
Submitted:
15 January 2026
Posted:
19 January 2026
You are already at the latest version
Abstract
Objective. To evaluate the association between adherence to the Mediterranean Diet (MedDiet) and the risk of developing type 2 diabetes mellitus (T2D) in an urban Ecuadorian population, with emphasis on the protective effect of specific dietary components and body composition. Methods. A cross-sectional analytical study was conducted with 1,373 adults aged 18–75 years. Adherence to the MedDiet was assessed using the MEDAS-14 questionnaire, while the risk of developing T2D was estimated using the Finnish Diabetes Risk Scale (FINDRISC). Anthropometric and body composition parameters were measured using standardized procedures. Adjusted associations between exposure variables and T2D risk were estimated using Poisson regression with robust variance, calculating prevalence ratios and controlling for sociodemographic and lifestyle factors. Results. The majority of participants showed low adherence to the MedDiet (85.2%), which was significantly associated with the risk of T2D. Multivariate analysis of individual dietary components showed relevant associations. Regular consumption of sofrito was associated with a lower risk (PR=0.817; 95% CI: 0.682–0.979; p = 0.028). Similarly, low fruit consumption was associated with a substantially higher risk of T2D (PR = 1.350; 95% CI: 1.146–1.589; p = 0.001). In addition, higher body mass index (BMI) and waist circumference (WC) were consistently related to greater T2D risk. Conclusions. Adherence to the Med Diet and the consumption of key components such as sofrito and fruits are associated with a lower risk of developing T2D, highlighting the importance of preventive lifestyle interventions adapted to the Latin American context.
Keywords:
mediterranean diet
; type 2 diabetes
; adherence score
; protective factors
; sofrito sauce
1. Introduction
Type 2 diabetes is a chronic multifactorial disease characterized by elevated blood glucose levels, mainly due to insulin resistance and pancreatic β-cell dysfunction [1]. Its prevalence has risen sharply in recent decades, becoming a major public health challenge with profound implications for quality of life and healthcare systems [2]. According to the International Diabetes Federation (IDF), T2D is influenced by both non-modifiable factors, such as age and genetic predisposition, and modifiable factors, including overweight or obesity, physical inactivity and unhealthy dietary habits [3].
Among preventive strategies, diet plays a central role. The Mediterranean diet (MedDiet) has been widely studied and identified as a dietary pattern with significant health benefits [4,5], particularly in relation to T2D prevention and management [6,7,8]. Evidence indicates that the MedDiet supports glycemic control, reduces inflammation, improves insulin sensitivity, and promotes healthy weight [6,9,10,11]. This dietary model emphasizes high consumption of plant-based foods [legumes, nuts, whole grains, vegetables, fruits, with olive oil as the primary fat source]; includes moderate intake of fish and poultry; and limits red meat, ultra-processed foods, and refined sugars [12]. Conversely, frequent consumption of industrially baked goods and sugary foods has been associated with increased risk of developing T2D [13,14].
In Latin America, traditional dietary patterns also share protective features. These are characterized by higher consumption of whole grains, legumes, fruits, vegetables, and tubers, combined with relatively low levels of food processing [15]. In Ecuador, for example, the traditional Andean dietary pattern includes corn, quinoa, potatoes, sweet potatoes, cassava, beans, and local fruits, providing fiber, micronutrients, and low-glycemic carbohydrates. Such patterns have been associated with reduced prevalence of overweight and obesity, key mediators of the development of T2D [16]. However, these protective models are increasingly displaced by the increased consumption of ultra-processed foods rich in sugars and fats, reflecting the ongoing nutritional transition and its growing public health burden [17,18].
Within the MedDiet, certain components may have particularly relevant protective effects. Fruit consumption is consistently linked to reduced risk of T2D, especially when whole fruits are consumed rather than juices, which have a higher glycemic load and lower fiber content [19,20,21]. Sofrito sauce, a traditional Mediterranean preparation made by slowly cooking tomatoes, onions or leeks, garlic, and olive oil [22] enhances the bioavailability of carotenoids and polyphenols, compounds with antioxidant and anti-inflammatory properties [23]. Although direct evidence linking sofrito to the risk of developing T2D is lacking, its bioactive composition suggests a potential protective role in metabolic health. Avocados, while less central to the MedDiet, are rich in monounsaturated fatty acids and have been associated with improvements on lipid profile and insulin sensitivity, though evidence for their role in T2D prevention remains less robust remains less robust [24,25,26].
It is important to note that the MedDiet reflects not only specific foods but also the broader cultural, social, and environmental context of Mediterranean populations, including active lifestyles and relatively low psychosocial stress, which together contribute to its protective effects [27,28,29]. These determinants differ substantially from those in Latin America, where rapid urbanization, socioeconomic inequalities, and the rising availability of ultra-processed foods significantly shape the risk of T2D [30,31,32].
Given these contextual differences, assessing the applicability of the MedDiet in Ecuador requires both the evaluation of the overall adherence and the examination of specific dietary components with potential protective effects. The present study therefore aimed to evaluate adherence to MedDiet and its association with the risk of developing T2D in an urban Ecuadorian population, with particular focus on the role of fruit and sofrito consumption as potentially protective factors.
2. Materials and Methods
2.1. Desing
This study employed a cross-sectional, analytical, observational design to evaluate the risk of T2D in relation to MedDiet adherence and body composition parameters. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed to ensure methodological rigor and transparent reporting.
2.2. Population and Sample
The sample was drawn from an urban population of 214,855 individuals residing in Loja, Ecuador. The required sample size was calculated at 1,218 participants, assuming a 15% expected risk of developing T2D, 2% precision, and 95% confidence level. To account for an estimated 14% attrition rate, the final target sample was increased to 1,388 individuals. The sample size estimation was performed using Epidat version 3.1. Sampling procedure and eligibility: This study utilized a non-probability, convenience sampling approach. The selection was based on institutional access and voluntary participation. Eligible participants were employees of public or private institutions from various population sectors [academic, transportation, education, healthcare, or economics] and were affiliated with the National Social Security Institute (IESS), aged between 18 and 75 years. Invitations were disseminated through institutional human resources departments and public notices within IESS-affiliated institutions to recruit a diverse professional subset of the urban workforce. This method wase employed to leverage established professional networks and ensure feasibility (Figure 1).
2.3. Data Collection
Data were collected using the STEPwise 3.2 questionnaire, adapted for Ecuador by the Ministry of Public Health (MSP), the National Institute of Statistics and Censuses (INEC), and the Pan American Health Organization/World Health Organization (PAHO/WHO) [33]. Information was gathered on sociodemographic characteristics; tobacco use and alcohol consumption. Physical activity levels were assessed using the short version of the International Physical Activity Questionnaire (IPAQ) [34].
2.4. Anthropometric and Body Composition
Anthropometric and body composition measurements were obtained using standardized procedures and validated equipment. A multifrequency segmental analyzer (InBody 120) with a reported reliability of 98% was used to measure body weight (kg), BMI, body fat percentage, visceral fat, SMM, and waist-to-hip ratio (WHR) were obtained.
Height was measured to the nearest millimeter using a portable stadiometer (Seca 217), with participants standing upright in the Frankfurt horizontal plane. WC was measured at the level of the navel at the end of a normal expiration using a Cescorf measuring tape (+/- 1 mm resolution).
2.5. Adherence to the Mediterranean Diet
Adherence to the MedDiet was assessed exclusively through the 14-item Mediterranean Diet Adherence Screener (MEDAS-14), administered in person by trained observers who had been standardized in data collection techniques. The questionnaire evaluates nutritional intake across 14 core components, including vegetables, fruits, legumes, whole grains, nuts, and olive oil, with predefined serving-based cutoffs. No complementary dietary assessment instruments were used. MEDAS-14 is a validated instrument with a total score ranging from 0 to 14, with adherence categorized as low (<9 points) or high (≥9 points) [22].
2.6. Risk of Type 2 Diabetes Mellitus
The FINDRISC was employed to estimate participant’s 10-year risk of developing T2D. This tool integrates eight established risk factors including age, BMI, waist circumference, physical activity, family history of diabetes, history of impaired glycemia, antihypertensive medication use, and a single dietary item referring to daily fruit and vegetable consumption. The questionnaire was administered through standardized, observer-supervised interviews. FINDRISC has been extensively validated across European and non-European populations, including Latin America, showing moderate to good discriminative accuracy (AUC between 0.65 and 0.75) for identifying undiagnosed T2D and prediabetes [35,36,37]. Scores range from 0 to 26, with scores ≥12 points indicating moderate to high risk for T2D. The outcome variable in this study was those with a moderate or greater risk of developing T2D [38]. This cutoff was used to define the outcome variable in the analysis.
2.7. Ethical Approval
This study was approved by the Bioethics Committee of San Francisco General Hospital (approval code: 031). Written informed consent was obtained from all participants prior to inclusion. Participants were informed of their right to decline participation or withdraw at any time without penalty. Confidentiality was maintained throughout the study by anonymizing all collected data.
2.8. Analysis
Data was analyzed using SPSS version 26 and EPIDAT version 3.1. Normality and homoscedasticity of variables were verified prior to hypothesis testing. To ensure data integrity, only participants with complete information on the different instruments and key anthropometric/body composition measures were included in the final analysis. Individuals with missing data on these variables were excluded.
Descriptive statistics for categorical variables were presented as frequencies and percentages, and their associations were examined using the Chi-square test. Continuous variables were reported as means ± standard deviations (SD) or medians (interquartile range, IQR), as appropriate, and compared using the Student’s t-test for independent samples.
Regression Models for Type 2 Diabetes Risk:
Given the cross-sectional design and the nature of the outcome variable (prevalent risk of initial T2D), unadjusted PRs were calculated to examine the initial association between the risk of developing T2D and adherence to MedDiet. Subsequently, two distinct multivariate regression models were constructed, with dependent variable being the risk of T2D (FINDRISC ≥12).
Model 1 (dietary components): this model used a robust-variance Poison regression approach to estimate the adjusted Prevalence Ratios (aPRs) for the individual components of the MEDAS-14 questionnaire, controlling specifically for the other dietary criteria of the adherence score to isolate the independent effect of each item (e.g., sofrito consumption).
Model 2 (socio-demographic and body compositional factors): a separate model was executed, incorporating a wider range of sociodemographic and body composition variables to control for key confounding factors. This second model utilized logistic regression with the Hosmer-Lemeshow statistic used for assessing model fit. Covariables included were educational level, marital status, alcohol and tobacco consumption, BMI, body fat percentage, visceral fat, SMM, WC and WHR.
Model 3 (dietary components and associated risk factors): This model used a robust variance Poison regression approach to estimate the adjusted prevalence ratios (aPR) of the individual components of the MEDAS-14 questionnaire (stir-fry, fruits, and carbonated beverages), specifically controlling for variables such as age, sex, smoking, BMI, abdominal circumference, and muscle mass that were risk factors for models 1 and 2. To assess the possible presence of multicollinearity between the covariates, the variance inflation factor (IVF) was calculated, considering an IVF value > 5.
Model 4 (Mediterranean diet and associated risk factors): This model used a robust variance Poison regression approach to estimate adjusted prevalence ratios (aPR) MEDAS-14 questionnaire, specifically controlling for variables such as age, sex, smoking, BMI, abdominal circumference, and muscle mass that were risk factors for models 1 and 2. To assess the possible presence of multicollinearity between the covariates, the IVF was calculated, considering an IVF value > 5.
Multicollinearity assessment:
Before the construction of the multivariate models, the presence of multicollinearity among the explanatory variables was rigorously evaluated. Bivariate correlations between all predictors were calculated, and the VIF was estimated for each variable. Following expert criteria, variables exhibiting VIF>5 were excluded from the final adjusted models to ensure stability, reliability, and independent interpretability of the estimated ratios.
3. Results
The baseline characteristics of the study participants, stratified by adherence to the MedDiet, are summarized in Table 1. Of the total cohort (n=1,373), a majority (85.8%) exhibited low MedDiet adherence. Individuals with high adherence to the MedDiet were significantly differentiated from those with low adherence across several socio-demographic and lifestyle factors. High adherers were on average, older (43.56 vs 40.27 years; p<0.001), more frequently female (69.7%; p=0.003) and demonstrated higher educational attainment, predominantly at the undergraduate and postgraduate levels (p=0.002). Regarding lifestyle characteristics, high adherence was associated with a significantly lower prevalence of smoking (8.7% vs 14.7%; p=0.025). While alcohol consumption was lower among high adherers (50.3% vs 53.3%; p=0.429), this difference was not statistically significant.
Tables S1 and S2 delineate the distribution of diabetes risk score, physical activity level, and body composition measures stratified by adherence status to the MedDiet, for male and female participants. While a consistent, non–significant trend emerged across both sexes, where lower Med Diet adherence correlated with and elevated T2D risk score and a less favorable anthropometric profile, a statistically significant association was detected exclusively among women, whose physical activity levels were significantly related to MedDiet adherence (p<0.05). The comprehensive set of these stratified findings is provided in Supplementary Material 1 (S1).
Analysis of individual components of the MedDiet showed that only sofrito was associated with a significant reduction in the risk of T2D (PR=0.802; 95%IC: 0.671-0.959; p=0.016). Whereas, in the adjusted Poisson model, with a prior diagnosis of multicollinearity and adjustment tests, it was obtained that participants who consumed sofrito had an 18.3% lower risk of developing T2D compared to those who did not (PR=0.817; 95%CI: 0.682–0.979; p=0.028). In contrast, those who consumed carbonated or sugary beverages had a 25% higher risk of T2D compared to non-consumers (PR=1.247; 95%IC: 1.002–1.552; p=0.048). Other components of the MedDiet, such as fruits, olive oil, and fish, showed a protective trend; however, these associations did not reach statistical significance (Table 2).
In Table 3, for men, when analyzing the anthropometric and body composition measures (unadjusted OR), it is observed that factors such as high BMI (OR=1.481; 95%IC: 1.373-1.596; p <0.001), a high WC (OR= 1.167; 95%IC: 1.133-1.201; p<0.001) and less SMM (OR=1.088; 95%IC: 1.041-1.137; p<0.011) were associated with a higher probability of risk of type 2 diabetes. While in the adjusted regression model, prior to multicollinearity tests (VIF > 5) where variables such as body fat percentage, fat mass and WHR were removed. The results obtained showed that each increase in BMI is associated with a 24% higher risk of T2D (OR= 1.241; 95%IC: 1.105-1.393; p<0.001). In addition, an increase in WC implies an 11% greater risk of T2D (OR=1.11; 95%IC: 1.063-1.162; p<0.001). On the other hand, greater muscle mass is associated with an 8% lower risk of T2D (OR=0.914; 95%IC: 0.861-0.971; p<0.001).
In Table 4 for women, in the anthropometric and body composition [unadjusted OR], it is observed that factors such as high BMI (OR: 1.328 (95%IC: 1.265-1.394)), p<0.001), and high WC (OR: 1.137 (95%IC: 1.114-1.161)), p <0.001) are associated with the risk of T2D. While in the adjusted regression model, prior to multicollinearity tests (VIF >5) where variables such as body fat percentage, fat mass and waist-to-hip ratio were removed, the results obtained reflect that for each increase in BMI it is associated with a 13% higher risk of T2D (OR: 1.132 (95%IC: 1.056-1.213), p<0.001). Furthermore, an increase in WC implies a 9% higher risk of T2D [OR: 1.094 (95%IC: 1.062-1.127), p <0.001). On the other hand, greater muscle mass is associated with a 7% lower risk of T2D (OR: 0.928 (95%IC: 0.873-0.987), p <0.001).
In Table 5, when analyzing anthropometric and sociodemographic factors, and components of the MedDiet (adjusted prevalence ratios, PR), it was observed that being male was associated with a 35.4% lower probability of developing T2D, while not smoking was associated with a 32.5% lower probability of T2D. On the other hand, a high BMI was associated with a 5.7% increase in the risk of T2D, and a higher waist circumference was associated with a 2.6% higher probability of developing the disease. In addition, each additional year of age was associated with a 3.6% increase in the risk of T2D. Regarding eating habits, non-preparation of sofrito at meals was associated with a 15.4% higher risk of T2D (PR: 1.154; 95% CI: 1.017–1.308; p = 0.026), and non-consumption of fruits with a 35% higher risk of T2D (PR: 1.350; 95% CI: 1.146–1.589; p = 0.001).
The final comprehensive model (using Poisson regression) estimated the adjusted PR using overall MEDAS-14 score as the primary dietary exposure, alongside key non-dietary risk factors, like anthropometric and sociodemographic. It was observed that being male, not smoking, and the high adherence to the MEDAS-14 score (≥9) were associated as protective factors against the risk of developing T2D (p <0.05). In contrast, a high BMI and an increased WC were associated with an increased likelihood of T2D risk (Table 6).
4. Discussion
In this study, the analysis of anthropometric, sociodemographic, and dietary factors revealed that being male, non-smoking, and exhibiting high adherence to the MedDiet were associated with a lower risk of developing T2D. This finding underscores a significant public health opportunity: improving adherence to this dietary pattern could provide meaningful benefits. Prior research has shown that each incremental point in the MEDAS score corresponds to a progressive reduction in T2D risk, with high adherence associated with up to a 50% lower incidence of the disease, mediated by enhanced insulin sensitivity, improved lipid metabolism, and reduced systemic inflammation [39]. However, the low adherence found in this study is consistent with observations from other Latin American populations [40,41,42], where cultural and environmental barriers hinder the adoption of the Mediterranean pattern. Nevertheless, traditional Latin American diets, such as corn, legume, and vegetable-based diets in Mexico; rice and beans in Costa Rica; and complex carbohydrate-based diets in Bolivia share core principles of the MedDiet and have shown protective effects against metabolic disorders [43,44,45,46]. Ecuador, however, has undergone a marked nutritional transition, with rural T2D prevalence reaching 20.4% and urban low-income communities showing high rates of obesity and central adiposity, driven by diets poor in fruits and vegetables and high in salt and sugar [47,48].
Regarding specific dietary habits, this study has shown that not preparing sofrito as part of meals was associated with a 15.4% higher risk of T2D and not consuming fruits increased the risk by 35%. Through different studies, fruit-based beverages and purees demonstrated favorable metabolic and vascular effects, including reduced diabetes risk in genetically predisposed populations, low glycemic responses, and improved vascular function and muscle maintenance under training conditions [49,50,51]. Valder et al. suggest that regular consumption of polyphenol rich or low-glycemic fruit preparations may contribute to better metabolic health [49].
The increasing consumption of ultra-processed foods (UPFs) and the decline in home cooking further distance current dietary habits from the MedDiet model [51,52,53,54]. Although our data, initially indicated that participants who consumed carbonated or sugary beverages, which are classified as UPFs, had a 25% higher risk of T2D compared to non-consumers, the association lost statistical significance in the multivariate analysis. Within the MEDAS framework, this behavior represents a marker of low adherence to the Mediterranean dietary pattern, characterized by minimal consumption of added sugars and preference for water or natural beverages. The observed association therefore reinforces the internal consistency of the MEDAS construct, in which items reflecting poor-quality dietary practice-such as regular consumption of sugary drinks-diminish the overall protective potential of the diet. These findings are consistent with extensive evidence linking high intake of sugar-sweetened beverages to adverse metabolic outcomes [55,56,57]. In the Latin American region, where consumption of these beverages remains particularly high, the population-attributable burden of disease is substantial. In Mexico, 19% of deaths from diabetes, cardiovascular disease, and obesity-related cancers are attributable to sugary beverages, with the greatest impact among younger adults and low-income groups [55]. Similar trends are observed in various Latin American countries [30,56], representing a public health concern in the region, and demanding preventive strategies.
Higher consumption of sofrito sauce (≥ 2 servings/week) and fruit (≥ 3 servings/day) were independently associated with a lower risk of developing T2D. These associations remained significant after multivariate adjustment, indicating that individual components of the MEDAS score can exert meaningful metabolic effects even when overall adherence is low. From a mechanistic perspective, these components act synergistically within the Mediterranean dietary pattern to enhance glycemic control and reduce oxidative stress.
The protective association observed for sofrito intake is consistent with the biological plausibility of the Mediterranean dietary model, in which tomato-based dishes prepared with olive oil and vegetables contribute to a high density of bioactive compounds. The sofrito preparation-made with tomato, onion, garlic, and oil, is rich in carotenoids, lycopene, organosulfur compounds, and other bioactive molecules with anti-inflammatory and antioxidant properties. Lycopene, the main carotenoid in tomatoes, helps reduce oxidative stress and lipid peroxidation, processes known to impair insulin signaling and glucose metabolism [57,58]. Polyphenols from olive oil and vegetables exert anti-inflammatory effects by inhibiting pro-inflammatory cytokines and modulating pathways such as NF-κB and PPARγ, which are closely related to glucose metabolism and insulin action [59,60,61]. Additionally, organosulfur compounds from garlic and onion display hypoglycemic effects by enhancing insulin secretion and protecting pancreatic β-cells, as well as reducing systemic inflammation [62,63,64]. Collectively, these mechanisms align with the broader biological rationale of the MedDiet, where the synergistic interaction of multiple plant-derived foods and healthy fats contributes to improved metabolic outcomes and lower risk of T2D.
Although beneficial elements of the MedDiet such as sofrito are present in Ecuadorian cuisine, their potential protective effects may be diminished by dietary patterns dominated by refined oils, flours, and processed carbohydrates that elevate glycemic load and worsen lipid profiles. Unlike the MedDiet, which prioritizes extra virgin olive oil as a source of monounsaturated fats and polyphenol, Ecuadorian households commonly use refined sunflower, soybean or palm oils [65], which lack the bioactive compounds responsible for much of olive oil’s cardioprotective effects [65].
In the multivariate models, higher BMI and WC were consistently associated with an increased risk of developing T2D, whereas a contrasting finding emerged that greater SMM was independently associated with a reduced risk of T2D. This protective association was distinct and statistically significant in the sex-specific adjusted models, which rigorously controlled for adiposity factors. These findings reinforce the well-established role of body composition as a major determinant of metabolic health [66].
About the difference between sexes, being a man was a protective factor of T2D. These sex-specific findings align with prior research showing that fat distribution modulates metabolic risk, with WC differences being more pronounced in women and visceral fat differences greater in men [66]. Hormonal and physiological differences-particularly the divergent effects of testosterone and estradiol on fat deposition and muscle maintenance-may explain these disparities [67].
Conversely, greater skeletal muscle mass was associated with lower risk of T2D, in the sex specific adjusted logistic regression models, but this was substantially attenuated in the final comprehensive models, when it was controlled for the potent confounding effects of BMI and WC. This attenuation does not negate the biological protective role of muscle mass, instead suggesting a profound epidemiological principle: the risk-modifying effect of SMM is likely mediated by the absolute measure of adiposity. Individuals with higher adiposity may present apparent increases in muscle size that are less functional because of fatty infiltration [66]. Moreover, individuals with sarcopenic obesity exhibit a higher risk of T2D than those with obesity or sarcopenia alone [68]. These observations are consistent with prior evidence demonstrating that the Mediterranean dietary pattern contributes to the preservation of muscle mass and the reduction of visceral fat [66,68,69,70]. From a public-health standpoint, these findings suggest that interventions aiming to improve adherence to the MedDiet could simultaneously target adiposity reduction and muscle preservation, amplifying their impact on metabolic health and diabetes prevention.
Our analysis also showed no significant differences in anthropometric indicators (BMI, WC, WHR, body fat and visceral fat) between participants with low versus high MedDiet adherence. However, physical activity displayed a clear relationship with dietary quality: women with higher levels of physical activity were more likely to adhere to the MedDiet, a pattern consistent with evidence indicating that physically active individuals tend to score higher on MEDAS due to greater health awareness and behavioral self-regulation [71,72,73]. This synergy between dietary and physical activity patterns reinforces the holistic nature of the Mediterranean lifestyle, in which diet and movement jointly contribute to metabolic resilience.
Sociodemographic factors were also strongly associated with T2D. Older participants exhibited a higher risk, consistent with the findings of Pan et al., who described that individuals with greater biological age and higher genetic risk showed a markedly higher incidence of type 2 diabetes compared with those presenting lower biological age and genetic risk [74]. Educational attainment also plays a role [75]; participants with university or postgraduate education had significantly higher adherence, consistent with literature linking education to greater health literacy and ability to make informed choices [27,76,77,78,79]. Studies in Ecuador documented a double burden of malnutrition in rural areas, where non-native women more frequently purchase processed foods, while native women predominantly rely on home-produced foods, although they still suffer from micronutrient deficiencies. Dietary diversity remains limited and is strongly influenced by education, income, and food insecurity [80,81].
Lifestyle factors followed similar trends. Our analysis confirmed non-smoking status as a strong protective factor against T2D after multivariate adjustment. Chi et al., demonstrated that smoking status was associated with a higher risk of type 2 diabetes, coronary artery disease, myocardial infarction, and heart failure [82]. This concordance reinforces the hypothesis of shared biological mechanisms linking smoking to insulin resistance.
This study presents several methodological strengths. It was conducted according to STROBE 375 guidelines and included a large, well-powered sample (n=1,373), enhancing the reliability of the findings. The use of validated instruments, MEDAS-14 to assess dietary adherence, FINDRISC to estimate the risk of developing T2D, and IPAQ for physical activity, alongside standardized anthropometric and body composition measurements (including skeletal muscle mass and visceral fat via InBody120) ensured the collection of high-quality, multidimensional data. Importantly, instruments were contextually adapted for the Ecuadorian population, increasing local relevance, and the use of multivariate models allowed for adjustment across sociodemographic, lifestyle, and physiological factors.
Several limitations should be also acknowledged. First, the non-randomized sampling of individuals may limit generalizations of findings to the wider population, though participants were drawn from diverse occupational sectors. Second, cross-sectional design prevents causal inference and raises the possibility of reverse causality. Third, reliance on self-reported questionnaires introduces the potential for recall and social desirability bias. Although both FINDRISC and MEDAS-14 include items on fruit and vegetable consumption, FINDRISC only captures a single dichotomous item on daily intake, whereas MEDAS-14 provides a broader assessment of dietary components and portion-based ranges. In this study, FINDRISC was used strictly as a validated endpoint for the risk of developing T2D estimation, while MEDAS-14 served to characterize dietary patterns.
Additionally, the imbalance between low- and high-adherence groups when applying the standard MEDAS-14 cut-off (<9 vs. ≥9 points) may have reduced statistical power in the high-adherence group. Nevertheless, this cut-off follows validated criteria [27,83] and reflects the true dietary distribution of the population, where low adherence has been documented in other Latin American settings, including the ELANS study across eight countries [84], and among Colombian university students [41].
Finally, the MEDAS-14, although validated and widely applied in Mediterranean and non-Mediterranean contexts, is a simple tool that captures dietary type, frequency, and approximate quantity, without gram-level detail. Its use in Ecuador may not fully reflect cultural and contextual dietary practices, which could affect the precision of dietary exposure measurement. Regarding alcohol consumption, it was assessed only as a lifetime yes/no variable, without capturing type, frequency, or quantity, which limits interpretation, particularly in the context of Mediterranean diet, where moderate wine consumption is considered a traditional component, sour findings regarding alcohol should be interpreted with caution. Furthermore, unmeasured confounders such as stress, sleep quality, and genetic predisposition were not assessed. Future studies in Latin America should incorporate longitudinal designs and more detailed dietary assessment tools, including quantitative food frequency questionnaires and biomarkers-based measures, to strengthen causal inference and improve exposure accuracy.
5. Conclusions
This cross-sectional investigation established context-specific determinants of T2D risk within an urban Ecuadorian cohort, characterized by a prevailing low adherence to the MedDiet pattern. Overall adherence to the MedDiet, when rigorously controlled for the effects of primary anthropometric and lifestyle confounders, demonstrated a statistically significant protective association with T2D risk. Disaggregated analysis revealed highly potent associations tied to specific dietary components and physiological factors, such as the consumption of sofrito sauce and fruits, which were independently associated with significantly lower prevalence ratio of T2D risk. Besides, elevated BMI and WC emerged as the most consistently robust determinants of heightened T2D risk across all models, conversely, greater skeletal muscle mass was independently associated with lower risk in sex-specific models. Additionally, male sex and non-smoking status were identified as significant protective factors, and age as risk factor. These findings underscore the critical value of promoting culturally grounded, specific dietary interventions, such as maximizing sofrito and fruit consumption. Furthermore, public health strategies in Latin America populations could prioritize dual-focus body composition improvements, both reducing central adiposity and preserving or increasing metabolically active muscle mass. Longitudinal research is warranted to confirm the causal pathways suggested by these associations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
LVG: Writing – review & editing, Writing – original draft. EBV: Writing – original draft, Data curation, Formal analysis. VCM: Writing – review & editing. RS: Writing – original draft, Data curation, Writing – review & editing. SC: Writing – original draft. MM: Writing – original draft. PC: Methodology, Conceptualization, Investigation, Resources, Writing – original draft, Writing – review & editing. EFT: Writing – review & editing, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Universidad Técnica Particular de Loja, Ecuador within the code project PROY_PROY_ARTIC_CS_2022_3676.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Bioethics Committee of San Francisco General Hospital (approval code: 031). Written informed consent was obtained from all participants prior to inclusion. Participants were informed of their right to decline participation or withdraw at any time without penalty. Confidentiality was maintained throughout the study by anonymizing all collected data.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data Availability Statement: The data presented in this study are available on request from the corresponding author.
Acknowledgments
We are sincerely thankful to the Ecuadorian Institute of Social Security (IESS), Loja Province, Ecuador, and all subjects being tested for their assistance in our study.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Marques, ES; Formato, E; Liang, W; Leonard, E; Timme-Laragy, AR. Relationships between type 2 diabetes, cell dysfunction, and redox signaling: A meta-analysis of single-cell gene expression of human pancreatic α- and β-cells. J Diabetes 2022, 14[1], 34–51. [Google Scholar] [PubMed]
- Fuster-Parra, P; Yañez, AM; López-González, A; Aguiló, A; Bennasar-Veny, M. Identifying risk factors of developing type 2 diabetes from an adult population with initial prediabetes using a Bayesian network. Front Public Health 2022, 10, 1035025. [Google Scholar] [CrossRef]
- Saeedi, P; Petersohn, I; Salpea, P; Malanda, B; Karuranga, S; Unwin, N; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019, 157, 107843. [Google Scholar] [CrossRef]
- Milenkovic, T; Bozhinovska, N; Macut, D; Bjekic-Macut, J; Rahelic, D; Velija Asimi, Z; et al. Mediterranean Diet and Type 2 Diabetes Mellitus: A Perpetual Inspiration for the Scientific World. A Review. Nutrients 2021, 13[4], 1307. [Google Scholar] [CrossRef]
- Sarsangi, P; Salehi-Abargouei, A; Ebrahimpour-Koujan, S; Esmaillzadeh, A. Association between Adherence to the Mediterranean Diet and Risk of Type 2 Diabetes: An Updated Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv Nutr 2022, 13[5], 1787–98. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L; Verde, L; Simancas-Racines, D; Zambrano, AK; Frias-Toral, E; Colao, A; et al. Adherence to the Mediterranean diet as a possible additional tool to be used for screening the metabolically unhealthy obesity [MUO] phenotype. J Transl Med. 2023, 21[1], 675. [Google Scholar] [CrossRef]
- Kotzakioulafi, E; Bakaloudi, DR; Chrysoula, L; Theodoridis, X; Antza, C; Tirodimos, I; et al. High Versus Low Adherence to the Mediterranean Diet for Prevention of Diabetes Mellitus Type 2: A Systematic Review and Meta-Analysis. Metabolites 2023, 13[7], 779. [Google Scholar] [CrossRef] [PubMed]
- Sleiman, D; Al-Badri, MR; Azar, ST. Effect of mediterranean diet in diabetes control and cardiovascular risk modification: a systematic review. Front Public Health 2015, 3, 69. [Google Scholar] [CrossRef]
- Tosatti, JAG; Alves, MT; Gomes, KB. The Role of the Mediterranean Dietary Pattern on Metabolic Control of Patients with Diabetes Mellitus: A Narrative Review. Adv Exp Med Biol. 2021, 1307, 115–28. [Google Scholar]
- Godos, J; Zappalà, G; Mistretta, A; Galvano, F; Grosso, G. Mediterranean diet, diet quality, and adequacy to Italian dietary recommendations in southern Italian adults. Mediterranean Journal of Nutrition and Metabolism 2024, 17[3], 191–204. [Google Scholar] [CrossRef]
- Ruiz-Pozo, V; Guevara, P; Paz Cruz, E; Tamayo Trujillo, R; Cadena-Ullauri, S; Frias-Toral, E; et al. The role of the Mediterranean diet in prediabetes management and prevention: a review of molecular mechanisms and clinical outcomes. Food and Agricultural Immunology 2024, 35. [Google Scholar] [CrossRef]
- Kiani, AK; Medori, MC; Bonetti, G; Aquilanti, B; Velluti, V; Matera, G; et al. Modern vision of the Mediterranean diet. J Prev Med Hyg. 2022, 63 2 Suppl 3, E36-43. [Google Scholar]
- Chen, Z; Khandpur, N; Desjardins, C; Wang, L; Monteiro, CA; Rossato, SL; et al. Ultra-Processed Food Consumption and Risk of Type 2 Diabetes: Three Large Prospective U.S. Cohort Studies. Diabetes Care 2023, 46[7], 1335–44. [Google Scholar] [CrossRef]
- Du, S; Sullivan, VK; Fang, M; Appel, LJ; Selvin, E; Rebholz, CM. Ultra-processed food consumption and risk of diabetes: results from a population-based prospective cohort. Diabetologia 2024, 67[10], 2225–35. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ramírez, S; Martinez-Tapia, B; González-Castell, D; Cuevas-Nasu, L; Shamah-Levy, T. Westernized and Diverse Dietary Patterns Are Associated With Overweight-Obesity and Abdominal Obesity in Mexican Adult Men. Front Nutr. 2022, 9, 891609. [Google Scholar] [CrossRef]
- Baldeón, ME; Felix, C; Fornasini, M; Zertuche, F; Largo, C; Paucar, MJ; et al. Prevalence of metabolic syndrome and diabetes mellitus type-2 and their association with intake of dairy and legume in Andean communities of Ecuador. PLoS One 2021, 16[7], e0254812. [Google Scholar] [CrossRef] [PubMed]
- Gao, M; Jebb, SA; Aveyard, P; Ambrosini, GL; Perez-Cornago, A; Papier, K; et al. Associations Between Dietary Patterns and Incident Type 2 Diabetes: Prospective Cohort Study of 120,343 UK Biobank Participants. Diabetes Care 2022, 45[6], 1315–25. [Google Scholar] [CrossRef]
- Ochoa-Avilés, A; Verstraeten, R; Lachat, C; Andrade, S; Van Camp, J; Donoso, S; et al. Dietary intake practices associated with cardiovascular risk in urban and rural Ecuadorian adolescents: a cross-sectional study. BMC Public Health 2014, 14, 939. [Google Scholar] [CrossRef] [PubMed]
- Suresh, A; Shobna; Salaria, M; Morya, S; Khalid, W; Afzal, FA; et al. Dietary fiber: an unmatched food component for sustainable health. Food and Agricultural Immunology 2024, 35[1], 2384420. [Google Scholar] [CrossRef]
- Bondonno, NP; Davey, RJ; Murray, K; Radavelli-Bagatini, S; Bondonno, CP; Blekkenhorst, LC; et al. Associations Between Fruit Intake and Risk of Diabetes in the AusDiab Cohort. J Clin Endocrinol Metab. 2021, 106[10], e4097-108. [Google Scholar] [CrossRef]
- Li, H; Christman, LM; Li, R; Gu, L. Synergic interactions between polyphenols and gut microbiota in mitigating inflammatory bowel diseases. Food Funct 2020, 11[6], 4878–91. [Google Scholar]
- Martínez-González, MA; García-Arellano, A; Toledo, E; Salas-Salvadó, J; Buil-Cosiales, P; Corella, D; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: the PREDIMED trial. PLoS One 2012, 7[8], e43134. [Google Scholar]
- Hurtado-Barroso, S; Martínez-Huélamo, M; Rinaldi de Alvarenga, JF; Quifer-Rada, P; Vallverdú-Queralt, A; Pérez-Fernández, S; et al. Acute Effect of a Single Dose of Tomato Sofrito on Plasmatic Inflammatory Biomarkers in Healthy Men. Nutrients 2019, 11[4], 851. [Google Scholar]
- James-Martin, G; Brooker, PG; Hendrie, GA; Stonehouse, W. Avocado Consumption and Cardiometabolic Health: A Systematic Review and Meta-Analysis. J Acad Nutr Diet. 2024, 124[2], 233–248.e4. [Google Scholar] [CrossRef]
- Hirani, K; Sundheim, B; Blaschke, M; Lemos, JRN; Mittal, R. A global call to action: strengthening strategies to combat dysglycemia and improve public health outcomes. Front Public Health 2025, 13, 1597128. [Google Scholar] [CrossRef]
- Probst, Y; Guan, V; Neale, E. Avocado intake and cardiometabolic risk factors in a representative survey of Australians: a secondary analysis of the 2011-2012 national nutrition and physical activity survey. Nutr J 2024, 23[1], 12. [Google Scholar] [CrossRef]
- Guasch-Ferré, M; Willett, WC. The Mediterranean diet and health: a comprehensive overview. J Intern Med. 2021, 290[3], 549–66. [Google Scholar]
- Schwingshackl, L; Morze, J; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. Br J Pharmacol 2020, 177[6], 1241–57. [Google Scholar]
- Dernini, S; Berry, EM. Mediterranean Diet: From a Healthy Diet to a Sustainable Dietary Pattern. Front Nutr 2015, 2, 15. [Google Scholar] [PubMed]
- Matos, RA; Adams, M; Sabaté, J. Review: The Consumption of Ultra-Processed Foods and Non-communicable Diseases in Latin America. Front Nutr. 2021, 8, 622714. [Google Scholar]
- Anza-Ramirez, C; Lazo, M; Zafra-Tanaka, JH; Avila-Palencia, I; Bilal, U; Hernández-Vásquez, A; et al. The urban built environment and adult BMI, obesity, and diabetes in Latin American cities. Nat Commun 2022, 13[1], 7977. [Google Scholar] [CrossRef]
- Suárez, R; Bautista-Valarezo, E; Matos, A; Calderón, P; Fascì-Spurio, F; Castano-Jimenez, J; et al. Obesity and nutritional strategies: advancing prevention and management through evidence-based approaches. Food and Agricultural Immunology 2025, 36[1], 2491597. [Google Scholar] [CrossRef]
- Manual de vigilancia STEPS de la OMS: el método STEPwise de la OMS para la vigilancia de los factores de riesgo de las enfermedades crónicas [Internet]. [citado 8 de enero de 2026]. Available online: https://iris.who.int/items/0d955541-1144-4934-9867-616946337c57.
- Craig, CL; Marshall, AL; Sjöström, M; Bauman, AE; Booth, ML; Ainsworth, BE; et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 2003, 35[8], 1381–95. [Google Scholar] [CrossRef]
- Bernabe-Ortiz, A; Perel, P; Miranda, JJ; Smeeth, L. Diagnostic accuracy of the Finnish Diabetes Risk Score [FINDRISC] for undiagnosed T2DM in Peruvian population. Prim Care Diabetes 2018, 12[6], 517–25. [Google Scholar]
- Carrillo-Larco, RM; Aparcana-Granda, DJ; Mejia, JR; Bernabé-Ortiz, A. FINDRISC in Latin America: a systematic review of diagnosis and prognosis models. BMJ Open Diabetes Res Care 2020, 8[1], e001169. [Google Scholar] [PubMed]
- Silvestre, MP; Jiang, Y; Volkova, K; Chisholm, H; Lee, W; Poppitt, SD. Evaluating FINDRISC as a screening tool for type 2 diabetes among overweight adults in the PREVIEW:NZ cohort. Prim Care Diabetes 2017, 11[6], 561–9. [Google Scholar] [CrossRef]
- Guías de práctica Clínica 2017 – Ministerio de Salud Pública [Internet]. [citado 8 de enero de 2026]. Available online: https://www.salud.gob.ec/guias-de-practica-clinica-2017/.
- Lee, JY; Kim, S; Lee, Y; Kwon, YJ; Lee, JW. Higher Adherence to the Mediterranean Diet Is Associated with a Lower Risk of Steatotic, Alcohol-Related, and Metabolic Dysfunction-Associated Steatotic Liver Disease: A Retrospective Analysis. Nutrients 2024, 16[20], 3551. [Google Scholar] [CrossRef]
- Caizaguano, MAC; Carpio, V; del, PC. Adherence to the mediterranean diet in an urban population of the ecuadorian sierra. Salud, Ciencia y Tecnología 2022, 2, 229–229. [Google Scholar] [CrossRef]
- Vinaccia, S; Serra-Majem, L; Ruano, C; Quintero Marzola, M; Ortega, A; Momo Cabrera, P; et al. Artículo Original Adherencia a la dieta mediterránea en población universitaria colombiana Mediterranean diet adherence in Colombian university population. Nutricion Clinica y Dietetica Hospitalaria 2019, 39, 93–100. [Google Scholar]
- Gómez, G; Fisberg, RM; Nogueira Previdelli, Á; Hermes Sales, C; Kovalskys, I; Fisberg, M; et al. Diet Quality and Diet Diversity in Eight Latin American Countries: Results from the Latin American Study of Nutrition and Health [ELANS]. Nutrients 2019, 11[7], 1605. [Google Scholar] [CrossRef]
- Denova-Gutiérrez, E; Tucker, KL; Flores, M; Barquera, S; Salmerón, J. Dietary Patterns Are Associated with Predicted Cardiovascular Disease Risk in an Urban Mexican Adult Population. J Nutr. 2016, 146[1], 90–7. [Google Scholar] [CrossRef]
- Zhang, Y; Cortés-Ortiz, MV; Baylin, A; Leung, CW; Rosero-Bixby, L; Ruiz-Narváez, EA. Traditional rural dietary pattern and all-cause mortality in a prospective cohort study of elderly Costa Ricans: the Costa Rican Longevity and Healthy Aging Study [CRELES]. Am J Clin Nutr 2024, 120[3], 656–63. [Google Scholar] [CrossRef] [PubMed]
- Valerino-Perea, S; Armstrong, MEG; Papadaki, A. Adherence to a traditional Mexican diet and non-communicable disease-related outcomes: secondary data analysis of the cross-sectional Mexican National Health and Nutrition Survey. Br J Nutr 2023, 129[7], 1266–79. [Google Scholar] [CrossRef]
- Kraft, TS; Stieglitz, J; Trumble, BC; Martin, M; Kaplan, H; Gurven, M. Nutrition transition in 2 lowland Bolivian subsistence populations. Am J Clin Nutr 2018, 108[6], 1183–95. [Google Scholar] [CrossRef] [PubMed]
- Gualan, M; Ster, IC; Veloz, T; Granadillo, E; Llangari-Arizo, LM; Rodriguez, A; et al. Cardiometabolic diseases and associated risk factors in transitional rural communities in tropical coastal Ecuador. PLoS One 2024, 19[7], e0307403. [Google Scholar] [CrossRef]
- Morales-Garzón, S; Vasconez, J; Delgado, JP; Barrera-Guarderas, F; Chilet-Rosell, E; Puig-García, M; et al. The burden of non-communicable disease risk factors in a low-income population: Findings from a cross-sectional study highlighting the prevalence of obesity, hypertension, and metabolic disorders in the south of Quito, Ecuador. PLoS One 2025, 20[9], e0332159. [Google Scholar] [CrossRef]
- Valder, S; Schick, F; Pietsch, N; Wagner, T; Urban, H; Lindemann, P; et al. Effects of two weeks of daily consumption of [poly]phenol-rich red berry fruit juice, with and without high-intensity physical training, on health outcomes in individuals with pre-diabetes mellitus. Nutr Metab Cardiovasc Dis 2025, 35[10], 104121. [Google Scholar] [CrossRef] [PubMed]
- Lecerf, JM; Moreno Aznar, L; Rjimati, L; Atkinson, FS; Richonnet, C. Glycemic and Insulinemic Index Values of Apple Puree. Food Sci Nutr 2025, 13[9], e70844. [Google Scholar] [CrossRef]
- Kawahara, T; Nawa, N; Oze, I; Ikezaki, H; Hara, M; Kubo, Y; et al. Inverse association between fruit juice consumption and type 2 diabetes among individuals with high genetic risk on type 2 diabetes: the Japan Multi-Institutional Collaborative Cohort [J-MICC] study. Br J Nutr. 2025, 134[2], 89–96. [Google Scholar] [CrossRef]
- Watanabe, JA; Nieto, JA; Suarez-Diéguez, T; Silva, M. Influence of culinary skills on ultraprocessed food consumption and Mediterranean diet adherence: An integrative review. Nutrition 2024, 121, 112354. [Google Scholar] [CrossRef]
- Martins, CA; Andrade, GC; de Oliveira, MFB; Rauber, F; de Castro, IRR; Couto, MT; et al. «Healthy», «usual» and «convenience» cooking practices patterns: How do they influence children’s food consumption? Appetite 2021, 158, 105018. [Google Scholar] [CrossRef]
- Sato, P de M; Couto, MT; Wells, J; Cardoso, MA; Devakumar, D; Scagliusi, FB. Mothers’ food choices and consumption of ultra-processed foods in the Brazilian Amazon: A grounded theory study. Appetite 2020, 148, 104602. [Google Scholar] [CrossRef]
- Braverman-Bronstein, A; Camacho-García-Formentí, D; Zepeda-Tello, R; Cudhea, F; Singh, GM; Mozaffarian, D; et al. Mortality attributable to sugar sweetened beverages consumption in Mexico: an update. Int J Obes [Lond] 2020, 44[6], 1341–9. [Google Scholar] [CrossRef]
- Bardach, AE; Espínola, N; Cairoli, FR; Perelli, L; Balan, D; Palacios, A; et al. The burden of disease and economic impact of sugar-sweetened beverages’ consumption in Argentina: A modeling study. PLoS One 2023, 18[2], e0279978. [Google Scholar] [CrossRef]
- Kulawik, A; Cielecka-Piontek, J; Zalewski, P. The Importance of Antioxidant Activity for the Health-Promoting Effect of Lycopene. Nutrients 2023, 15[17], 3821. [Google Scholar] [CrossRef]
- Li, N; Wu, X; Zhuang, W; Xia, L; Chen, Y; Wu, C; et al. Tomato and lycopene and multiple health outcomes: Umbrella review. Food Chem. 2021, 343, 128396. [Google Scholar] [CrossRef]
- Storniolo, CE; Sacanella, I; Lamuela-Raventos, RM; Moreno, JJ. Bioactive Compounds of Mediterranean Cooked Tomato Sauce [Sofrito] Modulate Intestinal Epithelial Cancer Cell Growth Through Oxidative Stress/Arachidonic Acid Cascade Regulation. ACS Omega 2020, 5[28], 17071–7. [Google Scholar] [CrossRef]
- Connolly, LJ; Nordsborg, NB; Nyberg, M; Weihe, P; Krustrup, P; Mohr, M. Low-volume high-intensity swim training is superior to high-volume low-intensity training in relation to insulin sensitivity and glucose control in inactive middle-aged women. Eur J Appl Physiol. 2016, 116[10], 1889–97. [Google Scholar] [CrossRef] [PubMed]
- Dovinova, I; Kvandová, M; Balis, P; Gresova, L; Majzunova, M; Horakova, L; et al. The role of Nrf2 and PPARgamma in the improvement of oxidative stress in hypertension and cardiovascular diseases. Physiol Res. 2020, 69 Suppl 4, S541–53. [Google Scholar] [CrossRef] [PubMed]
- Jideani, AIO; Silungwe, H; Takalani, T; Omolola, AO; Udeh, HO; Anyasi, TA. Antioxidant-rich natural fruit and vegetable products and human health. International Journal of Food Properties [Internet]. 1 de enero de 2021 [citado 9 de marzo de 2025]. Available online: https://www.tandfonline.com/doi/abs/10.1080/10942912.2020.1866597.
- Rinaldi de Alvarenga, JF; Quifer-Rada, P; Westrin, V; Hurtado-Barroso, S; Torrado-Prat, X; Lamuela-Raventós, RM. Mediterranean sofrito home-cooking technique enhances polyphenol content in tomato sauce. J Sci Food Agric. 2019, 99[14], 6535–45. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, V; Rodríguez-Rodríguez, R; Martínez-Garza, Ú; Rosell-Cardona, C; Lamuela-Raventós, RM; Marrero, PF; et al. Mediterranean Tomato-Based Sofrito Sauce Improves Fibroblast Growth Factor 21 [FGF21] Signaling in White Adipose Tissue of Obese ZUCKER Rats. Mol Nutr Food Res 2018, 62[4]. [Google Scholar] [CrossRef]
- Sandoval, LA; Carpio, CE; Sanchez-Plata, M. The effect of «Traffic-Light» nutritional labelling in carbonated soft drink purchases in Ecuador. PLoS One 2019, 14[10], e0222866. [Google Scholar] [CrossRef] [PubMed]
- de Ritter, R; Sep, SJS; van Greevenbroek, MMJ; Kusters, YHAM; Vos, RC; Bots, ML; et al. Sex differences in body composition in people with prediabetes and type 2 diabetes as compared with people with normal glucose metabolism: the Maastricht Study. Diabetologia 2023, 66[5], 861–72. [Google Scholar] [CrossRef]
- Ciardullo, S; Zerbini, F; Cannistraci, R; Muraca, E; Perra, S; Oltolini, A; et al. Differential Association of Sex Hormones with Metabolic Parameters and Body Composition in Men and Women from the United States. J Clin Med. 2023, 12[14], 4783. [Google Scholar] [CrossRef]
- Lu, Z; Hu, Y; He, H; Chen, X; Ou, Q; Liu, Y; et al. Associations of muscle mass, strength, and quality with diabetes and the mediating role of inflammation in two National surveys from China and the United states. Diabetes Res Clin Pract 2024, 214, 111783. [Google Scholar] [CrossRef]
- Suárez, R; Andrade, C; Bautista-Valarezo, E; Sarmiento-Andrade, Y; Matos, A; Jimenez, O; et al. Low muscle mass index is associated with type 2 diabetes risk in a Latin-American population: a cross-sectional study. Front Nutr. 2024, 11, 1448834. [Google Scholar] [CrossRef]
- Jayedi, A; Soltani, S; Motlagh, SZT; Emadi, A; Shahinfar, H; Moosavi, H; et al. Anthropometric and adiposity indicators and risk of type 2 diabetes: systematic review and dose-response meta-analysis of cohort studies. BMJ 2022, 376, e067516. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, JF; García-Hermoso, A; Martínez-González, MÁ; Rodríguez-Artalejo, F. Mediterranean Diet and Cardiometabolic Biomarkers in Children and Adolescents: A Systematic Review and Meta-Analysis. JAMA Netw Open 2024, 7[7], e2421976. [Google Scholar] [CrossRef]
- San Onofre Bernat, N; Quiles, I; Izquierdo, J; Trescastro-López, EM. Health Determinants Associated with the Mediterranean Diet: A Cross-Sectional Study. Nutrients 2022, 14[19], 4110. [Google Scholar] [CrossRef]
- Conde-Pipó, J; Martinez-Amat, A; Mora-Fernández, A; Mariscal-Arcas, M. Impact of Mediterranean Diet Pattern Adherence on the Physical Component of Health-Related Quality of Life in Middle-Aged and Older Active Adults. Nutrients 2024, 16[22], 3877. [Google Scholar] [CrossRef] [PubMed]
- Pan, L; Liu, Y; Huang, C; Huang, Y; Lin, R; Wei, K; et al. Association of accelerated phenotypic aging, genetic risk, and lifestyle with progression of type 2 diabetes: a prospective study using multi-state model. BMC Med 2025, 23[1], 62. [Google Scholar] [CrossRef] [PubMed]
- Rosi, A; Scazzina, F; Giampieri, F; Abdelkarim, O; Aly, M; Pons, J; et al. Adherence to the Mediterranean diet in 5 Mediterranean countries: A descriptive analysis of the DELICIOUS project. 1 de noviembre de 2024 [citado 8 de enero de 2026]. Available online: https://www.growkudos.com/publications/10.1177%252F1973798x241296440.
- Nucci, D; Stacchini, L; Villa, M; Passeri, C; Romano, N; Ferranti, R; et al. The role of Mediterranean diet in reducing household food waste: the UniFoodWaste study among italian students. Int J Food Sci Nutr 2025, 76[4], 443–55. [Google Scholar] [CrossRef]
- Alakaam, A; Lett, M; Puckett, H; Kite, K. Associations among Eating Habits, Health Conditions, and Education Level in North Dakota Adults. Health Behavior and Policy Review 2022, 9. [Google Scholar] [CrossRef]
- Verde, L; Barrea, L; Bowman-Busato, J; Yumuk, VD; Colao, A; Muscogiuri, G. Obesogenic environments as major determinants of a disease: It is time to re-shape our cities. Diabetes Metab Res Rev 2024, 40[1], e3748. [Google Scholar] [CrossRef]
- Nilsen, L; Hopstock, LA; Skeie, G; Grimsgaard, S; Lundblad, MW. The Educational Gradient in Intake of Energy and Macronutrients in the General Adult and Elderly Population: The Tromsø Study 2015-2016. Nutrients 2021, 13[2], 405. [Google Scholar] [CrossRef] [PubMed]
- Melby, CL; Orozco, F; Ochoa, D; Muquinche, M; Padro, M; Munoz, FN. Nutrition and physical activity transitions in the Ecuadorian Andes: Differences among urban and rural-dwelling women. Am J Hum Biol. 2017, 29[4]. [Google Scholar] [CrossRef] [PubMed]
- Melby, CL; Orozco, F; Averett, J; Muñoz, F; Romero, MJ; Barahona, A; et al. Agricultural Food Production Diversity and Dietary Diversity among Female Small Holder Farmers in a Region of the Ecuadorian Andes Experiencing Nutrition Transition. Nutrients [Internet]. 14 de agosto de 2020 [citado 8 de enero de 2026];12[8]. Available online: https://www.mdpi.com/2072-6643/12/8/2454.
- Chi, Y; Wang, X; Jia, J; Huang, T. Smoking Status and Type 2 Diabetes, and Cardiovascular Disease: A Comprehensive Analysis of Shared Genetic Etiology and Causal Relationship. Front Endocrinol [Lausanne] 2022, 13, 809445. [Google Scholar] [CrossRef]
- Schröder, H; Fitó, M; Estruch, R; Martínez-González, MA; Corella, D; Salas-Salvadó, J; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J Nutr. 2011, 141[6], 1140–5. [Google Scholar] [CrossRef]
- Kovalskys, I; Rigotti, A; Koletzko, B; Fisberg, M; Gómez, G; Herrera-Cuenca, M; et al. Latin American consumption of major food groups: Results from the ELANS study. PLoS One 2019, 14[12], e0225101. [Google Scholar] [CrossRef]
Figure 1.
Exclusion criteria included previous T2D diagnosis, pregnancy, and cognitive impairment. Of the 1,388 individuals who met the eligibility criteria, 15 with T2D were excluded, resulting in 1,373.
Figure 1.
Exclusion criteria included previous T2D diagnosis, pregnancy, and cognitive impairment. Of the 1,388 individuals who met the eligibility criteria, 15 with T2D were excluded, resulting in 1,373.
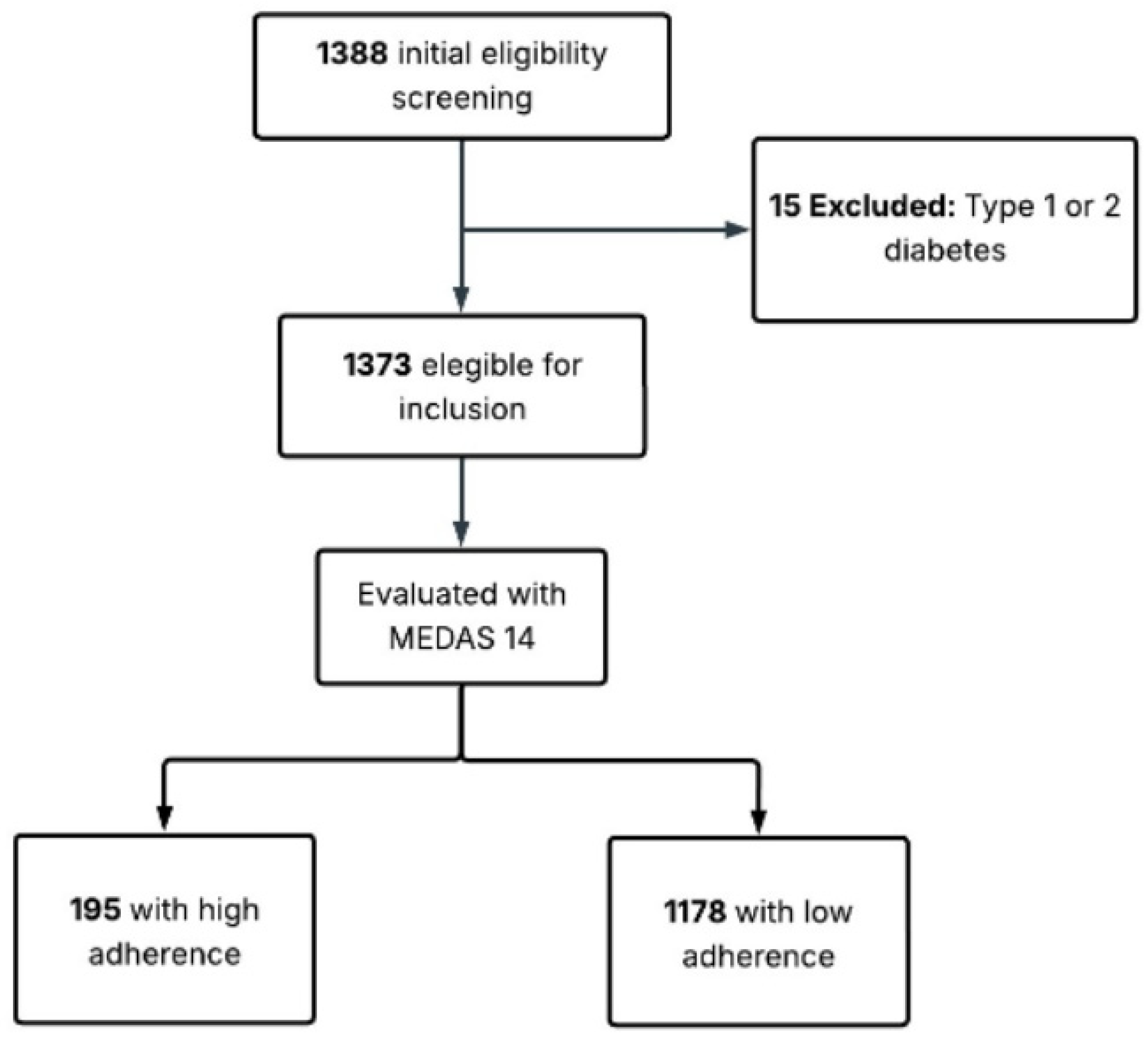

Table 1.
Association between MedDiet adherence and sociodemographic parameters.
| Adherence to MedDiet | |||||
|---|---|---|---|---|---|
| High 195 (14.2%) |
Low 1178 (85.8%)] |
P value | |||
| Age, years | Mean (SD) | 43.56 (10.2) | 40.27 (10.11) | 0.000* | |
| Gender (n,%) | Male | 59 (30.3%) | 490 (41.6%) | 0.003* | |
| Female | 136 (69.7%) | 688 (58.4%) | |||
|
Education (n,%) |
Elementary school | 3 (1.5%) | 41 (3.4%) | 0.002* | |
| High school | 23 (11.8%) | 195 (16.6%) | |||
| College | 98 (50.3%) | 667 (56.6%) | |||
| Graduate | 71 (36.4%) | 275 (23.3%) | |||
|
Current smoker (n,%) |
No | 178 (91.3%) | 1005 (85.3%) | 0.025* | |
| Yes | 17 (8.7%) | 173 (14.7%) | |||
|
Alcohol consumption, last 30 days(n,%) |
No | 97 (49.7%) | 550 (46.7%) | 0.429 | |
| Yes | 98 (50.3%) | 628 (53.3%) | |||
*pvalue<0.005.
Table 2.
Unadjusted and Multivariable Adjusted Prevalence Ratios (PRs) of Type 2 Diabetes Risk Associated with Individual MedDiet Components.
Table 2.
Unadjusted and Multivariable Adjusted Prevalence Ratios (PRs) of Type 2 Diabetes Risk Associated with Individual MedDiet Components.
| T2D Risk | T2D risk (FINDRISC <12) |
T2D risk (FINDRISC >12) |
Unadjusted | Adjusted | ||||
|---|---|---|---|---|---|---|---|---|
| 874 F (%) |
499 F (%) |
RP (95%CI) |
P value | RP (95%CI) |
P value | |||
| MedDiet component | ||||||||
| Olive oil | 302 (67.4%) | 146 (32.6%) | 0.854 (0.704-1.036) |
0.109 | 0,868 (0.711-1.059) |
0.163 | ||
| Vegetablesa | 182 (68.2%) | 85 (31.8%) | 0.850 (0.673-1.074) |
0.174 | 0.889 (0.697-1.133) |
0.341 | ||
| Fruitsa | 212 (69.3%) | 94 (30.7%) | 0.809 (0,647-1.013) |
0.065 | 0.821 (0.654-1.032) |
0.091 | ||
| Processed or red meatsa | 588 (62.6%) | 351 (37.4%) | 1.096 (0.905-1.328) |
0.349 | 1.082 (0.889-1.317) |
0.433 | ||
| Butter or cream or margarinea | 670 (63%) |
394 (37%) |
1.090 (0.879-1.351) |
0.434 | 1.028 (0.823-1.284) |
0.805 | ||
| Carbonated or sugary beveragesa |
621 (61.8%) | 384 (38.2%) | 1.223 (0.993-1.506) |
0.059 |
1.247 (1.002-1.552) |
0.048* | ||
| Winea | 59 [67.8] | 32.2 (%) | 0.879 (0,600-1.287) |
0.506 | 0.982 (0.665-1.448) |
0.925 | ||
| Legumesa | 523 (64.8%) | 284 (35.2%) | 0.926 (0,776-1.106) |
0.398 | 0.960 (0.803-1.149) |
0.660 | ||
| Fisha | 112 (69.1%) | 50 (30.9%) |
0.832 (0,622-1.115) |
0.219 | 0.878 (0.654-1.180) |
0.389 | ||
| Pastries. cakes. cookies or pastaa | 517 (62.2%) | 309 (37.4%) | 1.077 (0.899-1.290) |
0.421 | 1.069 (0.888-1.286) |
0.480 | ||
| Nutsa | 381 (65.1%) | 204 (34.9%) | 0.931 (0.779-1.113) |
0.436 | 0.969 (0.805-1.167) |
0.742 | ||
| Preference for white meata | 723 (63.6%) | 413 (36.4%) | 0.993 (1.333-0.962) |
0.962 | 0.991 (0.782-1.255) |
0.938 | ||
| Sofrito saucea | 593 [66.6%] | 298 [33.4%] | 0.802 [0.671-0.959] |
0.016* | 0.817 [0.682-0.979] |
0.028* | ||
The multivariable adjusted model examine the T2D risk association to variables like a≥ 2 servings/day of vegetables; ≥ 3 servings/day of fruit; < 1/day red or processed meats; < 1/day butter or margarine or cream; > 1/day carbonated or sugary beverages; ≥ 7 glasses/week of wine; ≥ 3 servings/week of legumes; ≥ 3 servings/week of fish; > 2/week industrial pastries. cakes. cookies or pasta; ≥ 3 servings/week of nuts; ≥ 2 servings/week of sofrito sauce with oil and tomato, garlic, onion or leek. * p value<0.005. The scoring criteria for the MEDAS-14 are defined.
Table 3.
Association of Risk Factors with Type 2 Diabetes Risk (Unadjusted and Adjusted ORs) in Males.
Table 3.
Association of Risk Factors with Type 2 Diabetes Risk (Unadjusted and Adjusted ORs) in Males.
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| OR (95%IC) |
P value | OR (95%IC) |
P value | |
| BMI | 1.481 (1.373-1.596) |
<0.001 | 1.303 (1.122-1.513) |
<0.001 |
| WC | 1.167 (1.133-1.201) |
<0.001 | 1.129 (1.068-1.193) |
<0.001 |
| SMM | 1.088 (1.041-1.137) |
<0.001 | 0.907 (0.849-0.970) |
<0.004 |
In the initial logistic regression model, the dependent variable was the risk of type 2 diabetes, and the following covariates were included: educational level, marital status, tobacco and alcohol consumption, blood pressure, body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), skeletal muscle mass (SMM), visceral fat level (VFL), body fat percentage (BFP), and fat mass (FM). A multicollinearity diagnosis was performed using the variance inflation factor (VIF), establishing a cutoff point of VIF > 5 to identify problematic collinearity. As a result, the variables WHR, BFP, and FM were excluded from the final model, with the aim of avoiding multicollinearity and improving the stability of the estimates. P value <0.05.
Table 4.
Association of Risk Factors with Type 2 Diabetes Risk (Unadjusted and Adjusted ORs) in Females.
Table 4.
Association of Risk Factors with Type 2 Diabetes Risk (Unadjusted and Adjusted ORs) in Females.
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| OR (95%IC) |
P value | OR (95%IC) |
P value | |
| BMI | 1.328 (1.265-1.394) |
<0.001 | 1.132 (1.056-1.213) |
<0.001 |
| WC | 1.137 (1.114-1.161) |
<0.001 | 1.094 (1.062-1.127) |
<0.001 |
| SMM | 1.107 (1.056-1.161) |
<0.001 | 0.928 (0.873-0.987) |
0.018 |
Table 5.
Comprehensive model for a combination of anthropometric, sociodemographic, and key individual dietary factors (Fruits, Sofrito, Carbonated or sugary beverages).
Table 5.
Comprehensive model for a combination of anthropometric, sociodemographic, and key individual dietary factors (Fruits, Sofrito, Carbonated or sugary beverages).
| P value |
PR |
(95%IC) Inferior |
Superior |
|
|---|---|---|---|---|
| Gender, (male) | 0,000 | 0,646 | 0,514 | 0,812 |
| Smoke, (don’t smoke) | 0,009 | 0,798 | 0,675 | 0,944 |
| BMI | 0,000 | 1,057 | 1,034 | 1,080 |
| WC | 0,000 | 1,026 | 1,015 | 1,036 |
| SMM | 0,897 | 0,999 | 0,979 | 1,019 |
| Age | 0,000 | 1,036 | 1,029 | 1,043 |
| Fruits (do not Consume) |
0,000 | 1,350 | 1,146 | 1,589 |
| Sofrito (not Prepare) |
0,026 | 1,154 | 1,017 | 1,308 |
| Carbonated or sugary beverages (consume) | 0,841 | 1,015 | 0,877 | 1,175 |
In the generalized regression model, the dependent variable was the risk of developing type 2 diabetes. Sex, tobacco use, fruit consumption, sofrito, carbonated beverages, body mass index (BMI), waist circumference (WC) and skeletal muscle mass (SMM) were included as covariates. To assess the possible presence of multicollinearity among the covariates, the variance inflation factor (IVF) was calculated, considering an IVF value > 5 as an indicator of problematic collinearity. The results showed the absence of multicollinearity between the variables included in the model.
Table 6.
Comprehensive model using the overall Mediterranean Diet score as the primary dietary exposure, alongside key non-dietary risk factors.
Table 6.
Comprehensive model using the overall Mediterranean Diet score as the primary dietary exposure, alongside key non-dietary risk factors.
| P value | PR | 95% CI | ||
|---|---|---|---|---|
| Inferior | Superior | |||
| Gender (male) | <0.001 | 0,658 | 0,526 | 0,823 |
| Smoking (Non- Smoking) |
0,015 | 0,814 | 0,690 | 0,961 |
| BMI | <0.001 | 1,057 | 1,035 | 1,079 |
| WC | <0.001 | 1,026 | 1,016 | 1,037 |
| SMM | 0,688 | 0,996 | 0,976 | 1,016 |
| Age | <0.001 | 1,035 | 1,028 | 1,043 |
| MEDAS-14 score | 0,001 | 0,947 | 0,918 | 0,978 |
In the generalized regression model, the dependent variable was the risk of developing type 2 diabetes. Sex, tobacco use, Mediterranean diet, body mass index (BMI), waist circumference (WC) and skeletal muscle mass (SMM) were included as covariates. To assess the possible presence of multicollinearity among the covariates, the variance inflation factor (IVF) was calculated, considering an IVF value > 5 as an indicator of problematic collinearity. The results showed the absence of multicollinearity between the variables included in the model.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



