approach. Integrating physical, psychological, and educational interventions provides sustainable improvements in pain relief, physical function, and quality of life. Future research and clinical practice should continue to advance the implementation of holistic rehabilitation strategies that not only alleviate pain but also restore independence, productivity, and well-being across diverse patient populations.
List of Abbreviations
| ACSM | American College of Sports Medicine |
| ACT | Acceptance and Commitment Therapy |
| ADIM | Abdominal Drawing-In Maneuver |
| AHAS | Asymmetry of Hip Abductor Strength |
| ALL | Anterior Longitudinal Ligament |
| ASLR | Active Straight Leg Raise |
| BBQ | Back Beliefs Questionnaire |
| BGA | Behavioural Graded Activity |
| BHT | Breath Hold Time |
| BMI | Body Mass Index |
| CBT | Cognitive Behavioural Therapy |
| CDSR | Cochrane Database of Systematic Reviews |
| CENTRAL | Cochrane Central Register of Controlled Trials |
| CES-D | Center for Epidemiologic Studies Depression Scale |
| CFT | Cognitive Functional Therapy |
| CG | Control Group |
| CHT | Commitment to Health Theory |
| CI | Confidence Interval |
| CINAHL | Cumulative Index to Nursing and Allied Health Literature |
| CLBP | Chronic Low Back Pain |
| CNSLBP | Chronic Non-Specific Low Back Pain |
| CPM | Conditioned Pain Modulation |
| CROB | Cochrane Risk of Bias |
| CT | Cognitive Therapy |
| DST | Dynamic Systems Theory |
| EA | Electroacupuncture |
| EARS | Exercise Adherence Rating Scale |
| EG | Experimental Group |
| EMG | Electromyography |
| ESWT | Extracorporeal Shockwave Therapy |
| FABQ | Fear-Avoidance Beliefs Questionnaire |
| GBD | Global Burden of Disease |
| GRADE | Grading of Recommendations, Assessment, Development, and Evaluations |
| GROC | Global Rating of Change |
| HBM | Health Belief Model |
| HRQOL / HRQoL | Health-Related Quality of Life |
| IASP | International Association for the Study of Pain |
| IMT | Inspiratory Muscle Training |
| IPAQ | International Physical Activity Questionnaire |
| ITT | Intention-To-Treat |
| LBP | Low Back Pain |
| LMICs | Low- and Middle-Income Countries |
| MA | Manual Acupuncture |
| MBR | Multidisciplinary Biopsychosocial Rehabilitation |
| MBSR | Mindfulness-Based Stress Reduction |
| MCE | Motor Control Exercises |
| MD | Mean Difference |
| MDT | McKenzie Method |
| MeSH | Medical Subject Headings |
| MODI | Modified Oswestry Disability Index |
| MODQ | Modified Oswestry Disability Questionnaire |
| N/A | Not Applicable |
| NICE | National Institute for Health and Care Excellence |
| NIHR | National Institute of Health Research |
| NPRS | Numerical Pain Rating Scale |
| NRS | Numerical Rating Scale |
| NSAIDs | Non-Steroidal Anti-Inflammatory Drugs |
| ODI | Oswestry Disability Index |
| OMT | Orthopaedic Manual Therapy |
| PACT | Physiotherapy informed by Acceptance and Commitment Therapy |
| PEDro | Physiotherapy Evidence Database |
| PHQ-8 | Patient Health Questionnaire-8 |
| PICOS | Population, Intervention, Comparison, Outcomes, Study Design |
| PLL | Posterior Longitudinal Ligament |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PSFS | Patient-Specific Functional Scale |
| PT | Physical Therapy / Physiotherapy |
| QBPDS | Quebec Back Pain Disability Scale |
| QoL / QOL | Quality of Life |
| RA | Rectus Abdominis |
| RCT | Randomized Controlled Trial |
| RMDQ | Roland-Morris Disability Questionnaire |
| RR | Respiratory Rate; Risk Ratio |
| SD | Standard Deviation |
| SDNN | Standard Deviation of NN Intervals (Heart Rate Variability) |
| SDT | Self-Determination Theory |
| SEM | Social Ecological Model; Structural Equation Modeling |
| SES | Schmerzempfindungs-Skala (Pain Perception Scale) |
| SF-12 / SF-36 | Short Form Health Survey (12 or 36 items) |
| SHR | Simulated Horseback Riding |
| SMD | Standardised Mean Difference |
| SMR | Self-Myofascial Release |
| SSE | Stabilization Exercises |
| STB | Stabilization |
| TCM | Traditional Chinese Medicine |
| TENS | Transcutaneous Electrical Nerve Stimulation |
| TrA | Transversus Abdominis |
| TSK | Tampa Scale of Kinesiophobia |
| TTM | Transtheoretical Model |
| TUG | Timed Up and Go |
| UC | Usual Care |
| VAS | Visual Analogue Scale |
| VR / VRT | Virtual Reality (Training) |
| WHO | World Health Organization |
| WHOQOL | World Health Organization Quality of Life |
| WMD | Weighted Mean Difference |
| YLDs | Years Lived with Disability |
Ethics Approval and Consent to Participate
As this study was based on previously published data and did not involve direct interaction with human participants, ethics approval and informed consent were not required. The review adhered to the principles outlined in the Declaration of Helsinki and followed accepted ethical standards for secondary analyses.
Consent for Publication
Not applicable, as no individual person’s data (including images, videos, or personal details) are contained in this manuscript.
Availability of Data and Materials
All data generated or analyzed during this study are included in the published article and its supplementary files. Additional datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Competing Interests
The author declares no competing interests related to this work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ Contributions
Nweke Vincent Chinonso conceptualized and designed the study, conducted the literature search, data extraction, critical appraisal, statistical analysis, and prepared the initial draft of the manuscript. Prof. Charles I. Ezema provided overall supervision, mentorship, and critical review of the work. Fatai Ekundayo contributed to the interpretation of findings and provided intellectual and technical input during manuscript refinement. Onyekwelu Adaeze assisted in data screening, reference verification, and formatting of tables and figures. Nweke Queeneth kadilobari participated in the literature review, data validation, and proofreading of the final manuscript draft. All authours supported the synthesis of evidence and contributed to the quality appraisal of included studies. Nweke Augustine contributed to the review organization, formatting, and manuscript editing for journal submission. All authors read and approved the final version of the manuscript prior to submission.
Authors’ Information
Nweke Vincent Chinonso is a physiotherapist and researcher specializing in Musculoskeletal rehabilitation. Prof. Charles I. Ezema is a Professor of Physiotherapy and the author’s research supervisor at the University of Nigeria, Enugu Campus.
References
- World Health Organization WHO. Low back pain. World Health Organization: WHO [Internet], 19 Jun 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/low-back-pain? (accessed on 16 December 2025).
- Gill, T.K.; Mittinty, M.M.; March, L.M.; Steinmetz, J.D.; Culbreth, G.T.; Cross, M.; et al. Global, regional, and national burden of other musculoskeletal disorders, 1990–2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. The Lancet Rheumatology. 2023, 5, e670–e682. [Google Scholar] [CrossRef]
- Buchbinder, R.; Underwood, M.; Hartvigsen, J.; Maher, C.G. The Lancet Series call to action to reduce low value care for low back pain: an update. Pain. 2020, 161, S57–S64. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Main, C.J.; George, S.Z. Psychosocial influences on low back pain: why should you care? Physical therapy. 2011, 91, 609–613. [Google Scholar] [CrossRef]
- Ageing (AAH), H. WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings. World Health Organization [Internet], 7 Dec 2023. Available online: https://www.who.int/publications/i/item/9789240081789 (accessed on 16 December 2025).
- Hayden, J.A.; Ogilvie, R.; Kashif, S.; Singh, S.; Boulos, L.; Stewart, S.A.; et al. Exercise treatments for chronic low back pain: a network meta-analysis - PMC. The Cochrane Database of Systematic Reviews 2023, 6. [Google Scholar]
- Nicholas, M.K.; Linton, S.J.; Watson, P.J.; Main, C.J. Early Identification and Management of Psychological Risk Factors (“Yellow Flags”) in Patients With Low Back Pain: A Reappraisal. Physical Therapy 2011, 91, 737–753. [Google Scholar] [CrossRef]
- Cherkin, D.C.; Sherman, K.J.; Balderson, B.H.; Cook, A.J.; Anderson, M.L.; Hawkes, R.J.; et al. Effect of Mindfulness-Based Stress Reduction vs Cognitive Behavioral Therapy or Usual Care on Back Pain and Functional Limitations in Adults With Chronic Low Back Pain: A Randomized Clinical Trial. JAMA 2016, 315, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J.; Apeldoorn, A.T.; Chiarotto, A.; Smeets, R.J.E.M.; Ostelo, R.W.J.G.; Guzman, J.; et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. The Cochrane database of systematic reviews 2014, 2014, CD000963. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef] [PubMed]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. The Cochrane database of systematic reviews 2017, 4, CD011279. [Google Scholar]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef]
- Sharma, S.; Traeger, A.C.; Reed, B.; Hamilton, M.; O’Connor, D.A.; Hoffmann, T.C.; et al. Clinician and patient beliefs about diagnostic imaging for low back pain: a systematic qualitative evidence synthesis. BMJ open. 2020, 10, e037820. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical research ed) 2021, 372, n71. [Google Scholar]
- Cochrane [Internet]. [cited 2025 Dec 16]. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://www.cochrane.org/authors/handbooks-and-manuals/handbook.
- Cochrane Handbook for Systematic Reviews of Interventions; 20 Sep 2019.
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Physical therapy 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. Journal of physiotherapy 2020, 66, 59. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R.W.; Foley, N.C.; Bhogal, S.K.; Speechley, M.R. An evidence-based review of stroke rehabilitation. Topics in stroke rehabilitation 2003, 10, 29–58. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.D. Systematic Reviews to Answer Health Care Questions; Lippincott Williams & Wilkins, 2024. [Google Scholar]
- Aasa, B.; Berglund, L.; Michaelson, P.; Aasa, U. Individualized Low-Load Motor Control Exercises and Education Versus a High-Load Lifting Exercise and Education to Improve Activity, Pain Intensity, and Physical Performance in Patients With Low Back Pain: A Randomized Controlled Trial. Journal of Orthopaedic & Sports Physical Therapy 2015, 45, 77–85. [Google Scholar]
- Afzal, M.W.; Ahmad, A.; Mohseni Bandpei, M.A.; Gillani, S.A.; Hanif, A.; Sharif Waqas, M. Effects of virtual reality exercises and routine physical therapy on pain intensity and functional disability in patients with chronic low back pain. Journal of the Pakistan Medical Association 2022, 72. [Google Scholar] [CrossRef]
- Ahmadi, H.; Adib, H.; Selk-Ghaffari, M.; Shafizad, M.; Moradi, S.; Madani, Z.; et al. Comparison of the effects of the Feldenkrais method versus core stability exercise in the management of chronic low back pain: a randomised control trial. Clinical Rehabilitation 2020, 34, 1449–1457. [Google Scholar] [CrossRef]
- Ahmadnezhad, L.; Yalfani, A.; Gholami Borujeni, B. Inspiratory Muscle Training in Rehabilitation of Low Back Pain: A Randomized Controlled Trial. Journal of sport rehabilitation 2020, 29, 1151–1158. [Google Scholar] [CrossRef]
- Akbaş, E.; Özdemir, M.; Akbaş, A.; Usgu, S.; Bulut, H.T. Investigation of the effect of different intensity stabilization exercises on core muscle stiffness and pain in chronic low back pain: a single-blind, randomized controlled trial. Rheumatology international 2025, 45, 201. [Google Scholar] [CrossRef] [PubMed]
- Back, C.G.N.; Peron, R.; Lopes, C.V.R.; de Souza, J.V.E.; Liebano, R.E. Immediate effect of extracorporeal shockwave therapy in patients with chronic nonspecific low back pain: A randomized placebo-controlled triple-blind trial. Clinical Rehabilitation 2025, 39, 701–702. [Google Scholar] [CrossRef]
- Bagg, M.K.; Wand, B.M.; Cashin, A.G.; Lee, H.; Hübscher, M.; Stanton, T.R.; et al. Effect of Graded Sensorimotor Retraining on Pain Intensity in Patients With Chronic Low Back Pain. JAMA 2022, 328, 430. [Google Scholar] [CrossRef]
- Bagheri, R.; Hedayati, R.; Ehsani, F.; Hemati-Boruojeni, N.; Abri, A.; Taghizadeh Delkhosh, C. Cognitive Behavioral Therapy With Stabilization Exercises Affects Transverse Abdominis Muscle Thickness in Patients With Chronic Low Back Pain: A Double-Blinded Randomized Trial Study. Journal of manipulative and physiological therapeutics 2020, 43, 418–428. [Google Scholar] [CrossRef]
- Bello, A.I.; Quartey, J.; Lartey, M. Efficacy of Behavioural Graded Activity Compared with Conventional Exercise Therapy in Chronic Non-Specific Low Back Pain: Implication for Direct Health Care Cost. Ghana medical journal. 2015, 49, 173–180. [Google Scholar] [CrossRef]
- Blanco-Giménez, P.; Vicente-Mampel, J.; Gargallo, P.; Maroto-Izquierdo, S.; Martín-Ruíz, J.; Jaenada-Carrilero, E.; et al. Effect of exercise and manual therapy or kinesiotaping on sEMG and pain perception in chronic low back pain: a randomized trial. BMC musculoskeletal disorders 2024, 25, 583. [Google Scholar] [CrossRef]
- Brandt, Y.; Currier, L.; Plante, T.W.; Schubert Kabban, C.M.; Tvaryanas, A.P. A Randomized Controlled Trial of Core Strengthening Exercises in Helicopter Crewmembers with Low Back Pain. Aerospace medicine and human performance 2015, 86, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.A.; Anderson, M.L.; Cherkin, D.C.; Balderson, B.H.; Cook, A.J.; Sherman, K.J.; et al. Moderators and Nonspecific Predictors of Treatment Benefits in a Randomized Trial of Mindfulness-Based Stress Reduction vs Cognitive-Behavioral Therapy vs Usual Care for Chronic Low Back Pain. The journal of pain. 2023, 24, 282–303. [Google Scholar] [CrossRef] [PubMed]
- Comachio, J.; Oliveira, C.C.; Silva, I.F.R.; Magalhães, M.O.; Marques, A.P. Effectiveness of Manual and Electrical Acupuncture for Chronic Non-specific Low Back Pain: A Randomized Controlled Trial. Journal of acupuncture and meridian studies 2020, 13, 87–93. [Google Scholar] [CrossRef]
- Cortell-Tormo, J.M.; Sánchez, P.T.; Chulvi-Medrano, I.; Tortosa-Martínez, J.; Manchado-López, C.; Llana-Belloch, S.; et al. Effects of functional resistance training on fitness and quality of life in females with chronic nonspecific low-back pain. Journal of back and musculoskeletal rehabilitation 2018, 31, 95–105. [Google Scholar] [CrossRef]
- Cruz-Díaz, D.; Martínez-Amat, A.; Osuna-Pérez, M.C.; De la Torre-Cruz, M.J.; Hita-Contreras, F. Short- and long-term effects of a six-week clinical Pilates program in addition to physical therapy on postmenopausal women with chronic low back pain: a randomized controlled trial. Disability and rehabilitation 2016, 38, 1300–1308. [Google Scholar] [CrossRef]
- Cruz-Díaz, D.; Bergamin, M.; Gobbo, S.; Martínez-Amat, A.; Hita-Contreras, F. Comparative effects of 12 weeks of equipment based and mat Pilates in patients with Chronic Low Back Pain on pain, function and transversus abdominis activation. A randomized controlled trial. Complementary therapies in medicine 2017, 33, 72–77. [Google Scholar] [CrossRef]
- Cruz-Díaz, D.; Romeu, M.; Velasco-González, C.; Martínez-Amat, A.; Hita-Contreras, F. The effectiveness of 12 weeks of Pilates intervention on disability, pain and kinesiophobia in patients with chronic low back pain: a randomized controlled trial. Clinical rehabilitation 2018, 32, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Day, M.A.; Ciol, M.A.; Mendoza, M.E.; Borckardt, J.; Ehde, D.M.; Newman, A.K.; et al. The effects of telehealth-delivered mindfulness meditation, cognitive therapy, and behavioral activation for chronic low back pain: a randomized clinical trial. BMC medicine 2024, 22, 156. [Google Scholar] [CrossRef] [PubMed]
- 40de Lira, M.R.; Meziat-Filho, N.; Zuelli Martins Silva, G.; Castro, J.; Fernandez, J.; Guirro RRde, J. Efficacy of cognitive functional therapy for pain intensity and disability in patients with non-specific chronic low back pain: a randomised sham-controlled trial. British journal of sports medicine 2025, 59, 912–920. [Google Scholar] [CrossRef]
- Elabd, A.M.; Elabd, O.M. Effect of aerobic exercises on patients with chronic mechanical low back pain: A randomized controlled clinical trial. Journal of bodywork and movement therapies 2024, 37, 379–385. [Google Scholar] [CrossRef]
- Feng, Y.; Zhu, C.; Liu, H.; Bao, T.; Wang, C.; Wang, Z.; et al. Effect of telemedicine-supported structured exercise program in patients with chronic low back pain: a randomized controlled trial. PloS one 2025, 20, e0326218. [Google Scholar]
- Ford, J.J.; Hahne, A.J.; Surkitt, L.D.; Chan, A.Y.P.; Richards, M.C.; Slater, S.L.; et al. Individualised physiotherapy as an adjunct to guideline-based advice for low back disorders in primary care: a randomised controlled trial. British journal of sports medicine 2016, 50, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Freiwald, J.; Hoppe, M.W.; Beermann, W.; Krajewski, J.; Baumgart, C. Effects of supplemental heat therapy in multimodal treated chronic low back pain patients on strength and flexibility. Clinical biomechanics 2018, 57, 107–113. [Google Scholar] [CrossRef]
- Ghavipanje, V.; Rahimi, N.M.; Akhlaghi, F. Six Weeks Effects of Dynamic Neuromuscular Stabilization (DNS) Training in Obese Postpartum Women With Low Back Pain: A Randomized Controlled Trial. Biological research for nursing 2022, 24, 106–114. [Google Scholar] [CrossRef]
- Glombiewski, J.A.; Holzapfel, S.; Riecke, J.; Vlaeyen, J.W.S.; de Jong, J.; Lemmer, G.; et al. Exposure and CBT for chronic back pain: An RCT on differential efficacy and optimal length of treatment. Journal of consulting and clinical psychology 2018, 86, 533–545. [Google Scholar] [CrossRef]
- Godfrey, E.; Wileman, V.; Galea Holmes, M.; McCracken, L.M.; Norton, S.; Moss-Morris, R.; et al. Physical Therapy Informed by Acceptance and Commitment Therapy (PACT) Versus Usual Care Physical Therapy for Adults With Chronic Low Back Pain: A Randomized Controlled Trial. The journal of pain. 2020, 21, 71–81. [Google Scholar] [CrossRef]
- Grande-Alonso, M.; Suso-Martí, L.; Cuenca-Martínez, F.; Pardo-Montero, J.; Gil-Martínez, A.; La Touche, R. Physiotherapy Based on a Biobehavioral Approach with or Without Orthopedic Manual Physical Therapy in the Treatment of Nonspecific Chronic Low Back Pain: A Randomized Controlled Trial. Pain medicine 2019, 20, 2571–2587. [Google Scholar] [CrossRef]
- Gwon, A.J.; Kim, S.Y.; Oh, D.W. Effects of integrating Neurac vibration into a side-lying bridge exercise on a sling in patients with chronic low back pain: a randomized controlled study. Physiotherapy theory and practice 2020, 36, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Halliday, M.H.; Pappas, E.; Hancock, M.J.; Clare, H.A.; Pinto, R.Z.; Robertson, G.; et al. A Randomized Controlled Trial Comparing the McKenzie Method to Motor Control Exercises in People With Chronic Low Back Pain and a Directional Preference. The Journal of orthopaedic and sports physical therapy 2016, 46, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Lucas, P.; Leirós-Rodríguez, R.; Mota, J.; García-Soidán, J.L. Effects of a back school-based intervention on non-specific low back pain in adults: a randomized controlled trial. BMC complementary medicine and therapies 2023, 23, 229. [Google Scholar] [CrossRef]
- Hohmann, C.D.; Stange, R.; Steckhan, N.; Robens, S.; Ostermann, T.; Paetow, A.; et al. The Effectiveness of Leech Therapy in Chronic Low Back Pain. Deutsches Arzteblatt international 2018, 115, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Kamali, F.; Sinaei, E.; Taherkhani, E. Comparing spinal manipulation with and without Kinesio Taping® in the treatment of chronic low back pain. Journal of bodywork and movement therapies 2018, 22, 540–545. [Google Scholar] [CrossRef]
- Khan, K.; Ahmad, A.; Mohseni Bandpei, M.A.; Kashif, M. Comparison of the effects of dry needling and spinal manipulative therapy versus spinal manipulative therapy alone on functional disability and endurance in patients with nonspecific chronic low back pain: An experimental study. Medicine 2024, 103, e39734. [Google Scholar] [CrossRef]
- Kim, S.K.; Park, H. The Effect of Auricular Acupressure for Chronic Low Back Pain in Elders: A Randomized Controlled Study. Holistic nursing practice 2021, 35, 182–190. [Google Scholar] [CrossRef]
- Kim, T.; Lee, J.; Oh, S.; Kim, S.; Yoon, B. Effectiveness of Simulated Horseback Riding for Patients With Chronic Low Back Pain: A Randomized Controlled Trial. Journal of sport rehabilitation 2020, 29, 179–185. [Google Scholar] [CrossRef]
- Kong, J.T.; Puetz, C.; Tian, L.; Haynes, I.; Lee, E.; Stafford, R.S.; et al. Effect of Electroacupuncture vs Sham Treatment on Change in Pain Severity Among Adults With Chronic Low Back Pain: A Randomized Clinical Trial. JAMA network open. 2020, 3, e2022787. [Google Scholar] [CrossRef] [PubMed]
- Kuvačić, G.; Fratini, P.; Padulo, J.; Antonio, D.I.; De Giorgio, A. Effectiveness of yoga and educational intervention on disability, anxiety, depression, and pain in people with CLBP: A randomized controlled trial. Complementary therapies in clinical practice 2018, 31, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Lang, A.E.; Hendrick, P.A.; Clay, L.; Mondal, P.; Trask, C.M.; Bath, B.; et al. A randomized controlled trial investigating effects of an individualized pedometer driven walking program on chronic low back pain. BMC musculoskeletal disorders 2021, 22, 206. [Google Scholar] [CrossRef]
- Lee, M.; Kim, J. Effects of aquarobics on back pain, sleep, and memory in older women with chronic pain. Medicine 2025, 104, e43199. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, Q.; Zhang, X.; E, Y.; Su, Y. The impact of core training combined with breathing exercises on individuals with chronic non-specific low back pain. Frontiers in public health 2025, 13, 1518612. [Google Scholar] [CrossRef]
- Luo, Y.; Yang, M.; Liu, T.; Zhong, X.; Tang, W.; Guo, M.; et al. Effect of hand-ear acupuncture on chronic low-back pain: a randomized controlled trial. Journal of traditional Chinese medicine = Chung i tsa chih ying wen pan 2019, 39, 587–598. [Google Scholar]
- Song, J.; Yim, J. Effects of Self-Myofascial Release and Dynamic Neuromuscular Stabilization Exercises on Pain, Balance, Muscle Function, and the Autonomic Nervous System in Women with Chronic Low Back Pain. Medical science monitor : international medical journal of experimental and clinical research 2025, 31, e949985. [Google Scholar] [CrossRef]
- Yalfani, A.; Abedi, M.; Raeisi, Z.; Asgarpour, A. The effects of virtual reality training on postural sway and physical function performance on older women with chronic low back pain: A double-blind randomized clinical trial. Journal of back and musculoskeletal rehabilitation 2024, 37, 761–770. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews 2015, 4. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Traeger, A.C.; Lee, H.; Hübscher, M.; Skinner, I.W.; Moseley, G.L.; Nicholas, M.K.; et al. Effect of Intensive Patient Education vs Placebo Patient Education on Outcomes in Patients With Acute Low Back Pain: A Randomized Clinical Trial. JAMA neurology 2019, 76, 161–169. [Google Scholar] [CrossRef]
- Ghamkhar, L.; Kahlaee, A.H. Pain and Pain-Related Disability Associated With Proprioceptive Impairment in Chronic Low Back Pain Patients: A Systematic Review. Journal of Manipulative and Physiological Therapeutics 2019, 42, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; Ada, L.; Dean, C.M.; Preston, E. Biofeedback improves performance in lower limb activities more than usual therapy in people following stroke: a systematic review. Journal of physiotherapy 2017, 63, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Roseen, E.J.; Conyers, F.G.; Atlas, S.J.; Mehta, D.H. Initial Management of Acute and Chronic Low Back Pain: Responses from Brief Interviews of Primary Care Providers. Journal of alternative and complementary medicine 2021, 27, S106–S114. [Google Scholar] [CrossRef]
- Allet, L.; Armand, S.; de Bie, R.A.; Golay, A.; Monnin, D.; Aminian, K.; et al. The gait and balance of patients with diabetes can be improved: a randomised controlled trial. Diabetologia 2010, 53, 458–466. [Google Scholar] [CrossRef] [PubMed]
- NCBI Bookshelf [Internet]. National Institute for Health and Care Excellence: Guidelines. 2003. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11822/ (accessed on 18 December 2025).
Figure 1.
PRISMA Diagram for muscle strength, walking balance, and quality of life; adapted from Moher, Shamseer & Clarke et al., [65] Preferred Reporting Items for Systematic Reviews and Meta Analyses.
Figure 1.
PRISMA Diagram for muscle strength, walking balance, and quality of life; adapted from Moher, Shamseer & Clarke et al., [65] Preferred Reporting Items for Systematic Reviews and Meta Analyses.
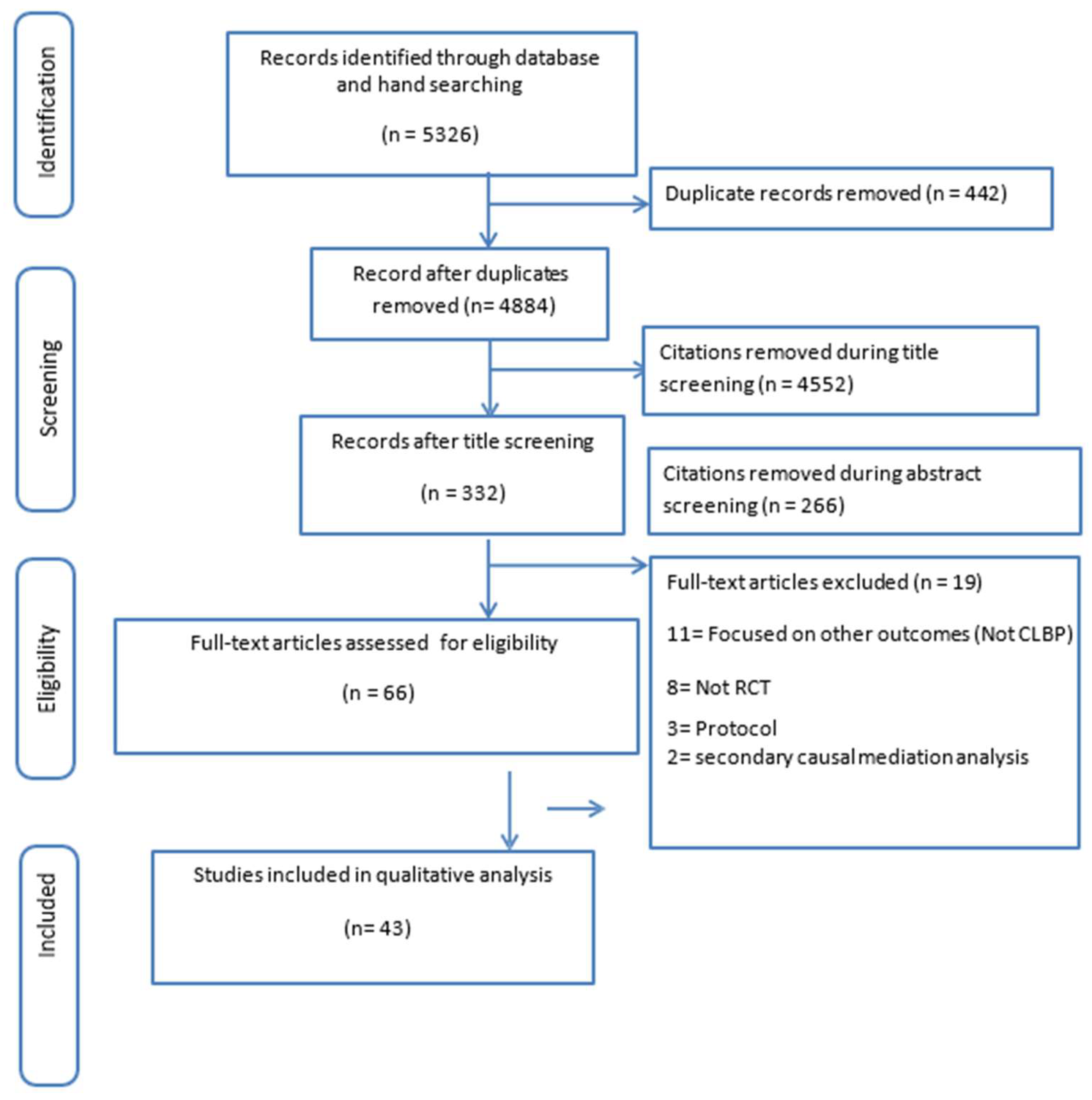
Figure 2.
Evidence-based studies on holistic management of low back pain.


Table 2.
Table of Study Characteristics.
| S/N | AUTHOR/YEAR | COUNTRY/ SETTING | PARTICIPANTS (AGE RANGE/MEAN, GENDER, SAMPLE SIZE, RETENTION, DISEASE HISTORY/DURATION, SEVERITY) | INTERVENTION (TYPE, COMPONENTS, THEORETICAL FRAMEWORK, PROVIDER, SETTING, DURATION, FOLLOW-UP) | CONTROL/ COMPARATOR | OUTCOMES ASSESSED | OUTCOME MEASURES | TIMEPOINTS ASSESSED | SUMMARY OF RESULTS |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Aasa et al., 2015 [22] |
Sweden / Outpatient physiotherapy setting | Adults with non-specific low back pain; mean age ~40 years; N = 70 randomised (62 completed); majority chronic (>12 weeks duration); both male and female | Individualized low-load motor control exercise + education: focus on retraining deep trunk stabilizers and postural control; supervised by physiotherapists; 12 weeks, 2 sessions/week; education included ergonomics and self-management | High-load lifting exercise + education: general strengthening with progressive resistance, plus same education content; supervised physiotherapy | Pain intensity, activity limitation, physical performance | Visual Analogue Scale (VAS), Patient-Specific Functional Scale (PSFS), physical performance tests (lifting, endurance tasks) | Baseline, post-intervention (12 weeks), follow-up at 6 months | Both groups improved significantly in pain and activity. No significant between-group differences. Low-load motor control and high-load lifting exercise were equally effective when combined with education. |
| 2 | Afzal et al., 2022 [23] |
Pakistan / Physiotherapy department | Adults with chronic low back pain; N = 68 randomised (34 per group, 62 completed); mean age ~40 years; both genders included; symptom duration >12 weeks | Virtual reality exercise programme + routine physical therapy: interactive VR-based exercises designed to enhance engagement and adherence, combined with conventional physiotherapy; 4 weeks, 3 sessions/week | Routine physical therapy alone: conventional exercises and physiotherapy management without VR component | Pain intensity, functional disability | Visual Analogue Scale (VAS), Oswestry Disability Index (ODI) | Baseline, post-intervention (4 weeks) | VR + physiotherapy group showed greater reductions in pain intensity and disability compared to physiotherapy alone. Intervention was feasible and well-tolerated. |
| 3 | Ahmadi et al., 2020 [24] |
Iran / Outpatient, Sports Medicine Clinic, Mazandaran Medical University | 60 patients with chronic non-specific low back pain; equally randomised into two groups; mean age ~40 years; both genders included; symptom duration >12 weeks | Feldenkrais Method: supervised exercise therapy + theoretical training content, 2 sessions/week for 5 weeks | Core stability exercise + education: educational programme and home-based core stability training for 5 weeks | Pain intensity, disability, quality of life, interoceptive awareness | WHO Quality of Life Questionnaire, McGill Pain Questionnaire, Oswestry Disability Index (ODI), Multidimensional Assessment of Interoceptive Awareness | Baseline, post-intervention (5 weeks) | Both groups improved in pain, but Feldenkrais group showed greater improvements in quality of life (p = 0.006), interoceptive awareness (p < 0.001), and disability (p = 0.021). No significant between-group difference in McGill pain scores. |
| 4 | Ahmadnezhad et al., 2020 [25] |
Iran / Clinical rehabilitation laboratory | 47 athletes with CLBP (23 male, 24 female) with chronic low back pain; randomly divided into intervention and control groups; mean age not reported | Inspiratory Muscle Training (IMT): performed using POWERbreathe KH1; 8 weeks, 7 days/week, 2 sessions/day; initial load at 50% of maximum inspiratory pressure with progressive increases | Control group: no IMT; continued with standard rehabilitation management | Pain intensity, core muscle activity, pulmonary function | Surface EMG (erector spinae, multifidus, transverse abdominis, rectus abdominis), spirometry for respiratory parameters, Visual Analogue Scale (VAS) | Baseline, post-intervention (8 weeks) | IMT group showed significant increases in multifidus and transverse abdominis activity, improved pulmonary function, and a reduction in pain intensity (p < 0.05). Control group did not show comparable changes. |
| 5 | Akbaş et al., 2025 [26] |
Turkey / Rheumatology outpatient clinic | 50 adults with chronic low back pain; randomised into 3 groups (Group 1 = 16, Group 2 = 17, Control = 17); mean age not specified; all completed | Stabilization exercises (SSE): Group 1 = supervised 4 days/week; Group 2 = supervised 2 days/week; duration = 12 weeks; delivered by physiotherapists | Home exercise programme only | Core muscle stiffness, pain intensity, disability | Shear wave elastography (TrA stiffness), Visual Analogue Scale (VAS), Oswestry Disability Index (ODI) | Baseline, 6 weeks, 12 weeks | Group 1 (SSE 4x/week) showed significantly greater improvements in core muscle stiffness and disability compared to Group 2 and control (p < 0.05). Both SSE groups reduced pain vs. control, but no significant difference between Group 1 and 2 for pain. |
| 6 | Back et al., 2024 [27] |
Brazil / Primary care physiotherapy clinic | 81 patients with chronic non-specific low back pain; aged 18–80 years; pain ≥3 months; baseline pain ≥3 on VAS; randomised into 3 groups (concave tip, convex tip, placebo) | Extracorporeal shockwave therapy (ESWT): single session, radial type; 2000 discharges, 100 mJ energy, 5 Hz frequency; applied with concave or convex applicator tips | Placebo treatment: sham application (no therapeutic dose delivered) | Pain intensity, pressure pain threshold, temporal summation of pain, functional performance | Visual Analogue Scale (VAS), algometry for pressure pain threshold, temporal summation protocols, functional tests | Baseline, immediate post-intervention | Concave tip ESWT produced a 2-point greater reduction in pain compared to placebo (p < 0.01), and significantly higher pressure pain thresholds compared to convex tip and placebo groups (p < 0.05). Convex tip produced smaller, non-significant effects. |
| 7 | Bagg et al., 2022 [28] |
Australia / Medical research institute, Sydney | 276 adults with chronic non-specific low back pain (>3 months); mean age 46 (SD 14.3); 50% women; recruited from primary care and community; 261 (95%) completed | Graded sensorimotor retraining (RESOLVE): 12 weekly clinical sessions + home training; included movement retraining, education, and graded physical activity; supervised by trained clinicians | Sham and attention control: 12 weekly sessions including sham laser, sham diathermy, sham brain stimulation, and non-specific home training without focus on movement or activity | Pain intensity (primary), function, disability | Numerical Rating Scale (0–10), disability questionnaires (not detailed in abstract) | Baseline, 18 weeks (primary endpoint) | Intervention group improved more than control: mean pain reduced from 5.6 → 3.1 vs. 5.8 → 4.0; between-group mean difference = –1.0 (95% CI: –1.5 to –0.4, p = .001). Effect statistically significant but small. |
| 8 | Bagheri et al., 2020 [29] |
Iran / Outpatient physiotherapy clinic | 40 adults with non-specific chronic low back pain; randomised into 2 groups (n = 20 per group); mean age not specified; both genders included | CBT + Stabilization Exercises (SE): supervised SE combined with cognitive behavioural therapy sessions addressing fear-avoidance, coping strategies; duration not specified in abstract | Stabilization Exercises alone: no CBT component | TrA muscle thickness, fear-avoidance beliefs, disability | Ultrasound imaging of TrA contraction (during ADIM & ASLR), Fear-Avoidance Beliefs Questionnaire (FABQ), Roland-Morris Disability Questionnaire (RMDQ) | Baseline, post-intervention (timeframe not stated, estimated short-term) | Experimental group (CBT + SE) showed greater TrA thickness increases during ADIM (p = .001), and significant improvements in FABQ (p = .04) and disability (RMDQ, p = .01) compared to SE alone. No group differences for TrA thickness during ASLR. |
| 9 | Bello et al., 2015 [30] |
Ghana / Outpatient physiotherapy clinic | 80 adults with chronic non-specific low back pain; mean age ~44 years; 62 participants (77.5%) completed (CET = 29, BGA = 33) | Behavioural Graded Activity (BGA): time-contingent, sub-maximal activities individually prescribed; 2 sessions/week for 12 weeks; supervised physiotherapy | Conventional Exercise Therapy (CET): supervised structured exercise sessions; 2 sessions/week for 12 weeks | Pain intensity, quality of life, healthcare cost | Numerical Rating Scale (NRS), RAND-36 health survey, physiotherapy cost questionnaire | Baseline, 4 weeks, 12 weeks | Both groups showed significant improvements in pain and quality of life (p < 0.001). No significant differences between groups. Cost analysis indicated that both CET and BGA could have implications for healthcare resource allocation. |
| 10 | Blanco-Giménez et al., 2024 [31] |
Spain / Outpatient physiotherapy clinics | Adults with chronic low back pain (mild disability by ODI); N=80 (3 parallel groups, intention-to-treat); mean age not specified | Exercise + adjunct therapy: 12-week supervised lumbo-pelvic core stability and motor-control program, supplemented by (a) manual therapy (MT) or (b) kinesiotaping (KT); delivered by physiotherapists | Exercise + adjunct comparison: exercise program combined with either MT or KT (both active comparators, no pure placebo/sham arm) | Pain perception, trunk muscle activation | Visual Analogue Scale (VAS), surface EMG of rectus abdominis (RA) and multifidus (MF) | Baseline, post-intervention (12 weeks) | Both MT + exercise and KT + exercise led to significant reductions in perceived pain. EMG analysis showed improved RA activation in exercise groups, but changes in MF were less consistent. No clear superiority between MT and KT adjuncts; benefits appeared to derive mainly from the exercise component. |
| 11 | Brandt et al., 2015 [32] |
USA / U.S. Air Force helicopter aircrew | 12 helicopter crewmembers with low back pain; 5 randomized to intervention, 7 to control; mean age not reported; military subgroup | Core strengthening exercises: 5 specific exercises performed 4 days/week for 12 weeks; supervised program | Control group: maintained regular exercise regimen | Pain intensity (daily and in-flight), disability, global improvement | Numerical Pain Rating Scale (NPRS daily & in-flight), Modified Oswestry Disability Index (MODI), Global Rating of Change Scale (GRCS) | Baseline, 12 weeks | Intervention group reported reduced in-flight pain (–1.8 points), decreased disability (–4.8 MODI points), and higher global improvement compared to control. No significant between-group difference in daily NPRS pain. |
| 12 | Chen et al., 2023 [33] |
USA / Outpatient, multicenter | 297 adults aged 20–70 with chronic low back pain; recruited from community; randomized into 3 groups: MBSR (n≈100), CBT (n≈100), usual care (n≈100) | Mindfulness-Based Stress Reduction (MBSR): 8-week program including meditation, mindful movement, and group sessions. Cognitive Behavioral Therapy (CBT): 8-week program targeting pain coping, catastrophizing, and behavior modification. | Usual Care (UC): standard medical management with no structured MBSR or CBT | Function, pain bothersomeness, depression, moderators of treatment response | Modified Roland Disability Questionnaire (function), 0–10 Numerical Rating Scale (pain bothersomeness), PHQ-8 (depression), mindfulness questionnaires | Baseline, 8 weeks, follow-up (duration not specified in abstract, likely 26+ weeks per trial registry) | Both MBSR and CBT significantly improved function and reduced pain compared to usual care. Moderators: mindfulness “nonjudging” trait predicted differential benefit (better outcomes with MBSR). Pain control beliefs and lower anxiety predicted improvement across all groups. |
| 13 | Comachio et al., 2020 [34] |
Brazil / Outpatient physiotherapy-acupuncture clinic | 66 adults aged 20–60 years with chronic non-specific low back pain (>3 months, pain ≥3/10); randomized equally to MA or EA groups | Manual Acupuncture (MA): 12 sessions at local, distal, and sensitized acupoints. Electroacupuncture (EA): 12 sessions with electrical stimulation through acupuncture needles. | Comparison between MA and EA (no sham/placebo group). | Pain intensity, disability, kinesiophobia | Numeric Rating Scale (NRS), Roland-Morris Disability Questionnaire (RMDQ), Tampa Scale of Kinesiophobia | Baseline, post-intervention (12 sessions), 3-month follow-up | Both MA and EA groups showed significant improvements in pain and disability, sustained at 3 months. No significant between-group differences, except reduced kinesiophobia in the MA group (–4.1 points, 95% CI = –7.0 to –1.1). |
| 14 | Cortell-Tormo et al., 2018 [35] |
Spain / University-based rehabilitation program | 19 adult females with chronic non-specific low back pain, recruited via Paris Task Force criteria; randomized to exercise (n=10) or control (n=9) | Functional resistance training: 12-week periodized program, 24 sessions (2x/week), focusing on functional movements, trunk stability, and progressive loading | Control group: no structured exercise intervention | Pain, disability, health-related quality of life, physical fitness | Visual Analogue Scale (VAS), Oswestry Disability Index (ODI), SF-36, physical fitness tests (flamingo, back endurance, side bridge, curl-up, squat) | Baseline, post-intervention (12 weeks) | Exercise group showed significant improvements in pain (–62.5%), disability (–61.3%), HRQOL (physical function, vitality, physical component scale), and physical fitness tests (balance, endurance, squat, core strength) compared to control (p < 0.05 to < 0.01). |
| 15 | Cruz-Díaz et al., 2017 [36] |
Spain / Physiotherapy rehabilitation program | 98 adults with chronic non-specific low back pain; randomized into 3 groups: Mat Pilates (PMG), Equipment-based Pilates (PAG), or Control group (CG); mean age not specified | Mat Pilates (PMG): 12-week program of mat-based Pilates exercises. Equipment Pilates (PAG): 12-week program using Pilates apparatus providing feedback and resistance. Both: supervised, 2–3x/week | Control group: no structured Pilates intervention | Pain, disability, kinesiophobia, TrA activation | Roland-Morris Disability Questionnaire (RMDQ), Visual Analogue Scale (VAS), Tampa Scale of Kinesiophobia (TSK), real-time ultrasound (TrA activation) | Baseline, 6 weeks, 12 weeks | Both Pilates groups improved significantly in pain, disability, TrA activation, and kinesiophobia (p < 0.001). Equipment-based Pilates showed faster improvements than mat Pilates (p = 0.007), suggesting apparatus feedback enhanced engagement with Pilates principles. |
| 16 | Cruz-Díaz et al., 2016 [37] |
Spain / Physiotherapy rehabilitation clinics | 101 postmenopausal women with chronic low back pain; randomized into Pilates + PT group (PPT) vs PT-only group; retention not fully reported | Clinical Pilates + Physical Therapy (PPT): 6-week program combining Pilates-based supervised exercise with standard PT | Physical Therapy (PT) alone: conventional physiotherapy without Pilates | Pain, disability | Visual Analogue Scale (VAS), Oswestry Disability Index (ODI) | Baseline, 6 weeks, 1-year follow-up | After 6 weeks, PPT group showed significant reductions in pain and disability compared to PT alone (effect sizes: pain d = 3.14, disability d = 2.33). At 1-year follow-up, improvements persisted in the PPT group (d = 2.49 for pain, d = 4.98 for disability), whereas PT-only group returned to baseline levels. |
| 17 | Cruz-Díaz et al., 2018 [38] |
Spain / University laboratory | 64 adults with chronic non-specific low back pain; randomized to Pilates group (n = 32) or control (n = 32); mean age not specified | Pilates intervention: supervised exercise program, 12 weeks, focusing on lumbo-pelvic stability, posture, and core control | Control group: no treatment | Disability, pain, kinesiophobia | Roland-Morris Disability Questionnaire (RMDQ), Visual Analogue Scale (VAS), Tampa Scale of Kinesiophobia (TSK) | Baseline, 6 weeks, 12 weeks | Pilates group showed significant improvements in disability, pain, and kinesiophobia compared to control (p < 0.001). Largest changes in disability and kinesiophobia were seen at 6 weeks, with continued pain improvement at 12 weeks. Mean between-group differences: RMDQ = 4.0, TSK = 5.5, VAS = 2.4. |
| 18 | Day et al., 2024 [39] |
USA / Telehealth (videoconference delivery) | 302 adults with chronic low back pain; randomized to Cognitive Therapy (CT), Mindfulness Meditation (MM), or Behavioral Activation (BA); balanced gender; retention high (exact % not in abstract) | CT, BA, or MM: all delivered in groups via videoconference; focused on pain coping, mindfulness skills, or activity engagement; program duration not detailed in abstract; follow-up to 6 months | No inert/sham control; comparison between 3 active treatment arms | Pain interference (primary), secondary outcomes (pain intensity, function, sleep disturbance, mental health) | Standardized scales (pain interference scores, sleep disturbance questionnaires, functional and mental health measures) | Pre- to post-treatment, 3 months, 6 months | All three interventions (CT, BA, MM) produced medium-to-large reductions in pain interference (ds –0.71 to –1.00), maintained at 3 and 6 months. Secondary outcomes improved with small-to-medium effects. No significant differences between groups, except BA showed greater improvement in sleep disturbance vs MM (d = –0.49). |
| 19 | de Lira et al., 2025 [40] |
Brazil / Primary care public health service | 152 adults with non-specific chronic low back pain; randomized to CFT (n=76) or sham (n=76); >97% follow-up retention | Cognitive Functional Therapy (CFT): 6 individualized one-hour sessions; tailored approach combining pain reconceptualization, lifestyle advice, movement retraining, and self-management strategies | Sham control: 6 sessions of neutral talking + detuned photobiomodulation (placebo laser); both groups also received a CLBP education booklet | Pain intensity, disability | Numerical Rating Scale (pain), disability index (tool not specified in abstract, likely ODI or RMDQ) | Baseline, 6 weeks, 3 months, 6 months | CFT group showed greater reductions in pain (MD = –1.8; 95% CI –2.5 to –1.1) and disability (MD = –9.9; 95% CI –13.2 to –6.5) compared with sham at 6 weeks. Improvements were sustained at 3- and 6-month follow-up. |
| 20 | Elabd & Elabd, 2024 [41] |
Egypt / University hospital physiotherapy clinic | 50 young adults with chronic mechanical low back pain; 22 males, 28 females; randomized equally into 2 groups; 8-week program | Experimental group: conventional physiotherapy (infrared, ultrasound, burst TENS, exercise) + aerobic training (stationary bicycle) | Control group: conventional physiotherapy only (infrared, ultrasound, burst TENS, exercise) | Pain intensity, disability, endurance, physical performance | Visual Analogue Scale (VAS), Oswestry Disability Index (ODI), Sorensen test (back extensor endurance), Back Performance Scale, 6-Minute Walk Test (6MWT) | Baseline, post-intervention (8 weeks) | Both groups improved significantly in pain and function (p < 0.001). Experimental group showed greater improvements in disability (p = 0.043), extensor endurance (p = 0.023), and 6MWT performance (p = 0.023). No significant group-by-time differences for pain intensity or Back Performance Scale. |
| 21 | Feng et al., 2025 [42] |
China / Telemedicine (mobile health apps) | 78 adults with chronic low back pain; randomized 1:1 into experimental (n=39) and control (n=39); mean age not reported | Telemedicine-supported structured exercise program: 8 weeks, delivered via mHealth apps; included patient education, health coaching, and structured exercise | Usual care therapy: education + paper handouts describing home exercises | Disability, pain intensity, mental health, quality of life, walking ability, adherence | Roland Morris Disability Questionnaire (RMDQ), Numerical Rating Scale (NRS), DASS-21, SF-12, Timed Up and Go (TUG), Exercise Adherence Rating Scale (EARS) | Baseline, 4 weeks (mid-treatment), 8 weeks (post-treatment) | Telemedicine group had greater improvements in disability (MD = –3.96), pain (MD = –1.69), and physical QoL (MD = +4.5) compared to control (p < 0.01). Within-group improvements were also observed for mental health, walking ability, and QoL mental component, though between-group differences were not significant. |
| 22 | Ford et al., 2016 [43] |
Australia / 16 primary care physiotherapy practices (multicentre) | 300 adults with low back disorders persisting ≥6 weeks to ≤6 months; randomized to individualised PT (n=156) vs advice (n=144) | Individualised physiotherapy + guideline-based advice: 10 sessions; tailored treatment addressing pathoanatomical, psychosocial, and neurophysiological barriers to recovery | Guideline-based advice alone: 2 physiotherapist-delivered sessions | Disability, back pain, leg pain | Oswestry Disability Index (ODI), Numerical Rating Scale (NRS) for back and leg pain | 5, 10, 26, and 52 weeks | Individualised physiotherapy significantly improved ODI at 10 weeks (4.7 points), 26 weeks (5.4), and 52 weeks (4.3) compared to advice. Back and leg pain also improved more in the intervention at 10 and 26 weeks. At 12 months, intervention group more likely to achieve ≥50% improvement in ODI (RR 1.5) and pain (RR 1.3). |
| 23 | Freiwald et al., 2018 [44] |
Germany / Multimodal rehabilitation program | 176 adults with chronic low back pain; enrolled in individualized multimodal treatment program; randomized to multimodal treatment with or without heat wraps | Multimodal therapy + supplemental heat therapy (thermotherapy): daily application of heat wrap for several hours in addition to standard multimodal treatment | Multimodal therapy alone (exercise, education, and other guideline-based components) | Trunk strength, flexibility, range of motion | Biomechanical testing of trunk flexion, extension, lateral flexion, and rotation | Baseline, post-intervention (12 weeks) | Both groups improved significantly in strength and range of motion. Heat therapy group showed additional improvements in trunk strength (extension and rotation), though differences were modest and not statistically strong (p ~ 0.08–0.09). No significant differences in flexibility. |
| 24 | Ghavipanje et al., 2022 [45] |
Iran / Clinical rehabilitation setting | 40 obese postpartum women with low back pain; mean age 29.3 ± 3.8 years; BMI ~32; randomized equally to DNS (n=20) or General Exercise (n=20); all completed 6 weeks | Dynamic Neuromuscular Stabilization (DNS): 6 sessions/week for 6 weeks; exercises based on developmental kinesiology patterns to restore posture, breathing, and core control | General Exercise (GE): 6 sessions/week for 6 weeks; conventional exercises not based on DNS principles | Pain, disability, fear-avoidance, respiratory function | Numeric Pain Rating Scale (NPRS), Modified Oswestry Disability Questionnaire (MODQ), Fear-Avoidance Beliefs Questionnaire (FABQ), Breath Hold Time (BHT), Respiratory Rate (RR), Global Rating of Change (GROC) | Baseline, post-intervention (6 weeks) | Both groups improved, but DNS group showed significantly greater improvements across all measures, including pain, disability, FABQ, respiratory control, and GROC scores (p < .05). |
| 25 | Glombiewski et al., 2018 [46] |
Germany / Outpatient psychological setting | 88 participants with chronic low back pain (≥3 months) and high fear-avoidance; 55% women; randomized to three groups | Exposure therapy: tailored, fear-focused; delivered in short (10 sessions) or long versions; focused on reducing pain-related anxiety & fear-avoidance | Cognitive Behavioral Therapy (CBT): active comparator focusing on coping strategies and cognitive restructuring | Disability, pain intensity, pain-related anxiety, psychological flexibility, coping, depression | Quebec Back Pain Disability Scale (QBPDS), Pain Disability Index (PDI), average pain NRS, FABQ, coping and depression scales | Pre-treatment, mid-treatment, post-treatment, 6-month follow-up | Exposure > CBT for reducing movement-related disability (QBPDS) and improving psychological flexibility. No difference in pain intensity or disability (PDI). CBT outperformed Exposure in coping strategies. Shorter Exposure was more effective than longer version for speed of improvement. More dropouts in Exposure groups. |
| 26 | Godfrey et al., 2020 [47] |
UK / Four public hospital physiotherapy clinics | 248 adults with chronic low back pain (≥12 weeks, mean duration ~3 years); mean age 48; 59% female | PACT (Physical Therapy informed by ACT): standard physiotherapy integrated with Acceptance and Commitment Therapy strategies; delivered by trained physiotherapists; fidelity ≥80% | Usual care physiotherapy without ACT elements | Disability (primary), physical function, health-related quality of life, treatment credibility | Roland Morris Disability Questionnaire (RMDQ), Patient Specific Functioning, SF-12, Treatment Credibility Scale | Baseline, 3 months, 12 months | PACT group improved more at 3 months for disability (mean diff RMDQ = -1.07, p = .037), functioning (p = .008), SF-12 physical health (p = .032), and credibility (p < .001). No between-group differences at 12 months. PACT was feasible, acceptable, and delivered with high fidelity. |
| 27 | Grande-Alonso et al., 2019 [48] |
Spain / Outpatient physiotherapy setting | 50 adults with nonspecific chronic low back pain; randomized equally; mean age not reported; mixed gender | Biobehavioral therapy + Orthopedic Manual Therapy (OMT): 8 sessions, 2/week; combined education, exercise, behavioral strategies with OMT techniques | Biobehavioral therapy alone: identical dose/frequency without OMT | Pain intensity, pain frequency, somatosensory, physical and psychological variables | Numeric Pain Rating Scale (NPRS), psychological/functional assessments | Baseline, 1 month, 3 months | Both groups improved significantly across all variables (pain, function, psychological outcomes) with large effect sizes (>0.80). No significant differences between groups, suggesting that OMT did not add extra benefit beyond the biobehavioral approach. |
| 28 | Gwon et al., 2020 [49] |
South Korea / Physiotherapy clinical setting | 30 adults with chronic low back pain; randomized into experimental group (n=15) and control group (n=15) | Experimental group (EG): Side-lying bridge exercise on a sling system + Neurac vibration | Control group (CG): Same side-lying bridge exercise on sling without vibration | Pain, asymmetry of weight distribution, asymmetry of hip abductor strength (AHAS), static balance (one-leg stance) | Visual Analog Scale (VAS) for pain; weight distribution & hip abductor strength asymmetry indices; static balance measures | Baseline, post-intervention | EG showed significant improvements in all outcomes (pain, AHAS, weight distribution, balance, p < 0.05). CG improved only in pain and AHAS. Pain reduction had the largest effect size (d=0.77, moderate effect). Neurac vibration enhanced exercise effectiveness. |
| 29 | Halliday et al., 2019 [50] |
Australia / Secondary public health facility, Sydney | 70 adults with chronic low back pain (>3 months) and directional preference; randomized equally | McKenzie Method (MDT): 12 supervised sessions over 8 weeks, focusing on repeated movement testing and patient self-management strategies | Motor Control Exercises (MCE): 12 supervised sessions over 8 weeks, focusing on deep trunk muscle activation and control | Primary: Trunk muscle thickness (TrA, obliquus internus, obliquus externus). Secondary: Pain, function, perceived recovery | Ultrasound imaging for muscle thickness; pain scales; functional questionnaires | Baseline, 8 weeks (post-intervention), 1 year (follow-up) | No significant differences between groups at 1-year for muscle thickness, pain, function, or recovery. Both interventions demonstrated similar long-term effects, indicating that MDT and MCE are equally effective for this subgroup of CLBP patients with directional preference. |
| 30 | Hernandez-Lucas et al., 2023 [51] |
Spain / Clinical and community setting | 40 adults with non-specific low back pain; randomized into experimental and control groups | Back School program (8 weeks): 14 practical sessions (strengthening + flexibility exercises) + 2 theoretical sessions (anatomy, lifestyle education) | Control group: maintained usual lifestyle (no structured program) | Pain, disability, quality of life, kinesiophobia | Visual Analogue Scale (VAS), Roland-Morris Disability Questionnaire (RMDQ), Short Form-36 (SF-36), Tampa Scale of Kinesiophobia (TSK) | Baseline, post-intervention (8 weeks) | Experimental group showed significant improvements in pain, disability, physical QoL (SF-36), and kinesiophobia (p < 0.05). No significant changes in psychosocial QoL. Control group showed no significant improvements. |
| 31 | Hohmann et al., 2018 [52] |
Germany / Outpatient clinical setting | 44 adults with chronic low back pain (≥3 months); randomized to leech therapy (n=25) or exercise therapy (n=19) | Leech therapy: single local application of 4–7 leeches | Exercise therapy: 4 weekly sessions (1 hour each) led by physiotherapist | Pain intensity (primary); physical impairment, function, QoL, pain perception, depression, analgesic use (secondary) | Visual Analogue Scale (VAS), Roland-Morris Disability Questionnaire (RMDQ), Hannover Functional Ability Questionnaire, SF-36, SES, CES-D, analgesic diary | Baseline, 28 days, 56 days | Leech therapy group showed significantly greater pain reduction (VAS: -25.2 points vs control, p = 0.0018), and better functional and QoL outcomes at 4 and 8 weeks. No significant effect of patient expectations. Limitations: small sample, unblinded design, short follow-up. |
| 32 | Kamali et al., 2018 [53] |
Iran / Sports rehabilitation setting | 42 athletes (21 male, 21 female) with chronic non-specific LBP; randomized equally | Spinal Manipulation (SM) + Kinesio Taping (KT): applied during treatment | Spinal Manipulation (SM) only: identical frequency without KT | Pain, functional disability, trunk flexor–extensor endurance | Numerical Rating Scale (NRS), Oswestry Disability Index (ODI), McQuade test, Unsupported trunk holding test | Baseline, immediately post, 1 day, 1 week, 1 month | Both groups showed significant improvements in pain, disability, and endurance over time (p < 0.05). No significant between-group differences at any time point. Adding KT to SM did not confer extra benefit. |
| 33 | Khan et al., 2024 [54] |
Pakistan / Outpatient physiotherapy setting | Adults with chronic nonspecific low back pain (n not specified; both genders) N=114; randomized to SMT+DN or SMT alone |
Experimental group: Spinal Manipulative Therapy (SMT) + Dry Needling (DN); delivered over 8 weeks | Control group: SMT alone, identical duration/frequency | Functional disability, endurance | Roland-Morris Disability Questionnaire (RMDQ), endurance tests | Baseline, 8 weeks | Both groups improved significantly in disability and endurance. SMT+DN group showed greater reductions in RMDQ scores (mean diff baseline–8 weeks: -2.75, p = .003) and larger endurance gains compared to SMT alone. |
| 34 | Kim & Park, 2021 [55] |
South Korea / Community setting | 51 elderly participants with chronic low back pain; randomized to experimental (n=26) and placebo (n=25) | Auricular acupressure (AA): applied to LBP-related ear points; 6 weeks, weekly cycles | Placebo AA: applied to unrelated ear points, identical schedule | Pain intensity, pain threshold, disability | Visual Analogue Scale (VAS), Pain threshold test, Oswestry Disability Index (ODI) | Baseline, post-intervention (6 weeks) | Experimental group showed significant improvements in pain (VAS, p < .001), pain threshold (p < .001), and disability (ODI, p < .001) compared to placebo. Suggests AA is a safe, effective, noninvasive alternative for CLBP in elders. |
| 35 | Kim et al., 2020 [56] |
South Korea / Community & university campus | 48 adults with chronic low back pain; randomized equally to SHR (n=24) and stabilization (STB) (n=24) | Simulated Horseback Riding (SHR): seated exercise mimicking horseback riding motion; 30 min, 2x/week for 8 weeks | Stabilization (STB): conventional trunk stabilization exercises; identical schedule | Pain, disability, fear-avoidance | Numeric Rating Scale (NRS), Oswestry Disability Index (ODI), Roland-Morris Disability Questionnaire (RMDQ), Fear-Avoidance Beliefs Questionnaire (FABQ) | Baseline, 4 weeks, 8 weeks, 6 months | Both SHR and STB improved pain and disability significantly within groups. Between groups: SHR reduced FABQ-work more effectively (p = .01), while other outcomes (NRS, ODI, RMDQ, FABQ-physical) showed no significant differences. SHR uniquely sustained long-term fear-avoidance improvements at 6 months. |
| 36 | Kong et al., 2020 [57] |
USA / Stanford University, single-center | 121 adults with chronic low back pain (≥6 months, pain ≥4/10, no radiculopathy); randomized: real EA (n=59), sham EA (n=62) | Real Electroacupuncture (EA): 12 sessions, 2x/week for 6 weeks | Sham EA: identical procedure but with placebo stimulation | Pain intensity (primary), disability (secondary), psychosocial/demographic moderators | PROMIS Pain Intensity T-scores, Roland-Morris Disability Questionnaire (RMDQ), psychophysical testing (e.g., temporal summation, CPM), coping, self-efficacy, catastrophizing | Baseline, 2 weeks post-treatment | No significant difference in primary outcome (PROMIS pain intensity) between groups (p=0.06). Significant improvement in disability (RMDQ) for EA vs sham (mean diff = -2.11, p=0.01). Coping skills predicted better outcomes; White participants had poorer responses than non-White. |
| 37 | Kuvačić et al., 2018 [58] |
Croatia / Clinical setting | 30 adults with chronic low back pain (mean age 34.2 ± 4.5 yrs); randomized equally to yoga group (n=15) and pamphlet group (n=15) | Yoga + education: 8-week program, 2x/week; included yoga postures plus education on spine anatomy/biomechanics and CLBP management | Pamphlet group: received informational pamphlet only (usual advice) | Disability, depression, anxiety, pain | Oswestry Disability Index (ODI-I), Zung Self-Rating Depression Scale (SDS), Zung Self-Rating Anxiety Scale (SAS), Numeric Rating Scale (NRS) | Baseline, post-intervention (8 weeks) | Yoga + education group showed significant improvements in depression, anxiety, and pain (p < 0.05) compared to pamphlet. Both groups improved in disability, but no significant between-group difference in ODI. |
| 38 | Lang et al., 2021 [59] |
Australia / Community setting | 174 adults with chronic low back pain; randomized 2:1 to walking group (WG) and standardized care (SG); 138 (79%) completed at 12 weeks; 96 (55%) at 12 months | Walking group (WG): 12-week pedometer-driven, physiotherapist-guided program; individualized weekly step targets negotiated with participants | Standardized care group (SG): education + advice package (self-management, stay active, benefits of PA) | Disability (primary), pain, physical activity, beliefs, QoL, self-efficacy | Oswestry Disability Index (ODI), Numeric Pain Rating Scale (NRS), IPAQ, FABQ, Back Beliefs Questionnaire (BBQ), PA Self-efficacy, EQ-5D-5L | Baseline, 12 weeks, 6 months, 12 months | No significant group differences for ODI or secondary outcomes at any time point. Subgroup analyses: participants with moderate disability (ODI ≥21) and those with low baseline step counts (<7500/day) showed greater ODI improvements in the walking group. Suggests walking may benefit subgroups rather than all CLBP patients. |
| 39 | Lee & Kim, 2025 [60] |
South Korea / Community setting | 152 older women aged ≥65 years with CLBP >1 year (Experimental: n=68; Control: n=84). Mean age 70.1 ± 1.5 (exp) vs 71.1 ± 1.0 (ctrl); mean CLBP duration 8.7 years | Aquarobics group: 60-min aquatic aerobics sessions, twice per week, for 12 weeks | Control group: sedentary lifestyle, no structured exercise | Pain/disability, sleep disturbance, subjective memory impairment | Back Pain Disability Index, standardized sleep disturbance scale, subjective memory impairment questionnaire; SEM for mediating effects | Baseline and post-12 weeks | Significant improvements in the aquarobics group vs control: pain disability ↓ (MD = -7.6, 95% CI: -10.5 to -4.9, p<.001), sleep disturbance ↓ (MD = -4.2, 95% CI: -6.8 to -1.5, p<.001), memory impairment ↓ (MD = -3.9, 95% CI: -6.1 to -1.7, p<.001). SEM showed pain reduction mediated improvements in sleep and memory outcomes. Concluded aquarobic exercise is effective for both physical and cognitive enhancement in older women with CLBP. |
| 40 | Li, Y., et al., 2025 [61] |
China / University rehabilitation setting | 18 patients with chronic non-specific LBP | Core training + breathing exercises for 12 weeks | Core training only; Control (no exercise) | Pain, disability, muscle strength | VAS (pain), ODI (disability), muscle strength test | Baseline and post 12-week intervention | Combined core + breathing group showed significantly greater reduction in pain, improved functional outcomes, and enhanced muscle strength compared to core-only and control. |
| 41 | Luo, Y., et al., 2019 [62] |
China / General Hospital of Western Theater Command | 152 adults with chronic LBP | Hand-ear acupuncture (18 sessions over 7 weeks) | Standard acupuncture; Usual care | Pain, disability, overall efficacy | Visual Analogue Scale (VAS), Roland-Morris Disability Questionnaire (RMDQ), TCM Symptom Curative Effect Standard | Baseline, 2 months, 6 months | Hand-ear acupuncture showed significant improvement in VAS and RMDQ compared to standard acupuncture and usual care. At 6 months, RMDQ improved by 7.74 points in the hand-ear acupuncture group. Overall efficacy was 88.9% vs 45.8% in usual care. |
| 42 | Song & Yim, 2025 [63] |
South Korea / Exercise center, Seongnam City | 40 women with CLBP | Self-myofascial release (SMR) + DNS (20 min SMR + 30 min DNS, 2x/week, 6 weeks) | DNS alone (30 min, 2x/week, 6 weeks) | Pain, static & dynamic balance, muscle endurance, flexibility, muscle tone/stiffness, disability, autonomic regulation | VAS, Functional Reach Test (FRT), Y-Balance Test, Supine Bridge, Sit-and-Reach, Myoton PRO, ODI (Korean version), SDNN (HRV) | Baseline, post-intervention (6 weeks) | Both groups improved in all outcomes (p<0.05). Experimental group achieved significantly greater improvements in pain, balance, flexibility, endurance, muscle tone, ODI, and SDNN. Integration of SMR with DNS yielded superior clinical and autonomic benefits. |
| 43 | Yalfani et al., 2022 [64] |
Iran / Elderly care & rehabilitation setting | 25 elderly women (65–75 yrs) with CLBP | Virtual Reality Training (VRT) using Xbox Kinect, 30 min, 3x/week for 8 weeks | Control group (no VR training, usual lifestyle) | Pain intensity, fall risk, quality of life | VAS, Biodex Balance System, SF-36 | Baseline, post-intervention (8 weeks) | VRT group showed significant improvements: ↓ pain intensity (p=0.001), ↓ fall risk (p=0.001), ↑ QoL (p=0.001). Virtual reality provided enhanced exercise engagement and therapeutic benefit. |
CON: control groups; INT: intervention groups; LLMC: low-load motor control training plus education; HLLE: high-load lifting exercise plus education; VR+PT: virtual reality combined with physiotherapy; PT: physiotherapy; FM: Feldenkrais Method; CSE: core stability exercise; IMT: inspiratory muscle training; SC: sham control; SSE-2x / SSE-4x: stabilization exercise delivered at two versus four weekly sessions; HEP: home exercise program; SWT: shockwave therapy; PA+Ed: physical activity plus education; SE+CBT: stabilization exercise with cognitive behavioral therapy; SE: stabilization exercise; BGA: behavioral graded activity; CET: conventional exercise therapy; SMT+Ex: spinal manipulative therapy plus exercise; Ex: exercise only; CSP: core strengthening program; UC: usual care; MBSR: mindfulness-based stress reduction; CBT: cognitive behavioral therapy; MA: manual acupuncture; EA: electroacupuncture; Sham: sham acupuncture/electroacupuncture; FRT: functional resistance training; CP+PT: clinical Pilates plus physiotherapy; CP: clinical Pilates; VR-Ex: virtual reality–based exercise; CFT: cognitive functional therapy; Sham+Ed: sham intervention plus education; AT+PT: aerobic training plus physiotherapy; Tele-Ex: telemedicine-supported exercise; FBT: functional balance training; MMR+TT: multimodal rehabilitation with thermotherapy; MMR: multimodal rehabilitation alone; SMT: spinal manipulative therapy; Sham SMT: sham spinal manipulative therapy; CBT+PT: cognitive behavioral therapy plus physiotherapy; PACT: physiotherapy informed by acceptance and commitment therapy; UC-PT: usual physiotherapy care; CT+MT: cognitive therapy plus manual therapy; MT: manual therapy; SLB+Neurac: side-lying bridge with Neurac vibration; SLB: side-lying bridge exercise; MDT: McKenzie method; MCE: motor control exercises; Back School: structured back school education and exercise program; SMT+KT: spinal manipulation with kinesio taping; SMT+DN: spinal manipulation plus dry needling; SHR: simulated horseback riding; STB: trunk stabilization exercise; AA: auricular acupressure; Sham AA: sham auricular acupressure; Yoga-Ed: yoga plus education; Pamphlet/EC: education-only control (pamphlet or sedentary advice); rTMS+Sling: repetitive transcranial magnetic stimulation with sling exercise; Sling: sling exercise; Core+Breath: core training combined with breathing exercises; Core: core training only; HEA: hand-ear acupuncture; Sham HEA: sham hand-ear acupuncture; SMR+DNS: self-myofascial release with dynamic neuromuscular stabilization; DNS: dynamic neuromuscular stabilization; Aqua: aquarobics / aquatic exercise.
Table 1.
Quality Appraisal /Risks of Bias of Included studies (PEDro Tool).
| STUDY | SOURCES/POTENTIAL SOURCES OF BIASA | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Name | Eligibil ity Criteri a | Rando m Allocati on | Concealed Allocation | Baseline Similari ty | Bindin g Of Sub- Jects |
Blinding Of thera- pists | Blinding Of Accessor s | Measures Of key Outcomes From 85% of the initially allocated | Intenti on To treat/1 00% partici pation |
Betwee n Group | Point measure & variabiles | Grade Quality ROB | Level of Evidence |
| Aasa et al., 2015 [22] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
8 High Quality Low RoB |
Level I |
| Afzal et al., 2022 [23] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level I |
| Ahmadi et al., 2020 [24] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
8 High Quality Low RoB |
Level I |
| Ahmadnezhad et al., 2020 [25] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level II |
| Akbaş et al., 2025 [26] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
7 High Quality Low RoB |
Level I |
| Back et al., 2024 [27] |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
10 High Quality Low RoB |
Level I |
| Bagg et al., 2022 [28] |
Yes |
Yes |
Yes |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
9 High Quality Low RoB |
Level I |
| Bagheri et al., 2020 [29] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level II |
| Bello et al., 2015 [30] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
No |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Blanco-Giménez et al., 2024 [31] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
8 High Quality Low RoB |
Level I |
| Brandt et al., 2015 [32] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
No |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Chen et al., 2023 [33] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
8 High Quality Low RoB |
Level I |
| Comachio et al., 2020 [34] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
8 High Quality Low RoB |
Level I |
| Cortell-Tormo et al., 2018 [35] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level II |
| Cruz-Díaz et al., 2017 [36] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Cruz-Díaz et al., 2016 [37] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Cruz-Díaz et al., 2018 [38] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
7 High Quality Low RoB |
Level I |
| Day et al., 2024 [39] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
7 High Quality Low RoB |
Level I |
| de Lira et al., 2025 [40] |
Yes |
Yes |
Yes |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
9 High Quality Low RoB |
Level I |
| Elabd & Elabd, 2024 [41] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level I |
| Feng et al., 2025 [42] |
Yes |
Yes |
Yes |
Yes |
No |
No |
No |
Yes |
Yes |
Yes |
Yes |
7 High Quality Low RoB |
Level I |
| Ford et al., 2016 [43] |
Yes |
Yes |
Yes |
Yes |
No |
No |
No |
Yes |
Yes |
Yes |
Yes |
7 High Quality Low RoB |
Level I |
| Freiwald et al., 2018 [44] |
Yes |
Yes |
Yes |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level I |
| Ghavipanje et al., 2022 [45] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Glombiewski et al., 2018 [46] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Godfrey et al., 2020 [47] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
8 High Quality Low RoB |
Level I |
| Grande-Alonso et al., 2019 [48] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
Yes |
Yes |
Yes |
6 High Quality Low RoB |
Level I |
| Gwon et al., 2020 [49] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
7 High Quality Low RoB |
Level II |
| Halliday et al., 2019 [50] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
No |
Yes |
Yes |
Yes |
7 High Quality Low RoB |
Level I |
| Hernandez-Lucas et al., 2023 [51] |
Yes |
Yes |
Yes |
Yes |
No |
No |
No |
Yes |
Yes |
Yes |
Yes |
7 High Quality Low RoB |
Level II |
| Hohmann et al., 2018 [52] |
Yes |
Yes |
Yes |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
9 High Quality Low RoB |
Level II |
| Kamali et al., 2018 [53] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Khan et al., 2024 [54] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level I |
| Kim & Park, 2021 [55] |
Yes |
Yes |
No |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
No |
Yes |
7 High Quality Low RoB |
Level I |
| Kim et al., 2020 [56] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Kong et al., 2020 [57] |
Yes |
Yes |
Yes |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
9 High Quality Low RoB |
Level I |
| Kuvačić et al., 2018 [58] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level II |
| Lang et al., 2021 [59] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level I |
| Lee & Kim, 2025 [60] |
Yes |
Yes |
No |
Yes |
No |
No |
No |
Yes |
No |
Yes |
Yes |
5 Moderate Quality Some Concern RoB |
Level II |
| Li, Y., et al., 2025 [61] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level I |
| Luo, Y., et al., 2019 [62] |
Yes |
Yes |
No |
Yes |
Yes |
No |
Yes |
Yes |
No |
Yes |
Yes |
7 High Quality Low RoB |
Level II |
| Song & Yim, 2025 [63] |
Yes |
Yes |
Yes |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
7 High Quality Low RoB |
Level II |
| Yalfani et al., 2022 [64] |
Yes |
Yes |
No |
Yes |
No |
No |
Yes |
Yes |
No |
Yes |
Yes |
6 High Quality Low RoB |
Level II |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



